immunofluorescent localization of immunoglobulins, plement ...€¦ · immunofluorescent...
TRANSCRIPT

Journal of Clinical InvestigationVol. 44, No. 10, 1965
Immunofluorescent Localization of Immunoglobulins, Com-plement, and Fibrinogen in HumanDiseases. II.
Acute, Subacute, and ChronicGlomerulonephritis *
DAVID KOFFLERt ANDFIoRENZO PARONETTOt(From the Department of Pathology, The Mount Sinai Hospital, New York, N. Y.)
Gammaglobulin and complement have beendemonstrated in renal glomeruli of patients withglomerulonephritis (1-10). Certain problems,which are the subject of the present investigation,remain to be elucidated: 1) the type of immuno-globulin (y2, 71m, or yiA) present in the renal le-sion and its relation to complement localization;and 2) the significance of fibrinogen localization.Kidneys from patients with acute, subacute, andchronic glomerulonephritis were examined by thefluorescent antibody technique to assess the natureof protein deposition in the renal parenchyma.
Methods
Specimens from 17 patients with acute, subacute, andchronic glomerulonephritis were quick-frozen in dry iceand isopentane at -70° C. The methods of tissue fixa-tion, preparation of fluoresceinated antisera, and fluores-cence microscopy have been described in a previous pa-per (11). Histological examination was performed onparaffin sections stained with hematoxylin and eosin andsubjected to the periodic acid Schiff reagent after diastasetreatment. Phosphotungstic acid hematoxylin (PTAH)and Lendrum stains for detection of fibrin were alsoemployed.
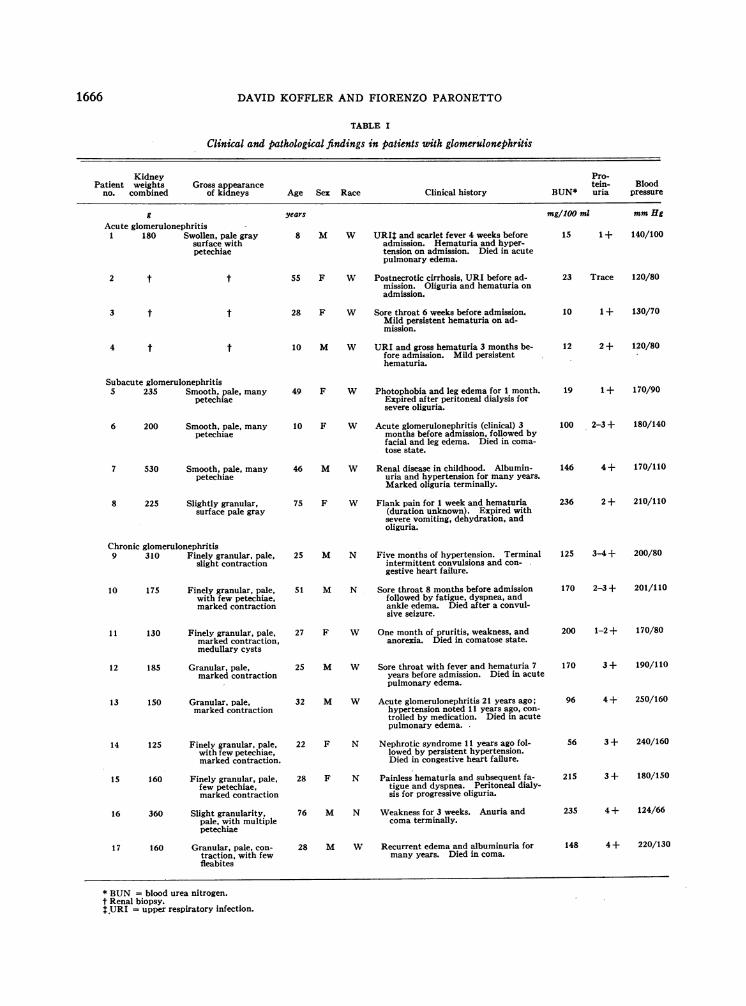
Major clinical and pathological findings pertinent tothe present study are summarized in Table I. Any pa-tient with clinical symptoms suggestive of systemic lupuserythematosus (SLE) was excluded. All patients withsubacute and chronic glomerulonephritis were uremic andhypertensive on their final admissions to the hospital,except for two patients (No. 5 and 16). Autopsy tis-sues were obtained in all cases except for renal biopsiesobtained in three patients with acute glomerulonephritis.
* Submitted for publication March 31, 1965; acceptedJune 28, 1965.
This investigation was supported by U. S. PublicHealth Service grants AM-07790, AM-03846, and AM-20199.
t Research fellow, U. S. Public Health Service.t Address requests for reprints to Dr. Fiorenzo Paro-
netto, The Mount Sinai Hospital, 100th St. and Fifth Ave.,New York, N. Y. 10029.
Acute glomerulonephritis. Patients 1 and 2 showedacute proliferative glomerulonephritis with marked swell-ing and proliferation of glomerular capillary endothelium.Focal hemorrhage was noted in Bowman's space andwithin tubules. Patients 3 and 4 revealed a milder de-gree of glomerular endothelial swelling and proliferationwithout hemorrhage.
Subacute glomerulonephritis. All patients exhibiteddiffuse proliferative glomerulonephritis with extensivecrescent formation and occasional partially hyalinizedglomerular tufts. There were intimal proliferation andthickening of medium sized arterioles. In Patient 6, seg-mental fibrinoid- necrosis and hemorrhage were found inthe media of several arterioles.
Chronic glomerulonephritis. All patients revealedmoderate to severe sclerosing glomerulonephritis withpartial or complete hyalinization of glomerular tufts,atrophy, and concomitant hypertrophy of tubules and in-terstitial fibrosis. Glomerular obliteration was of great-est severity in Patients 11, 13, and 14. Patient 11, inaddition to stigmata of chronic glomerulonephritis, hadmultiple medullary cysts involving collecting tubules.
Arterioles uniformly demonstrated medial hypertrophyand intimal proliferation, but vascular necrosis was notobserved.
Results
Immunoglobulin localization. Gamma2-and ylm-globulins were demonstrated in glomeruli in allstages of glomerulonephritis (Table II). Theseproteins appeared to be deposited in a diffusemembranous fashion throughout the glomerulus(Figure 1), and they could be partially eluted byacid buffer. Occasionally, homogeneous foci offluorescence were noted at the hilus or in partiallyhyalinized glomerular tufts. Gammaglobulin depo-sition was usually limited to intact, nonhyalinizedglomeruli. Patients with acute glomerulonephritisshowed a few glomeruli containing Y2- and yim-globulins. In subacute glomerulonephritis glo-meruli were stained with greater frequency and in-tensity than in chronic glomerulonephritis. Stain-ing for ylA-globulin did not reveal a membranous
1665
DAVID KOFFLERAND FIORENZO PARONETTO
TABLE I
Clinical and pathological findings in patients with glomerulonephritis
Kidney Pro-Patient weights Gross appearance tein- Blood
no. combined of kidneys Age Sex Race Clinical history BUN* uria pressure
g years mg/100 ml mmHgAcute glomerulonephritis
1 180 Swollen, pale graysurface withpetechiae
2 t t
3 t t
4 t t
Subacute glomerulonephritis5 235 Smooth, pale, many
petechiae
6 200 Smooth, pale, manypetechiae
7 530 Smooth, pale, manypetechiae
8 225 Slightly granular,surface pale gray
8 M W URIt and scarlet fever 4 weeks beforeadmission. Hematuria and hyper-tension on admission. Died in acutepulmonary edema.
55 F W Postnecrotic cirrhosis, URI before ad-mission. Oliguria and hematuria onadmission.
28 F W Sore throat 6 weeks before admission.Mild persistent hematuria on ad-mission.
10 M W URI and gross hematuria 3 months be-fore admission. Mild persistenthematuria.
49 F W Photophobia and leg edema for 1 month.Expired after peritoneal dialysis forsevere oliguria.
10 F W Acute glomerulonephritis (clinical) 3months before admission, followed byfacial and leg edema. Died in coma-tose state.
46 M W Renal disease in childhood. Albumin-uria and hypertension for many years.Marked oliguria terminally.
75 F W Flank pain for 1 week and hematuria(duration unknown). Expired withsevere vomiting, dehydration, andoliguria.
15 1 + 140/100
23 Trace 120/80
10 1 + 130/70
12
19
2 + 120/80
1 + 170/90
100 2-3 + 180/140
146 4+ 170/110
236 2 + 210/110
Chronic glomerulonephritis9 310 Finely granular, pale,
slight contraction
10 175 Finely granular, pale,with few petechiae,marked contraction
11 130 Finely granular, pale,marked contraction,medullary cysts
12 185 Granular, pale,marked contraction
13 150 Granular, pale,marked contraction
14 125 Finely granular, pale,with few petechiae,marked contraction.
15 160 Finely granular, pale,few petechiae,marked contraction
16 360 Slight granularity,pale, with multiplepetechiae
17 160 Granular, pale, con-traction, with fewfleabites
25 M N Five months of hypertension. Terminalintermittent convulsions and con-gestive heart failure.
51 M N Sore throat 8 months before admissionfollowed by fatigue, dyspnea, andankle edema. Died after a convul-sive seizure.
27 F W One month of pruritis, weakness, andanorexia. Died in comatose state.
25 M W Sore throat with fever and hematuria 7years before admission. Died in acutepulmonary edema.
32 M W Acute glomerulonephritis 21 years ago;hypertension noted 11 years ago, con-trolled by medication. Died in acutepulmonary edema.
22 F N Nephrotic syndrome 11 years ago fol-lowed by persistent hypertension.Died in congestive heart failure.
28 F N Painless hematuria and subsequent fa-tigue and dyspnea. Peritoneal dialy-sis for progressive oliguria.
76 M N Weakness for 3 weeks. Anuria andcoma terminally.
28 M W Recurrent edema and albuminuria formany years. Died in coma.
125 3-4+ 200/80
170 2-3 + 201/110
200 1-2 + 170/80
170 3 + 190/110
96 4 + 250/160
56 3 + 240/160
215 3 + 180/150
235 4 + 124/66
148 4+ 220/130
* BUN = blood urea nitrogen.t Renal biopsy.tURI = upper respiratory infection.
1666

IMMUNOGLOBULINS,COMPLEMENT,AND FIBRINOGEN IN GLOMERULONEPHRITIS
TABLE II
Renal localization of immunoglobulins, complement, and fibrinogen in glomerulonephritis
Pic-Globulinin vitro
Patient no. .Y2-Globulin* -yiM-Globulin -yiA-Globulin Fibrinogen Pc-Globulin fixation
Acuteglomerulonephritis
1 + 0 0 + ++ ++2 ++ i1 + ++3 + + ++4 + + ++
Subacuteglomerulonephritis + + + + 0 + + + + +
5 d vessels ± vessels :1: vessels 4± vessels6 i +
4 vessels + vessels7 ++ + ++8 ++ + + i1
Chronicglomerulonephritis ++ + + + + ++ + + +
9 :1 vessels :1= vessels 1 vessels10 4 + 0 + 4 ++11 + + + + ± :112 ++ + 0 ++ + ++13 + + 0 4 + +14 + + 0 + +15 ++ + ±
+ vessels ± vessels + vessels16 + + +
+ vessels ± vessels :1 vessels17 + :1 0 ++ +++ +++
+ vessels + vessels + + vessels
*0 = negative; 1 = rare glomerulus or vessel; + = few glomeruli or vessels; + + = moderate number of glomerulior vessels; + + + = many glomeruli or vessels; blank space = not done.
distribution in glomeruli at any stage of glomeru-lonephritis, but occasionally focal interstitial fluor-escence was observed in the subacute and chronicstages. Tubular epithelium was stained by anti-YIA-serum (Figure 2), in all stages of glomerulo-nephritis, but occasionally weak fluorescence withanti--y2- and ylm-sera was also present. GammalAlocalization in tubular epithelium was most markedin cases of chronic glomerulonephritis with severeproteinuria. Deposits of immunoglobulins wererarely observed in the walls of the small arterioles,some of which showed fibrinoid degeneration (Pa-tient 6).
Betale-globulin localization. Complement wasdeposited in the renal glomerulus in a pattern simi-lar to Y2- and ylM-globulins. The glomerularfluorescence was least intense in cases of chronicglomerulonephritis. When sections from thesekidneys were incubated with fresh human serumbefore treatment with fluoresceinated anti-comple-ment serum, a marked increase in fluorescence wasnoted (Figure 3). Acute and subacute glomerulo-nephritis showed more significant in vivo deposi-
tion of complement in glomeruli. Complementwas not present in tubular epithelium, although anoccasional cast was positively stained. Blood ves-
FIG. 1. DIFFUSE FLUORESCENCEIN A RENAL GLOMERU-LUS STAINED FOR y2-GLOBULIN. Note bright homogeneousfluorescence in partially hyalinized tuft (arrow). Chronicglomerulonephritis, Patient 12 (X 250).
1667

DAVID KOFFLERAND FIORENZO PARONETTO
in a few glomeruli when sections were incubatedwith antifibrinogen serum.
Membranous and interstitial deposition of fibrin-ogen in glomeruli (Figure 4A) and diffuse locali-zation in some crescents were observed in subacuteand chronic glomerulonephritis. Many glomeruliin which fibrinogen could be localized also con-
FIG. 2. TUBULAREPITHELIAL CELLS STAINED BY ANTI-Y1A-GLOBULIN SERUM. Chronic glomerulonephritis, Pa-tient 12 (X250).
sels exhibiting immunoglobulins also containedcomplement.
Fibrinogen localization. In acute glomerulo-nephritis, patchy interstitial staining was observed
FIG. 3. SEGMENTOF GLOMERULUSSHOWINGBASEMENTMEMBRANEFLUORESCENCEAFTER TREATMENTWITH FRESHHUMANSERUMFOLLOWEDBY FLUORESCEINATEDANTI-Pio-GLOBULIN SERUM. Chronic glomerulonephritis, Patient12 (X970).
FIG. 4. RENAL GLOMERULI EXHIBITING FIBRINOGEN LO-CALIZATION DEMONSTRATEDBY STAINING WITH FLUORES-CEINATED ANTIHUMAN FIBRINOGEN SERUM. A. Diffusemembranous and interstitial glomerular fluorescence.Chronic glomerulonephritis, Patient 12 (X 400). B.Partially hyalinized glomerulus with undulating mem-branous structure exhibiting fluorescence. Chronic glo-merulonephritis, Patient 12 (X400).
1668
IMMUNOGLOBULINS,COMPLEMENT,AND FIBRINOGEN IN GLOMERULONEPHRITIS
tained Y2- and -yiM-globulins. Partially or almostcompletely hyalinized glomeruli in advanced glo-merulonephritis contained undulating membranousstructures brightly stained with antifibrinogen se-rum and weakly stained by anti-y2-sera (Figure4B). Blood vessels with immunoglobulins andcomplement deposition showed fibrinogen depositsas well. PTAHand Lendrum stains revealed rarefocal fibrin deposits in crescents and glomer-uli of subacute and chronic glomerulonephritis. Amembranous fibrin distribution was not demon-strable by these stains.
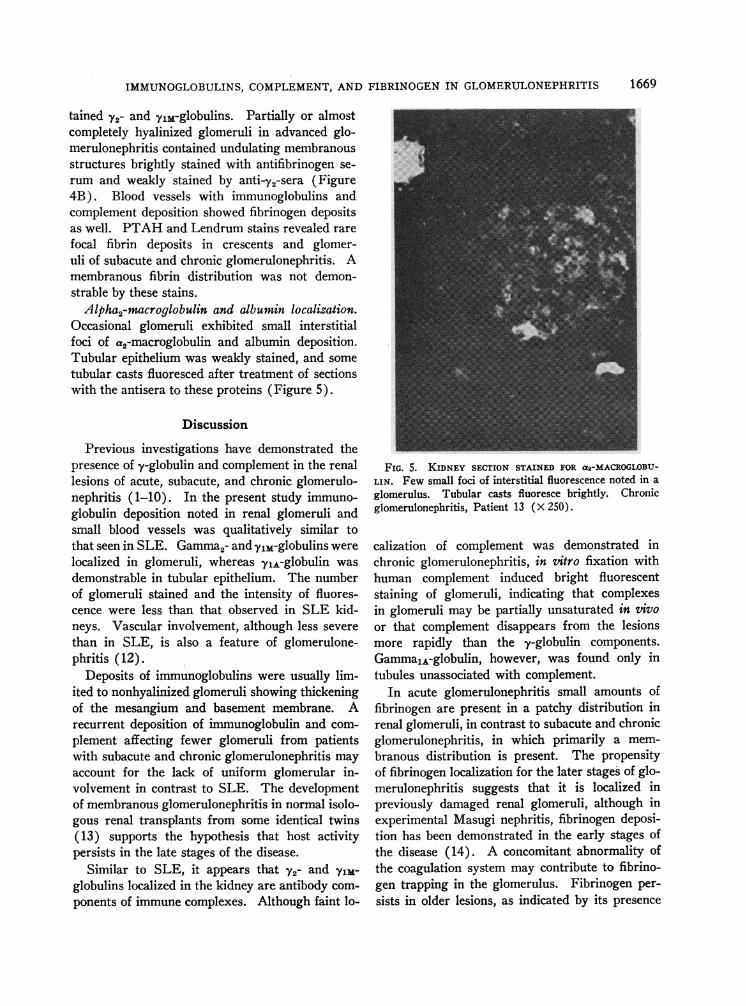
Alpha2-macroglobulin and albumin localization.Occasional glomeruli exhibited small interstitialfoci of %2-macroglobulin and albumin deposition.Tubular epithelium was weakly stained, and sometubular casts fluoresced after treatment of sectionswith the antisera to these proteins (Figure 5).
Discussion
Previous investigations have demonstrated thepresence of y-globulin and complement in the renallesions of acute, subacute, and chronic glomerulo-nephritis (1-10). In the present study immuno-globulin deposition noted in renal glomeruli andsmall blood vessels was qualitatively similar tothat seen in SLE. Gamma2-and yjM-globulins werelocalized in glomeruli, whereas ylA-globulin wasdemonstrable in tubular epithelium. The numberof glomeruli stained and the intensity of fluores-cence were less than that observed in SLE kid-neys. Vascular involvement, although less severethan in SLE, is also a feature of glomerulone-phritis (12).
Deposits of immunoglobulins were usually lim-ited to nonhyalinized glomeruli showing thickeningof the mesangium and basement membrane. Arecurrent deposition of immunoglobulin and com-plement affecting fewer glomeruli from patientswith subacute and chronic glomerulonephritis mayaccount for the lack of uniform glomerular in-volvement in contrast to SLE. The developmentof membranous glomerulonephritis in normal isolo-gous renal transplants from some identical twins(13) supports the hypothesis that host activitypersists in the late stages of the disease.
Similar to SLE, it appears that Y2- and ylm-globulins localized in the kidney are antibody com-ponents of immune complexes. Although faint lo-
FIG. 5. KIDNEY SECTION STAINED FOR a2-MACROGLOBU-LIN. Few small foci of interstitial fluorescence noted in aglomerulus. Tubular casts fluoresce brightly. Chronicglomerulonephritis, Patient 13 (X 250).
calization of complement was demonstrated inchronic glomerulonephritis, in vitro fixation withhuman complement induced bright fluorescentstaining of glomeruli, indicating that complexesin glomeruli may be partially unsaturated in tivoor that complement disappears from the lesionsmore rapidly than the y-globulin components.GammalA-globulin, however, was found only intubules unassociated with complement.
In acute glomerulonephritis small amounts offibrinogen are present in a patchy distribution inrenal glomeruli, in contrast to subacute and chronicglomerulonephritis, in which primarily a mem-branous distribution is present. The propensityof fibrinogen localization for the later stages of glo-merulonephritis suggests that it is localized inpreviously damaged renal glomeruli, although inexperimental Masugi nephritis, fibrinogen deposi-tion has been demonstrated in the early stages ofthe disease (14). A concomitant abnormality ofthe coagulation system may contribute to fibrino-gen trapping in the glomerulus. Fibrinogen per-sists in older lesions, as indicated by its presence
1669

DAVID KOFFLERAND FIORENZO PARONETTO
in partially hyalinized glomerulus, and it may con-tribute to the glomerulosclerotic process (15).Demonstration of this protein in SLE (11), toxe-mia of pregnancy (16), renal cortical necrosis(17), periarteritis nodosa (18), and malignantnephrosclerosis (19, 20) indicates that it is not aunique feature of glomerulonephritis. The failureof histochemical stains to detect the membranousdistribution of fibrinogen may be related to the oc-currence of urea soluble fibrinogen polymers inthe basement membrane (21).
The striking similarity of the immunoglobulin,complement, and fibrinogen localization in patientswith glomerulonephritis and SLE may imply acommon immunologic pathogenesis. The selectivedeposition of two immunoglobulins and complementin renal glomeruli, and the similarity of the glo-merular distribution of y-globulin and comple-ment to experimental immunologic renal disease(22, 23) support the hypothesis that antibody isan etiologic factor. Differences in the antigenicmoieties of the immune complexes and in the in-tensity of the antibody response to these antigensmay be reflected in the more prolonged course ofchronic glomerulonephritis.
Summary
Gamma2- and ylm-globulins in association withcomplement and fibrinogen have been localized inthe glomeruli of kidneys showing acute, subacute,and chronic glomerulonephritis. GammalA-globu-lin was present in tubular epithelium in the ab-sence of complement. Complement was also fixedto glomeruli in vitro. The similarity of immuno-logical findings in systemic lupus erythematosusand glomerulonephritis implies a common injuryinduced by antigen-antibody complexes and pos-sibly by fibrinogen.
Acknowledgments
We gratefully acknowledge the excellent technical as-sistance of Miss Patricia Saigo and Miss Sara Echever-ria-Cruz, the encouragement and criticism of Dr. HansPopper, and the help of Dr. Mardoqueo Salomon, whogranted us permission to study two of his patients.
References
1. Mellors, R. C., and L. G. Ortega. Analytical pa-thology. III. New observations on the pathogene-
sis of glomerulonephritis, lipid nephrosis, periar-teritis nodosa, and secondary amyloidosis in man.Amer. J. Path. 1956, 32, 455.
2. Mellors, R. C., L. G. Ortega, and H. R. Holman.Role of gamma globulins in pathogenesis of renallesions in systemic lupus erythematosus and chronicmembranous glomerulonephritis, with an observa-tion on the lupus erythematosus cell reaction. J.exp. Med. 1957, 106, 191.
3. Taft, L. I., J. K. Dineen, and I. R. MacKay. Lo-calization and binding of serum proteins in glo-meruli of kidney biopsies in disseminated lupuserythematosus and glomerulonephritis. Aust. Ann.Med. 1958, 7, 5.
4. Freedman, P., J. H. Peters, and R. M. Kark. Lo-calization of gamma-globulin in the diseased kid-ney. Arch. intern. Med. 1960, 105, 524.
5. MacKay, I. R., and L. I. Taft. Renal biopsy. Withparticular reference to the study of diabetes mel-litus, systemic lupus erythematosus and subacuteglomerulonephritis. Aust. Ann. Med. 1961, 10,178.
6. Burkholder, P. M. Complement fixation in diseasedtissues. I. Fixation of guinea pig complement insections of kidney from humans with membranousglomerulonephritis and rats injected with anti-rat kidney serum. J. exp. Med. 1961, 114, 605.
7. Freedman, P., and A. S. Markowitz. Gammaglobu-lin and complement in the diseased kidney. J. clin.Invest. 1962, 41, 328.
8. Lachmann, P. J., H. J. Muiller-Eberhard, H. G.Kunkel, and F. Paronetto. The localization of invivo bound complement in tissue sections. J. exp.Med. 1962, 115, 63.
9. Burkholder, P. M. Complement fixation in diseasedtissues. II. Fixation of guinea pig complement inrenal lesions of systemic lupus erythematosus.Amer. J. Path. 1963, 42, 201.
10. Seegal, B. C., G. A. Andres, K. C. Hsu, and J. B.Zabriski. Studies on the pathogenesis of acute andprogressive glomerulonephritis in man by immuno-fluorescein and immunoferritin techniques. Fed.Proc. 1965, 24, 100.
11. Paronetto, F., and D. Koffler. Immunofluorescent lo-calization of immunoglobulins, complement, andfibrinogen in human diseases. I. Systemic lupuserythematosus. J. clin. Invest. 1965, 44, 1657.
12. Fishberg, A. M. The arteriolar lesions of glomeru-lonephritis. Arch. intern. Med. 1927, 40, 80.
13. Murray, J. E., J. P. Merrill, and J. H. Harrison.Kidney transplantation between seven pairs ofidentical twins. Ann. Surg. 1958, 148, 343.
14. Vassalli, P., and R. T. McCluskey. The pathogenicrole of the coagulation process in rabbit Masuginephritis. Amer. J. Path. 1964, 45, 653.
15. Vassalli, P., G. Simon, and C. Rouiller. Electronmicroscopic study of glomerular lesions resultingfrom intravascular fibrin formation. Amer. J.Path. 1963, 43, 579.
1670

IMMUNOGLOBULINS,COMPLEMENT,AND FIBRINOGEN IN GLOMERULONEPHRITIS
16. Vassalli, P., R. H. Morris, and R. T. McCluskey.The pathogenic role of fibrin deposition in theglomerular lesions of toxemia of pregnancy. J.exp. Med. 1963, 118, 467.
17. Koffler, D., and F. Paronetto. Unpublished observa-tions.
18. Paronetto, F., and L. Strauss. Immunocytochemicalobservations in periarteritis nodosa. Ann. intern.Med. 1962, 56, 289.
19. Paronetto, F. Immunocytochemical observations on
the vascular necrosis and renal glomerular lesionsof malignant nephrosclerosis. Amer. J. Path. 1965,46, 901.
20. Fennel, R. H., Jr., C. R. R. M. Reddy, and J. J.Vazquez. Progressive systemic sclerosis and ma-
lignant hypertension. Arch. Path. 1961, 72, 209.21. Gitlin, D., and J. M. Craig. Variations in the stain-
ing characteristics of human fibrin. Amer. J.Path. 1957, 33, 267.
22. Dixon, F. J., J. D. Feldman, and J. J. Vazquez. Ex-perimental glomerulonephritis. The pathogenesisof a laboratory model resembling the spectrum ofhuman glomerulonephritis. J. exp. Med. 1961, 113,899.
23. Unanue, E., and F. J. Dixon. Experimental glomeru-lonephritis. IV. Participation of complement innephrotoxic nephritis. J. exp. Med. 1964, 119, 965.
1671