immunoglobulin rearrangement immunoproliferative
TRANSCRIPT
J Clin Pathol 1987;40:1291-1297
Immunoglobulin gene rearrangement inimmunoproliferative small intestinal disease (IPSID)
WENDY J SMITH, S K PRICE,* P G ISAACSON
From the Department ofHistopathology, School ofMedicine, University College London and the *DepartmentofPathology, Medical School, University ofCape Town, Observatory, South Africa
SUMMARY Analysis of DNA from the mucosal tissue of three patients with immunoproliferativesmall intestinal disease (IPSID) and a chain disease, two ofwhom had early stage disease responsiveto antibiotics, showed monoclonal heavy and light chain gene rearrangements in all cases. Thesefindings suggest that IPSID is neoplastic even in its early stages, but that the neoplastic cells respondto normal stimuli. Monoclonal lymphoid populations could not be detected in circulating lympho-cytes from these patients, which raises the possibility that the circulatory pathways of lymphocytesderived from human gut associated lymphoid tissue may not necessarily parallel those in experi-mental animals.
Immunoproliferative small intestinal disease (IPSID)occurs predominantly, but not exclusively, in theMiddle East, and is characterised by diarrhoea,weight loss, abdominal pain and finger clubbing.'2The pathological basis of these features is a heavyplasmacytic or lymphoplasmacytic infiltrate of theupper small intestinal mucosa and related mesentericlymph nodes. In most, if not all, cases these plasmacells synthesise, without necessarily secreting,3an abnormal a, immunoglobulin heavy chain(a chain disease). Malignant intestinal lymphoma(Mediterranean lymphoma) often arises in the settingof IPSID and opinions are divided as to whetherIPSID is a malignant proliferation de novo orwhether the onset of Mediterranean lymphoma repre-sents a complication of a benign disorder.'24 Thelatter view is supported by the evident response ofsome cases of uncomplicated IPSID to broad spec-trum antibiotics' 245 while cases of Mediterraneanlymphoma require more radical treatment. Decisionsregarding treatment are based on the interpretation ofthe histology of intestinal biopsy specimens.' The his-topathological differential diagnosis between uncom-plicated IPSID and Mediterranean lymphoma can,however, be extremely difficult and is subject to sam-pling error.
Central to the argument on the nature of the lym-phoproliferation in IPSID, and hence the optimum
Accepted for publication 2 June 1987
choice of treatment, is the clonality of the mucosalplasma cell infiltrate in the early stages of the disease.The absence of light chains and the loss of the vari-able region of the abnormal cxl heavy chain precludesthe use of the two most common criteria of mono-clonality: light chain restriction and monoclonal idi-otype expression. Although cases showing light chainrestriction have been described,6 7 these were in estab-lished cases of Mediterranean lymphoma rather thanin examples of early IPSID. Accordingly, we analysedthe DNA from three cases of IPSID for evidence ofmonoclonal rearrangements of both heavy and lightchain immunoglobulin genes. Two cases were exam-ples of early IPSID that had responded to conser-vative treatment and one was of establishedMediterranean lymphoma. All three patients werefrom the Cape region of South Africa, where IPSID isa well recognised disease.
Patients and methods
CASE 1A 26 year old woman complained of diarrhoea andabdominal pain associated with a weight loss of 6 kg.Apart from emaciation, there were no abnormalphysical findings. Gastroduodenoscopy showed slightnodularity of the first part of the duodenum. The onlyclinically important biochemical finding was the pres-ence of serum a chains. The duodenal biopsy speci-men was consistent with a diagnosis of IPSID and the
1291
copyright. on D
ecember 2, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.11.1291 on 1 Novem
ber 1987. Dow
nloaded from
1292patient underwent a staging laparotomy with fullthickness jejunal and mesenteric lymph node biopsy,at which time fresh tissue was collected. Treatmentconsisted initially of metronizadol to eradicate Giar-dia followed by long term tetracycline 1 g twice a day.Six months after diagnosis the patient remained well,having regained her original weight. Serum a chainswere undetectable. Fourteen months after diagnosis,when peripheral blood was taken, she remained welland was 30 weeks pregnant at the time of writing.
CASE 2A 20 year old man gave a four year history of diar-rhoea and a weight loss of 18 kg. Examinationshowed that he was physically wasted with no otherclinically important findings. Gastroduodenoscopyyielded normal results as did biochemicalinvestigations, except for the presence of serum achain. Laparotomy with full thickness jejunal andmesenteric lymph node biopsy was carried out andfresh tissue retained. Peripheral blood was collectedsimultaneously. The patient started on tetracycline 1 gtwice a day and parenteral nutrition-with pro-nounced clinical improvement. A follow up jejunalbiopsy at four months was unchanged.
CASE 3A 15 year old boy gave a three month history ofabdominal pain, weight loss, and diarrhoea.Examination showed general wasting and clubbing ofhis nails. Gastroduodenoscopy showed nodularinfiltration of the duodenum; serum a chain waspresent. Laparotomy showed thickening of the entiresmall intestine with enlarged mesenteric lymph nodes,and full thickness jejunal and mesenteric lymph nodebiopsy specimens were taken and submitted fresh.Prednisone 40mg daily, tetracycline 500mg twicedaily, and parenteral nutrition were started. At followup 15 months after admission the patient remainedsymptomatic and a chain was still detectable in hisserum. Peripheral blood was collected at this time.Follow up biopsies were refused by the patient whothen received total abdominal irradiation with goodclinical response.
Standard formalin fixed, paraffin embedded sec-tions from the full thickness jejunal and mesentericlymph node biopsy specimens were prepared andstained with haematoxylin and eosin. Immuno-histochemistry was performed on these and on cryo-stat sections prepared from fresh tissue, snap frozenin liquid nitrogen. Sections were stained with anti-bodies to all immunoglobulin heavy and light chainand selected B cell and T cell antigens.
Frozen sections were prepared from tissue snapfrozen in liquid nitrogen to check that the tissue beingsubmitted for DNA analysis was representative. After
Smith, Price, Isaacsoncollection in edetic acid, lymphocytes from peripheralblood from all three patients were separated on a Fic-oll hypaque gradient, harvested, and snap frozen inliquid nitrogen. High molecular weight DNA wasextracted by standard methods from the biopsy speci-mens and peripheral blood lymphocytes.8 Afterdigestion with HindlIl, EcoRI, BamHl, and BglIIrestriction enzymes the fragments were separatedaccording to size on an agarose gel by electrophoresisand Southern blots9 prepared using Gene Screen Plusfilters (DuPont). Table 1 details the recombinantDNA probes used and their sources. They were radio-labelled with 32P-dCTP by the random hexa-nucleotide method10 and hybridised to the filtersunder conditions recommended by the manufacturer.After stringent washing the filters were exposed topre-fogged x-ray film.
Results
The histological appearances (table 2) of the biopsyspecimens in cases 1 and 2 showed a dense plasma cellinfiltrate confined by the muscularis mucosae. Thiswas focal in case 1, whose biopsy specimen alsoshowed lymphoepithelial lesions,' 1 and diffuse in case2. The lymph node of case 1 showed reactive hyper-plasia while that of case 2 showed infiltration withmature plasma cells. The small intestinal biopsy speci-men of case 3 showed a nodular mucosal lympho-plasmacytic infiltrate which breached the muscularismucosae. Lymphoepithelial lesions were 'present;lymph node architecture was effaced by a similarinfiltrate.
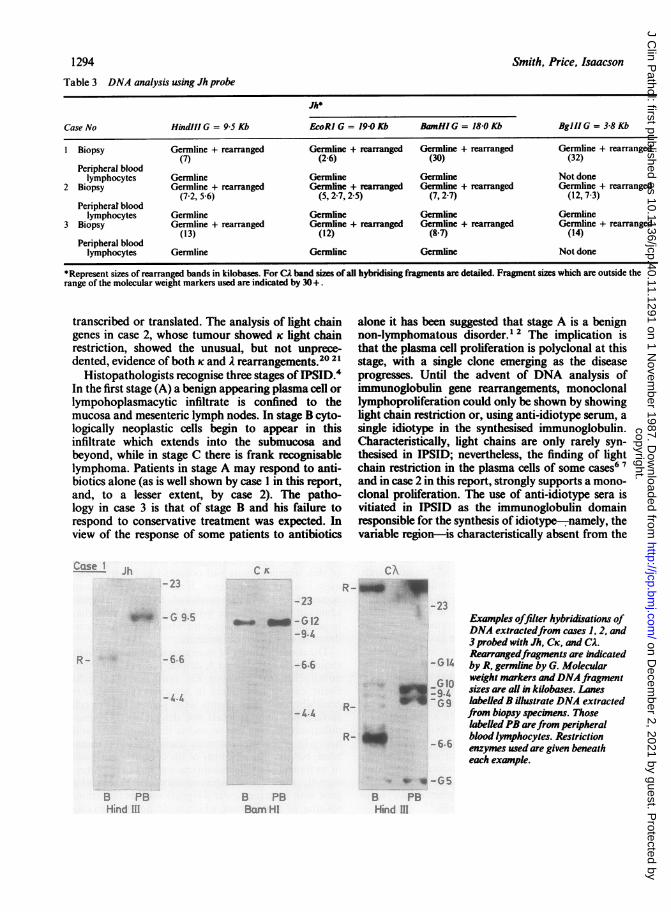
Immunohistochemistry of paraffin sections showedcytoplasmic Ig of the a, subclass in the plasma cells ofall patients. No light chain was shown in cases 1 and3, but K light chain restriction was present in case 2.Using frozen sections the mucosal lymphocytes incase 1 were SIg negative while in case 3 SIgA, withoutlight chain was demonstrable. Mucosal lymphocyteswere virtually absent in case 2.DNA analysis (table 3, figure) using the Jh probe"2
showed the presence of a clone of B cells in all threebiopsy specimens. Rearrangements were detectedwith four different restriction enzymes. In samplesfrom cases 1 and 3 only one rearranged band wasdetected. Both alleles, however, exhibited a non-germline configuration in case 2. Only germline frag-
Table I Recombinant DNA probes used
Probe Code name Reference
Heavy chain joining region (Jh) C76R51A 12K light chain constant region (CK) pUCR17 13A light chain constant region (CA) pUCA5 14
copyright. on D
ecember 2, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.11.1291 on 1 Novem
ber 1987. Dow
nloaded from
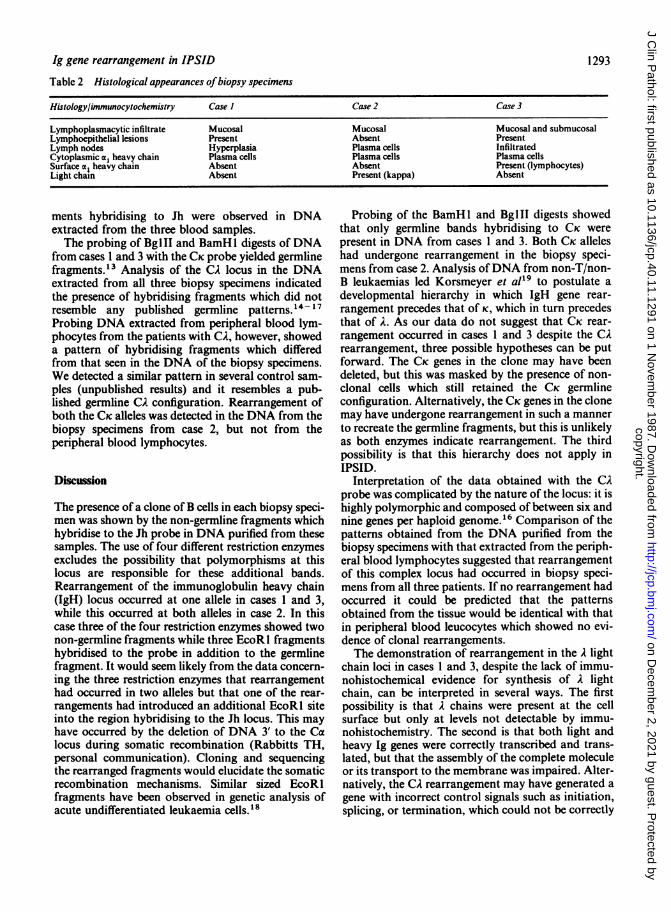
Table 2 Histological appearances ofbiopsy specimens
Histology/immunocytochemistry Case I Case 2 Case 3
Lymphoplasmacytic infiltrate Mucosal Mucosal Mucosal and submucosalLymphoepithelial lesions Present Absent PresentLymph nodes Hyperplasia Plasma cells InfiltratedCytoplasmic al heavy chain Plasma cells Plasma cells Plasma cellsSurface al heavy chain Absent Absent Present (lymphocytes)Light chain Absent Present (kappa) Absent
ments hybridising to Jh were observed in DNAextracted from the three blood samples.The probing of Bg1II and BamHl digests of DNA
from cases 1 and 3 with the CK probe yielded germlinefragments.'3 Analysis of the CA locus in the DNAextracted from all three biopsy specimens indicatedthe presence of hybridising fragments which did notresemble any published germline patterns." -17Probing DNA extracted from peripheral blood lym-
phocytes from the patients with CA, however, showeda pattern of hybridising fragments which differedfrom that seen in the DNA of the biopsy specimens.
We detected a similar pattern in several control sam-ples (unpublished results) and it resembles a pub-lished germline CA configuration. Rearrangement ofboth the CK alleles was detected in the DNA from thebiopsy specimens from case 2, but not from theperipheral blood lymphocytes.
Discussion
The presence of a clone ofB cells in each biopsy speci-men was shown by the non-germline fragments whichhybridise to the Jh probe in DNA purified from thesesamples. The use of four different restriction enzymesexcludes the possibility that polymorphisms at thislocus are responsible for these additional bands.Rearrangement of the immunoglobulin heavy chain(IgH) locus occurred at one allele in cases I and 3,while this occurred at both alleles in case 2. In thiscase three of the four restriction enzymes showed twonon-germline fragments while three EcoRl fragmentshybridised to the probe in addition to the germlinefragment. It would seem likely from the data concern-
ing the three restriction enzymes that rearrangementhad occurred in two alleles but that one of the rear-
rangements had introduced an additional EcoRl siteinto the region hybridising to the Jh locus. This mayhave occurred by the deletion of DNA 3' to the Calocus during somatic recombination (Rabbitts TH,personal communication). Cloning and sequencingthe rearranged fragments would elucidate the somaticrecombination mechanisms. Similar sized EcoRlfragments have been observed in genetic analysis ofacute undifferentiated leukaemia cells.'8
Probing of the BamHl and BglII digests showedthat only germline bands hybridising to CK werepresent in DNA from cases 1 and 3. Both CK alleleshad undergone rearrangement in the biopsy speci-mens from case 2. Analysis ofDNA from non-T/non-B leukaemias led Korsmeyer et al'9 to postulate adevelopmental hierarchy in which IgH gene rear-rangement precedes that of K, which in turn precedesthat of A. As our data do not suggest that CK rear-rangement occurred in cases I and 3 despite the CArearrangement, three possible hypotheses can be putforward. The CK genes in the clone may have beendeleted, but this was masked by the presence of non-clonal cells which still retained the CK germlineconfiguration. Alternatively, the CK genes in the clonemay have undergone rearrangement in such a mannerto recreate the germline fragments, but this is unlikelyas both enzymes indicate rearrangement. The thirdpossibility is that this hierarchy does not apply inIPSID.
Interpretation of the data obtained with the CAprobe was complicated by the nature of the locus: it ishighly polymorphic and composed of between six andnine genes per haploid genome. 6 Comparison of thepatterns obtained from the DNA purified from thebiopsy specimens with that extracted from the periph-eral blood lymphocytes suggested that rearrangementof this complex locus had occurred in biopsy speci-mens from all three patients. If no rearrangement hadoccurred it could be predicted that the patternsobtained from the tissue would be identical with thatin peripheral blood leucocytes which showed no evi-dence of clonal rearrangements.The demonstration of rearrangement in the A light
chain loci in cases 1 and 3, despite the lack of immu-nohistochemical evidence for synthesis of A lightchain, can be interpreted in several ways. The firstpossibility is that A chains were present at the cellsurface but only at levels not detectable by immu-nohistochemistry. The second is that both light andheavy Ig genes were correctly transcribed and trans-lated, but that the assembly of the complete moleculeor its transport to the membrane was impaired. Alter-natively, the CA rearrangement may have generated agene with incorrect control signals such as initiation,splicing, or termination, which could not be correctly
Ig gene rearrangement in IPSID 1293
copyright. on D
ecember 2, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.11.1291 on 1 Novem
ber 1987. Dow
nloaded from
Smith, Price, Isaacson1294
Table 3 DNA analysis using Jh probe
Jh*
Case No Hindl!l G = 9-5 Kb EcoRI G = 1940 Kb BamNHIG = 18-0 Kb BglllG = 3-8 Kb
I Biopsy Germline + rearranged Germline + rearranged Germline + rearranged Germline + rearranged(7) (2-6) (30) (32)
Peripheral bloodlymphocytes Germline Germline Germline Not done
2 Biopsy Gernline + rearranged Germline + rearranged Germline + rearranged Germline + rearranged(72,56) (5,27,25) (7,27) (12,73)
Peripherat bloodlymphocytes Germline Gennline Germline Genlmine
3 Biopsy Germline + rearranged Germline + rearranged Gernline + rearranged Gennline + rearranged(13) (12) (8-7) (14)
Peripheral bloodlymphocytes Germline Germline Germline Not done
*Represent sizes of rearranged bands in kilobases. For CA band sizes of all hybridising fragments are detailed. Fragment sizes which are outside therange of the molecular weight markers used are indicated by 30 +.
transcribed or translated. The analysis of light chaingenes in case 2, whose tumour showed K light chainrestriction, showed the unusual, but not unprece-dented, evidence of both K and A rearrangements.202'
Histopathologists recognise three stages of IPSID.'In the first stage (A) a benign appearing plasma cell orlympohoplasmacytic infiltrate is confined to themucosa and mesenteric lymph nodes. In stage B cyto-logically neoplastic cells begin to appear in thisinfiltrate which extends into the submucosa andbeyond, while in stage C there is frank recognisablelymphoma. Patients in stage A may respond to anti-biotics alone (as is well shown by case I in this report,and, to a lesser extent, by case 2). The patho-logy in case 3 is that of stage B and his failure torespond to conservative treatment was expected. Inview of the response of some patients to antibiotics
C"ase
-23W:L - G 9g* _.* -G12
-9.4
- 6r -66
4
- 4.4
B PBHind III
alone it has been suggested that stage A is a benignnon-lymphomatous disorder.'2 The implication isthat the plasma cell proliferation is polyclonal at thisstage, with a single clone emerging as the diseaseprogresses. Until the advent of DNA analysis ofimmunoglobulin gene rearrangements, monoclonallymphoproliferation could only be shown by showinglight chain restriction or, using anti-idiotype serum, asingle idiotype in the synthesised immunoglobulin.Characteristically, light chains are only rarely syn-thesised in IPSID; nevertheless, the finding of lightchain restriction in the plasma cells of some cases6 7and in case 2 in this report, strongly supports a mono-clonal proliferation. The use of anti-idiotype sera isvitiated in IPSID as the immunoglobulin domainresponsible for the synthesis of idiotype-namely, thevariable region-is characteristically absent from the
CNR-_
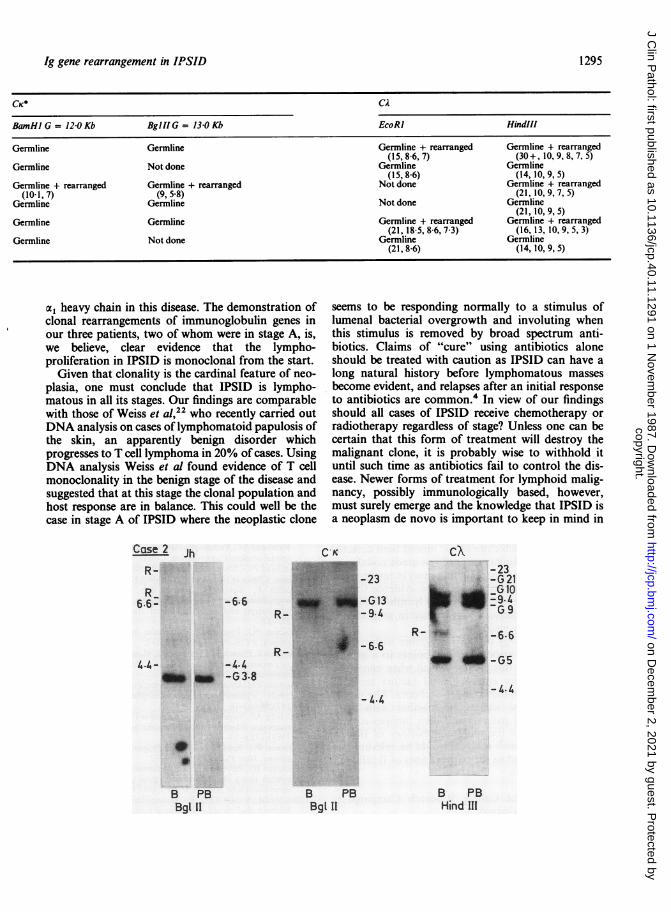
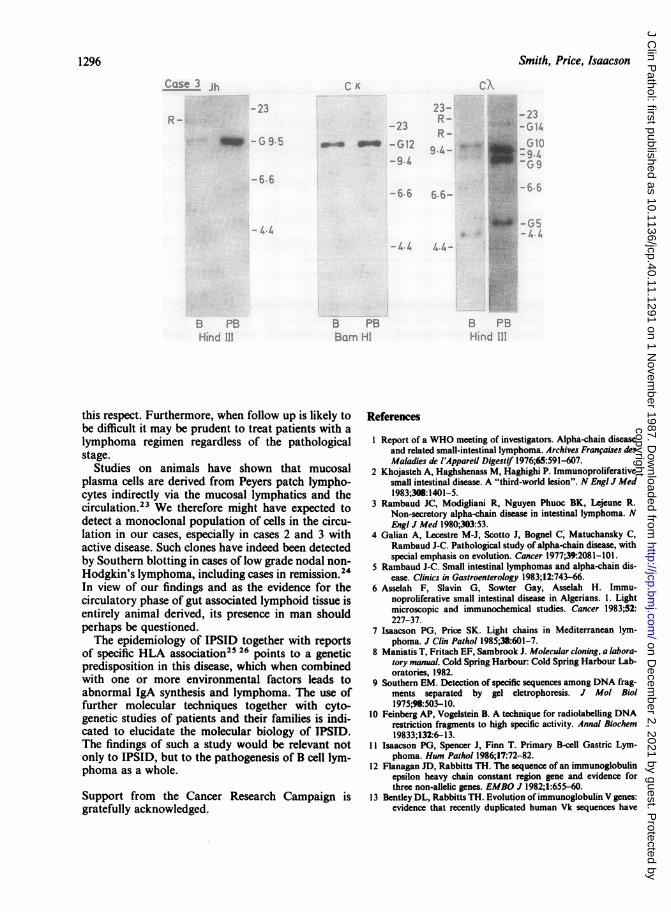
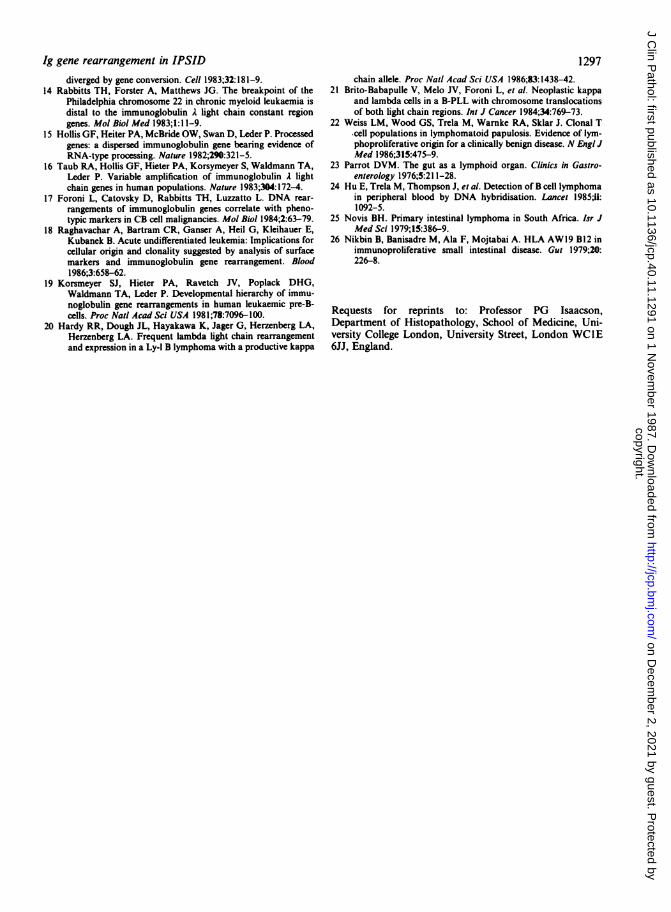
-23Examples offilter hybridisations ofDNA extractedfrom cases 1, 2, and3 probed with Jh, CK, and CA.Rearrangedfragments are indicated
- G 14 by R, germline by G. MolecularG 1 weight markers andDNA fragment
-9.4 sizes are all in kilobases. LanesR- _ _G9 labelledB illustrate DNA extracted
from biopsy specimens. Thoselabelled PB arefrom peripheral
R- _6.6 blood lymphocytes. Restrictionenzymes used are given beneatheach example.
u u-G5B PB B PBBam HI Hind IIl
copyright. on D
ecember 2, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.11.1291 on 1 Novem
ber 1987. Dow
nloaded from
Ig gene rearrangement in IPSID
CK* CA
BamHI G = 120Kb Bgll!G = 13-0Kb EcoRI Hindlll
Germline Germline Germline + rearranged Germline + rearranged(15,8-6,7) (30+, 10,9,8,7,5)
Germline Not done Germline Germline(15, 86) (14, 10,9,5)
Germline + rearranged Germline + rearranged Not done Germline + rearranged(10-1,7) (9,5-8) (21,10,9,7,5)
Germline Germline Not done Germline(21, 10,9,5)
Germline Germline Germline + rearranged Germline + rearranged(21, 185,86,73) (16, 13, 10,9,5,3)
Germline Not done Germline Germline(21, 86) (14, 10,9,5)
a, heavy chain in this disease. The demonstration ofclonal rearrangements of immunoglobulin genes inour three patients, two of whom were in stage A, is,we believe, clear evidence that the lympho-proliferation in IPSID is monoclonal from the start.
Given that clonality is the cardinal feature of neo-plasia, one must conclude that IPSID is lympho-matous in all its stages. Our findings are comparablewith those of Weiss et al,22 who recently carried outDNA analysis on cases of lymphomatoid papulosis ofthe skin, an apparently benign disorder whichprogresses to T cell lymphoma in 20% of cases. UsingDNA analysis Weiss et al found evidence of T cellmonoclonality in the benign stage of the disease andsuggested that at this stage the clonal population andhost response are in balance. This could well be thecase in stage A of IPSID where the neoplastic clone
Case 2 Jh
R_6.6-
*m _.
-6.6
-4.4-G3-8
seems to be responding normally to a stimulus oflumenal bacterial overgrowth and involuting whenthis stimulus is removed by broad spectrum anti-biotics. Claims of "cure" using antibiotics aloneshould be treated with caution as IPSID can have along natural history before lymphomatous massesbecome evident, and relapses after an initial responseto antibiotics are common.4 In view of our findingsshould all cases of IPSID receive chemotherapy orradiotherapy regardless of stage? Unless one can becertain that this form of treatment will destroy themalignant clone, it is probably wise to withhold ituntil such time as antibiotics fail to control the dis-ease. Newer forms of treatment for lymphoid malig-nancy, possibly immunologically based, however,must surely emerge and the knowledge that IPSID isa neoplasm de novo is important to keep in mind in
C K
-23
-G13-9.4
- 6.6
- 4.4
B PBBgl 1I
BBgl 11
PB
CX-23
X -G21
rL -G9R- I -6.6
0a-G5-L4.
B PBHind 11
1295
copyright. on D
ecember 2, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.11.1291 on 1 Novem
ber 1987. Dow
nloaded from
1296 Smith, Price, Isaacson
Cuc . r CIK. A
._ 23-?3 -2 322-~~~~~~~R
_up ~ -S e -G1223(59-L.-5-~~~~~~~ :i;. ;.
66 6.6::-9.4~~~~~~~~-K
it.
pp, B PB k BU ~~~~~~BornHI Hi:ndI
this respect. Furthermore, when follow up is likely tobe difficult it may be prudent to treat patients with alymphoma regimen regardless of the pathologicalstage.
Studies on animals have shown that mucosalplasma cells are derived from Peyers patch lympho-cytes indirectly via the mucosal lymphatics and thecirculation.23 We therefore might have expected todetect a monoclonal population of cells in the circu-lation in our cases, especially in cases 2 and 3 withactive disease. Such clones have indeed been detectedby Southern blotting in cases of low grade nodal non-Hodgkin's lymphoma, including cases in remission.24In view of our findings and as the evidence for thecirculatory phase of gut associated lymphoid tissue isentirely animal derived, its presence in man shouldperhaps be questioned.The epidemiology of IPSID together with reports
of specific HLA association25 26 points to a geneticpredisposition in this disease, which when combinedwith one or more environmental factors leads toabnormal IgA synthesis and lymphoma. The use offurther molecular techniques together with cyto-genetic studies of patients and their families is indi-cated to elucidate the molecular biology of IPSID.The findings of such a study would be relevant notonly to IPSID, but to the pathogenesis of B cell lym-phoma as a whole.
Support from the Cancer Research Campaign isgratefully acknowledged.
References
I Report of a WHO meeting of investigators. Alpha-chain diseaseand related small-intestinal lymphoma. Archives Franfaises desMaladies de l'Appareil Digestif 1976;65:591-607.
2 Khojasteh A, Haghshenass M, Haghighi P. Immunoproliferativesmall intestinal disease. A "third-world lesion". N Engl J Med1983;308:1401-5.
3 Rambaud JC, Modigliani R, Nguyen Phuoc BK, Lejeune R.Non-secretory alpha-chain disease in intestinal lymphoma. NEngl J Med 1980;303:53.
4 Galian A, Lecestre M-J, Scotto J, Bognel C, Matuchansky C,Rambaud J-C. Pathological study of alpha-chain disease, withspecial emphasis on evolution. Cancer 1977;39:2081-101.
5 Rambaud J-C. Small intestinal lymphomas and alpha-chain dis-ease. Clinics in Gastroenterology 1983;12:743-66.
6 Asselah F, Slavin G, Sowter Gay, Asselah H. Immu-noproliferative small intestinal disease in Algerians. 1. Lightmicroscopic and immunochemical studies. Cancer 1983;52:227-37.
7 Isaacson PG, Price SK. Light chains in Mediterranean lym-phoma. J Clin Pathol 1985;38:601-7.
8 Maniatis T, Fritach EF, Sambrook J. Molecular cloning, a labora-tory manual. Cold Spring Harbour: Cold Spring Harbour Lab-oratories, 1982.
9 Southern EM. Detection of specific sequences among DNA frag-ments separated by gel eletrophoresis. J Mol Biol1975;98:503-10.
10 Feinberg AP, Vogelstein B. A technique for radiolabelling DNArestriction fragments to high specific activity. Annal Biochem19833;132:6-13.
11 Isaacson PG, Spencer J, Finn T. Primary B-cell Gastric Lym-phoma. Hum Pathol 1986;17:72-82.
12 Flanagan JD, Rabbitts TH. The sequence of an immunoglobulinepsilon heavy chain constant region gene and evidence forthree non-allelic genes. EMBO J 1982;1:655-60.
13 Bentley DL, Rabbitts TH. Evolution ofimmunoglobulin V genes:evidence that recently duplicated human Vk sequences have
copyright. on D
ecember 2, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.11.1291 on 1 Novem
ber 1987. Dow
nloaded from
Ig gene rearrangement in IPSID 1297diverged by gene conversion. Cell 1983;32:181-9.
14 Rabbitts TH, Forster A, Matthews JG. The breakpoint of thePhiladelphia chromosome 22 in chronic myeloid leukaemia isdistal to the immunoglobulin A light chain constant regiongenes. Mol Biol Med 1983;1:11-9.
15 Hollis GF, Heiter PA, McBride OW, Swan D, Leder P. Processedgenes: a dispersed immunoglobulin gene bearing evidence ofRNA-type processing. Nature 1982;290:321-5.
16 Taub RA, Hollis GF, Hieter PA, Korsymeyer S, Waldmann TA,Leder P. Variable amplification of immunoglobulin A lightchain genes in human populations. Nature 1983;304:172-4.
17 Foroni L, Catovsky D, Rabbitts TH, Luzzatto L. DNA rear-rangements of immunoglobulin genes correlate with pheno-typic markers in CB cell malignancies. Mol Biol 1984;2:63-79.
18 Raghavachar A, Bartram CR, Ganser A, Heil G, Kleihauer E,Kubanek B. Acute undifferentiated leukemia: Implications forcellular origin and clonality suggested by analysis of surfacemarkers and immunoglobulin gene rearrangement. Blood1986;3:658-62.
19 Korsmeyer SJ, Hieter PA, Ravetch JV, Poplack DHG,Waldmann TA, Leder P. Developmental hierarchy of immu-noglobulin gene rearrangements in human leukaemic pre-B-cells. Proc Natl Acad Sci USA 1981;78:7096-100.
20 Hardy RR, Dough JL, Hayakawa K, Jager G, Herzenberg LA,Herzenberg LA. Frequent lambda light chain rearrangementand expression in a Ly-1 B lymphoma with a productive kappa
chain allele. Proc Natl Acad Sci USA 1986;83:1438-42.21 Brito-Babapulle V, Melo JV, Foroni L, et al. Neoplastic kappa
and lambda cells in a B-PLL with chromosome translocationsof both light chain regions. Int J Cancer 1984;34:769-73.
22 Weiss LM, Wood GS, Trela M, Warnke RA, Sklar J. Clonal Tcell populations in lymphomatoid papulosis. Evidence of lym-phoproliferative origin for a clinically benign disease. N Engi JMed 1986;315:475-9.
23 Parrot DVM. The gut as a lymphoid organ. Clinics in Gastro-enterology 1976;5:21 1-28.
24 Hu E, Trela M, Thompson J, et al. Detection of B cell lymphomain peripheral blood by DNA hybridisation. Lancet 1985;ii:1092-5.
25 Novis BH. Primary intestinal lymphoma in South Africa. Isr JMed Sci 1979;I5:386-9.
26 Nikbin B, Banisadre M, Ala F, Mojtabai A. HLA AWl9 B12 inimmunoproliferative small intestinal disease. Gut 1979;20:226-8.
Requests for reprints to: Professor PG Isaacson,Department of Histopathology, School of Medicine, Uni-versity College London, University Street, London WC1E6JJ, England.
copyright. on D
ecember 2, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.40.11.1291 on 1 Novem
ber 1987. Dow
nloaded from