implementation of virtual handoff with a standardized tool
TRANSCRIPT
Implementation of Virtual Handoff
with a Standardized ToolTemitope Ajayi, BSN, RN
Bridgitte Gourley, DNP, CRNP
• Patient handoff is a vulnerable time for patients and nurses • The Joint Commission recommends accurate, high-quality
handoffs occur for every patient during every transition of care.
• Host Organization uses BSR within units but struggles to ensure accurate handoffs when patients transfer between units.
• The PACU is an active, high turnover, unit that requires nurses to remain in the unit to care for other patients and maintain workflow making interdepartmental hand off impractical.
• The PACU reported 40 events since August 2018; eight (66.66%) were from the PACU to GSU and may have been avoided with the use of virtual handoff.
Background
The purpose of this Quality Improvement project was to implement and evaluate the effectiveness of virtual handoff using SBAR format during patient transfer from the Post-Operative Care Unit to the General Surgical Care Unit
Short-term Goal:
By October 30th, 75% of Nurses in the PACU will complete patient handoff using the SBAR tool virtually, allowing for efficiency and accuracy during report/ patient handoff.
Long-term Goal:
By December 31th, 2019, Post- implementation of Virtual SBAR will result in 100% reduction in the number of Patient handoff related events originating from the PACU to GSU
Purpose
Results
Discussion
• The feedback from the intervention showed that there was no significant change in the rate of incidents related to patient handoff from PACU to GSU during the implementation phase compared to the pre-implementation phase.
• Valuable lessons learned include feasibility and barriers • Nurses were able to successfully utilize the new technology• Anecdotally shared the ability to visualize patients was
helpful. • Using a standardized SBAR increased the clarity of the
communication and the quality of the information shared. • This pilot of virtual patient handoff was successful in
delivering accurate and comprehensive communication of pertinent patient information.
Conclusions
• Joint Commission Center for Transforming Healthcare. Joint Commission Center for Transforming Healthcare Releases Targeted Solutions Tool for Hand-Off Communications. Jt Comm Perspect2012; 32:1 https://www.jointcommission.org/assets/1/6/tst_hoc_persp_08_12.pdf (Accessed on April 24, 2018).• Renz, S. M., Boltz, M. P., Wagner, L. M., Capezuti, E. A., & Lawrence, T. E. (2013). Examining The Feasibility and Utility of an SBAR Protocol in Long-term care. Geriatric Nursing, 34(4), 295-301. doi:10.1016/j.gerinurse.2013.04.010• Riesenberg LA, Leisch J, Cunningham JM. Nursing Handoffs: A Systematic Review of the Literature. AmJ Nurs. 2010; 110(4):24-34; quiz 35-36•Sand-Jecklin, K., & Sherman, J. (2014). A Quantitative Assessment of Patient and Nurse Outcomes of Bedside Nursing Report Implementation. Journal of Clinical Nursing, 23(19-20), 2854-2863. doi:10.1111/jocn.12575
References
• Quality improvement project took place over a 13 weeks• Setting: Community hospital.• Population: Adult post op patients transferred from the
PACU to GSU.• PACU, GSU leadership team and the IT team created a
safe, HIPAA compliant zoom video call network for patient handoff for PACU and GSU nurses to access.
• Process measures: Percentage of nurses trained to use complete patient handoff virtually.
• Outcome measures: number of incidents related to patient handoff from GSU to PACU, length of time it takes to complete patient handoff and nurse perception of handoff.
Methods
Figures
This project was completed as part of a Doctor of Nursing Practice project. I would like to express my gratitude to Dr. Bridgitte Gourley for her guidance and support throughout this project. I would also like to thank Michelle Lusby, Dr. Cathaleen Ley, IT team and the nursing staff of the host organization for their support and participation in this project.
Acknowledgements• Anecdotal reports from the nurses indicated that Virtual handoff was helpful in completing patient handoff.
• Demonstrated feasibility of process and implementation• Nurses appreciated ability to meet and visualize patients prior to transfer• Virtual handoff was an optional form of completing patient handoff• Consistent availability of technology resources was a barrier• Nurses from other units were excluded from completing patient handoff virtually.
• No incidents related to patient handoff from PACU to GSU were reported pre and post implementation.
• The average length of time to complete patient handoff via video call was 7 minutes compared to those done via phone call which average at 5 minutes.
• There were no changes in nurses’ perception of handoff using Handover Evaluation tool.
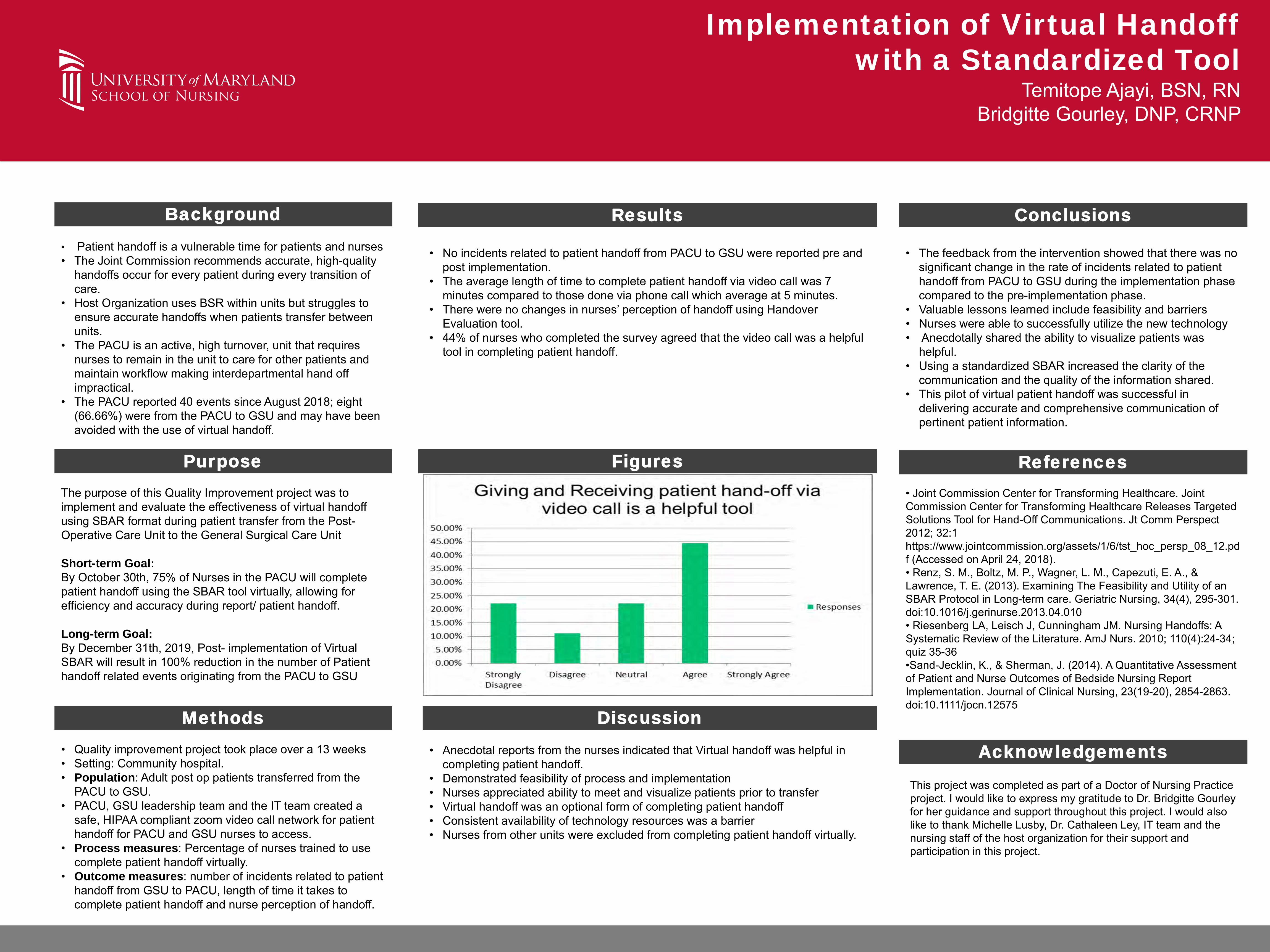
• 44% of nurses who completed the survey agreed that the video call was a helpful tool in completing patient handoff.

Implementation of Carbohydrate-Based Liquid Nutrition in Labor
Richard Conley MS, CRNA, Elaine Bundy DNP, CRNP, FNP-CDavid Sinopoli MD, MPH, MBA, Natasha Belanger, BSN, RNC-OB, David Ghadisha, MD
Problem Statement
Objectives
Results Discussion
Conclusions
Methods
Acknowledgements
References
• At a large community hospital in the mid-Atlantic region, with over 2,400 deliveries a year, all women were kept fasting during labor
• This outdated practice can lead to:• Increased stress• Increased labor pain• Dissatisfaction with the labor experience
• Current evidence and guidelines support providing clear liquids to laboring women at low risk of an operative delivery and pulmonary aspiration
• Create and implement an evidence-based policy for oral carbohydrate-based liquid nutrition in laboring women at low risk of an operative delivery
• Develop an evidence-based tool for use by the obstetrical providers too assess risk of an operative delivery
• Increase the availability of a liquid based nutrition for women in labor at low risk of an operative delivery
• Population: all women admitted for labor during the implementation period at a large community hospital
• Based upon an evidence search, a tool was developed to assess risk of operative delivery (Figure 1)
• Women at low risk were ordered a carbohydrate-based clear liquid diet
• Women at high risk were kept NPO with Ice Chips
• Education was provided for the staff prior to implementation• Anesthesia and Obstetrical staff at weekly department
meeting• Nursing staff during change of shift huddles over two
weeks
• Staff were given verbal and email reminders on use of the assessment tool, policy, and diet orders
• Patient charts were reviewed to record the frequency of high/low risk patients, diet orders and high risk characteristics (Table 1, Figure 2)
• Analyzed using descriptive statistics
• Debbie Kisner, PhD, RN, CNOR, NEA-BC, Chief Nursing Officer, Vice President Patient Care Services
• J. Lynn Petty, MA, RN, NE-BC, Clinical Administrator Women’s and Children’s Service Line
• Jennifer K Stephenson, DNP, RN, PDS-EBP and Research
1. American College of Nurse-Midwives. (2016). Providing Oral Nutrition to Women in Labor. Journal of Midwifery & Women’s Health, 61(4), 528–534.
2. American College of Obstetricians and Gynecologists. (2009). ACOG Committee Opinion No. 441: Oral intake during labor (Reaffirmed 2017). Obstetrics and Gynecology, 114(3), 714–714.
3. The American Society of Anesthesiologists. (2016). Practice Guidelines for Obstetric Anesthesia: An Updated Report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia and the Society for Obstetric Anesthesia and Perinatology. Anesthesiology, 124(2), 270–300.
• The project was successful in implementing a policy and assessment tool for carbohydrate-based liquid nutrition in labor
• According to the literature, allowing women carbohydrate-based clear liquids in labor can decrease stress, labor pain and increase satisfaction with the birth experience
• Next Steps: assessment of these quality indicators
• Recommendations for future QI projects include:• Assessment of satisfaction, impact on vaginal versus
cesarean delivery rates, and impact on workload for the nursing staff
• Due to this practice change 98 women were identified as low risk and allowed to have clear liquids during their labor
• Consistent with the literature, there were no reported complications
• Identified barriers to compliance:• Additional step of adding the clear liquid diet order • Disagreement with the high risk characteristics in the
assessment tool (maternal age, gestational HTN)
• Recommendations for continued success:• Add the clear liquid diet order to the admission order set
• Include the assessment tool in the electronic medical record
• Adjust the operative delivery assessment tool• Remove maternal age, gestational HTN, and Illicit
drug/alcohol use from the high risk category
Integration of TeamSTEPPS Framework and Escape Room to
Improve Teamwork and Collaboration Suzanna Fitzpatrick, MS, CRNP; Dr. Hazel Jones-Parker, DNP, CRNP, AACRN;
& Dr. Andrea Smith, MBA, DNP, CRNPUniversity of Maryland School of Nursing
Difficulty with communication and teamwork in a large adult emergency department has been identified and senior nursing leadership wanted to enhance collaboration and communication in their workplace. This DNP project leveraged the integration of TeamSTEPPS training and tools in an escape room setting in order to optimize team performance of a group of senior nurse leaders. • Currently, standard leadership courses, conferences and other
didactic learning methods are utilized for teamwork improvement. • Poor communication and team work can threaten patient safety• Escape rooms, live action, team-based exercises (Adams & Crawford,
2018), supplemented with TeamSTEPPS tools can assist in optimizing team performance, while keeping the participant engaged in a new learning environment and has been shown to improve leadership skills.
Problem Statement
An evidence-based Quality Improvement project at a large inner city Adult Emergency Room with senior clinical nurses aimed to:
• Improve communication and teamwork skills• Utilize an escape room as a training tactic• Assess escape room concept as a training tool
Goals: • Short Term: 4-6 members of the quality improvement team will
have completed TeamSTEPPS training and familiarization with escape room and exercise so they may train others on TeamSTEPPS utilizing the escape room tactic and team dynamics and leadership improvement for project sustainability.
• Long Term: All SCN Emergency Department nurses will change their leadership skills and improve team cohesiveness by completing an escape room and TeamSTEPPS course
Purpose
Results
This group of ED nurses completed 2 escape rooms and a TeamSTEPPS training and all agreed that an escape room can be a fun way to motivate while providing an effective team building activity. • This group of nurse leaders validated the integration of
TeamSTEPPS tools and strategies in an escape room setting• All participants voiced the experience was enjoyable and an
engaging way to learn while providing an effective team building activity.
• This small cohort, in line with the literature, demonstrates that new methods of learning such as an escape room should be explored for engaging participants and improving communication and teamwork skills.
Limitations:
• Small sample size• Time constraints• Varying escape room exercises• Lack of demographics• Not all survey questions were answered by all participants
Further recommendations:
• Larger sample size • Dedicated time for TeamSTEPPS training and strategies
Discussion
Escape rooms can be a dynamic and interactive way to promote team training and education. Integration of TeamSTEPPS tools and strategies within the escape room framework provides for an engaging learning environment where participants can deepen their understanding of concepts through active learning. While this was just a small sample in one intercity hospital, new methods for learning should be reviewed for successful teamwork
Conclusions
Study Design
• 14-week Quality Improvement Project Guided by MAP-IT Framework Includes Observation at staff meetings Weekly check-ins with manager and assistant manager Escape room exercise with TeamSTEPPS training completion of
perceptions tools Weekly education on teamwork via email following escape room
• Completion of pre/ post-escape room toolsSample
• 12 senior clinical nurse (n=12) 1- less than 1 year SCN experience 5 – 1-4 years SCN experience 6- greater than 4 years SCN experience
• Including 1 nurse manager• Including 1 assistant nurse manager
11 female: 1 male
Methods
• Adams, V., Burger, S., Crawford, K., & Setter, R. (2018). Can you escape? Creating an Escape Room to facilitate active learning. Journal for Nurses in Professional Development 34 (2). E1-E5. doi:10.1097/NND.0000000000000433.
• Sheppard, F., Williams, M., & Klein, V. (2013) TeamSTEPPS and patient safety in healthcare. Risk Management. 32(3); 5-10. doi: 10.1002/jmrm.21099.
• Yi, Y. (2015). Effects of team-building on communication and teamwork among nursing students. International council of nurses. 63 (1) 33-40. doi: 10.111/inr.12224.
References
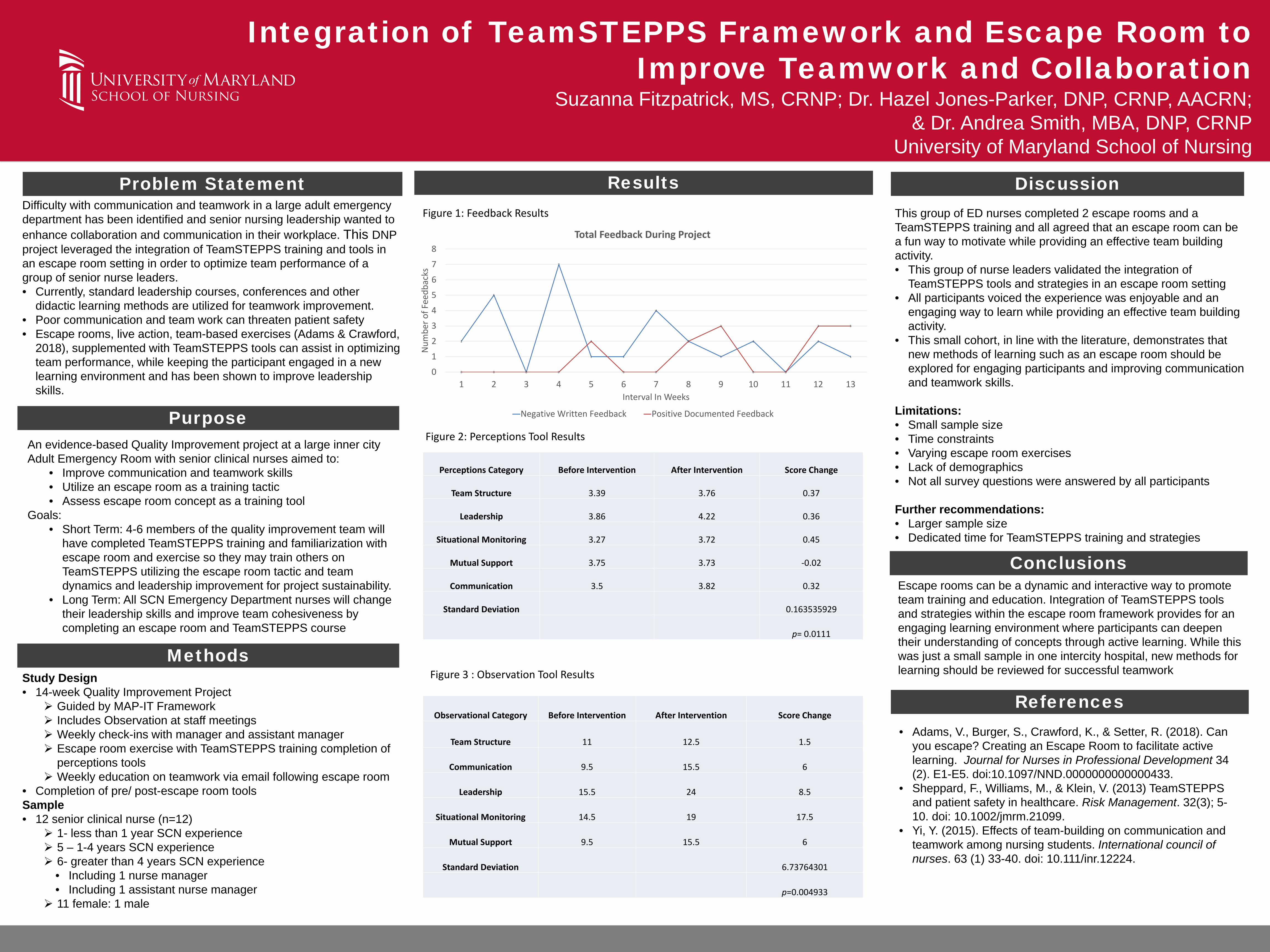
Figure 1: Feedback Results
Figure 2: Perceptions Tool Results
2
5
0
7
1 1
4
2
1
2
0
2
1
0 0 0 0
2
0 0
2
3
0 0
3 3
0
1
2
3
4
5
6
7
8
1 2 3 4 5 6 7 8 9 10 11 12 13
Num
ber o
f Fee
dbac
ks
Interval In Weeks
Total Feedback During Project
Negative Written Feedback Positive Documented Feedback
Perceptions Category Before Intervention After Intervention Score Change
Team Structure 3.39 3.76 0.37
Leadership 3.86 4.22 0.36
Situational Monitoring 3.27 3.72 0.45
Mutual Support 3.75 3.73 -0.02
Communication 3.5 3.82 0.32
Standard Deviation 0.163535929
p= 0.0111
Figure 3 : Observation Tool Results
Observational Category Before Intervention After Intervention Score Change
Team Structure 11 12.5 1.5
Communication 9.5 15.5 6
Leadership 15.5 24 8.5
Situational Monitoring 14.5 19 17.5
Mutual Support 9.5 15.5 6
Standard Deviation 6.73764301
p=0.004933
• Neonates are a vulnerable population with unique skin care needs and physiological differences compared to adults and children
• The 2018 Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) Neonatal Skin Care Evidenced-Based Clinical Practice Guidelines recommends using the Neonatal Skin Condition Score (NSCS) tool for all infants aged 0-28 days, as an objective scale to quantify overall skin condition
.
Background
Purpose • To implement a skin care bundle in neonates 0-28 days
that decreases the risk of skin injury by modifying current skin care practices in the Pediatric Intensive Care Unit (PICU) at an urban academic medical center in the Mid-Atlantic region
Short-term Goals: • Increased documentation of skin care assessment using
the NSCS tool once per shift• Neonates would obtain a perfect score of three on NSCS
tool, meaning no skin dryness, erythema or breakdown• Increased documentation and use of emollient
application and diaper careLong-term Goals:
• Automatic population of NSCS tool in EPIC for patients 0 to 28 days of age
• Dissemination of bundle to units throughout the hospital caring for neonates 0 to 28 days of age
Purpose
Results
• The results support the use of the NSCS tool to screen for skin injury and make the appropriate referral to prevent skin injury
• The data does not indicate there is a connection between emollient application and CLABSI rate
• Limitations of DNP project• Competing QI projects impacted staff buy-in• Staff education was approved to be dispersed via e-mail.• NSCS tool did not auto-populate in patient’s chart. RN or
project lead had to pull the tool into EPIC • Availability of space to post resources, advertisement
and updates limited to a shared bulletin board with competing projects
Discussion
• Recommendation: Continue neonatal skin care bundle in the PICU to reduce skin injury
• Dissemination of bundle to units caring for neonates • Future QI project recommendations:
• In-person education sessions • Auto-population of NSCS tool for neonates 0 to 28 days
old with skin and diaper care recommendations to increase adherence
• Addition of skin and diaper care emollients to eMAR for increased documentation adherence and auditing
ConclusionMethods
Figures
• Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN), & National Association of Neonatal Nurses (NANN). (2018). Neonatal skin care: Evidence-based clinical practice guideline, 4th Edition
• Lund C. H, & Osborne, J. W. (2004). Validity and reliability of the neonatal skin condition score. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 33(3), 320–327.
References
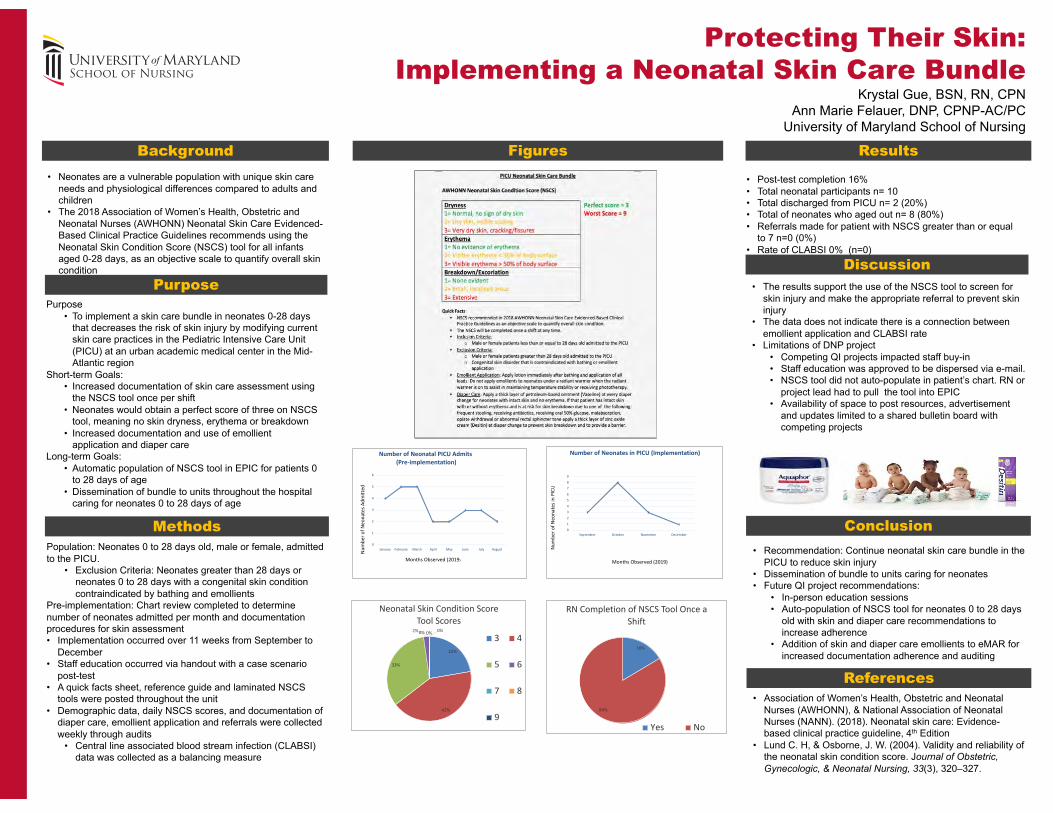
• Post-test completion 16%• Total neonatal participants n= 10• Total discharged from PICU n= 2 (20%)• Total of neonates who aged out n= 8 (80%)• Referrals made for patient with NSCS greater than or equal
to 7 n=0 (0%)• Rate of CLABSI 0% (n=0)
Protecting Their Skin:Implementing a Neonatal Skin Care Bundle
Krystal Gue, BSN, RN, CPNAnn Marie Felauer, DNP, CPNP-AC/PC
University of Maryland School of Nursing
22%
42%
33%
2%0% 0% 0%
Neonatal Skin Condition Score Tool Scores
3 4
5 6
7 8
9
4
5 5
2 2
3 3
2
0
1
2
3
4
5
6
January February March April May June July August
Number of Neonatal PICU Admits(Pre-implementation)
Num
bero
f Neo
nate
s Adm
itted
Months Observed (2019)
16%
84%
RN Completion of NSCS Tool Once a Shift
Yes No
3
8
3
10123456789
September October November December
Number of Neonates in PICU (Implementation)
Months Observed (2019)
Num
ber o
fNeo
nate
s in
PICU
Population: Neonates 0 to 28 days old, male or female, admitted to the PICU.
• Exclusion Criteria: Neonates greater than 28 days or neonates 0 to 28 days with a congenital skin condition contraindicated by bathing and emollients
Pre-implementation: Chart review completed to determine number of neonates admitted per month and documentation procedures for skin assessment• Implementation occurred over 11 weeks from September to
December• Staff education occurred via handout with a case scenario
post-test • A quick facts sheet, reference guide and laminated NSCS
tools were posted throughout the unit • Demographic data, daily NSCS scores, and documentation of
diaper care, emollient application and referrals were collected weekly through audits
• Central line associated blood stream infection (CLABSI) data was collected as a balancing measure

STOP-BANG Screening for Obstructive Sleep Apnea
in Adult Pre-operative Patients
• Obstructive sleep apnea (OSA) is a fully or partially obstructed airway during sleep.
• Increases risk of cardiovascular disease, diabetes, and hypertension.
• If unidentified & untreated, OSA can result in escalation of care and prolonged hospital stays.
• Affects 20-30% of Americans and 25% of patients undergoing elective surgical procedures.
• No national required routine screening.
Problem Statement
• Implement STOP-BANG questionnaire for all pre-operative, adult patients with BMI> 35 kg/m2, who were admitted for surgery, not previously diagnosed with OSA, and not undergoing bariatric surgery.
• Short-term goal:• By October 1st, 2019
• 75% of pre-op and PACU RNs implement the STOP-BANG questionnaire and additional OSA risk questions to identify patients with suspected OSA and notify the anesthesiologist of high-risk patients to improve outcomes and reduce need for elevation of care.
• Long-term goal: • By December 31, 2019
• Pre-Op and PACU RNs implement STOP-BANG, notify the anaesthesiologist as needed, who will determine if patient requires elevation of care, which decreases the risk for negative and adverse outcomes for individuals with undiagnosed OSA .
PurposeFigures
Results
• 31% of patients screened were high risk; none required escalation of care.
• Unknown if patients may have required escalation of care but were discharged prematurely.
• More patients could have screened higher risk for OSA in early weeks due to more frequent administration of STOP-BANG questionnaire earlier in QI project .
Discussion
Chung, F., Subramanyam, R., Liao, P., Sasaki, E., Shapiro, C., & Sun, Y. (2012). High STOP-BANG score indicates a high probability of obstructive sleep apnea. British Journal of Anaesthesia, 108(5), 768-775. doi>10.1093/bja/aes022Chung, F., Liao, P., & Farney, R. (2015). Correlation between the STOP-Bang score and the severity of obstructive sleep apnea. Anesthesiology, 122(6), 1436-1437. doi:10.1097/ALN.0000000000000665Chung, F., Abdullah, H.R., & Liao, P. (2016a). STOP-Bang questionnaire. Chest Journal, 149(3), 631-638. doi:10.1378/chest.15-0903
References
• Setting: Community hospital.• Population: Adult, surgical, newly admitted patients with
BMI> 35 kg/m2, who were admitted for surgery, not previously diagnosed with OSA, and not undergoing bariatric surgery.
• Process measures: % of trained nurses. • Data outcome measures: % patients requiring escalation
in care in related to high-risk STOP-BANG scores.• Estimation of eligible patients: 15-20 patients per day. • 13-week implementation period during Fall 2019.
Methods
This project was completed as part of a Doctor of Nursing Practice project. I would like to express my gratitude to Dr.BridgitteGourley for her guidance and support. I would also like to thank Jennifer King, Sue Lee, Dr.CathaleenLey, and Dr.Maxim Orlov, for their support and participation in this project.
Acknowledgements
S Snoring B BMI>35 kg/m2
T Tiredness (daytime) A Age>50
O Observed Apnea N Neck Circumference
P Pressure, Hypertension G Gender (Male)
Kathleen Kang, BSN, RNBridgitte Gourley, DNP, CRNP
0102030405060
Median
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13
Patients Screened High-Risk for OSA
STOP BANG Tool
Patient Demographics and Scores
Weeks
# o
f P
ati
en
ts
Conclusions
• Tool does identify people with or at risk for OSA.• Feasible to use pre-operatively • Continued education encouraged for refreshing
importance of OSA screening.• Further evaluation of inclusion criteria, which was
purposefully strict, may identify opportunity to include more patients for screening.
• Weekly average:• 6 patients screened. • 7 patients eligible.
• 31% of patients screened were high-risk • No escalation of care required. • 41% of eligible males, 88% of eligible females screened. • 76% of PACU RNs and 85% of pre-op RNs were trained.

Improving Nurse-Nurse Communication to Reduce Patient Bounce-Back
Natalie Marchione, BSN, RNBridgitte Gourley, DNP, FNP-BC,Faculty Advisor
University of Maryland School of Nursing
A deficit in nurse communication was identified, causing approximately 3% of patients bounced-back (i.e., readmitted) to the emergency department (ED) from the psychiatric emergency services (PES) from April – August 2019. • This suboptimal communication contributes to a lack of
rapport, poor workflow, and reduced patient safety, making implementation of a communication tool for the receiving nurse in PES essential.
Background & Significance
To implement and evaluate a psychiatric SBAR tool (PSYCH) from October 1st through November 30th, 2019 utilized by all PES nurses (n = 21) when receiving report on patients from the ED in order to reduce patient bounce-back in PES to 0% through improvements in nurse-nurse communication.
Project Purpose & Goals
Methods
Despite showing an improvement in patient bounce-back nurse perception of communication decreased within PES, while improving within the ED. • The results of an independent t-test showed the
differences in perceptions of communication between the ED and PES to be statistically significant pre-implementation, but not post-implementation.
• Need further buy-in from ED. • Not all the same nurses filled out T-TAQ from pre- to
post-implementation.
Conclusions
• Mariano, M. T., Brooks, V., & DiGiacomo, M. (2016). PSYCH: A mnemonic to help psychiatric residents decrease patient handoff communication errors. The Joint Commission Journal On Quality and Patient Safety, 42(7), 316-320. doi:10.1016/s1553-7250(16)42043-x
• McAllen, E. R., Stephens, K., Swanson-Biearman, B., Kerr, K., & Whiteman, K. (2018). Moving shift report to the bedside: An evidence-based quality improvement project. OJIN: The Online Journal of Issues in Nursing, 23(2). doi:10.3912/OJIN.Vol23No02PPT22
• Richards, K. L. (2016). Improving quality and efficient communication between providers and nursing - A psychiatric SBAR tool (PSYCH) (Doctoral dissertation, University of San Francisco). Retrieved fromhttps://repository.usfca.edu/cgi/viewcontent.cgi?referer=https://scholar.google.com/&httpsredir=1&article=1450&context=capstone
• White-Trevino, K., & Dearmon, V. (2018). Transitioning nurse handoff to the bedside. Nursing Administration Quarterly, 42(3), 261-268. doi:10.1097/naq.0000000000000298
References
Showed feasibility of a psychiatric SBAR tool (PSYCH) used during report between two emergency units to improve communication:• Results reinforced the importance of gathering all
pertinent data using a standardized tool • Improved nurse adoption of efficient communication,
reducing redundancy and improving patient safety.• Further inquiry into security & safety risks identified.
o Patient possession of hidden weapons o Medical problems (broken arm).
• More in depth patient searches needed prior to transfer.
DiscussionResults
• Kurt Lewin’s Change Theory utilized nurses’ current dissatisfaction of communication (driving forces) to influence implementation of the PSYCH tool, furthering motivation from nurses for a change in the report process.
• T-TAQ communication scale was identified to collect data on nurse-nurse communication between PES and the ED.
889092949698
100102
Pre-Implementation
PercentageofPatientsNotBounced-BackfromPEStotheED
Implementation
• Through random observation compliance to PSYCH tool use reached 100% by end of project.
• Patient bounce-back reduced to 0.8% throughout the project• T-TAQ communication scale showed pre-implementation ED perceptions
of communication (M = 24.25, SD = 2.22, n = 12) to be lower than PES perceptions (M = 25.75, SD = 2.22, n = 20).
o PES nurse perceptions decreased from pre- to post- T-TAQ, while ED nurse perceptions improved.
• Post-implementation perceptions between PES (M = 24.33, SD = 1.68, n = 15) and the ED (M = 24.62, SD = 1.80, n = 13) were not significant t(26) = 0.43, p = 0.34.
• Overall pre- to post- T-TAQ scores were shown to not be significant, t(58) = 1.36, p = 0.09.
o 3 of the 6 T-TAQ items showed a positive post survey mean score improvement.
PSYCH SBAR Reference Card P Patient Info Name Age Sex Race
Hx: Psych, Medical, Infectious Disease
S Situation Leading to ED Visit How: Self/Family/ Police/ Ambo Why: SI HI AH VH Psych eval
Y Your (ED) Assessment Delusional Hallucinations manic suicidal homicidal Disorganized Sad Irritable Cooperative Arousal state Skin Issues PICC/ Access Port
C Critical Information Ambulatory ability/ Withdrawal/ Vitals/ Critical labs/ Medications given
H Help Medical clearance obtained Patient location in ED (Luggage)
0123456
0 1 2 3 4 5 6 7
Mean
Score
ExamItem
IndividualizedQuestionnaireItemMeanScoresforT-TAQPre-surveyandPost-survey
Pre- T-TAQ Post- T-TAQ
There are no disclosures or conflicts of interest for this project. The author of this project is a Doctor of Nursing Practice (DNP) student. This project is being completed as a DNP Project.Natalie A. Marchione may be reached via E-mail: [email protected]
Acknowledgements
Perinatal fetal death (PFD) - the death of a fetus of 28 or more weeks gestation or of an infant less than 7 days old.PFD is a significant problem:
The MD Department of Health and Fetal and Infant Mortality Review (FIMR) board has identified PFD as a top priority issue. Maternal perception of decreased fetal movement has been identified as the most sensitive predictor of adverse outcomes and PFD.However, up to 60% of women report lack of formal fetal movement education, lack of knowledge and ability to recognize clinically significant changes in fetal movement (FM).Results of several large trials indicate that standardized fetal movement patient education leads to
• increased maternal awareness of decreased fetal movement, • decreased delay in decreased fetal movement reporting, • increased prompt management of decreased fetal movement, and • decreased PFD rate by as much as 30%.
Problem Statement
Purpose:The purpose of this quality improvement project is to implement routine evidence-based fetal movement patient education and a fetal movement education handout provided to all women at 28 or more weeks gestation at all routine prenatal care visits to decrease PFD rate.
Project Purpose and Goals
Methods
Results
Discussion
Conclusions
References
Decreasing Fetal Mortality: Promoting Fetal Movement Awareness and Decreased Fetal Movement ManagementEvgenia Ogorodova, MS, RN; Claire Bode, DNP, MS, CRNP, Usha Varghese, MS, CRNP
University of Maryland School of Nursing
Mid-Atlantic OBGYN clinic at a large hospital system – no standardized fetal movement education or DFM management protocol.
25000 annual PFDs in
US
478 PFDs in MD in
2017
60 PFDs in MC in
2017
Short term goals:By December 31, 2019:
• 100% of staff registered nurses (RN’s) will demonstrate competency in providing and documenting comprehensive fetal movement education by achieving a minimum score of 90% on the knowledge assessment.
• 80% of all eligible pregnant women with at least one prenatal care appointment will receive standardized fetal movement education.
• 80% of all eligible pregnant women with more than one prenatal care appointment will receive standardized fetal movement education at all appointments.
Long term goal:
By December 31, 2022 - PFD rate for women receiving care at the project site will decrease by 30% (not measured during this project implementation).
Setting - OBGYN clinic at a large urban Mid-Atlantic hospital providing maternity care and services to as many as 1,000 low income and uninsured women each year regardless of their ability to pay.
Population - Pregnant women 28 or weeks’ gestation receiving routine prenatal care at the OBGYN clinic.
Implementation procedures
Implementation period – 10 weeks.
Evidence-based Fetal Movement Education:• All routine appointments at 28+ weeks gestation• Education components:
• Expected Fetal Movements• Maternal factors affecting fetal movements• Interpretation of fetal activity variation• Kick chat/fetal movement counting methods• Contacting provider if experiencing DFM• Fetal movement written handout
• Developed handout in English and Spanish• Developed RN documentation tool
Initial 2 weeks• RN training conducted• Pre and post training knowledge
assessment completed using adapted validated assessment tool
• Documentation form, handouts, posters, and reminders for use in clinic
Following 8 weeks• RNs provided fetal movement education to
pregnant women 28+ weeks gestation at routine prenatal care appointments
• RNs documented components of fetal movement education provided
• Reminders and informal interviews conducted to identify barriers and solutions
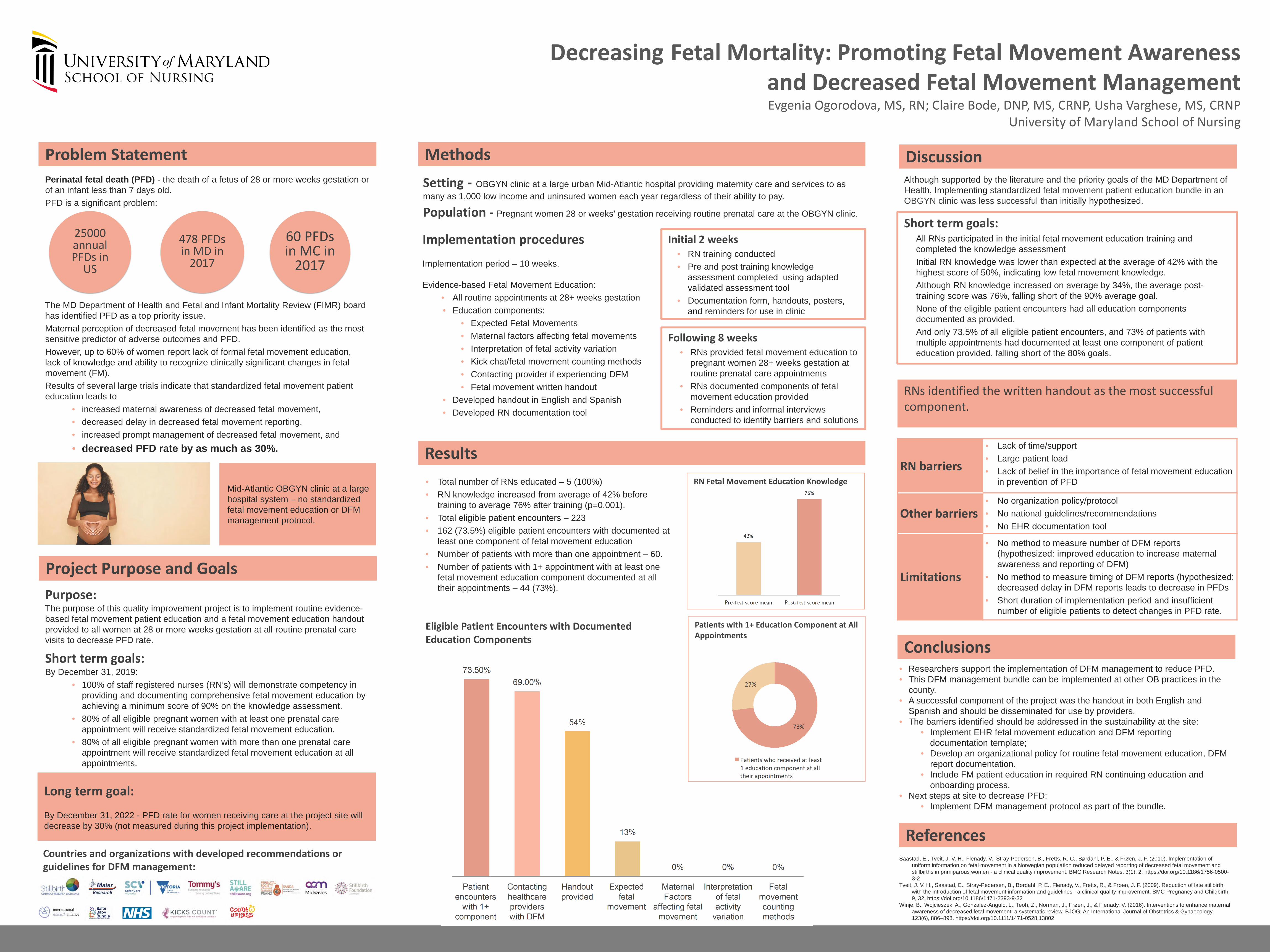
RN Fetal Movement Education Knowledge• Total number of RNs educated – 5 (100%)• RN knowledge increased from average of 42% before
training to average 76% after training (p=0.001).• Total eligible patient encounters – 223• 162 (73.5%) eligible patient encounters with documented at
least one component of fetal movement education• Number of patients with more than one appointment – 60.• Number of patients with 1+ appointment with at least one
fetal movement education component documented at all their appointments – 44 (73%).
Patients with 1+ Education Component at All Appointments
Eligible Patient Encounters with Documented Education Components
Although supported by the literature and the priority goals of the MD Department of Health, Implementing standardized fetal movement patient education bundle in an OBGYN clinic was less successful than initially hypothesized.
Short term goals:• All RNs participated in the initial fetal movement education training and
completed the knowledge assessment• Initial RN knowledge was lower than expected at the average of 42% with the
highest score of 50%, indicating low fetal movement knowledge. • Although RN knowledge increased on average by 34%, the average post-
training score was 76%, falling short of the 90% average goal. • None of the eligible patient encounters had all education components
documented as provided. • And only 73.5% of all eligible patient encounters, and 73% of patients with
multiple appointments had documented at least one component of patient education provided, falling short of the 80% goals.
RNs identified the written handout as the most successful component.
RN barriers
• Lack of time/support• Large patient load• Lack of belief in the importance of fetal movement education
in prevention of PFD
Other barriers• No organization policy/protocol• No national guidelines/recommendations• No EHR documentation tool
Limitations
• No method to measure number of DFM reports(hypothesized: improved education to increase maternal awareness and reporting of DFM)
• No method to measure timing of DFM reports (hypothesized: decreased delay in DFM reports leads to decrease in PFDs
• Short duration of implementation period and insufficient number of eligible patients to detect changes in PFD rate.
Countries and organizations with developed recommendations or guidelines for DFM management:
• Researchers support the implementation of DFM management to reduce PFD.• This DFM management bundle can be implemented at other OB practices in the
county.• A successful component of the project was the handout in both English and
Spanish and should be disseminated for use by providers.• The barriers identified should be addressed in the sustainability at the site:
• Implement EHR fetal movement education and DFM reporting documentation template;
• Develop an organizational policy for routine fetal movement education, DFM report documentation.
• Include FM patient education in required RN continuing education and onboarding process.
• Next steps at site to decrease PFD:• Implement DFM management protocol as part of the bundle.
Saastad, E., Tveit, J. V. H., Flenady, V., Stray-Pedersen, B., Fretts, R. C., Børdahl, P. E., & Frøen, J. F. (2010). Implementation of uniform information on fetal movement in a Norwegian population reduced delayed reporting of decreased fetal movement and stillbirths in primiparous women - a clinical quality improvement. BMC Research Notes, 3(1), 2. https://doi.org/10.1186/1756-0500-3-2
Tveit, J. V. H., Saastad, E., Stray-Pedersen, B., Børdahl, P. E., Flenady, V., Fretts, R., & Frøen, J. F. (2009). Reduction of late stillbirth with the introduction of fetal movement information and guidelines - a clinical quality improvement. BMC Pregnancy and Childbirth, 9, 32. https://doi.org/10.1186/1471-2393-9-32
Winje, B., Wojcieszek, A., Gonzalez-Angulo, L., Teoh, Z., Norman, J., Frøen, J., & Flenady, V. (2016). Interventions to enhance maternal awareness of decreased fetal movement: a systematic review. BJOG: An International Journal of Obstetrics & Gynaecology, 123(6), 886–898. https://doi.org/10.1111/1471-0528.13802

Violence Risk Assessment Tool:Dynamic Appraisal of Situational Aggression-Inpatient Version
Jyoti Rimal, BSN, RNBridgitte Gourley, DNP, FNP-BC, Faculty Advisor
University of Maryland School of Nursing
• Aggressive behaviors in inpatient psychiatric units are a challenging safety problem.
• Early identification of aggressive behavior is vital. • Structured violence risk assessments identify the level of risk
and allow for early interventions. • Despite this evidence, a violence risk assessment tool was not
utilized on an inpatient psychiatric unit and the rate of coercive measure as seclusion and restraints was higher than desired.
Background/Significance
Implement Dynamic Appraisal of Situational Aggression-Inpatient Version (DASA-IV) and evaluate effectiveness of tool to identify and manage patients with risk for aggression• 100% of nurses will utilize new report sheet with additional
DASA-IV items while receiving handoff report from the ED. • 100 % of the patients admitted to the unit will be screened by
nurses utilizing the DASA-IV tool.• 100% of patients who are screened moderate or high risk for
aggression will have a crisis safety plan or risk management plan.
• Incidents of seclusion, restraints and staff injuries will be reduced by 50%.
Project Purpose/Goals
Results
• The utilization of the tool was helpful in improving safety even though results were not significantly different.
• Fluctuation in acuity of the unit, staffing ratio, short implementation period and the severity of patients illness play an important role.
• Incorporating the DASA-IV tool into admission nursing assessment in EHR would increase nurses adherence.
• Establishing a standard crisis safety plan and risk management protocol would maintain consistency on the interventions provided to manage the aggressive behavior.
• Incorporating the DASA-IV score in nursing shift handoff will improve communication and also determine the acuity of the unit for the following shift.
Discussion
• The utilization of the DASA-IV tool increased staff overall awareness of patient at risk of aggression.
• Encouraged patient centered intervention to reduce the number of events such as seclusion, restraints and injuries.
• The addition of a structured tool to nurses clinical judgement for appraising risk for imminent aggression in psychiatric unit can assist nurses in the initiation or prevention intervention and improve safety.
Conclusion
DASA-IV is a violence screening tool that assesses for seven items: irritability, impulsivity, unwillingness to follow direction, sensitive to perceived provocation, easily angered when request are denied, negative attitudes and verbal threats. Each item is scored 0 if absent and 1 if present
Score of 0 or 1= low risk for aggression Score of 2-3 = moderate risk for aggression Score of >3 = high risk for aggression
• The project occurred within a 18 bed inpatient unit from October 1st through November 30th, 2019.
• Subjects included were all the unit nurses employed at the hospital (n = 17).
• The Theory of Interpersonal Relations by Hildegard Peplau (1997) guided by MAP-IT was the framework used in the project.
Implementation Procedures• Pre-education classes were held and one-on-one sessions
were given to nurses unable to attend.• All the nurses were provided with the tool and scoring guide.• Bright color reminders were posted in work stations and
computers.• Nurses utilized the report sheet updated with DASA- IV items to
receive report from ED and on all newly admitted patients.• Nurses initiated a crisis safety plan or risk management plan
based on the DASA –IV score.• Nurses filled out Post DASA Implementation Questionnaire
(PDIQ) after the completion of the project.
Methods
Figures
• Griffith, J. J., Daffern, M., & Godber, T. (2013). Examination of the predictive validity of the Dynamic Appraisal of Situational Aggression in two mental health units. International Journal of Mental Health Nursing, 22(6), 485-492. doi:10.1111/inm.12011
• Lantta, T., Kontio, R., Daffern, M., Adams, C. E., & Välimäki, M. (2016). Using the Dynamic Appraisal of Situational Aggression with mental health inpatients: A feasibility study. Patient Preference and Adherence, 10, 691-701. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4854232/
• Ramesh, T., Igoumenou, A., Montes, M. V., & Fazel, S. (2018). Use of risk assessment instruments to predict violence in forensic psychiatric hospitals: A systematic review and meta-analysis. European Psychiatry, 52, 47-53. doi.org/10.1016/j.eurpsy.2018.02.007
Acknowledgements: Thank you to my project advisor, second reader and a special thank you to Thera Blehar, MSN, RN, Unit Manager.
References
• 100% of staff nurses on the unit received training, either in class or one to one.• The compliance of using the tool during the implementation period was 63% to 89%,
with the average compliance of 74.5 %. • Out of 83 patients who were screened using DASA-IV tool, 10.8% (n = 9) screened
moderate risk for aggression and 12.05 % (n= 10) screened high risk for aggression.
• The compliance rate of nurses initiating a crisis safety plan and risk management plan individualized to patient was 100%.
• A Mann-Whitney U test showed there was not a significant difference in seclusion and restraints [U-stat = 873, U-critical = 682 (U-stat > U-critical )] and staff injuries [U-stat = 870, U-critical = 682 (U-stat > U- critical )] pre and post implementation of the tool.
• The five point Likert scale, PDIQ survey showed nurses positive perception towards the tool in managing patients aggression (M = 25.71, SD = 1.76, n = 17).
0 0 0 0
7179
63
82
6473
89
75
0102030405060708090
100
Percentage of Patients Screened During Admission Using DASA-IV Tool
Pre-implementation Implementation
01234567
Num
ber p
er 1
00 P
atie
nts
Week
Number of Seclusion/Restraints and Injuries
Staff Injury Seclusion/Restraints

Background Methods
Results
First evidence-based stress reduction program for healthy adults in the NW community
Literature supports MM and stress reduction
Despite smaller sample, less diversity and self reported measuresThis project demonstrated
MM is a brief and cost-effective program Easily to implement in various community settings Stress is reduced by practicing MM daily for 5 minutes The tool kit provided resources that can be used by PC and PP
Future QI projects should replicate MM project in Diverse sample Integrate physiological markers of stress for more reliable finding
Discussion & Conclusion
Galla, B. M., O'Reilly, G. A., Kitil, M. J., Smalley, S. L., & Black, D. S. (2015). Community based mindfulness program for disease prevention and health promotion: targeting stress reduction. American journal of health promotion, 30(1), 36-41
Nyklícek, I., Mommersteeg, P., Van Beugen, S., Ramakers, C., & Van Boxtel, G. J. (2013). Mindfulness-based stress reduction and physiological activity during acute stress: A randomized controlled trial. Health Psychology, 32(10), 1110
Sharma, M., & Rush, S. E. (2014). Mindfulness-based stress reduction as a stress management intervention for healthy individuals: a systematic review. Journal of evidence-based complementary & alternative medicine, 19(4), 271-286
Bibliography
Process : Twelve-week MM program
Pre-intervention Phase: Train the trainer program (2 hr. class) Didactic and Demonstrated sessions Prepared the PC to facilitate MM programs in various community setting. Used Pre-post questionnaires
Intervention Phase: Six-week pilot program Didactic and Demonstration sessions Prepared the PP to self manage their stress level Used an audit tool.
Post-intervention Phase: Five-weeks PP practiced 5 minutes MM daily until the end of the DNP project. Used a daily log to track MM practice The program concluded with a reunion Used a survey questionnaire at the end PP self monitored their stress using Perceived Stress Scale
Mindfulness-Based Meditation and Stress Reduction
in Healthy Adults
Nomy Thomas Jacob, RN, BSN, SCRN, CNRN, Dr. Karen Elizabeth Scheu, DNP, FNP-BC.
Stress is a public health concern as it affects the health of communities
2019 county health rankings reveal higher stress levels inNorthwest Maryland. e.g. driving alone 85% compared to74% in Maryland (MD)
Community members in Northwest (NW) county, MD were actively seeking solutions to their stress at the Community Outreach and Health Improvement (COHI) HealthLink
No stress reducing resources existed
Mindful Meditation (MM) is an integral part of an evidence-based Mindfulness Based Stress Reduction (MBSR) course that reduces stress.
Figure#1a Figure#1b
Figure#1c Figure#1d
Figure#2 Figure#3
The post-survey showed an increase in knowledge and skill level of PC and their perception of using the resource tool kit(figure#1a, 1b, 1c, 1d)
More than 70% of PP attended each week's pilot class (figure#2)
More than 50% PP stated MM program was useful to reduce stress (Fairly useful: 85.71%, Extremely useful: 14.29%) (figure#3)To evaluate the feasibility of a mindfulness-based meditation
program among healthy, stressed adults in the community.
Goals
Project champions (PC) knowledge and skill related to stress and MM may increase after the train the trainer class
The resource tool kit may be used as a guide
70% of the project participants (PP) may attend the entire 6-week pilot program
50% of the PP may state that MM is useful to reduce stress
Purpose & Goal
Results
How useful is MM
program?
Extremely Useful-1
Fairly Useful-2
Not very Useful-3
Not at all useful-4
Methods
Quality Improvement Project
Setting: COHI department.
Sample
Train the program: 4 participants Included staffs of COHI department (PC) Pilot Program: 8 participants Recruited through word of mouth and email Included healthy stressed adults ≥18 years old with no chronic
diseases