implementing cusp: a pilot experience - atlantic quality...
TRANSCRIPT
Implementing CUSP: A Pilot Experience Successes, Challenges, and Lessons Learned
St. Peter’s Hospital
February 11, 2016
.
. Susan Senecal, MBA, RN, CPHQ Susan is a healthcare administrator and researcher who has been providing oversight for development and implementation of patient safety and quality initiatives at St. Peter’s Health Partners Albany Acute Division since October 2013. With over 25 years in healthcare quality, she has held leadership positions in managed care, homecare and public health. Prior to joining SPHP she spent five years directing grant funded programs within the New York State Department of Health on pharmacy safety and a national medical malpractice demonstration project that sought to reduce costs associated with malpractice lawsuits and improve patient safety by reducing preventable medical injuries. She earned her Masters in Business Administration from Union University, her Baccalaureate degree from St. Lawrence University and is a registered professional nurse. Jennifer Ryan, MSN, RN, CIC, CEN Jennifer joined St. Peters Health Partners in 2011 and became the Manager of the Infection Prevention and Control Program in 2015. Throughout her career, Jennifer has worked with the NYS Pediatric Sepsis Workgroup and the NYS Perinatal Quality Collaborative Neonatal Intensive Care Unit CLABSI Reduction Initiative. She has held leadership positions in pediatric and adult EDs as well as the Pediatric Intensive Care Unit (PICU). Jennifer obtained her Bachelors in Science in Nursing from Nova Southeastern University in 2008, and a Masters of Science in Nursing, with a focus on Nursing Education from the University of Mary in 2015. She has a dual certification in infection control and epidemiology, as well as emergency nursing.

. Natasha Delehanty, RN, BSN Natasha has worked at St. Peter’s Hospital for 20 years. In 2013, Natasha became Operations Manager of 6 McAuley – a General Surgery, Urology, and Gynecology/Oncology unit. In addition to her current managerial role, Natasha has an extensive background in medicine, and has specialized in Diabetes and Respiratory Care. She also has a strong interest in public health, including community health. Natasha obtained an Associates Degree in Nursing at SUNY Morrisville, and a Bachelor’s of Science in Nursing from SUNY Institute of Technology. Elaina Heagerty, MPH Elaina joined St. Peter’s Hospital in 2015 as a Patient Safety and Quality Improvement Specialist, and is responsible for providing project management, facilitation, and implementation support with a variety of interdisciplinary teams and system-wide quality indicators. Prior to joining St. Peter’s, Elaina was Program Manager of Quality Improvement at the United Hospital Fund in New York City, during which she provided program management support for multiple grant initiatives, and served as a Project Manager with the New York State Partnership for Patients. Elaina has a bachelor’s degree in Biology and Public Policy from Syracuse University, and a masters in public health, with a concentration in health policy, from the Mailman School of Public Health at Columbia University.
St. Peter’s Hospital • St Peter’s Hospital is a 482 bed acute
tertiary care facility in Albany, NY that provides comprehensive care to the community.
• SPH provides care to more than 4,000 persons daily. In 2015 SPH experienced 132,232 Patient Days with 26,771 In-Patient Discharges, 2,598 Births and 16,435 Surgical Cases.
• In addition to inpatient services, there were 55,843 Emergency Room Visits, 524,347 Outpatient Visits, and 69,376 visits to our Ambulatory Care Network Sites.

Core Pilot Team Members

Creating Patient Safety Culture at St Peters Hospital
• Patient Safety and Quality Improvement Department
• Administration of the AHRQ HSOPS culture • Educate staff on tools used in patient safety • Organizational PDSA projects aimed at
preventing harm • Collaboration with external partners • Leverage success

CAUTI Rates by Intervention Timeline Ra
te p
er 1
000
cath
day
s
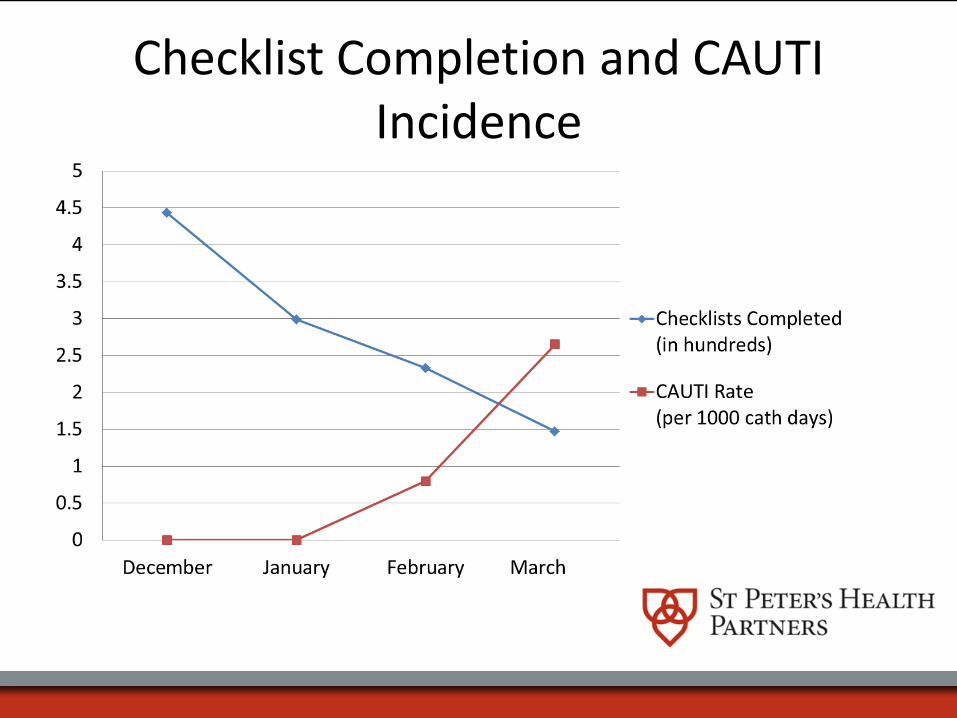
Checklist Completion and CAUTI Incidence
Urinalysis with Reflex to Urine Culture • 2014: 25% of CAUTIs
– Negative Urinalysis – No urinalysis at all
• 5/2015: Urine Culture with Urinalysis order – UA WBCs≥10 – Nitrites – Urine Culture for Special Considerations:
• Pregnant women • Infants up to 6 months of age • Neutropenic patients • Patients undergoing a urologic procedure • Outpatients (Offices may have a dipstick)
SPH Wins:
• 41% decrease in number of inpatient urine cultures processed
• 38% decrease in urine cultures from the ED • Antimicrobial stewarding: No treatment of asymptomatic bacteriuria
• 56% reduction in CAUTI’s

The Unicorn: Sustainability
Strong improvements are made, but with concurrent goals, how to maintain focus/gains?
MD/Nurse-Driven Protocol for Removal Device Rounds Twice Weekly
Concept of Unit-based safety champion as a means to focus efforts

Multi-Unit CUSP Pilot • 3 Inpatient Units:
– ICU – 4 Pavilion (Telemetry/Post-Cardiac Intervention
Medical Unit) – 6 McAuley (Urology/Gynecology Surgical Unit)
• Unit operation managers, infection control, and quality staff attended HANYS/IPRO kickoff conference in May 2015
• Pilot Planning began in Summer 2015
Pre-CUSP Activities • Bi-weekly meetings with infection prevention and unit operation
managers and monthly HANYS/IPRO CUSP-CAUTI Prevention webinars
• Reviewed unit-level CAUTI rates and catheter utilization
• Conducted CAUTI Guide to Patient Safety (GPS) Survey – Found opportunities for improvement with physician
championing/engagement and patient/family requests for catheter insertion
• Presented pilot plan and pre-CUSP activities to senior hospital
management
CUSP Implementation • October 2015: Conducted CUSP Staff Safety Assessment on
each of the 3 pilot units. Operations Managers began to talk about CUSP informally with staff.
• November 2015: Posted “CUSP Boards” on units for early awareness and introduction to CUSP concepts.
• January 2016: Launched intensive 1 hour staff education sessions on CUSP and Science of Safety on 6 McAuley. – Captured day, night, and weekend staff – 4 Pavilion and ICU session planning in progress

6 McAuley CUSP Sessions

CUSP Staff Safety Assessment 6 McAuley

6 McAuley CUSP Board

6 McAuley CUSP Structure • CUSP Meetings:
– Monthly 6 MC CUSP team meetings; alternate with Staff Meetings
– Will address “defects” (issues) on the unit that are brought forward by staff
– Physician and mid-level provider engagement
• CUSP Staff Safety Assessment: – Can be done anytime for any defect or issue staff think could
harm a patient – Will be done formally with all staff every ~6 months
• Teamwork and Communication – Ongoing use of CUSP tools and methodology

Challenges
• Unit readiness – Pre-CUSP staff awareness, learning, and planning are essential.
• Time constraints with holding staff educational sessions
– Initial time investment in learning, implementing and spreading the CUSP model is necessary.
• Perception of competing initiatives and projects
– Clear messaging on how various quality, safety, and Just Culture efforts can be integrated into the CUSP model.
Next Steps • Conduct CUSP Educational Sessions on two remaining
pilot units
• Utilize eCUSP project management software for ongoing issue/“defect” project planning and resolution
• Spread CUSP to 2 additional units by Spring 2016
• Integrate CUSP into AHRQ Safety Culture Survey efforts

eCUSP: Project Tracking
Thank you!