implications of the inpatient prospective payment system final rules
TRANSCRIPT
JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4 13
This article was prepared in response to theCenters for Medicare & Medicaid Services (CMS)publication of the Inpatient Prospective PaymentSystem (IPPS) Final Rules for FY 2008 and 2009which placed additional requirements on hospitalsfor certain hospital-acquired conditions. This articleaddresses these rulings and the implications forhealthcare facilities, including strategies for dealingwith challenges created by the rulings.
INTRODUCTION
The Centers for Medicare & Medicaid Services (CMS) of the Department of Health and Human Services issueda final rule on Aug.1, 2007, to revise the acute care hospitalInpatient Prospective Payment Systems (IPPS).
It is safe to say that previously most risk management professionals did not fully comprehend the intricacies ofthe IPPS nor did they deal directly with the IPPS as partof their daily activities. That is not the case today.
While the final rule (published in the Federal Register Vol. 72, No. 162 on Aug. 22, 2007) made significant changes,some of which will be highlighted here, most disquieting torisk management professionals is the provision that preventsMedicare from paying hospitals higher diagnosis-relatedgroup (DRG) payments for additional costs associated withcertain hospital-acquired conditions effective beginningfiscal year 2009 (Oct.1, 2008).
Subsequent to the rule published in August 2007, addi-tional requirements were added in the fiscal year 2009IPPS final rule released July 31, 2008, and published inthe Federal register on Aug. 19, 2008. Of particular note:the addition of new hospital-acquired conditions (HAC).
In the draft rules, CMS had recommended and requestedpublic comment on adding nine new hospital-acquiredconditions (HACs). The IPPS final rule for FY 2009selected two out of the nine for inclusion, and expandedone previously listed HAC bringing the total number ofHACs up to 10 effective Oct. 1, 2008 (the start of CMSfiscal year 2009).
Other changes to previously approved HACs include:• An additional code to the HAC for a foreign body
retained after surgery to now include an acute reactionto foreign substances accidentally left during a procedure
• Two new ICD-9-CM codes for pressure ulcers stagesIII and IV.
Background of the IPPS final ruleThe IPPS creates incentives for hospitals to operate efficientlywhile ensuring that payments adequately compensate hospitalsfor legitimate costs. The minimization of unnecessary costis another objective.(1)
Two noteworthy pieces of legislation were, in part, responsiblefor the IPPS final rule as published for fiscal year 2008: the Deficit Reduction Act of 2005 (Pub. L. 109-171)(DRA) and the Medicare Improvement and Extension Actunder Division B, Title 1 of the Tax Relief and Health CareAct of 2006 (Pub. L. 109-417).
The Deficit Reduction Act. Under the final rule,amendments made by the DRA Section 5001(a) wereimplemented to expand hospital reporting requirementsfor quality data effective for fiscal year 2007 (beginningOct. 1, 2007) and subsequent years. The most discussedprovisions of the final rule centered on Section 5001(c) ofthe DRA, which required the secretary of Health andHuman Services to select, by Oct. 1, 2007, at least twoHACs that meet certain specified criteria that will be sub-ject to a quality adjustment in DRG payments during fis-cal year 2008.(2)
The criteria for selection of the two conditions were thatthey are a) high cost or high volume or both, b) result inthe assignment of a case to a DRG that has a higher pay-ment when present as a secondary diagnosis and c) couldreasonably have been prevented through the application ofevidence-based guidelines.(3) Section 5001(c) also requireshospitals to submit the secondary diagnoses that are presenton admission (POA) when reporting payment informationfor discharges on or after Oct.1, 2007.
ENTERPR I S E R I SK MANAGEMENT
Implications of the Inpatient ProspectivePayment System final rulesBy Roberta Carroll, RN, ARM, MBA, CPCU, CPHQ, CPHRM, LHRM, HRM, DFASHRM
continued on next page
14 JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4
Medicare Improvements and Extension Act(Under Division B, Title 1 of the Tax Relief and HealthCare Act of 2006). Section 1886(d)(4)(C) of the actrequires that the secretary adjust the DRG classificationand relative weights at least annually. Adjustments aremade to reflect changes in treatment patterns, technologyand any other factors that may change the relative use ofhospital resources.(4)
The Medicare Payment Advisory Commission (MedPAC)is required to submit an annual report to Congress on itsreview and recommendations on Medicare payment policies.The CMS efforts focused on making significant reformsto the IPPS consistent with the recommendations madeby MedPAC in its “Report to the Congress, Physician-Owned Specialty Hospitals” in March 2005. MedPACrecommended that the secretary refine the entire DRGsystem by taking into account the severity of illness andapply hospital-specific relative value (HSRV) weights toDRGs.(5)
To facilitate those changes, the current CMS-DRG classi-fication system that has been in use for Medicare paymentsfor more than 20 years was reformed. The final rule for theIPPS revised and expanded the then current CMS-DRGclassification system in fiscal year 2007 from 538 DRGsrepresenting 25 major diagnostic categories to the newMedicare Severity-Diagnosis-Related Group (MS-DRG)classification system of 745 DRGs.
Hospital-acquired conditions, including infections
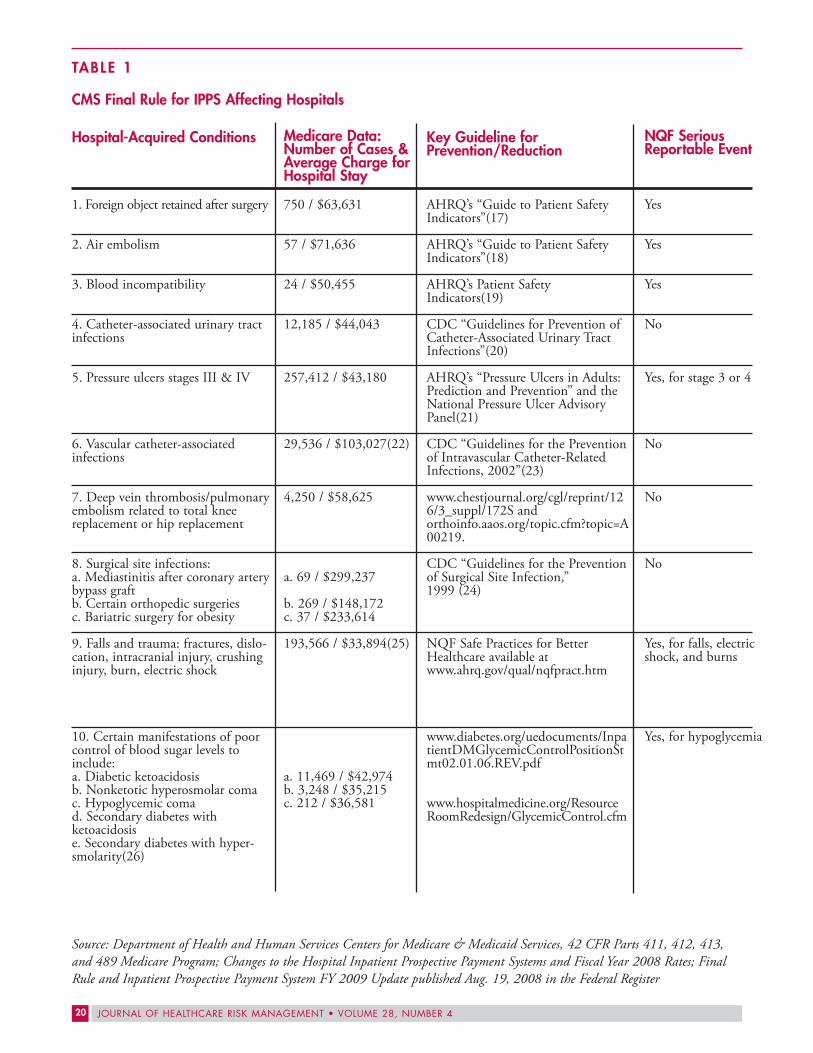
For discharges occurring on or after Oct. 1, 2008 (fiscalyear 2009) hospitals will not receive additional paymentfor cases in which one of the selected conditions (as seenin Table 1) was not present upon admission or if the documentation is insufficient to determine if the conditionwas present at the time of admission. The case will bepaid as though the secondary diagnosis was not present.
As noted in the Regulatory Impact Analysis Section VII Aof the final rules, these provisions will only apply when theselected condition (as seen in Table 1 on page 20) is theonly secondary diagnosis present on the claim that willlead to a higher payment. If a non-selected (not on theHAC list) secondary diagnosis that leads to the samehigher payment is on the claim, the case will continue to be assigned to the higher paying DRG.
Patients having one major complication or co-morbidity(MCC) or complication or co-morbidity (CC) will frequentlyhave additional conditions that also lead to higher payment.Therefore in only a small percentage of cases will the patienthave only one secondary diagnosis that would lead to thehigher un-reimbursed payment.
While most hospitals have already determined the financialimpact of non-payment for hospital-acquired conditions,others that have not done so should determine the impactby reviewing Medicare billing data for fiscal year 2008
(ending Sept. 30, 2008) with DRG codes that would haveresulted in a higher payment. The Regulatory ImpactAnalysis for HACs as reported in the fiscal year 2008 finalrule (at page 48168) estimates savings for the five fiscalyears starting in fiscal year 2009 to be $20 million per year.
In an effort to deliver patient-centered care, most healthcareorganizations have developed and implemented compre-hensive strategies supported by initiatives in patient safety,quality improvement and enterprise risk management –all with the goal to enhance the quality of care, decreaseclinical variability and promote a safe environment.
RISK MANAGEMENT STRATEGIES
There are many strategies that can be implemented toreduce the potential for loss of reimbursement to anorganization. The following are a few of those strategies:
• Prevent hospital-acquired conditions, including infections.The final rules suggest several evidence-based preventiveguidelines (See Table 1 for a list of recommendedguidelines.). Ensure that all preventive guidelines are in place as recommended or that equivalent protocolsare implemented.
• Review physician compliance with adopted protocols,guidelines and best practices as part of the peer reviewprocess. Evaluate ongoing clinical competency of indi-vidual practitioners rather than the semi-annual reviewconducted on reappointment.
• Develop pre-admission and admitting screening/testingguidelines to determine diagnoses that are present atadmission such as pressure ulcers, fractures, burns, etc.
• Educate staff on “present on admission” (POA) codingrequirements.
• Report HACs to others in the organization, such aspatient safety and quality management. Many of theHACs may be potentially compensable events (PCEs),generate a claim of negligence or a demand for compensation, and require disclosure to the patientand/or family.
• Understand jurisdictional requirements as they pertainto the mandatory external reporting of adverse events.Many of the HACs listed in Table 1 are also reportableunder adverse event reporting statutes in many states.
• Evaluate HACs and any dollars expended to settlepotential claims for mandatory reporting to CMS asJuly 1, 2008, as required by the Medicare, Medicaidand SCHIP Extension Act of 2007(6)

JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4 15
continued next page
• Stress the importance of appropriate and adequate documentation. Coders, physicians and nurses need tofully comprehend the implication of poor documentationon the ability of the organization to code, bill and collecton diagnoses that are POA.
• Consider the development of standardized assessmenttools and admission checklist to facilitate the identifi-cation of POA secondary diagnoses.
Exclusions to the IPPS final ruleThe following facilities are excludedfrom the IPPS final rule:
• Rehabilitation hospitals and units• Long-term care hospitals• Psychiatric hospitals and units• Children’s hospitals• Cancer hospitals• Maryland waiver hospitals• Religious nonmedical healthcare
institutions.
Risk management implicationsand initiativesImplications for non-compliancewith certain sections of the finalrules are clear.(7) However, lack ofadherence with other sections of the final rules are yet to beseen, but clearly include loss of future revenue, additionalcost to comply and negative impact on an organization’sreputation.
The impact of the public on the final rules will be long-reaching as patients continue to be informed about HACsand as healthcare providers continue efforts to communicatewith patients and the public in a transparent manner.
It is also important to keep in mind that other payers haveinitiated non-payment policies that directly affect the paymentfor adverse events that occur in the hospital.
HealthPartners, a Minneapolis-based health plan, imple-mented a policy in January 2005 that provides for with-holding payments to hospitals for “never events.” “Neverevents” is the term coined for the original list of 27 eventsidentified by the National Quality Forum (NQF) in 2002as events that should not occur in a hospital. That list waslater revised and expanded to include 28 serious reportableevents.
The Leapfrog Group and other organizations are callingfor hospitals to waive billing for HACs as well. Individualstates such as Massachusetts and Minnesota, working withtheir respective state hospital associations, are following suitin not billing patients and payers for what are consideredpreventable adverse events.
In addition, state Medicaid programs will quickly followsuit as CMS (upon release of the IPPS for FY 2009 onJuly 31, 2008) sent every state Medicaid director a letterproviding information about how states can adopt the samenever events practices. They were encouraged to adopt thesame non-payment policies outlines in the fiscal year 2009final rule. Approximately 20 states have considered or areconsidering methods to eliminate payment for some neverevents.(8)
So, what does this mean to risk management professionals?What role can and should they take? What initiatives can theyimplement that will improve patient safety, maintain com-
pliance, enhance fiscal soundness andadd value? What should they do first?
Ten steps to compliance: An ERM approach
The following steps can be used as arisk management guide for developingstrategies:
1. Understand that compliance withthe final rules requires a broad approachthat encompasses the total organization,in other words, an enterprise riskmanagement (9) approach. Enterpriserisk management initiatives are notthe responsibility of a single person.They require the active participation
of many from all levels of the organization.2. Enlist the active involvement of the appropriate people
and have a coordinated, planned approach to conserveresources. It is recommended that a multi-disciplinarytask force be created to address the requirements of thefinal rules. This task force should represent the variousconstituents responsible for implementing the varioussections of the final rules and may include representa-tives from the medical staff, nursing, infection control,medical records, finance, billing and coding, qualityassurance/quality improvement, information technology,patient safety, risk management, patient advocacy, corporate compliance and legal.
3. Once the initial task force members have been assignedand have had the opportunity to meet, each membershould read the text of both fiscal years 2008 and 2009final rules.(10) Next, the task force should determinehow the work will be divided and assignments made.Individual task force members can be assigned accounta-bility according to areas of expertise or responsibility tolead a designated sub-group (work-group) to focus onspecified sections of the final rules.
4. Evaluate the financial impact. Assigned work groupsshould determine the potential revenue impact for eachsection of the final rules. The cost to implement thevarious sections of the final rules should be quantified,also. In several sections of the final rules, CMS analyzed
So, what does thismean to risk manage-ment professionals?What role can andshould they take?

16 JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4
the resource consumption in terms of dollars and time;with many others sections, however, the cost has notbeen analyzed.Consider what impact lost revenue and additionalexpense related to resource consumption to complywith the final rules will have on the total cost of risk. A determination of how the organization will accountfor waivers, write-offs and non-payment of HACs incosts allocation and claims attribution programs needsto be made as well. A determination as to the impactthe MMSEA of 2007 will have on mandatory reportingneeds to be made as well; keeping in mind the abilityof CMS to levy fines of $1,000 per day/per claims fornon-reporting.
5. Using the individual work groups to identify any new(or existing) exposures to loss created by the final rules,review the efficacy of current loss prevention effortsand recommend initiatives to mitigate new risks. Aslisted in Table 1, the final rules clearly identify currentlyavailable preventive standards and guidelines foundedon evidence-based medicine that hospitals can adopt to prevent HACs.
6. Engage the task force in a review of the list of exposuresand risk mitigation initiatives recommended by the workgroups and assist in prioritizing those recommendations.The following factors ought to be considered:• Seriousness of the risk• Availability and cost of necessary resources• Frequency of the risk• Availability of loss prevention guidelines• Time to implement.
7. Develop and implement a communication plan for allaffected employees and units.
8. Develop and implement the risk mitigation initiativesrecommended.
9. Monitor the effectiveness of all risk mitigation initiativesimplemented to ensure compliance with the final rules,determine the effectiveness of the risk mitigation initiatives, and determine the financial impact.
10. Continue to monitor and make changes when andwherever necessary.
The final rules offer a great deal of background informationincluding comments from the field reviews along with theformal responses from CMS. Part of that backgroundmaterial also highlights the rationale of why each HACwas chosen as well as why other conditions were not selectedfor inclusion at this time. While it is difficult to determineexactly what conditions will be added/eliminated in subsequentyears, the fiscal year 2009 final rule identifies additionalpotential candidate HACs that were suggested throughcomments. They include the following:
Additional potential candidate HACs, suggestedthrough comment
• Surgical site infection following device procedures• Failure to rescue• Death or disability associated with drugs, devices or
biologics• Events on the NQFs list of Serious Reportable Adverse
Events, not previously addressed by the HAC paymentprovision
• Dehydration• Malnutrition• Water-borne pathogens, not previously addressed by
the HAC payment provision.
Other significant revisionsSeveral other revisions in the IPPS final rule that shouldbe of interest to the risk management professional, buthave been overshadowed by the HAC requirements, are:• Reporting of quality measures for fiscal year 2008• Changes in Emergency Medical Treatment and Labor Act,
42 U.S.C. §1395dd (EMTALA) regulations during andeclared emergency
• Disclosure of physician ownership in hospitals andpatient safety measures
• Development of a Medicare hospital value-based purchasing plan.
Quality measuresSection 5001(a) of the DRA sets out new requirements forthe Reporting Hospital Quality Data for Annual PaymentUpdate (RHQDAPU) program. RHQDAPU builds onthe ongoing voluntary Hospital Quality Initiative (HQI).Hospitals are required to report quality measures ofprocess, structure, outcomes, patient’s perspective on care,efficiency and cost of care that relate to services furnished ininpatient settings on the CMS Web site. Hospitals submitquality data through the QualityNet Exchange secure Website (www.qnetexchange.org). Data from this initiative areused to populate the Hospital Compare Web site,www.hospitalcompare.hhs.gov.(11)
Effective fiscal year 2007 and for all subsequent fiscalyears, the financial penalty for not reporting quality dataas provided under section 5001(a) of the DRA is a 2.0percentage point reduction in the payment update.Section 1886(b)(3)(B)(viii)(I) of the act also provides thatany reduction in a hospital’s payment update will applyonly with respect to the fiscal year involved, and will not betaken into account for computing the applicable percentageincrease.(12)

JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4 17
continued on next page
To be eligible for a full market-basket update in fiscal year2009, hospitals must report on 30 quality measures.These 30 measures include all of the previously reportedmeasures as well as three additional measures adopted lastfall. The new measures include one new outcome measureof pneumonia care and two measures of surgical care,including:• Pneumonia 30-day mortality• Cardiac surgery patients with controlled 6 a.m.
postoperative serum glucose• Surgery patients with appropriate hair removal.(13)The fiscal year 2009 final rule also made changes to theRHQDAPU program effective fiscal year 2010. CMS hadoriginally proposed in the draft rule for fiscal year 2009that 43 quality measures be added to the already required30, bringing the recommended quality measures to bereported up to 73. Because of public comments receivedfrom ASHRM and lobbying efforts by organizations suchas the American Hospital Association, CMS elected to onlyimplement 13 of the 43 recommended measures, retiringone quality measure (pneumonia oxygenation assessment),bringing the number of reportable quality measures forfiscal year 2010 (effective Oct.1, 2009) to 42. The 13 new measures include:
• Surgical Care Improvement Project (SCIP)o Surgery patients on a beta-blocker prior to arrival
who received beta blocker during the perioperativeperiod
• Nursing Sensitive Measureso Failure to rescue
• Readmission Measureso Heart failure 30-day risk standardized
readmission measure (Medicare only)
• AHRQ Inpatient Quality Indicators (IQI):o Abdominal aortic aneurysm (AAA) mortality rate
(with or without volume)o Hip fracture mortality rate
• AHRQ Patient Safety Indicatorso Death among surgical patients with treatable
complicationso Iatrogenic pneumothorax, adulto Postoperative wound dehiscenceo Accidental puncture or laceration
• AHQ IQI Composite Measureso Mortality for selected medical conditions
(composite)o Mortality for selected surgical procedures
(composite)o Complication/patient safety for selected
indicators (composite)o IQIs
• Cardiac Surgery Measureso Participation in a systematic database for cardiac
surgery.Note: Two additional measures for heart attack and pneumo-nia are expected to be endorsed by the National QualityForum in 2009 with CMS adoption in 2010.
Additional IPPS clarificationsWhile the IPPS final rule for fiscal year 2009 addressedother changes too numerous to discuss in this article,there are a few additional clarifications that deserve men-tioning. They include the following:
• Clarification that a hospitals EMTALA obligation endswith a patient’s admission.
• Approval for hospital to meet its on-call obligationthrough participation in a “community-call plan”:o Community call allows for a group of self-
selected hospitals in a self-designated region to collectively provide on-call services
o Community call allows for a specific hospital to be the designated on-call facility for all of the hospitals involved for a specified service, specified time or both.
• The new community call regulations require a formalplan that includes the following elements:o Clear delineation of responsibilities for each
participating hospitalo A description of geographical area covered by
the plano Representative’s signature of participating
hospitalo Assurances local/regional EMS protocols include
information on community on-call arrangementso Statement reaffirming the obligation of each
participant to meet EMTALA obligations for medical screening exam and stabilizing treatment within its capacity, and comply with transfer requirements
o Annual assessment of the plan by hospital participants.
Emergency Medical Treatment and Labor Act(EMTALA)EMTALA regulations at 42 CFR 489.24 were amendedto reflect changes made by the Pandemic and All-HazardsPreparedness Act, Pub. L. 109-417 section 302(b) and toensure that the final rule accurately reflects section 1135of the Social Security Act.
The proposed revisions to §489.24 were adopted as final,without modification, and “specify that the sanctions thatdo not apply are those for either the inappropriate transferof an individual who has not been stabilized, or those forthe direction or relocation of an individual to receivemedical screening at an alternate location.”
Pearls of Risk Management WisdomTo Minimize Liability Exposures
ObstetricsA medical specialty with high professionalliability exposure.
Communication BreakdownsA leading root cause of sentinel events.
ASHRM experts address these hot areas with two new booklets.In a pocket-sized, user-friendly format ideal for sharingwith staff, ASHRM’s Pearls cover risk management issuesthat healthcare workers encounter on a daily basis:
“Risk Management Pearls for Obstetrics” (2nd ed.) • Informed Consent and Documentation• Disclosure• EMTALA• Reducing Adverse Outcomes: A Systems Approach• Quality Improvement• The Placenta as a Risk Management Tool• Ethical and Mental Health Issues
“Risk Management Pearls To Enhance Communication”• Communication with Patient and Family• Communication Among Caregivers• Critical Communication Processes
... with scenarios to illustrate the tips and strategies in various healthcare settings
Available singly or in specially priced 5-packs. Preview and purchase online at www.ashrm.org/pearls
JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4 19
“Waiver of these sanctions for EMTALA violations is limitedto a 72-hour period beginning upon the implementation of ahospital disaster protocol, except that if a public health emergencyinvolves a pandemic infectious disease (such as pandemicinfluenza), the duration of the waiver will be determined in accordance with section 1135(e) of the Act as it applies to public health emergencies.”(14)
Disclosure of physician ownership in hospitalsand patient safety measuresIn the furtherance of patient-centered care, disclosure,transparency and patient safety, it is in the interest ofpatients who are provided services by the hospital to bemade aware of certain issues concerning the availability of physicians for inpatient emergencies and any ownershipinterest physicians have in the hospital where theirpatients are receiving services.(15)
Physician Ownership. Section 489.20(u)(1) requiresphysician-owned hospitals, as defined in §489.3, to furnishwritten notice to all patients that the hospital is a physician-owned hospital and that the list of physician owners isavailable upon request. The notice must be furnished atthe beginning of their hospital stay or outpatient visit.
In order to enforce these proposed requirements, §489.12is amended to permit CMS to deny a provider agreementto a hospital that does not have procedures in place tonotify patients of physician ownership in the hospital. Inaddition, §489.53 is amended to permit CMS to terminatea provider agreement with a physician-owned hospital ifthe hospital fails to comply with the requirements of§489.20(u).
Fiscal year 2009 IPPS final rule clarifies disclosure require-ments to include an immediate family member of a physicianwho holds an ownership or investment interest.
Exemptions:• No physician owners who refer patients to the hospital• No referring physicians who have an immediate family
member with an ownership or investment interest inthe hospital.
Patient Safety Measures. 42 CFR 489.20(v) requires thathospitals and critical access hospitals (CAHs) furnish allpatients written notice at the beginning of their hospitalstay or outpatient service if a doctor of medicine or a doctorof osteopathy is not present in the hospital 24 hours perday, 7 days per week, and to describe how the hospital orCAH will meet the medical needs of any patient whodevelops an emergency medical condition at a time whenno physician is present in the hospital.
Development of the Medicare hospital value-based purchasing planSection 5001(b) of the Deficit Reduction Act of 2005requires the Secretary of Health and Human Services to“develop a plan to implement a value-based purchasingprogram for payments under the Medicare program forsubsection (d) hospitals beginning with fiscal year 2009.”Congress specified that the plan include consideration ofthe following issues:
• The ongoing development, selection and modificationprocess for measures of quality and efficiency in hospitalinpatient settings
• The reporting, collection, and validation of qualitydata
• The structure of value-based payment adjustments,including the determination of thresholds or improve-ments in quality that would substantiate a paymentadjustment, the size of such payments, and the sourcesof funding for the value-based payments
• The disclosure of information on hospital performance.
CONCLUSIONThe revised IPPS as seen in the final rules released inAugust 2007 and July 2008 supports a wide variety ofviews and opinions. Many healthcare stakeholders offerdiffering opinions as to its value, ability to implement andfairness. Patients, clinical practitioners, healthcare admin-istrators, payers, and regulators (to name a few), all haveopinions.
Even within the healthcare facility there are wide differencesin opinions. The quality assurance and patient safety professional may say, “Finally! Now we'll get moreresources to implement much needed safety strategies,”while the practitioner may be fearful of the time and extrapaperwork necessary to document secondary diagnosesPOA. Comprehending the details and full ramifications of the final rules on the organization will take the riskmanagement professional time and the assistance of manyothers within the organization.
The final rules mandate that hospitals be accountable, fiscallyprudent, patient-centered and responsible providers ofcare. Healthcare providers can no longer offer rhetoric toevidence-based practice. They must translate and implementthat knowledge into everyday practice. While this shouldnot be a new charge for hospitals, it nonetheless offers newchallenges and opportunities. How they manage thesechanges will dictate how successful they will be in the future.
(continued on next page)
20 JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4
TABLE 1
CMS Final Rule for IPPS Affecting Hospitals
Hospital-Acquired Conditions
1. Foreign object retained after surgery
2. Air embolism
3. Blood incompatibility
4. Catheter-associated urinary tractinfections
5. Pressure ulcers stages III & IV
6. Vascular catheter-associated infections
7. Deep vein thrombosis/pulmonaryembolism related to total kneereplacement or hip replacement
8. Surgical site infections:a. Mediastinitis after coronary arterybypass graftb. Certain orthopedic surgeriesc. Bariatric surgery for obesity
9. Falls and trauma: fractures, dislo-cation, intracranial injury, crushinginjury, burn, electric shock
10. Certain manifestations of poorcontrol of blood sugar levels toinclude:a. Diabetic ketoacidosisb. Nonketotic hyperosmolar comac. Hypoglycemic comad. Secondary diabetes with ketoacidosise. Secondary diabetes with hyper-smolarity(26)
NQF SeriousReportable Event
Yes
Yes
Yes
No
Yes, for stage 3 or 4
No
No
No
Yes, for falls, electricshock, and burns
Yes, for hypoglycemia
Key Guideline forPrevention/Reduction
AHRQ’s “Guide to Patient SafetyIndicators”(17)
AHRQ’s “Guide to Patient SafetyIndicators”(18)
AHRQ’s Patient SafetyIndicators(19)
CDC “Guidelines for Prevention ofCatheter-Associated Urinary TractInfections”(20)
AHRQ’s “Pressure Ulcers in Adults:Prediction and Prevention” and theNational Pressure Ulcer AdvisoryPanel(21)
CDC “Guidelines for the Preventionof Intravascular Catheter-RelatedInfections, 2002”(23)
www.chestjournal.org/cgl/reprint/126/3_suppl/172S andorthoinfo.aaos.org/topic.cfm?topic=A00219.
CDC “Guidelines for the Preventionof Surgical Site Infection,” 1999 (24)
NQF Safe Practices for BetterHealthcare available atwww.ahrq.gov/qual/nqfpract.htm
www.diabetes.org/uedocuments/InpatientDMGlycemicControlPositionStmt02.01.06.REV.pdf
www.hospitalmedicine.org/ResourceRoomRedesign/GlycemicControl.cfm
Medicare Data:Number of Cases &Average Charge forHospital Stay
750 / $63,631
57 / $71,636
24 / $50,455
12,185 / $44,043
257,412 / $43,180
29,536 / $103,027(22)
4,250 / $58,625
a. 69 / $299,237
b. 269 / $148,172c. 37 / $233,614
193,566 / $33,894(25)
a. 11,469 / $42,974b. 3,248 / $35,215c. 212 / $36,581
Source: Department of Health and Human Services Centers for Medicare & Medicaid Services, 42 CFR Parts 411, 412, 413,and 489 Medicare Program; Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates; FinalRule and Inpatient Prospective Payment System FY 2009 Update published Aug. 19, 2008 in the Federal Register

JOURNAL OF HEALTHCARE RISK MANAGEMENT • VOLUME 28, NUMBER 4 21
ABOUT THE AUTHORRoberta Carroll, RN, ARM, MBA, CPCU, CPHQ,CPHRM, LHRM, HRM, DFASHRM, is senior vice president,Aon Healthcare, Tampa, FL, and editor of ASHRM’s RiskManagement Handbook for Healthcare Organizations.
REFERENCES
1. Federal Register Vol. 72, No. 162 / Aug.22, 2007 /Rules and Regulations, p. 48157
2. Federal Register Vol. 72, No. 162 / August 22, 2007 /Rules and Regulations, p. 47136
3. Federal Register Vol. 72, No. 162 / Aug. 22, 2007 /Rules and Regulations, p. 47200
4. Federal Register Vol. 72, No. 162 / Aug. 22, 2007 /Rules and Regulations, p. 47138
5. Federal Register Vol. 72, No. 162 / Aug. 22, 2007 /Rules and Regulations, p. 47138
6. Mandatory Insurer Reporting Requirements of Section111 of the Medicare, Medicaid and SCHIP Act of2007 (MMSEA) (Pub. L. 110-173); Section 111 of theMedicare, Medicaid and SCHIP Extension Act of 2007(Pub. L. 110-173) amends the Medicare SecondaryPayer (MSP) provisions of the Social Security Act (42U.S.C. 1395y(b)) to provide for mandatory reportingby group health plan arrangements and by liabilityinsurance (including self-insurance), no fault insurance,and workers’ compensation laws and plans
7. As an example: Hospitals that fail to notify patients ofphysician ownership can permit CMS to terminate theprovider agreement or to deny a provider agreement toa hospital that does not have a procedure in place tonotify patients of physician ownership in the hospital.Financial penalties apply to those hospitals that elect notto report the required 27 quality measures in FY 2008.
8. CMS Press Release Thursday, July 31, 2008, “Medicareand Medicaid move aggressively to encourage greaterpatient safety in hospitals and reduce never events.”
9. “Enterprise Risk Management (ERM) is an ongoingbusiness decision-making process instituted and supported by the healthcare organization’s board ofdirectors, executive administration and medical staffleadership. Recognizing the synergistic effect of riskacross the continuum of care, the goal of ERM is toassist the organization realize its mission by reducinguncertainty and process variability, promoting patientsafety and maximizing the return on investment (ROI)by asset preservation, and the recognition of actionablerisk opportunities.” Carroll, R. December 2007.
10. The FY 2008 final rule as published in the FederalRegister on Aug. 22, 2007, is 1047 pages in length,however, just over 300 pages are narrative; the remainingpages are tables representing supporting data
11. Federal Register Vol. 72, No. 162 / Aug. 22, 2007,Rules and Regulations pp. 47345-47347
12. Federal Register Vol. 72, No. 162 / Aug. 22, 2007,Rules and Regulations, pp. 47345
13. American Hospital Association. Regulatory Advisory.Medicare Inpatient PPS: The Final Rule for Fiscal Year2009, Aug.18, 2009
14. Federal Register Vol. 72, No. 162 / Aug. 22, 2007,Rules and Regulations, p. 47385
15. Federal Register Vol. 72, No. 162 / Aug. 22, 2007,Rules and Regulations, p. 47385-47391
16. CMS estimates of Medicare cases and average charge forhospital stays in FY 2006. A case represents a patientdischarge identified from the MedPAR database thatmet the associated HAC diagnosis/procedure criteria (a secondary diagnosis on the HAC list and, whereappropriate, a procedure code described in conjunctionwith a specific HAC). The standardized charge is thetotal charge for a patient discharge record based on theCMS standardization file. The average standardizedcharge for the HAC is the average charge for all patientdischarge records that met the associated HAC criteria.
17. Guide to Patient Safety Indicators Version 3.1 March12, 2007, available at www.qualityindicators.ahrq.gov/psi_downloads.htm, pp. 32-33
18. Guide to Patient Safety Indicators Version 3.1 March12, 2007, available at www.qualityindicators.ahrq.gov/psi_downloads.htm, pp. 47-48
19. Guide to Patient Safety Indicators Version 3.1 March12, 2007, available at www.qualityindicators.ahrq.gov/psi_downloads.htm, pp. 55-56
20. CDC Guidelines available at http://www.cdc.gov/ncidod/dhqp/gl_catheter_assoc.html
21. The number of cases of pressure ulcers reflects CC/MCCassignments for codes 707.00 through 707.07 and 707.09,which were reported until Oct.1, 2008. New MCC codes707.23 and 707.24 were implemented on Oct.1, 2008.Prevention guidelines available at www.npuap.org/ positn1.html and www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.chapter.4409
22. CDC reports 248,678 central-line associated blood-stream infections per year. However CMS was unableto identify Medicare cost data as there is currently nounique existing ICD-9-CM code
23. CDC guidelines are available atwww.cdc.gov/ncidod/dhqp/gl_intravascular.html
24. Details at www.cdc.gov/ncidod/dhqp/gl_surgicalsite.html25. Final rule p. 47215, No dollar estimates given; number
is an aggregate number for all ICD-9 code for fracturesand other traumatic injuries in the categories listed
26. Medicare data were not available for FY 2007 becauseICD-9-CM codes were not effective until Oct. 1, 2008