importance of monitoring comorbidities in patients with ... psych grand... · importance of...
TRANSCRIPT

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
Importance of Monitoring Comorbidities in
Patients with Mental Illness
Ajay Chaudhuri, MBBS, MRCP (UK)
Clinical Professor, Department of Medicine
Program Director, Endocrinology Fellowship
UB|MD Internal Medicine – Endocrinology,
Diabetes & Metabolism
Director, Kaleida’s Diabetes & Endocrinology
Center of WNY, President WNY ADA

1. CDC. Available at: http://www.cdc.gov/diabetes/statistics/slides/maps_diabetes_trends.pdf. Accessed Nov 7, 2008.2. CDC. Available at: http://www.cdc.gov/media/pressrel/2007/r071128.htm. Accessed Nov 7, 2008.3. NDIC. Available at: http://diabetes.niddk.nih.gov/dm/pubs/statistics/DM_Statistics.pdf. Accessed Nov 7, 2008.
Percentage of US Adults With Diagnosed Diabetes1*
Multiple factors contribute to the increasing prevalence of diabetes
Aging population
Increasing obesity: 72 million Americans were obese in 2005-2006 (BMI 30)2
Growing population of people of non-Caucasian ethnicity
24 million Americans have diabetes3
6 million are undiagnosed3
90-95% of the diagnosed population have type 2 diabetes3
19972002 <4.5%
4.5-5.9%
6.0-7.4%
7.5-8.9%
9%
2007 1997 2002
<4.5 4.5-5.9% 6.0-7.4% 7.5-8.9% 9%
2007
*Age adjusted. BMI=body mass index.

The Diabetes Epidemic: Global Projections, 2010–2030
IDF. Diabetes Atlas 5th Ed. 2011


Disease Burden of Type 2 Diabetes
• Macrovascular disease
– 2- to 4-fold more likely to have heart disease or stroke
– 2- to 8-fold more likely to have heart failure
– Accounts for 60% to 70% of all diabetes-related deaths
– Lower extremity amputations
• Microvascular disease
– Up to 24,000 new cases of blindness annually
– Leading cause of end-stage renal disease
– Neuropathy (including erectile dysfunction)
Centers for Disease Control and Prevention. National Diabetes Fact Sheet. 1998.
American Heart Association. 2001 Heart and Stroke Statistical Update.
National Heart, Lung, and Blood Institute. Facts about heart failure. 1997, online edition.

Impact of Mental Illness and Diabetes on Life Expectancy, Morbidity, and Mortality
Diabetes was the 7th leading cause of death in the US in 20061
The risk of premature death among people with diabetes is ~2x greater than for thosewithout diabetes of a similar age1,2
The Framingham Heart Study indicated diabetes decreases life expectancy by ~8 years2
Average potential years of life lost due to mental illness range from 13 to 30 years3
A major contributor to premature deaths is cardiovascular disease3
Individuals with severe mental illness have ~1.5 to 2x more diabetes and obesity than the general population4-7
1. NDIC. Available at: http://diabetes.niddk.nih.gov/dm/pubs/statistics/DM_Statistics.pdf. Accessed Nov 7, 2008.
2. Franco O, et al. Arch Intern Med. 2007;167(11):1145-1151.3. Colton C, Manderscheid R. Prev Chronic Dis. 2006;3(2):A42.
MENTAL ILLNESSDIABETES
4. Dixon L, et al. Schizophr Bull. 2000;26(4):903-912.5. Mukherjee S, et al. Compr Psychiatry. 1996;37(1):68-73.6. Fagiolini A, et al. Bipolar Dis. 2005;7:424-430.7. ADA. Diabetes Care. 2004;27(2):596-601.

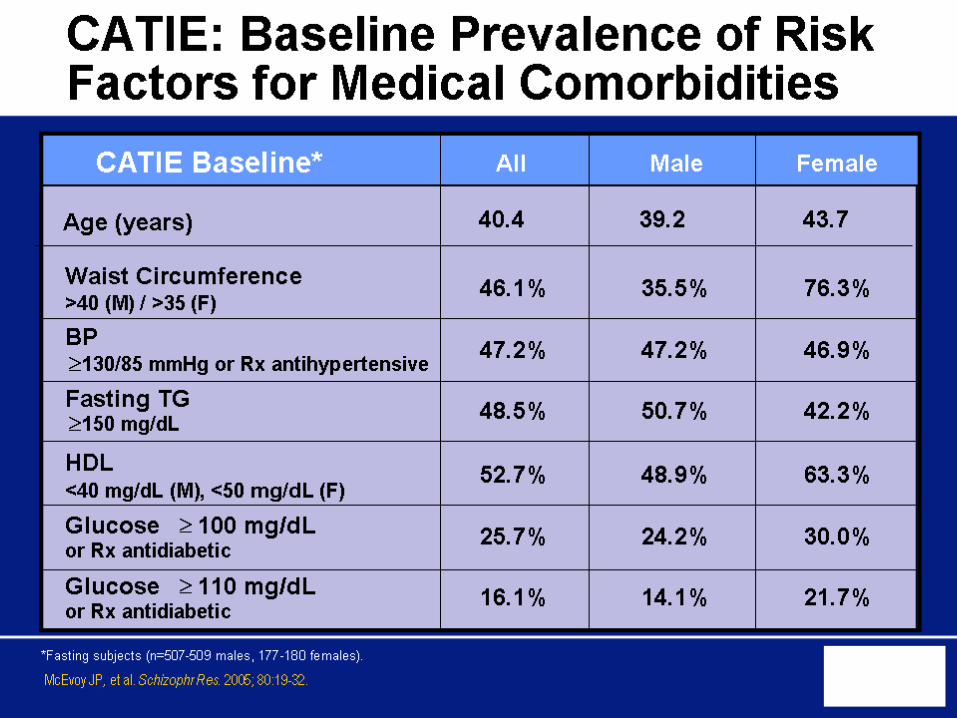
CATIE: Baseline Prevalence of Risk Factors for Medical Comorbidities

Mortality and Medical Comorbidity Among Patients With Serious Mental Illness
Miller B, et al. Psychiatr Serv. 2006;57(10):1482-1488.
Comorbidities Among Patients for
Whom Underlying Cause of Death
Was Heart Disease (n=126)*
Causes of Death Among Patients
Admitted to Mental Health Hospital
Between 1998 and 2002 (n=608)
Unclassified (5%) Cancer (7%)
Suicide (18%)
Pneumonia/Influenza (3%)
Chronic Lower Respiratory Disease (5%)
Accidents (14%)
Diabetes (3%)
Homicide (2%)
Cerebrovascular Disease (2%)
Other Causes (20%)
100
30
20
10
0
Heart Disease
(21%)
Hypertension Obesity Diabetes COPD Dyslipidemia
37%34%
19%
10% 9%
% o
f P
ati
en
ts W
ith
Co
mo
rbid
ity
*With Axis III diagnosis.
COPD=chronic obstructive pulmonary disease.

PREDIABETES1 METABOLIC SYNDROME2,3
(Defined as having 3 traits)
IFG: ↑ FBG
100-125 mg/dL
IGT: ↑ 2-hr OGTT
140-199 mg/dL
↑ FBG
100 mg/dL
↓ HDL
<40 mg/dL (M),
<50 mg/dL (F)
↑ Triglycerides
150 mg/dL
↑ Waist circumference
>40 inches (M)
>35 inches (F)
↑ BP
130/≥85 mm Hg
Prediabetes, Metabolic Syndrome, and Cardiometabolic Risk
1. ADA. Diabetes Care. 2008;31(suppl 1):S12-S54.2. Adult Treatment Panel. JAMA. 2001;285(19):2486-2497.3. Grundy SM, et al. Circulation. 2005;112:2735-2752.
Poor Diet
↑ Triglycerides
Overweight/
Obesity
Sedentary
Lifestyle
HypertensionInflammation/
Hypercoagulation
Age, Race,
Gender
Smoking
Family
History
↓ HDL
↑ LDL
↑ FBG
Insulin
Resistance
CARDIOMETABOLIC RISK4
The overall risk of developing type 2 diabetes and cardiovascular diseases
due to a cluster of risk factors
IFG=impaired fasting glucose. FBG=fasting blood glucose. IGT=impaired glucose tolerance. OGTT=oral glucose tolerance test. BP=blood pressure. HDL=high density lipoprotein. LDL=low density lipoprotein.
4. ADA. Available at: http://www.diabetes.org/for-health-professionals-and-scientists/cardiometabolic-risk.jsp. Accessed Nov 10, 2008.


Baseline 4 Weeks 8 Weeks 12 Weeks AnnuallyEvery 5
Years
Personal family history X X
Weight (BMI) X X X X
Waist circumference X X
BP X X X
Fasting plasma glucose X X X
Fasting lipid profile X X X
American Diabetes Association (ADA) Screening Guidelines for Patients on SGAs
ADA. Diabetes Care. 2004;27(2):596-601.
More frequent assessments may be warranted based on patient results and the monitoring recommendations in the package inserts for individual antipsychotic drugs used.
CASE SCENARIO #2
Unresponsive to current antipsychotic
medication for severe mental illness
IFG (Prediabetes)
Smoker (2 packs/day)
Recent weight gain
How does IFG impact your treatment decisions?
Is this patient at significant risk for developing diabetes?
How can the psychiatrist most appropriately manage this patient from this point forward?
CASE SCENARIO #3
Unresponsive to current antipsychotic
medication for severe mental illness
Suicidal ideation
History of cardiovascular disease and type 2 diabetes
Sedentary lifestyle
What are your treatment priorities?
How can the psychiatrist collaborate with other healthcare professionals to most appropriately monitor this patient?
What Is the Appropriate Course of Action?
CASE SCENARIO #1
Severe mental illness is well controlled
Good overall health
No significant cardiometabolic risk factors
Family history of diabetes
What type of monitoring (if any) is necessary for this patient?

Baseline 4 Weeks 8 Weeks 12 Weeks AnnuallyEvery 5
Years
Personal family history X X
Weight (BMI) X X X X
Waist circumference X X
BP X X X
Fasting plasma glucose X X X
Fasting lipid profile X X X
American Diabetes Association (ADA) Screening Guidelines for Patients on SGAs
ADA. Diabetes Care. 2004;27(2):596-601.
More frequent assessments may be warranted based on patient results and the monitoring recommendations in the package inserts for individual antipsychotic drugs used.

Criteria for the Diagnosis of Diabetes
A1C ≥6.5%
OR
Fasting plasma glucose (FPG)≥126 mg/dL (7.0 mmol/L)
OR
2-h plasma glucose ≥200 mg/dL(11.1 mmol/L) during an OGTT
OR
A random plasma glucose ≥200 mg/dL (11.1 mmol/L)
ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 2.

Screening For Diabetes
Testing at least every 3 yrs starting at age 45
American Diabetes Association. Diabetes Care. 2014:37, S14-80
Test Prediabetes Diabetes
FPG 100-125 mg/dL ≥126 mg/dL
OGTT 140-199 mg/dL ≥200 mg/dL
A1C 5.7-6.4% ≥6.5%

Younger/More Frequent Testing
If patient is overweight or obese and has 1 or more of the following risk factors (or 2 if not overweight):
1st degree relative with diabetes
Physically inactive
Certain race/ethnicity
Elevated blood glucose
Hypertension
Low HDL cholesterol and/or high triglyceride level
History of GDM
Delivering baby weighing >9 lbs
Polycystic ovary syndrome (PCOS)
American Diabetes Association. Diabetes Care. 2014:37, S14-80

Natural History of Type 2 Diabetes
Adapted from: Simonson GD, Kendall DM. Coron Artery Dis. 2005;16(8):465-472.
Years
Glu
co
se
(m
g/d
L)
Re
lati
ve
Fu
nc
tio
n (
%)
-10 -5 0 5 10 15 20 25 30
50
100
150
200
250
300
350
Clinical Diagnosis
Insulin Resistance
-Cell Function
Postmeal Glucose
Fasting Glucose
Prediabetes (IFG, IGT)
0
50
100
150
200
250
Onset of
Diabetes

Slide Source:
Lipids Online Slide Librarywww.lipidsonline.org
Reprinted with permission from DeFronzo R et al. Diabetes. 2009;58:773-795. Copyright © 2009 American Diabetes Association. All rights reserved.
Ominous Octet
IncreasedHGP
Hyperglycemia
ETIOLOGY OF T2DM
DEFN75-3/99 Decreased GlucoseUptake
Impaired InsulinSecretion Increased Lipolysis
Decreased
Incretin Effect
Decreased InsulinSecretion
IncreasedHepatic Glucose
Production
Islet– cell
IncreasedGlucagonSecretion
Decreased Glucose
Uptake
Increased Lipolysis
Increased
Glucose
Reabsorption
HYPERGLYCEMIA
NeurotransmitterDysfunction

Insulin Resistance in Treatment-Naïve Patients With Schizophrenia
Ryan MCM, et al. Am J Psychiatry. 2003;160(2):284-289.
Ins
uli
n (
U/m
L)
Co
rtis
ol (n
mo
l/m
L)
Ins
uli
n R
es
ista
nc
e(H
OM
A)
P<0.01
P<0.05
P<0.005
P<0.03
Glu
co
se (
mg
/dL
)
HOMA=homeostasis model assessment.

Schizophrenia AND Diabetes

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
Genetic predisposition


≤3.5
≥46.0
Hu FB, et al. Arch Intern Med. 2001;161(12):1542-1548.
Sedentary Lifestyle Increases the Risk for Development of Diabetes
Quartiles of Hours/Week
Spent Watching TV
Quartiles of MET-
Hours/Week
Spent on Physical
Activity
Re
lati
ve
Ris
k
>15.0 8.1-15.0 3.6-8.0
23.6-45.9
10.0-23.5
<10.0
MET-hours=metabolic equivalent hours.

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
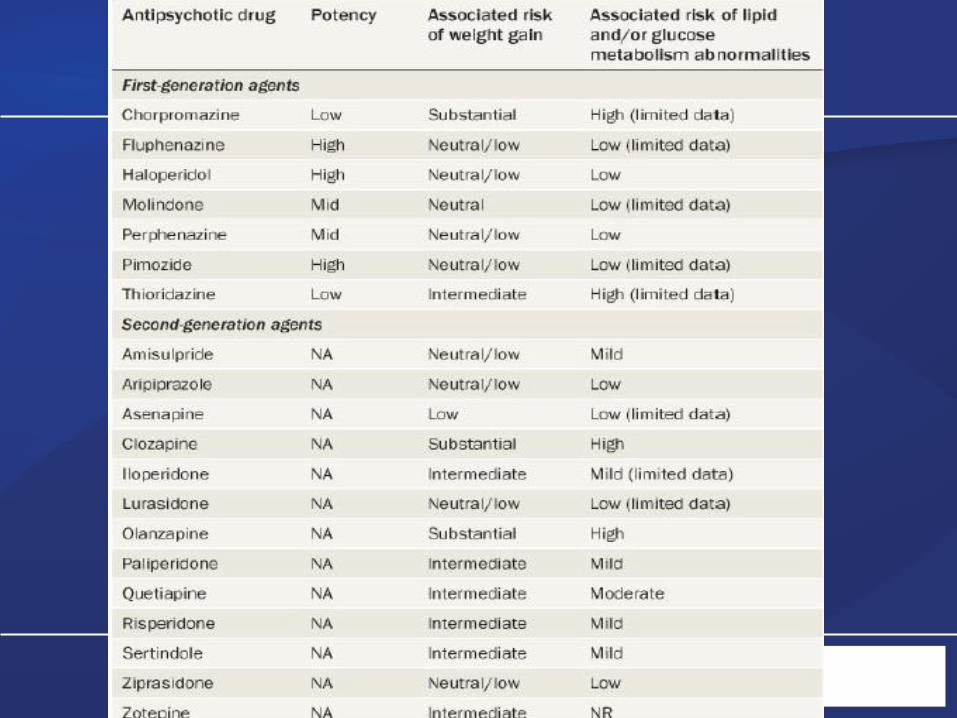
Effect of Antipsychotic drugs




CASE SCENARIO #2
Unresponsive to current antipsychotic
medication for severe mental illness
IFG (110 mg/dL, prediabetes)
Smoker (2 packs/day)
Recent weight gain
How does IFG impact your treatment decisions?
Is this patient at significant risk for developing diabetes?
How can the psychiatrist most appropriately manage this patient from this point forward?
CASE SCENARIO #3
Unresponsive to current antipsychotic
medication for severe mental illness
Suicidal ideation
History of cardiovascular disease and type 2 diabetes
Sedentary lifestyle
What are your treatment priorities?
How can the psychiatrist collaborate with other healthcare professionals to most appropriately monitor this patient?
What Is the Appropriate Course of Action?
CASE SCENARIO #1
Severe mental illness is well controlled
Good overall health
No significant cardiometabolic risk factors
Family history of diabetes
What type of monitoring (if any) is necessary for this patient?

Prediabetes
Prediabetes is an important risk factor for future diabetes and cardiovascular disease
Studies have shown that lifestyle modification can reduce the rate of progression from prediabetes to diabetes
American Diabetes Association. Diabetes Care. 2014:37, S14-80

Cu
mu
lati
ve
In
cid
en
ce
of
Dia
bete
s (
%)
Years
40
30
20
10
0
0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
Placebo
Metformin
Lifestyle
Knowler WC, et al. NEJM. 2002;346:393-403
Diabetes Prevention Program
Older Adults(Cases/100 person-yrs)
Placebo 10.8
Metformin 9.6
Lifestyle 3.1

A1C ≥ 6.0%IFG and IGT
+ Other Features
Lifestyle intervention and/or metformin, follow-up @6 mo
Intervention and Follow-Up
Screen for Diabetes:A1C - or -FPG – or -
2-hour, 75-g OGTT
Normal
Re-evaluate in 3 years if risk
factors remain
METFORMIN IS NOT FDA APPROVED FOR PREVENTION
American Diabetes Association. Diabetes Care. 2014:37, S14-80
Lifestyle intervention,
follow-up @1 year
A1C ≥ 5.7%IFG or IGT
DIABETES
Lifestyle intervention plus metformin,follow-up @3 mo

Patients With Severe Mental Illness Can Benefit From Lifestyle Modifications
Behavioral strategies
Self-monitoring of eating
Physical activity
Stress management
Nutrition principles
Meal planning
Label reading
Portion size
Healthy snacking
Exercise
Light to moderate for 20 minutes, 3-5 times/week
Menza M, et al. J Clin Psychiatry. 2004;65(4):471-477.
Weight Loss After a Year-Long Participation in “Healthy Living” Program
Month
*P=0.005 vs usual care
BM
I
Intervention (n=31) Usual care (n=23)
*

Patients With Severe Mental Illness Who Were Enrolled in a Solutions for Wellness Personalized Program Lost Weight
Based on changes in weight as reported on returned follow-up surveys
Individual results may vary
Hoffmann VP, et al. J Clin Psychiatry. 2005;66(12):1576-1579.Hoffmann VP, et al. Presented at: APA; May 1-6, 2004: New York, NY.
Imp
rove
me
nt
(n=2666) (n=1916) (n=1599) (n=1252) (n=872)
Me
an
Ch
an
ge
in
BM
I
Follow-Up 2:
Week 7
Follow-Up 3:
Week 11
Follow-Up 4:
Week 15
Follow-Up 5:
Week 19
Follow-Up 6:
Week 22

CASE SCENARIO #3
Unresponsive to current antipsychotic
medication for severe mental illness
Suicidal ideation
History of cardiovascular disease and type 2 diabetes
Sedentary lifestyle
What are your treatment priorities?
How can the psychiatrist collaborate with other healthcare professionals to most appropriately monitor this patient?
What Is the Appropriate Course of Action?
CASE SCENARIO #1
Severe mental illness is well controlled
Good overall health
No significant cardiometabolic risk factors
Family history of diabetes
What type of monitoring (if any) is necessary for this patient?
CASE SCENARIO #2
Unresponsive to current antipsychotic
medication for severe mental illness
IFG (110 mg/dL, prediabetes)
Smoker (2 packs/day)
Recent weight gain
How does IFG impact your treatment decisions?
Is this patient at significant risk for developing diabetes?
How can the psychiatrist appropriately manage this patient from this point forward?

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
Management of diabetes

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
1993-1997 2005-2010

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
SUMMARY OF THE LANDMARK
CLINICAL TRIALS
• Intensive glycemic control reduces
microvascular complications
• Intensive glycemic control reduces
macrovascular complications
• shorter duration of diabetes
• without established CVD
• In long term follow up studies

0
10
20
30
40
50
60
COMPOSITE ENDPOINT OF DEATH FROM CV CAUSES, NONFATAL MI, CABG, PCI, NONFATAL STROKE, AMPUTATION, OR SURGERY FOR PAD: STENO-2
Prim
ary
Com
posite
Endpoin
t (%
)
Months of Follow-up
0 24 48 60 9636 847212
Conventional Therapy
Intensive Therapy
P=0.007
Hazard ratio = 0.47 (95% CI, 0.24–0.73; P=0.008)
Gæde P et al. N Engl J Med 2003;348:383-393. Copyright 2003 Massachusetts Medical Society. All rights reserved.
53%

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
ABC OF DIABETES CARE
A A1C
B Blood pressure
C Cholesterol
SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE

Slide Source:
Lipids Online Slide Librarywww.lipidsonline.org
Reprinted with permission from DeFronzo R et al. Diabetes. 2009;58:773-795. Copyright © 2009 American Diabetes Association. All rights reserved.
Ominous Octet
IncreasedHGP
Hyperglycemia
ETIOLOGY OF T2DM
DEFN75-3/99 Decreased GlucoseUptake
Impaired InsulinSecretion Increased Lipolysis
Decreased
Incretin Effect
Decreased InsulinSecretion
IncreasedHepatic Glucose
Production
Islet– cell
IncreasedGlucagonSecretion
Decreased Glucose
Uptake
Increased Lipolysis
Increased
Glucose
Reabsorption
HYPERGLYCEMIA
NeurotransmitterDysfunction
SGLT2
inhibitor
Incretins
BromSR


SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
ANTIDIABETES THERAPY: TREATMENT
EFFECTS1,2
Class
Expected Decrease in A1C
(%)
Biguanides 1 – 2
Sulfonylureas 1 – 2
Glinides 0.5 – 1.5
Alpha glucosidase inhibitors
0.5 – 0.8
Thiazolidinediones
0.5 – 1.4
DPP-IV inhibitors 0.5 – 0.8
GLP-1 receptor agonists
0.5 – 1.5
Insulin 1.5 – 3.51. Nathan DM et al. Diabetes Care. 2009;32(1):193-203.
2. American Association of Clinical Endocrinologists. Endocrine Practice. 2007;13:3-68.
SGLT2 inhibitor 0.6 to 1.1%

Copyright © 2015 AACE. May not be reprinted in any form without express written permission from AACE.

SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCESDEPARTMENT OF MEDICINE
• Individualize glycemic goals based on patient
characteristics and avoid hypoglycemia
• Promptly intensify antihyperglycemic therapy to maintain
blood glucose at individual targets
• Combination therapy necessary for most patients
• Base choice of agent(s) on individual patient medical history, behaviors and risk factors, ethno-cultural
background, and environment
• Insulin eventually necessary for many patients
• SMBG vital for day-to-day management of blood sugar
• All patients using insulin
• Many patients not using insulin
Common Principles in AACE/ACE and
ADA/EASD T2DM Treatment Algorithms