improving access to emergency healthcare in sub
TRANSCRIPT

IMPROVING ACCESS TO EMERGENCY HEALTHCARE IN SUB SAHARAN AFRICA
RA Dennis 1 and K R Pullen2
Abstract
Lack of affordable transport is a major constraint on access to emergency healthcare in rural areas of Sub Saharan Africa and one of the main barriers to achieving Milennium Development Goals 4 and 5 in these countries. Conventional ambulances are expensive to acquire and operate and this paper argues that there is a strong case for introducing lower-cost versions. The paper describes the successful trials of a motorcycle-ambulance trailer (MAT) in Zambia and discusses the implications of the findings in regard to setting up an emergency transport service based on low-cost ambulances. Keywords: Emergency transport service; rural Africa; motorcycle ambulance-trailer; performance data; operating costs; sustainability 1 Introduction
Two key goals in improving health care in developing countries are reducing maternal and new-borne mortality rates (MDGs 5 and 4 respectively). A number of publications over the past few years have reviewed methods for achieving this and progress made (for example References 1 to 6). The general conclusion is that good progress has been made in some regions but it is still very slow in sub-Saharan Africa where much more needs to be done. There is also general agreement that the priority aim to achieve these goals is to increase the number of births which take place with a skilled birth attendant (SBA) present. In general this requires attendance at a clinic with basic EMOC (Emergency Obstetric Care) facilities. The literature identifies three main barriers to this, based on the ‘three delays model’ (Thadeus & Main, 1994), as summarised in Table 1. Table 1: Barriers to attendance at healthcare facility
Barrier Factors 1 Decision of prospective mothers to attend
Husband and family influences; family commitments and time away from family; traditional beliefs; getting to the clinic; perceived effectiveness of treatment; having a carer to travel with them
2 Access to clinic Distance; accessibility of roads and tracks; availability of suitable and affordable transport
3 Effectiveness of treatment Trained staff ; necessary equipment and medicines; attitudes of staff; cost of treatment
The availability of appropriate and affordable tranport is therefore an essential component in efforts to reduce maternity and new-borne mortality not only in improving access to health facilities but also in encouraging prospective mothers to attend by making travel more convenient, timely and comfortable. It is likely that this would also be of general benefit to rural communities in improving access to health facilities for all emergency illnesses and accidents. Conventional ambulances such as the Toyota Landcruiser are costly to purchase and operate. There is a great need for more affordable emergency transport services (ETS) and there have been a number of innovations to provide low-cost options. These include bicycle ambulances ( Forster et al, 2009), the e-Ranger motorcycle-sidecar ambulance ( Hofman et al, 2008) and contracts with transport service operators ( Mwebaze et al, 2013 and Silva, 2011). All have provided a useful service but little information is available yet on their long-term sustainability. 1 Co-ordinator Developing Technologies, City University London (email: [email protected]) 2 Professor of Energy Systems, City University London

Options for low-cost ambulances have been discussed by Krasovec (Krasovec, 2004) who suggests that they need to provide the following features:
• A significant reduction in travel time to healthcare • Satisfy cultural concerns about privacy • Provide capacity to carry a carer or guardian to accompany the patient
He suggests that some form of motorised transport is most likely to be acceptable and effective. He also suggests that since most obstetric emergencies occur in the home the priority role of ambulances should be to collect patients from the home to the first level of healthcare. Motorcycles are the fastest growing form of motorised transport in Sub Saharan Africa and have played a signicant role in improving rural mobility in some countries through ‘boda-boda’ services in which one or two passengers are carried on the pillion seat. However, there are concerns for comfort and safety for less physically able passengers such as pregnant woment, the seriously ill or disabled and the elderly (Amleset Tewodros, 2014). It is therefore considered there is a considerable potential for motorcycle-based vehicles that improve comfort, carrying capacity and safety. This paper describes the development and trials of a motorcycle ambulance-trailer (MAT) that meets these criteria. 2 Design and development of a MAT The following specifications were considered for a low-cost ambulance:
• To carry a patient on a stretcher in a reclined or semi-reclined position and also a carer to look after the patient
• To be able to transport the patient to a health facility within 2 hours • To provide a comfortable and convenient ride on typical rural earth roads
The need to carry a carer prompted the choice of a trailer-ambulance rather than the more widely used sidecar. Although there has been little use of trailers with motorcycles, they are quite widely used in a few countries such as Cambodia and Vietnam for carrying people and goods and this provided the backing for their choice as an ambulance. Initial testing to investigate the effects of the trailer on control of the motorcycle indicated that the best position for the hitch was directly above the rear axle and that braking of the trailer was desirable. A prototype, see Figure 1, was then trialled in a project in Mtwara, Tanzania, transporting emergency patients from a rural clinic to Mtwara hospital, a distance of 48km (IT Transport, 2001). The prototype was also used as a general transport service to subsidise the ambulance service, carrying up to 6 people and their goods. It completed over 10,000km over a period of 9 months without any safety problems. Figure 1: Prototype MAT in Mtwara, Tanzania The performance of the MAT concept having showed considerable promise, an improved version was developed by Developing Technologies, see Figure 2, and two prototypes have been extensively tested in Lundazi District, Eastern Province, Zambia, within the Africa Community Access Programme (www.afcap.org). The two prototypes were locally manufactured in Lusaka by the Disacare Wheelchair Centre. The main features of this prototype are:
• Wheels from a small car with leaf-spring suspension • Removeable lightweight stretcher • Seating for up to two carers • Automatic braking through a pivoting hitch pin • Ball and socket hitch directly above rear axle.
Figure 2: Improved MAT tested in Zambia

One MAT was towed by a Honda XR125 and the other a Yamaha AG200 to assess the effect of motorcycle power and weight on towing performance. The Honda in fact proved very adequate in towing the MAT . Ideally an “agricultural” type motorcycle with low speed and high traction torque is needed with a capacity of 125 to 200cc. 3 Trials of MAT in Zambia 3.1 Organisation of the trials Following discussions with a number of health authorities it was decided to locate the trials in Lundazi District where there was a particular need to improve access to health facilities to complement other mother-care programmes. The District Health Authority was keen to collaborate and located the MAT at two clinics, Mwase-Lundazi and Kanyanga (see map in Figure 3). These are first level centres for maternity patients with basic obstetric care serving their own catchment areas plus a number of Health Centres and referring more serious emergencies to the district hospital. Details are shown in Table 2. Figure 3: Map of Lundazi District Table 2: Details of clinics where MAT were located Clinic Catchment
population Health Centres served
Population served by HCs
Distance to district hospital, km
Mwase-Lundazi 19,124 5 (1) 26,994 31 Kanyanga 13,946 7 59,096 35 Note 1: these HCs in fact generally referred emergency patients directly to the district hospital as facilities at the clinic were little better than at the HCs. Mwase-Lundazi clinic was already served by 3 Landcruiser ambulances, 2 old and 1 new, and Kanyanga clinic by 2 Landcruisers, both old. These were used primarily for transferring referred patients to the district hospital. The old ambulances were unreliable and often out of service. The MATs were placed with the clinics who decided how they could be most effectively used to benefit their health services. In Mwase-Lundazi it was decided that it would be used primarily to collect emergency patients from villages in their catchment area, whilst in Kanyanga it was decided that their MAT would be used to collect emergency patients from both villages and also HCs. Both clinics served villages over an average radius of around 8km and up to a maximum distance of around 20km. The distance of HCs from Kanyanga clinic ranged from 10 to 20km. The MAT operators were selected by the clinics from their staff, two at each clinic to provide a 24 hour service. The operators had other duties but operating the MAT was their first priority and they were required to be able to answer a call within 20 minutes. They were given a one week training course in good riding habits, preventative maintenance and handling of the MAT by Riders for Health, Zambia, an NGO specialising in rider training, and provided with protective clothing. Riders for Health was also contracted to provide technical support to the trials, organising fuel supply and providing maintenance and repair as required. This worked very effectively with minimal downtime of the MATs allowing the maximum output from the trials. 3.2 Results from trials Table 3 shows a summary of emergency trips made by the MATs over 16 months of the funded trials. Since the end of the project in December 2013 they have continued to be operated by the clinics with government funding at an average level of 25 trips per month at Mwase-Lundazi and about half this at Kanyanga. All trips were classified as ‘emergency’ but unfortunately further details were not collected, and all patients were accompanied by at least one carer. The most heavily used MAT, that at Mwase-Lundazi, collected patients from over 50 villages.

Table 3: Summary of MAT trips
3.3 Assessment of MAT performance The trials were accompanied by an extensive monitoring programme which included - a logbook of trips for each MAT; monitoring of other ambulance services in the district, namely bicycle ambulances and Landcruisers; data on attendances and referrals at the clinics and a selection of HCs; and collection of feedback from key informants and MAT users on the impact of the MATs. The findings are summarised in the following sections. 3.3.1 Control, safety The operators reported that it took a few trips to get used to the handling of the motorcycle with the MAT attached but once they had this experience they were comfortable with the towing of the MAT. The main issue was the extra strain on the arms which limited comfortable continuous operation to about one hour. The main risks tend to be for the rider which encourages responsible operation and no safety issues were reported in over 15,000km of operation. 3.3.2 Accessibility Lundazi district is fairly flat with few significant hills. The rural roads are earth and gravel of varying quality. The trials were run over both dry and wet seasons with no significant difference in the number of trips per month. The main problem found with accessibility of the MAT was skidding due to lack of grip on very wet and also sandy roads. This limited access on a few roads particularly in the wet season but where this occurred the operator made arrangements for the patient to be collected from the nearest accessible location so no cases were reported where patients could not be collected. 3.3.3 Timeliness of service Figure 4 shows the relationship between the distance to the village and the time from receiving a request call for the MAT to reach the patient and also to deliver the patient at the clinic. This shows that the MATs generally met the target of getting the patient to medical care within 2 hours up to distances of 20km from the clinics. The average trip velocity is around 25km/hr. Figure 4: Timeliness of MAT service 3.3.4 Impact on access to healthcare Figure 5 shows records of attendance at clinics and a selection of HCs in Lundazi district over a 9 month period. At both clinics monthly attendance for non-maternity cases is many times higher than MAT trips and transport would be primarily by walking, bicycle or ox-cart. It is clear that in this area the main impact of the MAT would be in getting critical emergency cases that are too sick to travel by the above means to healthcare in time for effective treatment and therefore in saving lives. However, at Mwase-Lundazi clinic MAT trips are a significant proportion, around 40%, of maternity attendance and might therefore be expected to show some impact of the MAT on attendance. Figure 6, which shows births at the clinic, does in fact show a trend for increased births at the clinic since the introduction of the MAT compared to other health facilities, clearly indicating an impact on increasing access to the clinic. It seems likely that the MATs have not only reduced the physical barrier to attending the clinics by providing convenient transport, but also the psychological barriers by making the trip easier and less of a burden. Figure 5: Average monthly attendance at clinics and HCs
Total trips
Total km
% Trips for various medical conditions
Maternity Malaria Other Accident
383 15,500 65.7 18.5 15.0 0.8

Figure 6: Impact of MAT on monthly births at Mwase-Lundazi clinic Some indication of people’s views on travel to the clinic is provided in Figure 7 which shows two sets of data from interviews with MAT users: • Lines 1,2,3 show replies to a question would they have travelled to the clinic if the MAT was not available
and the mode of transport they would have used • Lines 4,5,6 show the mode of transport used for the return journey from the clinic to their home when they
had to find their own transport This data is for maternity cases and suggests that women are prepared to walk up to around 8km but above this will consider using a vehicle or not travelling to the clinic. The vehicle cost was reported as around $3 for a bus and up to $5 for a taxi or oxcart. Figure 7: Modes of travel to the clinic without the availability of the MAT 3.3.5 Feed-back from medical staff and MAT users The introduction of the MATs has been welcomed by both medical staff and users as indicated in the feed-back in boxes 1 to 4 below. BOX 1: Clinic in-‐charge– Mwase-‐Lundazi ‘The coming of the MAT to the selected clinics has cheered many especially the medical staff. This is because of transport challenges the health care system has for a long time been facing. We have not experienced any problems with it except for the stretcher which was not very tight and caused some discomfort to patients. That had been sorted out .We thought of inserting a mattress which was more comfortable. The other thing is some of our roads are narrow and during the rainy season they become impassable by the MAT. At night, we are particularly concerned with the security of the operator and theft of bike when going to collect the patients. We thought it were possible to hiring a security personnel to ensure the security of both the MAT and the operator.’ ‘When going to collect a maternal case, it is advisable to be accompanied by a qualified staff just in case of abnormality.’ BOX 2: Sister-‐in-‐charge, Kanyanga clinic ‘It was on when we received a call from Chasefu that there was an anaemic emergency. The MAT without wasting time was on its way. The condition of the patient was critical as the blood level was only 3grams. Quickly the MAT started off for Lundazi and met the ambulance on the way which carried the patient to the hospital. Had it not been for the MAT, life would have been lost’, BOX 3: Maternity patient I live at Chilola village (6km from clinic) in Mwase chiefdom. I want to share with you how the MAT rescued my life. My labour pains started during the day but for unknown reasons, I was delayed to be taken to the clinic. At about mid-night my condition grew worse. My husband looked for transport but could not find it. I could not sit on the bicycle. When the condition grew from bad to worse, one of my in-law went to the nearby village to get the contact number for the MAT operator. The next thing I saw was that I was in the labour room where I was assisted to deliver by trained medical personnel.’ BOX 4: Malaria patient I was unconscious was taken to clinic. It was the following day when I was told what had happened. This service has saved my life. At the time I was referred, my wife was already in tears. Today here I am testifying the critical role the MAT is playing. I wish to urge the service providers to continue delivering this saving life service’.

A total of 24 users were interviewed. All commented that the service was simple to request (see below), arrived quickly and that the trip was comfortable. Many also commented that a major advantage was that the service was free. The Government of Zambia has decreed that all medical care should be free and therefore it was not considered possible to test out how the imposition of a user fee would affect usage. This is a crucial issue for long-term sustainability since government health services will generally have limited funds, particularly for ETS, and therefore some level of support may be needed. In Lundazi the clinics are continuing to operate the MATs supplying fuel and operators. However, it is not clear if support extends to maintenance and repairs if the MATs break down and it is often these factors which are the main barriers to introducing innovations on a sustainable basis. 3.4 Communication Efficient communication is an essential component of an effective emergency transport system when the ambulance is centrally located. Although radios are still in use, communication is increasingly by mobile phones as ownership increases rapidly in Sub Saharan Africa. A survey in 2010 (Montez, 2010) estimated that subscribers to mobile phone services in Zambia increased from around 400,000 to over 4 million in the period 2004 to 2009, and in 2009 was 34.1% of the population. This was about average for African countries, being rated at 18th out of 36 countries. Although ownership was initially concentrated in urban areas it has increased rapidly in rural areas over the past few years. It was therefore decided this would be an effective and relatively low-cost means of communication. Different systems were investigated at the two clinics: 1 At one, calls were directed to the MAT operator who then informed clinic duty staff. This is the most
direct with less risk of miscommunication and delays but requires the operator to have sufficient medical knowledge to make judgements on whether an ambulance is required.
2 At the other, calls were directed to the clinic staff who then passed on the request to the operator. This is less direct but possibly allows better judgement on the need for an ambulance.
Both systems in fact seemed to work effectively with no reports of delays or misuse of the service. As part of a sensitisation activity to introduce the MATs, health workers located in the villages were provided with the phone numbers to call for the MAT service and it seems that these numbers quickly became fairly well known by phone owners. It was estimated that ownership was about 30 to 50 % of families with overall access up to 75% through neighbours or health workers. Montez (ibid) indicates that the situation would be similar in many other locations in Sub Saharan Africa suggesting that mobile phones will generally provide an effective means of communication for ETS. 4 Discussion of findings in relation to design of ETS An ETS has to be designed to meet the local situation and conditions and the findings of this project may not match the situation in other locations. However, there are a number of common considerations for an ETS and this section discusses the findings of the project in relation to these. 4.1 Organisation of ETS As funding for ETS is likely to be limited it is important to make the most cost-effective use of existing resources and those that need to be introduced to improve local healthcare. If there are already suitable vehicles in the local communities it may be possible to incorporate these in an ETS (Mwebaze et al, 2013 and A.L. Silva, 2011). If new vehicles need to be introduced they need to used cost-effectively. Should they be used for transporting emergency patients from villages to the first level of healthcare, patients referred from first level to second level, or both? In Lundazi district the average total referrals was 1.3% of attendance and for maternity cases just under 2% and there were Landcruiser ambulances and also taxis that could largely cope with these transfers. It was therefore decided by the clinics that the most effective role of the MAT to improve healthcare was to collect emergency patients from the villages where the average distance to healthcare was around 8km, a severe problem for emergency patients without appropriate transport. However, the MATs were also used occasionally to transport referred patients when the Landcruisers were not available. In another project run by a partner in Malawi where the average distance to first level care was 3km, the level of referrals around 7% and the distance from clinic to referral hospital 11km with no ambulance, it was

decided the most effective role of a MAT was in transporting referred patients. It is therefore important to assess the local priority need. Where ETS are used for transport to first-level care they may be community or facility based. Community-based provides the most direct route to care but also limits usage and level of technical support. With their low cost and simple technology bicycle ambulances are appropriate for this role in suitable areas with relatively level, firm tracks but to be cost-effective more costly motorised amulances need to be facility –based where they can serve a larger population. 4.2 Options for low-cost ambulance service The characteristics of options that have been tried out as low-cost ambulances are presented in Table 4 and compared with a conventional Landcruiser ambulance. [3-wheeler (trikes) motorcycle ambulances are also available from China but no information has been found on the performance of these.] Table 4: Options for low-cost ambulances
Indicative costs from monitoring programmes for these options are shown in Table 5. This shows that around 10 MBA can be obtained at the same cost as a Landcruiser ambulance and running costs are only 1/3 to ½ of the conventional ambulance. Since they give good access, good comfort and a reasonable speed, in many cases they will provide a more cost-effective ETS, particularly from village to clinic.
Ambulance type
Average speed km/hr
Carrying capacity Characteristics
Landcruiser 60 At least 2 patients plus carers
Can operate on most road conditions and safer in mixed traffic. Width is a constraint for narrow tracks
Motorcycle-trailer
25 Patient + carer
Carer rides in trailer and has direct contact with patient
Needs experience to build operating confidence. Difficult to operate on very sandy and wet roads where motorcycles have problems. Flexible, motorcycle is easily unhitched for other use.
Can be locally manufactured with readily available materials and used with any motorcycle
Motorcycle-sidecar
25 Patient + carer
Carer rides on motorcycle pillion and has less contact with patient
More stable and easier to control than MAT but extra loading on motorcycle from sidecar may increase maintenance costs, particularly for wheels and suspension
They are an integral unit less suited to local manufacture so availability of spare parts may be a problem until numbers are large enough to support local stocking of parts
Bicycle ambulance
10 Patient only High human effort needed restricts it to relatively flat areas. Carer travelling with patient can be a problem. Less comfortable than other options

Table 5: Comparative costs of ambulances
Notes 1 Based on fuel price of $1.7/litre; 2 Costs from Zambia project 3 Cost from project in Malawi – eRanger is a sidecar ambulance produced in S Africa and there may be extra freight costs 4 This is the annual replacement cost based on 4% inflation and assuming –
(i) Landcruiser - 25,000km/yr and total life 300,000km (ii) MAT and eRanger – 10,000km/yr and total life 80,000km (iii) Bicycle ambulance – 500km/yr and total life 4000km 5 Other costs may include annual road tax and insurance (depending on Government requirements), operator costs and protective
clothing for riders 4.3 Funding and sustainability of ETS Although MBA are much cheaper to run than conventional ambulances, trip costs at around $0.40 per km, taking into account a two-way journey and not including operator costs, would still be unaffordable to a large proportion of rural families and user-pay schemes would likely exclude many poorer families. For instance, one of the major benefits mentioned by users of the MAT service was that it was free. A MBA service covering 10,000 km per year and serving a population of around 20,000 would require operational funding of about $2,000 per year ($3,000 if replacement cost is included) plus operator costs. Providing this funding is the major barrier to introducing motorised ETS on a sustainable basis. Some of the options include: Government funded – Krasovec (Krasovec, 2004) reports some examples of government funded ETS but with no details of long-term sustainability. Hofman (Hofman et al., 2008) reports on the introduction of three ‘eRanger’ ambulances by Government clinics in Malawi and mentions problems of downtime due to unavailability of fuel or an operator. The paper only covers the first 12 months or so of operation before the onset of any major repair costs and therefore the response to these is not known. In the authors’ project in Zambia the two clinics have continued to fund fuel and operator costs for the MATs over 6 months since the end of the project but no maintenance has been carried out and it is not known whether they will be able to cover repair costs when they occur. In government funded schemes it is often the response to repair and maintenance needs that are the main barriers to reliable and sustainable services due both to inadequate funding and the lack of effective procedures. Community supported ETS – these are usually based on bicycle ambulances which are cheap to run and can be maintained by the community. The feedback on these is mixed. In Lundazi district 8 bicycle trailers had been introduced together with grain grinders to generate income to support the ambulances. Although a good concept in theory the scheme relied too much on community health workers with too little support from the community for sustainability. It is clear from the successful introduction of bicycle ambulances within the MAMaZ programme in other districts of Zambia (Green et al, 2014) that full involvement and support of the community is essential to the success of community-based ETS. However, it is not considered that community-based schemes are suitable for motorised ETS because of the higher costs and skills needed.
Ambulance Type
Initial cost Running costs/km Depreciat’n/km (4)
Total operating cost/km
Fuel used km/l
Fuel cost/km
(1)
Repair and
maint’ce
Total
Landcruiser (2)
60,000 6.5 0.26 0.32 0.58 0.26 0.84
MAT with 125cc m/c (2)
5,500 28 0.06 0.12 0.18 0.08 0.26
eRanger (3) 6,000 + freight cost
17 0.10 0.17 0.27 0..08 0.35
Bicycle + ambulance (2)
700 0 0 0.016 0.016 0.16 0.18

Community-based insurance schemes – in the MAMaZ programme mentioned above, funding for operation of the bicycle ambulances was provided from community savings. The use of community insurance schemes to fund healthcare has been tried with varying success in a number of countries where free healthcare is not provided by government. A review of schemes in a number of SSA countries (Obeyemi, 2014) indicates that some success has been achieved but in general take-up has been low, particularly by the poorest who find flat-rate subscriptions difficult to pay. One of the most successful schemes is in Rwanda (Shimeles, 2010) where a take-up of 85% has been achieved with an annual subscription rate of $2 per person. Formal schemes are generally aimed at reducing the financial shock of emergency healthcare but informal, community run schemes may be set up to cover more general emergencies and seem to have had more success. For example an NGO run scheme in Samburu district in Kenya was set up specifically to fund transport for emergency referral trips to the district hospital (Macintyre and Hotchkiss, 1999). The annual subscription was around $0.5 per person and the take-up about 30% of the community. The authors indicate that a critical factor in achieving success of this type of scheme is building trust and collaboration between the communities and the service providers, with communities needing to be convinced they will obtain reliable benefits from the scheme. The above discussion suggests that community-based insurance schemes could be a viable approach to funding motorised ETS but will need to be accompanied by an effective maintenance and repair scheme to minimise downtime and provide reliable operation of the vehicles. For an MBA based on an annual operating cost of $3,000, including replacement cost, and serving a community of 20,000 the annual subscription assuming a 50% take-up would be $0.3 per person or $1.50 for an average size family which is considered acceptable. In some cases the scheme might only have to fund part of the service to support the district health authority. For instance, it might only have to support maintenance and repair costs in which case annual subscriptions could be reduced to $0.15 per person. It is suggested that this type of scheme might best be organised at village level, working closely with village chiefs and building on any existing emergency savings schemes. Conclusions The paper reports the successful trials of two motorcycle ambulance-trailers in Lundazi district, Zambia. It shows that motorcycle-based ambulances are a viable option for providing low-cost ETS in rural areas of Africa, providing good accessibility at an effective speed. In particular they improve access to health facilities for maternity cases and reduce psychological barriers to attendance, key factors in reducing maternal mortality rates. Although they are far more affordable than conventional ambulances, there will still be many cases where health authorities do not have sufficient resources to operate them on a sustainable basis. It is suggested that supplementary support might be obtained from community-based insurance schemes run at village level. A key factor in achieving sustainability is to establish an effective scheme for maintenance and repair of vehicles to ensure prolonged operation with minimum downtime. References 1 Forster, G. et al.(2009) Use of intermediate modes of transport for patient transport: a literature review
contrasted with the findings of the Transaid Bicycle Ambulance Project in Eastern Zambia. Transaid: Transport for life, London, https://www.transaid.org
2 Hofman, J.J. et al. (2008) Motorcycle ambulances for referral of obstetric emergencies in rural Malawi: Do they reduce delay and what do they cost? International Journal of Gynecology and Obstetrics, 102: 191-197
3 Holmes, W. and Kennedy, E. (2010) Reaching emergency obstetric care: overcoming the ‘second delay’. Briefing paper prepared for Compass: The women’s and children’s health hub, June 2010 Kobusingye, O.C. et al. (2005) Emergency medical systems in low and middle-income countries: recommendations for action. Bulletin of WHO, 83: 626-631
4 Krasovec, K. (2004) Auxiliary technologies related to transport and communication for obstetric emergencies. International Journal of Gyneacology and Obstetrics, 85, Suppl 1: S14 – S23

5 IT Transport Ltd. (2001) Low-cost transport for access to water and health facilities. DfID KaR project R7157 Final Report, London, 2001
6 Lema, V.M. (2011) Maternal and new-born health and emergency transport in Sub-Saharan Africa.". https://www.afcap.org
7 Montez, D. (2010) Mobile communication in Zambia – a demand-side survey analysis of mobile phone access and use. Development Research Series, www.audiencescapes.org
8 Macintyre, K. and Hotchkiss, D. (1999) Referral revisited: community financing schemes and emergency transport in rural Africa. Social Sciences and Medicine, 49: 1473 - 1487
9 Mwebaze, P. et al. (2013) A pregnant woman on a motorbike? Early Experiences of Setting up a Maternal Health Community Transport System in Rural Uganda. Gobal Maternal Health Conference 2013, Arusha, Tanzania.
10 Obeyemi, I.A.O. (2014) Community-based health insurance programmes and the national insurance health scheme of Nigeria: challenges to uptake and integration. International Journal for Equity in Health, 13:20
11 Shimeles, A. (2010) Community-based health insurance schemes in Africa: the case of Rwanda. African Development Bank Working paper No. 120
12 Silva, A.L. (2011) Maternal health and transport: implementing an emergency transport scheme in Northern Nigeria. Transaid, UK, https://www.afcap.org
13 Tewodros, A. (2014) Learning with older people about their transport and mobility problems: improving access to health services and livelihoods. HelpAge International workshop, Dar es Salaam, Tanzania, March 2014
14 Thaddeus, S. and Maine, D. (1994) Too far to walk: maternal mortality in context. Social Science and Medicine, 38(8): 1091 - 1110
15 WHO. (2010) Working with individuals, families and communities to improve maternal and new-borne health. WHO, Geneva
16 World Bank. (2008) Strengthening emergency medical services: a matter of life and death in low-income countries. World Bank and WHO Diseases Control Priorities Project, http://www.dcp2.org
Glossary The following abbreviations are used in the text: AFCAP Africa Community Access Programme funded by the UK Government Department for
International Development ETS Emergency transport service HC Health centre MAMaz Mobilising access to maternal health services in Zambia MAT Motorcycle ambulance-trailer MBA Motorcycle-based ambulance NGO Non-government organisation SSA Sub Saharan Africa Acknowledgements The authors wish to thank AFCAP for the funding that enabled the trials in Zambia to be carried out and to acknowledge the important role played by our partners in Zambia, the Disacare Wheelchair Centre and Riders for Health, Zambia, in making the trials a success Figure 1

Figure 2
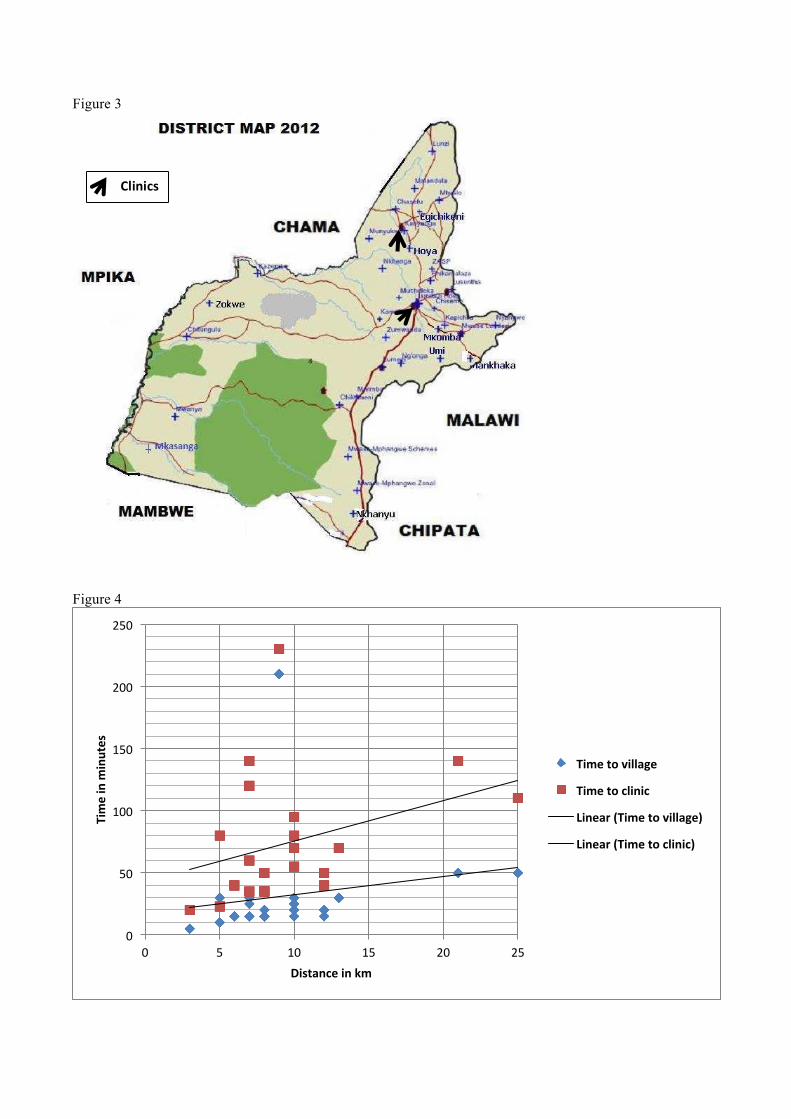
Figure 3
Figure 4
0
50
100
150
200
250
0 5 10 15 20 25
Time in m
inutes
Distance in km
Time to village
Time to clinic
Linear (Time to village)
Linear (Time to clinic)
Clinics

Figure 5
Figure 6
0
200
400
600
800
1000
1200
1400
Range
Maternity Malaria Other condi=on
0
10
20
30
40
50
60
70
80
0 5 10 15 20 25 30
Num
br of b
irths
Month
Mwase clinic
Hoya HP
Mankhaka HP
Linear (Mwase clinic)
Linear (Hoya HP)
Linear (Mankhaka HP)
MAT

Figure 7
0
1
2
3
4
5
6
7
0 5 10 15 20 25 30
Mod
e of tran
sport
Distance (km)
From-‐ vehicle
From -‐ bicycle
From -‐ walk
To -‐ no travel
To -‐ vehicle
To -‐ walk