improving access to seven day services event pontefract 4th june 2015
TRANSCRIPT

Improving Access to Seven Day Services Event
NHS England Yorkshire & The Humber Region
Thursday, 4th June 2015, 09:30 – 2.30pmPremier Suite, Pontefract Racecourse
NHS Improving Qualityand NHS England

Chair’s Welcome and Introduction
Dr David Black, Medical DirectorNHSE Yorkshire & The Humber Region
NHS Improving Qualityand NHS England

7 Day Services across Yorkshire and Humber
Dr David Black, Medical Director (joint) (Yorkshire & Humber)

Objectives of the day
• To update you on 7 day services national requirements
• To support integration with urgent and emergency care review requirements
• To discuss as health communities (System Resilience Groups) the planning to deliver access to 7 day services
• To identify any support that you may need to deliver the 7 day agenda
• To identify what your action will be

NHSE – Our Business Plan

NHSE – Our Priorities
NHS | Presentation to [XXXX Company] | [Type Date]6

NHS | Presentation to [XXXX Company] | [Type Date]7
“At the end of last year, the research company Dr Foster found mortality rates rose by 10% at weekends. Other studies have shown similar correlations.
”BBC News, Health
Higher:
Mortality
Length of
Stay
Readmission
rates
Five day service model not meeting patient needs or expectations.

8
Fewer people are admitted to hospital as an emergency at the weekend but… chances of dying are noticeably higher
100
200
300
400
500
600
700
800
900
MON TUE WED THU FRI SAT SUN
Dis
ch
arg
es
(0
00
's)
3.4%
3.5%
3.6%
3.7%
3.8%
3.9%
4.0%
4.1%
Emerency admissions
Percentage who are discharged dead
DH analysis of HES data 2010/11
National figures, England 2010/11

Variation in diagnostic services
National self-assessment tool Standared 5 and 6
“The NHS will move towards routine services being available
seven days a week. This is essential to offer a much more
patient-focused service and also offers
the opportunity to improve clinical outcomes”
Ten Clinical Standards describing minimum standards of care patients
should expect to receive seven days a week.

“This change will be difficult - but it is the right thing
to do.”
Sir Bruce Keogh, National Medical Director NHS England
Time for Change
12

7Day Services – The 10 Clinical Standards
Patient Experience
Time to first consultant
review
MDTReview
Shift Handovers
Transfer to community and Primary
and social care
MentalHealth
Quality Improvement Diagnostics
On-going review
Intervention/Key services

The Standards, 1-5
1. Patient-focused care
2. All admissions seen by a suitable consultant within 14 hrs of admission, or
within 6 hours between 0800-2000 except,
Patients who are very ill, where it should be 1 hour.
3. 14 hour review by a Multidisciplinary Team inc. Physio, Pharmacist, (and OT if a Medical patient)
4. Handovers by competent decision maker
5. Hospital inpatients must have scheduled seven-day access to diagnostic services

The Standards, 6-8
6. Hospital inpatients must have timely 24 hour access, seven days a week, to
consultant-directed interventions
7. Where a mental health need is identified following an acute admission the patient must be assessed by psychiatric liaison within the appropriate timescales, 24 hours a day, seven days a week:
1 hour- Emergency, 14 hours Urgent
8. Once transferred from the acute area of the hospital to a general ward patients should be reviewed during a
consultant-delivered ward round at least once every 24 hours, seven days a week,
unless “not necessary”
The Standards, 9-10
9. Support services, both in the hospital and in primary, community and mental health settings must be available seven days a week
10. All those involved in the delivery of acute care must participate in the review of patient outcomes to drive
care quality improvement. The duties, working hours and supervision of trainees in all healthcare professions must be consistent with the delivery of high-quality, safe
patient care, seven days a week.

The “When”

Working together to support seven day services

The latest on Urgent and Emergency careUrgent and Emergency Care Networks
• strategic oversight on a regional footprint.
• 1-5 million, depending on local factors.
• to improve consistency and quality of UEC by addressing challenges that are difficult for single SRGs
• This includes setting shared objectives for the Network e.g: Ambulance protocols, 111 services, Clinical decision support, Access protocols to specialist services
• System Resilience Groups - Operational leadership of local services.

NHSIQ Seven Day Services Team
• Help with the ‘how to’ – support health communities, foster collaboration, build momentum, spread change
• Gathering intelligence – understand context, content and culture, impact
• Making connections - Learn, Share, Connect, Curate knowledge, Advise
• Building large scale transformational change capability and capacity – ‘hands on’ facilitation, coach, ‘honest broker’, clinical and public champions
• Shape future policy – identify national, regional, local barriers and challenges

Experienced dedicated team from across the health and care economy
13 Early Adopter Sites:
1. Diagnostics: Spreading evidence-based models
2. Drive for spread: Engaging all healthcare communities in moving towards services that meet the clinical standards and identifying the top interventions
3. Designing new models of seven day services

Have you completed your 7DS self-assessment?
• On-line self-assessment tool to measure progress
• Enables you to baseline your current level of service provision as a local health community
• Find out how your are progressing towards meeting the clinical standards and service provision
• Recent Updates:
Review your progress and benchmark yourself against others and create reports
To access the Seven Day Self Assessment tool, register http://www.7daysat.nhs.uk/

7 Day Self Assessment Tool (7DSAT)
Online Self-Assessment Tool
Multiple Users
Easy to Register
Baseline current service provision
Covers Local Health Economy (LHE) provision
Brings data together
Links to useful information
sources
FAQs
Access Support
Measure progress of services &
Clinical Standards
New tools:
Benchmark yourself against others
http://www.7daysat.nhs.uk/

Benchmark your progress – now available!

7 Day Services SAT & Digest Survey
• Opportunity to have an introduction to this today:
• rolling presentation on screen and laptops for hands-on experience
• Primary Research – interviews and online survey – we need your input – to be launched in June
• Let us know if you would like to take part.
• Speak to your 7 Day Services Facilitator on your tables today!
NHS | Presentation to [XXXX Company] | [Type Date]25

The weekend effect! - Easy Metric

Interactive Session – Key Pad Voting
Where we are now with the Challenge of 7 Day Services implementation …
NHS Improving Qualityand NHS England

A. Less than 10 miles
B. Between 10 and 20 miles
C. Between 20 and 30 miles
D. Between 30 and 40 miles
E. More than 40 miles
Test : How far did you travel to get here today?
NHS Improving Qualityand NHS England

Please tell us if you are a...
1. A Patient / carer / member of the public
2. Voluntary or third sector
3. A Provider
4. A Commissioner
5. NHS England / National body
NHS Improving Qualityand NHS England
Demographic question

How aware are you about the national agenda for improving access to 7 Day Services?A. Very aware
B. Aware
C. Somewhat aware
D. Not aware
NHS Improving Qualityand NHS England

How have patients/public been involved in local 7 Day Service plans?
A. Led on work
B. Involved
C. Not involved
D. Don’t know
NHS Improving Qualityand NHS England

A. Completion of baseline and setting of
priorities
B. Development of a community wide
7DS plan
C. Relationship building with local
partners
D. Improvement support to understand
and redesign the service
E. Sharing and signposting of learning
F. Don’t know
Which element do you think your health and care community needs support with most?
NHS Improving Qualityand NHS England

Thank you for your responses so far.
Please keep hold of your voting handsets as we will use these
again later on…
NHS Improving Qualityand NHS England

Thank you for your responses so far.
Please keep hold of your voting handsets as we will use these
again later on …
NHS Improving Qualityand NHS England
Jane Haywood &Ian Briggs
County Durham and Darlington Early Adopter
Working as a local health community to meet the 7 Day challenge
NHS Improving Qualityand NHS England

www.cddft.nhs.uk
7 Day Services – Beyond Assessment

www.cddft.nhs.uk
County Durham & Darlington Profile
• Population base served:– 610,000 approximately
• 3 Clinical Commissioning Groups
– North Durham, DDES &Darlington– 82 GP practices
• County Durham and Darlington NHS Foundation Trust – integrated acute / community health care provider
– 2 Acute hospitals– Access to six community hospitals
• Tees, Esk and Wear Valley NHS Foundation Trust– Provides inpatient and community services
• Two local authorities– Darlington Borough Council– Durham County Council
• North East Ambulance Service (NEAS)

www.cddft.nhs.uk
Approach to 7 Day Services
• Whole economy integrated approach• Health• Social Care• Third Sector• Patient groups
• Service Transformation• Integrated governance and planning across all partners• Align with locality strategies such as ‘Better Care Fund’.
• Programme Methodology for delivery with three priority areas• Frail elderly• Urgent Care• Diagnostics
www.cddft.nhs.uk
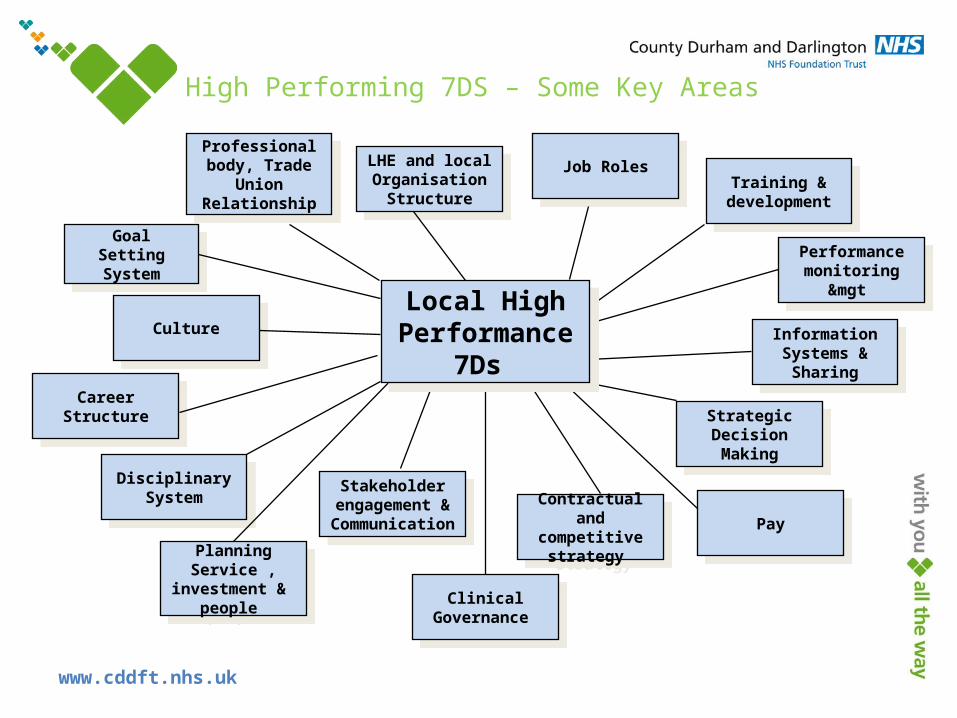
High Performing 7DS – Some Key Areas
Career StructureCareer Structure
Goal Setting System
Goal Setting System
CultureCulture
Disciplinary System
Disciplinary System Stakeholder
engagement & Communication
Stakeholder engagement &
Communication
Clinical Governance
Clinical Governance
Contractual and competitive
strategy
Contractual and competitive
strategy PayPay
Training & development
Training & development
LHE and local Organisation
Structure
LHE and local Organisation
Structure
Professional body, Trade
Union Relationship
Professional body, Trade
Union Relationship
PlanningService ,
investment & people
PlanningService ,
investment & people
Strategic Decision Making
Strategic Decision Making
Information Systems &
Sharing
Information Systems &
Sharing
Performance monitoring
&mgt
Performance monitoring
&mgt
Job RolesJob Roles
Local High Performance
7Ds
Local High Performance
7Ds

www.cddft.nhs.uk
A shared vision creates aligned policy?
20142014
7 day access
BCF
PMCFFederated GP
GP, IT systemMedical contracts
Competition& Cost reduction
DES
2019Vision &position
2019Vision &position
20142014
7 day access
DES
BCF
New contracts
Competition and cost reduction
“Without a sensible shared vision, a transformation effort can easily dissolve into a list of confusing and incompatible projects that can take the organisation in the wrong direction or nowhere at all.”
John P Kotter

www.cddft.nhs.uk
Lessons learned from previous programmes of joint work
Lack of clarity about performance gains to be delivered in each org
Rushing to solutions
Change infrastructure and plans not in place
No concrete management support, management not aligned
Resource needs not recognised
Assumptions & givens not clarified and communicated
Visioning just a paper exercise – not a real picture of the future
Change activity & communications confined to ‘specialists’
Change process begins in the old way – imposition not involvement
Key staff issues and concerns not addressed
Not enough information about the case for change
Once-off communications no continuous process
Sheep dip training/ engagement
Failure to achieve tangible goalsPoor role modelling
Programme taking too long
No redesign – so the new organisation has the wrong configuration
Technical system redesign only – people side short-changed
Imposed by ‘experts’
Using pilots to prove/disprove viability rather than test the design
Inadequate implementation planning and preparationResources not available
Performance dip
Training practicalities ignored
Contingent systems changes not ready
No effective learning processes
Failure to evaluate and review effectiveness of the changesPlateau effect
Leaders stuck in old ways of working
Reverting to old ways in times of crisisRoles not clear
Deliverables not clear
Going too far too fast
Poor role modelling from the top

www.cddft.nhs.uk
Our bespoke change program
B(1)
A(2) Local Critical Success
Failure / Factors (5)
Gap (3)
Change Priorities (4)
+
Change programme

www.cddft.nhs.uk
Programme MethodologyEstablish The programme
• Agree key 7 day principles
• Define point B & understand point A
• 7 day working gap analysis & change agenda
• Programme Plan
• Business case• Create steering
group, change support team & key pathway teams
• Preparing key clinicians & mangers to lead change
Mobilise
• Establish the case for change
• Stakeholder analysis & comms strategy
• Creating a shared 7DS vision
• External visits\
benchmark• Staff input
into 7DS change agenda
• Simple wins
Breakthrough
3 Key pathfinder areas• Frail Elderly• Diagnostics• Urgent care• Cascade vision
into pathfinder areas
• Early Wins
System re-design• Re-designing work
process and systems• Social systems
design• Service configuration• Governance &
Infrastructure design• Define capability
needs• Performance mgt
design• HR\Workforce
systems design
• Review & evaluate pathfinders
• Finalise 7 day working system & design
• Consultation• Develop
phased full roll-out business case & Plan
* Red Text – Areas of Progress
www.cddft.nhs.uk
Areas of Progress
• County Durham and Darlington Foundation Trust acute baseline assessment
• Multi-disciplinary team development:• Acute based• Community based
• Analysis of key barriers to change
• Integrated planning documentation including vision, principles and service blueprints
• Information sharing Agreements (ISA)
• Template and populated ISAs
• Case study on information sharing

www.cddft.nhs.uk
Standard 3 - Multi-disciplinary Team (MDT) review
“All emergency inpatients must be assessed for complex or on-going needs within 14 hours by a multi-professional team, overseen by a competent decision-maker, unless deemed unnecessary by the responsible consultant. An integrated management plan with estimated discharge date and physiological and functional criteria for discharge must be in place along with completed medicines reconciliation within 24 hours.”
Supporting information:• The MDT will vary by specialty but as a minimum will include Nursing, Medicine, Pharmacy, Physiotherapy and for medical patients, Occupational Therapy.• Other professionals that may be required include but are not limited to: dieticians, podiatrists, speech and language therapy and psychologists and consultants in other specialist areas such as geriatrics.• Reviews should be informed by patients existing primary and community• Appropriate staff must be available for the treatment/management plan to be carried out

www.cddft.nhs.uk
Achievements
7 DAY MDT
Average Discharge Increase by 7%
Reduction in LOS 5%
Medical Boarders Per Day
Reduction of 67%
AM discharges
Increase by 13%
Non acute tfr of patients per week
Increase by 27%
ED Activity
Increase by 5%
Falls per week
Reduced by 25%

www.cddft.nhs.uk
Further 7 day Projects Which Have Stemmed From The Implementation Of Standard 3…
There are 4 key issues which are blocking medically fit patients from leaving the ward…
On average the information centres across the six wards are typically seeing 30 patients per week who are now medically fit for discharge but are “blocked” in the system due to problems which are being addressed.
Just over one third of the patients ready to move on are under the Trust’s control
By making problems visible on information centres, the teams have highlighted 4 key areas of focus: CHC assessments, Nursing Home discharges, Diagnostics and community hospitals.

www.cddft.nhs.uk
Community / primary based MDT’s
Engaging the LHE in the process – cross organisational changes to break down barriers

www.cddft.nhs.uk
What We Are Trying To Achieve
• Improve patient experience
• More effective care planning and packages centred on individual needs
• Care in the community or at home where preferred option
• Increase in self-management
• Increased involvement of Voluntary Care sector
• Prevent unnecessary acute admission/re-admission
• Reduce length of stay (e.g. through ‘in-reach’)
• Reduce number of patients transferred to long term care

www.cddft.nhs.uk
Stakeholders Involved
• Darlington CCG & Associated Practices
• County Durham and Darlington FT
• Darlington Borough Council
• Tees, Esk and Wear Valley FT
• Voluntary Sector
• Care Home Sector
• HealthWatch
• NEAS
• North of England Commissioning Support

www.cddft.nhs.uk
Progress since March 2014 –Primary Care
• Practice MDT’s take place monthly in place with attendance from Social Workers, Community matrons and Voluntary Sector brokers
• Advanced care plans being developed for 2% of population at highest risk of emergency admission
• Monthly meetings to discuss those who have had emergency admission in previous month & agree how care plan/support package needs to be amended to prevent re-occurrence
• Voluntary sector broker liaises with other VS organisations as appropriate
• Referrals made to other teams as appropriate e.g. mental health
• Evolutionary development
• Twice weekly MDT meetings with all Community Matrons/Social Workers/Voluntary Sector and TEWV

www.cddft.nhs.uk
Progress since March 2014 – Care Homes and initial feedback
• Community Matrons now working 8am – 8pm; 7 days a week – linked to Top 20 Care Homes
• District Nurses pick up any referrals overnight
• Community Matrons attending all GP practices monthly MDT’s
• EHCP/Advanced Care Plans starting to be put in place for all patients in care homes.
• NEAS aware of new ways of working and ring Matrons prior to patients conveyance to hospital

www.cddft.nhs.uk
Outcomes So Far:Emergency Admissions from Care Homes – April 2014 – April 2015
Location Name Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 TotalsDarlington Manor Care Home 6 4 5 4 4 3 2 5 3 1 1 38Eastbourne Care Home 7 7 1 9 4 4 5 5 10 10 3 11 9 85Eden Cottage Care Home 7 7 1 9 4 4 5 5 10 10 3 11 9 85Grosvenor Park Care Home 8 7 10 8 4 8 4 7 7 6 5 2 3 79Rydal Care Home 3 1 5 5 5 7 2 2 1 3 4 2 40St Georges Hall and Lodge 5 6 6 5 8 6 8 4 10 2 12 2 74The Gardens Care Home 10 4 6 5 6 9 6 8 6 4 2 4 2 72The Grange 9 18 11 3 8 6 6 8 4 10 6 7 6 102Willow Green Care Home 16 7 11 9 6 4 6 3 9 9 5 5 3 93Ventress Hall Care Home 6 8 8 13 10 12 8 15 7 10 2 2 5 106 Elderwood Residential Home 4 2 2 8 4 4 5 4 2 3 1 1 3 43Hundens Park 3 2 5 1 2 2 3 5 3 26Lakeside Care Centre 6 1 1 1 1 2 4 6 3 4 2 3 34Middleton Lodge 2 1 2 2 1 2 2 12
Middleton St George Healthcare Limited 1 1 1 1 4Moorlands Residential Care Home 1 1 5 1 2 1 2 2 2 5 3 1 26North Park 1 3 3 7 2 3 3 4 8 4 2 4 1 45Oak Lodge Nursing Home 2 2 1 2 2 1 1 1 1 2 15Springfield Care Home 3 3 2 2 1 2 5 2 4 3 2 3 1 33St William's Residential Home 2 1 1 1 3 2 10The Lawns Care Home 8 11 1 7 9 3 2 1 5 6 6 2 3 64Wilton House Nursing Home 2 5 6 6 5 7 5 2 1 1 1 2 2 45
Totals 104 99 89 114 79 94 79 87 85 103 55 82 61 1131
www.cddft.nhs.uk
Issues – Or Challenges And Opportunities
• Multi organisation working
• Aligning national strategies against challenging timelines
• Information sharing
• IM & T
• Communication

www.cddft.nhs.uk
New Developments• Geriatrician telephone advice line 12:00 – 14:00 Monday to
Friday
• Hospital to Home 2 nurses working closely with the DMT and facilitating earlier discharge
• Matrons/GP working weekends at DMH in MAU and ED preventing admissions
• GP’s working in ED and MAU on a Sunday
• Due to visibility reducing admissions by 5/6 patients per day on a weekend
• Working with local authority developing assisted technology and Telecare for patients to achieve more self management

www.cddft.nhs.uk
Case Studies
Attending ED picked up one patient from Eastbourne Care Home who had a fall. Was deemed medically fit but had skin tears discharged back to the care home and referred to district nurses for on going management of wounds.
Another patient who lives alone and had a mechanical fall. Medically fit but anxious about returning home alone and admitted she was not coping well. Referred to RIACT+ for urgent assessment and package of care. Supported discharge from ED.
Another patient identified on MAU who was admitted due to Hypertension and change of medication. Discharged home with District nurses monitoring BP and GP made aware.

www.cddft.nhs.uk
Next Steps
• Additional matrons to support Community Rapid Assessment Service - Front of House
• Remaining care homes to commence July 2015
• Identification of areas for future development/investment

www.cddft.nhs.uk
Overcoming the IG ‘Barriers’
• It’s not ‘we can’t share’ – its ‘how can we share’
• An Information Sharing Agreement (ISA) is a document for all parties to agree :
• Assist compliance with information rights law and practice.
• Set’s out standards and consistency that have to be met by all signatories.
• Ensure patient consent is achieved in process

www.cddft.nhs.uk
How will we know where we are going?
shared vision – shared understanding - shared outcomes

www.cddft.nhs.uk
Arriving at a GP practice at 2pm on a Saturday, we note that
• The practice is open and offering both emergency appointments and clinical sessions to patients who have booked there appointment through the multi-agency SPA.
• A mixture of local point of testing, locality based x ray and digital health care systems providing a local integrated diagnostic support system.
• We note the GPs working on the Saturday sessions are from a range of local practices, the local GP federation providing a locality based approach to 7 day working and medical cover.
• A frail elderly MDT meeting is in progress with a local specialist GPwSI, Social worker, a NA&S collaborative nurse , a community diabetic specialist nurse and CPN are holding a video conference with a community geriatrician who is linked in from the local community hospital where she is helping on assessments of patients to move back to home based settings.
• The MDT are all using TPP Systmone as the core single record and basis of the case mgt of both high risk patients and those who are being discharged from hospital. The social and community staff linking in through their mobile working laptop system, all patients on the MDT system having agreed to share their information
• Leaving the practice we note that a program of LTC support sessions are planned for Monday, at these sessions consultants and specialist nurses are booked to provide integrated support sessions to frail elderly patients with multiple conditions - diabetes, vascular and supporting podiatry and retinal screening sessions being carefully planned to allow access to clients until 7pm

www.cddft.nhs.uk
Travelling to a local care home on Sunday we note
• A NA&S collaborative nurse is undertaking a review of 6 patients, 3 identified in a local MDT meeting from risk stratification process as having a risk of escalation and 3 recent arrivals from a planned discharge process 2 from a community hospital and one from a DGH.
• The patient discharged from hospital, arrived an hour ago, the community led integrated intermediate care / discharge team planned the discharge from the hospital with essential medication being provided from the new 7 day pharmacy service. The script being sent electronically from the hospital
• The patients hospital discharge information pack, included a web generated nutrition plan, and a digital health monitoring pack. This cheap and flexible digital health pack, brought by the ISIS HCA in the boot of his car, was connected and put on line and started taking readings within 10 mins. The information being cloud based, allows decisions around additional care to be made by local GPs accessing clinical information. This INR dependant patient is also utilising the digital monitoring system to dose check as required.
• The care home staff are preparing for a visit from a local care home support team of GP, a NA&S collaborative nurse and pharmacist who provide focussed support to help avoid hospital admissions

www.cddft.nhs.uk
In a local elderly persons home
• An NA&S nurse practitioner is visiting to check out a person on the local risk of admission register, the persons carer has called for help from the SPA as they were concerned.
• The nurse is using a digital stethoscope to listen and transmit in real time the heart and lung function to a COPD consultant operating in ‘the front of house’ team of the local A&E unit. The conclusion is that a course of IV antibiotics supported by the local nursing team in the persons home and an enhanced support package , which includes a 3rd sector sitting service, organised by the social worker through the SPA will prevent risk of admission.
• The carer has on their carer patient portal a contact name and support person named to discuss their concerns if required.
• Falls tracker call has been taken by the patient and carer – this asks simple questions to help triage whether after a recent fall the falls team need to come out

www.cddft.nhs.uk
NA&S wrap around service model
• minor injuries• Help line• Emergency care
• Elective• LTC• Self mgt• Health imp
• dementia• Care mgt• Nutrition• isolation
• maternity•Obs & Gynae• childrens•Poorly child•Prevention•Talking therapies Women
and families
Frail elderly
Urgent careAdult
7 day diagnostics & path
lab
Men
tal h
ealth
MD
T –
di
srup
tive
life
styl
e /
addi
ctio
n
Specialist teams consultant / ANP
Community H&WB / Outpatient / digital
hub
Self mgt support digital monitoring
Palli
ative
ca
reSi
ngle
poi
nt o
f ac
cess
SPA
ISIS / Rehab / H
ospital to hom
e
Comm
unity Beds

www.cddft.nhs.uk
Clinical Programme Board (Transformation Board)
County Durham and Darlington Strategic Programme Board
Darlington Organisational
Leads
Better Care Fund
7 Day Working
Care Closer To Home
Unscheduled Care
Planned Care
County Durham Organisational
Leads
Strategic Enabling Programmes Informatics, Estates, Workforce, etc
County Durham and Darlington Transformation Hub
Darlington Transformation Hub
PROGRAMMEPORTFOLIO
GOVERNANCE
RESOURCES
Clinical Advisory Group
Darlington Unit of Planning
County DurhamUnit of Planning
PLANNING
Health and Wellbeing Boards
County Durham Transformation Hub

www.cddft.nhs.uk
IM&T & Equipment infrastructure
• Shared records based on NHS Number • Community and primary teams on same system• Portal technology to link acute /primary/ community/ social care /
tewv/3rd sector and patient / carer• Mobile working with common communications / Wi-Fi to allow
access at any part of LHE system• Digital health systems with multi input capability and able to link
to patient record electronically • All infrastructure (wires / kit / support from common supplier /
maintenance / helpdesk system )• All clinical equipment standardised • Single process for immunisation & vaccinations management –
managed by upgraded child health approach

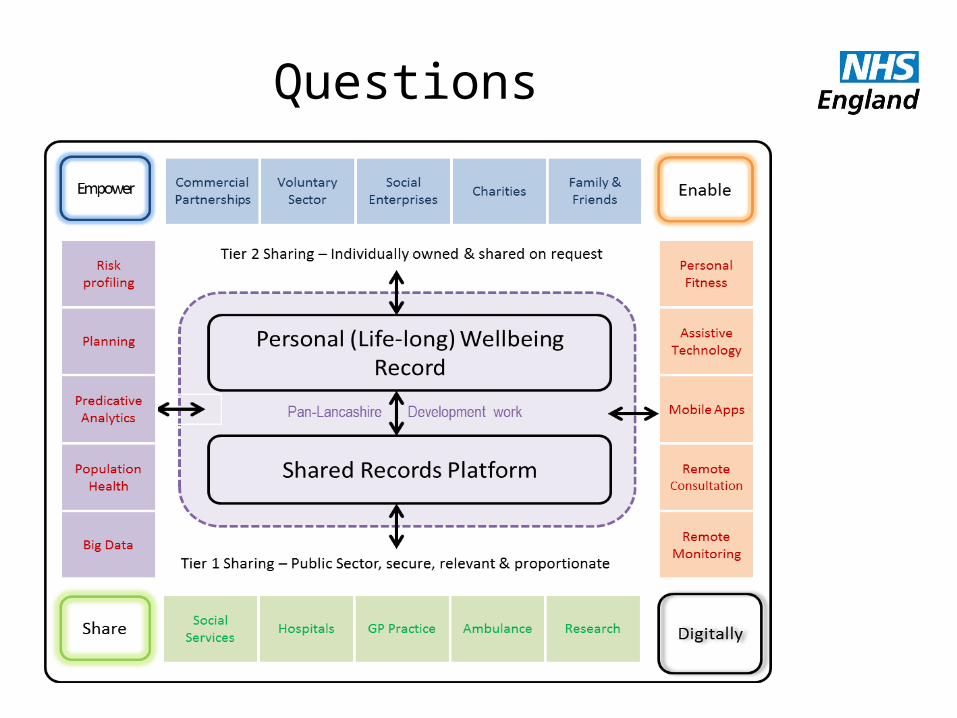
Tony SchaffelHead of LPRES
Lancashire Patient Record Exchange Service (LPRES)
NHS Improving Qualityand NHS England
Seven Day Servicesand
The Lancashire Patient Record Exchange Service
November 2014
Tony SchaffelHead of LPRES

Seven Day Services and LPRES
• Seven days a week, 365 days a year seems to be the holy grail of our politicians and media commentators.
• As an aside, a building company in Burscough for many years used an advertising slogan that could be adopted by the NHS!

Even better than 7 days
Open 8 days a week
Sunday through to
Doomsday!!!

Seven Day Services and LPRES

Seven Day Services and LPRES
• Or to misquote the inimitable Eric Morecambe – “we have all of the right services --- Not
necessarily in the right place or right time.”
The person record
All through your life people, public bodies, banks,
commercial organisations are collecting information about you and your family
The health and social care record is stored in many
systems

Who knows what?
Is technology the silver bullet?
• No, but It should be a major part of the answer
• However we have done the same with the technology as we have with the services.
• Randomly scattering systems and solutions across the NHS landscape.
• In contrast to many European and North American health and social care systems.

Is technology the silver bullet ?

Interoperability!!!
Clinical SystemsOrganisation A
Clinical SystemsOrganisation B
Clinical SystemsOrganisation C
Care SystemsOrganisation D
GP Practice 3rd Sector / Other
Patient / Carer / Citizen
Discharge summaries, scanned letters, path labs results, medication, care plans..
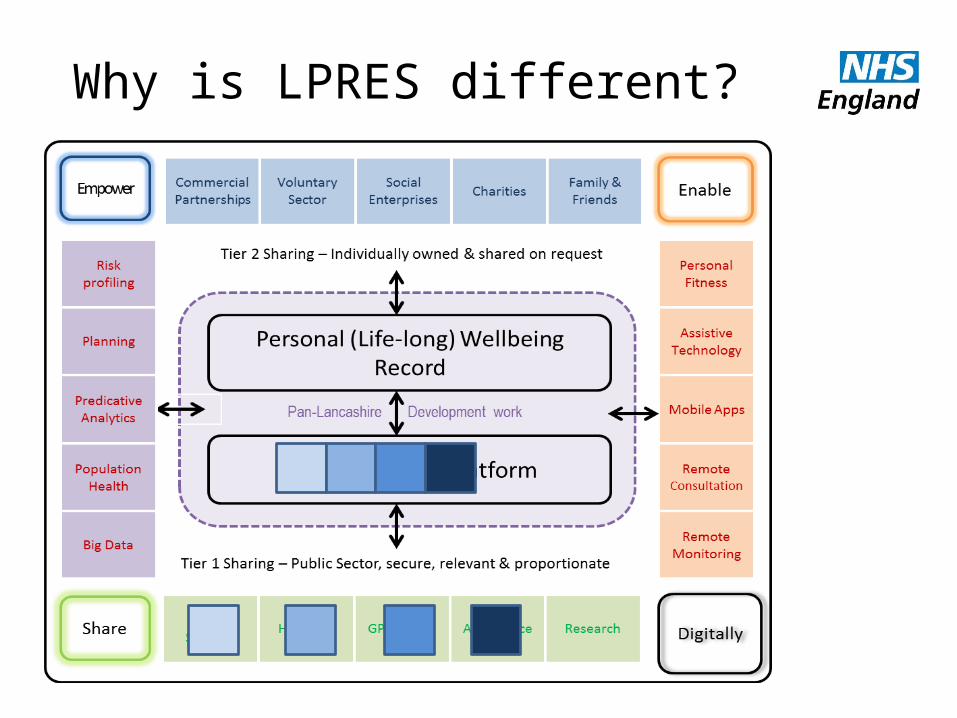
Why is LPRES different?

Empowering citizens - information
Consent model
Application layer

Enabling – assistive technology
Consent model
Application layer

Why is LPRES different?
Primary Care
Community Mental Health
Child Health
Care SystemsOrganisation C
Clinical SystemsOrganisation B
Clinical SystemsOrganisation A
H&WB Platform

Does it work?

Lower Austria statistics

The problem

The Answer

Key Statistics

Benefits to Patients

Benefits to clinicians

Built into the existing systems

Key statistics
LPRES
• Proof of concept in place for last 12 months• Data flowing from EMIS, Liquid Logic, Mental
Health, Acute systems.• ‘Real’ live data tested across platform and
expected live running by September• New Electronic IG register (with PIA module)
up and running• Support from Tech fund and NWCAHSN

Partnerships

Timeline
• We are planning for a 3-5 year programme with the goal of connecting all organisations in Lancashire and to run cross boundary connections to Merseyside, Cumbria and Manchester.
• A rough (very) estimate of the costs is between £5m to £10m.
Questions

The Leeds West CCG Experience of Delivering 7 Day General Practice
Susan Robins, Director of Commissioning
& Kirsty Turner, Associate Director of Primary Care
NHS Improving Qualityand NHS England

Susan Robins Director of
Commissioning
Kirsty Turner Associate Director of
Primary Care
The Leeds West CCG Experience of Delivering 7
Day General Practice

• 37 practices
• Population of 350,000
• Large student population
• Rising >85 population
Leeds West

Population

Our Journey
A small number of practices applied for Prime Ministers Challenge Fund Wave One – unsuccessful
Created an appetite to explore 7 day working
Large number of practices disengaged from the process

CCG created a steering group and invited interested parties to join
Co-developed a specification that would provide flexibility to;
• support those practices that wanted to test out 7 day working
• provide an opportunity for those just wanting to explore enhanced access

Our Model• Routine general practice – not a replacement for
out of hours• Not walk in and not see and treat• Provide appointments at times convenient to the
patient• Provide some flexibility for practices to re-look at
their current provision across the week• Promoted innovation – not one size fits all• 18 month project• Fully funded

Our Model cont……Level 1
Increased Capacity through Extended Hours
Level 2 Increased Capacity through Extended Access (5 days) (7-7 or 8-8 Mon-Fri or Mon-Thurs plus Saturdays)
Level 3 Increased Capacity through Extended Access (7 days) for populations over 35,000 including bank holidays

Current Progress16 practices delivering 7 day access • 2 networks of practices• Via 4 hubs
18 practices delivering enhanced access over 5 days (Monday – Friday or Monday – Thursday plus Saturdays)• 7-7• 8-8

Enablers
• CSU Procurement / NHSE / Monitor
• Clinical engagement and involvement
• Available funds in CCG• Stakeholder consultation• A Great Comms team

Governance• Comprehensive business case developed
(available on the NHS Leeds West CCG website)
• Discussed at our Governing Body and recommendation made to our Assurance Committee who made final decision
• GPs removed from all decision making to avoid conflicts of interest

Evaluation
•Patient experience•Staff experience and opinion•Input data- appointments / workforce / opening times•Impact on system- AED, non elective admissions, 111/ Ambulance/ GP OOH etc

Success?•Phased approach to implementation – address teething problems•Good take up of appointments (with minimal publicity) 10,000 extra commissioned•Increased practice engagement•Positive patient feedback•First evaluation report on wider health system impact in July 2015

Enhanced Primary Care Timeline
October 2014
1st pilot
September 2014
Invited bids
August 2014
Governing Body
Approval
May 2014
March 2014
January 20157 day
service launched
March 2015
Challenge Fund
approval

Challenges We Recognise• Cultural shift • Facilitating change across 37 practices • Information governance • Sustainability • Tension amongst practices – those who were
keen and those who were not• How to support smaller practices• Practices wanting to move levels within project• Comprehensive evaluation process – data and
analysis• Communication – with patients and other
organisations• Impact on OOH GP

Learning
• How do we measure success?
• Think about supporting services – pathology collections has been a significant consideration!
• IT challenges

• Successful bid to PMCF Wave 2• Complements our enhanced access
scheme Broader focus on access Reflects some of the gaps we have
identified locally Responds to what our patients tell us
Developments Post Implementation


Dr Andrew GibsonSteven Haigh
Sheffield – Progress Made Towards
Improving Access to Services
NHS Improving Qualityand NHS England

Sheffield: Progress Made to Improving 7 Day Access to Health
and Social Care Services
DR ANDREW GIBSON, SHEFFIELD TEACHING HOSPITALS ANDSTEVEN HAIGH, JOINT PROVIDER PARTNERSHIP LEAD AND DIRECTOR OF PRIMARY
CARE SHEFFIELD

THE SHEFFIELD CONTEXT
Strong on partnerships and partnership workingAmbitious commissioning intentionsCommitment amongst major providers (FTs, Primary Care Sheffield, Adult Social Care, the Voluntary Sector) to collaborateGood at engaging with the citizens of Sheffield

THE CHALLENGES: READINESS TO DELIVER 7 DAY ACCESS?
Increasing demand (ageing, disease prevalence) and a more expectant populationLess money to useServices already at capacity and stretched furtherWorkforce recruitment and retentionComplex system Strong organisational and professional boundaries

THE OPPORTUNITIES FOR 7 DAY SERVICES
A lot is already there!Not everything has to be accessible 7 days a weekIntegrated Care (commissioned effectively and provided in a joined up way) can deliver 7 day access more easilyA system wide approach to 7 day access might be more efficient, spread the load and make working lives better, and it might even be safer

Where do Sheffield residents want to see improvement to health and social care access?

Results from online 7 day consultation January 2015
• 7 day services should be a priority
• Most people have never been asked their opinion with regards to 7 day services
• Most of the responses were concerning GP practices
• Some people have problems getting a routine appointment within current standard hours
• Most people cannot make a routine appointment in the evening or a weekend

7DS Clinical Standards & SAT: Stakeholder Survey• Don’t currently align well with:
– Community, Social Care, Children’s or Mental Health Services
• Extend to wellbeing standards, prevention, low-level intervention and reduced social isolation
• Leaders need to understand the standards and what they are trying to achieve
• Self-Assessment Tool needs to include Mental Health & Children’s Services

Public Awareness /
EducationWorkforce Finance
Whole System
Integrated
Mental Health
Key Stakeholders: Top Messages
Provision of Seven Day Services Across Sheffield

How does it feel to key stakeholders in Sheffield?
• Power differential between the stakeholders• Not all key stakeholders involved?• How do we make this whole system• Knowledge gap with 7DS and Clinical Standards• Engaging with young people – does it happen?• ‘Just in case’ GP appointments to avoid 1
month wait for routines• “Practices not even open 5 days a week”

Stakeholder Priorities• Access to senior decision makers OOH to
prevent admission – GPs, Community Matrons, Social Care etc.
• Not all services need to be seven days – which do/don’t?
• Older people’s services – gaps particularly mental health
• Transport – health/care agenda not joined up

More …• Primary Care:
– access needs to be across seven days, inc. evenings– more resource at peak times e.g. Monday morning– better support for care homes to reduce admissions – workforce – difficulty recruiting, GPs can’t cover five
days currently – look to skill mix using wider MDT • Social Care:
– Impact of reduced social services – difficultly in supporting weekend discharges
– loss of links/relationships through reorganisations/ £ cuts

Three examples from Sheffield
1. PMCF – Primary care2. Reducing delayed discharges – D2A, 7/7
access to intermediate care3. Acute
– Workforce– Service Review– Service Redesign

1. Sheffield Enhanced Integrated Primary Care (EIPC) Programme: Prime Minister’s Challenge
•A jointly developed proposal led by Sheffield’s GPPB that builds on emerging provider relationships to deliver whole system change.
•Seeks to invest £9.7m in Primary Care and it’s supporting services in the community in Sheffield
•Developed in collaboration with STHFT, SCHSC, GP Collaborative, Service Users, Right First Time (RFT) Programme Office
•Supported by LMC, CCG and LAT
•Primary Care Sheffield to hold contract to fit with strategic objectives

EIPC Programme Objectives• To enhance patient access to Primary care
services throughout the day and week ensuring consistency across the city
• To stimulate system wide change to bring about true integration of services that align in the interests of the patient.
• To build the foundations of transformational change in how General Practice is delivered in Sheffield resulting in improved working lives for GP’s and a better experience for Patients

EIPC Programme Outline•Enhanced access to Primary care services both in and out of hours (weekdays, evenings and weekends) improving consistency of services for patients across the city.•Supported by enhanced community/domiciliary support (to include community nursing, mental health, therapy, pharmacy and social care) and a level of local innovation•Improved communication across the system with a more seamless transition at handover periods and facilitated by connecting the various clinical IT systems•Better self management support for patients
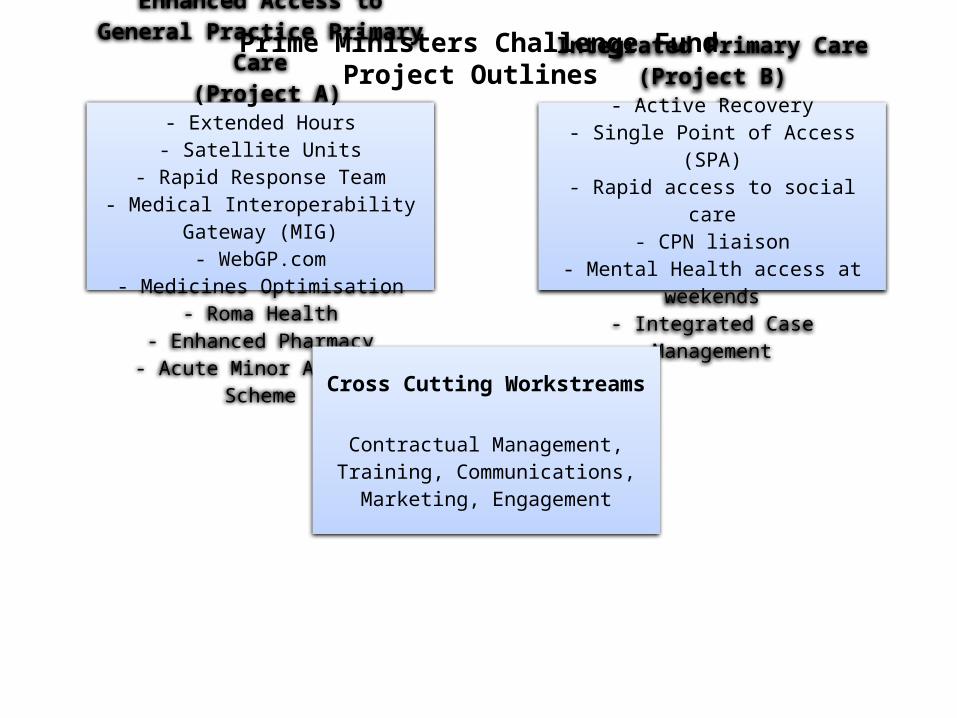
Prime Ministers Challenge FundProject Outlines Enhanced Access to General
Practice Primary Care (Project A)
- Extended Hours- Satellite Units
- Rapid Response Team- Medical Interoperability Gateway
(MIG)- WebGP.com
- Medicines Optimisation- Roma Health
- Enhanced Pharmacy- Acute Minor Ailment Scheme
Integrated Primary Care(Project B)
- Active Recovery- Single Point of Access (SPA)- Rapid access to social care
- CPN liaison- Mental Health access at weekends
- Integrated Case Management
Cross Cutting Workstreams
Contractual Management, Training, Communications, Marketing,
Engagement

2. Seven Day services and Acute Care
• Partnerships– NHS IQ– HiSLAC
• Workforce– Out of Hours– Consultant– Innovation
• Service Redesign– Three A’s Programme
• Urgent and Emergency Care Services Review– STHFT– CCG

Workforce changes and Seven Day Services
• Consultant Job Plans– Devolved Care by Consultant to Consultant – Attending systems– Physician/Surgeon of the week
• Coordinated Care– The OOH Challenge– Competency based – Increased clinical support function
• Physicians associates Expansion Programme• Advanced Practice Faculty Development

Service Review and Redesign• STHFT
– Three A’s Programme• Assess to Admit• Enhanced Ambulatory Care• Workforce Innovation
– Emergency Care Review• 4 workstreams• ECIST
• CCG– Urgent Care Review

3. Discharge to Assess: What have we done?
• Switching from assess to discharge to discharge to assess
• Built capacity in the community (Active Recovery) to take discharges in 24 hours, 7/7
• Developed the for IC bed model to take transfers in 24 hours, 7/7
• Need to address long term care in the same way
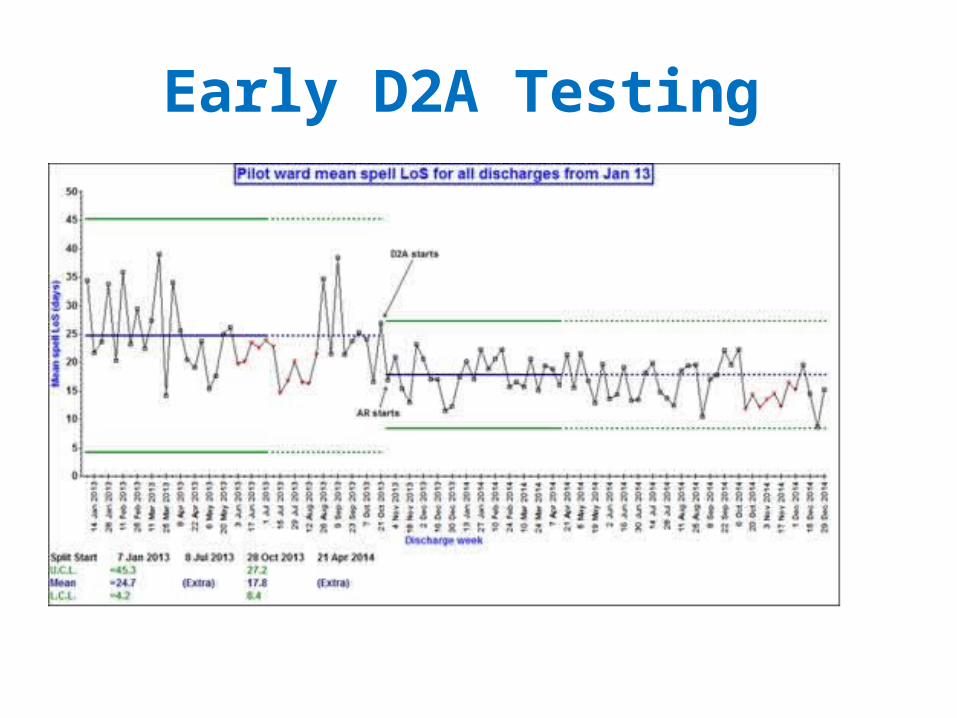
Early D2A Testing

Where are we now?
• D2A now established on GSM wards and will rollout to other medical specialties
• Active Recovery is down to a 24 hour wait (from a mean of 7 days)
• Discharging to off site beds at weekends is better
• DTOCs currently down to around 40 (not good but better than 125+ this time last year)

What’s next for 7 day discharging?
COMMUNITY STANDARDS:• Stabilise D2A – making it business as usual• EVALUATION – is it better for patients, is it
affordable• Link to the Commissioners plans for the Better
Care Fund

What needs to happen next?
1. Cultural change2. Integrated planning and service provision3. Locality based working4. Better partnership working5. Sort the IM&T challenge

Refreshment Break
NHS Improving Qualityand NHS England

Panel of Presenters
Q & A
NHS Improving Qualityand NHS England

Workshop
NHS Improving Qualityand NHS England

Facilitated Workshop Session to discuss
NHS Improving Qualityand NHS England
1. Local Challenges and Barriers
2. What enablers or support is needed to deliver 7 Day Services
Remember to complete your forms about the type of support you would find useful

Final Voting Session
NHS Improving Qualityand NHS England

How aware are you about the national agenda for improving access to 7 Day Services?
A. Very aware
B. Aware
C. Somewhat aware
D. Not aware
NHS Improving Qualityand NHS England

A. Considerable change in view
B. Little change in view
C. No change in view
D. No previous view
NHS Improving Qualityand NHS EnglandHave discussions with your health and
care community changed your views on priorities to deliver?

A. Essential
B. Very valuable
C. Quite valuable
D. Not valuable
NHS Improving Qualityand NHS EnglandHow valuable have the discussions with
your health and care community been to develop future plans?

A. More involved with baseline and planning
B. Identify and meet local leads and get involved
C. Develop plans for engaging with patients and the public
D. Review 7DS provision
E. Review priorities further as a health community
Which action will you take first within the next 30 days?
NHS Improving Qualityand NHS England

Dr David Black
Summary, Next Steps and Close
NHS Improving Qualityand NHS England

Lunch &
Market Place Networking
www.nhsiq.nhs.ukhttp://www.7daysat.nhs.uk/
NHS Improving Qualityand NHS England