improving behavioral health for latino populations
TRANSCRIPT

IMPROVING BEHAVIORAL HEALTH FOR LATINO
POPULATIONS: CREATING POSITIVE CHANGE
MARGARITA ALEGRÍA, PH.D. AND GILBERTO PÉREZ, JR., MSW, ACSW
1

HOUSEKEEPING
Recording and PowerPoint Slide Deck
All Lines Muted
Q&A Session
Chat Box
Q&A Box
Post-Training Evaluation
External Link
2

NLBHA’S VISION AND MISSION
Our vision is to reduce the great disparities that exist in the areas of funding, access,
and quality of care for Latino consumers and families needing mental health and
substance abuse services and supports.
The mission of NLBHA is to influence national behavioral health policy, eliminate
disparities in funding and access to services, and improve the quality of services and
treatment outcomes for Latino populations.
3
IMPROVING BEHAVIORAL HEALTH FOR LATINO
POPULATIONS: CREATING POSITIVE CHANGE
MARGARITA ALEGRÍA, PH.D. AND GILBERTO PÉREZ, JR., MSW, ACSW
4

PRESENTERS
5
Margarita Alegría, Ph.D.
Presenter
Gilberto Pérez, Jr., MSW, ACSW
Facilitator
OVERVIEW
6
1. Changing demographics of the United States and persistent disparities
in behavioral health care.
2. Consistent barriers to Latino behavioral health care.
3. Cultural considerations for Latino behavioral health
4. Promising strategies for programs to improve the behavioral health
workforce for Latino populations

WHAT ARE THE CHANGING DEMOGRAPHICS OF THE
UNITED STATES?
7

CHANGING DEMOGRAPHICS OF THE UNITED
STATES
8
Over the next four decades:
▪ The U.S. population is projected to
grow from 326 million to 404 million.
▪ The non-Hispanic white population
remains the largest, although it is
projected to decline as a result of
falling birth rates and rising death rates.
▪ Racial/ethnic minority populations will
continue to grow, becoming more than
50 percent of total population.
U.S. Census Bureau, 2018.
9
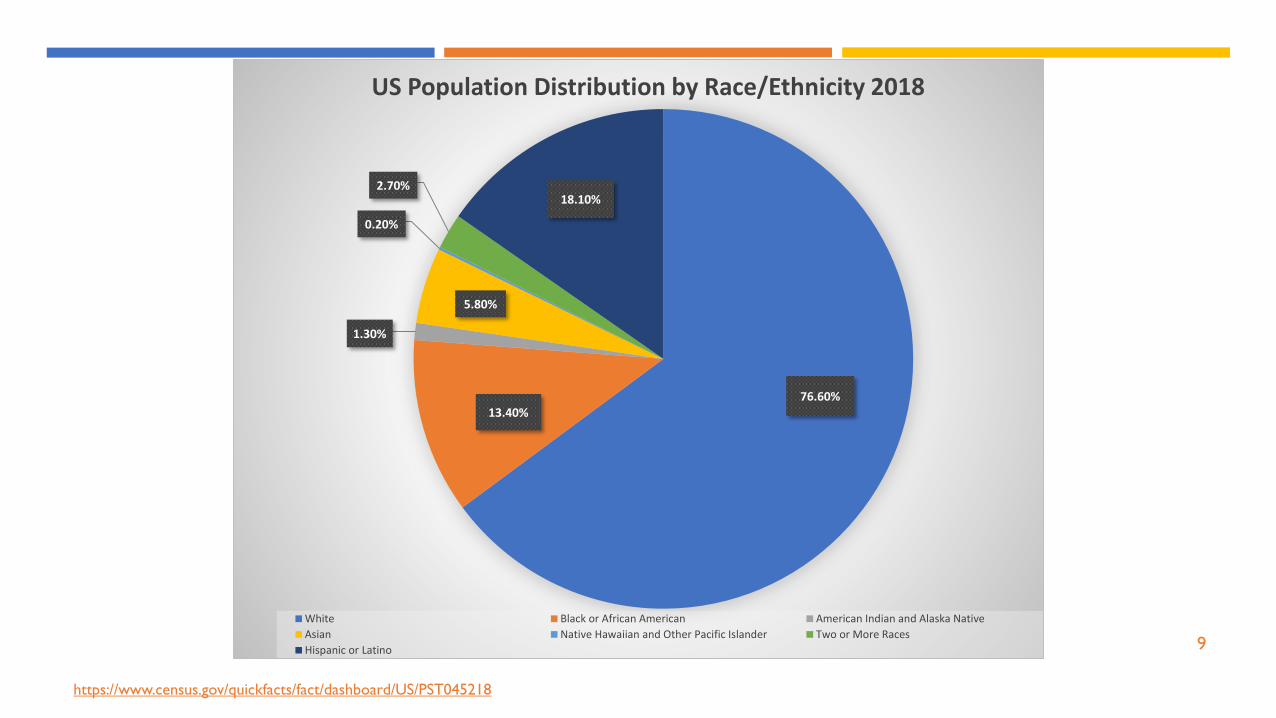
76.60%13.40%
1.30%
5.80%
0.20%
2.70%18.10%
US Population Distribution by Race/Ethnicity 2018
White Black or African American American Indian and Alaska Native
Asian Native Hawaiian and Other Pacific Islander Two or More Races
Hispanic or Latino
https://www.census.gov/quickfacts/fact/dashboard/US/PST045218

10
PROJECTED U.S.
HISPANIC
POPULATION,
2017-2060
U.S. Census Bureau, Quick Facts: https://www.census.gov/library/visualizations/2018/comm/hispanic-projected-pop.html

11https://www.nielsen.com/us/en/insights/news/2016/hispanic-influence-reaches-new-heights-in-the-us.html

WHAT ARE THE CURRENT BARRIERS TO PHYSICAL AND
BEHAVIORAL HEALTHCARE FOR LATINO POPULATIONS?
12

PERSISTING DISPARITIES IN HEALTHCARE
13
• Despite the growing diversity of the U.S. population, disparities continue to
exist in the behavioral healthcare system for Latino populations.
• Racial/ethnic minorities represent more than 50 percent of the uninsured
population.
• Research and reports continue to show that gaining access to behavioral
health services alone does not eliminate service disparities.
• There is a need for a more collaborative, patient-centered approach to care,
including understanding patient preferences of Latinos.
• Need for in-depth understanding of social determinants of health.

DISPARITIES ACROSS PATHWAY OF CARE
Disparities persist along this entire pathway:
Across 10 states, 85% of privately insured patients could get an appointment, compared to 78% of uninsured patients (with $75 payment) and 58% of Medicaid patients (Pauly, Naylor and Weiner, 2014).
Health disparities are too frequently confused with their determinants. This has limited ability of scientific interventions and etiological studies in health disparities to demonstrate the impact in reducing health disparities.
14

THE NATIONAL HEALTHCARE QUALITY REPORT: 2017
DISPARITIES IN ACCESS: 2014-2016
15
• Poor individuals (at or below
100% of federal poverty line)
experienced worsening access
for 18 of 20 access measures
• Blacks experienced worse
access to care for 52% of
measures
• Hispanics experienced worse
access to care for 70% of the
measures

93.7
73.9
35.9
89.5
56.5
43.7
92.4
52.4
40.1
84
74.2
27.1
ANY INSURANCE PRIVATE INSURANCE GOVERNMENT
INSURANCE
non-Latino Whites Blacks Latinos Asians
U.S. HEALTH INSURANCE COVERAGE (%) BY RACE- 2016
Barnett, Jessica C. and Edward R. Berchick, Current Population Reports, P60-260,
Health Insurance Coverage in the United States: 2016, U.S. Government Printing
Office, Washington, DC, 2017.
https://www.census.gov/content/dam/Census/library/publications/2017/demo/p60-
260.pdf
HEALTH INSURANCE COVERAGE BY RACE
(2016)
16

SYSTEMIC BARRIERS TO QUALITY HEALTHCARE FOR
DIVERSE POPULATIONS
17
Low provider diversity or diversity in
leadership
Few culturally and linguistically
competent providers and/or institutions
Service silos and limited understanding of social determinants
of health and their impacts
Unequal community resources and
investments in care
Geographical differences to care
availability: urban, rural, frontier, borders
GEOGRAPHIC DISPARITIES IN BEHAVIORAL
HEALTHCARE DELIVERY
18
• Residential proximity to services and availability of affordable public transportation is an
important factor in access to and utilization of health and behavioral health services.
• Farm laborers experience long work days and isolation.
• Isolated racial and ethnic minority neighborhoods are disproportionately affected by
provider shortages.

TREATMENT LEVEL BARRIERS FOR BEHAVIORAL HEALTHCARE
FOR DIVERSE POPULATIONS
19Limited access and low-quality care may lead to greater use of psychiatric ER.
Limited provider options accepting low payments.
Low geographic supply of diverse providers, particularly multilingual providers.
States limit Medicaid payments.

FACTORS INFLUENCING TREATMENT IN
RACIAL/ETHNIC MINORITY POPULATIONS
• Perception that mental health
services and systems could
not help
• Somatic interpretations of
mental illness
• Stigma, including concerns of
family dishonor, immigration
status, fears of confidentiality
breaches, and hospitalization
Aggarwal, N. K., Pieh, M. C., Dixon, L., Guarnaccia, P., Alegría, M., & Lewis-Fernández, R. (2016). Clinician descriptions of communication strategies to improve treatment engagement
by racial/ethnic minorities in mental health services: a systematic review. Patient education and counseling, 99(2), 198-209.
20
Factors for
Delay in Treatment
• Discomfort discussing
emotions with
clinicians/strangers
• Diverse cultural preferences
for communication styles
(directive vs. exploratory)
• Patient concern about
clinician misuse of power
Factors for
Treatment Participation
• Interpretation that
treatments are appropriate
• Clinician communication
based on patient
expressions of illness/use of
patient vocabulary
• Discussions about patient
confidentiality and inquiry
of patient-clinician
relationship concerns
Factors for
Treatment Continuation

BARRIERS TO CARE
Desire to
handle a
problem on
one’s own
Thinking
that
treatment
would not
workBeing
unsure of
where to
go or
whom to
seeA system that requires
face-to-face engagement
while disregarding the
personal costs of
transportation, time
demands, and lack of
linguistic and cultural
competence that
minority patients
confront
Falgas I. RZ, Herrera L., Qureshi A., Chavez L., Bonal C. , McPeck, S., Wang, Y., Cook B., & Alegría, M. Barriers to and Correlates of Retention in Behavioral Health Treatment
among Latinos in Two Different Host Countries: U.S. and Spain. Journal of Public Health Management and Practice. Forthcoming 2016.
Ponce NA, Hays RD, Cunningham WE. Linguistic disparities in health care access and health status among older adults. Journal of General Internal Medicine. 2006;21(7):786-91
21

DISPARITIES IN MENTAL HEALTH CARE
Aggressive outreach is at odds
with standard clinical practices
such as removing patients from a
caseload after several missed
appointments, and indicates the
need for substantial investment in
engagement and outreach.
Alegría M, Ludman E, Kafali EN, Lapatin S, Vila D, Shrout PE, et al. Effectiveness of the Engagement and Counseling for Latinos (ECLA) Intervention in Low-income Latinos.
Medical care. 2014;52(11):989-97.
Whitten P, Buis L. Private payer reimbursement for telemedicine services in the United States. Telemedicine and e-Health. 2007;13(1):15-24.
22

BREAK – Q&ADEMOGRAPHICS AND BARRIERS TO HEALTH FOR LATINO POPULATIONS
23

WHAT ARE CULTURAL CONSIDERATIONS FOR
ADDRESSING BEHAVIORAL HEALTH DISPARITIES IN
THE LATINO POPULATION?
24

25
Cultural
Considerations
for Behavioral
Health Services:
Working With
Diverse
Populations
• Be familiar with cultural
conceptions of health and mental
health
• Hire and support
bilingual/bicultural behavioral
health providers
• Use interpreters who are trained
in the mental health field
• Collaborate with health care
providers through integrated care
• Infuse traditional health and
healing practices
• Use approaches such as
psychoeducation and home visits

RECOMMENDED PRACTICES
• Adapt treatments to reduce language barriers, including client manuals and scripts for
bilingual clinicians, rather than relying on ad hoc translation
• Integrate behavioral health services into existing programs that provide social
services, such as housing or employment
• Employ culturally adapted social marketing to promote health access and remove
stigma-Bring forth the idea that the earlier you get treated the better!
• Use culturally adapted interventions, collaborating with patients and family advisory
boards to enhance understanding of patient concerns and obstacles in care.
• Diversify and expand behavioral health workforces and provide behavioral health
training to community health workers
Alegría, M., Alvarez, K., Ishikawa, R. Z., DiMarzio, K., & McPeck, S. (2016). Removing obstacles to eliminating racial and ethnic disparities in
behavioral health care. Health Affairs, 35(6), 991-999.
26

EXAMPLE
Delivery of services through telephone holds promise,
especially for low-income, employed Latino patients,
based on a multi-site intervention that delivered
culturally tailored counseling.
The study resulted in significant worry reduction for
those receiving the intervention, and greater worry
reduction in those who received phone intervention
over those who received face-to-face treatment.
Alcántara, C., Li, X., Wang, Y., Canino, G., & Alegría, M. (2016). Treatment moderators and effectiveness of Engagement and Counseling for Latinos intervention on worry reduction in a low-income primary care sample. Journal
of consulting and clinical psychology, 84(11), 1016.
27
TELEPHONE COUNSELING

EVIDENCE-BASED PRACTICES ARE NOT READILY AVAILABLE
FOR LATINO POPULATIONS.
For example, between September 2015-June 2016, there were 36 new
evidence-based programs in SAMHSA’s National Registry.
Less than half were developed with racial and ethnic minority
populations.
Only two described treatment that was culturally-tailored to treat these
populations.
Alegria et al., 2016
28

HOW CAN WE IMPROVE THE BEHAVIORAL HEALTH
WORKFORCE FOR LATINO POPULATIONS?
29
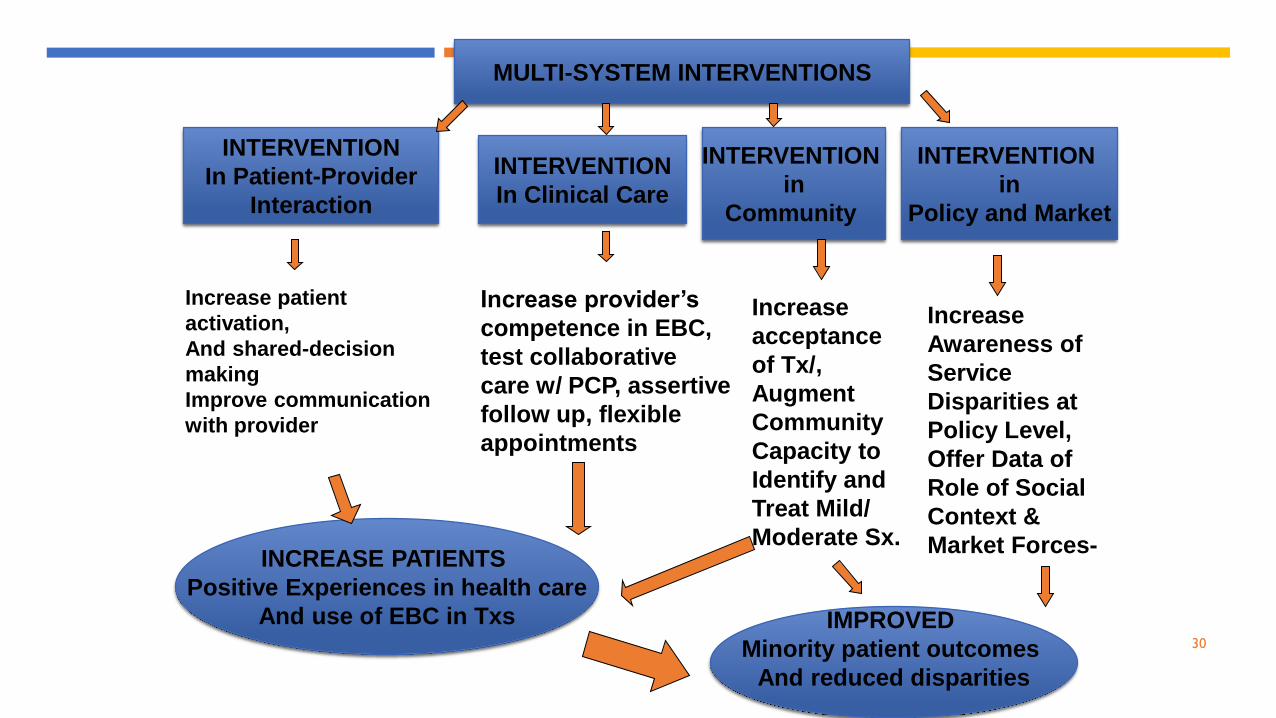
Increase patient
activation,
And shared-decision
making
Improve communication
with provider
Increase provider’s
competence in EBC,
test collaborative
care w/ PCP, assertive
follow up, flexible
appointments
Increase
acceptance
of Tx/,
Augment
Community
Capacity to
Identify and
Treat Mild/
Moderate Sx.
INTERVENTION
In Patient-Provider
Interaction
INTERVENTION
In Clinical Care
INTERVENTION
in
Community
INCREASE PATIENTS
Positive Experiences in health care
And use of EBC in Txs
MULTI-SYSTEM INTERVENTIONS
IMPROVED
Minority patient outcomes
And reduced disparities
INTERVENTION
in
Policy and Market
Increase
Awareness of
Service
Disparities at
Policy Level,
Offer Data of
Role of Social
Context &
Market Forces-
30

INTERVENTIONS IN THE POLICY
ARENA
31

CHANGING ORGANIZATIONAL CULTURE
32
• Provider organizations cannot typically become more culturally responsive
without supplemental resources and technical assistance at the federal, state, and
local levels.
• Provider’s increased cultural awareness requires explicit planning and resources, as
well as staff coaching and increased institutional support and supervision.
• Federal, state, and private insurance payers must incorporate indirect costs into
their fee schedules or find other mechanisms to pay for the expense of change,
such as technical assistance centers that offer training and support without cost to
the provider organization.

33
https://data.hrsa.gov/topics/health-workforce/shortage-areas
The federal government has a formal process
for areas that have shortages of health
professionals – designated as Health
Professional Shortage Areas (HPSA).
These designations can bring opportunity for
federal or state funding for mental health
workforce development.
HEALTH PROFESSIONAL SHORTAGE
AREAS:

INTERVENTIONS IN COMMUNITY
34

BEHAVIORAL HEALTHCARE DISPARITIES IN MINORITY ELDERS
Mental disorders represent 14%
of the global burden of disease
and the third cause of disability.
1 in 5 older Latino adults has 1
psychiatric or substance abuse
Dx. Minority elders appear to
be a risk for greater severity,
persistence, and recurrence of
symptoms
IOM, 201235

SUCH GREAT NEED BUT SERVICE DISPARITIES
Among older adults, NO Treatment for Linguistic Minorities:
90% of those with MH conditions (Karlin et al., 2008).
66% of older adults with MDD
72% of older adults with anxiety disorders (Garrido et al., 2011).
We found only 1 in every ten received minimally adequate care
Partly due to workforce shortages and few evidence-based treatments in community health clinics or ineffective trials in primary care.
36
POSITIVE MINDS-STRONG BODIES (PM-SB)
Build collaborative research to provide disability prevention
treatments in community-based organizations (CBOs) that serve
ethnic/racial minority and immigrant elder clients.
37

Positive Minds (CERED)
10 session manualized individual CBT intervention.
Based on CERED* intervention among Latinos (Alegría et al., 2014).
Adapted for use among elders, and for use with African American and Chinese elders.
Delivered by CHWs.
36-session group exercise program. 12 weeks
Resistance-based exercises to build strength and improve mobility.
Delivered by exercise trainers.
Strong Bodies (INVEST)
PM-SB INTERVENTION
38
*Kafali, N., Cook, B., Canino, G., & Alegria, M. (2014). Cost-effectiveness of a randomized trial to treat depression among Latinos. The journal of mental health policy and
economics, 17(2), 41.

LATE LIFE FUNCTION & DISABILITY INSTRUMENT
(LLFDI)
Assesses function and disability
Function: Refers to individual’s ability to do
specific actions (e.g. stepping on and off a bus)
Disability: Refers to individual’s performance of
expected life tasks within a typical sociocultural
and physical environment (e.g. visit friends and
family in their home)
39

RESULTS OF POSITIVE MINDS-STRONG BODIES
40
• Function and Disability: The PM-SB intervention
exhibited improved scores for late life function and
lowered self-reported disability compared to the control
group
• Mood:The intervention lowered (improved) mood
symptoms, except for generalized anxiety disorder

INCORPORATING COMMUNITY HEALTH WORKERS (CHWs) IN THE
BEHAVIORAL HEALTH WORKFORCE
Frontline public health worker
Trusted member of community or one
with close understanding of community
served
Liaison between health/social services
and community
Facilitate access to services and improve
delivery of culturally competent care
41
Increase knowledge about health through:
Outreach
Community education
Informal counseling
Social support
Advocacy
Who are CHWs? What do CHWs do?
https://www.apha.org/apha-communities/member-sections/community-health-workers

42
HISTORY OF PROMOTORES IN THE US
The work of promotores in the US has been documented since the 1960’s.
Here is a timeline of key events:
2010 2013 2016
A workforce code for
promotores was issued by
the US Bureau of Labor
Statistics under
community health/social
services
The Centers for Medicare and Medicaid
Services created a new rule providing
state Medicaid agencies with the option
to reimburse for more community-
based preventive services, including
community health workers
Since 2016, 16 states
report having CHW
standard operating
procedures or
certification laws
in place
https://mhpsalud.org/programs/who-are-promotoresas-chws/the-chw-landscape/

STRENGTHS OF PROMOTORES DE SALUD
43
EDUCATE &
SUPPORT
ABOUT
RESOURCES
ADDRESS
UNMET
HEALTH NEEDS
COORDINATE
WITH
HEALTH
SYSTEMS
• Help non-English speaking families navigate health care system
• Work towards preventative care, increasing awareness, and getting
the message out
• Help make health systems more responsive to needs in the
community
• Improve access to and quality of care within Latino communities
• Have unique ability to address unmet health needs of minorities
• Address needs of Latino immigrants, such as acceptability to
treatment and how to feel more empowered
• Provide the community and patients with an intervention that makes
sense to the patient and takes into account multicultural issues

STRENGTHS OF PROMOTORES DE SALUD
44
REDUCE
BARRIERS TO
HEALTH
SERVICES
LINK
COMMUNITY
MEMBERS TO
SERVICES
• Integrate information about health into community culture,
language, and values to reduce barriers to health services
• Reduce language barriers to improve patient-provider
communication
• Adapt interventions for Latinos through culturally matched
Promotores
• Improve the health of the community by linking neighbors to health
and social services
• Take into consideration the audience’s presenting problem,
symptoms, and perspectives, including how cultural awareness and
beliefs may influence the method of treatment delivery

INTERVENTIONS IN CLINICAL CARE
45

THE “CONNECTION CHASM”
• Findings from the Patient-Provider Encounter Study:
• Interpersonal factors matter (e.g., language compatibility, cultural preferences, speaking in egalitarian terms)
• Cultural preferences vary across racial/ethnic groups
• Three consistent themes: listening, understanding, and managing difference
• However, definitions for each varied across groups.
46

CLINIC ENGAGEMENT
Characteristics of clinics with successful engagement with
minority patients include having dedicated outreach staff, which
reduces missed appointments.
Trainings such as DECIDE (Decide the problem; Explore the
questions; Closed or open-ended questions; Identify the who,
why, or how of a problem; Direct questions to your health care
professional; Enjoy a shared solution) can positively influence
patient activation for racial/ethnic minorities, although challenges
to engagement and retention may remain.
Alegría, M., Carson, N., Flores, M., Li, X., Shi, P., Lessios, A. S., ... & Jimenez, A. (2014). Activation, self-management, engagement, and retention in behavioral health care: a randomized clinical trial of the DECIDE intervention.
JAMA psychiatry, 71(5), 557-565.
OTHER CONSIDERATIONS
47
TARGETING SDM TO REDUCE DISPARITIES IN CLINICAL VISIT
One way to improve quality and retention in behavioral health care is to implement shared decision making (SDM).
When patients and providers engage in SDM, patients’ preferences are taken into consideration for their treatment, resulting in more appropriate care, increased satisfaction, and ideally, better health outcomes.
48

OPPORTUNITIES FOR SDM -PROVIDERS DECIDE-PC-4 ARM RCT OF
312 PATIENTS AND ~79 PROVIDERS
• Help providers improve patient-provider communication and therapeutic alliance as a possible underlying pathway by which shared decision making can take place.
• Consists of 3-part training sessions totaling 20 hours
• Part 1 – 3 Half-Day Workshops (14 Hours total)
• Targets the five areas of the intervention
• Consist of follow-up individual training within one month of the Part 2 training.
• Calls to coach providers regarding the training using 6 audio-recorded sessions between patients and the provider.
49

QUESTIONS?
50
THANK YOU!
51
Disparities Research Unit Support:
• Larimar Fuentes, MS
• Marie Fukuda
• Ravali Mukthineni
Massachusetts General Hospital
Disparities Research Unit
www.massgeneral.org/disparitiesresearch