improving care for medicare-medicaid enrollees marc steinberg medicare-medicaid coordination office...
TRANSCRIPT
Improving Care for Medicare-Medicaid EnrolleesImproving Care for Medicare-Medicaid Enrollees
Marc SteinbergMedicare-Medicaid Coordination OfficeCenters for Medicare & Medicaid Services
August 5, 2015
Medicare-Medicaid Coordination OfficeMedicare-Medicaid Coordination Office
Section 2602 of the Affordable Care Act Purpose: Improve quality, reduce costs and improve the beneficiary
experience.
– Ensure Medicare-Medicaid enrollees have full access to the services to which they are entitled.
– Improve the coordination between the federal government and states.
– Identify and test innovative care coordination and integration models.
– Eliminate financial misalignments that lead to poor quality and cost shifting.
2
Medicare-Medicaid Enrollee Delivery System Transformation
Medicare-Medicaid Enrollee Delivery System Transformation
FUTURE STATE
Person-Centered
Coordinated Care
Outcomes-Driven
Simplified Processes
CURRENT STATE
Provider and Payor-Centered
Fragmented Care Volume-Driven
Complicated Benefit Overlap
3
Medicare-Medicaid Enrollee Population
Medicare-Medicaid Enrollee Population
Medicare-only
Medicaid-only
Medicare-Medicaid Enrollees (Duals)
10.7 Million Medicare-Medicaid Enrollees with benefits from both Medicare and Medicaid
4
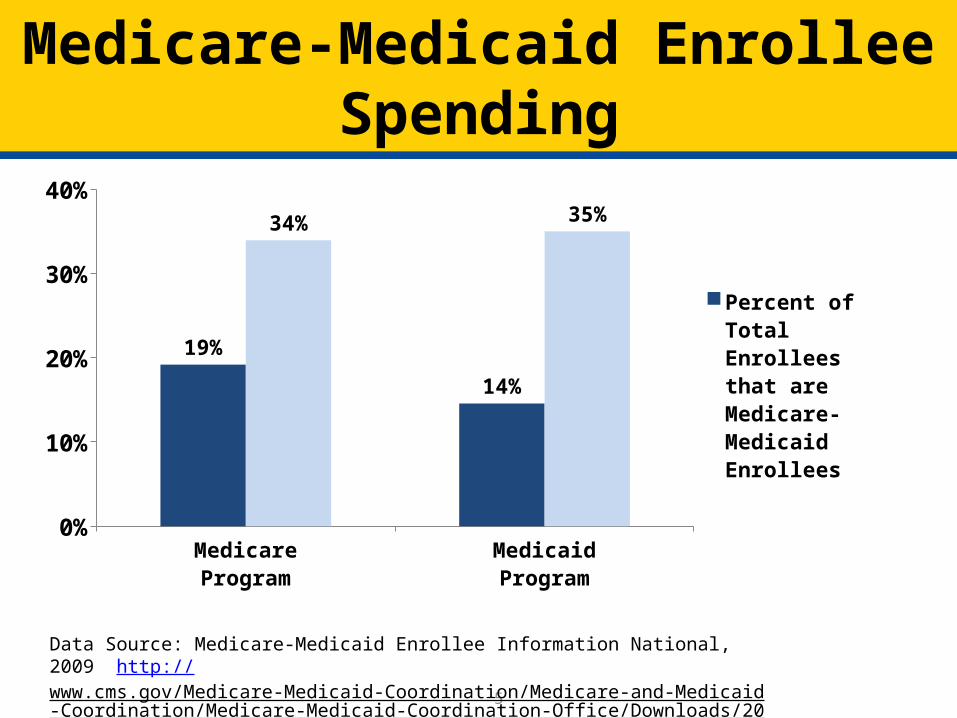
Medicare-Medicaid Enrollee SpendingMedicare-Medicaid Enrollee Spending
5
MedicareProgram
MedicaidProgram
0%
10%
20%
30%
40%
19%
14%
34% 35%
Percent of Total Enrollees that are Medicare-Medicaid En-rollees
Percent of Total Expenditures that are Medi-care-Medicaid Enrollees
Data Source: Medicare-Medicaid Enrollee Information National, 2009 http://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/Downloads/2009NationalProfile.pdf
6
Background: In 2011, the Medicare-Medicaid Coordination Office compiled the Opportunities for Alignment List, which included a broad range of content areas in which the Medicare and Medicaid programs have conflicting requirements or create incentives that prevent Medicare-Medicaid enrollees from receiving seamless, high quality care.
Goal: Identify and implement solutions that advance better care, improve health, and lower costs through improvements.
Examples:• Cost-sharing: Raise Awareness of Prohibition Against Balance Billing
• Appeals: Integrated Denial Notice For Medicare/Medicaid and Medicare Advantage plans
• Durable Medical Equipment: Access to effective repairs, especially for new Medicare-Medicaid enrollees.
• Home Health
The Alignment InitiativeThe Alignment Initiative
6
Data Sharing and Best PracticesData Sharing and Best Practices
Medicare Data to States: • Improved access to Medicare Parts A/B/D and assessment data to support care
coordination and improve quality for Medicare-Medicaid enrollees, and support state program integrity efforts.
State Profiles:• New State profiles that examine the demographic characteristics, utilization,
condition prevalence, and spending patterns of Medicare-Medicaid enrollees and the programs that serve them in each State.
Clinical Condition Flags for the Chronic Condition Data Warehouse (CCW): • New condition flags to streamline research on mental health, conditions related to
disabilities, and tobacco use; Expanded CCW condition flags from Medicare-only claims data to Medicaid-only and Medicare-Medicaid Enrollees; creation of a linked Medicare-Medicaid enrollee data set.
Integrated Care Resource Center (ICRC): • Technical resource center for states. The ICRC supports states in developing
integrated care programs and promoting best practices for better serving Medicare-Medicaid enrollees and other beneficiaries with chronic conditions. 7
Reforming the Delivery System: Financial Alignment Initiative
Reforming the Delivery System: Financial Alignment Initiative
• In 2011, CMS announced new models to integrate the service delivery and financing of both Medicare and Medicaid through Federal-State demonstrations to better serve the population.
• Goal: Increase access to quality, seamlessly integrated programs for Medicare-Medicaid enrollees.
• Demonstration Models:
– Capitated Model: Three-way contracts among States, CMS and health plans to provide comprehensive, coordinated care in a more cost-effective way.
– Managed FFS Model: Agreements between States and CMS under which states would be eligible to benefit from savings resulting from initiatives to reduce costs in both Medicaid and Medicare.
8
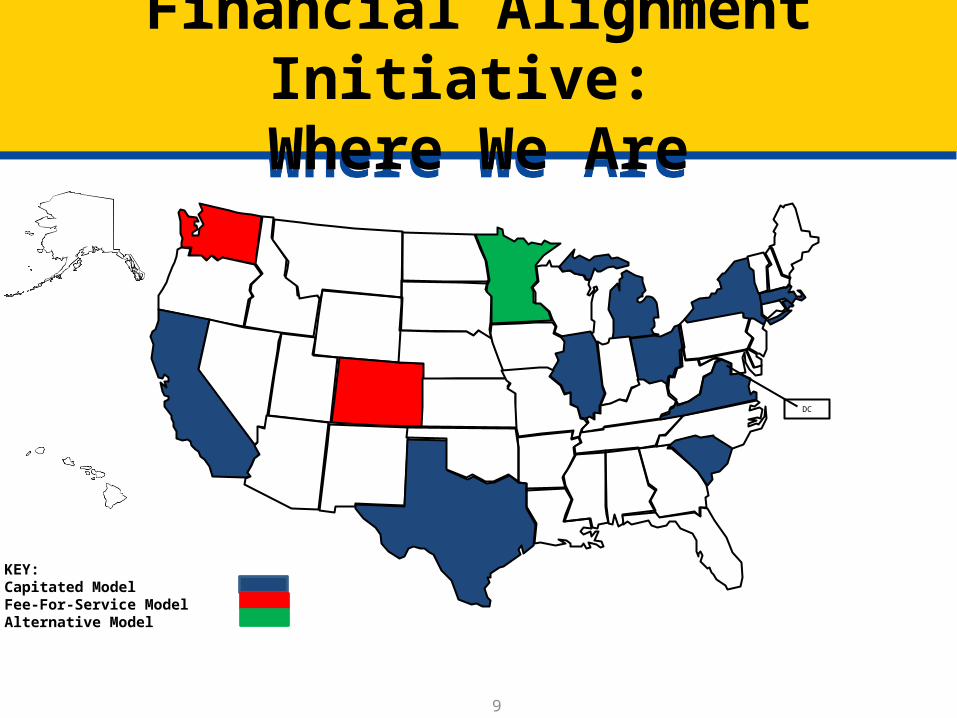
DC
Financial Alignment Initiative: Where We Are
Financial Alignment Initiative: Where We Are
KEY:Capitated ModelFee-For-Service ModelAlternative Model
9
The VisionThe Vision
The Financial Alignment Initiative will promote an improved experience for beneficiaries by:– Focusing on person-centered models that promote coordination missing
from today’s fragmented system– Developing a more easily navigable and simplified system of services for
beneficiaries– Ensuring beneficiary access to needed services and incorporating
beneficiary protections into each aspect of the new demonstrations– Establishing accountability for outcomes across Medicaid and Medicare– Requiring robust network adequacy standards for both Medicaid and
Medicare– Evaluating data on access, outcomes and beneficiary experience to
ensure beneficiaries receive higher quality, more cost-effective care
10
Examples of Beneficiary EnhancementsExamples of Beneficiary Enhancements
• Person-centered care planning• Choice of plans and providers• Continuity of care provisions• Care coordination and assistance with care transitions • Enrollment assistance and options counseling• One identification card for all benefits and services• Single statement of all rights and responsibilities• Integrated grievances and appeals process• Maximum travel and distance times• Limitations on wait and appointment times
11
Support for BeneficiariesSupport for Beneficiaries
• State Health Insurance Counseling and Assistance Programs (SHIPs) and Aging and Disability Resource Centers (ADRCs): To ensure beneficiaries have access to information and counseling around these demonstrations, CMS announced a funding opportunity for both SHIPs and ADRCs in approved demonstration states. This funding will support local SHIPs and ADRCs in providing beneficiary outreach and one-on-one options counseling.
• Ombudsman Services: CMS continues to work with states, advocates and other key partners to ensure Ombudsman services are available for beneficiaries in the demonstrations, and has awarded funding to provide support for these efforts.
12
Initiative to Reduce Avoidable Hospitalizations
Initiative to Reduce Avoidable Hospitalizations
• Initiative funded by the CMS Innovation Center to reduce preventable inpatient hospitalizations among residents of nursing facilities.– Selected organizations are partnering with 144 nursing facilities currently
serving beneficiaries. – Each organization has on-site staff partnering with nursing facility staff to
provide preventive services as well as improve assessments and management of medical conditions.
• Selected Organizations:– Alabama Quality Assurance Foundation (Alabama), Alegent Health
(Nebraska), The Curators of the University of Missouri (Missouri), Greater New York Hospital Foundation, Inc. (New York), HealthInsight of Nevada (Nevada), Indiana University (Indiana), UPMC Community Provider Services (Pennsylvania)
13 9
Report to Congress – Legislative Recommendations
Report to Congress – Legislative Recommendations
– Provide the Secretary the authority to integrate the Medicare and Medicaid appeals processes
– Make “The Medicare Part D Demonstration for Retroactive and Point of Sale Coverage for Certain Low-Income Beneficiaries” (LI NET Demonstration) a permanent program
– Create pilot to expand the Program for All-Inclusive Care for the Elderly (PACE) to individuals between ages 21 and 55
Report to Congress- Areas of Interest Report to Congress- Areas of Interest
• Areas of Interest: – Coverage standards for Medicare-Medicaid enrollees
• Where Medicaid and Medicare overlap on coverage rules and benefits, the programs may apply different threshold standards for items and services, which may result in confusion for states, providers, and Medicare-Medicaid enrollees.
– Cost-sharing rules for Qualified Medicare Beneficiaries (QMBs) • Providers are prohibited from billing QMBs for Medicare
cost-sharing, but complexities of the existing financing often result in cost-sharing not being reimbursed.
Resources on Balance BillingResources on Balance Billing
• Medicare Learning Network article on balance billing: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/SE1128.pdf
• MMCO-CMCS Informational Bulletins on balance billing:– www.medicaid.gov/Federal-Policy-Guidance/downloads/CIB-01-06-
12.pdf
– www.medicaid.gov/Federal-Policy-Guidance/downloads/CIB-06-07-2013.pdf
• MMCO Website FAQs: cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/MedicareMedicaidGeneralInformation.html
Resources on DME and Medicare-Medicaid Enrollees
Resources on DME and Medicare-Medicaid Enrollees
• DMEPOS Competitive Bidding FAQs: dmecompetitivebid.com/palmetto/cbicrd1recompete.nsf/DocsCat/8WYRKB6186
• CMCS August 2013 Informational Bulletin on DMEPOS and coordination with Medicaid: http://www.medicaid.gov/federal-policy-guidance/downloads/CIB-08-02-2013.pdf
More InformationMore Information
Medicare-Medicaid Coordination Office
www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/
18