improving communication between health-care professionals ... · improving communication between...
TRANSCRIPT

Improving communication between health-care professionals and patients with limited
English proficiency in the general practice setting
Melanie AttardA, Alexa McArthur
A,C, Dagmara Riitano
A, Edoardo Aromataris
A, Chris Bollen
B and
Alan PearsonA
AThe Joanna Briggs Institute, Faculty of Health Sciences, The University of Adelaide, Adelaide, SA
5005, Australia.
BAdelaide North East Division of General Practice, Level 1, Education Centre, Modbury Hospital,
Smart Road, Modbury, SA 5092, Australia.
CCorresponding author. Email: [email protected]
Better PracticeBetter PracticeBetter PracticeBetter PracticeEvidence-based information for health professionals
Recommendations• Collectingself-reporteddatafrompatientsoncountryoforigin,ethnicityandlanguageshouldbecarriedoutbypracticestaffbeforetheinitialconsultation.1(Grade A)
• Qualifiedmedicalinterpretersshouldbethecommunicationmediumofchoice.2,3(Grade A)
• Intheabsenceofaqualifiedmedicalinterpreter,andifthepresentingconditionisminor,friendsandrelativesmayinterpretifrequestedbythepatient.2,4(Grade B)
• Thegeneralpracticeshouldbesupportiveofstafftrainingaroundeffectiveandefficientuseofqualifiedmedicalinterpreters.5,6(Grade A)
• Ifpossible,recruitandretaingeneralpracticestaffwhoreflecttheculturaldiversityofthecommunityserved.7(Grade B)
• Culturalcompetencytrainingforallgeneralpracticestaff(bothclinicalandadministrative)ishighlyrecommended.1,2(Grade A)
ObjectivesThepurposeofthisBetterPracticeInformationSheetistopresentthebestavailableevidenceforpromotinginterventionsdesignedtoimprovecommunicationsbetweenhealthcareprofessionalsingeneralpracticeandpatientswithlimitedEnglishproficiency.
Why is this important?Healthcareprofessionalsingeneralpracticetreatpatientsfromadiverserangeofculturalandlinguisticbackgrounds,withasignificantproportionoftheAustralianpopulationspeakingaprimarylanguageotherthanEnglish.PeoplewithlimitedEnglishproficiency(LEP)arelesslikelytovisittheirclinicianandundergootherpreventativescreeningsandtests.8
Theyarealsolesslikelytoadheretomedicationregimesandfollow-upplans,havedecreasedunderstandingoftheirdiagnosis,andoveralllesssatisfactionwiththeircare.4Accesstohighqualitymedicalinterpreterservicesimprovesthequalityofcareforthesepatients.2,3Forthisreason,proactiveassessmentofpatientneedforaninterpretershouldoccuroneachencountertheyhavewiththepractice.
Languageassistancewillideallybeprovidedbyaprofessionallytrainedmedicalinterpreter,butcanalsocomefrommultilingualstaff,familyorfriends.4Byunderstandingthebenefitsthataninterpretingservicecanoffer,healthcareprofessionalscanhelpfacilitateculturallycompetentcare.9Thisisalsosupportedbyensuringstaffhavesufficientawarenessandunderstandingoftheneedsofpatientsfromdiverseculturalgroupsandwhatconstitutesaneffectiveculturallyappropriateservice.
Improving communication between healthcare professionals in general practice and patients
with limited English proficiency
Improving communication between healthcare professionals in general practice and patients with limited English proficiency
Better Practice 2012 | 1
Grades of RecommendationRecommendationsaregradedonthebasisofboththelevelofevidencethatunderpinsthemandfactorsrelatedtotheirimplementation.TheGradesofRecommendationusedherearebasedonthosedevelopedandcurrentlyinusebytheJoannaBriggsInstitute10:Grade AStrongsupportthatmeritsapplicationGrade BModeratesupportthatwarrantsconsiderationofapplicationGrade CNotsupported
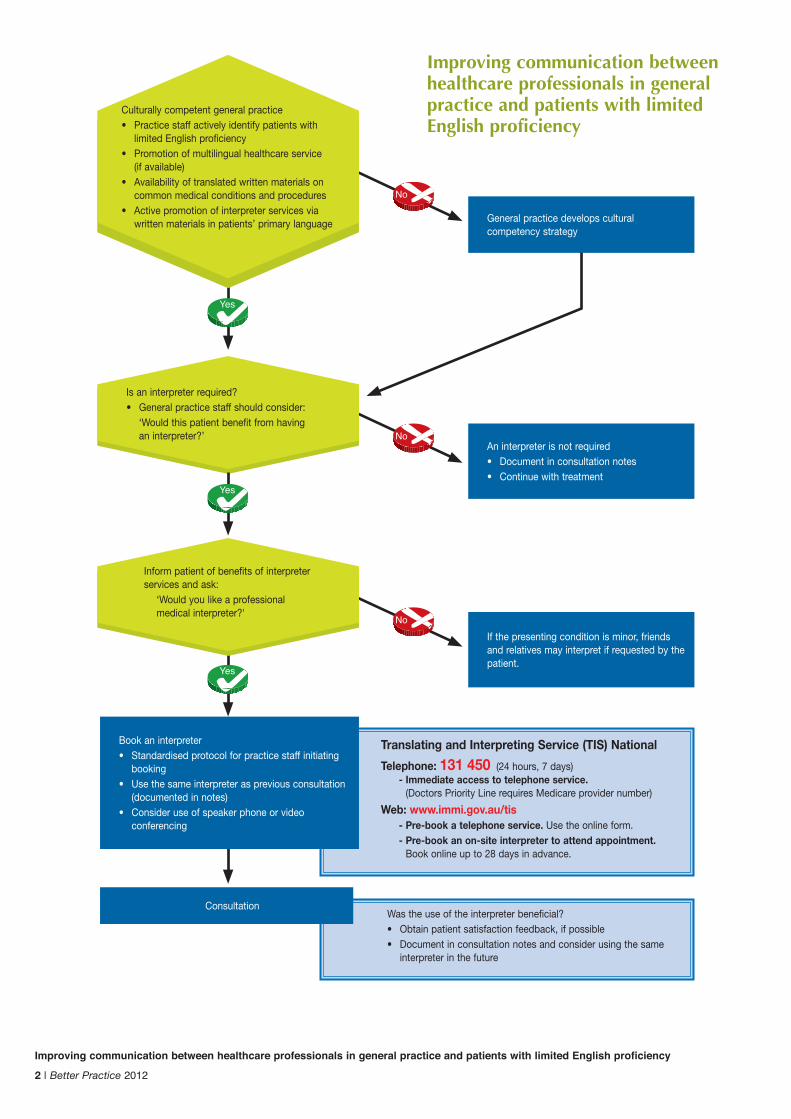
Translating and Interpreting Service (TIS) National
Telephone: 131 450 (24hours,7days) - Immediate access to telephone service.
(DoctorsPriorityLinerequiresMedicareprovidernumber)
Web: www.immi.gov.au/tis - Pre-book a telephone service. Usetheonlineform. - Pre-book an on-site interpreter to attend appointment.
Bookonlineupto28daysinadvance.
Yes
Improving communication between healthcare professionals in general practice and patients with limited English proficiency
2 | Better Practice 2012
Culturallycompetentgeneralpractice• Practicestaffactivelyidentifypatientswith
limitedEnglishproficiency• Promotionofmultilingualhealthcareservice
(ifavailable)• Availabilityoftranslatedwrittenmaterialson
commonmedicalconditionsandprocedures• Activepromotionofinterpreterservicesvia
writtenmaterialsinpatients’primarylanguage
No
No
No
Generalpracticedevelopsculturalcompetencystrategy
Aninterpreterisnotrequired• Documentinconsultationnotes• Continuewithtreatment
Ifthepresentingconditionisminor,friendsandrelativesmayinterpretifrequestedbythepatient.
Consultation
Bookaninterpreter• Standardisedprotocolforpracticestaffinitiating
booking• Usethesameinterpreteraspreviousconsultation
(documentedinnotes)• Consideruseofspeakerphoneorvideo
conferencing
Yes
Yes
Isaninterpreterrequired?• Generalpracticestaffshouldconsider: ‘Wouldthispatientbenefitfromhaving
aninterpreter?’
Informpatientofbenefitsofinterpreterservicesandask: ‘Wouldyoulikeaprofessional
medicalinterpreter?'
Wastheuseoftheinterpreterbeneficial?• Obtainpatientsatisfactionfeedback,ifpossible• Documentinconsultationnotesandconsiderusingthesame
interpreterinthefuture
Improving communication between healthcare professionals in general practice and patients with limited English proficiency
Improving communication between healthcare professionals in general practice and patients with limited English proficiency Better Practice 2012 | 3
1. Enhancing cultural competency within the general practice
•Practicestaffshouldactivelycollectself-reporteddatafrompatientsoncountryoforigin,ethnicityandlanguagebeforetheinitialconsultation.
•Patientpamphletsexplainingtheavailabilityandbenefitsoffreeinterpreterservicesshouldbeondisplayinthereceptionareaofthegeneralpracticeinavarietyoflanguages.
•Recruitandretaingeneralpracticestaffwhoreflecttheculturaldiversityofthecommunityserved.
•Provideculturalcompetencytrainingforstaff(bothclinicalandadministrative),aswellastrainingintheuseofinterpreters.
•AusefulresourcewhichaimstoincreaseculturalunderstandingforserviceprovidersisTheCulturalDictionary.11
2. Communications in patients' primary language
•Wherestaff(bothclinicalandadministrative)havehighproficiencyandarewillingtocommunicatewithpatientsinlanguagesotherthanEnglish,thismultilingualaspectoftheserviceshouldbeactivelyadvertised.
- Languagesspokenbyclinicstaffshouldbehighlightedinthereceptionarea,inleafletsusedtopromotetheserviceandontheClinicwebsite.
- Adviserelevantgroupsofthelanguagesspokenatyourclinic,including:
-MigrantResourceCentreofSAwww.mrcsa.com.au
-RoyalAustralianCollegeofGeneralPractitioners(RACGP)www.racgp.org.au
-Localconsulateshttp://protocol.dfat.gov.au/Consulate/list.rails
•Providetranslatedwrittenmaterialstopatients,wherepossible,butdonotpresumethatallpatientswillnecessarilybeliterateorabletoreadwrittenmaterialsintheirprimarylanguage.
- EnsurematerialsinlanguagesotherthanEnglishmostcommonlyspokenbyyourpatientsarereadilyavailable.
- AsourceoftranslatedwrittenmaterialsrecommendedbytheRACGP2istheHealthInsitewebsiteatwww.healthinsite.gov.au,whichprovideshelpfuleducationalmaterialforpatientsonarangeofclinicalconditionsinavarietyoflanguages.
3. Assessing the need for an interpreter• Trainreceptionstafftoassessforpatientneedforaninterpreterandtoadvisepatientsofinterpretingserviceoptionsavailable.ThisshouldcommencefromthemomentthepatientorfamilymemberfirstmakescontactwiththeClinic.
• EmpowerreceptionstaffbyensuringtheyareawarethatappropriateuseofinterpretersattheClinicrequiresthemtobeproactiveincoordinatingthis.
•Qualifiedmedicalinterpretersshouldbethefirstchoiceforinterpretingservices.
•Familymembersandfriendswillcommonlyactasinterpreters.Thisisacceptableifthepatientproblemisminor,andtheyspecificallyaskfortheirfamilymembertointerpret,however:- Considerthatfamilymembersareunlikelytoact
asneutralinterpreters.- Donotallowfamilymemberstospeakforthe
patientiftheyareactingasinterpreters.- Theuseofchildrenasinterpretersisnot
encouraged.- Itcanbedifficulttodiscussmedicalandother
sensitiveinformationwhenfamilymembersareusedasinterpreters.
4. Accessing interpreter services• HaveastandardprotocolinplaceineachClinicforbookinginterpreters.Thiswillhighlight:
- Exactlywhichlanguage/dialect/culturalgroupisrequired(donotassumepatientalwayswantsinterpreterintheirprimarylanguage)
- Wheregendermaybeimportantduetocultural/familyfactors,trytomatchgenderofpatient,GPandinterpreterwithaimtoavoidhavingfamilymembersactasinterpreter.
- Ifthepatienthaspreviouslyusedaninterpreter,bookthesameoneiftheencounterwassatisfactorysothatanongoingrelationshipcanbedeveloped.
- Nameofinterpreterused(andcontactdetails)shouldbedocumentedintheconsultationnotestofacilitatebookingthesameinterpreter.
• Itisrecommendedthatthetelephoneinterpreterservicebeusedonspeakerphonesothatallpartiescanhearalldialogue.
• Providevideoconferencingoptionwherepreferableforallparties.

“The procedures described here must only be used by people who have appropriate expertise in the field to which the procedure relates. The applicability of any information must be established before relying on it. While care has been taken to ensure this Better Practice Information Sheet summarises available research and focus group input, any loss, damage, cost, expense or liability suffered or incurred as a result of reliance on these procedures (whether arising in contract, negligence or otherwise) is, to the extent permitted by law, excluded”.
• TheJoannaBriggsInstitute TheUniversityofAdelaide
NorthTerrace,SouthAustralia,5000
www.joannabriggs.edu.au ph:+61883134880 fax:+61883134881 email:[email protected]• PublishedbytheJoanna
BriggsInstitute© 2012
ThisBetterPracticeInformationSheetpresentsthebestavailableevidenceonthistopic.Implicationsforpracticearemadewithanexpectationthathealthprofessionalswillutilise thisevidencewithconsiderationoftheircontext,theirclient’spreferenceandtheir clinicaljudgement.
Evidence-based Practiceevidence, context,client preference
judgement
Information SourceThisBetterPracticeInformationSheethasbeenderivedfromanextensiveevidencesummaryandfocusgroupsconductedwithgeneralpractitionersandpracticenursesinMarch2012,withintheAdelaideNorthEastDivisionofGeneralPractice,SouthAustralia.12
AcknowledgementsThisBetterPracticeInformationSheetwasdevelopedbyaresearchteamattheJoannaBriggsInstituteaspartofajointprojectwiththeAdelaideNorthEastDivisionofGeneralPractice.12TheprojectwasfundedbyNorthernCommunitiesHealthFoundationInc.,Adelaide.
References1. FloresG,NguiE.Racial/ethnic
disparitiesandpatientsafety.PediatrClinNorthAm.2006Dec;53(6):1197-215.
2. TheRoyalAustralianCollegeofGeneralPractitioners.Standardsforgeneralpractice:4thedition.2010.
3. Garcia-CastilloD,FettersMD.Qualityinmedicaltranslations:areview.JHealthCarePoorUnderserved.2007Feb;18(1):74-84.
4. KarlinerLS,JacobsEA,ChenAH,MuthaS.DoprofessionalinterpretersimproveclinicalcareforpatientswithlimitedEnglishproficiency?Asystematicreviewoftheliterature.HealthServRes.2007Apr;42(2):727-54.
5. RamirezD,EngelKG,TangTS.Languageinterpreterutilizationintheemergencydepartmentsetting:aclinicalreview.JHealthCarePoorUnderserved.2008May;19(2):352-62.
6. GrayB,HilderJ,DonaldsonH.WhydowenotusetrainedinterpretersforallpatientswithlimitedEnglishproficiency?Isthereaplaceforusingfamilymembers?AustJPrimHealth.2011;17(3):240-9.
7. AndersonLM,ScrimshawSC,FulliloveMT,FieldingJE,NormandJ.Culturallycompetenthealthcaresystems.Asystematicreview.AmJPrevMed.2003Apr;24(3Suppl):68-79.
8. FloresG.Theimpactofmedicalinterpreterservicesonthequalityofhealthcare:asystematicreview.MedCareResRev.2005;62(3):255-299.
9. Dysart-GaleD.Cliniciansandmedicalinterpreters:negotiatingculturallyappropriatecareforpatientswithlimitedEnglishability.FamCommunityHealth.2007;30(3):237-46.
10.TheJoannaBriggsInstitute(AU).GradesofRecommendation[Internet].Adelaide(Australia):JoannaBriggsInstitute;2006[updated2012Feb19;cited2012Apr13].Availablefrom:http://www.joannabriggs.edu.au/Grades%20of%20Recommendation
11.MigrantResourceCentreofCanberra&Queanbeyan(AU).TheCulturalDictionary[Internet].ACTGovernmentCommunityServices(Australia);2003[cited2012Apr13]Availablefrom:http://www.dhcs.act.gov.au/__data/assets/pdf_file/0017/5282/Cultural_Dictionary.pdf
12.McArthurA,AttardM,RiitanoD,WilliamsM,AromatarisE,BollenC,PearsonA.ImprovingcommunicationbetweenhealthcareprofessionalsingeneralpracticeandpatientswithlimitedEnglishproficiency.Adelaide:TheJoannaBriggsInstitute,UniversityofAdelaide(Australia);2012May.
Improving communication between healthcare professionals in general practice and patients with limited English proficiency
4 | Better Practice 2012
Excellent resources from the Centre for Culture, Ethnicity & Health
TipSheetsavailablefordownloadinclude:• assessingtheneedforaninterpreter• arranginganinterpreter• workingwithinterpreters
www.ceh.org.au/mghp/problem_gambling_resources/mghp-using-interpreters.aspx