improving obesity prevention and treatment in gps clinic h sonali magdo, do pgy 2 chla
TRANSCRIPT
Improving obesity prevention and
treatment in GPS clinic
H Sonali Magdo, DO
PGY 2
CHLA

Background:
Prevalence of obesity in American children1
1999-2000 2003-2004
Girls 13.8% 16%
Boys 14% 18.2%
Health consequences of obesity in childhood5,6
Type II DM Hypertension OSA Depression/low self esteem Nonalcoholic fatty liver disease SCFE Pseudotumor cerebri
Objectives
1. Review existing literature on childhood obesity
2. Identify the obstacles faced by physicians in a general pediatrics clinic in assessing and treating children who are overweight through use of survey
3. Provide physicians in GPS clinic with resources to improve prevention/ management of overweight and obesity

Assessment of PCP management of obesity4
Of all children who met criteria for obesity, only 53% of visits documented obesity
69% documented an adequate dietary history 15% documented activity level

Medical history and PE
Condition % pediatricians % PNP
Hypertension 97 95
Type II DM 38 41
Genetic Syndromes
32 22
Sleep disorders 41 27
GI disorders 22 24
Orthopedic problems
38 46

Survey Results:Barriers to treatment of obesity/overweight
0
10
20
30
40
50
60
* Lack of time Lack of support *Lack ofknowledge of
communityprograms
Lack of clinicguidelines
Always a problem
Frequently a problem
Sometimes a problem
Never a problem

Survey results clinic resources
Survey Results:
1. Lack of time to counsel patients
2. Lack of clinic guidelines for disease management
3. Lack of knowledge of community programs
Intervention:
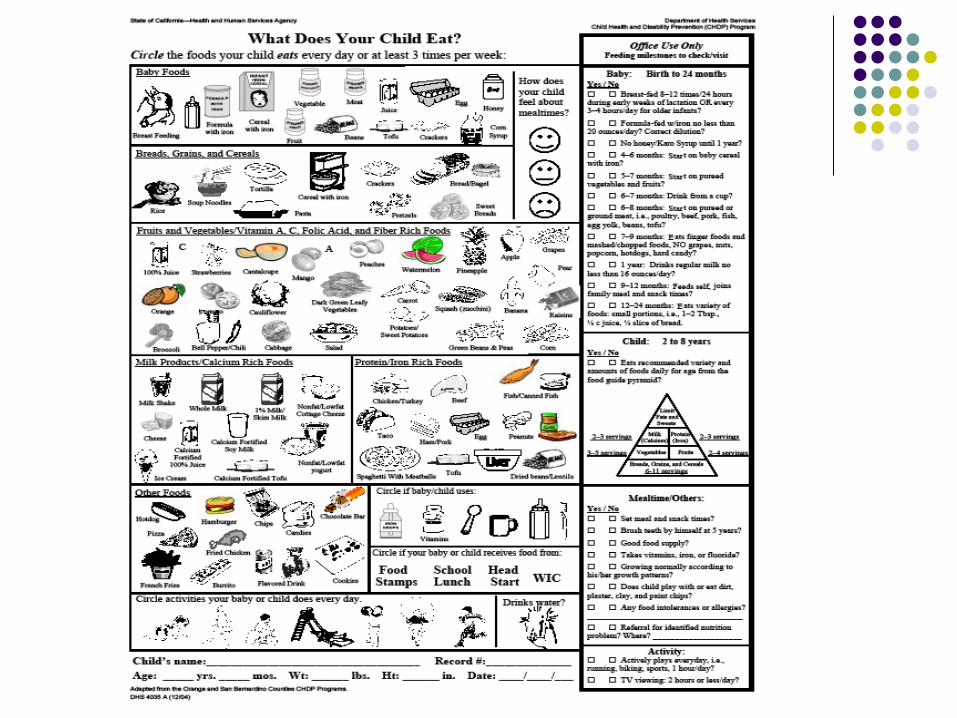
1. Nutritional intake form
2a. Creation of chart (adapted from Pediatric Annals article) for reference in clinic b. Weight check form
3. Creation of booklet compiling community programs for overweight/obese children in LA

Clinic flow chart
R If LDL > 110mg/dl Consider referral to orthopedics or
Nutritional evaluation Height and weight measurements BMI calculation and interpretation
Non-overweight BMI 5th-84th %
At risk for being overweight BMI 85-94%
Diet and physical activity counseling and management of family dynamics with frequent follow up
Family Patterns and Risk Assessment Family and child eating patterns and physical activity (including screen time) FHx: overweight, coronary artery disease, hypertension, type II DM, hypercholesterolemia Recent weight increase or concerns
Overweight BMI > 95%
Return in one year for follow up
Genetic syndromes Endocrine abnormalities Type II DM Hypertension Dyslipidemia Respiratory Disturbances Muscle/skeletal abnormalities
Assessment of At Risk and Overweight Children
Developmental Delay Dysmorphic Features Abnormal or absent genitalia Digital anomolies
Suspect: - Prader Willi - Turner Syndrome - Laurence-Moon-- Bardet-Biedle
Poor linear growth -Hirsutism -Moon facies -Acne -Buffalo hump -Striae
- FHx: Type II DM -Race/ethnicity - Signs of insulin resistance (HTN, dyslipidemia, acanthosis nigricans, PCOS)
If: BP >95% for height and gender on 3 separate occasions
+ Family hx of CV disease <55 yrs age OR Parent cholesterol > 240 and/or LDL >160 OR Child’s total cholesterol >250 and/or LDL >160 with no family hx * check fasting lipid panel in all children >10 with BMI >85%, add AST/ALT and fasting glucose if + risk factors
- Dyspnea on exertion - Shortness of breath
-Spinal asymmetry -Flat feet -Genu varus/valgus
-Obstructive sleep apnea - Disordered sleep breathing
Refer to genetics
Suspect: Hypothyroidism Check TSH, T4
Suspect: Cushing’s Syndrome Check 24 hr urine cortisol
Check FPG, if > 126 mg/dl
Refer to endocrinology Refer to cardiology Refer for sleep evaluation and/or ENT
Consider referral to orthopedics or PT
Adapted fromAriza AJ, RS Greenberg, R Unger. Childhood overweight: management approaches in young children. Pediatric Annals. January 2004; 33(1): 33-38.

Clinic weight check formALTA MED WEIGHT CLINIC VISIT Place sticker
hereDate:Vital signs: Temp BP / (___%) HR RR ___ Weight (___%) Height____ (____%) BMI____ (_____%) Previous BMI ____ (____%) on __/__Allergies: Medications:_____________________________Do you see your child as ___ overweight ____ normal weight ____ underweight?Diet History:1. How many meals a day do you eat? At the table, with whole family present? ______2. What is the largest meal of the day? How many snacks do you eat per day? ______3. How much juice do you drink? How much soda? ______ Activity History:1. How many hrs of TV do you watch? How many hours of video games/computer time? ______2. How much exercise do you get? Exercise enough to sweat: how many times/week? ______Medical History Questions:1.Obstructive sleep apnea: Snoring? Gasping for breath at night/long pauses in breathing? _____ 2. Shortness of breath with exertion? _____3. Irregular/scant periods? Known history of PCOS? _______4. Headaches? (pseudotumor cerebri) ______5. Depression:
Increased or decreased sleep? _______ Loss of interest in favorite activities? _______Feelings of guilt, hopelessness, regret? ______ Low energy? ______Difficulty concentrating? _______ Increased or decreased appetite? _______Psychomotor retardation/agitation? _______ Suicidality? _______ (Depression= 4 of the above + feelings of depression or anhedonia for at least 2 weeks)
6. Binging/Purging? (children >8-9 yrs old) _______Family History: 1. Race/Ethnicity: * African American *Hispanic *Asian/Pacific Islander *American Indian Caucasian2. FHx of Type II DM in 1st or 2nd degree relative? ____ Yes No3. FHx of obesity: Yes No One parent overweight? ______ Both parents overweight? ______4. FHx of cardiovascular disease: 1st or 2nd degree relative with MI, CVA, PVD, angina, sudden cardiac death before age 55? ______ Coronary arteriography + for atherosclerosis), coronary bypass, balloon angioplasty? _______ Parent with cholesterol >240? _______

Clinic weight check formFocused physical exam: HEENT: Tonsillar hypertrophy ______ Dysmorphic features _______Papilledema_____Neck: Palpable thyroid _______Lungs: Heart: Abdomen: Hepatomegaly ______Skin: Acne ____ Acanthosis nigricans ____ Hirsutism _____ Striae _____ Neuro: Developmental delay ______Musculoskeletal: Buffalo hump ______ Digital anomalies ______ Spinal asymmetry ____ Genu varum ______ Genu valgum ______ GU: Abnormal genitalia ______
Labs: Fasting glucose** Lipid panel ________ Liver function panel______ Thyroid function tests (if linear growth is poor, family hx, palpable thyroid)_____Referrals ____ ENT (OSA, disordered sleep breathing) ____ Overnight Sleep Study____ Cardiology (Dyspnea on exertion, LDL > 110mg/dl, + FHx, BP > 95% for height and gender on 3 visits)____ Endocrinology____ Orthopedics/PT(Spinal asymmetry, genu varum/valgum)____ Genetics (DD, dysmorphic, abnormal genitalia, digital anomalies)____ Gastroenterology____ Comprehensive Obesity Program (Powerplay, ENERGY, Fit Families, Happy Feet)____ Nutrition referral **Screen for diabetes:Any child/adolescent who is overweight (BMI >85%) + 2 risk factorsScreening should begin at age 10 or onset of puberty if puberty occurs at a younger age. Screen every two yrs Risk factors:1st or 2nd degree relativeRace (American Indian, African-American, Hispanic, Asian/Pacific Islander)Signs of insulin resistance/conditions associated with insulin resistance: acanthosis nigricans, hypertension, dyslipidemia, PCOSCurrent screening guidelines call for fasting glucose. (Random glucose, 2 hr post prandial glucose, HgAIc: not part of current guidelines)Follow up visit: 1 month 2 months Signature:
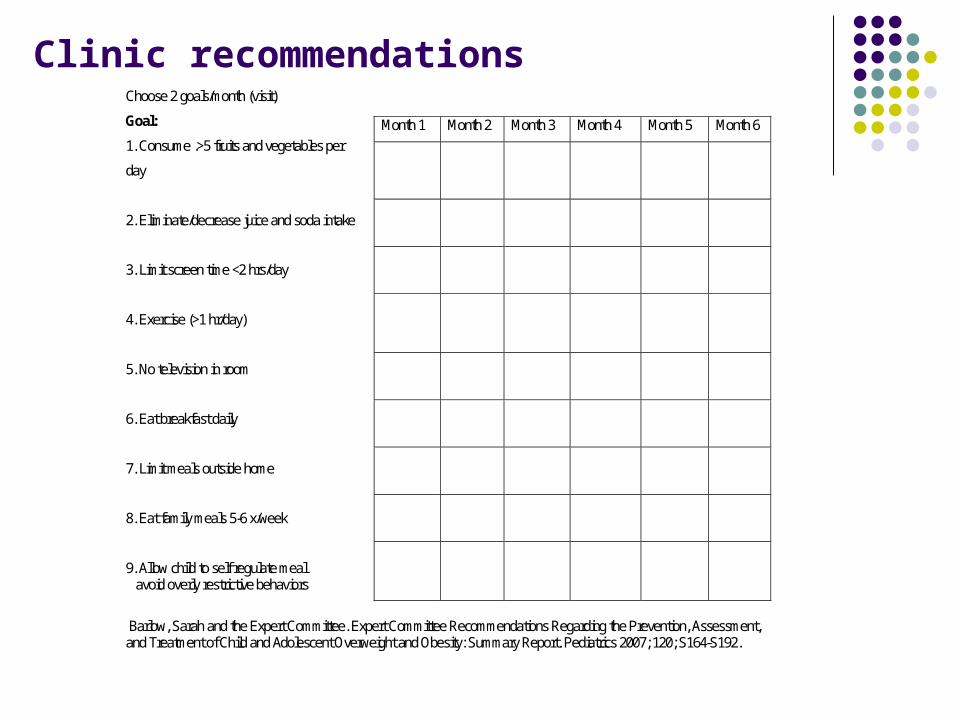
Clinic recommendationsChoose 2 goals/month (visit)
Goal:
1. Consume .>5 fruits and vegetables per
day
2. Eliminate/decrease juice and soda intake
3. Limit screen time <2 hrs/day
4. Exercise (>1 hr/day)
5. No television in room
6. Eat breakfast daily
7. Limit meals outside home
8. Eat family meals 5-6 x/week
9. Allow child to self regulate meal avoid overly restrictive behaviors
Barlow, Sarah and the Expert Committee. Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report. Pediatrics 2007; 120; S164-S192.
Month 1 Month 2 Month 3 Month 4 Month 5 Month 6

Future projects
Evaluation of success of project Survey of patients and their families Creation of webpage linked to CHLA website
to use for resources in the community Creation of nutrition and activity handouts
that are culturally sensitive

Thank you!
Susan Wu, MD Larry Yin, MD Hope Wills, RD Esther Berenhaut, RD Yvonne Gutierrez, MD

References:1. Ogden, CL, Carroll MD, Curtin LR et al. Prevalence of overweight and obesity in the United States,
1999-2004. JAMA. 2006 Apr 5 295; (13): 1549-1555.
2. Ariza AJ, RS Greenberg, R Unger. Childhood overweight: management approaches in young children. Pediatric Annals. January 2004; 33(1): 33-38.
3. Committee on Nutrition. Cholesterol in childhood. Pediatrics. Jan 1998; 101(1): 141-147.
4. Obrien SH, R Holubkov, EC Reis. Identification, evaluation and management of obesity in an academic primary care center. Pediatrics. Aug 2004; 114(2): e154-e159.
5. Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. Mar 1998; 101(3pt2): 518-525.
6. Hoppin, AG, ES Katz, LM Kaplan, GY Lauwers. Case 31-2006: A 15-year-Old girl with severe obesity. NEJM. Oct 2006; 355(15): 1593-1602.