improving the delivery of different news study report · improving the delivery of different news...
TRANSCRIPT

ImprovingtheDeliveryofDifferentNewstoFamiliesbyHealthcareProfessionals
MARCH2019
Esther Mugweni1, Melita Walker1, Samantha Goodliffe1, Sabrena Jaswal2, Catherine Lowenhoff3,
CheryllAdams1,AngieEmrys-Jones&SallyKendall1,2
1.InstituteofHealthVisiting
2.UniversityofKent
3.OxfordBrookesUniversity

ii
ACKNOWLEDGEMENTS
Wewouldliketothankthefamiliesandhealthcareprofessionalsforsharingtheirtimeintakingpart
inthisstudy.Wewouldliketothankthevariouscharitiesthatsupportedtherecruitmentoffamilies
intothisstudyandespeciallyacknowledgetheroleplayedbyMrsAngie-EmryJones.Wewouldlike
tothankMarianneLindfield(SurreyandSussexLibraryandKnowledgeServices)forconductingthe
evidencesearchforthisstudy.WewouldalsoliketothankHealthEducationEnglandworkingacross
Kent,SurreyandSussexforfundingthisresearch.Weparticularlyacknowledgethesupportprovided
by RhonaWestrip ProgrammeManager for Intellectual DisabilitiesHEE South Region andGeorge
MatuskaClinicalLeadIntellectualDisabilities–HEESouthofEnglandRegion.
Correspondence
Pleaseaddressallcorrespondencewithregardstothisresearchreportto:
DrEstherMugweniResearchLeadInstituteofHealthVisitingc/oRoyalSocietyforPublicHealth,JohnSnowHouse,59MansellStreet,London,[email protected]

iii
ABBREVIATIONS
BCW BehaviourChangeWheel
COM-B Capability,Opportunity,MotivationBehaviourmodel
DN DifferentNews
DDN DeliveringDifferentNews
DS Down’sSyndrome
HCPs HealthcareProfessionals
HEEKSS HealthEducationEnglandworkingacrossKent,SurreyandSussex
iHV InstituteofHealthVisiting
TDF TheoreticalDomainsFramework
iv
TABLEOFCONTENTS
ACKNOWLEDGEMENTS----------------------------------------------------------------------------------------------------II
ABBREVIATIONS------------------------------------------------------------------------------------------------------------III
TABLEOFCONTENTS------------------------------------------------------------------------------------------------------IV
LISTOFFIGURES------------------------------------------------------------------------------------------------------------V
LISTOFTABLES--------------------------------------------------------------------------------------------------------------VI
1. BACKGROUND----------------------------------------------------------------------------------------------------------1
1.1 STUDYAIM--------------------------------------------------------------------------------------------------------------21.2 STUDYOBJECTIVES------------------------------------------------------------------------------------------------------21.2.1PHASE1OBJECTIVES----------------------------------------------------------------------------------------------------21.2.2PHASE2OBJECTIVES----------------------------------------------------------------------------------------------------21.3STUDYOUTCOMES---------------------------------------------------------------------------------------------------------21.3.1PHASE1OUTCOMES----------------------------------------------------------------------------------------------------21.3.2PHASE2OUTCOMES----------------------------------------------------------------------------------------------------31.4REPORTSTRUCTURE--------------------------------------------------------------------------------------------------------3
2. METHODOLOGY-------------------------------------------------------------------------------------------------------4
2.1METHODOLOGYFORPHASE1---------------------------------------------------------------------------------------------4COMPONENT1:LITERATUREREVIEW-----------------------------------------------------------------------------------------4COMPONENT2:INTERVIEWS--------------------------------------------------------------------------------------------------5COMPONENT3:DEVELOPMENTOFTHETRAININGINTERVENTION---------------------------------------------------------6COMPONENT1:DELIVERYOFTHETRAININGINTERVENTION----------------------------------------------------------------8COMPONENT2:QUESTIONNAIRES--------------------------------------------------------------------------------------------8COMPONENT3:INTERVIEWS--------------------------------------------------------------------------------------------------82.3DATAANALYSIS-------------------------------------------------------------------------------------------------------------8
3.LITERATUREREVIEW----------------------------------------------------------------------------------------------------9
3.1POLICYREVIEW:GUIDELINESONTHEDELIVERYOFDN-----------------------------------------------------------------93.2RESULTSOFLITERATUREREVIEW----------------------------------------------------------------------------------------103.2.1THEIMPACTOFRECEIVINGDN---------------------------------------------------------------------------------------163.2.2IMPORTANTFACTORSFORDDNEFFECTIVELY--------------------------------------------------------------------173.2.3TRAININGINDDN-----------------------------------------------------------------------------------------------------183.3CONCLUSION--------------------------------------------------------------------------------------------------------------19
4. PHASE1FINDINGS--------------------------------------------------------------------------------------------------21
4.1DESCRIPTIONOFPARTICIPANTS-----------------------------------------------------------------------------------------214.2FACTORSTOCONSIDERWHENDDN------------------------------------------------------------------------------------214.2.1SOCIAL/PROFESSIONALROLES---------------------------------------------------------------------------------------224.2.2KNOWLEDGE,SKILLSANDBELIEFSABOUTCAPABILITIES------------------------------------------------------------24A. Experience------------------------------------------------------------------------------------------------------------24

v
B. Competence----------------------------------------------------------------------------------------------------------254.2.3ENVIRONMENTALCONTEXTANDRESOURCES-----------------------------------------------------------------------29A. Privacy-----------------------------------------------------------------------------------------------------------------29B. Time---------------------------------------------------------------------------------------------------------------------304.2.4OPTIMISM--------------------------------------------------------------------------------------------------------------324.2.5BELIEFSABOUTCONSEQUENCES--------------------------------------------------------------------------------------334.2.6EMOTION---------------------------------------------------------------------------------------------------------------344.3SUMMARYOFPHASE1FINDINGS---------------------------------------------------------------------------------------35
5. INTERVENTIONDEVELOPMENT---------------------------------------------------------------------------------36
5.1DEVELOPMENTOFTHETRAININGINTERVENTION---------------------------------------------------------------------365.2TRAININGCONTENT------------------------------------------------------------------------------------------------------425.2.1TRAININGAIMSANDOBJECTIVES ------------------------------------------------------------------------------------425.2.2DESCRIPTIONOFTHESESSIONSINDETAIL---------------------------------------------------------------------------43
6. PHASE2FINDINGS--------------------------------------------------------------------------------------------------46
6.1DESCRIPTIONOFPARTICIPANTS-----------------------------------------------------------------------------------------466.2SOCIAL/PROFESSIONALROLESANDIDENTITYANDSOCIALINFLUENCES--------------------------------------------476.3KNOWLEDGE,SKILLSANDBELIEFSABOUTCAPABILITIES--------------------------------------------------------------506.4ENVIRONMENTALCONTEXTANDRESOURCES--------------------------------------------------------------------------546.5OPTIMISM----------------------------------------------------------------------------------------------------------------566.6BELIEFSABOUTCONSEQUENCES-----------------------------------------------------------------------------------------586.7EMOTION-----------------------------------------------------------------------------------------------------------------59
7. DISCUSSION-----------------------------------------------------------------------------------------------------------61
7.1 KEYFINDINGS----------------------------------------------------------------------------------------------------------617.2LESSONSABOUTDATACOLLECTIONMETHODS-------------------------------------------------------------------------627.3RECOMMENDATIONS----------------------------------------------------------------------------------------------------637.3.1FUTURERESEARCH-----------------------------------------------------------------------------------------------------647.3.2TRAININGCONTENT----------------------------------------------------------------------------------------------------647.3.3ESTABLISHMENTOFPOLICIESANDPROTOCOLSONDDN------------------------------------------------------------657.3.4ROLLINGOUTTHETRAINING-------------------------------------------------------------------------------------------65
8. CONCLUSION---------------------------------------------------------------------------------------------------------66
REFERENCES-----------------------------------------------------------------------------------------------------------------36
L IST OF F IGURES
FIGURE1:COM-BMODEL............................................................................................................................................7FIGURE2:THEORETICALDOMAINSFRAMEWORK...............................................................................................................7FIGURE3:FLOWCHARTOFTHESTUDIES......................................................................................................................11FIGURE4:CHARACTERISTICSOFTHEFAMILIES................................................................................................................21FIGURE5:READYMNEMONIC.....................................................................................................................................45FIGURE6:DESCRIPTIONOFPROFESSIONALSWHOATTENDEDTHETRAINING.......................................................................46
vi
FIGURE7:FREQUENCYOFDDNBYHCPS.......................................................................................................................47FIGURE8:PREVIOUSTRAININGINDDN.........................................................................................................................48FIGURE9:CHANGESAFTERTRAINING...........................................................................................................................51FIGURE10:PREANDPOST-TRAININGUNDERSTANDINGABOUTSUPPORT...........................................................................55FIGURE11:CHANGESINKNOWLEDGEABOUTBALANCEDDESCRIPTION..............................................................................57FIGURE12:CHANGESINMANAGINGEMOTIONS............................................................................................................60
L IST OFTABLES
TABLE1:DESCRIPTIONOFSTUDIES..............................................................................................................................12TABLE2:KEYASPECTSOFDDN...................................................................................................................................35TABLE3:INTERVENTIONCOMPONENTS.........................................................................................................................37TABLE4:TRAININGCONTENT......................................................................................................................................43
1
1. BACKGROUND
As part of the foetal anomaly screening programme, all eligible pregnant women in the United
Kingdom are offered screening to assess the risk of their baby being born with Down’s (Trisomy
21/T21), Edwards’ (Trisomy 18/T18) and Patau’s (Trisomy 13/T13) syndromes or other structural
abnormalities [1]. Some congenital anomalies may be associated with a learning disability. This
includeschromosomaldisorderssuchasDown’sSyndromeaswellasotherfoetalstructuralanomalies
such as complex congenital heart diseases [2, 3]. Antenatal screening identifies mothers with an
increasedchanceofhavingachildwithfoetalanomaliesandenablesHCPsandthefamiliestomakea
moreinformeddecisionaboutwhethertoproceedwithdefinitiveprenataldiagnostictests[1].Italso
enablesHCPsandfamiliestoagreeonappropriateplansforthedelivery;treatmentoptionsifavailable
andinsomecasesandhavediscussionsonpossibleterminationofthepregnancy.
Whileantenatalscreeningmay identifysomeanomaliesduringpregnancy,somearenot identified
untilafterbirth.Whenanomaliesareidentified,familiesarefacedwiththeunexpectedexperienceof
receivingdifferentnewsabouttheirunbornornewlybornchild.Theterm“differentnews(DN)”is
usedinthisstudytodescribetheprocessofimpartingandreceivinginformationrelatingtoanunborn
ornewlybornchildbeingdiagnosedwithaconditionassociatedwithalearningdisability.
Inprevious studies,parentsexperienceda rangeofemotions immediatelyafterDNwasdelivered
includingsignificantdistress,fear,grief,depression,anxietyandchronicstress[4-6].Chronicstressin
parentsmaynegativelyaffectparentingskillsandmayresult inharshreactiveparentingwhichcan
impair the social-emotional, cognitiveandphysicaldevelopmentof children, increasing the riskof
mooddisordersinlaterlife[7].Maternalandpaternaldepressionarealsoknownpredictorsofpoorer
cognitive functioning, impaired adaptive functioning, increased risk of depression, anxiety and
conduct disorders in children exposed to this [8-10]. It is imperative that HCPs who DDN are
adequatelytrainedtominimisethenegativepsychologicalimpactofreceivingDNonfamilies.

2
1.1 STUDYAIM
1.1.1Phase1Aim
• TodevelopatraininginterventiontoimprovethedeliveryofDNtofamiliesbyHCPs.
1.1.2Phase2Aim
• Toconductanevaluationofatrainingprogrammetoassessitsacceptability,feasibilityandoptimal
interventiondesignforfutureroll-outofthetraining.
1.2 STUDYOBJECTIVES
1.2.1PHASE1OBJECTIVES
1. TodescribeandexplainthelivedexperienceofreceivingDNfromHCPs
2. TodescribeandexplainthelivedexperienceofDDNtofamiliesbyHCPs.
3. ToidentifythebarriersandfacilitatorstoeffectivedeliveryofDN.
4. ToidentifytrainingneedsforHCPswhodeliverDN.
5. TodevelopaDDNtraininginterventionforHCPs.
1.2.2PHASE2OBJECTIVES
1. ToassesstheacceptabilityandfeasibilityofimplementingthetraininginterventionforHCPsby
assessingrateofuptakeandcourseadherenceandcompletion.�
2. To establish barriers and facilitators to course attendance and participant views on course
contentandsessiondelivery.�
3. Todetermineproofof principleby gathering informationabout changes in knowledge, skills,
attitudesfromhealthcareprofessionalspre-andpost-intervention.
1.3STUDYOUTCOMES
1.3.1PHASE1OUTCOMES
Phase1wasprimarilyqualitativeinnatureduetotheHCPsurveyhavingaverylowresponserate.The
outcomesforPhase1were:
• Identificationofthetrainingneedsforeffectivelydeliveringdifferentnews.
3
• Identificationofbarrierstoeffectivedeliveryofdifferentnews.
• Identificationoffacilitatorstotheeffectivedeliveryofdifferentnews.
ThemainoutputfromPhase1wasthetrainingintervention.
1.3.2PHASE2OUTCOMES
A. PrimaryOutcomes
• Thepercentageofhealthcareprofessionalswhoareofferedandcompletethetraining.�
• Thepercentageofhealthcareprofessionalsreportingincreasedknowledge,skillsand
confidenceafterthetraininginterventionisdelivered.
B. SecondaryOutcomes
• Acceptabilityofthetrainingintervention.
• AcceptabilityandfeasibilityofdeliveringthesametraininginterventionamongvariousHCPs
whodeliverdifferentnews.
1.4REPORTSTRUCTURE
Thereportisdividedintoeightchapters.Wedescribetheresearchmethodologyinchapter2andthen
detailour findings fromthe literaturereview inchapter3. Inchapter4wepresent thequalitative
findingsfromPhase1andinchapter5wedescribethetraininginterventionandhowwedeveloped
it.Inchapter6,wepresentthefindingsfromPhase2andtheninchapter7,wepresentthediscussion
andinchapter8wepresenttheconclusionsfromthisstudy.
4
2. METHODOLOGY
Thiswasaprospective,mixed-methods,non-randomisedstudyconsistingoftwophases.
2.1METHODOLOGYFORPHASE1
TherewerethreecomponentstoPhase1datacollection:
COMPONENT1:LITERATUREREVIEW
AliteratureandpolicyreviewexploringtheprocessofDDNwasconductedto:
• providethecontextinwhichfamiliesreceiveDNintheUK.
• examinetheimpactofreceivingDNonfamilies.
• clarifygoodpracticewhenDDN.
• IdentifyareasforfurtherdevelopmentforHCPswhodeliverDN.
• identifythedifferenttypesoftraininginterventionstosupportthedeliveryofDN.
• clarifyimportantfactorstoconsiderinthedevelopmentofatrainingintervention.
Aliteraturesearch1wasperformedinApril2017bySurreyandSussexLibraryandKnowledgeService
in the following databases: CINAHL, HMIC, Medline, NICE Evidence, PsychINFO, Google Custom
Search,WileyOnlineLibrary.OnlystudieswritteninEnglishwereincluded.Conferenceproceedings
wereexcludedfromthereview.Thelibraryteamalsosearchedgreyliteratureforpolicydocuments
onDDN.OnefurthersearchwasundertakenbyEMonthe23rdofOctober2018inPubMedandWeb
ofSciencetoupdatethedatabaseofstudiesforthereview.Onlystudiespublishedbetween2004and
2018wereincludedtoreflectcurrentchangesinpracticeinthedeliveryofdifferentnews.Studies
wereonlyincludediftheywereconductedintheEU/EFTA,NorthAmerica,NewZealandorAustralia.
ThesearchincludedquantitativeandqualitativeevidenceonDDNandhadtoreporton:
• thelivedexperienceofreceivingDNduringpregnancyoratbirth.
• theprocessofDDN.
1Thesearchtermsusedwere:breakingnews,learningdisability,prenatal,diagnostictechniquesobstetrical,intellectualdisability,postnatalcare,disability,communication,news,breakingsadnews,breakingbadnews, informingparent,givingbadnews,givingsadnews,receivingbadnews,receivingsadnews,informationpreference,copingstyle,prenataldiagnosis,communicationbadnews,postnataldiagnosis,postnatalsupport,effect,impact,parentalexperiences,unbornchild.
5
• theimpactofreceivingDN
• theimpactofDDNonHCPs
• theservicesorsupportprovidedbothprenatallyandpostnatallyafterreceivingDN
• traininginterventionstoimproveDDN,theirfeasibility,acceptability,andeffectiveness.
Thelibraryteaminitiallyscreenedalltitlesandabstractsforeligibilityusingthesetcriteria.Eligible
studies were then passed on to the research team for full paper screening. This was done
independentlybyEMandSGusingascreeningtool.Astructureddataextractiontoolwasdeveloped
tocapturetherequiredinformationfromtheincludedpapers.Extracteddataweresummarisedby
EMand SG.Disagreements in interpretationwere resolved through discussion between the team
members.QualityoftheeligiblepaperswasappraisedbyEMusingstandardcriteria(CONSORTand
STROBE) to assess quantitative study quality [11, 12] and the Critical Appraisal Skills Programme
(CASP)checklist[13]fortheappraisalofqualitativeevidence.
COMPONENT2:INTERVIEWS
Weconductedninein-depthinterviewswithfamilieswhohavehadthelivedexperienceofreceiving
DNandconductedanadditional12interviewswithprofessionalswhohavedeliveredDNtofamilies.
Thesamplesizeforinterviewswaspragmaticandwaslargeenoughtoallowfordata[14].HCPswere
recruitedfromNHSTrustssupportedbyHEEKSSacrossKent,SurreyandSussex.Emailinvitationsto
participateintheinterviewsweresentoutviaHEEnetworks(suchasHeadsofMidwifery)topasson
toalleligiblestaffmemberswhoareinvolvedinthedeliveryofDNtofamilies.Interestedparticipants
contactedtheresearchteamdirectlyandthosewhofulfilledinclusioncriteriawererecruitedintothe
study.
Familieswere recruited from the Kent CommunityHealthNHS Foundation Trust (KCHFT) - Health
Visiting Serviceaswell as fromvarious charitiesnamelyUnique, 21&co, and theCornwallDown’s
SyndromeSupportGroup.Familieswererecruitedusingflyersortheparticipantinformationsheet
distributed during their usual meetings, usual communication updates or usual scheduled
appointmentsbyrepresentativesfromthecharitiesorbytheHCP.Familieseithercontactedthestudy
teamdirectlytoparticipateintheinterviewsorcontactedthepersonwhohaddistributedtheflyerto
registertheirinterestinparticipatinginthestudy.
Twointerviewguidesweredevelopedbasedontheliteraturereview,oneforfamiliesandtheother
6
forHCPs.TheinterviewsexaminedtheprocessofreceivingorDDN,whatwentwellandwhatcould
havebeenimprovedon.Theyalsoidentifiedperceivedtrainingneedsandpossibleinterventionsto
address the identified challenges. Interviews with HCPs were conducted over the phone while
interviewswithfamilieswereconductedfacetofaceatamutuallyconvenienttimeandplace.Both
HCPsandfamilyinterviewslastedbetween45minutesandanhour.
COMPONENT3:DEVELOPMENTOFTHETRAININGINTERVENTION
AtraininginterventiontoimprovethedeliveryofDNrepresentsacomplexinterventionasdefinedby
theUKMedicalResearchCouncil(MRC).Acomplexinterventionisonethathasanumberofseparate
elementswhich seem essential to the proper functioning of the intervention although the active
ingredient of the intervention that is effective is difficult to specify [15]. Evaluating complex
interventions requiresa stagedprocessasoutlined in theMRC’s Framework for theevaluationof
complex interventions. A critical first step is to establish the evidence base for the proposed
intervention and its underlying theoretical basis [15]. Second is to pilot and determine the
acceptabilityandfeasibilityofbothinterventiondeliveryandtheproposedevaluationmethods.The
process is iterative feedback into strengthening the intervention, its delivery and the evaluation
process.ThedevelopmentoftheinterventionfollowedtheabovementionedMRCguidanceincluding:
• QualitativedatatoascertainthebarriersandfacilitatorstotheeffectivedeliveryofDNwith
parentsaswellashealthcareprofessionals.
• Extensiveliteraturereviewstoexaminethefactorsaffectingdeliveryofdifferentnews;the
acceptabilityofvarioustraininginterventionsandtoidentifythecorecomponentsofhowto
breakDNsensitivelyandidentificationofsuitabletheorytounderpintheintervention.
• Seekingconsensusfromresearchteammembersandexpertsinthefield.
Tomitigatethecomplexityinherentindevelopinganinterventionaimedatchangingclinicalpractice
wefollowedasystematicfourstepapproachtointerventiondevelopmentdrawingonthebehaviour
changewheel[16].Useoftheorytounderstandthemechanismsofactionofinterventionstrategies
has been shown to improve their effectiveness [16]. The Behaviour Change Wheel (BCW) is a
theoretically driven framework designed to enable the systematic development of interventions
supportingthechangeofpracticebyHCPsandhasbeenusedextensivelyforthispurpose[16-19].It
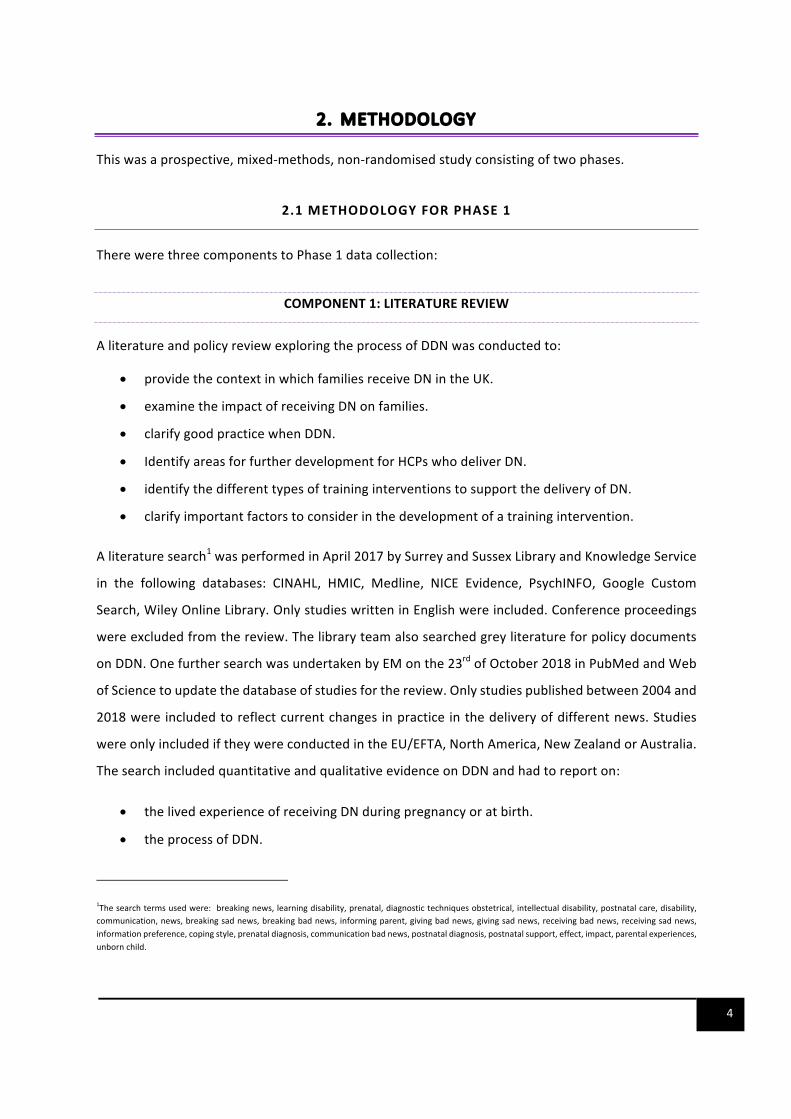
consists of multiple models of behaviour and is underpinned by the Capability, Opportunity,

7
Motivation-Behaviour(COM-B)modelwhichpositsthatchangeinbehaviourorpracticeisaffectedby
capability,opportunityandmotivation[16]asshownbelowinfigure1below:
FIGURE1:COM-BMODEL
Source [16]
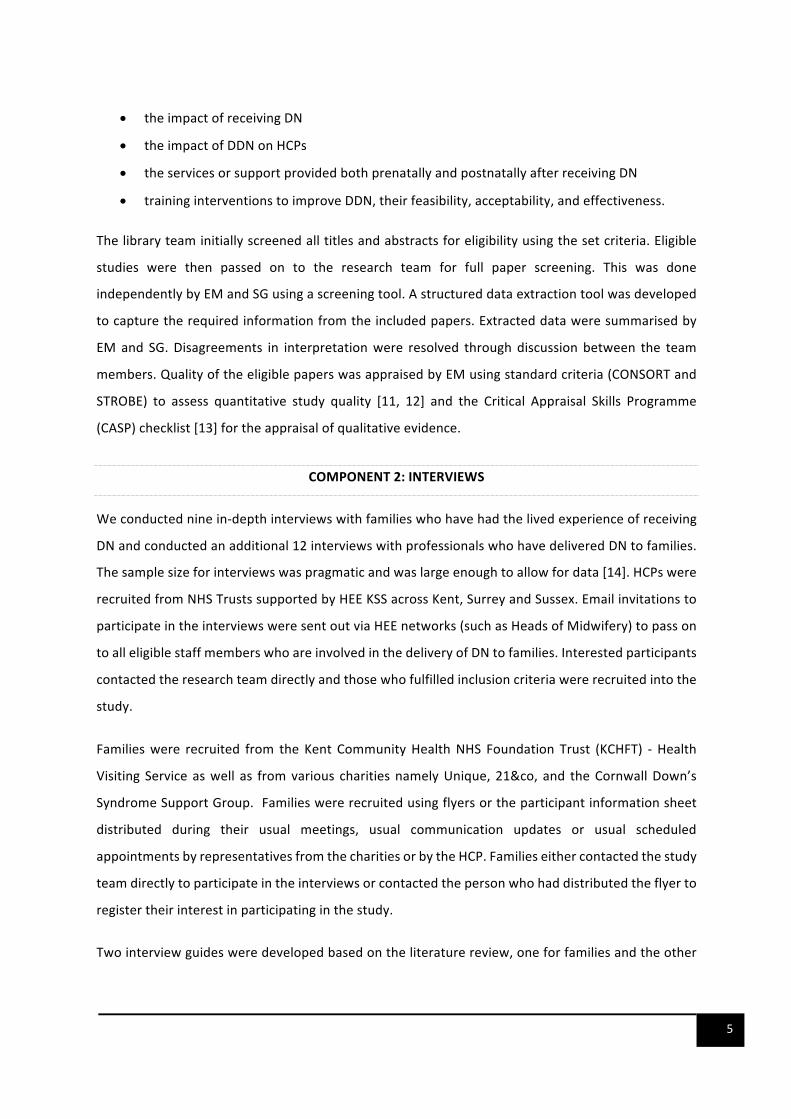
The COM-B model can be subdivided into fourteen constructs within the Theoretical Domains
Framework (TDF) [16, 20, 21].Mapping barriers to change in practice onto the TDF is useful for
identifying barriers and facilitators that need to be addressed to achieve behaviour change. The
differentdomainsareshowninfigure2.TheCOM-Bprovidessupportforappropriate intervention
functionsandbehaviourtechniquesbasedonthebehaviourchangetechniquetaxonomy[22].
FIGURE2:THEORETICALDOMAINSFRAMEWORK
Source [20]
8
ThetraininginterventionwasimplementedinPhase2ofthestudy.Therewerethreecomponentsto
Phase2datacollection:deliveryofthetrainingintervention;administrationofpreandpost-training
questionnairesandinterviewswithasmallgroupofHCPsamonthafterattendingthetraining.
COMPONENT1:DELIVERYOFTHETRAININGINTERVENTION
Invitations toparticipate inahalf-day trainingworkshopwere sentout to staffwhodeliverDN in
variousNHSTrustssupportedbyHEEKSS.ThetrainingtookplaceinCrawleyandCanterbury.Asthis
aspectofthestudywasapilot,itwasnotpoweredtodetectstatisticalsignificance.Werecruited26
HCPs in total. This sample size was pragmatic. Recommendations for pilot and feasibility studies
proposeexaminingchangesinagroupof24to50subjectsinordertoestimateparametersforafollow
onrandomisedcontroltrial[23-25].
COMPONENT2:QUESTIONNAIRES
All participants who took part in the training were asked to complete the pre and post-training
questionnairesonskills,knowledge,andattitudesrelatedtoDDN.Thepost-trainingquestionnaires
alsosoughtqualitativefeedbackonthestrengthsandpossibleimprovementstothetraining.
COMPONENT3:INTERVIEWS
Aspartofthetraining,participantswereaskedtoregistertheirinterestinparticipatinginqualitative
interviewsamonthafterthetraining.Interviewsaimedtoexploreperceivedchangesinknowledge,
attitude,andpracticesafter thetrainingaswellas toobtainadditional feedbackontheperceived
strengthsandlimitationsofthetraining.Thetelephoneinterviewswereconductedusinganinterview
guide and lasted between 25 and 45 minutes. The interviews were all audio-recorded, then
transcribed.
2.3DATAANALYSIS
AllqualitativedataweremanagedusingNVivoandanalysedusingFrameworkanalysis[26]guidedby
theTheoreticalDomainsFramework (TDF) [20,21].Frameworkanalysisbeginswith familiarisation
withthedata,followedbythedevelopmentofathematicframeworkwhichwillbeusedforindexing
thedata[26].Thiswillbefollowedbychartingthedataandthenmappingandinterpretationwhich
allows the development of descriptive and explanatory findings [26]. Thesewere illustrated using

9
various anonymised quotations. Pseudonyms were used to protect the identity of families that
participatedinthestudy.
Thepilottrainingwasnotpoweredtodeterminetheeffectivenessoftheinterventionbutwasused
todetermineparameterssuchasacceptabilityandfeasibilitythatareusefulforafuturelargerstudy.
Acceptabilitywas assessed by the number ofHCPswho attended the full training. Feasibilitywas
measuredbyassessing thepercentageofeligibleHCPswhoeventuallyenrolled in the training.All
secondaryoutcomemeasureswere summariseddescriptively. Categorical dataweredescribedby
countsandpercentagesasappropriate.AllanalyseswerecarriedoutinSPSS.
3.LITERATUREREVIEW
3.1POLICYREVIEW:GUIDELINESONTHEDELIVERYOFDN
Our policy review aimed to summarise current guidelines, policies and or protocols around the
deliveryofDNintheUK.WefoundfourguidelinespublishedbetweenJanuary2004andFebruary
2017. One was developed by a charity, another by a professional organisation and two were
developedbyNHSTrusts.
ContactaFamily,publishedguidelinestoassistHCPsworkingwithfamilieswithachildwithadisability
in 2006 [27]. The guidelines focus on assisting HCPs to provide meaningful support to families
followingthediagnosisofadisabilityfrompregnancytopre-schoolage.Theguidelinesalsoprovide
briefsuggestionsonhowtodeliverDN[27].Astheresourcewaspublished12yearsago,someofthe
informationfromtheresource,forexample,thesourcesofsupportcitedarenowoutdated.Other
guidelineswerepublishedin2013bytheRoyalCollegeofNursing(RCN)tosupportdeliveryofDNto
parentsbynurses,midwivesandhealthvisitors[6].Theseguidelinesoutlinetheapplicationofthe
RCNprinciplesofnursingpracticetoDDNandsuggestaframeworkforhowthiscanbedoneusing
the SPIKE (setting, perception, invitation, knowledge, empathise) Protocol [28] and the ABCDE
(advance preparation, build a therapeutic relationship, communicate well, deal with patient and
familyreactions,encourageandvalidateemotions)model[29].Theauthorsalsoacknowledgedthe
importanceofcontinuousprofessionaldevelopmentincommunicationskillsforHCPsandhowthis
canhaveapositiveimpactonfamilies[6].However,theguidelineswhilstcomprehensive,donothave
a complementary training intervention to equip HCPs how to translate the guidelines into their
everydaypractice.

10
WeretrievedlocallevelguidelinesforDDNfromtheRoyalCornwallNHSTrust(RCHT)andtheNorfolk
andNorwichUniversityHospitalNHSTrust(NNUH)[30,31].RCHThaveguidelinesonDDNtochildren,
youngpeople,andtheirfamiliesbasedonsomeoftheprinciplesfromtheSPIKESprotocol[28,31].
NNUHguidelinesarebasedonrecommendationsfromtheRightFromtheStartcampaignwhichwas
aimedatsupportingmeetingtheneedsofdisabledchildrenandequippingprofessionalsworkingwith
familieswithchildrenwithdisabilities[30].BothNHStrustguidelinesprovidesuggestionsonhowto
deliverDNincludingpossiblephrasesthatcanbeusedbyprofessionals.However,wewereunableto
findanydataontrainingrelatedtotheseguidelinesorthepossibleeffectoftheguidelinesontheself-
efficacyofHCPswhodeliverDN.Thedifferenceinthetwoguidelinesalsosuggeststhattheremaybe
variationinhowDNisdeliveredbetweentrusts.
3.2RESULTSOFLITERATUREREVIEW
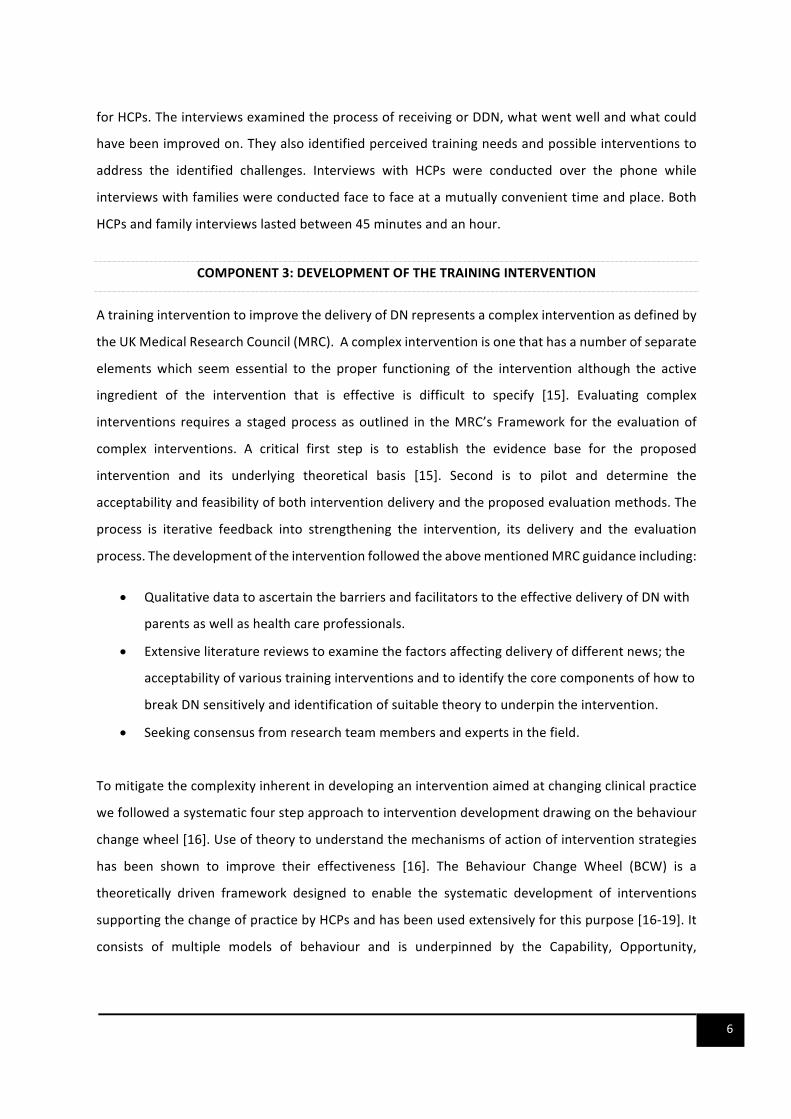
Over10002articleswereretrievedfromtheinitialsearchbythelibrary.Afterremovalofduplications
andscreeningof titlesandabstracts,37paperswere identifiedaseligible for fullpaper screening
throughtheinitialsearchandtheadditionalsearchbyEM.Fourteenpaperswereexcludedafterfull
paper screening because they were not in English (n=2), were inappropriate publications (n=6),
excludedpopulations(n=6).Figure3containsaflowchartofthestudysearchandselectionprocess.
23studieswereselectedforinclusionintheliteraturereview.Thesearedescribedintable1.
2 This numberisanestimate is based on documents from the library on the search processes.

11
FIGURE3:FLOWCHARTOFTHESTUDIES
Identification Recordsidentifiedthroughdatabase
n>1000
Eligibility
Fulltextarticlesassessedforeligibility
n=37
Included
Studiesincludedinthereview
n=23
Recordsidentifiedthroughdatabasesearch
n>1000
Screening
Recordsexcludedfornotmeeting
inclusioncriterian>963
Fulltextarticlesexcludedn=14
notbeinginEnglish(n=2),
inappropriatepublicationtype(n=6),
irrelevantpopulation(n=6)

12
TABLE1:DESCRIPTIONOFSTUDIES
Author Year Country Objectives Methods Population Mainresults
[32] 2018 Spain Toexaminethehealthcareprovidedtopregnantwomenwhosefoetuseshavecongenitalanomaliesandtofacilitatethedesignofamorepersonalisedhealthmodel.
Qualitative 22obstetricians,4midwives,3nurses,8nursingassistants
HCPsacknowledgedtheneedforsensitivitywhenDDNandtailoringinformationgivingtotheneedsofthefamily.HCPsindicatedalackoftrainingincommunicatingDNandhowthiswasoftenlearntbyobservingothercolleaguesorstandalonecommunicationseminars.
[33] 2018 Norway Toexploreobstetricians’experiencesandviewsoftheuseofobstetricultrasoundintheclinicalmanagementofpregnancy.
Qualitative 20obstetricians DDNwasdescribedasaverydifficultaspectoftheobstetricians’work.Obstetricianshadtobalancethemedicalandsocialaspectsoftheultrasoundexaminationwhendeliveringdifferentnews.
[5] 2017 Europe,USA,Australia
Explorethepsychologicaleffectsofaprenataldiagnosisofafoetalanomalyonexpectantparents.
Literaturereview
N/A ImpactofreceivingDNonparentsisdiscussedaswellasexperiencesofHCPs.
[34] 2017 USA Todescribeatrain-the-educatorworkshopaimedtoteacheducatorshowtocreateandconductworkshopsonfacilitatingdifficultfamilyconversationsthattargettheirownlearners'needs.
Reviewandpost-trainingevaluation
14HCPsworkinginneonatology,generalpaediatrics,criticalcare,palliativecareandothersub-specialtiesinpaediatrics
TheauthorsoutlinedhoweducatorscandevelopworkshopsonDDNusingsimulation.86%ofattendantsplannedtousetheskillsfromtheworkshopinthedevelopmentoftheirowncurriculum.
[35] 2016 USA TooutlinetheimportanceofprovidinguptodateinformationtoparentswhentheydeliverDNonDown’sSyndrome
Review N/A Theanticipatedoutcomesofaconditioncanchangesignificantlybasedonavailablesocialsupport,healthcare,andserviceshenceitisimportantforclinicianstostayup-to-dateaboutnewdevelopmentsandcredible,medicallyreviewedinformationaboutDownsyndromeandothergeneticconditions.
[36] 2016 USA Todiscusstheuseofcollaborativereflectivetrainingforbreakingbadnews.
Literaturereview
N/A. Descriptionofthecollaborativereflectivetrainingandhowthiscanbeadoptedbythosedevelopingtrainingondeliveringdifferentnews.

13
[37] 2016 USA Toexploreeffectivetechniquesinthedeliveryofdifferentnews
RCT
42participants Bothgroupsreportedimprovementsinbeingabletodeliverbadnewswiththosewhohaddebriefinginsteadofthelectureaftersimulationshowingthegreatestchanges.
[38] 2015 Canada Toenhancecareandqualityofcommunicationbetweenstaffandparentsinaneonatalintensivecareunit.
Literaturereview;Questionnairesandqualitativedata.
Notstated IncorporationofparentexperiencesofcommunicationintheNICUiseffectiveinaddressingchallengesassociatedwithdeliveringdifferentnews.
[39]
2015 USA,Europe
Toexplorethelinkbetweeninformationpreferenceandcopingstyle
Review Thenumberofpapersincludedisnotstated.
Theinformationneedsofparentswhenafoetalabnormalityisidentifiedontheultrasoundarediscussed.
[40] 2015 USA ToprovideaframeworktobreakbadnewsofananomalousfetusforphysicianscaringforpregnantwomenusingtheSPIKESprotocol
Review N/A ShowshowSPIKESprotocolcanbeusedasaframeworktodeliverDNtofamiliesfollowinganultrasoundscan.
[41] 2015 Italy Explorationoftheuseoffilmsasareflectivelearningtoolforemotionalawarenesstoaidthedeliveryofdifferentnews.
Qualitative 9midwiferystudents Participantsidentifiedgoodandpoorpracticeinthedeliveryofdifferentnews.Reflectionanduseofsimulationthroughthecinemawereusefullearningtoolsfordeliveringdifferentnews.
[42] 2014 USA Toevaluateatrainingonsharingoflife-alteringinformation(SLAI)inpaediatrics.
Survey 159pre-andpost-surveyswerecompleted.
Thetrainingimprovedself-efficacyinDDN.Medicaltraineesreportedthegreatestdifferenceinallareas.Thosewithfewerthan16yearsofexperiencehadthemostsignificantself-assessmentincreases.
[43] 2014 Netherlands ToanalysewhichdysmorphicfeaturesaremostrecognisedinnewbornswithDownsyndrome(DS)
ProspectiveCohort
586childrenwithDown’sSyndrome.
AppropriatecommunicationwiththeparentsofthemessagethattheirchildhasDScanbedifficult.Guidelinescanhelptomakecounsellingeasierandmoreeffective,whichinturnmayincreaseparentalsatisfaction.
14
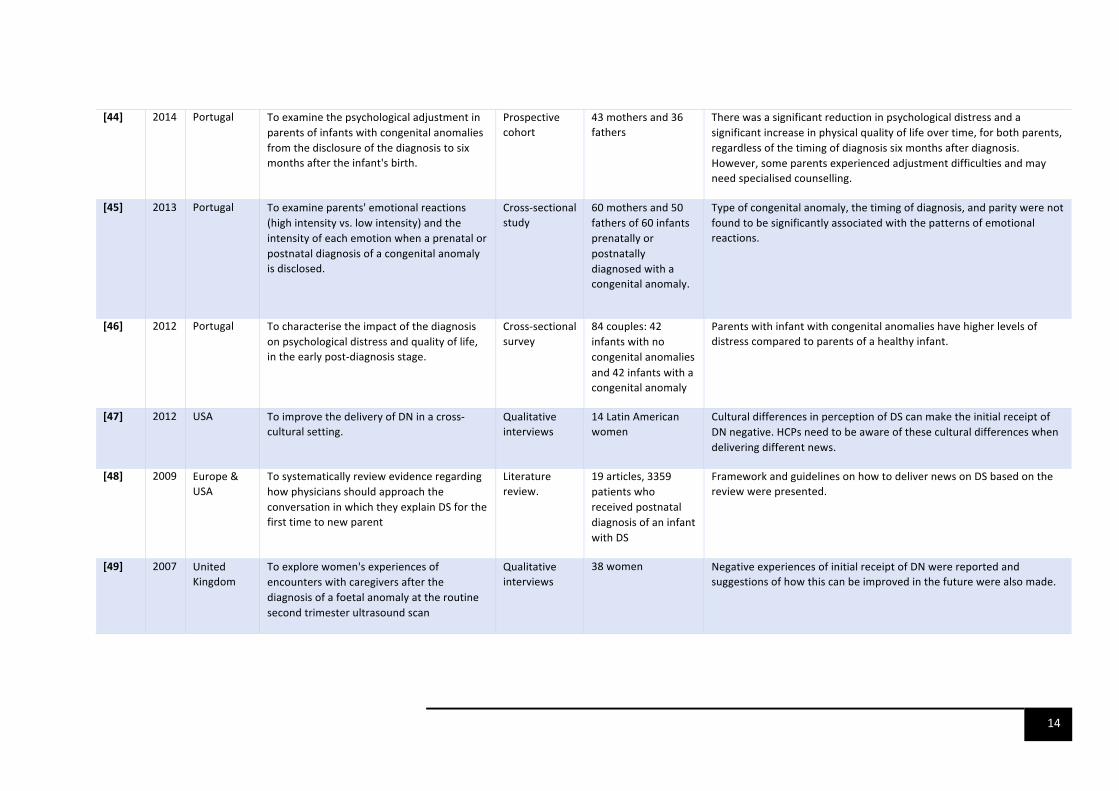
[44] 2014 Portugal Toexaminethepsychologicaladjustmentinparentsofinfantswithcongenitalanomaliesfromthedisclosureofthediagnosistosixmonthsaftertheinfant'sbirth.
Prospectivecohort
43mothersand36fathers
Therewasasignificantreductioninpsychologicaldistressandasignificantincreaseinphysicalqualityoflifeovertime,forbothparents,regardlessofthetimingofdiagnosissixmonthsafterdiagnosis.However,someparentsexperiencedadjustmentdifficultiesandmayneedspecialisedcounselling.
[45] 2013 Portugal Toexamineparents'emotionalreactions(highintensityvs.lowintensity)andtheintensityofeachemotionwhenaprenatalorpostnataldiagnosisofacongenitalanomalyisdisclosed.
Cross-sectionalstudy
60mothersand50fathersof60infantsprenatallyorpostnatallydiagnosedwithacongenitalanomaly.
Typeofcongenitalanomaly,thetimingofdiagnosis,andparitywerenotfoundtobesignificantlyassociatedwiththepatternsofemotionalreactions.
[46] 2012 Portugal Tocharacterisetheimpactofthediagnosisonpsychologicaldistressandqualityoflife,intheearlypost-diagnosisstage.
Cross-sectionalsurvey
84couples:42infantswithnocongenitalanomaliesand42infantswithacongenitalanomaly
Parentswithinfantwithcongenitalanomalieshavehigherlevelsofdistresscomparedtoparentsofahealthyinfant.
[47] 2012 USA ToimprovethedeliveryofDNinacross-culturalsetting.
Qualitativeinterviews
14LatinAmericanwomen
CulturaldifferencesinperceptionofDScanmaketheinitialreceiptofDNnegative.HCPsneedtobeawareoftheseculturaldifferenceswhendeliveringdifferentnews.
[48] 2009 Europe&USA
TosystematicallyreviewevidenceregardinghowphysiciansshouldapproachtheconversationinwhichtheyexplainDSforthefirsttimetonewparent
Literaturereview.
19articles,3359patientswhoreceivedpostnataldiagnosisofaninfantwithDS
FrameworkandguidelinesonhowtodelivernewsonDSbasedonthereviewwerepresented.
[49] 2007 UnitedKingdom
Toexplorewomen'sexperiencesofencounterswithcaregiversafterthediagnosisofafoetalanomalyattheroutinesecondtrimesterultrasoundscan
Qualitativeinterviews
38women NegativeexperiencesofinitialreceiptofDNwerereportedandsuggestionsofhowthiscanbeimprovedinthefuturewerealsomade.
15
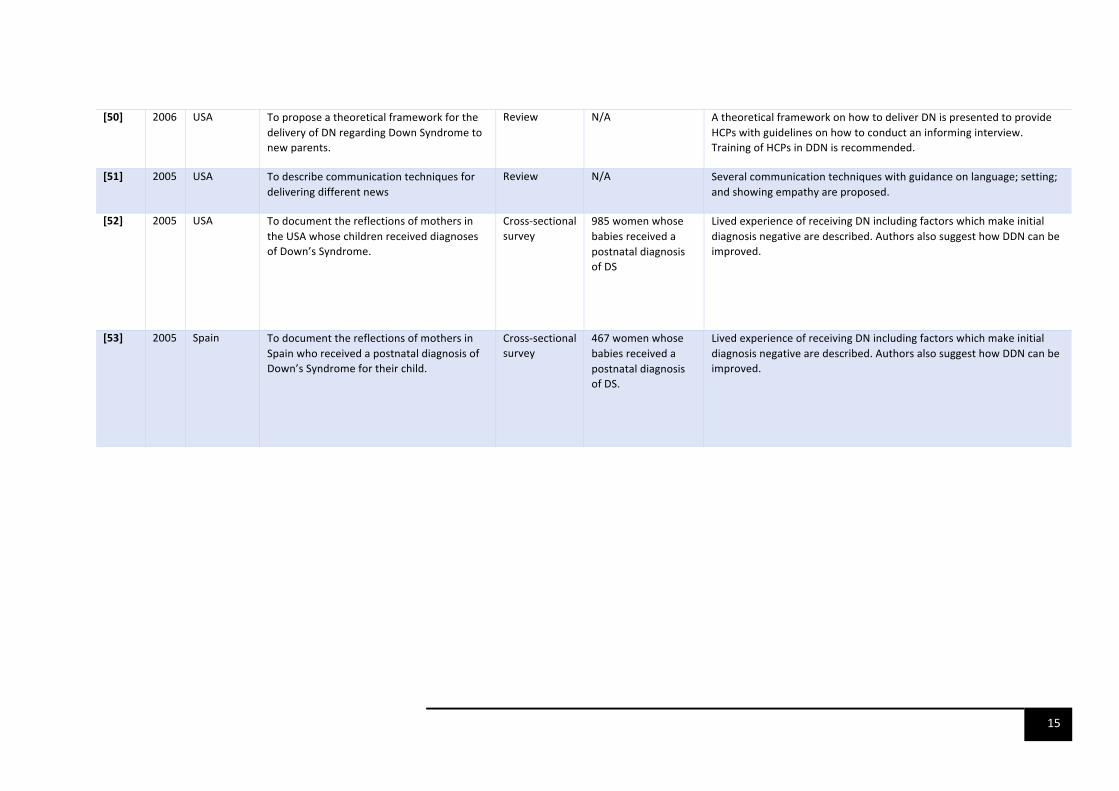
[50] 2006 USA ToproposeatheoreticalframeworkforthedeliveryofDNregardingDownSyndrometonewparents.
Review N/A AtheoreticalframeworkonhowtodeliverDNispresentedtoprovideHCPswithguidelinesonhowtoconductaninforminginterview.TrainingofHCPsinDDNisrecommended.
[51] 2005 USA Todescribecommunicationtechniquesfordeliveringdifferentnews
Review N/A Severalcommunicationtechniqueswithguidanceonlanguage;setting;andshowingempathyareproposed.
[52] 2005 USA TodocumentthereflectionsofmothersintheUSAwhosechildrenreceiveddiagnosesofDown’sSyndrome.
Cross-sectionalsurvey
985womenwhosebabiesreceivedapostnataldiagnosisofDS
LivedexperienceofreceivingDNincludingfactorswhichmakeinitialdiagnosisnegativearedescribed.AuthorsalsosuggesthowDDNcanbeimproved.
[53] 2005 Spain TodocumentthereflectionsofmothersinSpainwhoreceivedapostnataldiagnosisofDown’sSyndromefortheirchild.
Cross-sectionalsurvey
467womenwhosebabiesreceivedapostnataldiagnosisofDS.
LivedexperienceofreceivingDNincludingfactorswhichmakeinitialdiagnosisnegativearedescribed.AuthorsalsosuggesthowDDNcanbeimproved.

16
3.2.1THEIMPACTOFRECEIVINGDN
Regardlessofwhetheradiagnosiswasmadeprenatallyorpostnatally,receivingDNwasreportedas
distressingandunexpectedwithparentsexperiencingvariousemotionssuchasshock,denial,revolt,
anger,guilt,sadnessanddepression[5,33,39,44,45,47-50,52].Somestudieshaveshownaclear
correlationbetweenmaternalanxietyandthefocusoftheinitialconversationwhenHCPsdelivered
DN,thushighlightingtheimportanceofhowDNisdelivered[44,48].Previousstudiesindicatedthat
DNwasalsooftenunexpectedfortheHCPswhichcontributedtodeliveringsuchnewschallenging[5,
50]. However,most parents adjusted to the news over time [44, 47]. A cross-sectional survey of
parentsfoundthatoveraperiodofsixmonths,parentswhowerewellsupportedandhadaccessto
appropriate informationwhen theyneeded it, adjustedwell to thediagnosis; showedpatternsof
resilience;hadreducedsymptomsofanxietyanddepressionandanimprovedqualityoflife[46].
VariousstudiesshowedthatdeliveryofDNintheprenatalperiodhaditsowncomplicationsbecause
parentswereofferedtheopportunitytohaveadditionaldiagnostictestingaswellastheoptionto
terminateapregnancy.[32,39].Physiciansreportedprovidingadiagnosisinthiscontextdifficultdue
tothepressuretomakethediagnosis;makeatimelyreferraltofoetalmedicineandtodiscussthe
optiontoterminatethepregnancy[32,35,39,49].Findingsfromareviewsuggestthatparentsfound
thedecisiontoterminateapregnancybasedonfoetalanomalyscreeningdistressing[5,32,33,39,
49].Insomeinstances,thedecisiontoterminatewasinfluencedbythepotentialchallengesthatthe
childwouldfaceandtheperceivedpotentialdistresswhichsiblings,aswellasparentsthemselves
wouldface[39].Theseverityoftheanomalyaswellasreligionwereimportantfactorsinthedecision
toterminateapregnancyandHCPsneededtobesensitivetothese[39,54].Thepersonalviewsof
HCPs about terminating a pregnancy were reported as having a negative effect on how DN was
delivered[39].Somewomenreportedadeterioration inthequalityof their relationshipswiththe
HCPs after theydecided to continue apregnancywith a significant chanceof physical or learning
disability[39].
WhethertheDNwasdeliveredprenatallyorpostnatally,iftheinitialconversationwasnegativeand
parentswerenotgivenadequatesupport,theinfantwasatincreasedriskofpooreroutcomesdueto
thepoormentalhealthof theparent [46].Chronic stress inparents canadversely affectparental
functioningandtheparent-infantrelationship.Evidenceshowsitcanresultinparentingstyleswhich
17
may impair the social-emotional, cognitive and physical development of children, which in turn,
increasestherisksofmentalillnessacrossthelife-course.[7].Maternalandpaternaldepressionand
anxiety are also known risks for poorer cognitive functioning, impaired adaptive functioning, and
increasedriskofdepression,anxietyandconductdisordersinchildren.[8-10].Theeffectsareknown
tospanfrominfancyintoadolescence[8,55].Inviewofthis,thereisaneedtoensurethatHCPsare
equippedwiththeskillstodeliverDNeffectively.
3.2.2IMPORTANTFACTORSFORDDNEFFECTIVELY
PreviousresearchhashighlightedanumberoffactorswhichimprovetheinitialreceiptofDN[5].One
ofthemostcriticalthingshighlightedbytheliteratureisthetimingofthedeliveryofDN[43,47,50].
Invariousstudies,parentsindicatedtheimportanceofbeinggiventhediagnosisasearlyaspossible
toavoidoverhearingHCPsdiscussingtheirchild’sdiagnosiswithoutthembeingdirectlyinformed[50].
However,thisneededtobebalancedasparentsalsoindicatedtheimportanceofnotdeliveringthe
newswithinsecondsofthebirth,particularlyiftheconditionwasnotperceivedaslifethreatening
[52].
Closelyrelatedtotiming,previousstudiesalsoshowedtheimportanceofensuringthatasignificant
other,suchasaspousewaspresenttoremovetheburdenontheparentwhowasfirstnotifiedhaving
todeliverthenewstotheparentwhowasabsentattheinitialconversation[5,48-50,52,53].One
qualitativestudyfoundthatmothersvaluedthediscussionbeingdeliveredinawaythatinvolvedboth
themand theirpartner in thedecisionmakingabout their child.Not involvingparents indecision
makingwas reported as exacerbating feelings of powerlessness, distress, and loss of control [39].
Furthermore, to give both parents the space they needed to process the diagnosis, express their
emotionsortomakedecisions,itwasimportantthatthenewswasdeliveredprivately.
Thelanguageusedwasofimportancetotheparents[39,48-50,52,53].Severalstudiesreportedthat
parentsdidnotwantHCPstouselanguagetosuggestthatthebirthoftheirchildwasregrettable[39,
48-50,52,53]. Inaddition,parentsdidnotwantthe languageusedtobeoverlytechnical,parents
valuedHCPswhoensuredthattheirmessagewasunderstood.Thiswassometimesaproductofthe
HCPbeingavailabletoanswerquestionsduringorafterthediagnosis[5,50,51].Inaddition,parents
reportedtheimportanceofensuringthattheinitialdescriptionwasbalancedandnotoverlynegative
[5,39,47-49,52,53].Forexample,mothersfromalargecross-sectionalsurveyconductedintheUSA
18
reportedfindingsomeinformationprovidedsoonafterbirth,suchasstatisticsaboutadultobesity,
Alzheimer’s disease, behavioural problems or predicting the level of independence that the child
mighthaveinappropriate[52].Whileparentswantedinformationtobeprovided,HCPsneededtobe
abletogaugehowmuchinformationparentscouldtakeasgivingtoomuchinformation,particularly
ifitwasnegative,exacerbatedanxietyandordepressioninparents[35,48].
SeveralresearchershavepublishedframeworksandguidelinesonhowtodeliverDNduringpregnancy
or the neonatal period based on primary research or literature reviews [39, 48-50, 52, 53]. The
frameworksemphasisethefactorshighlightedabovebutalsoprovideusefulsuggestionsonwhenand
howtobreakthenews;theimportanceofverbalandnon-verballanguagewhendeliveringdifferent
news;theimportanceofcommunicatinginarespectful,sensitiveandnon-judgementalmannerto
parents;listeningtoparentsandmakingjointdecisionsaboutcare;beingempathetic;theimportance
of providing timely supplementarywritten information and followon support [39, 48-50, 52, 53].
Other authors have looked at the specific needs of ethnic minority women and provided
recommendationsondeliveringnewsinthecontextofdifferentreligiousandculturalbeliefs.[47].
3.2.3TRAININGINDDN
The literature search did not retrieve any studies on training to deliver DN specific to congenital
anomalies associated with a learning disability prenatally or at birth. However, we were able to
identify somestudieson training todeliverDN inmidwifery,paediatricandobstetric settings.We
excludedstudiesthatonlyreportedonspecificsub-specialties,forexample,paediatriconcologyand
only includedstudiesontrainingwhichwereapplicableacrossthespecialitiesastheseweremore
relevanttothedevelopmentofthetraininginterventionforthisstudy.
There is recognitionthatDDNmaybedifficultandstressful forHCPsandthatoftenHCPs lackthe
trainingtobeabletodeliverDDNnewswell[5,34,42].ManyHCPshavelearntDDNfromthe“see-
one-do-one”approachthatislimitedbecauseofthevariationintheskillsoftheseniorHCPobserved
byjuniorcolleagues[32,36].Simulations,reflectivepractice,debriefing,andlectureshavebeenused
toteachHCPshowtodeliverDNinthepaediatricandobstetricsettings[36-38,41].Simulationsmay
takedifferentformsincludingroleplaysandtheuseofnarrativesorvideosofthelivedexperienceof
receivingDNtoenableHCPstoidentifywiththeemotionsexperiencedbyparents.Inonestudy,the
research team developed a training on DDN in paediatric populations by modifying the SPIKES

19
protocoltoreflecttheneedsoftheirpatientpopulationandexperiencesofparents[42].Thetraining
improvedtheself-efficacyofHCPsinDDNparticularlythosewhohadbeenpractisingforlessthan
16 years [42]. Similar findings were also reported in a randomised control trial comparing the
effectivenessofsimulationcombinedwithlectureandsimulationfollowedbydebriefingonimproving
theDDN skills ofHCPs [37]. The knowledgeand skills improved for all participantsbut simulation
followedbydebriefingweresuperiortothelecture.Akeypointidentifiedbytheresearcherswasthe
importanceoffollowupoftraineesinretainingtheskillsobtainedfromthetraining[37].
This approachwas also advocated for by a groupof researcherswhodeveloped a framework for
communicating DN in the neonatal unit [38]. The training involved the use of videos, role plays,
pictures and narratives from parentswith the lived experience of receiving DN. The trainingwas
coupledwithorganisationalchangessuchasthedevelopmentofcommunicationguidelinesforHCPs
to follow, regular follow-upof trainees;protocol and familymeeting templates inwhich feedback
fromfamilieswascollected[38].Althoughthetrainingwasverywellreceivedbythedifferenttypes
ofHCPsworkingintheneonatalunit,therewerenopre-andpost-trainingdatacollectedwhichwould
havebeenusefulforunderstandingtheeffectofthetrainingonself-efficacyofthetrainees.However,
thetrainingcontentreflectedsomeoftheissuesthathavebeenidentifiedinearliersectionsasbeing
importantforthedeliveryofDN.
3.3CONCLUSION
TheliteratureindicatesthesignificantimpactofreceivingDNontheemotionalandmentalwellbeing
ofparents.TheprocessofDDNmaybechallengingforHCPsparticularlyassomemayhavelimited
trainingonhowtodeliverdifferentnews.Asignificantproportionoftherecommendationsonbest
practiceforDDNwerebasedontheexperiencesreportedbyfamiliesandonlythreestudiesreported
theexperiencesofHCPs.ThereisneedtogathermoreevidencefromHCPswhodeliverDNontheir
perceivedtrainingneeds;whatcurrentlyworkswell inpractice;howthiscanbeimprovedandthe
necessaryorganisationalchangestosupporttheeffectivedeliveryofDN.Inaddition,thereseemsto
be a gap between evidenced-based guidelines on DDN and their implementation into policy and
practice.ThisisalsoreflectedinthefactthatweonlyfoundpublicationsfromtwoNHStrustswhich
maysuggestvariationinthedeliveryofDNacrossNHStrusts.Thereviewalsosuggeststheimportance
ofdevelopingtrainingwhichreflectstheevidenceavailableonbestpracticesupplementedbyprimary

20
datafromfamiliesandHCPsintheUKasweonlyfoundoneUKstudytoincludeinthisreview.This
approachwouldensurethat thetrainingreflects theUKcontext.Trainingcould involvetheuseof
simulationsothatHCPstohaveasafeplacetolearnandpracticeDDN.
21
4. PHASE1FINDINGS
4.1DESCRIPTIONOFPARTICIPANTS
Weconductedinterviewswith12HCPswhodeliverDNonaregularbasisand9parentsofchildren
whoreceivedDNduringpregnancyoratbirth.TheprofessionalbackgroundoftheHCP’svariedand
includedmidwifery,nurses,registrars,andspecialistconsultants.6outofthe9parentshadchildren
with Down’s Syndrome and three had rare chromosomal disorders. A breakdown of the family
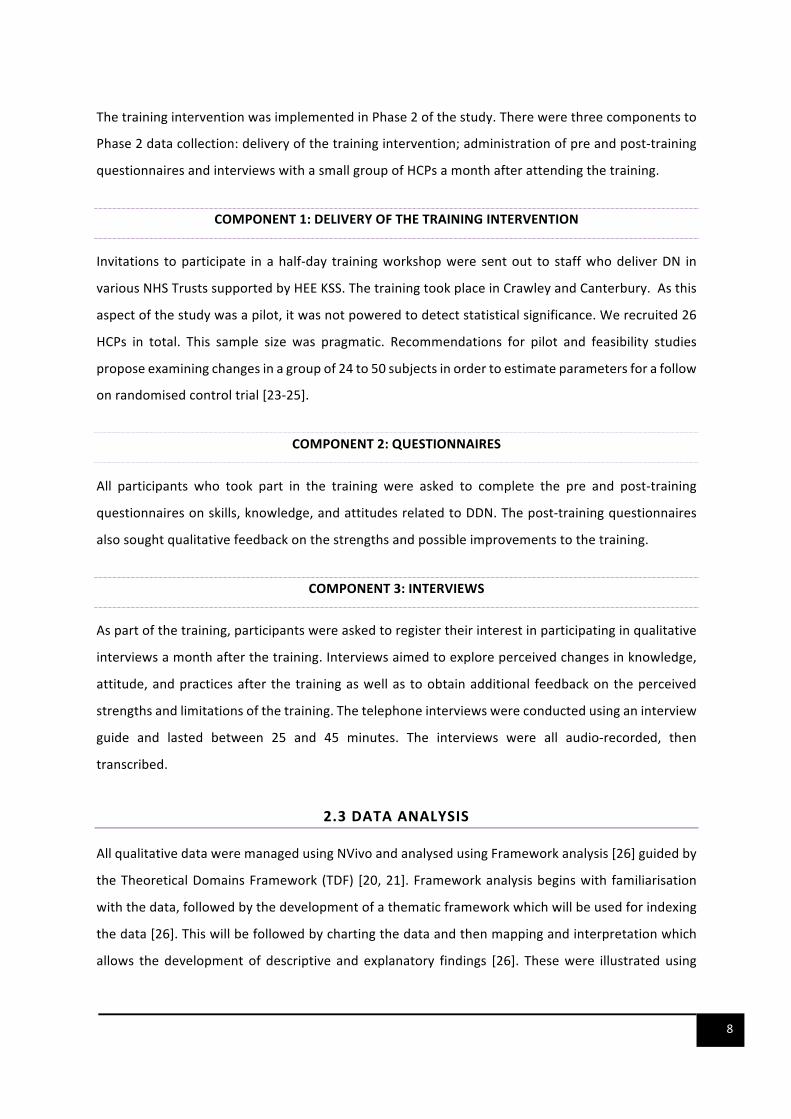
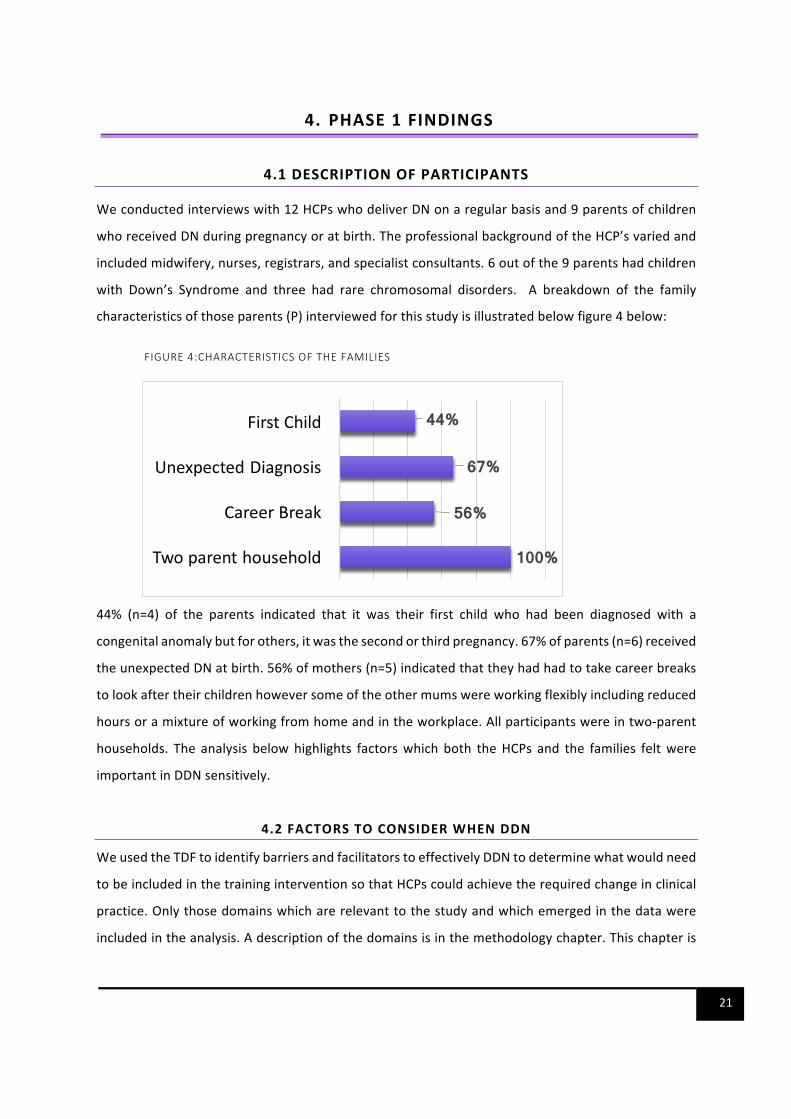
characteristicsofthoseparents(P)interviewedforthisstudyisillustratedbelowfigure4below:
FIGURE4:CHARACTERISTICSOFTHEFAMILIES
44% (n=4) of the parents indicated that it was their first child who had been diagnosed with a
congenitalanomalybutforothers,itwasthesecondorthirdpregnancy.67%ofparents(n=6)received
theunexpectedDNatbirth.56%ofmothers(n=5)indicatedthattheyhadhadtotakecareerbreaks
tolookaftertheirchildrenhoweversomeoftheothermumswereworkingflexiblyincludingreduced
hoursoramixtureofworkingfromhomeandintheworkplace.Allparticipantswereintwo-parent
households. The analysis belowhighlights factorswhich both theHCPs and the families feltwere
importantinDDNsensitively.
4.2FACTORSTOCONSIDERWHENDDN
WeusedtheTDFtoidentifybarriersandfacilitatorstoeffectivelyDDNtodeterminewhatwouldneed
tobeincludedinthetraininginterventionsothatHCPscouldachievetherequiredchangeinclinical
practice.Onlythosedomainswhicharerelevanttothestudyandwhichemergedinthedatawere
includedintheanalysis.Adescriptionofthedomainsisinthemethodologychapter.Thischapteris
100%
56%
67%
44%
Twoparenthousehold
CareerBreak
UnexpectedDiagnosis
FirstChild
22
interspersedwithrecommendationsforwhatshouldbeincludedinthetrainingasthiswasthemain
objectiveoftheinterviews.
4.2.1SOCIAL/PROFESSIONALROLES
This domain referred to the professional roles and boundaries of HCPs involved inDDN. Care for
mothersduringpregnancyandafterbirthwasprovidedbymultidisciplinaryteamswitheachteam
member having specific roles and professional boundaries. In the context of DDN, sonographers
identifiedconcernsaboutababyduringultrasoundscreening:
So, she's (sonographer), like "Oh, I need togoandgetadoctor",and therewasa shadow,ablack
shadow,that'salltherewas….".(Parent3)
She(sonographer)actedasusualandshedidn'treact,youknow,like,oh,anythinglikethat,butatthe
endshesaid,"Isawsomethingthat'snotquiteright,but Ican'tsayanything,so Ihavetospeakto
the...tospeakthedoctor",Isupposetheobstetrician,Ican'trememberum,"...andI'llletyouknow".
So,shewentout…andthenshecameback….andthenshesaid,"Yes, ifyoucancomebackatone
o'clockorsomething".(Parent4)
Midwivesidentifiedconcernsaspartoftheearlybabycheckoriftheyworkedasscreeningmidwives
thishappenedaftertheyreceivedtheresultsofthecombinedscreeningtestfromthelaboratory:
So,IwasinthemiddleofworkandmyphonewentsoIimmediatelyanswereditthinkingthatitwasan
[emergency],anditturnedouttobesomebodyfromtheNHS,whowantedtospeaktomeaboutmy
testresults.So,Istoodoutsidetheofficetotalktothem,andtheyimmediatelysaid,‘yourtesthascome
backwithaoneintwentyriskfactor,weneedyoutocomeintothehospitalassoonaspossible',which
didputmeintoabitof[laughs]apanic!(Parent9)
Inthecaseofthesonographers,whenanyanomalieswereidentified,professionalboundariesmeant
thattheyreferredthefamiliestothedoctortodiscussthefindingsandestablishadiagnosis.When
theresultsweredeliveredbythescreeningmidwivesoverthephone,afollowupemailwassentto
theparentsandtheywereinvitedtomeetwiththerespectivemidwifeattheirearliestconvenience
todiscussthemeaningofthescreeningresults;receivereferraltootherrelevantdepartmentssuch
as foetal medicine or to arrange for confirmatory tests or in some cases discuss the options of
continuingorterminatingthepregnancy.
23
Often,itwastheconsultant’sresponsibilitytoestablishthediagnosisandcommunicatethistothe
parents either during pregnancy or shortly after birth. Parents indicated that confirmation of the
diagnosiswasgivenaftertheresultsofthekaryotypingorotherrelevantinvestigations:
Youcan’tsay,yes,yourbabyhasDown’s,untilthechromosomaltestisbackandthat’squitedifficult
becausetheparentswantadefiniteandyoucanonlysayit’ssuspiciousofandthatsortofthingandI
personallyfoundthatquitedifficult.(HCP1)
Several parents indicated that they respected the opinion of their HCPs and particularly held the
consultantsinhighregard:
Whensomeoneinamedicalpositionlikethattellsyou,youtendtobelievethem.(Parent1)
Inviewofthis,parentswhowereunsureaboutterminatingapregnancyaskedtheirHCPsaboutwhat
theywoulddo if theywere inthesamesituation. Itwastherefore importantforHCPstousethis
positionalpowertosupporttheparentsnomatterwhattheydecided.Itwasnotjustwhattheysaid
whentheydeliveredtheDNthatparentsfeltwasimportantbuthowtheysaidtheinformationaswell
ashowtheytreatedtheparentsiftheirdecisionwascontrarytotheclinicians’expectations.
Given that often themedical conditionwas new tomost parents; parents relied on theHCPs for
accurateuptodateinformationaboutthemedicalconditioninquestion.Participantsfeltthatitwas
important for HCP’s to demonstrate a level of professionalism by preparing adequately before
communicatingnewsaboutacondition to families.BothHCPsandparents felt that the informing
clinician needed to be knowledgeable about the condition and if they were unfamiliar with the
conditiontherewasanexpectationforthemtohavesomebasiclevelofself-educationinanticipation
ofthequestionswhichcouldbeaskedbyparentsratherthanexpectingthemtofindoutanswerson
theirown:
Hegaveusaprint-outofthediagnosis,whichEzekiel’sisaduplicationonpartofhisChromosome-
XXX,ithasn’tgotabrandname,it’sjustalotofnumbersandmeantnothingtousbasically.Hesaidto
usthathe’donlyhaditthroughrecentlyviafax,hadn’thadachancetolookatthediagnosisreally
himself,didn’treallyknowmuchaboutit,andgaveusaleafletofacharity….andprettymuch,we
werelefttogoogleit.(Parent2)
24
Ithinkit’slikeyouasaclinician,ifyou’reprepared…beforeyouseethepatient,soyouare,likeyou’re
abletoanswertheirquestionsaboutlikewhat’sthemeaningofchromosomes,erm,orlikewhat’sthe
mean…whatinvestigationswilltheyhavetohaveorwhat,whatcomplicationsdoesitmean.(HCP3)
Itwasclearinthedatathatconsultantsandotherseniorclinicianshadtheprofessionalresponsibility
toprovidejuniorstaffwiththeopportunitytolearnfromtheirpractice.However,therewassome
suggestionforthisaspectoftheprofessionalroletobebalancedwithsensitivitytotheneedsofthe
families.Forexample,oneparentfeltthattheincessantvisitstoexaminethemandtheirbabybythe
consultantandthemedicalstudentsmadethemfeel liketheywereacasestudyandtheydidnot
wanttobeone:
Shewasdoingthescanandthenshewasshowingthestudentslike,youknow,thisismytummy,and
shewentlikethat[demonstratestointerviewer]andtellingthem,thisis,youknow,eyesorlegsor,and
shewasdescribingmybaby,itwasmybabyandshewasspeakinglike,Idon'tknow,anobjectthere.
AndwhenIexplainedtothemidwife,Isaidtoher,"Look,Iunderstand….whenit'sacaseyouwillstudy
thecaseandit'sinteresting,butI'mnotacaseandmybabyisnotacase….(Parent4)
Intermsofsocialandprofessionalroles,itwouldbeimportantforthetraininginterventiontosupport
thefactthatcareisdeliveredbyamultidisciplinaryteamandemphasisethevalueofthedifferent
professionalsandtheirspecificroleinthedeliveryofDN.Itwouldbeimportanttoalsoidentifyways
to improveeachaspectof theprocess fromthetimethatconcernsareraisedto thetimethatan
officialdiagnosisisprovidedbyrecognisingthatthesearenotdiscreteeventsbutareallpartofthe
processofDDN.
4.2.2KNOWLEDGE,SKILLSANDBELIEFSABOUTCAPABILITIES
ThisdomainreferredtotheperceivedknowledgeandskillstodeliverDN.Experienceandcompetence
weredescribedbyparticipantsasfactorswhicheitherenabledorhinderedeffectivedeliveryofDN.
A. EXPERIENCE
AlackofexperiencewasperceivedasoneofthemainbarrierstoeffectivelyconveyingDNbyHCPs:
Themoreopportunitiesyouhavetobreaknewslikethis,Ithinkthemoreer,themorecomfortableyou
becomeatchangingyourapproachduringtheconsultation,asajunior,youare,it’sveryeasytobecome
tongue-tiedbecauseyoujustdon’twanttosaythewrongthing…(HCP10)

25
Reading the triggers, reading,becausesomuchof it focussesonsortofwatchingand listeningand
observing,um,andjustkindofpickinguponcueswhichIguessonlycomeswithexperience.(HCP12)
TheabovediscoursessuggestthatthemoreexperienceaHCPhadatDDNthemorelikelyitwasthat
they improved their techniqueat this importantaspectof their job.AlthoughHCPs indicated that
experiencewasanimportantaspectofbeingabletodeliverDNeffectively,thedataalsoshowedthat
evenamongthemostexperiencedintermsofyearsofpracticeorclinicalranking,therewassignificant
variationinhowDNwasdelivered.SomeseniorcliniciansweredescribedasbeingverygoodatDDN
wellandothersweredescribedasneedingtoimprovehowtheydeliveredDN.
B. COMPETENCE
HCPs often indicated that they had received communication training either as part of their
undergraduateorpostgraduatetraining.Thiswasoftendescribedasgenericcommunicationtraining
withasmallcomponentofdeliveringdifficultnews.OnlyoneparticipantindicatedattendingaDDN
coursewhichwasofferedaspartofmandatorytrainingbythedeanerythatwasprovidingthemwith
postgraduatetraining.AcquisitionofknowledgeandskillsonDDNwasgenerallybasedonobserving
moreseniorcolleagues:
We all do this based on, on experience, although there are breaking bad news courses, we don’t
encouragejuniordoctorstojustdotheconsultationontheirown,sowhathappens…the,thewaythe
trainingworksistheycomewithaconsultant,sowhenwearedoingtheconsultationtheycomewith
usandtheyobserveus…(HCP11)
Althoughthisisacommonformoflearninginclinicalpractice,ithadlimitationsiftheseniorclinician
wasnotperceivedasbeingverygoodatDDN.ThisvariationinthestyleofDDNbyseniorcolleagues
mentoringjuniorstaffcouldbeovercomebyhavingstandardisedevidenced-basedguidelines,policies
or protocols. However,most HCPswere not aware of any locally developed policies or protocols
specificallyonDDN:
Ithinkthereprobablyisn'taprotocol,orifthereis,it'scertainlynotevenshowntoanybodyortalked
aboutever.(HCP3)
Idon’tknow,isthere[bothlaugh],wehavehundreds,wehave[bothlaugh],wehave,asyouprobably
knowwehavefrighteningly150,200differentprotocols……andIdon’tthinkI’veseenthatonethere.
ButI’mnotsayingthereisn’tone.(HCP6)

26
NotthatI’mawareof,yeah…...I’mnotawarethatthere’sguidanceinourtrust.Ithinkit’sprobablya
goodideatohavesomeguidance,yes.(HCP1)
Nomatterhowskillsorcompetencewereacquired,allparticipantsfeltthatitwasimportantforHCPs
whodeliverDNtobeadequatelytrainedtodothissensitivelyandtoalsobeabletoprovideeffective
supporttoparentsand/orreferraltoappropriateservices.Participantshighlightedseveralskillswhich
theyperceivedasimportantforDDN.Theseincludedbeingcompassionateandbeingempathetic:
Youcouldtellthathe(paediatrician)genuinelycared,heincludedEzekielintheconversations…Ifind
thatsomepaediatricians,weirdly,arenot[pause]childrenfriendly,strangely,erm,andwilljusttalk
aboutthem,won’tevenreallyacknowledgethemapartfromwhenthey’reexaminingthem.(Parent
2)
Hesatdownwithbothmeandmyhusbandand,and,hewasreallylovelyand,hewasn’tupsetbut
youcouldtellthathe,hereallycaredaboutourlittleboy….hewastheonewho’ddone,he’ddonean
echocardiogramonhimsoheknewthathewasgoingtofacesomechallengesandthathe’dneed,uh,
aheartoperationandhesaidthat,youknow“yourlovelylittleboyisjustgoingtoneedsomeextra
help”and,um,hewas,yeah,hewasjustreallygenuinelycaringand,um,verykindinhowheput,put
thenews.Becauseitis,itisareallyhardthingtotellsomebodythatyourchildhasbeen,thatyoukind
of,alsoIthinkbecausewe’dalreadyotherchildrenandtheywerebornwithoutDown’ssyndromeand
soyou’rekind,whenyou,whenthenextonearrivesandyou’renotexpectingit,itismoreofashockI
think.Soyeah,hewas,hewasreallygreat.(Parent7)
Soshewaskindofsatoveralittlebit,sortofbentforwardandshewastalkingquitequietlytousand
makingsurethatweunderstoodwhatshewassayingatalltimesactually……soIthinkinthatrespect
actuallythewayshewentaboutitwasquite,wasquitegoodyouknow,shemadesureweweresat
down,thatbothmeandmyhusbandwerethereandthatwewerebywheremysonwasaswellsowe
wererightbytheincubatorsowecouldseemysonatthetime(Parent5).
TheaboveparentshighlightedhowthecompassionateattitudeoftheirHCPswhichbalancedbeing
truthful and kind was important when they received their unexpected DN. Participants also
highlightedtheimportanceoftheHCPbeingtactfulintheirchoiceofwordsaswellastheirnon-verbal
languagewhich couldbemisinterpreted for blamingparentsormaking thebirthof their children
regrettable:
27
Andthenthenextdaywehadthemainpaediatrician….oneofthefirstthingshedidwhenhewalked
intheroom,hecameinwithhishandsbehindhisbackwhichwasjustobviouslyhisstature,howhe
walks,andhestoodupstraightandhelookedatmeandhelookedmeupanddown,andthenhesaid,
“Howoldareyou?”andIsaid,“Erm,wellI’m31now,butIwas,youknow,Iwas,youknow…”whatever
agewhenIconceivedorwhat…youknow,IwassortoffeltlikeIwashavingtojustifylike,andthenhe
lookedatmyhusbandandsaid,andlookedhimupanddownandhesaid,“Andhowoldareyou?”and
thenhelookedatmydaughter,andlookedather,andthat,andIwaslike,“Oh,”andthenhesaid,erm,
“Andwhatwasyourscore,whatwasyourscoreforDown’sSyndrome?”andIsaid,“Idon’tknow,they
didn’tgivemeascore,”Isaid,“thatitwasjusthighorlowrisk.”(Parent8)
Theonething,um,itwasn’tgivingbadnewsassuchbuttalkingabout,um,thiswasawoman,ayoung
woman, shewas therewith hermother and partner and she’d got a very small babywith Down’s
Syndromeand,um,sotheyhadcometotalkaboutfurtherscreeningandIsaid,oh,youknow,ifyou
wantanothertestto,um,youknow,findouttheriskofthishappeningagain,andthenofcourse,that
wasit,theconsultationjustprettymuchendedtherewhenthegrandmothersaid,“Well,whyareyou
sayingtheriskofthishappeningagain?Wewouldn’tmindifithappenedagain,thiswouldbeabsolutely
fine.”Um,and,youknow,everythingbrokedownatthatpoint,Ihadtogoandgetsomeoneelsein
becauseI’dsaidthewrongwords…(HCP12)
Insteadofsaying'youhaveaoneinahundredriskofhavingaDownSyndromebaby',we'resupposed
tosay,'aoneinahundredchance'andthat'scomefromapatientwhohassaidthattheword'risk'
hastoomanynegativeconnotations,andIactuallyagreewiththat(HCP3)
Thediscoursesabovehighlighthowtheuseofinappropriatewordsornon-verballanguageaffected
theHCP-patientrelationshipandinsomeinstancesresultedinthedegenerationoftherelationship.
Severalparents felt thathavinga childwithDS shouldnotbeperceivedasanegative regrettable
experiencealthoughtheyacknowledgedthatithaditschallenges.Theyalsofeltitwasimportantto
emphasisethejoythatachildbroughtandnotmerelyfocusonthediagnosis.
TheinterviewsalsohighlightedtheimportanceoftheHCPunderstandingtheimmediatepsychological
and emotional impact of receiving DN on parents. Parents reported having different emotions
includingacceptance,shock,guilt, shameanddeepsorrow.Thesefeelingscouldbefleetingbut in
some instances lasted beyond the hospital stay and even affected the couple relationship or
relationshipswithvariousHCPsforasignificantamountoftime:

28
Paulandmedidn'treallyrespondverymuchtoeachotherforalongtime,eventalktoeachother…..I
had very severe postnatal depression…for probably two years......Paul called it two years of hell
….BecauseeverytimehespoketomeI'deitherbecryingorshoutingorcrying,Ihadababythatwas
coveredin,youknow,thatIwouldhavetochangesix,seventimesadaybecausehewasjustsickallthe
time,anditwasmyfaultbecausemybodydidit.(Parent3)
Socertainlyfor24hourswejustdidn’tknowwhattodowithourselves,wewereliterallyandthenwe
werejustlikewewanttoannouncethatwe’vehadababybutlikehow...Whatdowesay,howdowe
explainthattoeverybody?Um,myhusband,myhusbandtoldorwenttoseemyparentsandtold,told
themandjustfeltawful,youknow,hewaslike,ohIfeel,IfeltbadandIfeltreallyguiltytellingthem
thisandwekindof...Wekindofbothfeltlikewe’ddonesomethingwrong.(Parent5)
ItwaslikeIwasinafilmandallthesethingswerehappeninginfrontofme,veryunrealandverypainful.
Andwhentheysaythat,IstartedtocryandIsay,"Oh,isitbecauseofmyage"….andsoIrealisedlater
ohIwasblamingmyself,butIknownowthatitcouldhappentoanywoman.(Parent4)
I think if I couldhave, if I couldhavephysically runawayat thatpoint Iwouldhavebut Iobviously
couldn’t(laughs)…. IthinkI justwantedto likegetawayfromeverything,but Idon’tthinkthatwas
becauseofhowshekindoftoldusit,Ithinkactuallyshetoldusitinavery,inaveryniceway.(Parent
6)
Onlyoneparentreportedimmediateacceptanceafterthenewswasdeliveredtoherbecauseshehad
knownsomeonewithasimilarconditiontotheirchildwhohaddonereasonablywellintermsoftheir
health,developmentandfamilylife.Alltheotherparentsreportedthatthenewshadsomekindof
negative emotional impact on them shortly after receiving it. The above accounts highlight the
importanceofHCPshavingacaring,compassionateattitudetominimisethenegativeimpactandto
enableparentstoaccessongoingsupportorreferraltootherappropriatesupport.
Intermsofcompetenceandexperience,itwouldbeimportantforthetraininginterventiontoinclude
thelivedexperienceofreceivingDNasthiswouldgiveHCPsanunderstandingoftheimpactofhow
DNisdeliveredaswellas insightintothegeneral impactofthenewsonafamily. Itwouldalsobe
importanttoaddresshealthcommunicationandsub-topicsofvalue-basedlanguageanddelivering
thenewsinabalancedmanner.Developingskillsofempathywerealsoidentifiedbyparentsasbeing
crucial.Manyoftheparentsinterviewednotedthattheydidnotwantpitynordidtheywantacold
detacheddeliveryoftheirchild’scondition,butratheradeliverywhichdemonstratedaprofessional
29
levelofunderstandingofwhattheyweregoingthrough. ItwasalsosuggestedbybothHCP’sand
parentsthatfuturetrainingincludedtheopportunityforHCP’stopracticewhattheyaretaughtvia
roleplayorpracticalexperience,therefore,allowingforamoretactilelearningapproach.
4.2.3ENVIRONMENTALCONTEXTANDRESOURCES
PrivacyandtimewerehighlightedasimportantfactorsforeffectivelyDDN.
A. PRIVACY
CertainscenariosinwhichDNwasdeliveredbyHCP’sand/orreceivedbyparentswasimpactedby
thelimitationsimposedbythehealthsetting.Forinstance,anumberofHCP’snotedthathospitals
didnothavethephysicalspacetoaccommodatethedeliveryofDNprivately:
Therejustisn’tlogisticsofspacewithinabusyNHShospitaltohavetheprivacytomakethosephone
calls,that’ssomethingI findreallydifficult….oneofthehardestthings if I'mtellingtheparentstheir
baby’sgotsomeconditionandthensomeonewilljuststormintomyofficeand,youknow,makeacup
ofteaorsomething.IfIwasface-to-facewiththatcoupleinalittleroom,um,no-onewouldwalkin
andmakeacupofteainthebackgroundbutno-onethinkstwiceaboutitwhenI’monthephone.(HCP
12)
Ithinkmaybe,erm,ifwe’dbeeninaprivateroomawayfromkindofbeingintheintensivecareunit
thatmighthavehelpedinsomerespectsbecausewewouldhavebeenabletokindofyouknow,erm,
cryortalkaboutitbutbecausewewerelike…inNICU,IfeltIhadtoholdmyemotionsin,thatIcouldn’t
kindofjustyouknow…Ithinkyouknow,if,ifIcouldgobackanddoitagainIwouldhaveaskedthatwe
couldhavebeenmoved,orwecouldhavebeen inaroomwherewecouldhavebeen leftto just,to
processourselvesratherthanbeingintheintensivecareunit.(Parent6).
It’s, unfortunately, it’snot ideal causeweare really,wehaven’tgota lotof spaceonourunit, but
unfortunatelyitallhastobedonewithintheunitwherethere’sstillworkgoingon….(HCP6)
However,severalparticipantsreportedthatafterthenewswasdeliveredpostnatally,parentswere
often given their own space away from the other babies and sometimes looked after in the
bereavementsuite.Parentsexpressedmixedfeelingsaboutthis.Whileinsomeinstancesthisgave
themtheprivacytoprocesstheirownemotions,being inabereavementsuitealsoreinforcedthe
negativeconnotationsofthebirthoftheirchild:

30
So,erm,so,it’sabitofadouble-edgedsword.Weweremovedintoaroombyourself,whichwasgood
becausemeandmyhusbandliterallyassoonaswegotinthatroomwejustcriedandhuggedeach
other,weliterallyjustlikecried,andjustheldeachothertightandthenwetalkedaboutthings…….and
then,myhusband,thehospitalallowedmyhusbandtostayonamattressonthefloorinmyroomso
thatwewereabletostaytogether,overnight,thatwasonegoodthingaboutbeingintheroom.Itdid
feelalittlebitlikewe’dbeen,becausetheyputusattheroomrightattheendofthecorridorsoitdid
feellikewe’dbeenshovedrightoutofthewayaswell,likenobodyreallywantedtohavetogopastus
orlikespeaktousatall,itdidfeelalittlebitlikethatattimes,likeifweputthemoutofthewayatthe
endofthecorridorthenwejustdon’thavetokindofhavetheconversationswiththem,theycan’tjust
catchusaswegopast,itdidfeellikethatattimes,likeifweshovethatproblemoutofthewayitgoes
away,soitfeltlikethatalittlebit.(Parent6)
B. TIME
HCPs reported that theyoftenhada significantnumberofpatients theywere lookingafterwhich
sometimeshinderedamorepersonalandpatientcentredapproach:
Thereareotherbabieswhichneeddeliveryaswell,soyouareconcentratingonotherbabies…sothatis
very challenging, and you just apologise to the patient …. “I am very sorry, I have to, go for an
emergency,andwillcomeback.”(HCP4)
Inthescenarioabove,itwasbeyondtheHCP’scontrolthattheywereneededforanotheremergency
however,aprotocolcouldhavebeeninplaceforanotherHCPwhoknewthefamilytotakeoverfrom
themandrespondtoanyquestionsthefamilyhad.Severalnarrativesfromtheparentsindicatedthat
they thought itwas important for the informingHCP to have time to answer questions after the
diagnosisortobeavailabletoanswerthequestionstheymayhaveastheyprocessedthenewsthey
have received. Parents valued HCPs who made time for this especially if they had an ongoing
relationshipwiththem:
Andtheremightbeawaitingroomoutsideandyouknowthatthereareotherpeoplethatarewaiting
buthealwaysgivesyouthe impressionthathe’sgottime,sonothing isrushed,hedoesn’tsitthere
lookingatthiswatch.Hedoesn’tkeeplikehurryingyoualong,hedoesn’ttryandcutyouoff.(Parent2)
Timeinthisstudynotonlyreferredtoavailabilitytodiscusstheprognosiswithparentsbuttheactual
timeatwhichtheHCPdecidedtodeliverthenews:
31
Isshereadytohandlethenewson2hourssleepwithoutherhusbandherewhenherchildisobviously
beingcheckedforthings?(Parent5)
IdidfeelthatthedoctorwhodeliveredthenewsatXXXHospital,thattheyfeltthatmybabyhadthe
signsofhavingDown'sSyndrome,IfeltthatwasdoneverysensitivelyandIwas,Iwashappywiththe
waytheydidthat,althoughIwouldhavepreferredthatmyhusbandwaswithmeatthetimeandthat
Iwasn'tonmyown[laughs]inthehospitalhavingjustgivenbirth,feelingabitisolated.(Parent9)
BothParent5andParent9reportedthattheywouldhavepreferredthattheHCPshaddeliveredDN
whentheywerenottired,aloneandwiththeirspousesabsent.Inanotherexample,theHCPdidnot
take into consideration both the need for a private space or the appropriateness of DDNwithin
minutesofthechild’sbirth:
…maybeifshe’dhavewaitedabitorgoneoutoftheroomandthoughtaboutitbeforeshesaidwhatshe
said…….Andjustgivenus20minutes,orsomething….butitwasliterally,ifyoucanimagine,soyou’vegot
Zoeliftedup,shownshe’sagirl,said,“Doyouwanttotellyourhusbandwhatitis?”sotheythencarryher
offandIgo,“It’sagirlZech,it’sagirl,”heburstintotears,happiness,andthenIlookaroundforsomeone’s
tryingtogetmyattention,andshe’slike,“Oh,youknow,yourbaby’sgotallitsfingersandtoesbutIthink
she’sgotDown’sSyndrome,”andit’s likeitallhappened, just like,and…Zoe’sovertherenowwithother
peopleandI’mlike,andthere’sjustallthesepeoplelookingatmethatthey’regonnagetreadytostitchme
up,and,youknow……So,I’mstillsortoflikelookingateverybodylookingme,waitingformeto….Idon’t
know,dowhatevertheywantmetodo.(Parent8)
Parent 8, made the point that the news was given abruptly, there were no immediate medical
emergencieswhichhadtobeaddressedforthechildandshefeltthattherewasnoneedtotellher
lifechanginginformationwithinminutesofherbabybeingborn,inthepresenceofmanyotherHCPs
andmostimportantlybeforeshehadbeengiventheopportunitytoseeandholdherbabyforthefirst
time,feedherdaughterandbondwithher.Inacontraryscenario,theconsultantnotedsomemarkers
forDown’sSyndromehowevertheydealtwiththemedicalemergenciesfirstandraisedtheirconcerns
aboutDown’sSyndromewhenthebabywasthreedaysold:
Um,sohewasintheneonatalward,blesshim,andhewasinanincubatorbecausetheyweretryingto
keephimwarmandtheykept,um,andbecausehisoxygenlevelkeptdippingbecausehehadthishole
inhisheartandsotherewasa lady, I thinkshewasa locum, itwasn’toneofthepeoplethatwere
generallyon,onandshecameinandshenoticedthatChrishadquiteaflatsortofback,hisbackofhis
headwasquiteflat,um,andshewasobviouslykindofputtingthepiecestogetherandtheheart,well
32
atthatpointwedidn’tquiteknowthathehadaheartproblembutthefactthathewasstrugglingto
keephimselfwarmandthathisSATSweredroppingandthingslikethat.Ithinkshenoticedhisalmond
shapedeyesandsoshehadherkindofconcernsthat,thatChriswasbornwithDown’ssyndromeand
ithadn’tkindofbeenvoiced,butImeanitwasonlythreedaysintohimbeinghere,blesshim,so,um,
soshekindof,shesaidtousaboutitandsaid“I’dliketodoabloodtest…(Parent7).
It is important to note that medical concerns for the mum or baby created scenarios in which
communicationwasabruptornon-existentfromHCP’sinanattempttodealwiththeemergencyat
hand.However,wheretherearenoimmediatelifethreateningemergenciesforthemotherorthe
babies,parentsfeltthatitwasimportantfortheHCPtotaketimetopreparethemselvestodeliver
thenewsbyfindingaprivateplacetodeliverthenews;consideringthemostappropriatetimeofthe
day to deliver the news, bearing inmind the importance of including significant others such as a
spouseandtohavetimetoanswerquestionsoridentifyingsomeonetotakeoveriftheyknewthat
theywould potentially be required to attend to other patients. Assessing the physical and social
environmentpriortoDDNwasperceivedasacriticalcomponenttominimisingthenegativeimpact
ofreceivingDN.
4.2.4OPTIMISM
Optimism referred toHCPs being able to reassure parents by providing a balanced description of
congenitalanomalies.Allbuttwooftheparentsinterviewednotedanunbalanceddeliveryoftheir
child’sconditionbyHCP’s.ItwasimportanttoparentsandHCPsthattheHCPhadtheskillstoprovide
a balanced description of themedical condition as they felt it enabled them to have hope and a
positiveoutlookontheirchildren,toseepastthediagnosiswhichtheirchildhadbeengivenandto
makeaninformeddecisionaboutcontinuingorterminatingapregnancyasindicatedinthenarratives
below:
Wedoneedtobecarefulwhatwesay,wedoneedtogetthatbalanceright,wedoneedtosupport
thewomeninwhicheverchoicetheydo]……Ithinkthereisamovementaroundsaying,makingsure
thatwomenareawarethat,actually,terminationisn'ttheonlyoption….(HCP2)
Theywerevery,youknow,"Werecommendyouterminate",notasin,"Ifhesurvives,hemayhavethese
problems",therewasn'tanyofthat,itwas,"Werecommendyouterminateandthisiswhathappens",
rather than,youknow,"Ifhesurviveshemaynotbeable todothis, this, thisandthis", itwasn'ta
balancedconversation.(Parent3)

33
We’vebeenreallyluckytohavealotofpositivesortofattitudestowards,oursonandhisDown’s
syndrome.So,Ithink,Ithinkit’sreallyimportanttokindofrecognisethepersonfirst,notjustthefact
thattheyhaveDown’ssyndrome(Parent7)
Icantellyousomanyfamiliesarethesame,theyjust,youneverforgetwhatissaidtoyou,andyou
overanalyseeverythingbecauseyou’retryingtoworkitallout,andifthere’sanythingthatmakesyou
questionyourself,you’ll,you’lljustplayitoverandoveragainandit’s,it’sreallyimportantthatthings
aren’tsaidinanexcitableway,oranegativeway,just,justthat’sthisiswhatitisand,youknow,it’s
gonnabeokay,like,youknow,youcangetaroundit,wecan,youknow,there’sthingsforyouto,but
it,it’snotatthemomentit’sallquitedoomyandgloomy.(Parent8)
While HCPs felt that it was important to be able to provide parents with information about the
conditiontheirchildhadbeendiagnosedwith,itwasimportantthatthiswasgiveninstagesassome
parents mentioned being overwhelmed and unable to take in the large amount of information
providedtothem.Itwasveryimportanttoparents,thatHCPsprovidedabalanceddescriptionoftheir
child’sdiagnosisanditsimplicationsbothintheshortandlongtermfuturewithoutanoveremphasis
ofnegativethingswhichmayormaynothappeninthefuturesuchasdevelopingAlzheimer’sdisease.
ParentsfeltitwasunfairtodiscusssuchissuesforchildrenwithDSforexampleandleavediscussion
ofsimilarmatterswithparentsofneurotypicalchildrenwhocouldwellhaveafamilyhistoryofsimilar
diseasesandpotentiallyhaveageneticpredispositiontothis.Parentswithlivedexperiencestressed
theneedforthetraininginterventiontohighlightsomeofthechallengesaswellasthejoysofhaving
achildwhowasdiagnosedwithacongenitalanomaly.
4.2.5BELIEFSABOUTCONSEQUENCES
We discussed in earlier sections the negative impact of receiving DN and how this could be
exacerbatedbythenewsbeingdeliveredinappropriately.Beliefsaboutconsequencesalsoreferred
totheimpactofhowDNwasdeliveredontheHCP-familyrelationship.Itisimportanttonotethata
numberofparentsinthisstudyindicatedthattheyhadmadeformalcomplaintsabouthowtheywere
giventhenews:
Yeah,ImeanthefirsttimeI,Ididactuallymakeacomplaintaboutthewaythenewswasdeliveredto
me,becauseIfeltthatnobodyhadaskedwhatIwasdoingatthetimeor,youknow......if Iwasina
placethatwas... ...safeformetobegiventhatinformation,andIalsofeltthatthewayitwasgiven

34
overthephoneandermtheurgencythatIhadtocometothehospitalassoonaspossible,it,itputme
intoabitofapanicwhichtherewasnoneedfor.(Parent9)
So,atthatpoint, Iwasveryupset,er,andeventually, it ledmetomakeacomplainttothePatient
AdviceandLiaisonServiceatthehospital,andweweretransferredtoanotherpaediatrician.Wegotan
apologyforthewaythatwehadbeentreated,butitjustmakesyouwonderhowmanyotherpeople
havehadthatsameexperience?(Parent2)
Infact,shemadeaformalcomplaintandshewasthenseenbyaConsultantandthatwassorted,most
peopledon't,it'senoughforthemtotalktous,whichactuallydoesn'thelpinthelongrunbecauseIcan
complain, I canemailand I'vedone it in thepast, I'veemailedConsultantssaying 'this iswhatyour
doctorsaidtoapatient'andnothingchangesunlessthepatientscomplain,buttheydon'tcomplain,
theyveryrarelydocomplain,becausethey'vetalkedtousandwe'vemadethemfeelbetter.(HCP3)
Makingformalcomplaintswasmotivatedbytheneedtoprotectotherparentsfromreceivingasimilar
standardofcare.ItisthereforeimportantforthetrainingtohighlightthatthenegativeimpactofDDN
canalsoaffecttheHCPinquestionaswellasthetrustasawholeintheeventofcomplaintsbeing
madeabouthowDNwasdelivered.
4.2.6EMOTION
SeveralHCPsindicatedthatDDNonanongoingbasisaffectedthememotionallyandthatsometimes
theeffectoftheconversationslingeredforyearsaftertheevent:
Idon'tthinkyoucouldevernotbeermaffectedbyit,especiallyifyouhavetheabilitytobeempathetic
andputyourselfinthat,becauseyouthink'ohmyGod,ifthatwasmybabyhowwouldIfeel',yeah….
trainingtohelppeopleputthemselvesinotherpeople'spositionstothinktothemselves'howwouldI
feelifthatwasmeorthatwasmydaughterormysisterormymotheror',youknow.(HCP3)
Ihavegoneintothatwoman’sworldcompletelyunannouncedandI’vedestroyedit…Ihavewalkedout
ofafeticideandabsolutelybrokenmyheart….butit’spartofthejob,isn’tit?(HCP2)
Itaffectsme,ofcourse,…butIhavetoacceptthatthisismyjob(HCP4)
WhilesomeNHStrustsweresaidtohavefacilitiesinplaceforteamdebriefingorcounsellingthiswas
notauniversalexperienceamongtheHCPs.ItwouldbeimportantforthetrainingtosupportHCPsto
identifywaystoacknowledgeandmanagetheirownemotionsaboutDDN.Thisaspectofmanaging
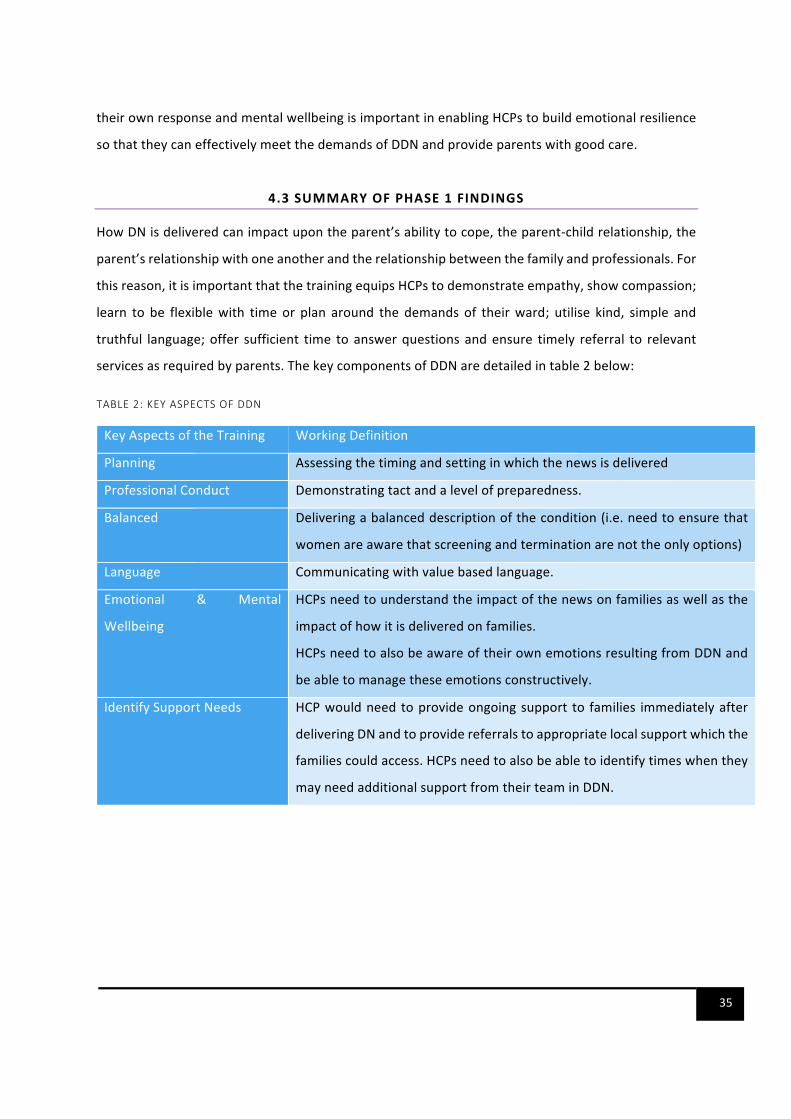
35
theirownresponseandmentalwellbeingisimportantinenablingHCPstobuildemotionalresilience
sothattheycaneffectivelymeetthedemandsofDDNandprovideparentswithgoodcare.
4.3SUMMARYOFPHASE1FINDINGS
HowDNisdeliveredcanimpactupontheparent’sabilitytocope,theparent-childrelationship,the
parent’srelationshipwithoneanotherandtherelationshipbetweenthefamilyandprofessionals.For
thisreason,itisimportantthatthetrainingequipsHCPstodemonstrateempathy,showcompassion;
learn to be flexiblewith timeor plan around the demands of theirward; utilise kind, simple and
truthful language;offer sufficient time toanswerquestionsandensure timely referral to relevant
servicesasrequiredbyparents.ThekeycomponentsofDDNaredetailedintable2below:
TABLE2:KEYASPECTSOFDDN
KeyAspectsoftheTraining WorkingDefinition
Planning Assessingthetimingandsettinginwhichthenewsisdelivered
ProfessionalConduct Demonstratingtactandalevelofpreparedness.
Balanced Deliveringabalanceddescriptionofthecondition(i.e.needtoensurethat
womenareawarethatscreeningandterminationarenottheonlyoptions)
Language Communicatingwithvaluebasedlanguage.
Emotional & Mental
Wellbeing
HCPsneedtounderstandtheimpactofthenewsonfamiliesaswellasthe
impactofhowitisdeliveredonfamilies.
HCPsneedtoalsobeawareoftheirownemotionsresultingfromDDNand
beabletomanagetheseemotionsconstructively.
IdentifySupportNeeds HCPwouldneedtoprovideongoingsupport to families immediatelyafter
deliveringDNandtoprovidereferralstoappropriatelocalsupportwhichthe
familiescouldaccess.HCPsneedtoalsobeabletoidentifytimeswhenthey
mayneedadditionalsupportfromtheirteaminDDN.
36
5. INTERVENTIONDEVELOPMENT
5.1DEVELOPMENTOFTHETRAININGINTERVENTION
Using findings from the literature review and interviewswith HCPs and parents, we developed a
training intervention for DDN. Drawing on the BCW and other previous studies [16, 17, 56], the
followingstepsweretakentodeveloptheintervention:
• Step 1: Delineating key intervention components. This involved an initial discussion of key
interventioncomponentsbasedonfindingsfromtheliteraturereviewandspecificationsofthe
requirementsfromHealthEducationEnglandworkingacrossKent,SurreyandSussexwhowere
fundingthestudy.
• Step 2: Mapping barriers to and enablers of the implementation of the intervention to the
theoretical domains framework. Data from the parent interviews, HCP interviews, and the
literaturereviewwereanalysedwiththeintentionofidentifyingthebarrierstoefficientdelivery
ofDNandtheenablerstothis.
• Step3:Identifyingpotentialinterventioncomponentsthatcanovercomemodifiablebarriersand
enhancetheenablerswithinafutureintervention.ThisinvolvedexaminationoftheCOM-Bmodel
andtheBehaviourChangeTaxonomytoidentifythefunctionsoftheinterventionrequiredand
the corresponding evidenced based behaviour change techniques which could achieve the
requiredfunctions.ThiswasthenadaptedtothecontextofDDN.Thestudyteammettoagreeon
thefinalcontentoftheintervention.
• Step 4: Ensuring the viability of the intervention using APEASE (Acceptability, Practicability,
Effectiveness/cost-effectiveness,Affordability,Safety/side-effects,Equity) [56].Thestudy team
and the steering committee members met to determine if the intervention was robust and
fulfilledrelevantcriteriaandifthiscouldbeimplemented.
Basedontheaboveprocess,weoutlinethekeycomponentsofthetraininginterventionintable3
below:
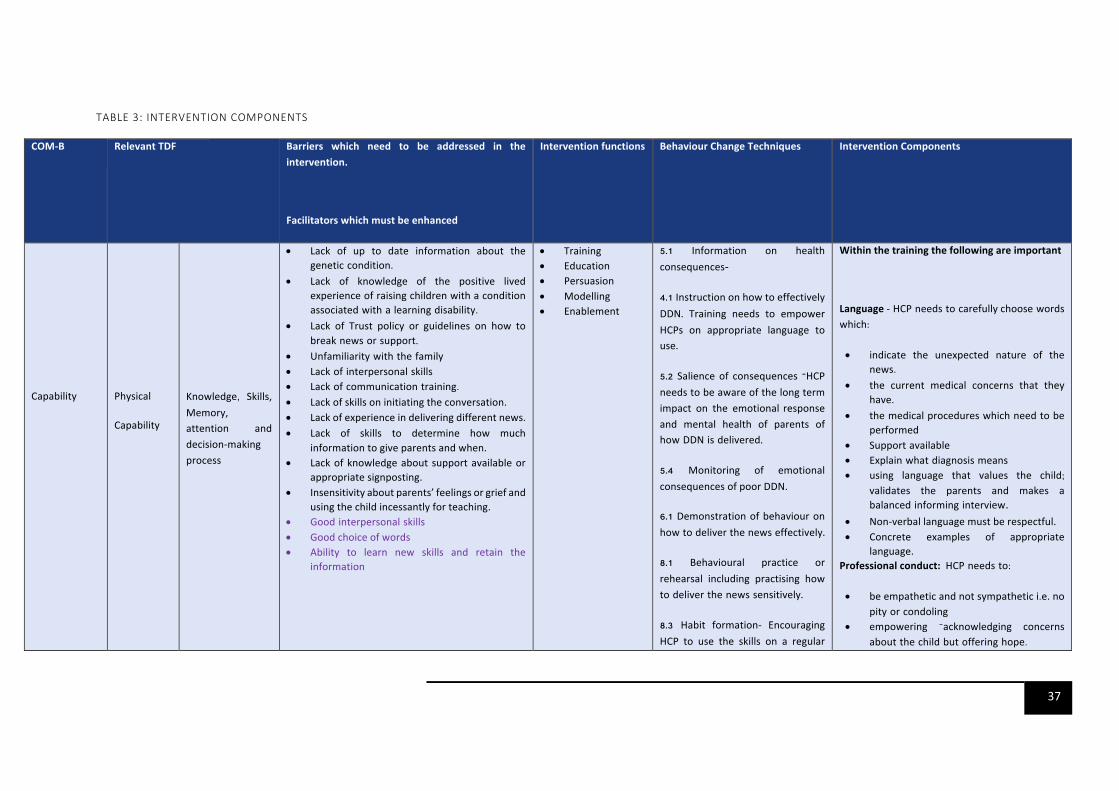
37
TABLE3:INTERVENTIONCOMPONENTS
COM-B RelevantTDF Barriers which need to be addressed in theintervention.
Facilitatorswhichmustbeenhanced
Interventionfunctions BehaviourChangeTechniques InterventionComponents
Capability
Physical
Capability
Knowledge, Skills,Memory,attention anddecision-makingprocess
• Lack of up to date information about thegenetic condition.
• Lack of knowledge of the positive lived experience of raising children with a condition associated with a learning disability.
• Lack of Trust policy or guidelines on how to break news or support.
• Unfamiliarity with the family • Lack of interpersonal skills • Lack of communication training.
• Lackofskillsoninitiatingtheconversation. • Lack of experience in delivering different news. • Lack of skills to determine how much
informationtogiveparentsandwhen. • Lackofknowledgeaboutsupportavailableor
appropriatesignposting. • Insensitivityaboutparents’feelingsorgriefand
usingthechildincessantlyforteaching. • Good interpersonal skills • Goodchoiceofwords • Ability to learn new skills and retain the
information
• Training
• Education • Persuasion • Modelling • Enablement
5.1 Information on health
consequences-
4.1 Instruction on how to effectively DDN. Training needs to empower HCPs on appropriate language to
use.
5.2 Salience of consequences –HCP
needs to be aware of the long term
impact on the emotional response
and mental health of parents of how DDN is delivered.
5.4 Monitoring of emotionalconsequencesofpoorDDN.
6.1 Demonstration of behaviour onhow to deliver the news effectively.
8.1 Behavioural practice or rehearsal including practising how
to deliver the news sensitively.
8.3 Habit formation- EncouragingHCP to use the skills on a regular
Withinthetrainingthefollowingareimportant
Language-HCP needs to carefullychoose words which:
• indicate the unexpected nature of the news.
• the current medical concerns that they have.
• the medical procedures which need to be performed
• Support available
• Explain what diagnosis means • using language that values the child;
validates the parents and makes a balanced informing interview.
• Non-verballanguagemustberespectful. • Concrete examples of appropriate
language. Professionalconduct:HCP needs to:
• be empathetic and not sympathetic i.e. no
pity or condoling
• empowering –acknowledging concerns about the child but offering hope.
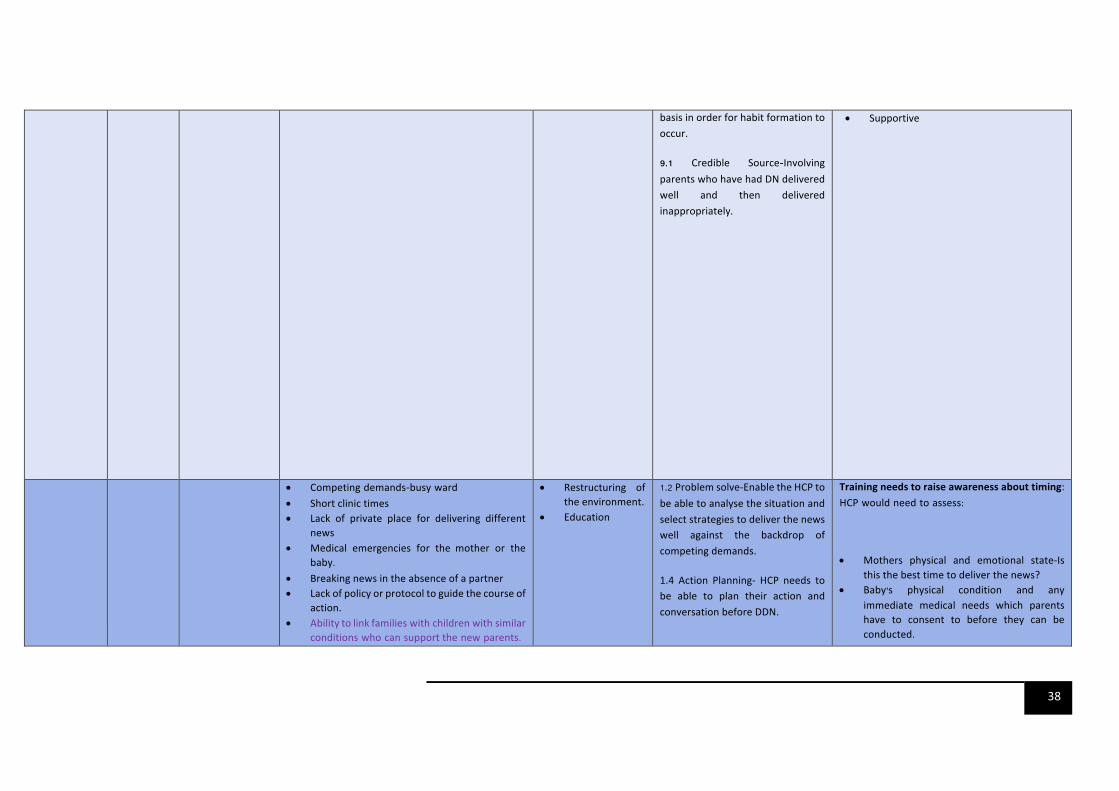
38
basisinorderforhabitformationtooccur.
9.1 Credible Source-Involving
parents who have had DN delivered
well and then delivered
inappropriately.
• Supportive
• Competing demands-busy ward
• Shortclinictimes • Lack of private place for delivering different
news • Medical emergencies for the mother or the
baby. • Breakingnewsintheabsenceofapartner • Lackofpolicyorprotocoltoguidethecourseof
action. • Abilitytolinkfamilies with children with similar
conditions who can supportthe new parents.
• Restructuring oftheenvironment.
• Education
1.2 Problemsolve-EnabletheHCPtobeabletoanalysethesituationandselectstrategiestodeliverthenewswell against the backdrop ofcompetingdemands.
1.4 Action Planning- HCP needs tobe able to plan their action andconversationbeforeDDN.
Trainingneedstoraiseawarenessabouttiming:HCP would need to assess:
• Mothers physical and emotional state-Isthisthebesttimetodeliverthenews?
• Baby’s physical condition and any immediate medical needs which parents have to consent to before they can be conducted.
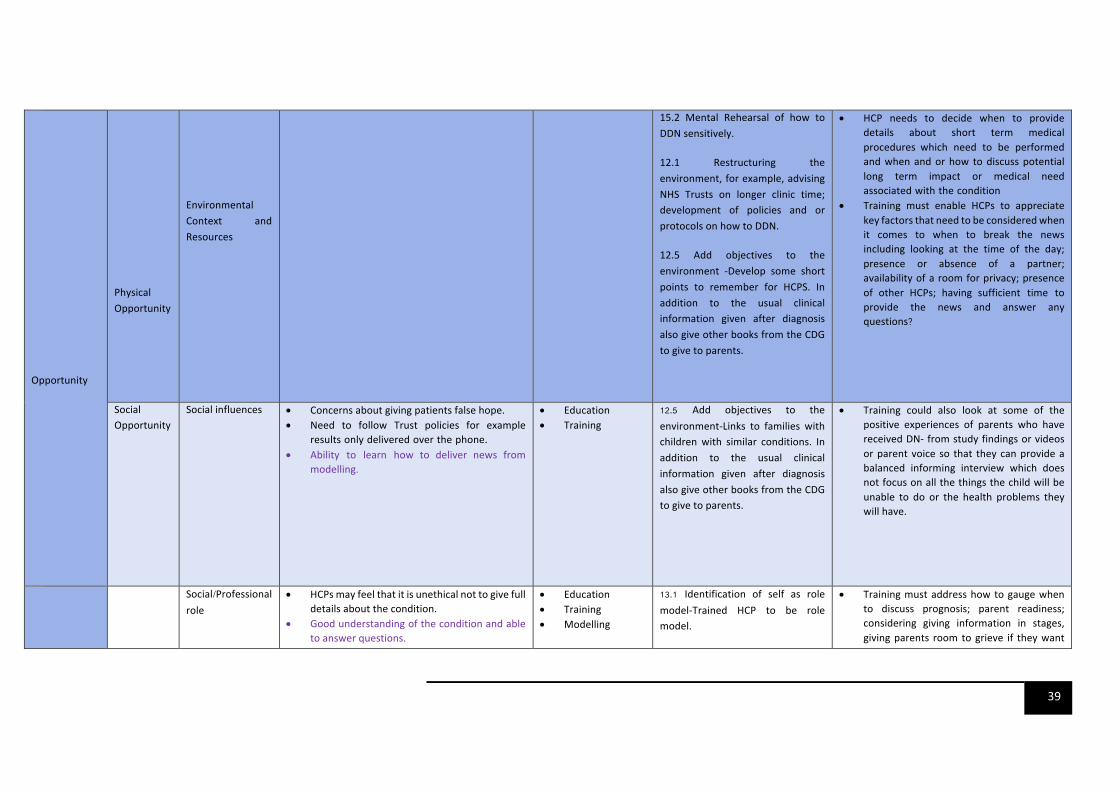
39
Opportunity
PhysicalOpportunity
EnvironmentalContext andResources
15.2 Mental Rehearsal of how toDDNsensitively.
12.1 Restructuring theenvironment,forexample,advisingNHS Trusts on longer clinic time;development of policies and orprotocolsonhowtoDDN.
12.5 Add objectives to theenvironment -Develop some shortpoints to remember for HCPS. Inaddition to the usual clinicalinformation given after diagnosisalsogiveotherbooksfromtheCDGtogivetoparents.
• HCP needs to decide when to provide details about short term medical procedures which need to be performed and when and or how to discuss potential long term impact or medical need associated with the condition
• Training must enable HCPs to appreciatekeyfactorsthatneedtobeconsideredwhenit comes to when to break the newsincluding looking at the time of the day;presence or absence of a partner;availabilityofaroomforprivacy;presenceof other HCPs; having sufficient time to provide the news and answer any questions?
SocialOpportunity
Socialinfluences • Concernsaboutgivingpatientsfalsehope.• Need to follow Trust policies for example
results only delivered over the phone.• Ability to learn how to deliver news from
modelling.
• Education
• Training 12.5 Add objectives to theenvironment-Links to families withchildren with similar conditions. Inaddition to the usual clinicalinformation given after diagnosisalsogiveotherbooksfromtheCDGtogivetoparents.
• Training could also look at some of thepositive experiences of parents who havereceivedDN-fromstudyfindingsorvideosorparentvoice so that theycanprovideabalanced informing interview which doesnotfocusonallthethingsthechildwillbeunable to do or the health problems theywillhave.
Social/Professional role
• HCPsmayfeelthatitisunethicalnottogivefulldetailsaboutthecondition.
• Goodunderstandingoftheconditionandabletoanswerquestions.
• Education • Training
• Modelling
13.1 Identification of self as rolemodel-Trained HCP to be rolemodel.
• Trainingmustaddresshowtogaugewhento discuss prognosis; parent readiness;considering giving information in stages,givingparents roomtogrieve if theywant
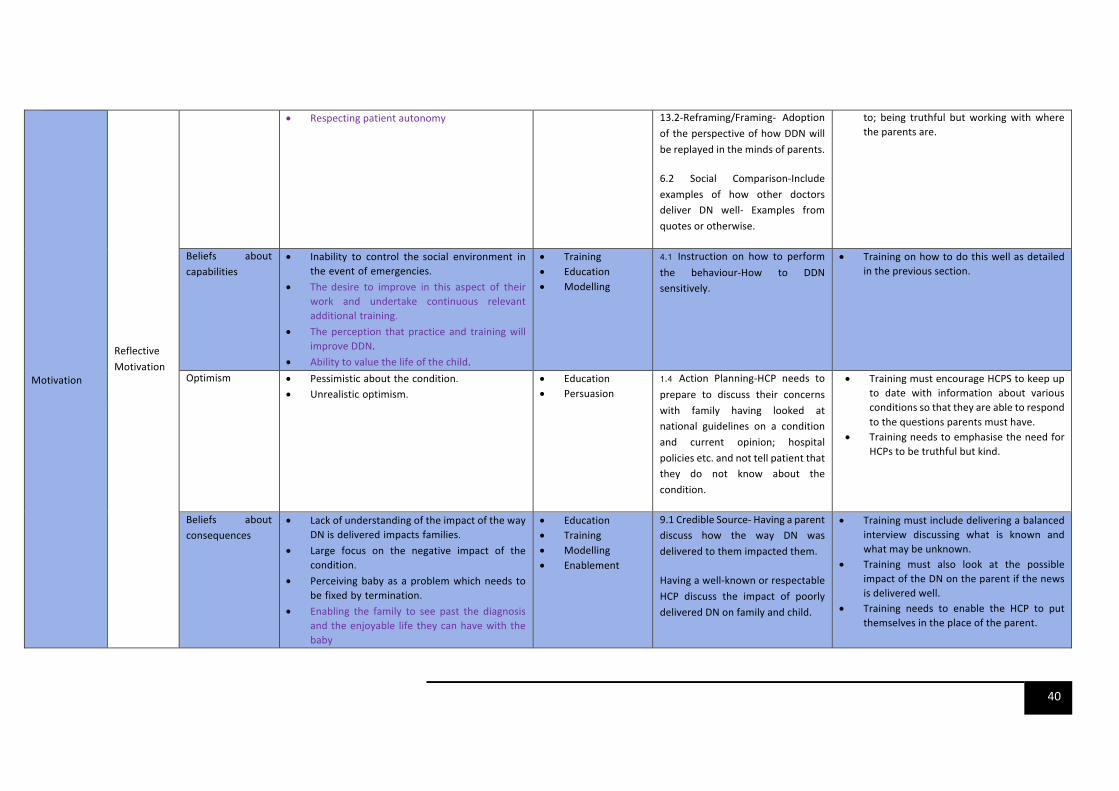
40
Motivation
ReflectiveMotivation
• Respectingpatientautonomy
13.2-Reframing/Framing- AdoptionoftheperspectiveofhowDDNwillbereplayedinthemindsofparents.
6.2 Social Comparison-Includeexamples of how other doctorsdeliver DN well- Examples fromquotesorotherwise.
to; being truthful butworkingwithwheretheparentsare.
Beliefs about capabilities
• Inability to control thesocial environment in the event of emergencies.
• Thedesire to improve in this aspect of their work and undertake continuous relevant additional training.
• Theperception that practice and trainingwillimproveDDN.
• Abilitytovaluethelifeofthechild.
• Training
• Education
• Modelling
4.1 Instruction on how to performthe behaviour-How to DDNsensitively.
• Trainingonhowtodothiswellasdetailedintheprevioussection.
Optimism • Pessimistic about the condition.
• Unrealistic optimism.
• Education
• Persuasion 1.4 Action Planning-HCP needs toprepare to discuss their concernswith family having looked atnational guidelines on a conditionand current opinion; hospitalpoliciesetc.andnottellpatientthatthey do not know about thecondition.
• TrainingmustencourageHCPStokeepupto date with information about variousconditionssothattheyareabletorespondtothequestionsparentsmusthave.
• TrainingneedstoemphasisetheneedforHCPstobetruthfulbutkind.
Beliefs about consequences
• Lack of understanding of the impact of the way DNis delivered impacts families.
• Large focus on the negative impact of the condition.
• Perceiving baby as a problem which needs to be fixed by termination.
• Enabling the family to see past the diagnosis and the enjoyable life they can have with the baby
• Education
• Training
• Modelling • Enablement
9.1CredibleSource-Havingaparentdiscuss how the way DN wasdeliveredtothemimpactedthem.
Havingawell-knownorrespectableHCP discuss the impact of poorlydeliveredDNonfamilyandchild.
• Trainingmustincludedeliveringabalancedinterview discussing what is known andwhatmaybeunknown.
• Training must also look at the possibleimpactoftheDNontheparentifthenewsisdeliveredwell.
• Training needs to enable the HCP to putthemselvesintheplaceoftheparent.
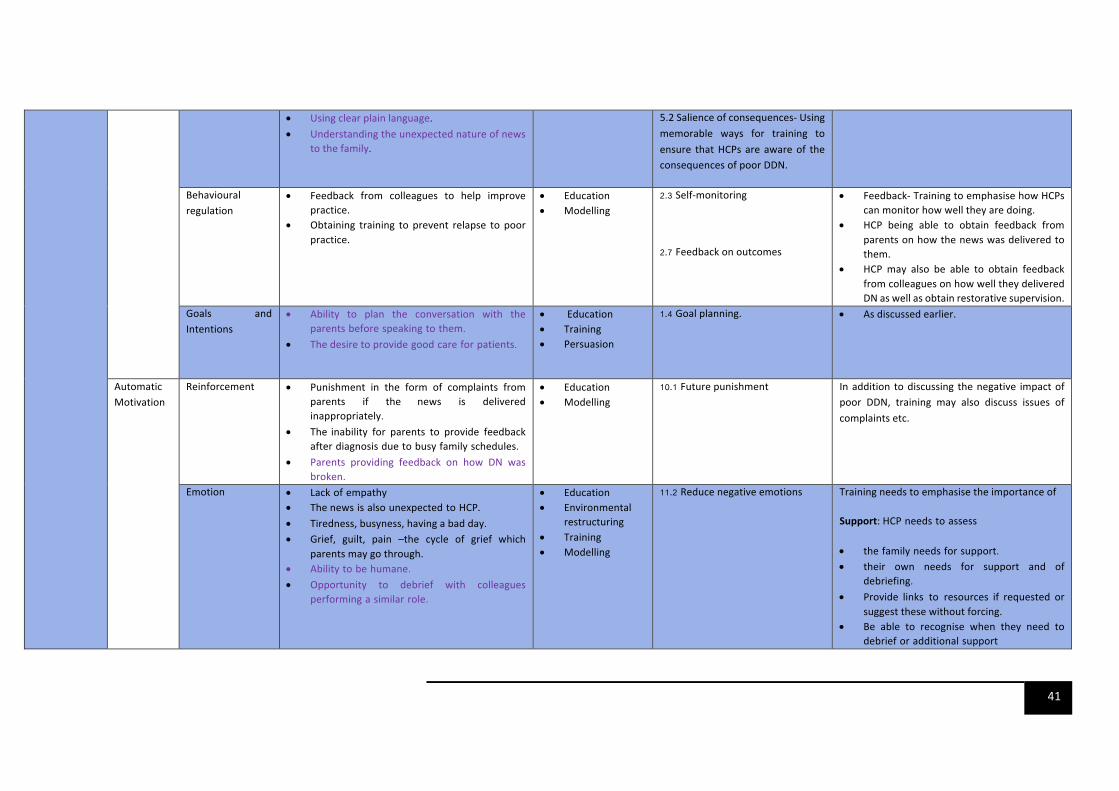
41
• Usingclearplainlanguage.
• Understandingtheunexpectednatureofnewstothefamily.
5.2Salienceofconsequences-Usingmemorable ways for training toensure thatHCPsareawareof theconsequencesofpoorDDN.
Behavioural regulation
• Feedback from colleagues to help improvepractice.
• Obtaining training to prevent relapse to poorpractice.
• Education
• Modelling 2.3 Self-monitoring
2.7 Feedbackonoutcomes
• Feedback-TrainingtoemphasisehowHCPscanmonitorhowwelltheyaredoing.
• HCP being able to obtain feedback fromparentsonhowthenewswasdeliveredtothem.
• HCP may also be able to obtain feedbackfromcolleaguesonhowwelltheydeliveredDNaswellasobtainrestorativesupervision.
Goals andIntentions
• Ability to plan the conversation with the parents before speaking to them.
• Thedesiretoprovide good care for patients.
• Education
• Training
• Persuasion
1.4 Goalplanning. • Asdiscussedearlier.
AutomaticMotivation
Reinforcement • Punishment in the form of complaints from parents if the news is delivered inappropriately.
• The inability for parents to provide feedback after diagnosis due to busy family schedules.
• Parents providing feedback on how DN wasbroken.
• Education
• Modelling 10.1 Futurepunishment Inaddition todiscussing thenegative impactof
poor DDN, training may also discuss issues ofcomplaintsetc.
Emotion • Lack of empathy • Thenews is also unexpected to HCP.
• Tiredness,busyness,havingabadday. • Grief, guilt, pain –the cycle of grief which
parentsmaygothrough. • Ability to be humane.
• Opportunity to debrief with colleagues performing a similar role.
• Education
• Environmentalrestructuring
• Training • Modelling
11.2 Reducenegativeemotions Trainingneedstoemphasisetheimportanceof
Support:HCP needs to assess
• the family needs for support. • their own needs for support and of
debriefing.
• Provide links to resources if requested orsuggestthesewithoutforcing.
• Be able to recognise when they need to debrief or additional support

42
5.2TRAININGCONTENT
5.2.1TRAININGAIMSANDOBJECTIVES
The training aimed to enable healthcare professionals to understand the short and long term
significance of non-verbal and verbal communication for parents emotional andmentalwellbeing
whenDNisdelivered.
Bytheendofthetrainingparticipantswereexpectedtohave:
• Recognised the importance of establishing the right physical, emotional, social and
environmentalspacetodeliverdifferentnews.
• Gainedunderstandingof the importanceofplanningbeforeDDN including identifying the
appropriate time to deliver the news, choosing the appropriate language to use and the
appropriateinformationtogiveatinitialandfollowupdiscussionswiththefamily.
• Becomeawareofresourceswhichmaybeavailablelocallyandnationallyforparentswhich
canhelpthemprocess,understandandinterpretthediagnosis.
• RecognisedtheimportanceofregularpersonalsupportandfeedbackonthedeliveryofDN
andhowthiscontributestotheirownmentalwellbeingandCPD.
• Gainedanunderstandingoftheimportanceofsharedresponsibilityfortheimmediateand
ongoingcareandsupportofthefamily.
Thetrainingwasaimedat:
• Paediatricians/NeonatologistsorSpecialtytraineesinthisfield
• ObstetriciansorObstetricSpecialtyTrainees
• MidwivesparticularlyScreeningMidwives
• SpecialistPaediatricnurses,AdvancedNursePractitioners,andNeonatalnurses
• Sonographers
Table4showsthedifferentsessionswhichwerecoveredduringthetraining.
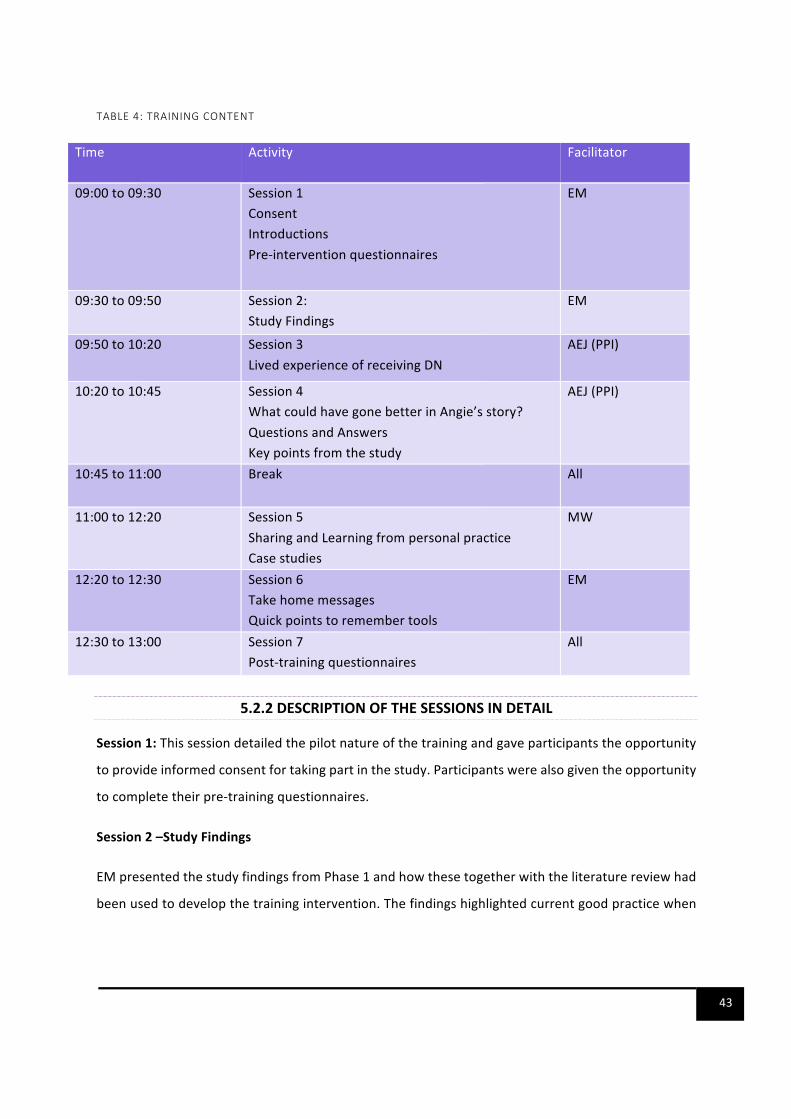
43
TABLE4:TRAININGCONTENT
5.2.2DESCRIPTIONOFTHESESSIONSINDETAIL
Session1:Thissessiondetailedthepilotnatureofthetrainingandgaveparticipantstheopportunity
toprovideinformedconsentfortakingpartinthestudy.Participantswerealsogiventheopportunity
tocompletetheirpre-trainingquestionnaires.
Session2–StudyFindings
EMpresentedthestudyfindingsfromPhase1andhowthesetogetherwiththeliteraturereviewhad
beenusedtodevelopthetrainingintervention.Thefindingshighlightedcurrentgoodpracticewhen
Time Activity Facilitator
09:00to09:30 Session1ConsentIntroductionsPre-interventionquestionnaires
EM
09:30to09:50 Session2:StudyFindings
EM
09:50to10:20 Session3LivedexperienceofreceivingDN
AEJ(PPI)
10:20to10:45 Session4WhatcouldhavegonebetterinAngie’sstory?QuestionsandAnswersKeypointsfromthestudy
AEJ(PPI)
10:45to11:00 Break All
11:00to12:20 Session5SharingandLearningfrompersonalpracticeCasestudies
MW
12:20to12:30 Session6TakehomemessagesQuickpointstoremembertools
EM
12:30to13:00 Session7Post-trainingquestionnaires
All

44
delivering different news; practice which could be improved and suggestions of how this can be
addressed.
Session3-TheLivedexperience
ThissessionwasfacilitatedbyAEJwhoisoneofourPatientandPublicRepresentativesandhaslived
experienceofreceivingDN.AEJdescribedherownjourneyofreceivingdifferentnews,whatwent
wellandwhatcouldhavegonebetter.AEJgaveabriefbackgroundonherfamily,describedhowDN
wasdeliveredtoheraswellastheimmediateandlongtermimpactofthenewsonher,herhusband
andherfamily.
Session4:Whatcouldhavegonebetter
Inthissession,AEJgavetheHCPsanopportunitytoexamineherstoryandreflectonhowthekey
requirementsforDDNaccordingtothestudyfindingscouldhavebeenusedinherjourney.
Session5:SharingandLearningfrompracticeandCasestudies
ThissessionwasfacilitatedbyMW.AstheMentalHealthLeadfortheinstitute,MWhasextensive
experienceinusingcasestudiesintraininghealthcareprofessionalsontheiHVPerinatalandInfant
Mental Health (PIMH) Champions Training programmes. Case studies are an excellent way for
participants to evidence their learning. They offer the opportunity to: positively reinforce good
practice;makeexplicitsafepractice;addressanyareasofconcernrelatingtopractice;re-emphasise
andconsolidatetheimportanceofcommunicatinginformationeffectively.Allthecasestudieswere
basedonactualreal-lifeexperienceswhichweresharedbyfamiliesduringtheinterviews.
Participantsweresplitintosmallgroups.Usingthepowerpointslidewhichwashyperlinkedtocase
scenarios,weaskedeach group in turn topick anumber, then reveal the case studybehind that
number.Thewholegroupreadthecasestudyandhadtheopportunityfora5minutes’discussion
withintheirsmallgroups.After5minutes,thegroupwhochosethenumbergavefeedbacktothe
wholegrouphighlighting
• Whattheyfeltthekeyissueswere
• Whattheywoulddo

45
• WhattheywouldsayordodifferentlybasedonthekeycomponentsofDDNhighlightedin
thestudyfindings.
Oncethesmallgroupgavetheirfeedbacktherewasanopportunityfortherestofthegrouptoshare
theirthinking,positivelychallenge,reinforcegoodpracticeandmakesuggestedalternatives.
Session6:TakehomemessagesandKeyMessages
EMgaveallparticipantsanopportunity tosharetheir takehomemessagefromthetraining.They
werealsogivenaREADYmnemonic(Figure5below)onkeyaspectsofDDN.
FIGURE5:READYMNEMONIC
Session7:
Thistrainingconcludedwithasummaryofkeypoints,avoteofthanksandcompletionofthepost-
trainingquestionnairesbyallparticipants.
R
A
D
Thismnemonicsupportsthedeliveryofdifferentnewsandisforusebyanyprofessionalwiththisresponsibilitye.g.obstetricians,paediatricians,midwives,sonographers.Thisisachallengingtaskfortheprofessionalataverytraumatictimeforparents.Takinganevidence-basedapproachcanhavebothshorttermandlong-termpositiveimpactforparents.Alackofpreparationmayleaveparentsre-experiencingthatmomentinatraumaticwayformanyyearsafter.Note:thistoolisdesignedtounderpinthestudyintervention.Itwillbesubjecttoversionchangesastheresearchstudyprogresses.
ightLanguage
Haveyoufoundtherightwordsusingplainlanguagethatparentswillunderstand?Isthemessagebalancedinwhatitconveys?
Haveyouthoughtabouthowyouwillpaceyourselfwhenyoudeliverthemessage?Whenyouthinkyouhavethewordsready-stop,reflectandimagineyourselfastheparents.Arethemessagesintheorderyouwouldwishtohearthem?
nvironment
Isthemostappropriateenvironment?Isthephysical,socialandemotionalspaceconducivetodeliveringdifferentnews?Doesitoffersufficientcomfort,privacyandfreedomfrominterruption?Willbothparentsbepresentandwhoelseshouldbethere?
ssessment
Haveyouundertakenanassessmentofparentreadinessandyourownreadinesstoengageindeliverythenews?Arethereanyimmediatemedicalconcernsforthemotherorthebaby?Canthetimingofdeliveryofthenewsbeoptimised?
oyourpreparationAreyouprepared?Haveyoureadthemedicalrecordsandliaised(ifnecessary)withotherprofessionals?Haveyoucheckedavailabilityoflocalornationalsupport?Haveyoucheckedifsomeoneisavailabletostaywiththeparentsifneeded?Areyouconfidentthatyoucanfinishtheconversationwithoutbeingcalledaway?
ouhaveoneopportunityatdeliveringdifferentnews–BEREADYRememberthatyouarecentraltothesafedeliveryandreceiptofpotentiallylife-changingnews.Youareabouttocreateamemorythatwillberevisitedinthelifetimeofthefamily.
Howdoyouwantthismomenttoberememberedbythefamily?
Version1-August2018
InstituteofHealthVisiting,c/oRoyalSocietyforPublicHealth,JohnSnowHouse,59MansellStreet,LondonE18AN
Supportedby:
AreyouREADY?
E
Y
Deliveringdifferentnews

46
6. PHASE2FINDINGS
6.1 DESCRIPTIONOFPARTICIPANTS
24HCPsparticipated in thePhase2 training. Inaddition,RhonaWestripProgrammeManager for
IntellectualDisabilitiesHEESouthRegionandGeorgeMatuskaClinicalLeadIntellectualDisabilities–
HEESouthofEnglandRegionalsoattendedthetrainingbringingthetotalofnumberofparticipants
to26. Feasibilityof the trainingwasassessedby thepercentageofeligibleparticipantswhowere
eventuallyenrolledinthetraining.37participantshadregisteredforthetrainingand26participants
attended(70.5%).Therewerevariousreasonsforwithdrawalsuchasillness,familyemergenciesand
someunexplained.AcceptabilitywasassessedbythepercentageofHCPswhocompletedallaspects
of the training as planned. All participants (100%) stayed for the duration of the training and
completedallaspectsofthetrainingasplanned.Theirprofessionsareindicatedinfigure6below.
FIGURE6:DESCRIPTIONOFPROFESSIONALSWHOATTENDEDTHETRAINING
Midwives
54%
SpecialistPaediatric
Nurses/Neonatal
Nurses/ANP
15%
Paediatrician/Neon
atologist/Trainee
15%
Sonographer
4%
Other
12%
Midwives SpecialistPaediatricNurses/NeonatalNurses/ANP
Paediatrician/Neonatologist/Trainee Sonographer
Other

47
AlthoughsomeparticipantshadnotyetstartedDDN,theyattendedthetrainingasthiswouldbe,a
futureintegralpartoftheirrole.Participantscompletedpreandpost-trainingquestionnaireswhich
assessedchangesintheirknowledge,attitudes,andskillsinDDNasaresultofthetraining.Ofthe26
participants,8HCPsagreedtoparticipateinsemi-structuredinterviewsfourweeksaftertraining.The
frequencyofDDNvariedamongparticipantsasshowninfigure7below:
FIGURE7:FREQUENCYOFDDNBYHCPS
Mostthetrainingparticipants34.6%(n=9)deliveredDNonafortnightlybasis.Thequantitativeand
qualitativephase2findingsarepresentedundertheTDFthatwererelevanttothestudyandwhich
emergedfromthedata.
6.2SOCIAL/PROFESSIONALROLESANDIDENTITYANDSOCIALINFLUENCES
Mostoftheinterviewparticipantsweremidwivesandmanyofthemexpressedtheirsenseofprivilege
atbeingabletoDDNtofamilies.Oftenthisaspectoftheirrolewasconsideredbothchallengingand
rewardinggiventhattheywereinvolvedinprovidinginformationtofamiliestoenablethemtomake
difficultdecisionswhenfoetalanomalieswereidentifiedprenatallyorhelpingthemtounderstand,
andadaptto,theimplicationsofspecificdisabilitiesfortheirchildandfamilylifeafterbirth.There
34.60%
23.10%
19.20%
11.50%
11.50%
0% 5% 10% 15% 20% 25% 30% 35% 40%
Fortnightly
Monthly
Biannually
Never
Weekly
PERCENT
FREQUENCYOFDDN

48
wasalsoaclearlystatedbeliefthatallHCPswhoDDNneededappropriatetrainingbecausehowthey
deliveredDNwasperceived asmaking a significant difference tohowparents responded to their
babiesandadjustedtotheirinfantintheearlydays.Only30.8%(n=8)ofthepilottrainingparticipants
indicatedthattheyhadreceivedsometraininginDDN.Themajority57.7%(n=15)statedthatthey
hadnotreceivedsuchtraininganddatawasmissingfortherestoftheparticipants11.5%(n=3)as
showninfigure8below:
FIGURE8:PREVIOUSTRAININGINDDN
ThetrainingaimedtogiveHCPstheopportunitytoreflectontheirprofessionalroleandhowthey
couldimprovetheexperiencesandoutcomesforfamiliesthatreceiveDN.Thedatasuggestthatthe
training was a useful social influence for changing clinical practice.Within the training, themost
powerfulinterpersonalinfluencesthatseemedtoaffecttheimpactofthetraininganditssubsequent
implementationinpracticeweretheparenttestimonyandcasestudies.Theinteractivenatureofthe
trainingwasalsomentionedasprovidingopportunitiesforattendeestoshareideasandexperiences
andtolearnfromeachother:
Ithinkevenjusthavingthetraining,thetrainingitselfispartofthesupportprocessbecauseyoumeet
otherpeopleinotherTrustswho,andotherprofessionsandyou,youknow,youlearnfromeachother.
(HCP4)
0% 10% 20% 30% 40% 50% 60%
PreviousDDNtraining
NoPreviousDDNTraining
Notstated
30.80%
57.70%
11.50%
PERCENT
HISTORYOFDDNTRAINING
49
HCPshighlightedseveralissueswhichwereperceivedaschallengingabouttheirroles.Forexample,
they highlighted that DNwas often tailored to families' unique circumstances and perceived and
actualexpectations,beliefs,andcapacityofindividualparents.HCPsspokeaboutthedifficultiesof
gaugingwhatparentswerereadyto,orwantedtohear,orknowinghowmuchinformationtoshare,
orinwhatorderitshouldbepresented:
It’sverydifficulttogetthebalancerightandI’veneverunderstoodformyself, Imean,IknowthatI
operatedifferentlyindifferentsituationsandIwillobservethewayI’mworkingwithawoman,witha
couple,orwithanextendedfamilywillchangedramatically,and,forexample,justtheverybasicthing
about…doIputtothemtheoptionofcontinuingthepregnancywiththesupportthat’stherefirst,or
doIputforwardtheoptionofendingthepregnancy,andhowdoIdecide…anddoesthatactuallymake
adifferencetowhattheyendupdoing,I’dbereallyinterestedtoknow.(HCP5)
Theseissueswereraisedinphase1andformedanintegralpartofthecurrenttraining.Therewere
severalsuggestionstostrengthenthetraining.Severalparticipants felt that itwouldbebeneficial,
althoughnot alwayspossible, to receive feedback from the families theyworkedwith inorder to
continuously improve theirpractice. Inaddition, therewereconcernsexpressedabout the lackof
supportforfamilieswhooptedtoterminateapregnancyandsuggestionstoincorporatethisinfuture
training:
I’msurethatwesaythingstoaladywhoterminates,thatresonateswiththemfortherestoftheirlife
aswell,I’msurethatthey,20yearsdownthelinestillrememberthatmidwifesayingsomethingthat
wasn’thelpful,…we’reonlyconcentratingontheoneswhohavechosentokeeptheirbabies.So,Ifeel
it’sjustashardforthoseladies,andIlookafteralotofthoseladies,andyouknow,thattheyhaveother
issues as to why they don’t want to keep their baby, that’s down to them, but we are negatively
impactingonthemlong-termbythethingsthatwesayandthebehavioursthatwehave.(HCP8)
Similartoourphase1findings,HCPsspokeaboutlearningfromthegood(andnotsogood)practice
ofothers:
IlearnteverythingIknewaboutDDNfromcolleagues,sofantasticcolleagues,brilliantcolleagues,but
Ilearnt,that’swhereIlearnteverything,bybasicallycopyingandlearningfromthem.(HCP8)
InviewofthisprevailingstyleoflearningamongHCPs,thepointwasraisedabouttheneedtobalance
DDNandgaugingtheappropriatetimetoaskparentsforpermissiontobeabletoteachmorejunior
staffaboutthemedicalconditionswhichtheirchildrenmaybediagnosedwith:
50
So,wehadthebabyontheresuscitaireandobviouslythenhadtodiscusstellingtheparentsbecause
theDadwascomingover.So,myselfandthepaediatricdoctorinvitedDadoverandcongratulatedhim
onthebirthofhisson,butitwastheobstetricsdoctorthatthencameoverandsaidtotheDad‘well,
obviously,youcanseethatthere’ssomethingwrongwithhishead.So,it’svery,veryrare,I’venever
seenanythinglikethisbefore,soI’dliketowriteacasestudyaboutyourson.(HCP6)
Inthescenarioabove,thejuniorHCPfeltthattheconsultantcouldhavewaitedandgiventhefamily
timetoprocesstheDNbeforeapproachingthemtomaketheirchildaninterestingcasestudy.
6.3KNOWLEDGE,SKILLSANDBELIEFSABOUTCAPABILITIES
The training aimed to enableHCPs to recognise the importanceof establishing the right physical,
emotional, social andenvironmental space todeliverDN. It alsoaimed toenableHCPs togainan
understandingoftheimportanceofplanningbeforeDDNincludingidentifyingtheappropriatetime
todeliverthenews,choosingtheappropriatelanguagetouseandtheappropriateinformationtogive
at initial and follow up discussionswith the family.We assessed the knowledge and attitudes of
participantswithregardstotheeffectofDDNonfamilies,theimportanceofempathy,thevarious
communicationstylesandtheHCPsconfidenceinDDNbeforeandafterthetraining.Followingthe
training,allparticipantsfeltmoreconfidentintheirabilitytoshareDNinacompassionate,responsive
andbalancedway.Someregretswereexpressedaboutthewaytheyinteractedwithparentspriorto
attendingthetraining:
IthinkIfeelkinder,Ifeelkindergivingtheinformation,Ifeel,um,yes,IwaskindbeforebutIfeeleven
kinder,thereweare.(HCP1)
…andthenyouget thissuddenonsetofguilt,becauseyoustart inyourheadyou immediatelystart
goingthroughallthesesituationswhereyou’vesaidthemthings,andyou’vealwayssaidthemwith
goodintentions,sowhenwe’vehadthedebateI’vesaidtothepeopleI’vespokento,don’tworry,Ifelt
thesame,Ifeltlike,ohno,I’vesaidthatbefore,ohno,Ishouldn’thavesaidthat,andohmygod,that
lady’sprobablygoingtorememberthatfortherestofherlife,sheprobablyis,butthere’snothingIcan
doaboutitnow,allIcandonowischangethelanguageIuse.(HCP8)
Thequantitativedatasupportedthequalitativefindingsandshowedthattherewereimprovements
inknowledgeabouttheeffectofDNonfamiliesandtheimportanceofempathywhencommunicating
DNasshowninfigure9below:
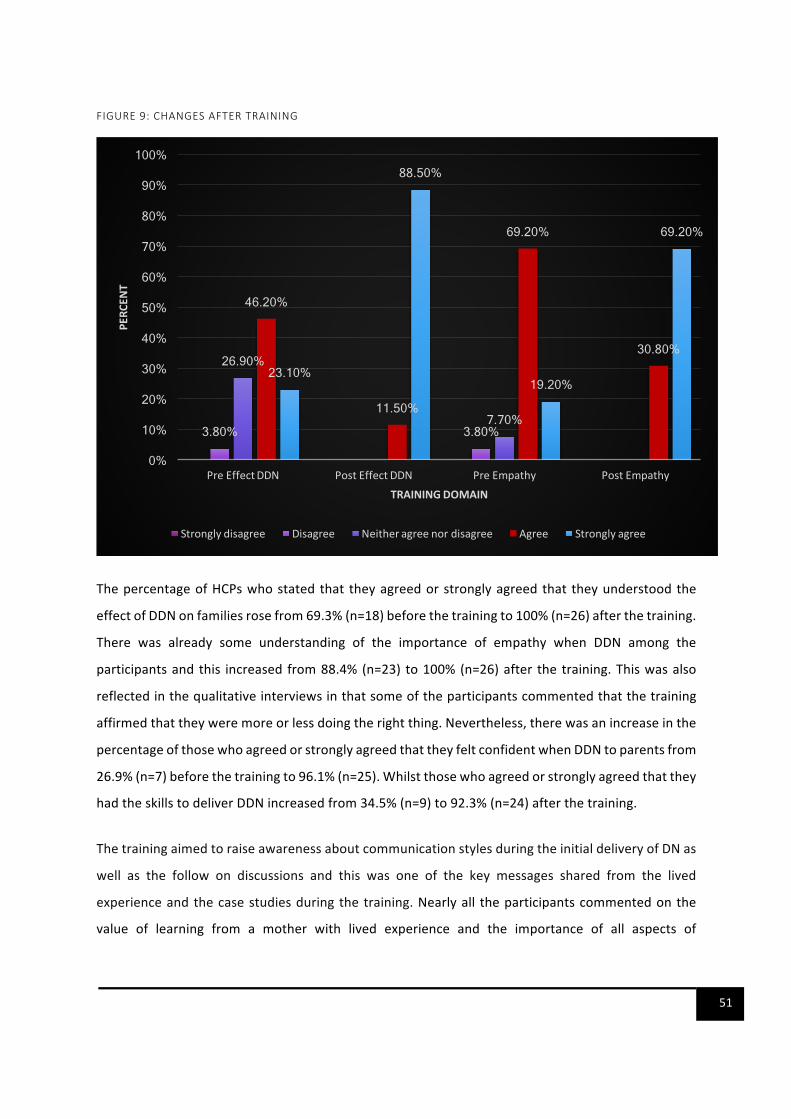
51
FIGURE9:CHANGESAFTERTRAINING
ThepercentageofHCPswhostatedthat theyagreedorstronglyagreedthat theyunderstoodthe
effectofDDNonfamiliesrosefrom69.3%(n=18)beforethetrainingto100%(n=26)afterthetraining.
There was already some understanding of the importance of empathy when DDN among the
participantsandthis increased from88.4%(n=23) to100%(n=26)after the training.Thiswasalso
reflectedinthequalitativeinterviewsinthatsomeoftheparticipantscommentedthatthetraining
affirmedthattheyweremoreorlessdoingtherightthing.Nevertheless,therewasanincreaseinthe
percentageofthosewhoagreedorstronglyagreedthattheyfeltconfidentwhenDDNtoparentsfrom
26.9%(n=7)beforethetrainingto96.1%(n=25).Whilstthosewhoagreedorstronglyagreedthatthey
hadtheskillstodeliverDDNincreasedfrom34.5%(n=9)to92.3%(n=24)afterthetraining.
ThetrainingaimedtoraiseawarenessaboutcommunicationstylesduringtheinitialdeliveryofDNas
well as the follow on discussions and this was one of the key messages shared from the lived
experienceandthecasestudiesduringthetraining.Nearlyall theparticipantscommentedonthe
value of learning from a mother with lived experience and the importance of all aspects of
3.80% 3.80%
26.90%
7.70%
46.20%
11.50%
69.20%
30.80% 23.10%
88.50%
19.20%
69.20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PreEffectDDN PostEffectDDN PreEmpathy PostEmpathy
PERCENT
TRAININGDOMAIN
Stronglydisagree Disagree Neitheragreenordisagree Agree Stronglyagree

52
communication, including thewords thatareused,and the toneandway informationwasshared
bothinthequalitativeinterviewsaswellasthequalitativecommentsmadeaspartofthepost-training
evaluation.Commentsweremadethatemphasisedthevalueofreplacingtheterm‘badnews'with
‘differentnews'anditwashopedthatthiswouldbecomethepreferredtermwhentalkingtoother
professionalsorrunningin-houseteachingsessions:
Toputitreallypractically,istonotsaybadnews,andtonotsayI’msorrybeforeyousayit,andto,
yeah,nottreatitassomethingthat’swrong…..theotherwordisrisk,weuseriskalot,andI’mtrying,
that’ssohard,becauseallourpaperworkanditisallourinformation,soandwe’resousedtosayingit,
soI’mtryingreallyhardtomoveawayfromrisk,butIcanbehonestwithyouandsaythatI’vefoundit
difficult.(HCP8)
Change in language, use the term different or unexpected news avoid words like risk and not to
apologise. Thinking about timing and environment. (HCP 9 Qualitative feedback from post-training
evaluationform)
Theemphasismadebytheparentwithlivedexperienceontheimportanceofworkinginpartnership
withfamilieswasalsomentionedasakeytake-homemessageandwasreflectedinthewaythatone
participantsubsequentlyengagedwithfamilies:
You'resteppingdownfromtakingthathierarchicalroleoftheprofessionalwhoknowseverythingand
thisishowwe'regoingtodoit,andyoukindofcomedowntotheleveloftheserviceuserandsayto
them,"Howdoyouwant...?",youknow,you'reincludingthem,"Howshallwedothis,whatcanwedo
toimprovethingsorhelpyourunderstanding?",orwhatever.(HCP2)
Aspartofthepost-trainingevaluation,participantswerealsoaskedabouthowtheywouldusethe
knowledgeandskillsfromthetrainingtochangetheirpractice.Mostresponseswerearoundadjusting
howtocommunicatewithparentsaswellassupportingthedisseminationofthecontentoftraining
toothercolleaguestosupportchangesintheirpractice:
Tospreadthenews.Ensureifthistraininggoesoutasmanykeypeopleaspossiblegettogoonit.I
work at 2 different trusts over different counties andwill; push for a similar thing in XXX (HCP 10
Qualitativefeedbackfrompost-trainingevaluationform)
Speaktoseniorsonhavingdepartmentalguidelinestofollow.(HCP11Qualitativefeedbackfrompost-
trainingevaluationform)

53
Usingtoday'sexperiencetoimprovethelanguageandenvironment.(HCP12Qualitativefeedbackfrom
post-trainingevaluationform)
I will organise teaching and training sessions for my junior doctors with my department. (HCP 13
Qualitativefeedbackfrompost-trainingevaluationform)
Similarcommentsweremadeinthequalitativeinterviewsaboutdisseminatingthetrainingtoensure
trustwidechangesinpractice.Othersuggestionswereaboutmakingotherchangesapartfromface
tofacecommunication.
Thereweresomeimmediatechangesinpracticewhichwerereportedbyparticipants,forexample,
oneparticipantreportedgoingbacktodiscusswiththeircolleaguesaboutchangingthestandardised
wordingoffollow-upemailssenttoparentsaftertheyreceivedaphonecallexplainingtheresultsof
theirtestsaswellasupdatingleafletsgiventoparents.
Actually,let'sstopusingthat,let'susethisoneinstead,soitjustgotustotalkaboutitratherthanus
goingonjustdoingwhatwe’vebeendoing,soitfreshenedwhatwedo,whichhasgottobegood.(HCP
5)
Therewereanumberofsuggestionsto improvethetraining includingmakingthetrainingsession
longerandincludingtheperspectivesofothercarers,suchasfathersandgrandparentssothatHCPs
also learnfromthese.Thesecommentswereraisedinthepost-trainingevaluationquestionnaires.
Oneparticipantalsoproposedthat futuretrainingsupportsHCPstoencourage families toexplore
theiroptionsfromthefundamentalfoundationoflovefortheirbabyandthemselves.
Yeah,Ithink,tome,thekeypoint,thekeymessage,thatIcomebacktooverandoveragaininthose
consultationsis,ifyoumakeadecisionbasedinlove,you'renotgoingtoofarwronganditalsoenables
youtolivewiththatdecisionbecausewhenyoulookback,iftheprimaryreasonyoumadethatdecision,
eithertocontinueortoendthepregnancy,isoutofloveforthatchildand,indeed,loveforyourself,
andloveforyourotherchildren,ifyouhaveany,thenhoweverdifficultitis,youknowyoudiditforthe
rightreason.(HCP5)
Overall,interviewparticipantsreiteratedanumberofcorecomponentsofDDNwhichwerealready
coveredinthecurrenttrainingandmadesuggestionswhicharehighlightedintherecommendations
sectionofthisreport.
54
6.4ENVIRONMENTALCONTEXTANDRESOURCES
Included under this heading are aspects of the training environment that were considered by
participantstoenhanceorimpedetheirlearningexperienceaswellasresourcesthatcouldbeused
in their workplace when DDN to families. Positive comments were made about the venue, the
refreshments,theatmosphere,theotherattendees,thefacilitators,themotherwithlivedexperience,
thecontentofthetrainingandthewayitwasdelivered.Thiswasalsoreflectedinthequantitative
data in that96.2%ofparticipants (n=25) agreed that the training covered topics relevant to their
practice;thatthecontentwaswellorganisedandeasytofollow;thatinteractionanddiscussionwere
encouragedduringthetraining.Dataweremissingforoneparticipant.Inthequalitativecomments
fromthepost-trainingevaluationandtheinterviews,participantsvaluedtheuseofthecasestudy
approach; learning from a lived experience, and the fact that the trainingwas relevant tomulti-
professionals and which allowed learning from others to occur. There were some conflicting
commentsaboutthelengthofthetraining:
Ithinkyoualwaysgetquitealotbackfromaserviceuser'spointofview,sotheladythatspokeabout
herowncasewithherchild,andIthink,youknow,asaprofessionalIgleanmorefromthatthanIdo
sometimesfromtheactualslidesandthePowerPointsandeverythingelse,becausethat'swhyI'mdoing
whatIdo,Iwanttomakeitrightandasgoodasitcanbeforthepatients.So,IthinkIgotthemostout
ofherinput,actually.(HCP2)
Thescenarioswherewedidgoingroups,thatwasreallyniceasitwasn'tparticularlythreateningina
senseofyouhavetoansweritallbecauseitwasopeneduptothereal…thewholegroup,actuallyI
reallylikedthatandhearingdifferentpeople'sopinionswasreallygood.(HCP3)
I,wellIlikethefacttherewassuchacross-sectionofprofessionals,differentprofessions,soIthought
thatwasreallygood.Becauseoftentheseeventsyouhaveallmidwivesorallsonographersbutthere
weredoctorsandsomeonefrommentalhealthservicesandit'sjustgreatwhenyougetlotsofdifferent
peopletogether.(HCP4)
Ithinktohaveahalfdayisreallyeffectivebecausepeople,wellIfeltlikeIcouldreallyfocusforthose
fewhoursandthenbecauseIknowsometimesifit’safulldayoftrainingyoucangetalittlebittired
andthenyou,youknow,afterlunch,youfindyouloseabitoffocus.(HCP7)
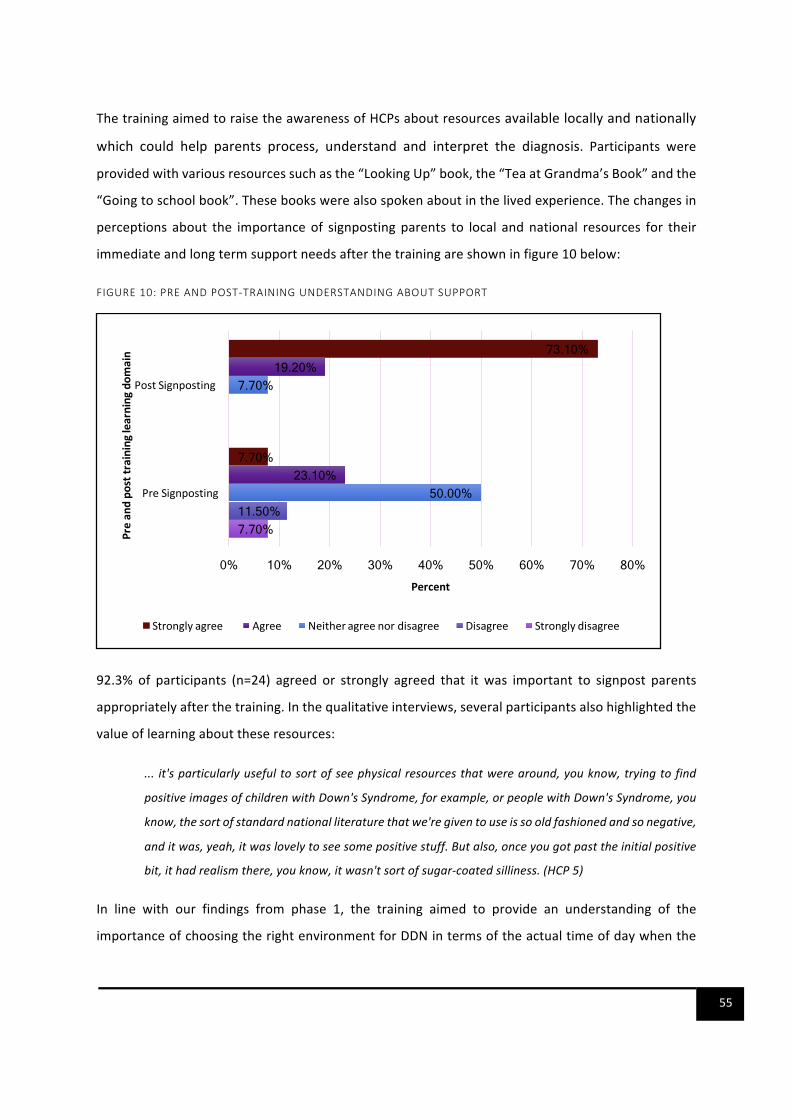
55
ThetrainingaimedtoraisetheawarenessofHCPsaboutresourcesavailablelocallyandnationally
which could help parents process, understand and interpret the diagnosis. Participants were
providedwithvariousresourcessuchasthe“LookingUp”book,the“TeaatGrandma’sBook”andthe
“Goingtoschoolbook”.Thesebookswerealsospokenaboutinthelivedexperience.Thechangesin
perceptions about the importanceof signpostingparents to local andnational resources for their
immediateandlongtermsupportneedsafterthetrainingareshowninfigure10below:
FIGURE10:PREANDPOST-TRAININGUNDERSTANDINGABOUTSUPPORT
92.3% of participants (n=24) agreed or strongly agreed that it was important to signpost parents
appropriatelyafterthetraining.Inthequalitativeinterviews,severalparticipantsalsohighlightedthe
valueoflearningabouttheseresources:
... it'sparticularlyusefultosortofseephysicalresourcesthatwerearound,youknow,tryingtofind
positiveimagesofchildrenwithDown'sSyndrome,forexample,orpeoplewithDown'sSyndrome,you
know,thesortofstandardnationalliteraturethatwe'regiventouseissooldfashionedandsonegative,
anditwas,yeah,itwaslovelytoseesomepositivestuff.Butalso,onceyougotpasttheinitialpositive
bit,ithadrealismthere,youknow,itwasn'tsortofsugar-coatedsilliness.(HCP5)
In line with our findings from phase 1, the training aimed to provide an understanding of the
importanceofchoosingtherightenvironmentforDDNintermsoftheactualtimeofdaywhenthe
7.70% 11.50%
50.00%
7.70%
23.10%
19.20%
7.70%
73.10%
0% 10% 20% 30% 40% 50% 60% 70% 80%
PreSignposting
PostSignposting
Percent
Preandposttraininglearningdomain
Stronglyagree Agree Neitheragreenordisagree Disagree Stronglydisagree
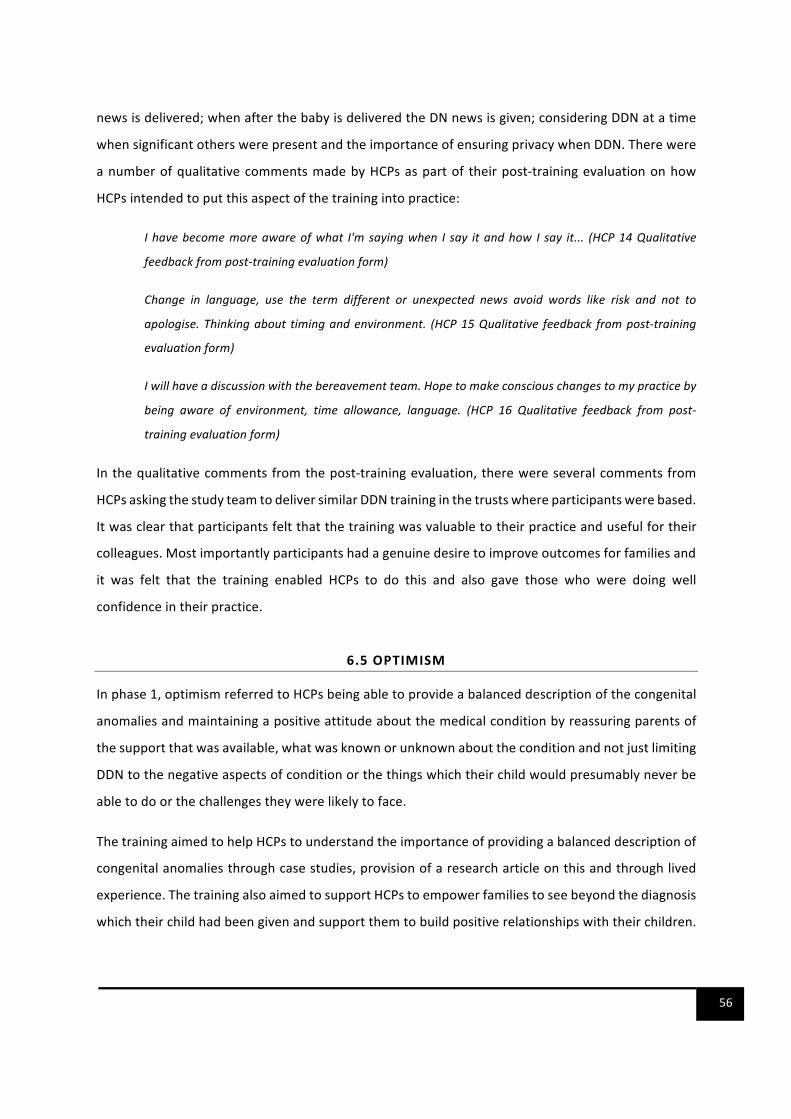
56
newsisdelivered;whenafterthebabyisdeliveredtheDNnewsisgiven;consideringDDNatatime
whensignificantotherswerepresentandtheimportanceofensuringprivacywhenDDN.Therewere
anumberofqualitativecommentsmadebyHCPsaspartof theirpost-trainingevaluationonhow
HCPsintendedtoputthisaspectofthetrainingintopractice:
Ihavebecomemoreawareofwhat I'msayingwhen I say itandhow I say it... (HCP14Qualitative
feedbackfrompost-trainingevaluationform)
Change in language, use the term different or unexpected news avoid words like risk and not to
apologise.Thinkingabout timingandenvironment. (HCP15Qualitative feedback frompost-training
evaluationform)
Iwillhaveadiscussionwiththebereavementteam.Hopetomakeconsciouschangestomypracticeby
being aware of environment, time allowance, language. (HCP 16 Qualitative feedback from post-
trainingevaluationform)
Inthequalitativecommentsfromthepost-trainingevaluation,therewereseveralcommentsfrom
HCPsaskingthestudyteamtodeliversimilarDDNtraininginthetrustswhereparticipantswerebased.
Itwasclearthatparticipantsfeltthatthetrainingwasvaluabletotheirpracticeandusefulfortheir
colleagues.Mostimportantlyparticipantshadagenuinedesiretoimproveoutcomesforfamiliesand
it was felt that the training enabled HCPs to do this and also gave those who were doing well
confidenceintheirpractice.
6.5OPTIMISM
Inphase1,optimismreferredtoHCPsbeingabletoprovideabalanceddescriptionofthecongenital
anomaliesandmaintainingapositiveattitudeaboutthemedicalconditionbyreassuringparentsof
thesupportthatwasavailable,whatwasknownorunknownabouttheconditionandnotjustlimiting
DDNtothenegativeaspectsofconditionorthethingswhichtheirchildwouldpresumablyneverbe
abletodoorthechallengestheywerelikelytoface.
ThetrainingaimedtohelpHCPstounderstandtheimportanceofprovidingabalanceddescriptionof
congenitalanomaliesthroughcasestudies,provisionofaresearcharticleonthisandthroughlived
experience.ThetrainingalsoaimedtosupportHCPstoempowerfamiliestoseebeyondthediagnosis
whichtheirchildhadbeengivenandsupportthemtobuildpositiverelationshipswiththeirchildren.

57
Inthepost-trainingquestionnaires,significantchangeswereobservedinthedomainofunderstanding
howtoprovideabalanceddescriptionofaconditiontoparents.Whilstonly19.2%(n=5)agreedor
stronglyagreedthattheyknewhowtoprovideabalanceddescriptionofcongenitalconditionsbefore
thetraining,thisincreasedto86.5%(n=23)afterthetrainingasshowninfigure11below:
FIGURE11:CHANGESINKNOWLEDGEABOUTBALANCEDDESCRIPTION
Hearing from a mother about the reality of looking after a child with a congenital anomaly was
reportedashelpingHCPs tobemorepositiveabout that specific congenital anomalyand tohave
greaterconfidenceabouttalkingtomothersabouttheiroptions.Seeingpicturesofdifferentchildren
withDown’ssyndromeforexamplefromtheresourceswhichwereprovidedandhearingabouttheir
liveswerealsomentionedasausefulwayofappreciatingindividualism,thespectrumofabilityand
theneedtofocusonwhatchildrencoulddoratherthanwhattheywouldnotbeabletodo:
So,it’sreallygoodtohearaparent’sperspectivebecausewhenyouhearactuallythatit’s,itwasokay
forher, itwasreallyhardwhen,whenwomenarereallythathonestabouthowdifficult itwas,that
actuallythey’vecomethroughitand,um,youknow,whenthey’reontheothersidethey,youknow,
11.50% 15.40%
53.80%
11.50% 15.40%
42.30%
3.80%
46.20%
0%
10%
20%
30%
40%
50%
60%
PreBalancedDescription PostBalancedDescription
PERCENT
TRAININGDOMAIN
Stronglydisagree Disagree Neitheragreenordisagree Agree Stronglyagree
58
thisisokay,tellparentsit’sgoingtobeokay,youhavetheconfidencetoreallybelieveinthatwhenyou
tellparents.(HCP4)
Ididn’trealiseit,butIhadsomepreconceivedideasbeforeIreadthearticle,sothearticlewasfantastic,
Igotareal…Ithinkthatwassuchagoodthing,becauseIdidhavesomepreconceivedideasthatIdidn’t
evenrealiseIhaduntilIreadthearticle,itsparkedalittledebate,anditmadememuchbetterprepared
forwhatweweregoingtocomeacross,andit'smademestarttothinkaboutmypracticealready,so
whenIhavearrivedatyourtrainingprogramme,Ihadalreadystartedthinkingabouttheconceptsthat
youwantedtotalkaboutandhowI,Ialwaysstartedtothink,ohmygod,Ihavesaidtosomeone,I've
gotsomebadnewsforyou,andIhavesaidthesethings,andstartedtothinkaboutmypractice,and
howit'srelevant,soonthedaywhenyoustarttoaskpeople,you'vealreadyhadathinkaboutthem.
Soyeah,I'dsaythatwasmuch,IfoundthatveryusefulandIwishmoreofthestudydaysI'vebeenon
haddonethat.(HCP8)
While a fewHCPswere concernedaboutbeingover-optimistic and givingparents falsehope, the
resourcessharedatthetrainingwereperceivedasusefulinthattheyshowedsomeofthechallenging
timesthatfamilieswentthroughbutalsoshowedsomeoftheirtriumphsandabilitytoenjoythings
which other families enjoyed which provided a balanced description of the raising a child with
congenitalanomalies.Themainsuggestionforenhancingthisaspectofthetrainingwastoalsoinclude
resourcesforvariouscongenitalanomalies.
6.6BELIEFSABOUTCONSEQUENCES
Whileinphase1,beliefsaboutconsequencesweremainlytodowithhowDNimpactedfamilies,in
phase2,thiswasalsoaboutthepotentialpositiveimpactofhavingtrainedHCPsdeliverDNonthe
outcomesandexperiencesoffamiliesreceivingDN:
Ithoughtitwasreallyusefultounderstandhowmuchoftheconversationtheyremember,soknowing
thatthefirstsortofminuteisthekindof,whenthey’rereallyfocusedandifyougivethemanynews
thattheyweren’texpectingthatwasdifferenttowhattheirexpectationswerethenactuallytheymight
switchoffafterthefirstminuteorso.Andthenalsothattheyreallyremembersortoflikethetoneand
thewayinwhichtheywerespokento,sotoalwaysgoinandgivethemtherespectthatthismightbe
oneofthefewinteractionsandthey’llrememberitlongerthanyoueverwill.(HCP7)

59
It sentme awaymore determined to do prettymuch what I'm doing anyway and to go on really
weighingeverywordthatIusewithwomenandwithfamilies,becauseunderstandinghowdesperately
importantthatistothem,andthosewordswillbeetchedontheirsouls.(HCP5)
Intermsoftheconsequencesofthetraining,theexpectedoutcomesrelatednotonlytothepractice
andimpactofindividualhealthprofessionalsattendingthetrainingbutalsototheextenttowhich
thetrainingcouldberolledoutandembedded inthepracticeenvironmentsof theattendeesand
otherHCPsingeneral.TherewereseveralsuggestionsaboutensuringthattheHCPsresponsiblefor
drivingtheagendaforwardremainedsupportedandmotivated;thattheinfrastructurerequiredfor
supportingtheestablishmentofprotocolsandpoliciesforeffectivelyDDNwere inplacetoensure
consistent,safeandbalancedpractice.Thereweresuggestionsaboutthedevelopmentofanetwork
oflocaltrainersabletodeliverinformative,up-to-dateDDNtraining:
Ithinkiftherewassomekindofliketeachingpackageresources,thatcouldbeusedatthelocallevel,
thatwouldbereallyusefulwhetherit'svideosor,videosarereallypowerfulandjusteasytodistribute.
Butitneedstobe,insmallerbitesizechunksifyoulikethatyoucandeliver…youknowIcansneak,we
havemandatory training for example thatwehave todeliver but you can sneak in tenminutes on
anothertopic,soit'squiteagoodwayoflikefeedingthatin.(HCP4)
…becauseyouknowyoucan’tchangethewholeworldbyteachingeveryindividualpersonseparately,
we’renevergoingtogetthere,we’vegottostartchangingcultures.Ithinkwe’veactuallydonequitea
lotandI’mquitepositiveaboutthewaywe’vechangedtheuseoflanguage,toaverylargeextentfrom
theuseofthewordrisktothewordchance.(HCP5)
6.7EMOTION
ThetrainingaimedtoallowHCPstorecognisetheimportanceofregularpersonalsupportandhow
thiscontributestotheirownmentalwellbeing.Therewasaunanimousacknowledgmentbyallthe
participantsoftheemotionalchallengesofsupportingfamiliesfacingdifficultdecisionsoruncertain
futures,especiallywhenthedecisionsthatsomefamiliesmadeweredifficulttoreconcilewiththe
HCPsownbeliefs.Theneedforasupportivenetworkinordertoreducestressandavoidburn-outwas
mentioned by several of the participants, so the session in the training programme on novel
approachestobuildpractitionerresiliencewasalsoconsideredhelpful.
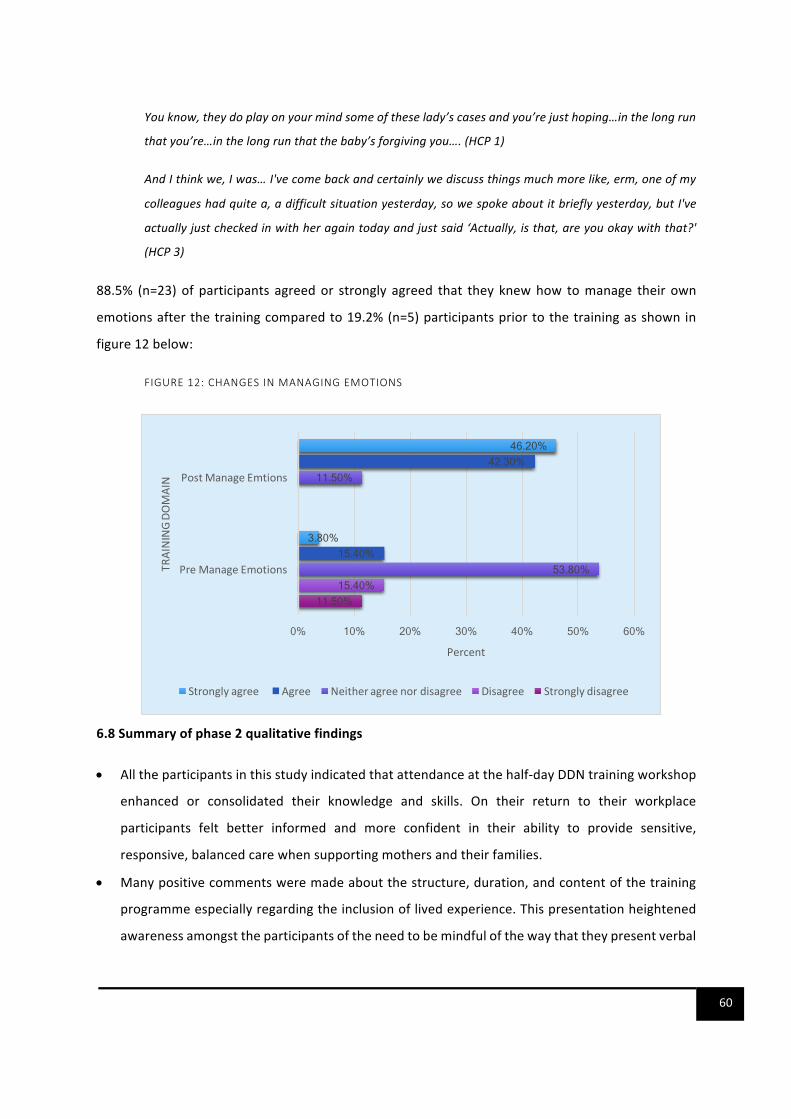
60
Youknow,theydoplayonyourmindsomeoftheselady’scasesandyou’rejusthoping…inthelongrun
thatyou’re…inthelongrunthatthebaby’sforgivingyou….(HCP1)
AndIthinkwe,Iwas…I'vecomebackandcertainlywediscussthingsmuchmorelike,erm,oneofmy
colleagueshadquitea,adifficultsituationyesterday,sowespokeaboutitbrieflyyesterday,butI've
actuallyjustcheckedinwithheragaintodayandjustsaid‘Actually,isthat,areyouokaywiththat?'
(HCP3)
88.5% (n=23)of participants agreedor strongly agreed that they knewhow tomanage their own
emotionsafterthetrainingcomparedto19.2%(n=5)participantspriortothetrainingasshownin
figure12below:
FIGURE12:CHANGESINMANAGINGEMOTIONS
6.8Summaryofphase2qualitativefindings
• Alltheparticipantsinthisstudyindicatedthatattendanceatthehalf-dayDDNtrainingworkshop
enhanced or consolidated their knowledge and skills. On their return to their workplace
participants felt better informed and more confident in their ability to provide sensitive,
responsive,balancedcarewhensupportingmothersandtheirfamilies.
• Manypositivecommentsweremadeaboutthestructure,duration,andcontentofthetraining
programmeespeciallyregardingtheinclusionoflivedexperience.Thispresentationheightened
awarenessamongsttheparticipantsoftheneedtobemindfulofthewaythattheypresentverbal
11.50% 15.40%
53.80%
11.50%
15.40%
42.30%
3.80%
46.20%
0% 10% 20% 30% 40% 50% 60%
PreManageEmotions
PostManageEmtions
Percent
TRAININGDO
MAIN
Stronglyagree Agree Neitheragreenordisagree Disagree Stronglydisagree
61
andwritteninformationtoparents,notonlyintermsofthewordsthatareusedandthetoneand
manner in which they are shared, but also with regard to the way that evident or potential
disabilitiesareperceivedanddescribed.
• Participants also acknowledged the emotional impact on HCPs of supporting families making
difficultdecisionsandtheneedtohavesupportfromcolleaguesaswellasawarenessofstrategies
tosupporttheirownwell-being.
7. DISCUSSION
7.1 KEYFINDINGS
OurstudyfindingsindicatethatreceivingDNwasasignificantlifeeventassuch,parentsremembered
invividdetail,howtheyreceivedDN,includingthetoneofvoiceoftheHCP,privacyaffordedthem
whenthenewswasdelivered,thequestionstheywereasked,thewordsusedtodescribetheirchild;
thecaregiventothem,theposturetakenbytheHCPs;thetimethatthenewswasdeliveredandthe
levelofpreparationthattheHCPhadtaken.Howthenewswasdeliveredhadasignificant impact
upon;theparent’sabilitytocopewiththenews,theiremotionalandmentalwellbeing,theparent-
childrelationship,theparents’relationshipwithoneanotherandtherelationshipbetweenthefamily
and the professionals as highlighted in previous studies [5, 33, 39, 44, 45, 47-52]. Two of these
previous studies showeda clear correlationbetweenmaternal anxietyand the focusof the initial
conversationwhenHCPshaddelivereddifferentnews,thushighlightingtheimportanceofhowDNis
delivered[44,48].Thesefindingssuggestthat it is important forallHCPs involved inDDNtohave
trainingwhichreflectstheneedsofthefamiliesthathavelivedexperienceofreceivingDN.
TheprocessofDDNwassometimeschallengingforHCPsparticularlyassomehadlimitedexperience
andtrainingtocomplementobservingseniorcolleaguesperformthetask.Duetolackofstandardised
trainingonDDNaswellaslackofpolicytoguideprofessionalsonthis,therewassignificantvariation
in the way that DN was delivered by HCPs. Other authors have also reported on this significant
variationinhowDNisdelivered[5,6].GiventhesignificantimpactofhowDNisdeliveredaswellas
thesignificanceoftheDNitself,parentsandHCPsmadeimportantsuggestionsaboutthecontentsof
a training intervention. These suggestions included training needs to equipHCPs to; demonstrate
empathy,showcompassion,beflexiblewithtimeorplanaroundthedemandsoftheirward,utilise
kind,simpleandtruthfullanguage;provideabalanceddescriptionofthecondition;offersufficient

62
time to answer questions and knowwhen andwhere to refer families on to for further care and
support.ThesekeyaspectsofDDNhavealsobeenhighlightedinotherstudiesascrucialforminimising
thenegativeimpactofreceivingDNonparents[5,47,48,50-52].
WedrewontheBCW[16,22]todevelopthetraininginterventionwhichincorporatedthesuggestions
fromfamiliesandHCPs.Wepilotedtheinterventionwithagroupof26HCPs.Thetrainingintervention
wasacceptable.AcceptabilitywasmeasuredbythepercentageofHCPswhocompletedthecourseas
planned.Onbothtrainingdays,allparticipantscompletedallaspectsofthetrainingandstayedfor
thedurationofthetraining.WealsofoundthatitwasfeasibletorecruitHCPstoattendthetraining
viaNHStrustsandHEEnetworks.Furthermore,itwasbothfeasibleandacceptabletomakeuseof
reallifescenariosinthecasestudiesalongsidelearningfromthevoiceofparentswithlivedexperience
insession.Theseaspectsofthetrainingwereverywellreceivedandperceivedasanintegralpartof
thelearningexperiencebyparticipants.
All participants indicated that attendance at the half-day DDN training workshop enhanced or
consolidatedtheirknowledgeandskills,thatitcoveredtopicswhichwererelevanttotheircurrent
practiceandthattheywouldrecommendthetrainingtotheircolleagues.Participantscouldhighlight
specificwaysthattheycouldchangetheirpracticebasedonwhattheyhadlearnedfromthetraining.
Ontheirreturntotheirworkplaceparticipantsfeltbetterinformedandmoreconfidentintheirability
to provide sensitive, responsive, balanced care when supporting families. Several HCPs reported
practicalchangeswhichtheyhadalreadymadeintheirdailypracticeasaresultofthetraining.We
foundthattheuseoftheBCWandspecificallytheuseoftheTDFinguidingthedevelopmentofthe
interventionwasusefulindevelopingtrainingwhichaddressedsomeofthechallengesandbarriers
toDDNeffectively.Thereportedchangesinpracticesuggestthattheoreticallydriveninterventions
maybeusefulinchangingclinicalpractice.
7.2LESSONSABOUTDATACOLLECTIONMETHODS
Weconductedatwo-phasestudytodevelopandpilotatraininginterventiontoimprovethedelivery
ofDNtofamiliesbyHCPs.Phase1wasqualitativeinnature.Likeotherqualitativestudies,thisdesign
allowedin-depthdescriptionofthelivedexperiencesofparentsandHCPs,however,thesmallsample
size inherent in qualitative studiesmeans that the findings from the studywill be transferable to
similar populations and not generalisable [14]. Phase 2 was not powered to detect statistical

63
significance however, we were able to assess the acceptability and feasibility of the training
intervention as well as changes in knowledge, skills, and attitudes about DDN. Despite these
limitationsinthemethods,thestudywaswelldesigned,answeredanumberofsignificantquestions
onhowto improvethedeliveryofDNbyHCPs intheUK.Thefollowing lessonswere learnt inthe
processofsettingupthestudyanddatacollection:
• Itwasimportanttoobtainlocalbuy-infromserviceleadsintheNHStrustsastheirendorsement
ofthestudyhadimplicationsforthesuccessfulrecruitmentofHCPsandfamiliesintothestudy.
• We included two parents with lived experience in the research team to facilitate effective
research design; optimise community sensitisation and engagement and to ensure that our
study reflected theneedsandexperiencesof familieswith the livedexperienceof receiving
differentnews.Theparentsactivelycontributedtodiscussionsonthefeasibilityofproposed
designsandhighlightedmethodstorefinetheproposal, the interviewguides,consentforms
andparticipantinformationsheetsforthefamiliesaswellasrecruitmentoffamiliesintothe
study.TheparentswerefromtheCornwallDown’sSyndromeSupportGroup,acharityrunby
familiesaffectedbyDown’sSyndromeinCornwall.
• The setup of the study including obtaining occupational health clearance for the NHS and
completingDBSchecksinordertohavethenecessaryhonorarycontractstoallowourresearch
teamtoconductresearchwithintheNHStooklongerthanwasanticipated.Thisdelayedthe
study.Otherresearchersmayfindithelpfultobelessoptimisticaboutthetimescalesforsuch
approvalstoensurethattheirstudiesruntotimeandbudget.
• WehadaslowstarttotherecruitmentoffamiliesasNHSstaffindicatedthatthefamilieswere
hardtoreach.Wefounditusefultoalsorecruitfamiliesintothestudyviacharitiesaswellas
localsupportgroups.
7.3RECOMMENDATIONS
The study findings suggest several potential research and training opportunities. It would be
important to ensure that the voice of parentswith lived experience remains part of these future
opportunitiessothattrainingcontinuestoreflecttheselivedexperiencesandthepossiblelongterm
impactonfamilies.Inviewofthis,wemakethefollowingrecommendationswithregardstofuture
research,thetrainingcontentaswellasrollingthisout.

64
7.3.1FUTURERESEARCH
Weconductedasmallstudytoassessthe feasibilityandacceptabilityofa training interventionto
improve thedeliveryofdifferentnews to families.We recommend thatHEEworkingacrossKent,
Surrey,andSussexsupporttheconductofa largerdefinitivelarge-scaletrialasanimportantnext
step.Thisstudycouldlookattheimplementationofthetraininganditsimpactonfamilyoutcomes.
The studycouldanswerquestionsabouthowhavingHCPswhohavebeen trained todeliverDDN
mightimprovetheemotionalresponseandmentalwellbeingofparentsimmediatelyafterthenews
isdeliveredandinsubsequentmonths.
Otherstudieshaveshownthatparentsmaytakesixormoremonthstoadjusttothenewsandto
developtheemotionalresiliencetoenablecommonfamilyfunction[44].Across-sectionalsurveyof
parentsfoundthatoveraperiodofsixmonths,parentswhowerewellsupportedandhadaccessto
appropriate informationwhen theyneeded it, adjustedwell to thediagnosis; showedpatternsof
resilience;hadreducedsymptomsofanxietyanddepressionandanimprovedqualityoflife[46].It
wouldbeusefultocompareifhavingsupportive,DDNtrainedstaffcanshortenthelengthoftimeit
takesparentstoadjusttothenewsandmitigatetheimpactthatthishasontheiremotional,mental
andfamilywellbeingaswellas thepotential longtermeffectsperinatalmentalproblemsonboth
parentsandchildren.
Itwouldbeimportanttoensurethatfamilieswithlivedexperiencesremainpartofresearchteams
thatconductthesefuturestudiesastheirinsightonthestudydesignandrecruitmentprocesseswould
becrucialforthesuccessofthestudies.
7.3.2TRAININGCONTENT
Thecurrent trainingemphasises theuniquepositionwhichHCPshave inbeingable to shapehow
parentsstarttheiroftenunexpected journey.BasedonthefindingsfromPhase2,werecommend
thatthetrainingisstrengthenedbyaddingthefollowingaspects:
• Including the livedexperienceof a fatherof a childwithadisability; a youngpersonwith
Down’sSyndromeorothercarerssuchasagrandparent;
• Includingtheperspectivesofparentsofchildrenwitharangeofdisabilities.

65
• Incorporatewaystosupportfamiliesthatchoosetoterminateapregnancybasedonfoetal
anomalyscreening.
• ExploringwaysofseekingfeedbackfromparentswhohavereceivedDNregardingthebest
waysofimprovingserviceprovision.
• Useofvideos,audiosonhowotherpeopledeliverandreceiveDN.
7.3.3ESTABLISHMENTOFPOLICIESANDPROTOCOLSONDDN
In order to close the gap between evidence and practice,we recommend that HEE KSS uses the
findingsfromthisstudyandanyfollowonstudiestolobbythedevelopmentofcomplementarypolicy
to ensure that DDN training becomes part of mandatory training for relevant NHS staff. This
infrastructurewouldsupportlargescalerollingoutofthetrainingtoallstaff.
WealsorecommendtheestablishmentoflocalprotocolsandpoliciesforeffectivelyDDNinNHStrusts
to ensure consistent, safe and balanced practice. These protocols and policies will address the
variationinpracticewhichwasreportedbyvariousstudyparticipants.
7.3.4ROLLINGOUTTHETRAINING
Followingonfromthelargerdefinitivestudy,werecommendthatthetrainingisrolledoutonalarge
scaleinordertoaddresstheunmetneedfortraininginDDN.Theproposaltorolloutthetrainingto
HCPswhoDDNonalargescalewasenthusiasticallyendorsedbyparentsandHCPsinboththephases
ofthestudy.
Werecommendacascademodelof trainingwhich involves theappointmentanddevelopmentof
localDDNchampionstoensurethatthereisongoingup-to-dateevidencedbasedlocalsupportfor
HCPswhodeliverdifferentnews.Asimilarmodelhadbeenusedbythe iHVfor itsaward-winning
perinatalmentalhealthtraining.Thistraininghasbeenrunningfor5yearsandthrough itsunique
Championcascademodel,ithasreachedtensofthousandsofpractitioners,including,butnotlimited
to;healthvisitors,midwives,psychiatrists,mentalhealthnurses,socialworkers,generalpractitioners,
and third sector practitioners. These professionals then implement their learning into everyday
practice.TheInstitutehastrainedover1650multi-agencyperinatalandinfantmentalhealth(PIMH)
championswho,afterattending the Institute training,goon tocascade it to their colleagues.The
PIMH Champions receive continued support for their role as local leaders from the Institute via;

66
regionalfacetofaceforums,anannualconferenceandalsothroughresourcesandnationalupdates
madeavailabletothemthroughthementalhealthsectionoftheiHVwebsite.TheDDNtrainingcould
useasimilarmodeltodevelopanetworkofchampionswhoserolewouldincludecascadingtraining
to practitioners. These champions could be also be equipped with electronic teaching
package/resourcesforrollingoutthetrainingincluding‘bite-sizechunks'forthosewhomaynotbe
abletoattendahalf-daytraining.
WerecommendthattheparentvoiceremainsakeyaspectofthetrainingasHCPsfound learning
fromlivedexperiencesasintegraltothemunderstandingtheimpactofDNonfamiliesaswellashow
itisdeliveredtofamilies.
8. CONCLUSION
TheDDN training has the potential to provide essential skills toHCPswhodeliverDN to parents.
EquippingHCPswiththenecessaryskillstoeffectivelydeliverDNmayreducethenegativeimpactof
thenewsonparents,families,andHCPs.Ifdeliveredwell,thereispotentialtominimisethedistress,
anxiety,anddepressionassociatedwithreceivingdifferentnews.Theimprovedmentalwellbeingand
adjustmentofparentswillalsoaffectthementalhealthoftheirchildrenwhichrepresentsakeyaspect
of the prevention of mental ill health across the life course. The significant improvements in
confidenceandskillsreportedbyHCPsafterthetrainingsuggestthatthetrainingmaybeeffectivein
providingtheaspectsofDDNthatparentssharedasbeingessentialforminimisingthenegativeimpact
ofthenews.GiventhepaucityofthisspecifictrainingforHCPs,theDDNtrainingwillfillasignificant
gapintrainingneedsandprovidesupporttoHCPstoimproveoutcomesforfamilieswhoreceiveDN.
67
REFERENCES
1. NHS,FetalAnomalyScreeningProgrammeStandards2015-2016.2016,NHSScreeningProgrammes:London.https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/421650/FASP_Standards_April_2015_final_2_.pdf
2. Morris,J.andA.Springett,TheNationalDownSyndromeCytogeneticRegisterforEnglandandWales2012AnnualReport.2014.
3. Wernovsky,G.,A.J.Shillingford,andJ.W.Gaynor,Centralnervoussystemoutcomesinchildrenwithcomplexcongenitalheartdisease.CurrentOpinioninCardiology,2005.20(2):p.94-99.
4. Aein,F.andM.Delaram,GivingBadNews:AQualitativeResearchExploration.IranianRedCrescentMedicalJournal,2014.16(6).
5. Luz,R.,etal.,Breakingbadnewsinprenatalmedicine:aliteraturereview.JournalofReproductiveandInfantPsychology,2017.35(1):p.14-31.
6. RoyalCollegeofNursing,Breakingbadnews:supportingparentswhentheyaretoldoftheirchild’sdiagnosisRCNguidancefornurses,midwivesandhealthvisitors.2013.
7. Deater-Deckard,K.,Parentingstressandchildren'sdevelopment:Introductiontothespecialissue.InfantandChildDevelopment,2005.14(2):p.111-115.
8. Hoffman,C.,D.M.Dunn,andW.F.M.Njoroge,ImpactofPostpartumMentalIllnessUponInfantDevelopment.CurrentPsychiatryReports,2017.19(12):p.6.
9. Drury,S.S.,L.Scaramella,andC.H.Zeanah,TheNeurobiologicalImpactofPostpartumMaternalDepression:PreventionandInterventionApproaches.ChildandAdolescentPsychiatricClinicsofNorthAmerica,2016.25(2):p.179-+.
10. Stein,A.,etal.,Effectsofperinatalmentaldisordersonthefetusandchild.Lancet,2014.384(9956):p.1800-1819.
11. vonElm,E.,etal.,TheStrengtheningtheReportingofObservationalStudiesinEpidemiology(STROBE)Statement:Guidelinesforreportingobservationalstudies.InternationalJournalofSurgery,2014.12(12):p.1495-1499.
12. Hopewell,S.,etal.,CONSORTforreportingrandomizedcontrolledtrialsinjournalandconferenceabstracts:Explanationandelaboration.PlosMedicine,2008.5(1):p.48-56.
13. CASP.Makingsenseofevidenceaboutclinicaleffectiveness:10questionstohelpyoumakesenseofqualitativeresearch.2010;Availablefrom:text-autospace:none">http://www.casp-uk.net/.
14. Ritchie,J.andJ.Lewis,Qualitativeresearchpractice:aguideforsocialsciencestudentsandresearchers.2003,Sage.
15. Craig,P.,etal.,Developingandevaluatingcomplexinterventions:thenewMedicalResearchCouncilguidance.BritishMedicalJournal,2008.337(7676).
16. Michie,S.,M.M.vanStralen,andR.West,Thebehaviourchangewheel:Anewmethodforcharacterisinganddesigningbehaviourchangeinterventions.ImplementationScience,2011.6.
68
17. Seguin,M.,etal.,Self-samplingkitstoincreaseHIVtestingamongblackAfricansintheUK:theHAUSmixed-methodsstudy.HealthTechnologyAssessment,2018.22(22):p.VII-+.
18. Fleming,A.,etal.,Antibioticprescribinginlong-termcarefacilities:aqualitative,multidisciplinaryinvestigation.BmjOpen,2014.4(11).
19. Debono,D.,etal.,ApplyingtheTheoreticalDomainsFrameworktoidentifybarriersandtargetedinterventionstoenhancenurses'useofelectronicmedicationmanagementsystemsintwoAustralianhospitals.ImplementationScience,2017.12.
20. Atkins,L.,etal.,AguidetousingtheTheoreticalDomainsFrameworkofbehaviourchangetoinvestigateimplementationproblems.ImplementationScience,2017.12.
21. Cane,J.,D.O'Connor,andS.Michie,Validationofthetheoreticaldomainsframeworkforuseinbehaviourchangeandimplementationresearch.ImplementationScience,2012.7.
22. Michie,S.,etal.,TheBehaviorChangeTechniqueTaxonomy(v1)of93HierarchicallyClusteredTechniques:BuildinganInternationalConsensusfortheReportingofBehaviorChangeInterventions.AnnalsofBehavioralMedicine,2013.46(1):p.81-95.
23. Sim,J.andM.Lewis,Thesizeofapilotstudyforaclinicaltrialshouldbecalculatedinrelationtoconsiderationsofprecisionandefficiency.JournalofClinicalEpidemiology,2012.65(3):p.301-308.
24. Lancaster,G.A.,S.Dodd,andP.R.Williamson,Designandanalysisofpilotstudies:recommendationsforgoodpractice.JournalofEvaluationinClinicalPractice,2004.10(2):p.307-312.
25. Hooper,R.Justifyingsamplesizeforafeasibilitystudy.[citedDecember2017.26. Ritchie,J.andL.Spencer,Qualitativedataanalysisforappliedpolicyresearch,in
Analyzingqualitativedata,A.BrymanandR.G.Burgess,Editors.1994.p.173-194.27. Family,C.a.,Workingwithfamiliesaffectedbyadisabilityorhealthconditionfrom
pregnancytopre-school.2006.28. Baile,W.,etal.,SPIKES—ASix-StepProtocolforDeliveringBadNews:Applicationto
thePatientwithCancer.TheOncologist,2000.5(4):p.302-311.29. Rabow,M.W.andS.J.McPhee,Beyondbreakingbadnews:howtohelppatientswho
suffer.WesternJournalofMedicine,1999.171(4):p.260-263.30. Kavanagh,C.,B,SharingBadNewswithParentsJCG0325v2.2016,Norfolkand
NorwichUniversityHospital.31. Hospital,R.C.,BreakingBadNews–aguidelinetoassisthealthcareprofessionalsin
communicatingandbreakingbadnewstochildren/youngpeopleandtheirfamilies.2016.
32. Atienza-Carrasco,J.,etal.,Breakingbadnewstoantenatalpatientswithstrategiestolessenthepain:aqualitativestudy.ReproductiveHealth,2018.15:p.11.
33. Edvardsson,K.,etal.,Norwegianobstetricians'experiencesoftheuseofultrasoundinpregnancymanagement.Aqualitativestudy.Sexual&ReproductiveHealthcare,2018.15:p.69-76.
34. Dadiz,R.,M.L.Spear,andE.Denney-Koelsch,TeachingtheArtofDifficultFamilyConversations.JournalofPainandSymptomManagement,2017.53(2):p.157-+.

69
35. Saul,R.A.andS.H.Meredith,BeyondtheGeneticDiagnosis:ProvidingParentsWhatTheyWanttoKnow.PediatricsinReview,2016.37(7):p.269-278.
36. Kim,L.,etal.,StimulatingReflectivePracticeUsingCollaborativeReflectiveTraininginBreakingBadNewsSimulations.FamiliesSystems&Health,2016.34(2):p.83-91.
37. Karkowsky,C.E.,etal.,BreakingBadNewsinobstetrics:arandomizedtrialofsimulationfollowedbydebriefingorlecture.JournalofMaternal-Fetal&NeonatalMedicine,2016.29(22):p.3717-3723.
38. Macdonell,K.,AnEffectiveCommunicationInitiative:Usingparents'experiencestoimprovethedeliveryofdifficultnewsintheNICU.JournalofNeonatalNursing2015.21(4):p.142-149.
39. Lalor,J.,GivingBadandAmbiguousNews,inPrenatalandPreimplantationDiagnosis:Theburdenofchoice,J.GalstandM.Verp,Editors.2015,Springer:Switzerland.p.131-151.
40. Greiner,A.L.andJ.Conklin,BreakingBadNewstoaPregnantWomanWithaFetalAbnormalityonUltrasound.Obstetrical&GynecologicalSurvey,2015.70(1).
41. Fieschi,L.,B.Burlon,andM.G.DeMarinis,Teachingmidwifestudentshowtobreakbadnewsusingthecinema:AnItalianqualitativestudy.NurseEducationinPractice,2015.15(2):p.141-147.
42. Wolfe,A.D.,etal.,SharingLife-AlteringInformation:DevelopmentofPediatricHospitalGuidelinesandTeamTraining.JournalofPalliativeMedicine,2014.17(9):p.1011-1018.
43. deGroot-vanderMooren,M.D.,etal.,NeonataldiagnosisofDownsyndromeintheNetherlands:suspicionandcommunicationwithparents.JournalofIntellectualDisabilityResearch,2014.58(10):p.953-961.
44. Fonseca,A.,B.Nazare,andM.C.Canavarro,Parentinganinfantwithacongenitalanomaly:Anexploratorystudyonpatternsofadjustmentfromdiagnosistosixmonthspostbirth.JournalofChildHealthCare,2014.18(2):p.111-122.
45. Fonseca,A.,B.Nazare,andM.C.Canavarro,ClinicalDeterminantsofParents'EmotionalReactionstotheDisclosureofaDiagnosisofCongenitalAnomaly.Jognn-JournalofObstetricGynecologicandNeonatalNursing,2013.42(2):p.178-190.
46. Fonseca,A.,B.Nazare,andM.C.Canavarro,Parentalpsychologicaldistressandqualityoflifeafteraprenatalorpostnataldiagnosisofcongenitalanomaly:Acontrolledcomparisonstudywithparentsofhealthyinfants.DisabilityandHealthJournal,2012.5(2):p.67-74.
47. Sheets,K.M.,etal.,BreakingDifficultNewsinaCross-culturalSetting:aQualitativeStudyaboutLatinaMothersofChildrenwithDownSyndrome.JournalofGeneticCounseling,2012.21(4):p.582-590.
48. Skotko,B.G.,etal.,PostnatalDiagnosisofDownSyndrome:SynthesisoftheEvidenceonHowBesttoDelivertheNews.Pediatrics,2009.124(4):p.E751-E758.
49. Lalor,J.G.,D.Devane,andC.M.Begley,Unexpecteddiagnosisoffetalabnormality:Women'sencounterswithcaregivers.Birth-IssuesinPerinatalCare,2007.34(1):p.80-88.

70
50. Dent,K.M.andJ.C.Carey,Breakingdifficultnewsinanewbornsetting:Downsyndromeasaparadigm.AmericanJournalofMedicalGeneticsPartC-SeminarsinMedicalGenetics,2006.142C(3):p.173-179.
51. Fox,S.,etal.,Talkingabouttheunthinkable:Perinatal/neonatalcommunicationissuesandprocedures.ClinicsinPerinatology,2005.32(1):p.157-+.
52. Skotko,B.,MothersofchildrenwithDownsyndromereflectontheirpostnatalsupport.Pediatrics,2005.115(1):p.64-77.
53. Skotko,B.andR.C.Bedia,PostnatalsupportformothersofchildrenwithDownsyndrome.MentalRetardation,2005.43(3):p.196-212.
54. Lalor,j.,GivingBadandAmbiguousNews,inPrenatalandPreimplantationDiagnosis:Theburdenofchoice,J.GalstandM.Verp,Editors.2015,Springer:Switzerland.p.131-151.
55. Wachs,T.D.,M.M.Black,andP.L.Engle,MaternalDepression:AGlobalThreattoChildren'sHealth,Development,andBehaviorandtoHumanRights.ChildDevelopmentPerspectives,2009.3(1):p.51-59.
56. Michie,S.,L.Atkins,andR.West,TheBehaviourChangeWheel:AGuidetoDesigning.2014,Sutton:SilverbackPublishing.