Improving the System of Care for STEMI Patientswcm/@mwa/documents/... · Improving the System of Care for STEMI Patients Improving the System of Care for STEMI Patients . 1 . Mission:
43
Improving the System of Care for STEMI Patients Improving the System of Care for STEMI Patients 1
Mission: Lifeline is the American Heart Association’s national community based multidisciplinary initiative to advance the systems of care for patients with ST-segment elevation myocardial infarction (STEMI). The overarching goal of the initiative is to reduce mortality and morbidity for STEMI patients to and improve their overall quality of care.
Improving the System of Care for STEMI Patients
Today’s Presentation
1. History of Mission: Lifeline
2. The “Ideal” State of Mission: Lifeline
3. Overview of national Mission: Lifeline initiatives
This slide lists the new updated ACC/AHA 2007 STEMI Reperfusion Recommendations.
Improving the System of Care for STEMI Patients
Systems of Care
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
NEW
Recommendation Each community should develop a STEMI system of care following the standards developed for Mission Lifeline (AHA) including: Ongoing multidisciplinary team
meetings with EMS, non-PCI & PCI centers
A process for prehosp identification and activation
Destination protocols for PCI centers Transfer protocols for non-PCI centers
There are many barriers to timely reperfusion that require careful consideration and practical solutions by multidisciplinary system teams. There are four main barriers to patients getting to the appropriate care. 1. The patient often fails to promptly recognize heart attack symptoms and call 9-1-1. Despite many public awareness trials and public health initiatives, there is hesitation to seek medical attention -- STEMI patients have, on average, 2 hours of symptoms before arriving to a hospital. 50% of STEMI patients call 9-1-1 for their symptoms. The other 50% self transport or have someone else drive them to the emergency department. Time to transport – Local policies often mandate that ambulances must be routed to the nearest hospital – regardless if the hospital has the capability to perform PCI AND/OR patients in rural areas cannot get to a hospital with PCI in the recommended timeframe. Decision on reperfusion strategy – If a STEMI patient arrives at a primary PCI center, the decision regarding the reperfusion strategy is an easy one – primary PCI. Only the issue of timeliness in off hours or simultaneous STEMIs with one team available remains problematic. Commitment to primary PCI at interventional capable hospitals is paramount. However, the decision process on arrival of the STEMI patient for reperfusion in a hospital without PCI needs to be predetermined. The hospital staff must decide if the STEMI patient will have timely transfer to a facility that provides primary PCI or be given fibrinolytics. In addition, in rural situations, STEMI patients that are fibrinolytic ineligible need urgent transfer, and use of medical air rescue should be considered. Time to implement treatment strategy – Cardiac catheterization lab teams time for assembly and procedural issues can also pose additional issues for the STEMI patient.
Improving the System of Care for STEMI Patients
The Reality of Today’s Patients
Not all STEMI patients call 9-1-1
•
“Walk-in” patients hinder:
••
••
6
Presenter
Presentation Notes
Only 50% of STEMI patients call 9-1-1 when they have heart attack symptoms. The other half present to their local emergency department (ED). When entering the ED by EMS, a heightened awareness of the heart attack is present and helps move the patient to rapid reperfusion. A “walk-in” patient can be problematic in several arenas: Registration clerks must understand the chest pain and chest pain equivalent symptoms and expedite these patients to triage. Obtaining a 12-lead ECG on chest pain patients in heart attack is paramount. The guidelines recommend a 12-lead ECG within 10 minutes of arrival to the ED. In a space-limited ED, providing a private space in triage for obtaining a 12-lead can be challenging. The importance of the EMS advance warning to activate hospital staff to prepare for reperfusion should be emphasized.
Improving the System of Care for STEMI Patients 7
How do we increase the number of patients with timely access to reperfusion therapy?
Presenter
Presentation Notes
Mission: Lifeline seeks to solve the question, “ How do we increase the number of patients with timely access to reperfusion therapy?”
Improving the System of Care for STEMI Patients
A Life-Saving Initiative
National, community-based initiative
Goals
••
8
Presenter
Presentation Notes
Mission: Lifeline is a national, community-based initiative designed to meet the needs of the STEMI patient throughout the continuum of care, beginning with the patient’s entry into the system (from symptom onset) through each component of the system, and return to the local community and physician for rehabilitative care. Mission: Lifeline uses a community-based, multidisciplinary, patient-centric approach. Mission: Lifeline is addressing systems of care for STEMI on multiple levels and through many collaborating organizations, starting with the STEMI patient and continuing through EMS, ED, STEMI Referral, and STEMI Receiving hospitals; implications for policy makers and third party payers are also being addressed within Mission: Lifeline. To meet the overarching goal, Mission: Lifeline will bring together the necessary partnerships between: Patients and care givers EMS Physicians, nurses and other providers Non-PCI capable (STEMI-referral) hospitals PCI capable (STEMI-receiving) hospitals Departments of health EMS regulatory authority/Office of EMS Rural health associations Quality improvement organizations State and local policymakers Third-party payers Health systems
Improving the System of Care for STEMI Patients
Mission: Lifeline’s Guiding Principles
The initiative values:
•••••••••
9
Presenter
Presentation Notes
Mission: Lifeline’s guiding principles will be upheld. Listed are the initiative values for review.
Improving the System of Care for STEMI Patients
The Uniqueness of Mission: Lifeline
Mission: Lifeline will:
••••
The initiative is unique in that it:
••••••
10
Presenter
Presentation Notes
What Makes Mission: Lifeline Unique? Mission: Lifeline: Addresses continuum of care for STEMI patients from entry into the system, through the system, and back to local community and provider for secondary prevention. Preserves a role for the community STEMI Referral hospital (non-PCI capable) -- one of Mission: Lifeline’s guiding principles Understands the issues specific to rural communities and importance of promoting different solutions/protocols for rural versus urban/suburban areas Understand the issues of implementing national recommendations on a community level (no “one size all” solution), considering local geography, resources, legislation, and regulation
Improving the System of Care for STEMI Patients
History 2004-2006
May 2004
•
June 2005
•
March 2006
•
••
•
11
Presenter
Presentation Notes
Here is a look at Mission: Lifeline’s history in brief. In May 2004, the American Heart Association (AHA) recruited an Advisory Working Group (AWG) to evaluate the quality of care for all acute myocardial infarction patients and to explore the issue of increasing the number of STEMI patients with timely access to primary percutaneous intervention (PCI). In June 2005, a market research study was conducted by Price Waterhouse Coopers in order to understand cardiac services for STEMI patients. The market research suggested that there was a recognized need to improve the systems of care for STEMI patients and that the American Heart Association should play a leading role in bringing together all of the constituents involved in the care of these patients. This research resulted in an AHA AWG Consensus Statement published in Circulation in 2006 and a stakeholder “Call to Action”. In late March 2006, the American Heart Association convened a three-day conference with multidisciplinary groups of physicians (noninvasive and interventional cardiologists, cardiac surgeons, emergency care and critical care practitioners, internists), nurses, EMS personnel, community and tertiary hospital administrators (including representation from rural areas), payers, quality and outcomes experts, and government officials involved in the care of STEMI patients.
Improving the System of Care for STEMI Patients
History 2007-Present
Early 2007
•
•
April 2007
•
May 2007
•
•
July 2008
•
12
Presenter
Presentation Notes
The findings and recommendations of the March 2006 conference were published in Circulation: Journal of the American Heart Association in May 2007. These conference proceedings form the basis for Mission: Lifeline. The focus of the initiative is to increase the number of patients with timely access to primary PCI. In July 2008, Mission: Lifeline held a staff kick-off that introduced close to 300 AHA staff to the Mission: Lifeline initiative. The staff represented almost all of the 50 states and all of the health strategies division of the organization.
For each component of the system, Mission: Lifeline will:
•••••
13
Presenter
Presentation Notes
The implementation phase will include: Defining the ideal practice; Recommending strategies to achieve the ideal practice; Providing resources/tools to achieve the ideal practice; Recommending metrics for structure, process and outcomes; and Recommending criteria for recognition and certification. The new “What is Mission: Lifeline” tool is available for your review via worldwide web.
Improving the System of Care for STEMI Patients
The Ideal STEMI System of Care
14
Presenter
Presentation Notes
Mission: Lifeline seeks to promote the ideal STEMI system of care in the United States. Public awareness and the patient factors of recognition of symptoms and calling 9-1-1 will always be considered as important to the AHA and Mission: Lifeline. However, in the first phases of the initiative, the primary focus will be on: Creating an ideal system of response of the healthcare team in all components of the system; and Emergency Medical Services (EMS) and implementation of destination protocols for improving access to primary PCI by either EMS bypass of non-PCI hospitals for primary PCI hospitals or timely transfer from non-PCI hospitals to primary PCI hospitals. Each hospital in the United States should have a plan in place for reperfusion and a back-up plan. Involvement of payers; health agencies; and local, state, and national policy makers will be critical to this initiative. [OPTIONAL NOTE TO PRESENTER: Use Chain of Survival Picture?]
Improving the System of Care for STEMI Patients
The Ideal Patient
Patients and the public:
••
°
°
••
The ideal system:
••
•
15
Presenter
Presentation Notes
In the ideal system, patients and the public would recognize the symptoms of STEMI and the importance of time to treatment, activate EMS promptly, be familiar with their community hospital’s role in the delivery of STEMI care, and understand the implications involved in inter-hospital (rapid) transfer for PCI. The ideal system promotes culturally competent education efforts, includes patient representatives on community planning coalitions, and provides coordinated and patient-centered care.
Improving the System of Care for STEMI Patients
The Ideal EMS
In an ideal system:
••
°
°
°
•
••
•
•
16
Presenter
Presentation Notes
In the ideal system for EMS, standardized point-of-entry (POE) protocols (created by regional or state-based coalitions of EMS personnel, emergency physicians and nurses, and cardiologists and supported by payers and administrators) would advocate which patients are transported to the nearest hospital and which patients are transported to the nearest primary PCI/STEMI-receiving hospital based in part on the acquisition, interpretation, and transmission of a pre-hospital 12-lead ECG. EMS plays a role in activating the primary PCI staff when proper equipment, training in 12-leads ECG interpretation and relaying the 12-lead information with adequate medical control is in place to STEMI-receiving hospital. If EMS takes patient to a non-PCI or STEMI-referral hospital, a strategy of leaving the patient on the EMS stretcher with EMS present for potential STEMI transfer to STEMI-receiving hospital would be time saving. In addition, when walk-in patients present to STEMI-referral hospital in need of primary PCI, activation of EMS, as in a call to 9-1-1, to transport should occur.
Improving the System of Care for STEMI Patients
The Ideal STEMI-Referral Hospital
In an ideal system:
•
°
°
°
•
•°
°
•••
••
17
Presenter
Presentation Notes
In the ideal system, standardized point-of-entry (POE) protocols would dictate those STEMI patients to be transported directly to a STEMI-receiving hospital based on specific criteria for risk, contraindications to fibrinolysis, and the proximity of the nearest PCI service. Standardized triage and transfer protocols are in place for patients presenting to a STEMI-referral hospital. Alignment of patient outcome and financial incentives are provided to: Rapidly treat STEMI in accordance with ACC/AHA guidelines; Transfer to a STEMI-receiving hospital for primary PCI using reperfusion checklist in regions that do not readily have access to STEMI-receiving hospitals, standardized pharmacological regimens, order sets and clinical pathways; There is rapid and efficient data transfer, data collection and feedback; and Integrated plans for return to the community for care are provided.
Improving the System of Care for STEMI Patients
Role of the Referring Hospital is based on science
Association of Door-In to Door-Out (DIDO) Time With Reperfusion Delays and Outcomes Among Patients Transferred for Primary Percutaneous Coronary Intervention
•Retrospective cohort of 14 821 patients with STEMI transferred to 298 STEMI receiving centers for primary PCI in the ACTION Registry–Get With the Guidelines between January 2007 and March 2010.
Improving the System of Care for STEMI Patients
The Ideal STEMI-Receiving Hospital
In an ideal system:
•
•°
°
•
•••••
19
Presenter
Presentation Notes
In the ideal system, pre-hospital ECG diagnosis of STEMI, ED notification and catheterization laboratory activation would occur according to standard algorithms that would facilitate a brief ED stay or transport directly from the field to the catheterization laboratory. Single-call in systems from STEMI-referral hospitals (and potentially progressive EMS) would allow “one-call” to put in motion the staff at the STEMI-receiving center to be ready to accept the outside STEMI ASAP. In addition: The STEMI-receiving center should ensure that primary PCI is provided as routine treatment for STEMI 24 hours, 7 days a week; The hospital’s administration puts their support in writing; A multidisciplinary team meets regularly to identify and solve problems; There is a continuing education program designed and instituted for staff; and There is an established mechanism for monitoring performance, process measures and patient outcomes.
Improving the System of Care for STEMI Patients
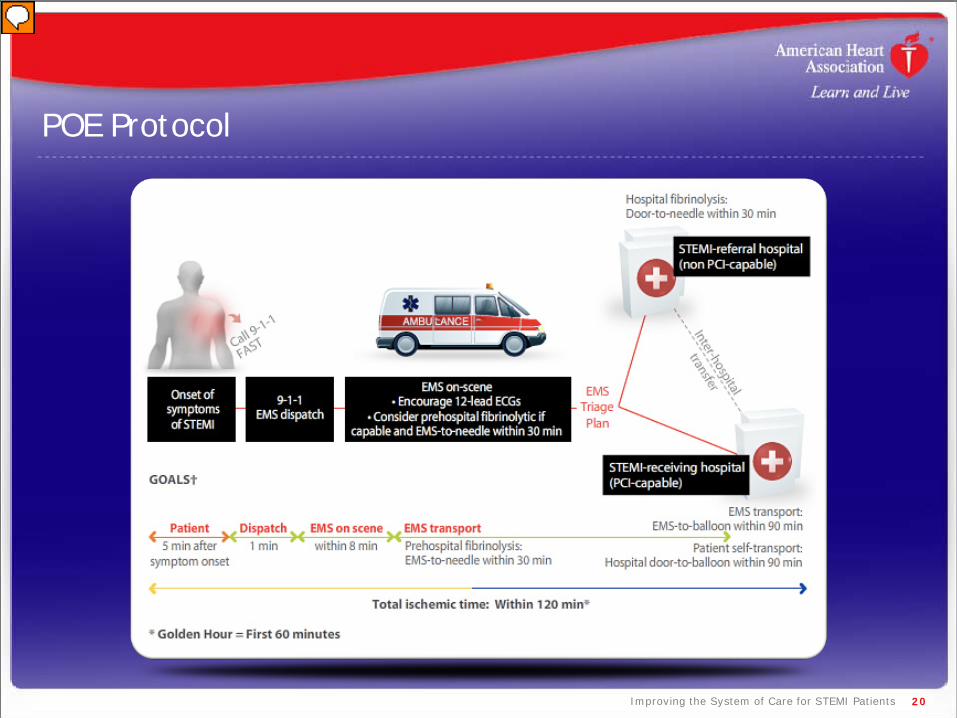
POE Protocol
20
Presenter
Presentation Notes
Patient point-of-entry (POE) protocols should be developed with the understanding that a patient may call 9-1-1 and be in an EMS zone that transports to a STEMI-referral or STEMI-receiving hospital. Also, patients may directly present to a non-PCI center and be in need of inter-hospital transfer or present to a primary PCI center. The ACC/AHA guidelines encourage EMS on scene be equipped with 12-Lead ECG technology. Advanced systems may consider pre-hospital fibrinolysis, but the majority in the U.S. EMS should have a destination protocol in place. [Note to Presenter: Following text from the 2004 Full Text STEMI ACC/AHA Guidelines caption (pg 19).] Patient transported by EMS after calling 9-1-1. 1: Reperfusion in patients with STEMI can be accomplished by the pharmacologic (fibrinolysis) or catheter-based (primary PCI) approaches. Implementation of these strategies varies based on the mode of transportation of the patient and capabilities at the receiving hospital. Transport time to the hospital is variable from case to case, but the goal is to keep total ischemic time within 120 minutes. There are three possibilities: a) If EMS has fibrinolytic capability and the patient qualifies for therapy, pre-hospital fibrinolysis should be started within 30 minutes of EMS arrival on scene; b) If EMS is not capable of administering pre-hospital fibrinolysis and the patient is transported to a non-PCI-capable hospital, the hospital door-to-needle time should be within 30 minutes for patients in whom fibrinolysis is indicated; c) If EMS is not capable of administering pre-hospital fibrinolysis and the patient is transported to a PCI-capable hospital, the hospital door-to-balloon time should be within 90 minutes. Inter-hospital transfer: It is also appropriate to consider emergency inter-hospital transfer of the patient to a PCI-capable hospital for mechanical revascularization if: 1: There is a contraindication to fibrinolysis; 2: PCI can be initiated promptly (within 90 minutes after the patient presented to the initial receiving hospital or within 60 minutes compared to when fibrinolysis with a fibrin-specific agent could be initiated at the initial receiving hospital); fibrinolysis is administered and is unsuccessful (i.e.,"rescue PCI"). Secondary non-emergency inter-hospital transfer can be considered for recurrent ischemia. Patient self transport: Patient self-transportation is discouraged. If the patient arrives at a non-PCI capable hospital, the door-to-needle time should within 30 minutes. If the patient arrives at a PCI-capable hospital, the door-to-balloon time should be within 90 minutes. The treatment options and time recommended after first hospital arrival are the same.
Improving the System of Care for STEMI Patients
Coordinated Actions
Assess and improve the EMS system
Evaluate existing STEMI system models
Establish local initiatives
Explore the possibility of developing a national STEMI-certification program and/or criteria
Launch Mission: Lifeline awareness campaigns
Create system resources
Engage strategic alliances
21
Presenter
Presentation Notes
Listed here are action items that Mission: Lifeline is currently promoting.
Improving the System of Care for STEMI Patients
Partners for Success
Patients and care givers
EMS providers
Physicians, nurses and other providers
STEM-referral (non-PCI) hospitals
STEMI-receiving (PCI-capable) hospitals
Health systems
Departments of health
EMS regulatory authority / office of EMS
Rural health associations
Quality improvement organizations
Third-party payers
State and local policymakers
22
Presenter
Presentation Notes
All partners listed are suggested. For your region, additional partners may be necessary for the promotion of regional systems.
Improving the System of Care for STEMI Patients
STEMI System Evaluation & Registration
Online questionnaire
•
•
°
°
°
°
Benefits
•
23
Presenter
Presentation Notes
STEMI Systems across the United States are asked to participate in a STEMI System Assessment. The survey is designed to understand the types of system that currently exist. The survey is geared toward STEMI systems. A "STEMI system" is an integrated group of separate entities focused on reperfusion therapy for STEMI within a region that typically includes emergency medical services (EMS) providers, at least one community (non-PCI) hospital and at least one tertiary (PCI) center. The system may include one or more of the following elements: Leadership teams of EMS, emergency medicine, cardiology, nursing and administration; Standardized communication (i.e. STEMI alert system); Standardized transportation; and Data collection and feedback. Please note: In some systems, there may be a single hospital with PCI capabilities that has established protocols with EMS providers and contains the elements stated above. If you have not registered your STEMI System with Mission: Lifeline, please access the web site and submit your system’s information. This will provide you with benefits of the Mission: Lifeline newsletter, AHA’s social networking platform, and other STEMI information. www.ahasurveys.com/se.ashx?s=0B87B7ED7A3B4136
Improving the System of Care for STEMI Patients
24
Improving the System of Care for STEMI Patients
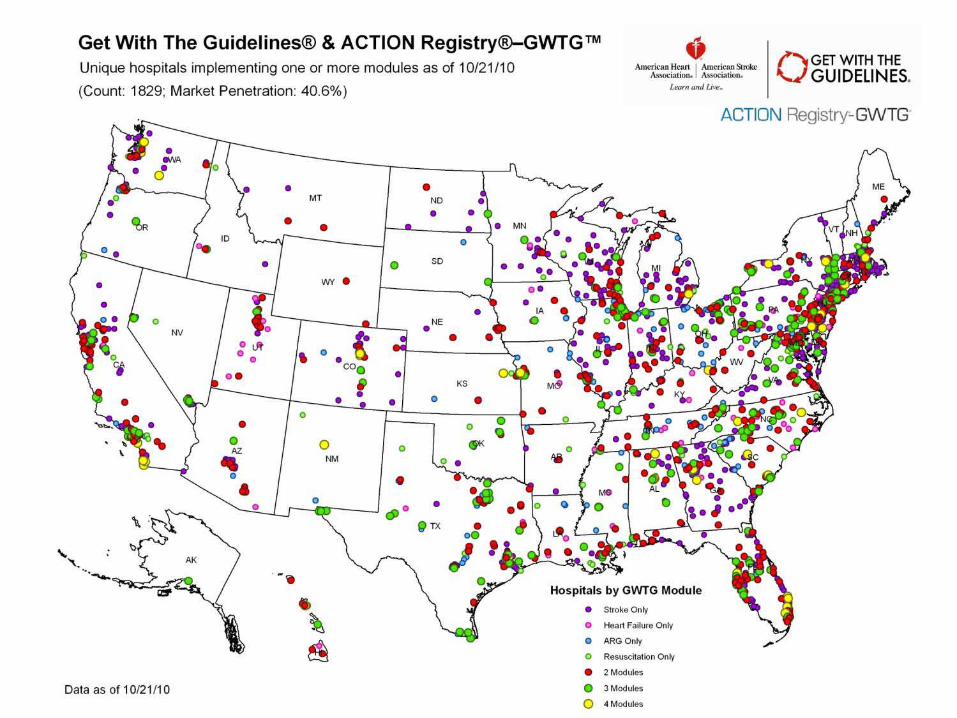
Mission: Lifeline STEMI System Coverage
25
Improving the System of Care for STEMI Patients
What is happening in other parts of the country?
The American Heart Association is:
••
•
26
Presenter
Presentation Notes
This slide provides a listing of local activities that will help professionals become engaged at the local level.
Improving the System of Care for STEMI Patients
Regional Systems of Care Demonstration Project: Mission: Lifeline™ STEMI Systems Accelerator program
The Duke Clinical Research Institute’s Center For Educational Excellence is excited to announce a call for regional STEMI System Conferences
A push to reform systems of care for the ST elevation myocardial infarction patient by engaging multiple systems that provide emergency medical care and reperfusion therapy within the same geographical region.
Bring together leading health care providers and institutions in a collaborative fashion facilitated by professional organizations, national experts in the organization of regional systems, local key thought leaders in cardiology and emergency medicine, and leading emergency cardiac care businesses.
Identify and establish regional leadership in emergency cardiac care that includes prominent physicians and administrators in hospitals, emergency medicine, and cardiology.
27
Improving the System of Care for STEMI Patients 28
How will we measure our impact?
Presenter
Presentation Notes
How will we measure our impact? ACTION Registry–GWTG will be the largest and most comprehensive national AMI patient database ever developed by the medical profession. It will establish a national standard for understanding and improving the quality, safety and outcomes of care provided for patients with coronary artery disease, specifically, high-risk STEMI and non-STEMI patients.
Improving the System of Care for STEMI Patients
Mission: Lifeline Metrics Data Sources
EMS
•••
Emergency department
•
STEMI-receiving (PCI-capable) hospitals
•
29
Presenter
Presentation Notes
Mission: Lifeline metrics will be evaluated predominantly though the ACC/AHA tool ACTION Registry-GWTG. There is a new version 2 available, and you may review it on the NCDR web site. A non-PCI version of STEMI-only data will be available in the new year to evaluate STEMI care in the emergency department and at discharge for institutions just getting started in integrating QI into their STEMI population. STEMI-receiving centers have been encouraged to participate in both NCDR Cath/PCI registry and ACTION-GTWG. EMS data needs to be integrated into the system assessment. Tools are being evaluated and piloted so that this area of Mission: Lifeline metrics will be highlighted.
Improving the System of Care for STEMI Patients
Current ACTION Registry-GWTG Site Distribution
Last updated: 9/22/2010
UT (1)
ND (2)
AK (1)
WA (7)
OR (8)
CA (26)
ID (2)
NV (6)
MT (2)
WY (0)
CO (15)
NM (2)
SD (3)
NE (3)
KS 10
OK (6)
TX (60)
MN (5)
IA (4)
MO (25)
AR (1)
LA (5)
WI (6) MI
(9)
MI (9)
AZ (3)
HI (3)
IL (31)
IN (13)
KY (6)
TN13
MS (17)
AL (8)
GA (15)
FL (20)
SC (17)
NC (25)
VA (15)
OH (23)
WV (1)
PA (23)
NY (14)
MD (24)
ME (1)
VT (0)
NH (1)
NJ (5) ()
MA (4)
CT (5)
DE (1)
RI (1)
DC (1)
PR(2)
Presenter
Presentation Notes
MO has 25 hospital that participate in AR-G
Improving the System of Care for STEMI Patients
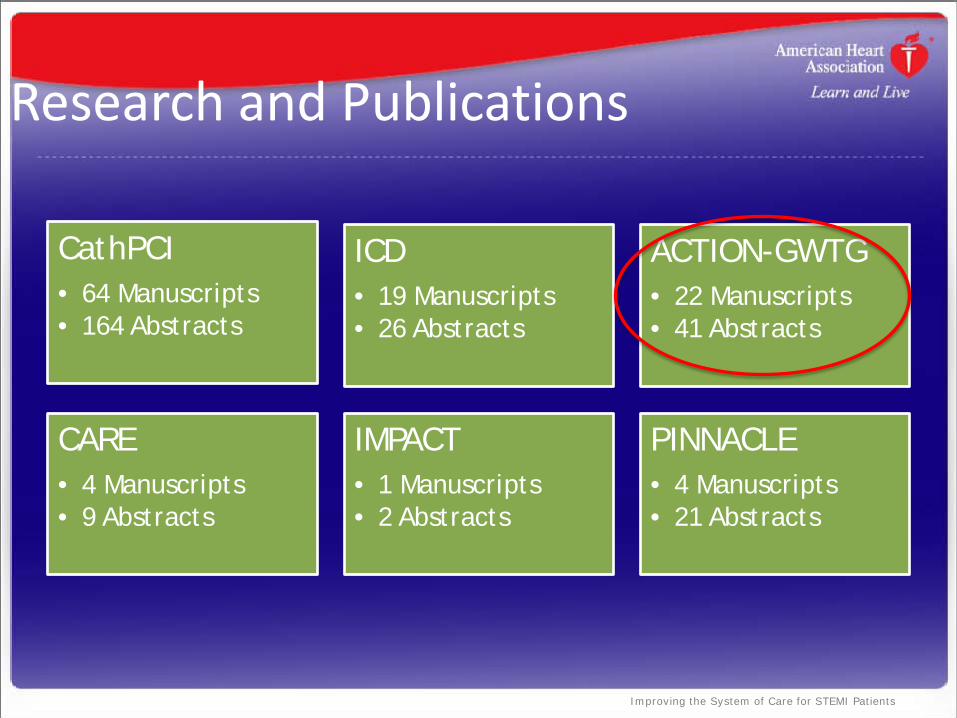
Research and Publications
CathPCI • 64 Manuscripts • 164 Abstracts
ICD • 19 Manuscripts • 26 Abstracts
ACTION-GWTG • 22 Manuscripts • 41 Abstracts
CARE • 4 Manuscripts • 9 Abstracts
IMPACT • 1 Manuscripts • 2 Abstracts
PINNACLE • 4 Manuscripts • 21 Abstracts
Improving the System of Care for STEMI Patients
Improving the System of Care for STEMI Patients
1/3/2012 33
Improving the System of Care for STEMI Patients
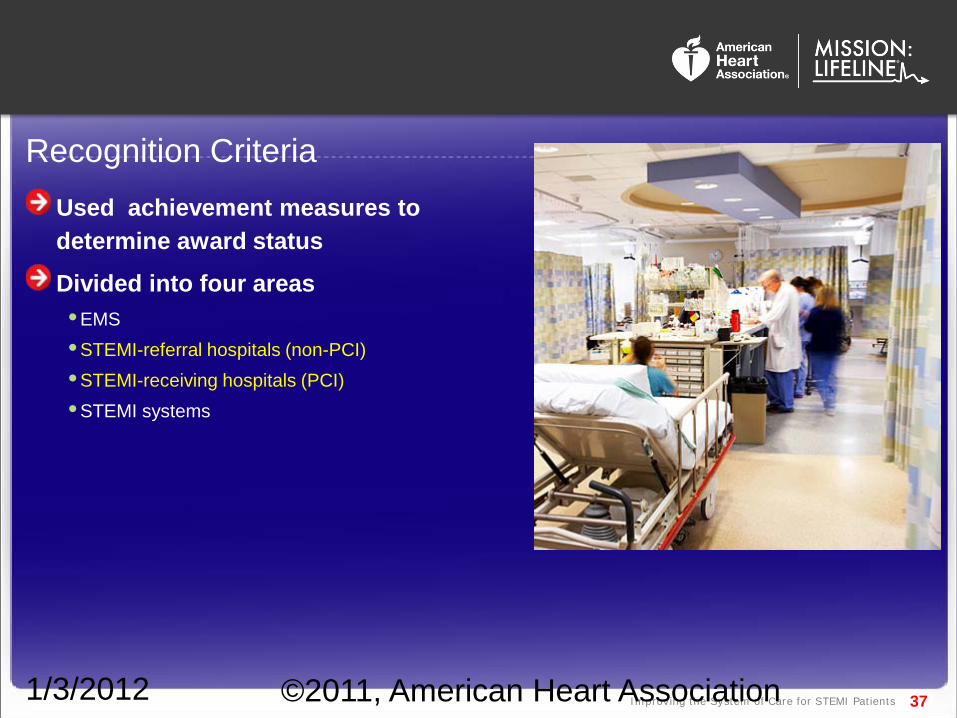
Achievement Measures STEMI Referral Center
Percentage of STEMI patients with a door-to-first ECG time <10 minutes
Percentage of reperfusion –eligible patients receiving any reperfusion (PCI or fibrinolysis) therapy
Percentage of reperfusion –eligible patients with door-to-needle time within 30 minutes
Percentage of reperfusion –eligible patients transferred to PCI center with door-in- to door-out time within 45 minutes
* Facility goal to make first door-to-balloon (first device used) time within 90 minutes (taking into consideration transport time)
Percentage of STEMI patients receiving aspirin within 24 hours
Percentage of STEMI patients on aspirin at discharge
Percentage of STEMI patients on Beta Blocker at discharge
Percentage of STEMI patients with LDL>100 who receive stains or lipid lowering drugs
Percentage of STEMI patients with LVSD on ACEI/ARB at discharge
Percentage of STEMI patients that smoke with smoking cessation counseling at discharge
34
Improving the System of Care for STEMI Patients
STEMI Accreditation & Recognition
The American Heart Association has:
•
•°
°
°
°
35
Presenter
Presentation Notes
The Mission: Lifeline leadership team is committed to the development of a certification and recognition program for STEMI systems of care and each component of the system (EMS, non-PCI, PCI). The American Heart Association will: Develop recommendations for a certification program; Generate and publish criteria to define a STEMI system of care, EMS, Non-PCI hospital, PCI hospital; Support policy approaches that advance the development of STEMI systems; Develop a recognition program to: -Salute health care teams who comply with guidelines; -Commend STEMI systems for raising quality of care; -Help compliant hospitals differentiate themselves; and -Motivate more health care providers to embrace the Mission: Lifeline standards.
Improving the System of Care for STEMI Patients 41
Society of Chest Pain Centers
Contract Signed and relationship announced in May 2012
•Co-branded Product Offerings:
° Stand-alone Mission: Lifeline STEMI Receiving Center or Referral Center Accreditation
° Existing Chest Pain Centers (cycle III) opportunity to add off-cycle Mission: Lifeline STEMI Receiving or Referral Center accreditation
° Beginning in Jan 2012: Offer new hospitals seeking Chest Pain Center accreditation (cycle IV) opportunity to add Mission: Lifeline STEMI Receiving Center or Referral Center Accreditation
Improving the System of Care for STEMI Patients 42
Guidelines will be published in the December 6, 2011 issues of:
• Journal of the American College of Cardiology, • Circulation: Journal of the American Heart Association • Catheterization and Cardiovascular Interventions