in-patient hyperglycemia management - integris health ... · • decreases hepatic glucose...
TRANSCRIPT

Pharmacology
Kacy Aderhold, MSN, APRN-CNS, CMSRN

Biguanides • Decreases hepatic glucose production and improves insulin sensitivity
(increases number of insulin receptors) • Common Adverse Reaction: diarrhea • Should be taken with food
• Can take 7 to 10 days to reach therapeutic levels
• Black Box Warning: lactic acidosis can occur • Use cautiously with liver disease, IV dye studies, renal insufficiency
• Hold the day of procedures that involve IV dyes & 48 hours following • Examples: • metformin (Glucophage) • metformin XR (Glucophage XR, Glumetza, Fortamet)
Thiazolidinediones (TZDs)
Increases insulin sensitivity (improves receptivity of receptors)
Black Box Warning: TZDs cause or
exacerbate CHF, Avandia ↑ risk of MI
Increase risk of peripheral fractures
Onset of action = 3 weeks
May take up to 12 weeks for maximum effect
Examples:
pioglitazone (Actos)
Rosiglitazone (Avandia)

Sulfonylureas
• Stimulate beta cells of pancreas to release more insulin
• Hypoglycemia can occur • Patients should not skip meals
• Examples:
• glyburide (Micronase, Glynase, DiaBeta)- daily with first meal
• glimipiride (Amaryl)-daily with first meal
• glipizide (Glucotrol)- daily or BID with food

Alpha-Glucosidase Inhibitors
• Slows breakdown of carbs in intestine
• Taken TID, at start of each meal
• SE: flatulence, bloating, abdominal pain
• May subside over time
• Examples:
• acarbose (Precose)
• miglitol (Glyset)
DPP-4 Inhibitors
• Inhibits dipeptidyl peptidase-4, slowing incretin metabolism, increasing insulin synthesis/release, decreasing glucagon levels
• “Incretin enhancers”, slows gastric emptying
• Given daily
• Examples:
• sitagliptin (Januvia)
• saxagliptin (Onglyza)
• linagliptin (Tradjenta)
• alogliptin (Nesina)

Meglitinides Stimulates pancreatic islet beta cell insulin release
rapid insulin “burst”
Hypoglycemia can occur
Must be taken before meals
Examples:
repaglinide (Prandin)
nateglinide (Starlix)
SGLT2 Inhibitors • Inhibits sodium-glucose cotransporter 2 (SGLT2) in the proximal
nephron, reducing glucose reabsorption and increasing urinary glucose excretion
• Taken daily before first meal
• Contraindicated in renal impairment CrCl<45
• SE: UTI, yeast infection
• Example
• canagliflozin (Invokana)
• dapagliflozin (Farxiga)
• empagliflozin (Jardiance)

Best Practice Oral Agents (OAs)
• OAs are inappropriate in most hospitalized patients
• Continued use may be appropriate in selected stable patients who consume meals at regular intervals
• Injectable noninsulin therapies such as exenatide and pramlintide have limitations similar to OAs
( Moghissi et al. , 2009)
• Consider precautions for each component when using combination oral agents

Injectable Medications Non-Insulin
• Incretin Mimetics or GLP-1 Receptor Agonists
• Amylin Mimetics

Incretin Mimetics GLP-1 Receptor Agonists
• Activates glucagon-like-peptide-1 receptors, increases insulin
secretion, decreases glucagon secretion, and slows gastric emptying (incretin mimetic), increasing satiety
• Injection
• SE: nausea, indigestion, weight loss
• Examples: • exenatide (Byetta)- Taken bid with am and pm meal • exenatide (Bydureon)- taken weekly • liraglutide (Victoza)- daily

Amylin Mimetic
• Activates insulin receptors, increases glucose secretion, slows gastric emptying, increase satiety
• Injection
• Taken before meals
• SE: nausea, weight loss
• Example
• pramlintide (Symlin)

Other:
• Bile acid sequestrant, colesevelam (Welchol) is a cholesterol lowering medication that also reduces blood glucose levels in patients with diabetes.
• Binds bile acid in intestinal tract, increasing hepatic bile acid production
• Bromocriptine (Cycloset) is a dopamine 2 agonist that activates neurotransmitters centrally, decreasing hyperglycemia without increasing insulin sensitivity
• Afrezza is a rapid-acting inhaled insulin that improves glycemic control in adults with diabetes mellitus, administered at the beginning of each meal.


Insulin

Types of Insulin Basal Insulin – controls blood glucose in the fasting state
glargine (Lantus)
detemir (Levemir)
NPH (Humulin N or Novolin N) (Intermediate Acting)
Prandial or Nutritional Insulin – blunts the rise in blood glucose following nutritional intake Short Acting
Regular (R) (Humulin R or Novolin R)
Rapid Acting
lispro (Humalog)
glulisine (Apidra)
aspart (NovoLog)
Correctional Insulin – corrects hyperglycemia due to mismatch of nutritional intake and/or illness related factors and scheduled insulin administration Should be same as prandial insulin

Basal Insulin
• The pancreas secretes a small amount of insulin into the bloodstream every few minutes to match the liver’s secretion of glucose. This allows a steady supply of glucose into the cells.
• Suppresses glucose production by the liver between meals and overnight.
• 50-60% of daily insulin needs (TDD – total daily dose) • targets fasting BG
Basal insulin available: • detemir (Levemir) • glargine (Lantus) • NPH (Novolin N, Humulin N)

Basal Insulin: Pharmacokinetics
*Dose dependent
Lantus (Glargine) Levemir (Detemir) NPH (Humulin N or Novolin N)
Action Long acting Long acting Intermediate
Onset 1 hour 1 hour 1-2 hours
Peak Relatively peakless Relatively peakless 4-14 hours
Duration 21-24 hours* 6-23 hours* 10-24 hours
Color Clear Clear Cloudy
Dosing 1-2 times/day 1-2 times/day 1-3 times/day
(Epocrates, 2015)

INS
UL
IN E
FF
EC
T
B L S HS B
Time
Glargine/Detemir
Bolus Insulin
• Provides a fast/rapid response to elevations in BG levels. • Nutritional/prandial insulin- also referred to as Y – “covers”
carbohydrates intake (food, liquids, IVs,TPN,TF), limits hyperglycemia after intake.
• Correctional insulin- also referred to as X – decreases elevations in BG, corrects for hyperglycemia.
• 40-50% of daily insulin needs (TDD) • targets post-prandial BG levels Bolus insulin available: • aspart (NovoLog) • lispro (Humalog) • glulisine (Apidra) • regular (Humulin R, Novolin R)

Nutritional and Correctional Insulin: Pharmacokinetics
Regular (Humulin R or Novolin R)
Humalog (Lispro)
Novolog (Aspart)
Apridra (Glulisine)
Action Fast acting Rapid acting Rapid acting Rapid acting
Onset 30-45 minutes 5-15 minutes 10-20 minutes 5-15 minutes
Peak 2-4 hours 20-90 minutes 1-3 hours 55 minutes
Duration 5-6 hours 3-4 hours 3-5 hours 3-4 hours
Color Clear Clear Clear Clear
Dosing 30-45 minutes before a meal
Right before or immediately after a meal, acts as basal insulin when used in an insulin pump with frequent delivery
(Epocrates, 2015)

Bolus Insulin

INS
UL
IN E
FF
EC
T
B L S HS B
MEALS
Morning Afternoon Evening Night
RAA* RAA* RAA*
Glargine/Detemir
RAA* = Rapid Acting Analog (Lispro/Aspart)
Basal/Bolus Insulin Regimen

INS
UL
IN E
FF
EC
T
B L S HS B
MEALS
Morning Afternoon Evening Night
Body’s basal insulin secretion
Body’s post prandial insulin secretion in response to carb
intake
Natural Insulin Secretion

Insulin Mixtures
• Contain a pre-mixed combination of intermediate acting basal insulin and short/rapid bolus insulin, stated as %/%
• Have double peaks of action
Types:
• Humulin 70/30, 50/50 and Novolin 70/30 contain NPH and regular insulin in stated percentages. Should be given 30-45 minutes before meal
• Humalog mix 75/25, 50/50 and NovoLog mix 70/30 contain a long and rapid insulin in stated percentages. May be given right before meal to immediately after meal
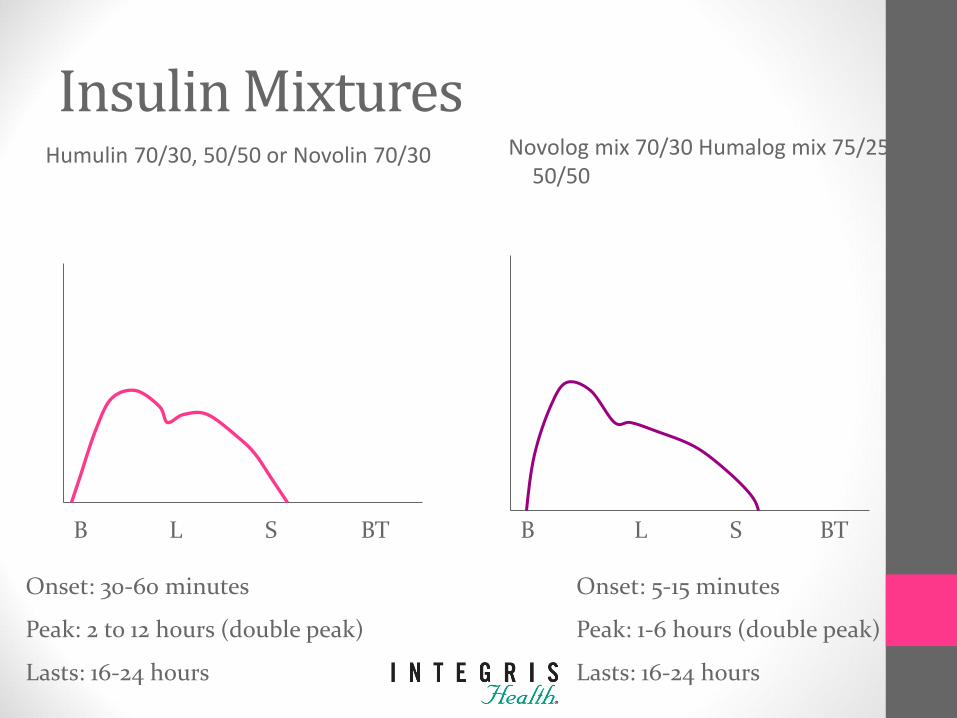
Insulin Mixtures Humulin 70/30, 50/50 or Novolin 70/30 Novolog mix 70/30 Humalog mix 75/25,
50/50
B L S BT
B L S BT
Onset: 30-60 minutes
Peak: 2 to 12 hours (double peak)
Lasts: 16-24 hours
Onset: 5-15 minutes
Peak: 1-6 hours (double peak)
Lasts: 16-24 hours
Sliding Scale Insulin
• Prolonged Sliding Scale Insulin (SSI) as the sole regimen is ineffective in the majority of patients.
• SSI increases risk of both hyperglycemia and hypoglycemia.
• SSI is associated with adverse outcomes in general surgery patients with T2DM.
• SSI is potentially dangerous in T1DM.
• “Corrective Insulin” or the use of additional short or rapid acting insulin in conjunction with scheduled insulin doses to treat BG levels above desired targets, is preferred.
(ADA, 2015)

Timing of Insulin
• Rapid acting insulin like Novolog may be given right before meal to immediately after meal
• Insulin doses given late can cause the next FSBS reading to be high since the insulin did not have enough time to fully work before we are taking the FSBS again
• FSBS should be taken 30 minutes or less before patient eats
• FSBS taken early can result in high FSBS readings due to the insulin not having time to complete duration before FSBS taken
Insulin Stacking
• Insulin stacking occurs when short or rapid acting S.Q. insulin doses are given too close together.
• Consider: Rapid insulin SQ should not be dosed any closer than 3 hours apart.
• Consider: Regular insulin SQ should not be dosed any sooner than 4 hours apart.

Insulin Alert • Insulin is a high-alert, high-risk drug. • Verify patient’s BG before calculation of dose is completed. • Verify dose calculation with another RN, LPN or clinical
pharmacist. • To prevent hypoglycemia from an insulin overdose, never give
an IV insulin bolus by increasing the infusion rate temporarily via the infusion pump.
Don’t confuse NovoLog ………….. Novolin Humalog ………….. Humulin Novolin 70/30 ……. NovoLog mix 70/30 Humulin 50/50 …….Humalog mix 50/50
INTEGRIS Health's policy on Insulin Administration

To Hold or Not to Hold? Oral Agents: What to do:
Secretagogues Sulfunylureas, Prandin, Starlix
Hold if not tolerating meals
Metformin
Hold if dehydrated, N&V, compromised renal or cardiac status, dye study, sepsis, any serious illness,
immediate post-op
Thiazolidinediones
May be given unless patient is unable to swallow or strict NPO
Insulin:
What to do:
Basal Insulin Glargine (Lantus), Detemir (Levemir)
Do not HOLD – NPO, patient should always have full dose without regard to food intake
Basal Insulin - NPH
Do not HOLD – If NPO, patient will need ½ to 2/3 of their usual dose
Bolus Insulin – Regular, lispro(Humalog), aspart(Novalog),
apidra
IF NPO, hold meal doses and give only correction doses for hyperglycemia

Insulin Infusion
Insulin infusions are a physician’s order. There are several insulin infusions that may be ordered at INTEGRIS Health: Intensive Insulin Infusion, Maintenance Insulin Infusion, or as part of the DKA protocol (low-dose insulin infusion).
Some indications for insulin infusion include:
• Critical Care Illness
• MI
• Carcinogenic Shock
• Perioperative care
• Surgical illness
• Corticosteroid therapy

Transitioning from Insulin Infusion to Subcutaneous Insulin
Why?
• Volume resuscitated
• Pressor support discontinued
• Ready to resume eating
How?
• Initiate subcutaneous insulin injections
• Give a dose of subcutaneous basal insulin 2 hours before discontinuing insulin infusion to prevent hyperglycemia

Insulin Pen Use in the Hospital Benefits: • Decrease nursing time needed to prepare an insulin injection • Decrease dosing errors • Decrease accidental needle sticks
Alerts: • DO NOT share pens with more than one patient. Studies have shown that
biological contamination of insulin occurred in up to half of all insulin pen cartridges that were reused with multiple patients.
• DO NOT use pen cartridges as a multi-dose ‘vial’. Insulin should not be withdrawn from the pen with a syringe- this will
result in inaccurate measurement of future doses.
Insulin Pen Instructions Insulin Pen Safety Video
How to Use Insulin Pen Video


What is the process?
Levemir, Aspart, and Regular insulin will be kept in the Omnicell.
1. Bring alcohol swabs and a syringe with you to the Omnicell.
2. Select your patient and the correct insulin from the Omnicell screen.
3. Enter the amount of units you are withdrawing from the vial as quantity. So, if you are giving an 8 unit dose, remove quantity of 8.
4. When the drawer opens, swab the insulin vial with alcohol, draw up the correct dose, replace the insulin vial in the drawer, select a barcode from the pocket, attach barcode to your syringe, shut the drawer, and log out.
Insulin Multi-dose Vial in Omnicell
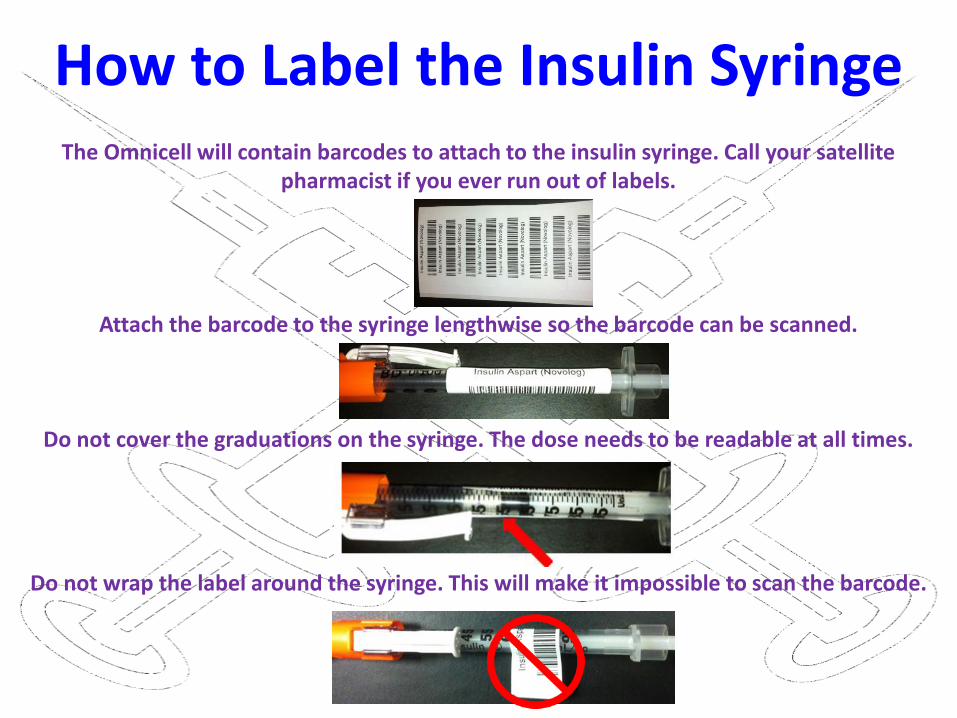
How to Label the Insulin Syringe
The Omnicell will contain barcodes to attach to the insulin syringe. Call your satellite pharmacist if you ever run out of labels.
Attach the barcode to the syringe lengthwise so the barcode can be scanned.
Do not cover the graduations on the syringe. The dose needs to be readable at all times.
Do not wrap the label around the syringe. This will make it impossible to scan the barcode.

Remember!
When giving an insulin injection using a syringe, pinch the skin using your thumb and index finger.
Insert the needle quickly and firmly at a 90° angle.

Insulin Expiration Date
Insulin can be stored at room temperature up to 28 days after opening.
Pharmacy will label all vials stored in the Omnicell
with the proper expiration date.

Insulin Pumps
• Consists of a pump, reservoir, and infusion set that delivers insulin through plastic tubing subcutaneously
• Allows flexibility in lifestyle and better glucose control
• Mimics normal functioning pancreas
• Patients may self-manage in the hospital if mentally and physically capable (physician’s order)
• Nursing must document basal and bolus doses
• Before pump is removed, ensure subQ insulin is initiated
• DKA can develop within 4-6 hours without insulin
• Insulin Pump sign should be hung in patient’s room
• INTEGRIS Health's Insulin Pump Policy
We must check FSBS with our glucometers!


High Potency Insulin U-500
• Usually insulin is 100 units/mL, U-500 is 500 units/mL (very concentrated)=U-500 insulin is 5 times as strong as regular insulin
• Used for treatment of patients with high daily insulin requirements
• Regular Insulin ONLY
• Requires special dosing calculation
• Given twice - three times daily before meals
• U-500 Policy
U-300
• Insulin glargine (Toujeo)
• Concentrated
• Doses preadjusted
• Provider who will manage DM after discharge
• Assess need for HH or outpatient DM education
• Diagnosis
• SMBG & home goals
• Information on consistent eating patterns
• When & how to take BG lowering medications
• Sick day management
• Proper use & disposal of needles & syringes
Survival Skills Discharge Education
(ADA, 2015)

Patient Teaching-Insulin Administration
Start patient teaching as soon as you know patient will go home on insulin.
Have patient demonstrate!
Discuss dosage, timing, and peaks of insulin they use
Discuss site selection & rotation
Safe injection practices!

Patient Teaching- Insulin Administration
Includes: site selection, drawing insulin from a vial, mixing insulin, using insulin
pens, and throwing away supplies

Safe Injection Practices

One Pen, One Person

References American Diabetes Association. Standards of Medical Care in Diabetes—2010 (Position Statement). Diabetes Care, 33(1), S11-S61. American Diabetes Association (2015). Standards of Care. Diabetes Care 38 (1), S1-S99. Bode, B., Braithwaite, S., Steed, D., Davidson, P., (2004). Ace Inpatient Diabetes and Metabolic Control Consensus Conference. Intravenous
insulin infusion therapy: indications, methods, and transition to subcutaneous insulin therapy. Endocrine Practice, 10(2), 71-80. Diabetes Blog Site (2015). What did dogs teach humans about diabetes? Retrieved from
http://blog.thediabetessite.com/dogsdiabetes/#w0BCYq62ycW2RQ49.97 Fonseca, V. A., (Ed.). (2006). Clinical diabetes: Translating research into practice. Philadelphia: Saunders Elsevier. Garber, A. J., Handelsman, Y., Einhorn, D., Bergman, D. A., Bloomgarden, Z. T., Fonseca, V., et al. (2008). Diagnosis and management of
prediabetes in the continuum of hyperglycemia—when do the risks of diabetes begin? A consensus statement from the American College of Endocrinology and the American Association of Clinical Endocrinologists. Endocrine Practice 14(7), 933-943.
Greenspan, F. S., Gardner, D. G. (Eds.). (2001). Basic and clinical endocrinology (6th ed.). New York: Lange/McGraw Hill Insulin. (201). In Epocrates Essentials for Apple iOS (Version 5.1) [Mobile application software]. Retrieved from
http://www.epocrates.com/mobile/iphone/essentials International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy
Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy, (2010). Diabetes Care, 33(3), 676-682).
Kruger, D. F., Aronoff, S. L., Edelman, S. V., 2007. Current and future perspectives on the role of hormonal interplay in glucose homeostasis.
The Diabetes Educator. 33(S2), 32S-46S. Moghissi, E. S., Korytkowski, M. T., DiNardo, M., Einhorn, D., Hellman, R., Hirsch, I. B., et al. (2009). American Association of Clinical
Endocrinologists and American Diabetes Association Consensus Statement on inpatient glycemic control. Endocrine Practice, 15(4), 1-15.