in the name of god dvt & pte hassan ghobadi md, pulmonologist assistant professor of internal...
TRANSCRIPT

In the name of In the name of GODGOD
DVT & PTEDVT & PTE
Hassan Ghobadi MD, Hassan Ghobadi MD, PulmonologistPulmonologist
Assistant Professor of Internal Assistant Professor of Internal MedicineMedicine
Ardabil University of Medical Ardabil University of Medical ScienceScience
EpidemiologyEpidemiology VTE-related deaths in the USA are estimated at 300,000 VTE-related deaths in the USA are estimated at 300,000
annually . annually .
Approximately two-thirds of symptomatic VTE events are Approximately two-thirds of symptomatic VTE events are hospital acquired, and the remainder are community hospital acquired, and the remainder are community acquired. acquired.
The most recent estimates of hospitalized patients at risk for The most recent estimates of hospitalized patients at risk for VTE in the USA total 13.4 million patients annually : 5.8 VTE in the USA total 13.4 million patients annually : 5.8 million surgical patients and 7.6 million medical patients.million surgical patients and 7.6 million medical patients.
PE can be fatal or can cause chronic thromboembolic PE can be fatal or can cause chronic thromboembolic pulmonary hypertension .pulmonary hypertension .
Patients with PE are more likely to suffer recurrent VTE than Patients with PE are more likely to suffer recurrent VTE than patients with DVT alone. patients with DVT alone.

Epidemiology - 2Epidemiology - 2
DVT occurs about 3 times more often than PE.DVT occurs about 3 times more often than PE.
The major adverse outcome of DVT alone, without PE, is The major adverse outcome of DVT alone, without PE, is the development of post phlebitic syndrome, which occurs the development of post phlebitic syndrome, which occurs in more than half of patients with DVT. in more than half of patients with DVT.
Postphlebitic syndrome is a late adverse effect of DVT .Postphlebitic syndrome is a late adverse effect of DVT .
Postphlebitic syndrome may not become clinically manifest Postphlebitic syndrome may not become clinically manifest until several years after the initial DVT.until several years after the initial DVT.
There is no effective medical therapy for postphlebitic There is no effective medical therapy for postphlebitic syndrome , which impairs quality of life and disables .syndrome , which impairs quality of life and disables .
Risk FactorsRisk Factors
1 - Genetic 1 - Genetic 2 - Acquired factors2 - Acquired factors
The two most common autosomal dominant genetic The two most common autosomal dominant genetic mutations are : mutations are :
A - Factor V Leiden A - Factor V Leiden B - Prothrombin gene mutationsB - Prothrombin gene mutations . .
Only a minority of patients with VTE have identifiable Only a minority of patients with VTE have identifiable predisposing genetic factors. predisposing genetic factors.
The majority of patients with predisposing genetic factors The majority of patients with predisposing genetic factors will not develop clinical evidence of clotting. will not develop clinical evidence of clotting.

Risk Factors (Risk Factors (AcquiredAcquired ) )
1 – Medical 2 – Surgical1 – Medical 2 – Surgical
Acquired predispositions include Acquired predispositions include long-haul air travel, long-haul air travel, obesity, obesity, cigarette smoking, cigarette smoking, oral contraceptives, oral contraceptives, pregnancy, pregnancy, postmenopausal hormone replacement, postmenopausal hormone replacement, surgery, surgery, trauma, andtrauma, and Medical conditions such as antiphospholipid antibody Medical conditions such as antiphospholipid antibody
syndrome, cancer, systemic arterial hypertension, and syndrome, cancer, systemic arterial hypertension, and chronic obstructive pulmonary disease.chronic obstructive pulmonary disease.

Pathophysiology Pathophysiology ((EmbolizationEmbolization ) ) When venous thrombi dislodge from their site of formation, When venous thrombi dislodge from their site of formation,
they embolize to the pulmonary arterial circulation .they embolize to the pulmonary arterial circulation .
About half of patients with pelvic vein thrombosis or proximal About half of patients with pelvic vein thrombosis or proximal leg DVT develop PE, which is usually asymptomatic.leg DVT develop PE, which is usually asymptomatic.
Isolated calf vein thrombi pose a much lower risk of PE, but Isolated calf vein thrombi pose a much lower risk of PE, but they are the most common source of paradoxical embolism. they are the most common source of paradoxical embolism.
These tiny thrombi can cross a small patent foramen ovale or These tiny thrombi can cross a small patent foramen ovale or atrial septal defect, unlike larger, more proximal leg thrombi. atrial septal defect, unlike larger, more proximal leg thrombi.
With increased use of chronic indwelling central venous With increased use of chronic indwelling central venous catheters upper extremity venous thrombosis is becoming a catheters upper extremity venous thrombosis is becoming a more common problem. more common problem.
PhysiologyPhysiology The most common gas exchange abnormalities are The most common gas exchange abnormalities are hypoxemiahypoxemia . .
Anatomic dead space increases. Anatomic dead space increases.
Increased pulmonary vascular resistance due to vascular Increased pulmonary vascular resistance due to vascular obstruction or platelet secretion of vasoconstricting obstruction or platelet secretion of vasoconstricting neurohumoral agents .neurohumoral agents .
Increased ventilation-perfusion mismatching at sites remote from Increased ventilation-perfusion mismatching at sites remote from the embolus and a large alveolar-arterial O 2 gradient.the embolus and a large alveolar-arterial O 2 gradient.
Alveolar hyperventilation due to reflex stimulation of irritant Alveolar hyperventilation due to reflex stimulation of irritant receptors.receptors.
Increased airway resistance due to constriction of airways distal Increased airway resistance due to constriction of airways distal to the bronchito the bronchi
Decreased pulmonary compliance due to lung edema, lung Decreased pulmonary compliance due to lung edema, lung hemorrhage, or loss of surfactant.hemorrhage, or loss of surfactant.
Right Ventricular Right Ventricular DysfunctionDysfunction
Progressive right heart failure is the usual cause of death Progressive right heart failure is the usual cause of death from PE. from PE.
As pulmonary vascular resistance increases, RV wall As pulmonary vascular resistance increases, RV wall tension rises and causes further RV dilatation and tension rises and causes further RV dilatation and dysfunction. dysfunction.
Diastolic LV impairment develops, attributable to septal Diastolic LV impairment develops, attributable to septal displacement.displacement.
Increased RV wall tension also compresses the right Increased RV wall tension also compresses the right coronary artery, limits myocardial oxygen supply, and may coronary artery, limits myocardial oxygen supply, and may precipitate myocardial ischemia and RV infarction. precipitate myocardial ischemia and RV infarction.
Eventually, circulatory collapse and death may ensue.Eventually, circulatory collapse and death may ensue.

Diagnosis (Diagnosis (Clinical Clinical
EvaluationEvaluation ) ) VTE mimics other illnesses, VTE mimics other illnesses, PE is known as "The Great Masquerader”.PE is known as "The Great Masquerader”.
For patients who have DVT, the most frequent history is a For patients who have DVT, the most frequent history is a cramp in the lower calf that persists for several days.cramp in the lower calf that persists for several days.
For patients who have PE, the most frequent history is For patients who have PE, the most frequent history is unexplained breathlessness. unexplained breathlessness.
When evaluating patients with possible DVT, the initial task When evaluating patients with possible DVT, the initial task is to decide whether the clinical likelihood for DVT & PTE .is to decide whether the clinical likelihood for DVT & PTE .
Patients with Patients with low likelihood of DVT & PTElow likelihood of DVT & PTE can undergo can undergo initial diagnostic evaluation with initial diagnostic evaluation with D - dimer D - dimer testing alone .testing alone .

Clinical likelihood for Clinical likelihood for DVTDVT
Low Clinical Likelihood of DVT If the Point Score Is Zero or Less
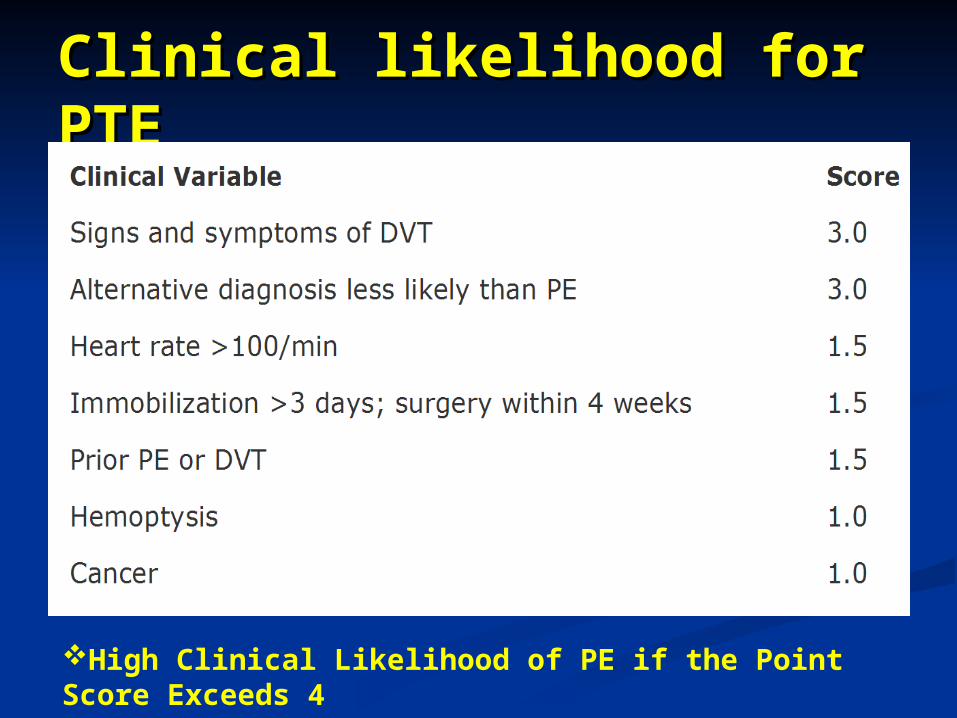
Clinical likelihood for Clinical likelihood for PTEPTE
High Clinical Likelihood of PE if the Point Score Exceeds 4

Algorithm for DiagnosisAlgorithm for Diagnosis

Clinical SyndromesClinical Syndromes Dyspnea is the most frequent symptom of PE, and Dyspnea is the most frequent symptom of PE, and
tachypnea is its most frequent sign. tachypnea is its most frequent sign.
Whereas dyspnea, syncope, hypotension, or cyanosis Whereas dyspnea, syncope, hypotension, or cyanosis indicates a massive PE, indicates a massive PE,
Pleuritic pain, cough, or hemoptysis often suggests a small Pleuritic pain, cough, or hemoptysis often suggests a small embolism located distally near the pleura. embolism located distally near the pleura.
On On physical examinationphysical examination, young and previously healthy , young and previously healthy individuals may appear anxious but otherwise seem individuals may appear anxious but otherwise seem deceptively well, even with an anatomically large PE. deceptively well, even with an anatomically large PE.
They often lack "They often lack "classicclassic" signs such as tachycardia, low-" signs such as tachycardia, low-grade fever, neck vein distension, or an accentuated grade fever, neck vein distension, or an accentuated pulmonic component of the second heart sound. pulmonic component of the second heart sound.

Clinical SyndromesClinical Syndromes
Patients with Patients with massive PE massive PE present with systemic arterial present with systemic arterial hypotensionhypotension and usually have anatomically widespread and usually have anatomically widespread thromboembolism. thromboembolism.
Those with Those with moderate to large PE moderate to large PE have have RVRV hypokinesishypokinesis on on echocardiography but normal systemic arterial pressure.echocardiography but normal systemic arterial pressure.
Patients with Patients with small to moderate PE small to moderate PE have both normal right have both normal right heart function and normal systemic arterial pressure. heart function and normal systemic arterial pressure.
The presence of pulmonary The presence of pulmonary infarctioninfarction usually indicates a usually indicates a small PEsmall PE..
Pleuritic chest pain is more common with small, peripheral Pleuritic chest pain is more common with small, peripheral emboli. emboli.

DifferentialDifferential DiagnosisDiagnosis
The differential diagnosis is critical because not all leg pain The differential diagnosis is critical because not all leg pain is due to DVT and not all dyspnea is due to PE .is due to DVT and not all dyspnea is due to PE .
Sudden, severe calf discomfort suggests a ruptured Sudden, severe calf discomfort suggests a ruptured Baker's Baker's cystcyst. .
Fever and chills usually herald Fever and chills usually herald cellulitiscellulitis rather than DVT, rather than DVT, though DVT may be present concomitantly. though DVT may be present concomitantly.
Physical findings, if present at all, may simply consist of Physical findings, if present at all, may simply consist of mild palpation discomfort in the lower calf. mild palpation discomfort in the lower calf.
In extreme cases, patients will be unable to walk or may In extreme cases, patients will be unable to walk or may require a cane, or walker. require a cane, or walker.

Differential DiagnosisDifferential Diagnosis
Diagnostic ModalitiesDiagnostic ModalitiesBlood TestsBlood Tests plasma D-dimer (ELISA)plasma D-dimer (ELISA)
Elevation of D-dimer indicates endogenous thrombolysis. Elevation of D-dimer indicates endogenous thrombolysis. The The D-dimerD-dimer is a useful is a useful "rule out" "rule out" test. test. The sensitivity of the D-dimer is greater than 80% for DVT The sensitivity of the D-dimer is greater than 80% for DVT
(including isolated calf DVT) and greater than 95% for PE. (including isolated calf DVT) and greater than 95% for PE. The D-dimer assay is not specific. The D-dimer assay is not specific. The D-dimer Levels increase in patients with myocardial The D-dimer Levels increase in patients with myocardial
infarction, pneumonia, sepsis, cancer, the postoperative infarction, pneumonia, sepsis, cancer, the postoperative state, and second or third trimester of pregnancy. state, and second or third trimester of pregnancy.
Arterial Blood Gas: Arterial Blood Gas: lack diagnostic utility lack diagnostic utility for PE, even though both the PO2 and PCO2 often decrease. for PE, even though both the PO2 and PCO2 often decrease.

Diagnostic ModalitiesDiagnostic ModalitiesElectrocardiogramElectrocardiogram
The most abnormality, The most abnormality,
Sinus tachycardia, Sinus tachycardia, The S1Q3T3 sign: an S wave in lead I, Q wave in The S1Q3T3 sign: an S wave in lead I, Q wave in
lead III, and inverted T wave in lead III .lead III, and inverted T wave in lead III .
This finding is relatively This finding is relatively specificspecific but but insensitiveinsensitive. . The most frequent abnormality is T-wave The most frequent abnormality is T-wave
inversion in leads V1 to V4.inversion in leads V1 to V4.

Diagnostic ModalitiesDiagnostic ModalitiesVenous UltrasonographyVenous Ultrasonography
Ultrasonography of the deep venous system relies upon Ultrasonography of the deep venous system relies upon loss of vein compressibilityloss of vein compressibility as the primary criterion for DVT. as the primary criterion for DVT.
When a normal vein is imaged in cross-section, it readily When a normal vein is imaged in cross-section, it readily collapses with gentle manual pressure from the ultrasound collapses with gentle manual pressure from the ultrasound transducer. transducer.
With With acuteacute DVT, the vein DVT, the vein loses its compressibility loses its compressibility because because of passive distension by acute thrombus. It appears of passive distension by acute thrombus. It appears homogeneoushomogeneous and has and has low echogenicity low echogenicity and collateral and collateral channels may be absent.channels may be absent.
A normal venous ultrasound does not exclude PE. A normal venous ultrasound does not exclude PE.

Sonographic Criteria for Sonographic Criteria for DxDx::

Diagnostic ModalitiesDiagnostic ModalitiesChest X-RayChest X-Ray
A normal or near-normal chest x-ray in a A normal or near-normal chest x-ray in a dyspneic patient often occurs in PE. dyspneic patient often occurs in PE.
Well-established abnormalities include Well-established abnormalities include Focal oligemia (Focal oligemia (Westermark's signWestermark's sign), ), A peripheral wedged-shaped density above A peripheral wedged-shaped density above
the diaphragm (the diaphragm (Hampton's humpHampton's hump), ), An enlarged right descending pulmonary An enlarged right descending pulmonary
artery (artery (Palla's signPalla's sign).).
Diagnostic Modalities Diagnostic Modalities CheatCheat CTCT
Computed tomography (CT) of the chest with intravenous Computed tomography (CT) of the chest with intravenous contrast is the principal imaging test for the diagnosis of PE .contrast is the principal imaging test for the diagnosis of PE .
The CT scan also obtains excellent images of the RV and LV and The CT scan also obtains excellent images of the RV and LV and can be used for a risk stratification as well as a diagnostic tool. can be used for a risk stratification as well as a diagnostic tool.
In patients with PE, RV enlargement on chest CT indicates a In patients with PE, RV enlargement on chest CT indicates a fivefold increased likelihood of death within the next 30 days fivefold increased likelihood of death within the next 30 days compared with PE patients with normal RV size on chest CT. compared with PE patients with normal RV size on chest CT.
In patients without PE, the lung parenchymal images may In patients without PE, the lung parenchymal images may establish alternative diagnoses not apparent on chest x-ray .establish alternative diagnoses not apparent on chest x-ray .

Diagnostic ModalitiesDiagnostic ModalitiesLungLung ScanScan Lung scanning is now a second-line diagnostic test for PE. Lung scanning is now a second-line diagnostic test for PE.
It is mostly used for patients who cannot tolerate It is mostly used for patients who cannot tolerate intravenous contrast. intravenous contrast.
The perfusion scan defect indicates absent or decreased The perfusion scan defect indicates absent or decreased blood flow, possibly due to PE. blood flow, possibly due to PE.
A high probability scan for PE is defined as having two or A high probability scan for PE is defined as having two or more segmental perfusion defects in the presence of more segmental perfusion defects in the presence of normal ventilation.normal ventilation.
The diagnosis of PE is very unlikely in patients with normal The diagnosis of PE is very unlikely in patients with normal and near-normal scans .and near-normal scans .
Diagnostic ModalitiesDiagnostic Modalities MagneticMagnetic ResonanceResonance When ultrasound is equivocal, MR venography is When ultrasound is equivocal, MR venography is
an excellent imaging modality to diagnose DVT. an excellent imaging modality to diagnose DVT.
MR utilizes gadolinium contrast agent, which, MR utilizes gadolinium contrast agent, which, unlike iodinated contrast , is not nephrotoxic. unlike iodinated contrast , is not nephrotoxic.
MRI should be considered for suspected DVT or PE MRI should be considered for suspected DVT or PE patients with renal insufficiency or contrast dye patients with renal insufficiency or contrast dye allergy. allergy.
MR pulmonary angiography detects large proximal MR pulmonary angiography detects large proximal PE but is not reliable for smaller subsegmental PE.PE but is not reliable for smaller subsegmental PE.

Diagnostic ModalitiesDiagnostic ModalitiesEchocardiographyEchocardiography Echocardiography is not a reliable diagnostic imaging tool for Echocardiography is not a reliable diagnostic imaging tool for
acute PE because most patients with PE have normal acute PE because most patients with PE have normal echocardiograms. echocardiograms.
Echocardiography is a very useful diagnostic tool for detecting Echocardiography is a very useful diagnostic tool for detecting conditions that might mimic PE, such as acute myocardial conditions that might mimic PE, such as acute myocardial infarction, pericardial tamponade, or aortic dissection.infarction, pericardial tamponade, or aortic dissection.
The best-known indirect sign of PE on echocardiography is The best-known indirect sign of PE on echocardiography is McConnell's signMcConnell's sign, hypokinesis of the RV free wall with normal , hypokinesis of the RV free wall with normal motion of the RV apex. motion of the RV apex.
Transesophageal echocardiography should be considered Transesophageal echocardiography should be considered when CT scanning facilities are not available or when a when CT scanning facilities are not available or when a patient has renal failure or severe contrast allergy.patient has renal failure or severe contrast allergy.

Diagnostic Modalities Diagnostic Modalities PulmonaryPulmonary AngiographyAngiography
Chest CT with contrast has virtually replaced Chest CT with contrast has virtually replaced invasive pulmonary angiography as a diagnostic test. invasive pulmonary angiography as a diagnostic test.
A definitive diagnosis of PE depends upon A definitive diagnosis of PE depends upon visualization of an intraluminal filling defect in more visualization of an intraluminal filling defect in more than one projection. than one projection.
Secondary signs of PE include abrupt occlusion ("Secondary signs of PE include abrupt occlusion ("cut-cut-offoff") of vessels, ") of vessels, segmental oligemiasegmental oligemia or or avascularityavascularity, , a prolonged arterial phase with slow filling, or a prolonged arterial phase with slow filling, or tortuous, tapering peripheral vessels.tortuous, tapering peripheral vessels.

Diagnostic ModalitiesDiagnostic Modalities ContrastContrast PhlebographyPhlebography
Venous ultrasonography has virtually Venous ultrasonography has virtually replaced contrast phlebography as replaced contrast phlebography as the diagnostic test for suspected the diagnostic test for suspected DVT. DVT.

Algorithm for DiagnosisAlgorithm for Diagnosis

Algorithm for DiagnosisAlgorithm for Diagnosis

TreatmentTreatment
Primary Therapy Primary Therapy
Primary therapy Primary therapy consists of clot dissolution with consists of clot dissolution with thrombolysisthrombolysis or removal of PE by or removal of PE by embolectomyembolectomy..
Secondary PreventionSecondary Prevention Anticoagulation with Anticoagulation with heparinheparin and and warfarinwarfarin or placement of or placement of
an inferior vena caval an inferior vena caval filterfilter constitutes constitutes secondary secondary prevention .prevention .
Primary therapy should be reserved for patients at high risk Primary therapy should be reserved for patients at high risk of an adverse clinical outcome. of an adverse clinical outcome.

Algorithm for PTE Algorithm for PTE ManagmentManagment
AnticoagulationAnticoagulation Anticoagulation is the foundation for successful treatment of DVT Anticoagulation is the foundation for successful treatment of DVT
and PE .and PE .
Immediately effective anticoagulation is initiated with a Immediately effective anticoagulation is initiated with a parenteral drug: parenteral drug: 1- Unfractionated heparin (UFH), 1- Unfractionated heparin (UFH),
2- Low molecular weight heparin (LMWH), 2- Low molecular weight heparin (LMWH),
3- Fondaparinux.3- Fondaparinux.
These parenteral drugs are continued as a transition or "These parenteral drugs are continued as a transition or "bridgebridge" " to long-term anticoagulation with a to long-term anticoagulation with a vitamin K antagonistvitamin K antagonist ” ” warfarinwarfarin “ . “ .
After 5–7 days of anticoagulation, residual thrombus begins to After 5–7 days of anticoagulation, residual thrombus begins to become endothelialized in the vein or pulmonary artery. become endothelialized in the vein or pulmonary artery.
Anticoagulants do not directly dissolve thrombus that already Anticoagulants do not directly dissolve thrombus that already exists.exists.

AnticoagulationAnticoagulation

Unfractionated HeparinUnfractionated Heparin Unfractionated heparin (UFH) anticoagulates by binding to Unfractionated heparin (UFH) anticoagulates by binding to
and accelerating the activity of and accelerating the activity of antithrombin IIIantithrombin III. .
UFH is dosed to achieve a target activated partial UFH is dosed to achieve a target activated partial thromboplastin time (aPTT) that is 2–3 times the upper thromboplastin time (aPTT) that is 2–3 times the upper normal limit . normal limit .
For UFH, a typical intravenous bolus is 5000–10,000 units For UFH, a typical intravenous bolus is 5000–10,000 units followed by a continuous infusion of 1000–1500 units/h. followed by a continuous infusion of 1000–1500 units/h.
An initial bolus of 80 units/kg, followed by an initial infusion An initial bolus of 80 units/kg, followed by an initial infusion rate of 18 units/kg per hour.rate of 18 units/kg per hour.
By using UFH, patients are at risk of developing heparin-By using UFH, patients are at risk of developing heparin-induced thrombocytopenia (HIT). induced thrombocytopenia (HIT).

Low Molecular Weight Low Molecular Weight HeparinsHeparins LMWH have greater bioavailability, a more LMWH have greater bioavailability, a more
predictable dose response, and a longer half-life than predictable dose response, and a longer half-life than UFH. UFH.
No monitoring or dose adjustment is needed unless No monitoring or dose adjustment is needed unless the patient is markedly obese or has renal the patient is markedly obese or has renal insufficiency.insufficiency.
Enoxaparin 1 mg/kg twice daily Enoxaparin 1 mg/kg twice daily . FDA approval for . FDA approval for treatment of patients who present with DVT. treatment of patients who present with DVT.
The weight-adjusted doses must be adjusted in renal The weight-adjusted doses must be adjusted in renal insufficiency because the kidneys excrete LMWH.insufficiency because the kidneys excrete LMWH.

FondaparinuxFondaparinux
FondaparinuxFondaparinux, an , an anti-Xa pentasaccharideanti-Xa pentasaccharide, is , is administered by once-daily subcutaneous injection and administered by once-daily subcutaneous injection and has been approved by the FDA to treat DVT and PE. has been approved by the FDA to treat DVT and PE.
No laboratory monitoring is requiredNo laboratory monitoring is required. Patients weighing . Patients weighing <50 kg receive 5 mg, 50–100 kg patients receive 7.5 <50 kg receive 5 mg, 50–100 kg patients receive 7.5 mg, and patients weighing >100 kg receive 10 mg. mg, and patients weighing >100 kg receive 10 mg.
The dose must be adjusted for patients with renal The dose must be adjusted for patients with renal dysfunction because the drug is excreted by the dysfunction because the drug is excreted by the kidneyskidneys

WarfarinWarfarin This This vitamin K antagonist vitamin K antagonist prevents carboxylation prevents carboxylation
activation of coagulation factors II, VII, IX, and X. activation of coagulation factors II, VII, IX, and X.
The full effect of warfarin requires at least 5 days, The full effect of warfarin requires at least 5 days, even if the prothrombin time, used for even if the prothrombin time, used for monitoring, becomes elevated more rapidly..monitoring, becomes elevated more rapidly..
If warfarin is initiated as monotherapy during an If warfarin is initiated as monotherapy during an acute thrombotic illness, a paradoxical acute thrombotic illness, a paradoxical exacerbation of hypercoagulability can increase exacerbation of hypercoagulability can increase the likelihood of thrombosis rather than prevent the likelihood of thrombosis rather than prevent it.it.

Warfarin : DosingWarfarin : Dosing In an average-sized adult, warfarin is usually initiated in a In an average-sized adult, warfarin is usually initiated in a
dose of 5 mg. dose of 5 mg.
Patients who are malnourished or who have received Patients who are malnourished or who have received prolonged courses of antibiotics are probably deficient in prolonged courses of antibiotics are probably deficient in vitamin K and should receive smaller initial doses of vitamin K and should receive smaller initial doses of warfarin, such as 2.5 mg. warfarin, such as 2.5 mg.
The target INR is usually 2.5, with a range of 2.0–3.0.The target INR is usually 2.5, with a range of 2.0–3.0.
Variables such as increasing age and comorbidities such as Variables such as increasing age and comorbidities such as systemic illness, malabsorption, and diarrhea reduce the systemic illness, malabsorption, and diarrhea reduce the warfarin-dosing requirement. warfarin-dosing requirement.

Complications of Complications of AnticoagulantsAnticoagulants The most important adverse effect of anticoagulation is The most important adverse effect of anticoagulation is
hemorrhage. hemorrhage.
For life-threatening or intracranial hemorrhage due to For life-threatening or intracranial hemorrhage due to heparin or LMWH, heparin or LMWH, protamine sulfate protamine sulfate can be administered. can be administered. There is no specific antidote for bleeding from There is no specific antidote for bleeding from fondaparinux. fondaparinux.
Major bleeding from warfarin is traditionally managed with Major bleeding from warfarin is traditionally managed with cryoprecipitatecryoprecipitate or or fresh-frozen plasmafresh-frozen plasma (usually 2–4 units) to (usually 2–4 units) to achieve rapid hemostasis. achieve rapid hemostasis.
For minor bleeding, or to manage an excessively high INR For minor bleeding, or to manage an excessively high INR in the absence of bleeding, a in the absence of bleeding, a small 2.5 mg dose of oral small 2.5 mg dose of oral vitamin K vitamin K may be administered.may be administered.

Complications of Complications of Anticoagulants - 2Anticoagulants - 2 Heparin-induced thrombocytopenia (HIT) and osteopenia are far Heparin-induced thrombocytopenia (HIT) and osteopenia are far
less common with LMWH than with UFH. less common with LMWH than with UFH.
Thrombosis due to HIT should be managed with a direct Thrombosis due to HIT should be managed with a direct thrombin inhibitor: thrombin inhibitor: 1- Argatroban 1- Argatroban for patients with renal for patients with renal insufficiency insufficiency
2- Lepirudin2- Lepirudin for patients with hepatic failure. for patients with hepatic failure.
In the setting of percutaneous coronary intervention, administer In the setting of percutaneous coronary intervention, administer bivalirudinbivalirudin..
The most common nonbleeding side effect of warfarin is The most common nonbleeding side effect of warfarin is alopecia. alopecia.
A rare complication is warfarin-induced skin necrosis, which may A rare complication is warfarin-induced skin necrosis, which may be related to warfarin-induced reduction of protein C.be related to warfarin-induced reduction of protein C.

Duration of Duration of Anticoagulation Anticoagulation For DVT isolated to an upper extremity or calf that For DVT isolated to an upper extremity or calf that
has been provoked by surgery or trauma, 3 months of has been provoked by surgery or trauma, 3 months of anticoagulation suffices. anticoagulation suffices.
For provoked proximal leg DVT or PE, 6 months of For provoked proximal leg DVT or PE, 6 months of anticoagulation is sufficient. anticoagulation is sufficient.
Patients with "Patients with "idiopathicidiopathic,“ DVT or PE, the recurrence ,“ DVT or PE, the recurrence rate is surprisingly high after cessation of rate is surprisingly high after cessation of anticoagulation. anticoagulation.
ACCP guidelines recommend anticoagulation for an ACCP guidelines recommend anticoagulation for an indefinite duration for patients with idiopathic VTE. indefinite duration for patients with idiopathic VTE.
Inferior Vena Caval (IVC) Inferior Vena Caval (IVC) FiltersFilters
The two principal indications for insertion of an IVC The two principal indications for insertion of an IVC filter are :filter are :
1- Active bleeding that precludes anticoagulation, 1- Active bleeding that precludes anticoagulation, 2- Recurrent venous thrombosis despite intensive 2- Recurrent venous thrombosis despite intensive
anticoagulation. anticoagulation.
Patients receiving IVC filters should also receive Patients receiving IVC filters should also receive concomitant anticoagulation. concomitant anticoagulation.
The filters can be retrieved up to several months The filters can be retrieved up to several months following insertion, unless thrombus forms and is following insertion, unless thrombus forms and is trapped within the filter. trapped within the filter.
Fibrinolysis - 1Fibrinolysis - 1
Successful fibrinolytic therapy rapidly reverses right Successful fibrinolytic therapy rapidly reverses right heart failure and leads to a lower rate of death and heart failure and leads to a lower rate of death and recurrent PE.recurrent PE.
Thrombolysis usually:Thrombolysis usually:1- Dissolves much of the anatomically obstructing pulmonary 1- Dissolves much of the anatomically obstructing pulmonary
arterial thrombus; arterial thrombus;
2- Prevents the continued release of serotonin and other 2- Prevents the continued release of serotonin and other neurohumoral factors that exacerbate pulmonary neurohumoral factors that exacerbate pulmonary hypertension;hypertension;
3- Dissolves the source of the thrombus in the pelvic or deep 3- Dissolves the source of the thrombus in the pelvic or deep leg veins, thereby decreasing the likelihood of recurrent PE.leg veins, thereby decreasing the likelihood of recurrent PE.

Fibrinolysis - 2Fibrinolysis - 2
100 mg of recombinant tissue plasminogen 100 mg of recombinant tissue plasminogen activator (tPA) administered as a continuous activator (tPA) administered as a continuous peripheral intravenous infusion over 2 h. peripheral intravenous infusion over 2 h.
Patients appear to respond to fibrinolysis for up to Patients appear to respond to fibrinolysis for up to 14 days after the PE has occurred. 14 days after the PE has occurred.
The overall major bleeding rate is about 10%, The overall major bleeding rate is about 10%, including a 1–3% risk of intracranial hemorrhage. including a 1–3% risk of intracranial hemorrhage.

Fibrinolysis ( Indications Fibrinolysis ( Indications )) The only FDA-approved indication for PE fibrinolysis is The only FDA-approved indication for PE fibrinolysis is
massive PE. massive PE.
Younger patients with submassive PE but without Younger patients with submassive PE but without comorbidities are generally excellent candidates for comorbidities are generally excellent candidates for fibrinolysis. fibrinolysis.
For older patients (>70 yrs) with risk of intracranial For older patients (>70 yrs) with risk of intracranial hemorrhage, a "watch and wait" approach is suitable .hemorrhage, a "watch and wait" approach is suitable .
Contraindications to fibrinolysis include intracranial Contraindications to fibrinolysis include intracranial disease, recent surgery, or trauma. disease, recent surgery, or trauma.

Pulmonary Pulmonary ThromboendarterectomyThromboendarterectomy Chronic thromboembolic pulmonary hypertension is caused Chronic thromboembolic pulmonary hypertension is caused
by vascular obstruction at the capillary level, not direct by vascular obstruction at the capillary level, not direct thromboembolic occlusion. thromboembolic occlusion.
CTEPH occurred in approximately 4% of patients who CTEPH occurred in approximately 4% of patients who develop acute PE. develop acute PE.
The mortality rate at experienced centers is approximately The mortality rate at experienced centers is approximately 5%. 5%.
The two most common complications are :The two most common complications are : 1- "pulmonary steal," where blood rushes from previously 1- "pulmonary steal," where blood rushes from previously
perfused areas to newly revascularized areas of the lung; perfused areas to newly revascularized areas of the lung; 2- Reperfusion pulmonary edema. 2- Reperfusion pulmonary edema.

Prevention of VTEPrevention of VTE Graduated compression Graduated compression stockingsstockings and pneumatic and pneumatic
compression devices may complement unfractionated compression devices may complement unfractionated heparinheparin (5000 units subcutaneously twice or preferably (5000 units subcutaneously twice or preferably three times daily), three times daily),
Low molecular weight heparinLow molecular weight heparin, a pentasaccharide , a pentasaccharide ((fondaparinuxfondaparinux 2.5 mg daily), or 2.5 mg daily), or warfarinwarfarin administration. administration.
Patients who have undergone total hip replacement, Patients who have undergone total hip replacement, total knee replacement, or cancer surgery will benefit total knee replacement, or cancer surgery will benefit from extended pharmacologic prophylaxis for a total of from extended pharmacologic prophylaxis for a total of 4–6 weeks.4–6 weeks.

ProphylaxisProphylaxis

Prevention of Prevention of Postphlebitic SyndromePostphlebitic Syndrome The only therapy to prevent postphlebitic syndrome is The only therapy to prevent postphlebitic syndrome is
daily use of vascular compression stockings. daily use of vascular compression stockings.
They halve the rate of developing postphlebitic They halve the rate of developing postphlebitic syndrome. syndrome.
These vascular compression stockings should be These vascular compression stockings should be prescribed as soon as DVT is diagnosed, and the prescribed as soon as DVT is diagnosed, and the stockings should be fitted carefully to maximize their stockings should be fitted carefully to maximize their benefit. benefit.
When patients are in bed, the stockings need not be When patients are in bed, the stockings need not be worn. worn.
