in the name of god -...
TRANSCRIPT

IN THE NAME OF GOD
POV:
CYSTIC OVARIAN LESION

CASE 1
• 20 years old girl with AUB and pelvic pain from 2 weeks ago


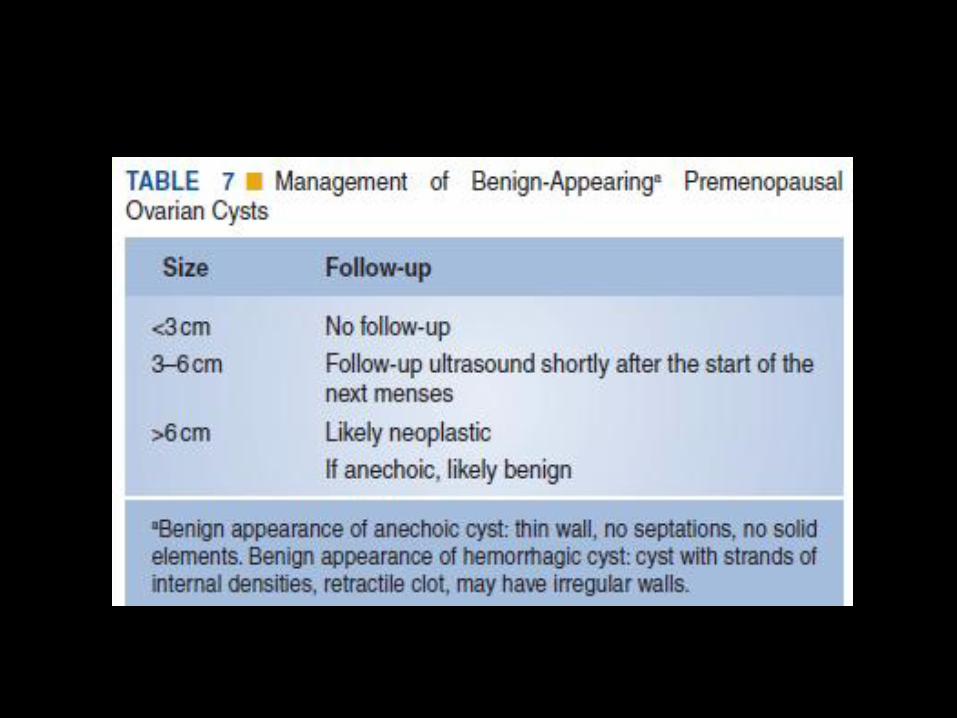
Impression :Simple unilocular 6 cm ovarian cyst
• Next step?• Almost certainly benign so FU with US until
resolved• If there is larger than 7cm simple cyst ,what we
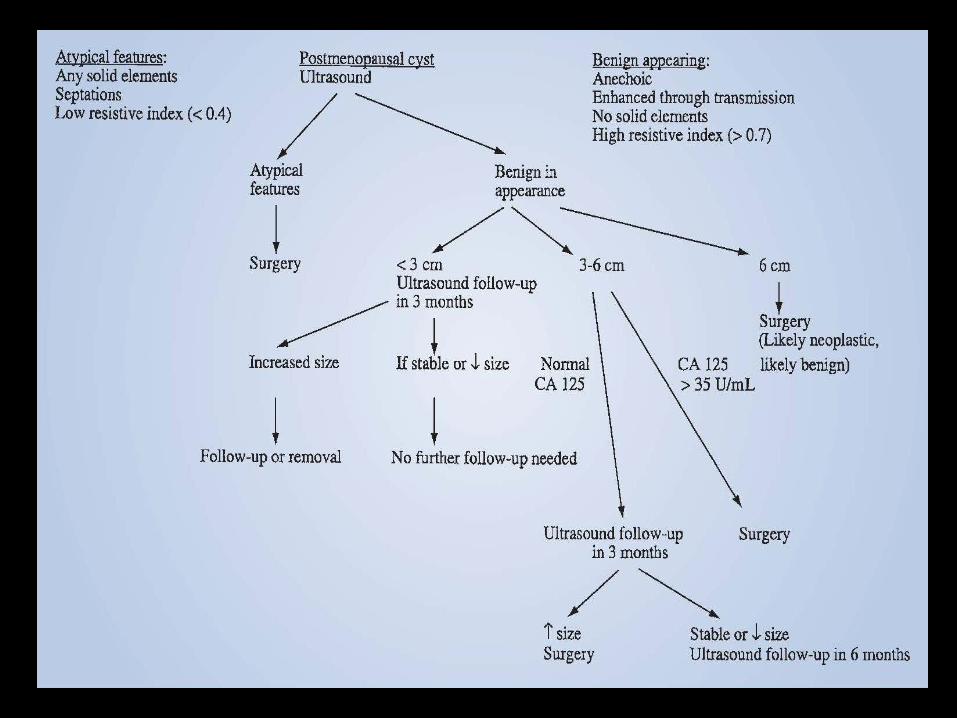
must do?• If the patient was post menopausal 70 Y/O female
?• If the patient had history of breast cancer in
herself or her sister


Case 2
• 50 years old woman with recent pelvic pain
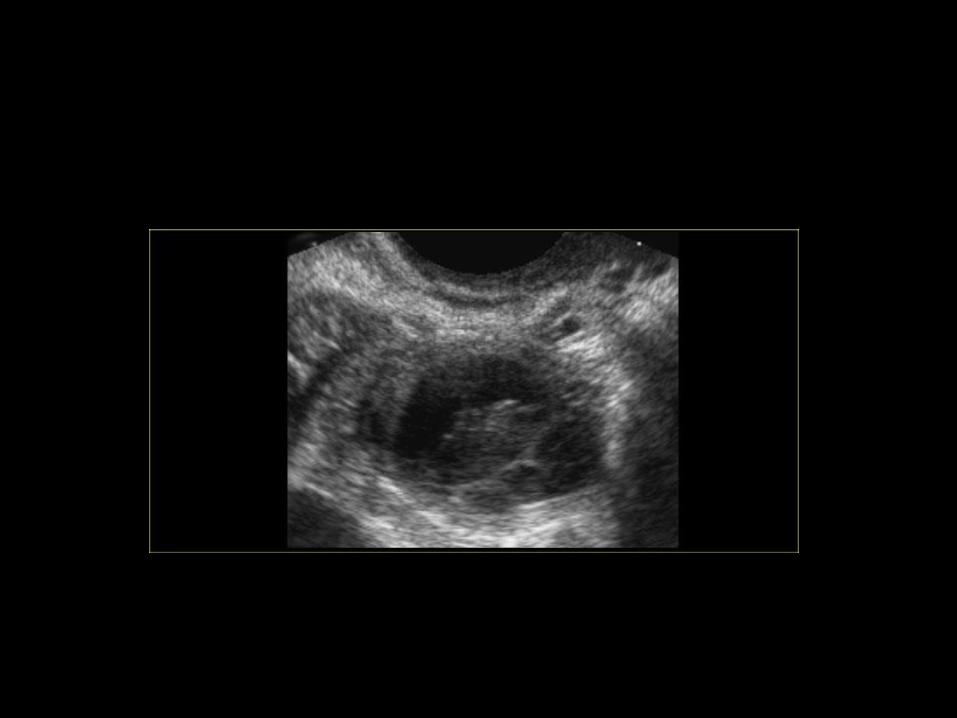
4 cm complex cyst with good through transmission ,without internal flow at CD and with concave margins
compatible with hemorrhagic cyst
• Sonographic notes in hemorrhagic ovarian cyst ?
• Use of MRI ?
• Next step?
• Under 50 Y/O and less than 5 cm HOC what we do ?
• In larger than 5 cm HOC or in late menopausal age or in high risk patents?


Case 3
• 30 years old female with dysmenorrheal symptoms
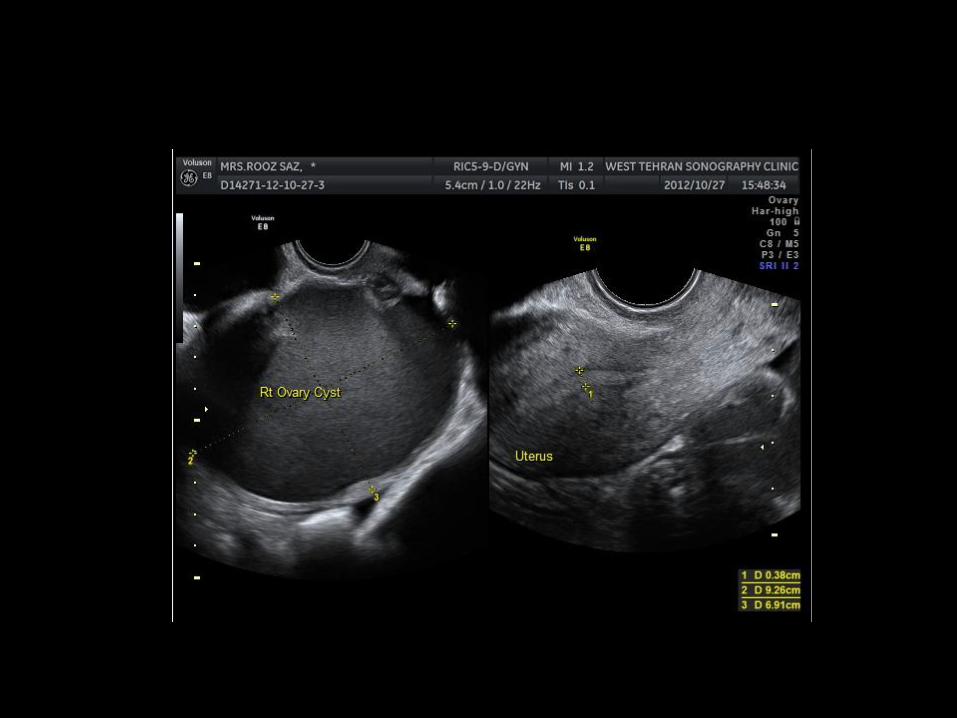

9 x 6 cm RT ovary cyst with homogenous low level internal echo , tow echogenic foci are seen near cyst wall characteristic for endometrioma
• Sonographic picture of endometrioma?
• Echogenic focus in cyst wall , significant ? Incidence percentage?
• Findings in MRI ?
• Management ?
• If patient was in early menopausal or late menopausal age or was high risk?



Case 4
• 36 years old woman with chronic pelvic pain


3.5 cm Dermoid of RT OV.Hemorrhagic cyst of LT.OV.
• Mature cystic teratoma or dermoid,next step ?
• 6-12 months FU with US• Sonographic characteristic findings ?
Hypoechoic mass with hyperechoic nodule (Rokitansky nodule or dermoid plug) Usually unilocular (90%) May contain calcifications (30%) May contain hyperechoic lines caused by floating hair May contain a fat-fluid level, i.e. fat floating on aqueous fluid May mimic intestinal loop
• Findings in CT Scan and MRI?• When surgery is indicated ? Is size of dermoid is determinant ?

Dermoid cyst


Case 5
• 59 years old woman by history of breast cancer with incidendal pelvic cyst in US

Complex RT ovarian cyst
Findings indicating possible neoplasm:
• Large sizeWhile benign lesions can be very large, the likelihood that a lesion is neoplastic increases with size. Also the likelihood that a neoplastic lesion is malignant, increases with the size of the lesion.
• Vascularized septationsThe presence of septations indicates a possible neoplasm. When septations have a thickness of more than 3mm and are well-vascularized - while non-specific - both increase the likelihood that a neoplasm is malignant.
• Vascularized solid componentsVascularized nodularities, papillary projections, or frank solid masses all increase the likelihood of a neoplastic nature.
• Vascularized thick, irregular wallLesions with thin walls are more often benign and lesions with thick, irregular walls are more often malignant. However, there is some overlap, making wall thickness a less useful criterion. For example a corpus luteum cyst may also have a thickened, vascularized wall.
• Secondary findings associated with malignant lesions:Large quantities of ascites, lymphadenopathy and peritoneal deposits are strongly associated with an increased likelihood of malignancy.



Management
• Surgical resection is needed by an oncologic gynaecologist, who may request prior imaging-based staging.
• If patient was low risk 45 Years old or there is simple cyst with a single thin septa or a single small wall calcification then next step ?


Normal ovary during a natural menstrual cycle demonstrating normal follicle population and distribution on day 12 postmenstruation. A dominant follicle is
visualized in the central portion of the image and several subordinate follicles from the wave (2–5 mm) are observed in the left lateral aspect of the ovary.
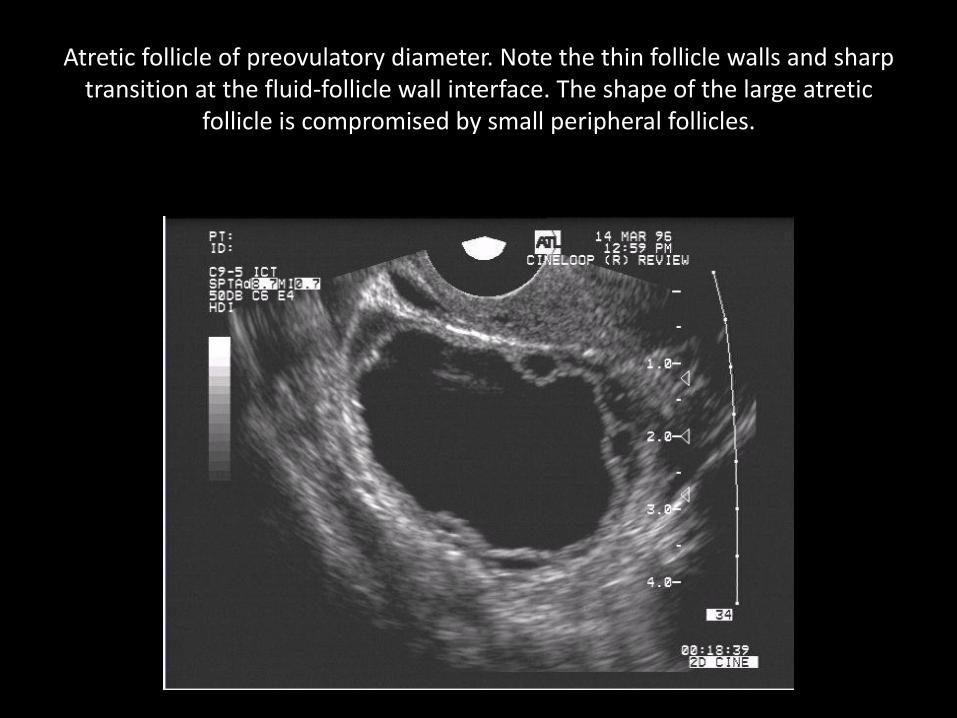
Atretic follicle of preovulatory diameter. Note the thin follicle walls and sharp transition at the fluid-follicle wall interface. The shape of the large atretic
follicle is compromised by small peripheral follicles.
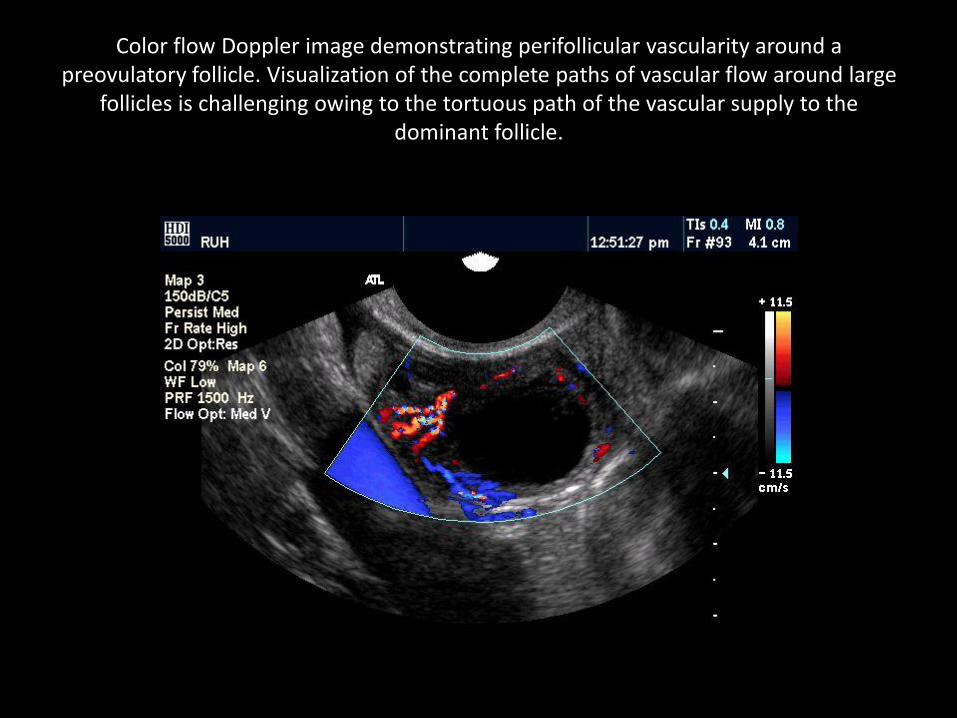
Color flow Doppler image demonstrating perifollicular vascularity around a preovulatory follicle. Visualization of the complete paths of vascular flow around large
follicles is challenging owing to the tortuous path of the vascular supply to the dominant follicle.
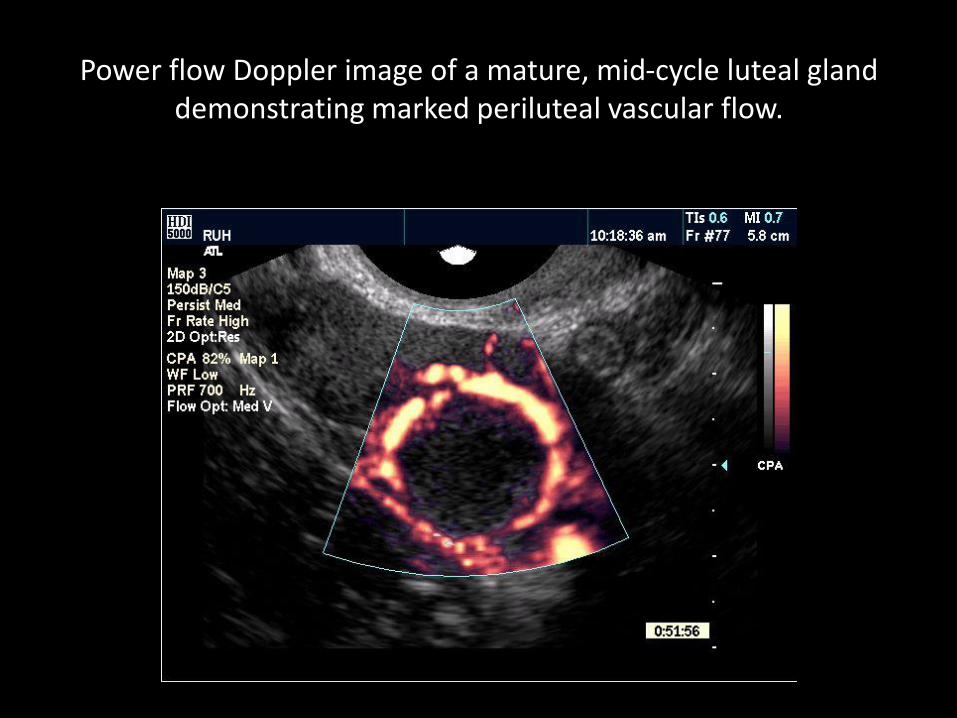
Power flow Doppler image of a mature, mid-cycle luteal gland demonstrating marked periluteal vascular flow.

Corpus hemorrhagicum demonstrating thick walls of peripheral luteal tissue and a central hemorrhagic clot with an interspersed fibrin network.
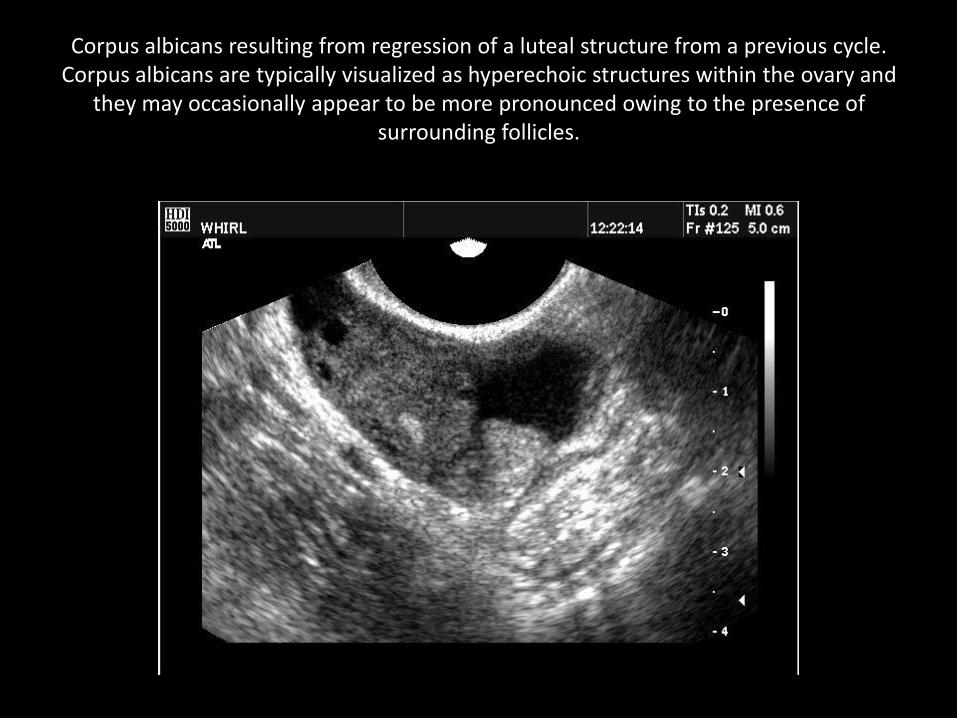
Corpus albicans resulting from regression of a luteal structure from a previous cycle. Corpus albicans are typically visualized as hyperechoic structures within the ovary and
they may occasionally appear to be more pronounced owing to the presence of surrounding follicles.
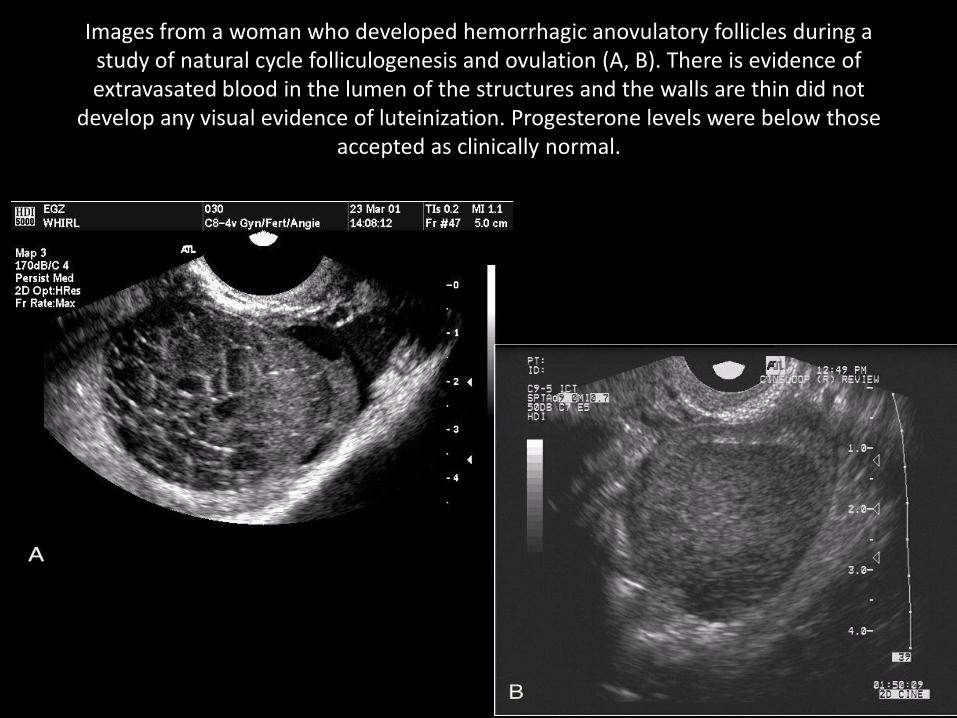
Images from a woman who developed hemorrhagic anovulatory follicles during a study of natural cycle folliculogenesis and ovulation (A, B). There is evidence of extravasated blood in the lumen of the structures and the walls are thin did not
develop any visual evidence of luteinization. Progesterone levels were below those accepted as clinically normal.

Failure of ovulation and development of “cystic” follicle. The follicle typically grows larger than the mean preovulatory follicle diameter of 23 mm, thin atretic follicle walls
are observed and small flecks of particulate matter are frequently seen in the lumen or aggregated at the side of the structure.

Image of a hemorrhagic anovulatory follicle. Extravasated blood and an interspersed fibrin network are observed within the lumen. The walls of this structure are thin,
echoic, and do not have the appearance of luteal tissue.

Images of a small intraovarian dermoid cyst (A, B). The cyst is completely embedded in the ovary and is surrounded by focal areas of hyperechoicity. Small follicles are
observed in the surrounding stroma. Folliculogenesis and ovulation were impaired in this ovary. The contralateral ovary demonstrated compensatory hypertrophy.
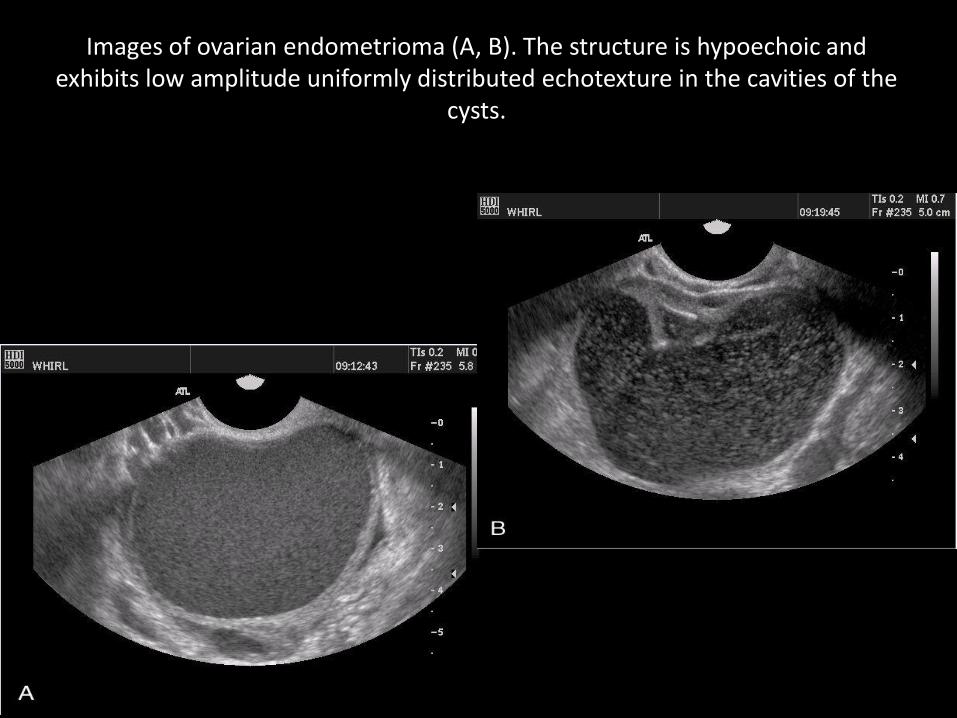
Images of ovarian endometrioma (A, B). The structure is hypoechoic and exhibits low amplitude uniformly distributed echotexture in the cavities of the
cysts.
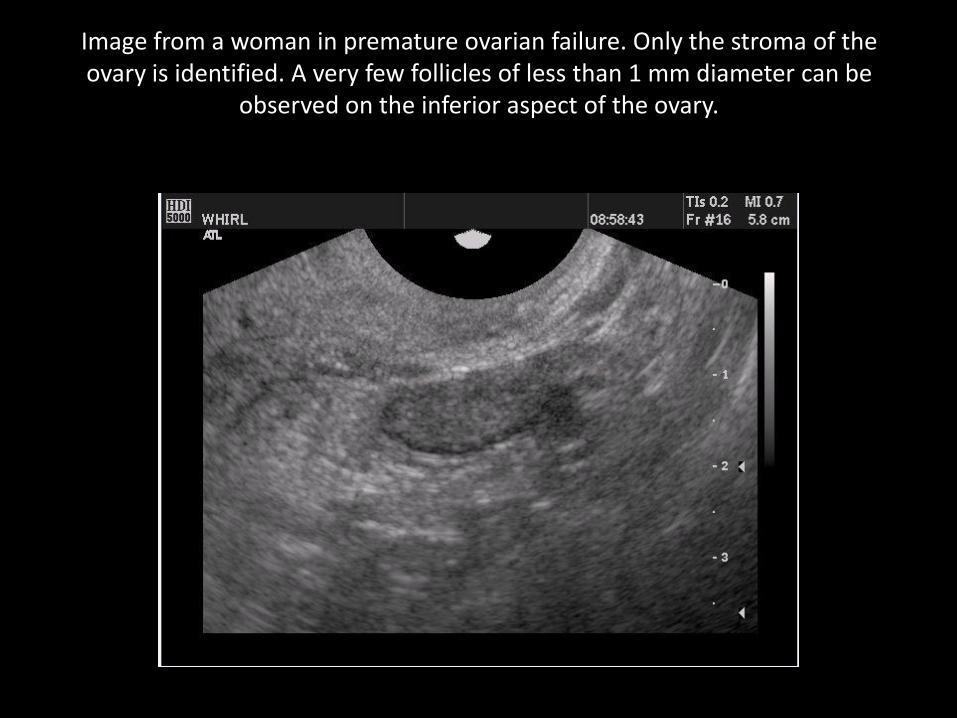
Image from a woman in premature ovarian failure. Only the stroma of the ovary is identified. A very few follicles of less than 1 mm diameter can be
observed on the inferior aspect of the ovary.
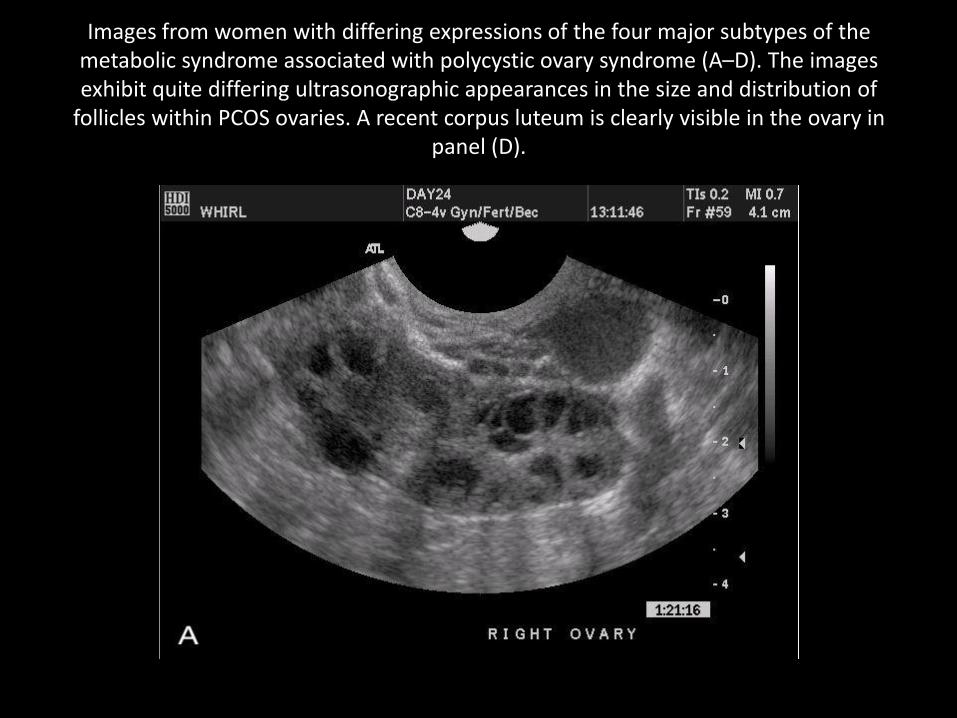
Images from women with differing expressions of the four major subtypes of the metabolic syndrome associated with polycystic ovary syndrome (A–D). The images exhibit quite differing ultrasonographic appearances in the size and distribution of
follicles within PCOS ovaries. A recent corpus luteum is clearly visible in the ovary in panel (D).



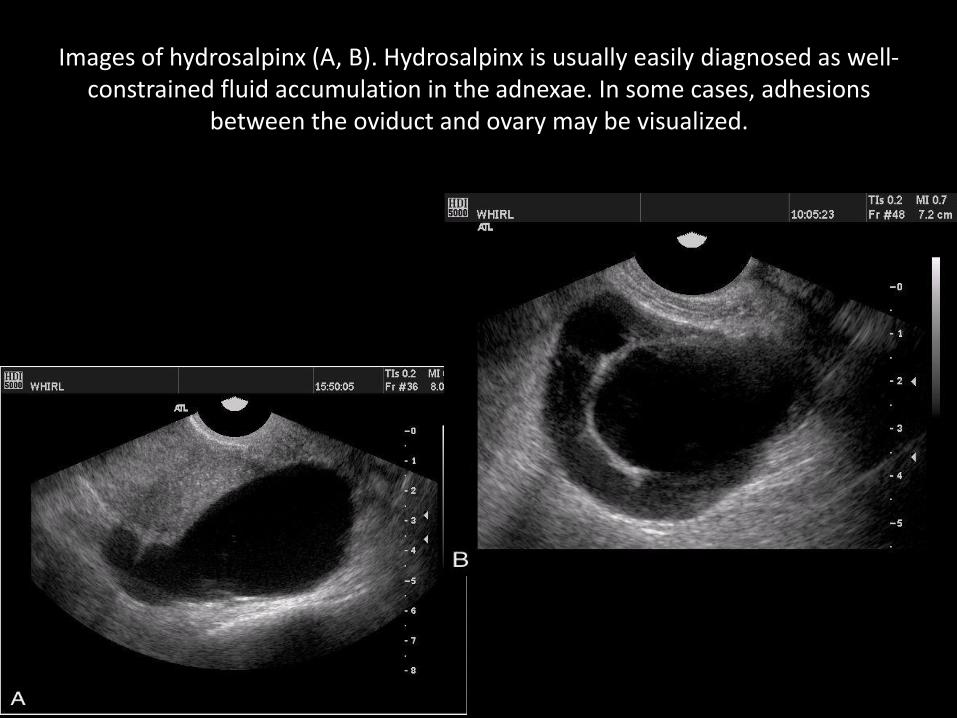
Images of hydrosalpinx (A, B). Hydrosalpinx is usually easily diagnosed as well-constrained fluid accumulation in the adnexae. In some cases, adhesions
between the oviduct and ovary may be visualized.
