in vivo magnetic resonance micro-imaging of the human toe at 3 tesla
TRANSCRIPT

Technical Note
In vivo magnetic resonance micro-imaging of the human toe at 3 tesla
Jozsef Constantin Sze´lesa, Bence Csapo´a, Markus Klarhoferb, Csilla Balassya, Raschid Hodaa,Andreas Bergb, Michael Rodenc, Peter Polterauera, Werner Waldha¨uslc, Ewald Moserb,d,*
aDepartment of Vascular Surgery, University of Vienna Medical School, Vienna, AustriabInstitute for Medical Physics, University of Vienna, Vienna, Austria
cDepartment of Internal Medicine III, Division of Endocrinology and Metabolism, University of Vienna Medical School, Vienna, AustriadDepartment of Radiology, University of Vienna Medical School, Vienna, Austria
Abstract
The feasibility of in vivo high-resolution magnetic resonance micro-imaging of fine anatomic structures of human toes was tested.Five healthy subjects were investigated on an experimental 3 Tesla whole body scanner, using standard 3D gradient echo sequences.A radio-frequency surface coil was used for signal detection. Feet, toes and surface coil were comfortably fixed using a home builtdevice for positioning and reduction of motion artifacts. The spatial resolution of 117� 313� 375�m3 allowed detailed visualizationof anatomic structures like skin layers, vessels and nerves. In addition, oval structures with diameters ranging from 500 to 1000�mwere observed in all subjects, which could represent the sensory nerve endings of Vater-Pacinian bodies. Thus, high resolution MRmicro-imaging at 3 Tesla may provide improved morphologic information in distal extremities of humans in vivo. © 2001 ElsevierScience Inc. All rights reserved.
Keywords: MRI; Micro-imaging; Human toe; Vater-Pacinian bodies; 3 Tesla
1. Introduction
Since its first application magnetic resonance imaging(MRI) rapidly developed into one of the most versatilediagnostic tools in medicine, yielding far better contrast insoft tissues than other imaging modalities like conven-tional X-ray, or computed tomography. Both the fastprogress in magnetic resonance (MR) and computer tech-nology as well as the growing interest in better spatialresolution led to MR microscopy, a field with manypromising prospects. MR imaging at spatial resolutionsbetter than those achievable with the naked human eye(i.e., better than 100 –200�m) are referred to as MRmicro-imaging or microscopy, depending on voxel size[1]. In animal and plant experiments, or investigations oncell cultures, exceptionally high resolutions of 4 –10�mhave been obtained [2,3]. These experiments requireultrahigh magnetic field strengths and, therefore, smallbore magnets to achieve reasonable signal-to-noise ratios(SNR). Unfortunately, such equipment is inappropriate
for human medical applications in vivo. In human skinstudies on whole body MRI systems spatial resolutionsfrom 19 � 78 � 800 �m3 to 156 � 936 � 1500 �m3
have been reported [4 – 6]. High-resolution imaging ofhuman extremities so far commonly concentrated on thehuman finger [7–9], whereas MRI investigations of thehuman toe were conducted only at field strengths of 1–1.5T for the description of rare morphologic disorders [10 –13]. The present study focused on designing a method toinvestigate the structure and fine morphology of the distalparts of human extremities. A number of pathologiesmanifest in this anatomic region whose early non-inva-sive detection could carry particular significance in pres-ervation of general health condition by enabling earlytherapy for prevention of associated complications. Con-sequently, this study was designed to evaluate the feasi-bility and practicability of in vivo high resolution MRinvestigation of fine anatomic details within the humantoe on high-field whole body MRI equipment. In partic-ular, attempts were made to detect Vater-Pacini sensorynerve endings [14] in healthy subjects to define normalMR based anatomy as a basis for future in vivo explora-tion of pathology in this confined region by MR micro-imaging.
* Corresponding author. Tel.:�431-4277-60713; fax:�431-4277-9607.
E-mail address: [email protected] (E. Moser).
Magnetic Resonance Imaging 19 (2001) 1235–1238
0730-725X/01/$ – see front matter © 2001 Elsevier Science Inc. All rights reserved.PII: S0730-725X(01)00461-1
2. Material and methods
Big toes of five healthy individuals (male/female: 4/1,25–46 years) were imaged at 3 T. Measurements wereperformed on a Bruker Medspec 30/80 (Bruker Medical Inc.,Ettlingen, Germany), equipped with an asymmetric head gra-dient system B-GA33 (inner diameter 33 cm, Gmax � 29mT/m) and a small radio-frequency (rf) surface coil (coil di-ameter 3 cm). A custom built positioning device was con-structed (Fig. 1), enabling exact positioning and fixation of feetand surface coil, markedly reducing motion artifacts and alsocompensating for different foot shapes and sizes. Imaging wascarried out on subjects lying in supine position with their feetplaced comfortably in the bore of the gradient system. Astandard 3D gradient echo sequence with the following param-eters was used for imaging: FOV: 30 � 30 � 18 mm3, matrix:256 � 96 � 48, spatial resolution: 117 � 313 � 625 �m3, TR:100 ms, TE: 10 ms, flip angle 25°, aquisition bandwidth: 50kHz, number of averages: 4, total acquisition time: 30.7 min.The Ethics Committee of the Medical School of the Universityof Vienna and the General Hospital of Vienna (EK-No. 394/97) approved the protocol.
3. Results
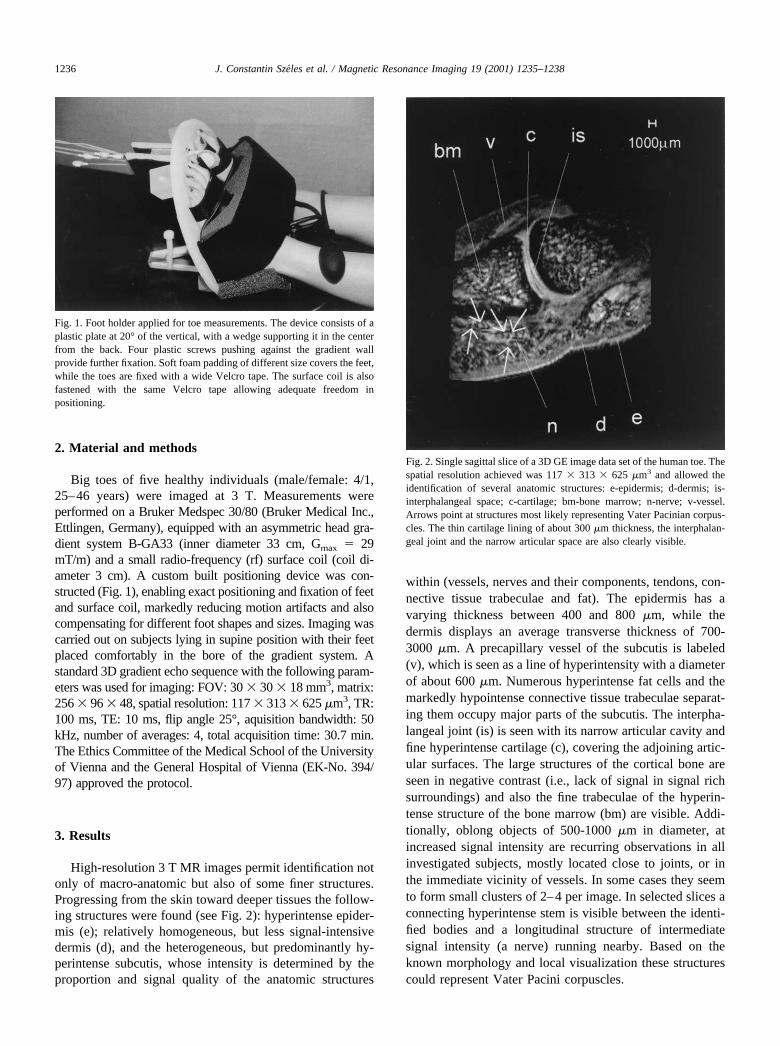
High-resolution 3 T MR images permit identification notonly of macro-anatomic but also of some finer structures.Progressing from the skin toward deeper tissues the follow-ing structures were found (see Fig. 2): hyperintense epider-mis (e); relatively homogeneous, but less signal-intensivedermis (d), and the heterogeneous, but predominantly hy-perintense subcutis, whose intensity is determined by theproportion and signal quality of the anatomic structures
within (vessels, nerves and their components, tendons, con-nective tissue trabeculae and fat). The epidermis has avarying thickness between 400 and 800 �m, while thedermis displays an average transverse thickness of 700-3000 �m. A precapillary vessel of the subcutis is labeled(v), which is seen as a line of hyperintensity with a diameterof about 600 �m. Numerous hyperintense fat cells and themarkedly hypointense connective tissue trabeculae separat-ing them occupy major parts of the subcutis. The interpha-langeal joint (is) is seen with its narrow articular cavity andfine hyperintense cartilage (c), covering the adjoining artic-ular surfaces. The large structures of the cortical bone areseen in negative contrast (i.e., lack of signal in signal richsurroundings) and also the fine trabeculae of the hyperin-tense structure of the bone marrow (bm) are visible. Addi-tionally, oblong objects of 500-1000 �m in diameter, atincreased signal intensity are recurring observations in allinvestigated subjects, mostly located close to joints, or inthe immediate vicinity of vessels. In some cases they seemto form small clusters of 2–4 per image. In selected slices aconnecting hyperintense stem is visible between the identi-fied bodies and a longitudinal structure of intermediatesignal intensity (a nerve) running nearby. Based on theknown morphology and local visualization these structurescould represent Vater Pacini corpuscles.
Fig. 1. Foot holder applied for toe measurements. The device consists of aplastic plate at 20° of the vertical, with a wedge supporting it in the centerfrom the back. Four plastic screws pushing against the gradient wallprovide further fixation. Soft foam padding of different size covers the feet,while the toes are fixed with a wide Velcro tape. The surface coil is alsofastened with the same Velcro tape allowing adequate freedom inpositioning.
Fig. 2. Single sagittal slice of a 3D GE image data set of the human toe. Thespatial resolution achieved was 117 � 313 � 625 �m3 and allowed theidentification of several anatomic structures: e-epidermis; d-dermis; is-interphalangeal space; c-cartilage; bm-bone marrow; n-nerve; v-vessel.Arrows point at structures most likely representing Vater Pacinian corpus-cles. The thin cartilage lining of about 300 �m thickness, the interphalan-geal joint and the narrow articular space are also clearly visible.
1236 J. Constantin Szeles et al. / Magnetic Resonance Imaging 19 (2001) 1235–1238

4. Discussion
Despite recent progress in in-vivo MR microscopy, theterm MR microscopy remains somewhat ambiguous as it isnot clearly defined. Isotropic spatial resolution of below 100�m is limited mostly to in vitro, or special in vivo animal orplant investigations, but are not generally available for hu-man studies. Thus any high-resolution studies not achievingsuch high in plane resolutions, should rather be termed MRmicro-imaging. The feasibility of MR micro-imaging forsmall structures of the toe is demonstrated in this study. Inorder to minimize motion artifacts a special fixation devicewas constructed which allows exact positioning of rf coiland feet of different sizes and shapes. Such a supportingdevice not only has to provide proper fixation, but will alsobe required to prevent any ischemic injuries during themeasurements, particularly in patients suffering from occlu-sive vascular disease. On all images acquired the standardmacro-anatomy of the human toes is identifiable with cer-tainty, such as skeletal structures and the different layers ofthe skin—epidermis, dermis, subcutis. The high proportionof keratinocytes in the epidermis in various stages of theirdevelopment are responsible for the bright signal [4].Within the subcutis the ample amount of fat cells gather insmaller or larger hyperintense groups, separated by hypoin-tense connective tissue trabeculas. As water in connectivetissue of the dermis and subcutis is tightly bound it has tooshort T2 values to be visible with conventional imagingprotocols. Small vessels of the toes running in the subcutisare also well detectable and give an intermediate signal, asthe strong signal intensity caused by the high proton densityof blood is somewhat decreased due to flow related dephas-ing effects. These vessels can serve as important landmarksfor orientation and detection of other, smaller structures. Incomparison, peripheral nerves running mostly along largervessels yield only a slightly higher signal intensity than theirsurroundings and so are difficult to identify. Different parts ofthe long bones in the toes are also observable. The corticalsubstance (stratum compactum, consisting of predominantlycalcium-hydroxyapatite crystals) gives hardly any signal withthe applied pulse-sequences, and thus appears dark in all im-ages. In sharp contrast bone marrow appears bright, demon-strating an inner structure of high signal intensity stroma (bonemarrow) and low intensity trabeculae. The articulating jointbetween two adjacent bones is also clearly presented, as thearticular cartilage gives a hyperintense signal, whereas theintraarticular liquid provides only intermediate signal intensity.The MR presentation of the described structures correspondswell to that observed by high resolution studies of the upperextremity [7].
Vater-Pacini sensory bodies in the subcutis of distalhuman extremities are known to be terminal nerve endingsresponsible for sensation of vibration [15]. Their innerstructure consists of a terminal nerve ending with its owncapillary supply, surrounded by a capsule of gel-like mate-rial [16] of high water content, separated into two distinct
compartments. The inner core is built up from up to 20concentric Schwann cell membranes, while the outer core ofsimilar arrangement is continuous with the perineurinum ofthe innervating axon, but with up to 70 layers. Their sizeranges between 50–100 �m [17] and 1500–2000 �m [18]depending on their location. Their special morphology(compartments of high water content) results in hyperin-tense presentation of these small oblong structures in thetypical location (i.e., close to vessels and joints) on appliedMR micro-images, indicating the educible location ofVater-Pacini bodies. This applies in particular to structuresthat are apparent to be connecting with a narrow stem to anadjoining peripheral nerve. Since the largest diameter of thesensory bodies and the direction of their stem do not alwaysfall into the same plane, their simultaneous presentationwithin an image can not always be expected. Alternativelyseveral other structures have to be considered as possiblecandidates for differential diagnosis. These include Meiss-ner bodies (�40–100 �m in diameter) and Golgi-Mazzonibodies (similar to Vater-Pacini bodies but without outercore: 20–40 �m in size). Differentiation is predominantlybased on size, as all these structures are markedly smallerthan Vater-Pacinian bodies. Despite the fact that the nomi-nal resolution is better than the expected diameter of neuralstructures investigated, it is estimated that for the positiveidentification of any homogeneous structure on a MR imagea minimal coverage of at least 1 pixel, for the identificationof shape at least 6–8 pixels are needed. The identification ofthe latter, however, is accessible by the resolution of 117 �313 � 375 �m3 achieved in this study.
In conclusion, MR micro-imaging offers the potential ofin vivo visualization of small anatomic structures at a res-olution and with contrast not achievable by other imagingmodalities. To achieve this, special instrumentation highfield strength and strong gradients are required. Visualiza-tion of fine structures of the human toe by MR micro-imaging may become a helpful tool for strengthening thediagnosis of some diseases including diabetic angio- andneuropathy, Raynaud’s phenomenon, alcoholic neuropathyas well as spondyloarthropathy and tophaceous gout, orother systemic diseases presenting in the lower extremities,in particular as 3 Tesla whole body systems are currentlytested for routine clinical work.
Acknowledgments
Grant sponsor: Fonds zur Forderung der wissenschaftli-chen Forschung (FWF), grant number P12041MED.
References
[1] Lauterbur P. MR microscopy using projection reconstruction. In:Blumich B, Kuhn W, editors. Magnetic resonance microscopy. Wein-heim: VCH, 1992. p. 3–25.
1237J. Constantin Szeles et al. / Magnetic Resonance Imaging 19 (2001) 1235–1238

[2] Aguayo JB, Blackband SJ, Schoeniger J. Nuclear Magnetic Reso-nance imaging in a single cell. Nature 1986;322:190–1.
[3] Cho ZH, Ahn CB, Juh SC, Lee HK, Jacobs RE, Lee S, Yi JH, Jo JM.Nuclear magnetic resonance microscopy with 4-�m resolution: the-oretical study and experimental results. Med Phys 1989;15:815–24.
[4] Song HK, Wehrli FW, Ma J. In vivo MR microscopy of the humanskin. Magn Reson Med 1997;37:85–91.
[5] Richard SB, Querleux BG, Bittoun J. Characterization of the skin invivo by high resolution magnetic resonance imaging: water behaviorand age-related effects. J Invest Dermatol 1993;100:705–9.
[6] Ablett S, Burdett NG, Carpenter TA, Hall LD, Salter DC. Short echotime MRI enables visualisation of the natural state of human stratumcorneum water in vivo. Magn Res Imaging 1996;14:357–60.
[7] Blackband SJ, Chakrabarti I, Gibbs P, Buckley DL, Horsman A.Fingers: three-dimensional MR imaging, and angiography with alocal gradient coil. Radiology 1994;190:895–9.
[8] Erickson SJ, Kneeland JB, Middleton WD, Jesmanowicz A, Hyde J,Lawson TL, Foley WD. MR imaging of the finger: correlation withnormal anatomic sections. Am J Roentgenol 1989;152:1013–9.
[9] Klarhofer M, Csapo B, Balassy C, Szeles JC, Moser E. Blood flowvelocities in the human finger. Magn Reson Med 2001;45:716–19.
[10] Drape JL, Idy-Peretti I, Goettmann S, Guerin-Surville H, Bittoun J.Standard and high resolution magnetic resonance imaging of glomustumors of toes and fingertips. J Am Acad Dermatol 1996;35:550–5.
[11] Zanetti M, Ledermann T, Zollinger H, Hodler J. Efficacy of MRimaging in patients suspected of having Morton’s neuroma. Am JRoentgenol 1997;168:529–32.
[12] D’Souza D, McDiarmid J, Tickle C. A polydactylous human footwith ‘double-dorsal’ toes. J Anat 1998;193:121–30.
[13] Katz JB. Progressive macrodactyly. J Foot Ankle Surg 1999;38:143–6.[14] Vater A. Dissertatio de consensu partium corporis humani. Haller.
isputationum Anatomicarum selectarum. Gottingaeh, vol. 2, pp. 953–72; 1741.
[15] Iggo A. Is the physiology of cutaneous receptors determined bymorphology? Prog Brain Res 1976;43:15–31.
[16] Fawcett DW, Jensh RP. Bloom & Fawcett: concise histology. NewYork: Chapman and Hall, 1997. p. 179.
[17] Bistevins R, Awad E. A structure and ultrastructure of mechanore-ceptors at the human musculotendinous junction. Arch Phys MedRehabil 1981;62:74–83.
[18] Stark B Carlstedt T, Hallin RG. Distribution of human Paciniancorpuscules in the hand. A cadaver study. Br J Hand Surg 1998;23:370–2.
1238 J. Constantin Szeles et al. / Magnetic Resonance Imaging 19 (2001) 1235–1238