inappropriate sinus tachycardia
DESCRIPTION
THE BEST MANAGEMENT OF ISTTRANSCRIPT

www.medscape.com
'Inappropriate' Sinus TachycardiaDoes the 100 Beats per min Cut-off Matter?Rashmi U Hottigoudar, Rakesh Gopinathannair
Future Cardiol. 2013;9(2):273-288.
Abstract and IntroductionAbstract
Sinus tachycardia is commonly encountered in clinical practice and when persistent, can result in significant symptoms and impaired quality of life, warranting further evaluation. On the other hand, a growing body of epidemiological and clinical evidence has shown that high resting heart rate (HR) within the accepted normal range is independently associated with increased risk of all-cause and cardiovascular mortality. However, higher HR as a risk factor for adverse cardiovascular outcomes is frequently underappreciated. In this review, we focus on two challenging problems that span the spectrum of abnormally fast sinus HR. The first section reviews inappropriate sinus tachycardia, a complex disorder characterized by rapid sinus HR without a clear underlying cause, with particular emphasis on current management options. The latter section discusses the prognostic significance of elevated resting HR and reviews clinical evidence aimed at modifying this simple, yet highly important risk factor.
Introduction
Heart rate (HR) is perhaps the most frequently monitored vital sign and affects medical decision-making in everyday clinical practice. It is a key determinant of myocardial work and metabolic requirements.[1,2] Of the cardiac arrhythmias, sinus tachycardia (ST; sinus rate >100 bpm) is perhaps the most frequently encountered in clinical practice. The evaluation and management of ST involves careful assessment to determine whether tachycardia is an appropriate response to an underlying illness. This appropriate ST can be secondary to a variety of pathological conditions whose discussion is beyond the scope of this article.
However, a small proportion of patients, mostly young adults, have marked resting ST without underlying secondary causes or structural heart disease. This can often lead to debilitating symptoms and is referred to as inappropriate ST (IST). IST is an often under-recognized problem with significant morbidity. There is a paucity of knowledge with regards to the pathophysiology of IST and this, along with identifying effective management options, remains an active area of research.
Animal studies first noted that increased HR is associated with detrimental vascular effects and decreased survival.[3] Epidemiological, as well as human, clinical trials have provided further evidence for a strong association between elevated HR and adverse cardiovascular outcomes.[4–10] Over the course of the past few years, high resting sinus HR within the normal range of 60–100 bpm has become an exciting area of investigation as more and more data have emerged supporting its role in predicting hard clinical end points,[9,11–
13] and has led to suggestions that it is time to redefine tachycardia.[14,15] This has resulted in the trial of pharmacological approaches at ameliorating this risk.[16,17]
In this review, we focus on the pathophysiology, clinical characteristics, diagnosis and management of IST. We also review the prognostic significance of high resting sinus HR, as well as outcome data on the ability to modify this important clinical variable.
ISTClinical Vignette
A 29-year-old female with no prior cardiac history presented for evaluation of a 2-year history of palpitations associated with significant nausea, dyspnea and dizziness that were exacerbated with minimal activity. These symptoms started after her second pregnancy and had been progressively worsening over the preceding few months, significantly impairing her quality of life. A 12-lead ECG during an episode of symptomatic palpitations

showed a narrow complex tachycardia at 187 bpm. P-wave morphology was difficult to characterize (Figure 1A). Upon gradual slowing of the tachycardia, a second ECG obtained clearly shows p-wave morphology similar to sinus rhythm (Figure 1B), suggestng ST as the culprit rhythm for the patient's symptoms. Total blood count, hematocrit and thyroid function were normal. Extensive evaluation failed to disclose any underlying acute or chronic illness contributing to tachycardia. A transthoracic echocardiogram showed a structurally normal heart. A 24-h Holter monitor revealed an average resting sinus HR of 130 bpm (range: 102–213 bpm) (Figure 2).
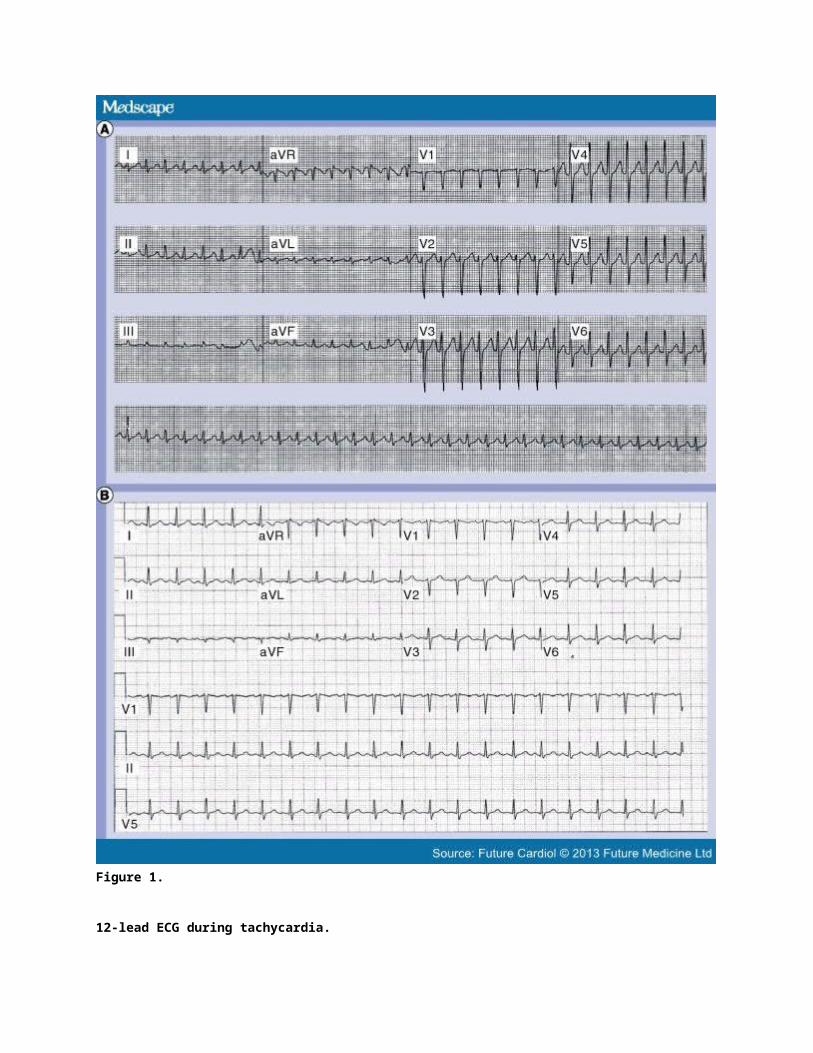
Figure 1.
12-lead ECG during tachycardia.
(A) 12-lead ECG during tachycardia in the patient presented in the 'Clinical vignette' section. This shows a
narrow complex tachycardia with a ventricular rate of 187 bpm and difficult-to-characterize p-waves. (B) Tachycardia gradually slowed without any sudden transition and a second ECG now shows sinus tachycardia (upright p-waves in leads 1, aVL, II, III, aVF, biphasic p-wave in V1 and negative p-wave in lead aVR) at 115 bpm.
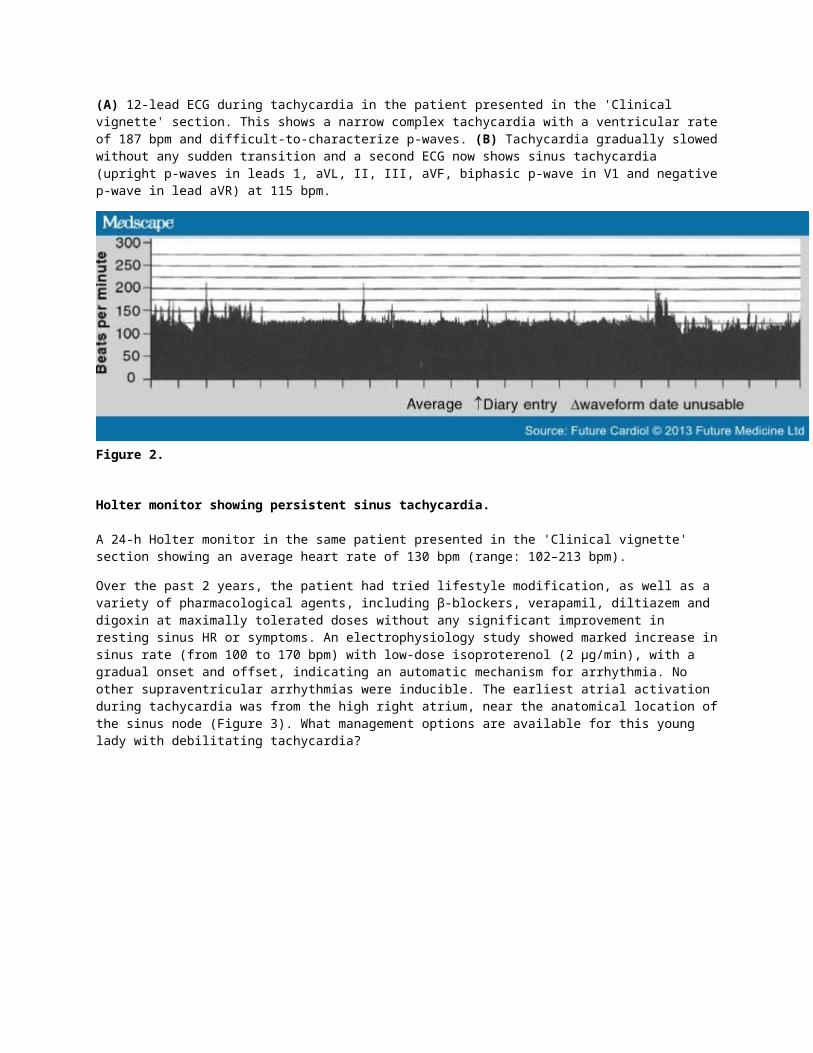
Figure 2.
Holter monitor showing persistent sinus tachycardia.
A 24-h Holter monitor in the same patient presented in the 'Clinical vignette' section showing an average heart rate of 130 bpm (range: 102–213 bpm).
Over the past 2 years, the patient had tried lifestyle modification, as well as a variety of pharmacological agents, including β-blockers, verapamil, diltiazem and digoxin at maximally tolerated doses without any significant improvement in resting sinus HR or symptoms. An electrophysiology study showed marked increase in sinus rate (from 100 to 170 bpm) with low-dose isoproterenol (2 µg/min), with a gradual onset and offset, indicating an automatic mechanism for arrhythmia. No other supraventricular arrhythmias were inducible. The earliest atrial activation during tachycardia was from the high right atrium, near the anatomical location of the sinus node (Figure 3). What management options are available for this young lady with debilitating tachycardia?
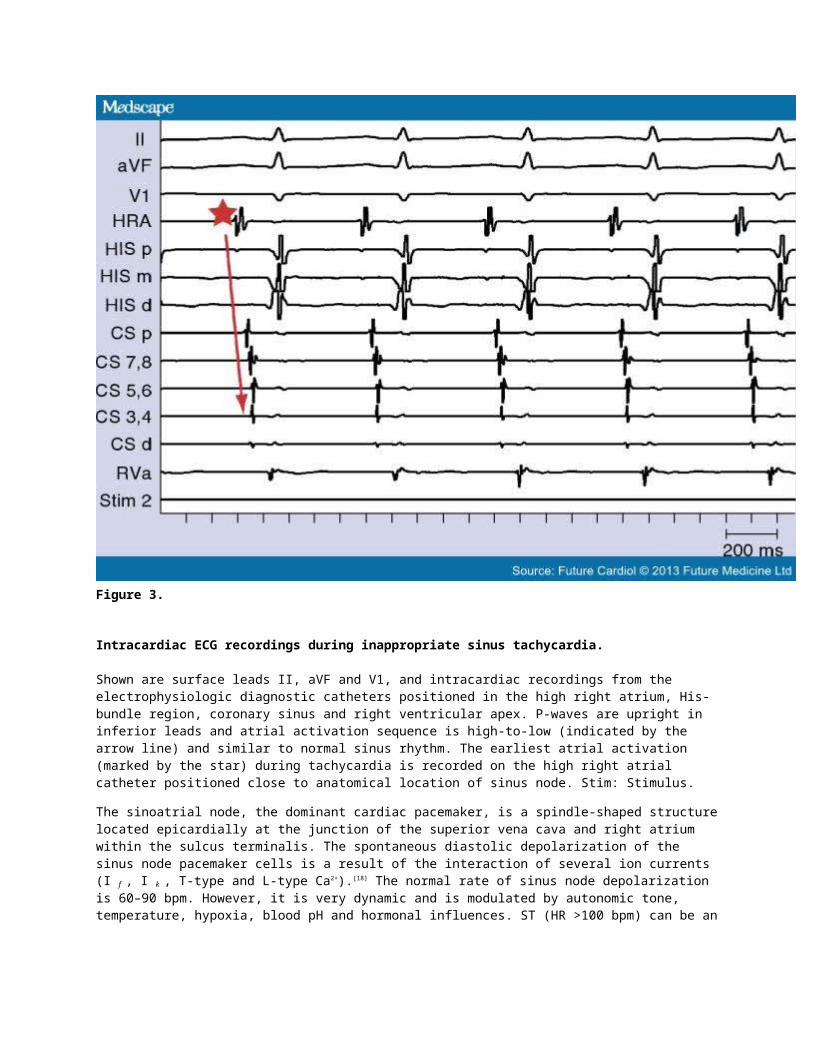
Figure 3.
Intracardiac ECG recordings during inappropriate sinus tachycardia.
Shown are surface leads II, aVF and V1, and intracardiac recordings from the electrophysiologic diagnostic catheters positioned in the high right atrium, His-bundle region, coronary sinus and right ventricular apex. P-waves are upright in inferior leads and atrial activation sequence is high-to-low (indicated by the arrow line) and similar to normal sinus rhythm. The earliest atrial activation (marked by the star) during tachycardia is recorded on the high right atrial catheter positioned close to anatomical location of sinus node. Stim: Stimulus.
The sinoatrial node, the dominant cardiac pacemaker, is a spindle-shaped structure located epicardially at the junction of the superior vena cava and right atrium within the sulcus terminalis. The spontaneous diastolic depolarization of the sinus node pacemaker cells is a result of the interaction of several ion currents (I f , I k , T-type and L-type Ca2+).[18] The normal rate of sinus node depolarization is 60–90 bpm. However, it is very dynamic and is modulated by autonomic tone, temperature, hypoxia, blood pH and hormonal influences. ST (HR >100 bpm) can be an appropriate or an inappropriate response to physiologic, pathologic or pharmacological triggers ().[19]
Box 1. Common causes of sinus tachycardia.
Fever
Hypovolemia
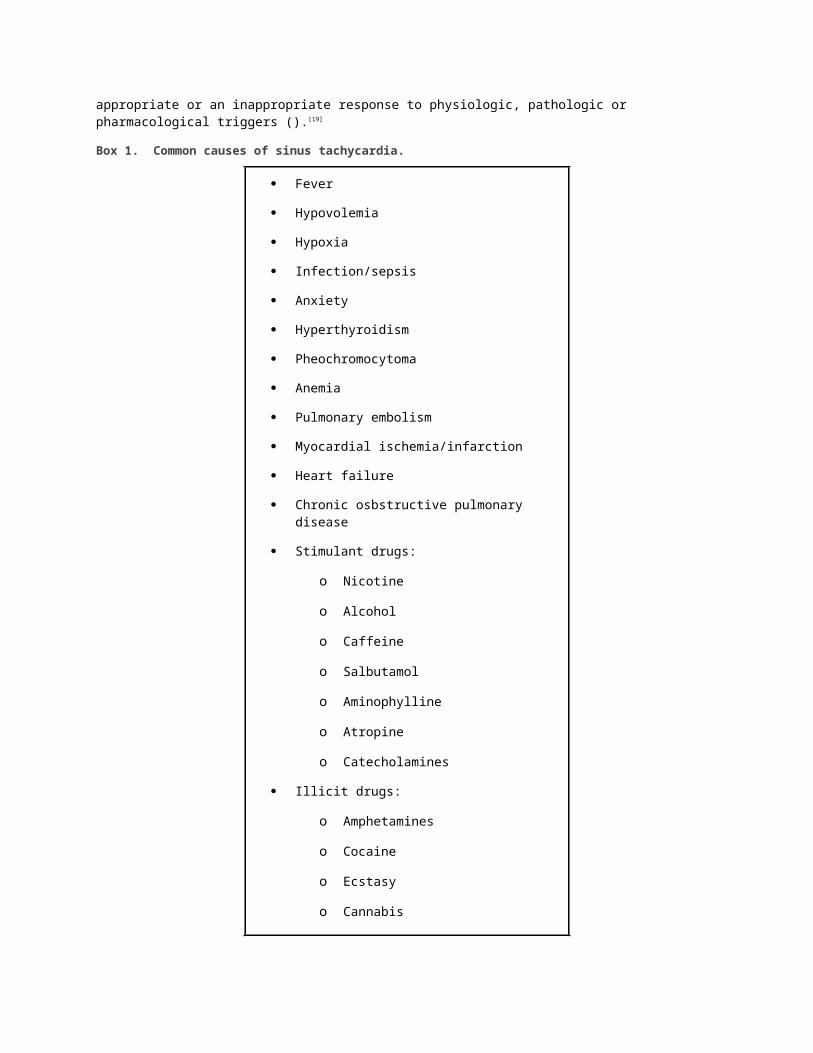
Hypoxia
Infection/sepsis
Anxiety
Hyperthyroidism
Pheochromocytoma
Anemia
Pulmonary embolism
Myocardial ischemia/infarction
Heart failure
Chronic osbstructive pulmonary disease
Stimulant drugs:
o Nicotine
o Alcohol
o Caffeine
o Salbutamol
o Aminophylline
o Atropine
o Catecholamines
Illicit drugs:
o Amphetamines
o Cocaine
o Ecstasy
o Cannabis
Anticancer drugs:
o Anthracycline compounds:
o Doxorubicin
o Daunorubicin
IST, a nonparoxysmal tachyarrhythmia, was originally described in 1939 by Codvelle and Boucher as a case of a healthy young adult man with a resting HR in the range of 160 bpm for more than 2 years.[20] In 1941, Wising reported a clustering of unexplained persistent ST of very long duration in a family of four members. [21] Bauernfeind et al., in 1979, performed electrophysiolgical studies on seven patients with IST and showed that a high-to-low right atrial activation sequence and atrial pacing neither terminated nor affected the tachycardia cycle length.[22] These findings suggested increased sinus node automaticity as the arrhythmia mechanism. In addition, HR response to pharmacologic autonomic blockade suggested an underlying defect either in the
sympathetic or vagal nerve control of resting sinus HR, with or without an abnormality of intrinsic HR. [22] The sympathovagal influence in IST was further explored by Morillo et al. in 1994 who proposed that IST was characterized by high intrinsic HR, depressed efferent cardiovagal reflex and β-adrenergic receptor hypersensitivity.[23] Over the years, this clinical entity has intrigued clinicians and researchers alike, and remains an active area of investigation to this day.
IST is characterized by a persistent increase in resting sinus HR out of proportion to physiological or pathological stress. It is a diagnosis of exclusion and, hence, the patient needs to be evaluated for secondary causes of ST, such as endocrinopathies, hypovolemia, anemia, infection, autonomic dysfunction, orthostatic hypotension and drug effects (Box 1).[19] IST is predominantly seen in young adult females in their second to fourth decade of life and commonly in healthcare professionals.[19] Less frequently, the dysrhythmia is also encountered in elderly patients.[24]
Pathophysiology
The pathophysiology of IST is complex and not well understood. Experimental and clinical studies have shown multiple pathophysiological mechanisms in IST. It is generally accepted that the pathogenesis of IST is multifactorial, with the principal mechanism potentially being enhanced intrinsic sinus node automaticity potentiated by altered sympathovagal balance. Other contributing mechanisms may include β-adrenergic hypersensitivity, M2 anticholinergic hyposensitivity, abnormal baroreflex activity and regional autonomic dysregulation.[25–27] The extent of contribution of each of the mechanisms in isolation remains unknown.
High intrinsic HR (IHR) in patients with IST has been reported, but with variable frequency. Bauernfeind et al. noted that four out of seven patients with IST had an IHR higher than the age-predicted normal range. [22] Morillo et al. noted a high IHR in all of the six patients with IST,[23] whereas another study reported a higher than age-predicted IHR (115.7 ± 2.7 vs 110.6 ± 1.4; p < 0.01) in seven out of eight patients with IST. [28] The occurrence of IST in transplanted hearts supports an intrinsic abnormality of the sinus node in IST.[29] In 18 patients with IST who had simultaneous sympathetic and parasympathetic pharmacological blockade, an adenosine-induced reflex increase in sinus HR was impaired in patients with IST compared with controls (8.5 ± 8.8% vs 21.2 ± 9.7%; p < 0.001), supporting enhanced sinus node automaticity as the underlying etiology of IST. At a cellular level, this effect was postulated to be due to the deficient function of acetylcholine- and adenosine-sensitive potassium channels.[30]
Sinus node function is regulated by a complex interaction of sympathetic and parasympathetic tone. Hence, autonomic dysfunction (decreased parasympathetic activity and/or excessive sympathetic activity) is suggested to have a pathogenic role in IST. However, the results are not consistent across the studies, likely to be due to different methods of assessment. Sympathovagal balance as assessed by HR variability (HRV) was similar in patients with IST and controls in both supine (low:high frequency ratio 2.8 ± 0.3 vs 2.6 ± 0.4; p = not significant) and upright tilt position (8.7 ± 1.3 vs 8.5 ± 0.8; p = not significant).[23] In a study by Bauernfeind et al., autonomic function was assessed by the resting HR response to propranolol and atropine.[22] IST due to excessive sympathetic activity was deemed the cause in patients with larger than normal decrement in resting HR with propranolol and normal increment in resting HR with atropine. By contrast, IST due to a deficient vagal tone was suggested in patients with normal resting HR decrement with propranolol, but smaller than normal increment in resting HR with atropine.[22] Holter monitor-derived time and frequency domain indices of HRV were studied in patients with IST by Castellanos et al. (ten patients, aged 22–46 years; seven women and three men)[31] and Lopera et al. (four patients, aged 61–71 years, four women),[24] and found that these indices were decreased in all patients with IST, and more so in females, despite HR normalization to 75 bpm. This suggested decreased parasympathetic tone. Depressed cardiovagal reflex and β-adrenergic hypersensitivity is observed in patients with IST, suggestive of impaired sinus node vagal response potentiating sinus node automaticity.[23] IST is also reported in patients after radiofrequency catheter ablation for supraventricular tachycardia.[32–36] While the precise mechanism of this effect remains unclear, it is thought to be secondary to sympathovagal imbalance from denervation injury following radiofrequency ablation.
An autoimmune mechanism mediated by the antiautonomic membrane receptor antibodies has been implicated in the pathogenesis of several cardiovascular disorders.[37] Likewise, in a study by Chiale et al., anti-β-adrenergic receptor antibodies were found in 11 out of 21 (52%; p = 0.001) patients with IST with associated excess sympathetic stimulation.[38]
Pathologic analysis of the surgically excised sinus node in three young female patients with IST by Lowe et al., demonstrated lipofuscin-laden vacuoles in the transitional cells of the sinus node suggesting that cellular degeneration is likely altering the hierarchial automaticity of the sinus node.[39]
Evidence of extracardiac autonomic dysfunction has been noted in patients with IST similar to postural orthostatic tachycardia syndrome.[31,40] In a study of seven patients with IST by Shen et al., autonomic function testing (sudomotor function, cardiovagal regulation and vasomotor regulation) was noted to be abnormal with findings suggestive of length-dependent autonomic denervation (four patients), decreased cardiovagal regulation (two patients), peripheral adrenergic deficit (two patients) and hyperadrenergic state (three patients).[40] These patients, despite undergoing sinus node modification, were noted to have a persistence of symptoms, suggesting limited systemic autonomic dysregulation as the etiology of extracardiac symptoms in IST.[40]
Clinical features & diagnosis
The clinical presentation of IST is highly variable and ranges from asymptomatic to highly debilitating. The symptoms include palpitations, near-syncope, syncope, chest pain, shortness of breath, anxiety, fatigue and exercise intolerance. Concurrent behavioral and psychological problems are frequent and persistent. It is often clinically challenging to reproduce and correlate patients' symptoms, activity and HR.[25–27] IST is a diagnosis of exclusion and requires thorough evaluation to rule out of secondary causes of ST (Box 1). Common diagnostic modalities such as 12-lead ECG, echocardiography, 24-h Holter monitoring and an exercise treadmill test can help document occurrence of ST out of proportion to physiologic need, and to rule out other supraventricular arrhythmias. Echocardiography should be considered for the evaluation of structural heart disease. An invasive electrophysiology study is indicated when the etiology of tachycardia is unclear. Electrophysiology testing, in addition to providing diagnostic clues for IST, is useful to evaluate and appropriately treat any non-IST tachyarrhythmias.[41]
The diagnostic electrocardiographic and electrophysiologic characteristics of IST include:
A resting sinus HR of >100 bpm;
An exaggerated HR response with minimal activity, such as an increase in sinus HR to >25–30 bpm from supine to upright position;
Reduction or normalization of sinus rate during sleep;
P-wave morphology and axis during tachycardia similar to normal sinus rhythm (Figure 1B).
During invasive electrophysiologic testing:
Absence of other inducible supraventricular tachyarrhythmias;
During tachycardia, a gradual increase and decrease in sinus HR spontaneously or with isoproterenol infusion suggestive of automatic mechanism of IST;
Electroanatomic mapping showing endocardial atrial activation of the tachycardia similar to sinus rhythm in a craniocaudal fashion (Figure 3), with the earliest activation localized at the superior aspect of the Crista Terminalis (estimated from fluoroscopic images, intracadiac echocardiography, or advanced 3D electroanatomic mapping techniques) and caudal migration of the earliest activation along the crista terminalis with a decrease in the tachycardia rate (Figure 4a).[19,25–27,41]
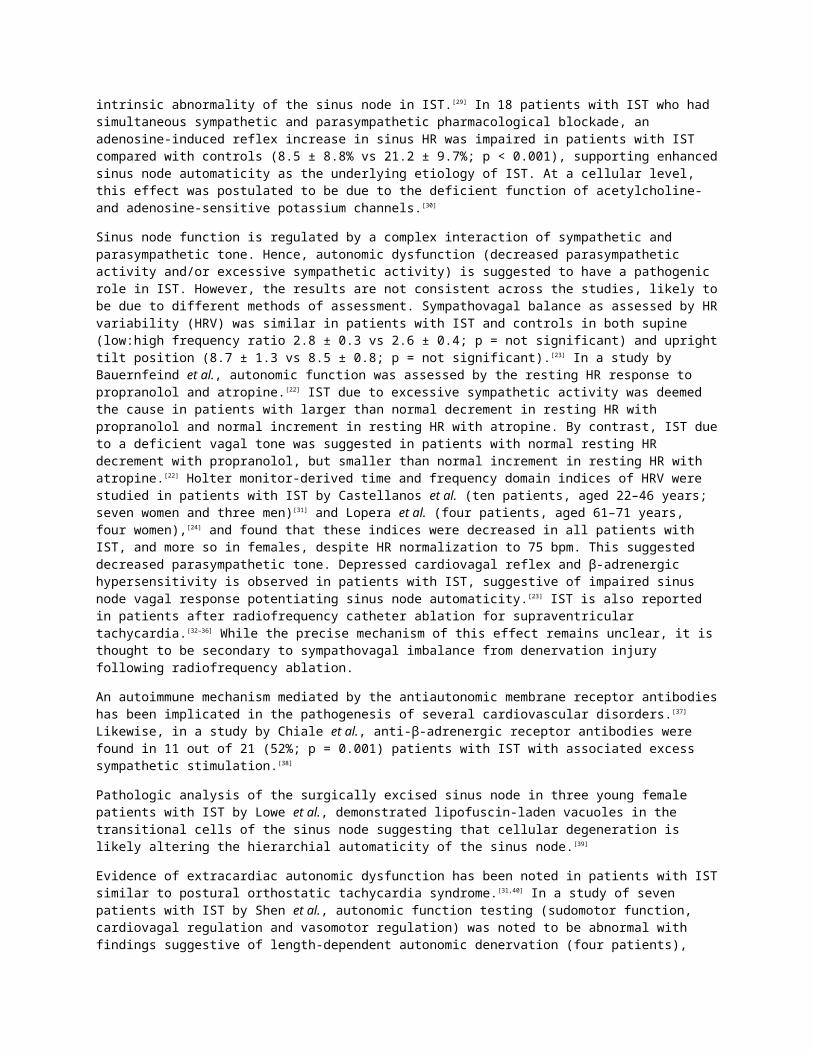
Figure 4.
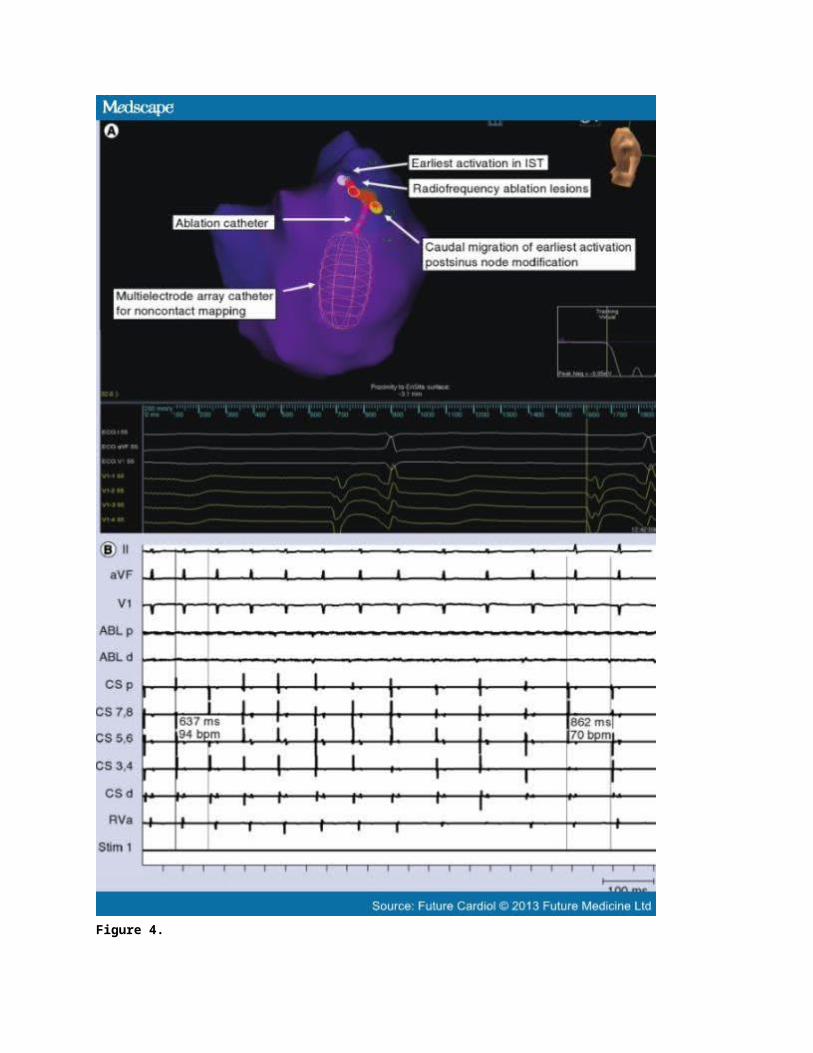
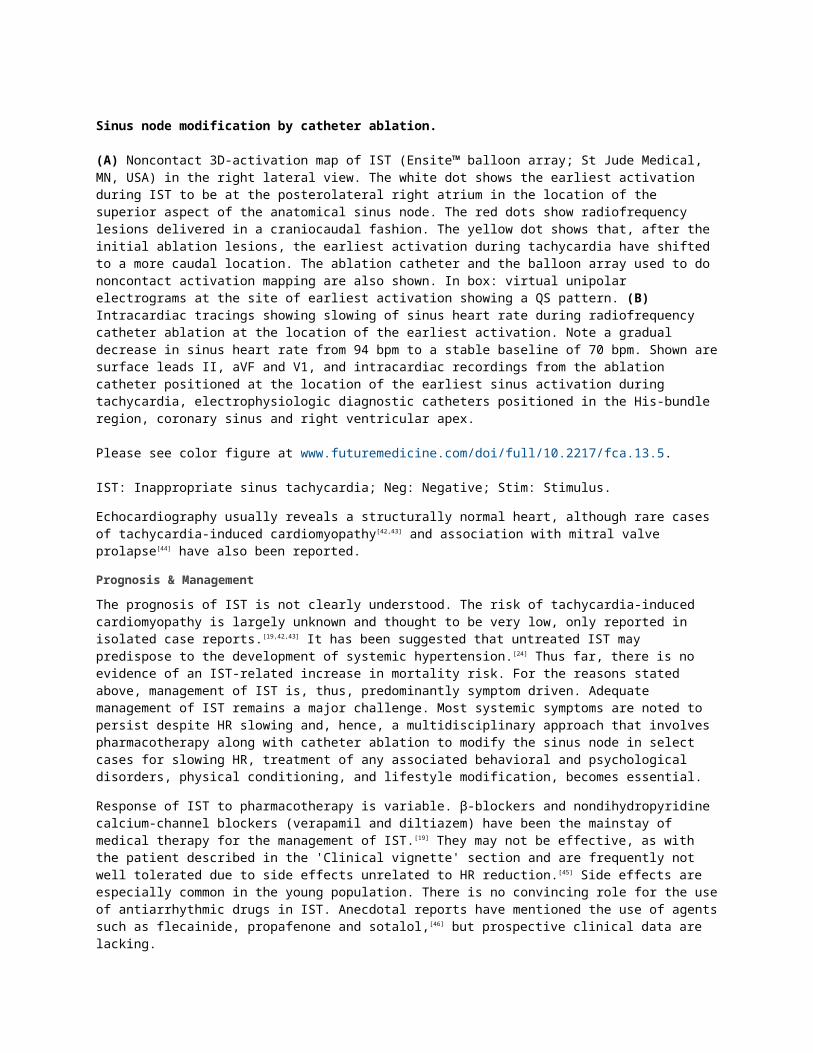
Sinus node modification by catheter ablation.
(A) Noncontact 3D-activation map of IST (Ensite™ balloon array; St Jude Medical, MN, USA) in the right lateral view. The white dot shows the earliest activation during IST to be at the posterolateral right atrium in the location of the superior aspect of the anatomical sinus node. The red dots show radiofrequency lesions delivered in a craniocaudal fashion. The yellow dot shows that, after the initial ablation lesions, the earliest activation during tachycardia have shifted to a more caudal location. The ablation catheter and the balloon array used to do noncontact activation mapping are also shown. In box: virtual unipolar electrograms at the site of earliest activation showing a QS pattern. (B) Intracardiac tracings showing slowing of sinus heart rate during radiofrequency catheter ablation at the location of the earliest activation. Note a gradual decrease in sinus heart rate from 94 bpm to a stable baseline of 70 bpm. Shown are surface leads II, aVF and V1, and intracardiac recordings from the ablation catheter positioned at the location of the earliest sinus activation during tachycardia, electrophysiologic diagnostic catheters positioned in the His-bundle region, coronary sinus and right ventricular apex.
Please see color figure at www.futuremedicine.com/doi/full/10.2217/fca.13.5.
IST: Inappropriate sinus tachycardia; Neg: Negative; Stim: Stimulus.
Echocardiography usually reveals a structurally normal heart, although rare cases of tachycardia-induced cardiomyopathy[42,43] and association with mitral valve prolapse[44] have also been reported.
Prognosis & Management
The prognosis of IST is not clearly understood. The risk of tachycardia-induced cardiomyopathy is largely unknown and thought to be very low, only reported in isolated case reports.[19,42,43] It has been suggested that untreated IST may predispose to the development of systemic hypertension.[24] Thus far, there is no evidence of an IST-related increase in mortality risk. For the reasons stated above, management of IST is, thus, predominantly symptom driven. Adequate management of IST remains a major challenge. Most systemic symptoms are noted to persist despite HR slowing and, hence, a multidisciplinary approach that involves pharmacotherapy along with catheter ablation to modify the sinus node in select cases for slowing HR, treatment of any associated behavioral and psychological disorders, physical conditioning, and lifestyle modification, becomes essential.
Response of IST to pharmacotherapy is variable. β-blockers and nondihydropyridine calcium-channel blockers (verapamil and diltiazem) have been the mainstay of medical therapy for the management of IST.[19] They may not be effective, as with the patient described in the 'Clinical vignette' section and are frequently not well tolerated due to side effects unrelated to HR reduction.[45] Side effects are especially common in the young population. There is no convincing role for the use of antiarrhythmic drugs in IST. Anecdotal reports have mentioned the use of agents such as flecainide, propafenone and sotalol,[46] but prospective clinical data are lacking.
The recent development of ivabradine, a selective hyperpolarization-activated I f current inhibitor, offers promise in the management of IST, especially given the restricted expression and activity of the I f current in the sinus node. Until recently, evidence supporting the effectiveness of ivabradine in IST was limited to case reports and case series.[45,47–50] Cappato et al. evaluated the role of ivabradine in IST refractory to β-blockers and nondihydropyridine calcium antagonists in a randomized, double-blind, placebo-controlled, crossover trial.[51] In this study, 21 patients with symptomatic IST on β-blockers or nondihydropyridine calcium antagonists were randomized to placebo versus ivabradine and followed for 6 weeks. IST was defined as mean resting HR of >95 bpm during the daytime hours of a 24-h Holter monitor and/or a rapid, stable symptomatic increase in resting HR >25 bpm when moving from a supine to a standing position, or in response to physiological stress. The study showed that, in patients with IST refractory to β-blockers and nondihydropyridine calcium antagonists, ivabradine eliminated >70% of symptoms reported at baseline with >50% of patients reporting elimination of all symptoms associated with a significant reduction of HR at various conditions (i.e., baseline, after standing, during 24 h, during the daytime, during the night-time and at maximum stress test).
Ptaszynski et al. studied the effectiveness of ivabradine monotherapy in 20 patients with IST refractory to β-blockers and reported that ivabradine was more effective than the maximally tolerated dose of metoprolol succinate in reducing HR and relieving symptoms of IST during daily activity or during exercise, and was well
tolerated.[45] Currently, there are no randomized clinical data to support first-line monotherapy with ivabradine in patients with symptomatic IST. However, the prospective CIBIST trial aims to study the effectiveness and safety of first-line monotherapy with ivabradine (5–7.5 mg twice-daily) when compared with the β-blocker bisoprolol (5–10 mg once-daily) in the treatment of IST and will hopefully answer this question.[201] The study is expected to complete in December 2014. Regarding long-term impact of ivabradine in IST, one study showed that HR reduction with ivabradine improves over time with a greater reduction at 6 months compared with 3 months.[47]
The role of catheter ablation in the management of IST is not well defined. Clinical evidence is sparse and controversial mainly due to a very small number of highly selective patients undergoing the procedure and the lack of a control patient population. Small case series support sinus node modification by radiofrequency catheter ablation as a potential therapeutic option in patients with medically refractory IST.[44] The craniocaudal rate-dependent activation of the sinus node facilitates targeted ablation along the superomedial aspect of the Crista Terminalis for elimination of faster sinus rates, while still maintaining the lower rate pacemaker activity of the sinus node with intact chronotropic competence.[52] During ablation, under a maximum adrenergic state, the ablation catheter is positioned at the most cranial portion of the Crista Terminalis and radiofrequency energy is delivered in a craniocaudal direction along the Crista Terminalis at sites where local endocardial activation precedes the surface p-wave by 15–60 msec.[25,53] High-output pacing should be performed prior to each radiofrequency energy delivery to assess diaphragmatic stimulation to minimize the risk of phrenic nerve injury. Catheter ablation may be guided by intracardiac echocardiography[54–56] or 3D electroanatomic mapping.[57]
Various end points for sinus node modification have been suggested and include an increase in resting sinus cycle length by 10% or a reduction of the resting/baseline sinus rate to <90 bpm, and to <20–25% of maximum HR during isoproterenol infusion,[44,53] with either retention of the normal p-wave axis in the frontal and horizontal planes, or a transient low atrial escape rhythm. Total sinus node ablation is defined as a reduction in HR of >50% of the tachycardia HR with a junctional escape rhythm.
The success rates of sinus node modification, although reported to be favorable in the short-term (76–100%), were noted not to be sustained in the long-term.[25] The success rates appear to be higher with total sinus node ablation, but with a substantially high risk of needing permanent pacing.[44] Procedural risks include phrenic nerve injury and diaphragmatic paralysis, severe bradycardia that may require permanent pacing, injury to the superior vena cava and vascular complications. Despite slowing of the HR with ablation, noncardiac symptoms often persist. Frequently, these patients are noted to have recurrence of IST, as well as occurrence of non-IST tachyarrhythmias at follow-up. In a study by Frankel et al., of the 33 patients who underwent sinus node modification over a mean follow-up of 2.0 ± 1.5 years, 18% were noted to have recurrence of IST and 27% developed new non-IST tachyarrhythmias.[41] Catheter ablation, thus, remains an option, albeit with variable success, for the management of patients with IST and debilitating symptoms who have failed available pharmacotherapy and possible lifestyle and psychosocial modifications.
Back to Our PatientIn our patient, IST was diagnosed based on the following electrophysiologic findings:
Narrow complex tachycardia with sinus p-wave morphology, with gradual onset and offset, suggesting an automatic mechanism. Earliest atrial activation during tachycardia localized to the high right atrium in the region of the anatomic sinus node;
Autonomic influences on the tachycardia (marked increase in HR in response to activity and low-dose isoproterenol, and decrease in HR with rest and sleep);
Electrophysiology study ruling out other supraventricular tachycardias.
Given the debilitating symptoms and failure of available pharmacotherapy (the patient did not receive ivabradine as the drug is not currently available in the USA), and after undertaking extensive discussion with the patient and her family, she decided to undergo endocardial radiofrequency catheter ablation aimed at sinus node modification. IST was easily induced by low-dose isoproterenol infusion with reproduction of patient symptoms. 3D noncontact activation mapping (Ensite™ balloon array; St Jude Medical, MN, USA) showed earliest activation localized to superolateral right atrium near the superior vena cava–right atrial junction. Radiofrequency lesions were delivered at this location that resulted in a decrease in the sinus rate and was associated with a caudal migration of the earliest endocardial sinus activation (Figure 4A). Ablation lesions
were delivered in a craniocaudal direction, targeting the earliest endocardial sinus activation until the baseline sinus rate decreased to approximately 60–70 bpm, with an increase to 100 bpm with 2 µg/min of isoproterenol (Figure 4B). Significant and immediate improvement in symptoms was noted postprocedure. At 1-year follow-up, the patient remained asymptomatic, with marked improvement in exercise tolerance.
One of the important differential diagnoses to consider in this situation is an automatic high right atrial tachycardia, which can at times be challenging to differentiate from IST.[46] Focal atrial tachcyardias often tend to be paroxysmal in nature, whereas, in our case, the chronicity and persistence of the tachycardia supports IST. Moreover, the gradual slowing of tachycardia in response to ablation with a caudal shift in activation pattern rules out focal atrial tachycardia as the mechanism.
Prognostic Significance of Resting HRA large body of experimental and clinical evidence have established high resting sinus HR to be an independent predictor of adverse cardiovascular outcomes, both in the general population, as well as in patients with heart disease.[4,7,10,58–63] Animal studies have shown high HR to have a significant impact at various stages of the pathologic spectrum of cardiovascular disease progression: vascular shear stress and cellular signaling, vascular compliance, endothelial function, coronary blood flow, atherogenesis, plaque rupture and myocardial infarction (MI).[64] Human studies have found elevated HR to be independently associated with the development of hypertension,[4] atherosclerosis,[5] heart failure (HF) and sudden cardiac death.[6,8]
Several epidemiologic studies have linked elevated resting HR with adverse cardiovascular outcomes in the general population, as well as patients with cardiovascular comorbidities, such as hypertension, coronary artery disease, diabetes mellitus and HF.[65] A progressive increase in HR predicted increased cardiovascular and coronary mortality independent of traditional cardiovascular risk factors in a Framingham cohort of 5070 patients free of cardiovascular disease.[9] Multivariate analysis in the CASS registry of approximately 25,000 patients with suspected or proven coronary artery disease followed over a period of 15 years showed that patients with a resting sinus HR of >83 bpm had a significantly higher risk of cardiovascular mortality than subjects with a resting sinus HR of <62 bpm.[58] Castagno et al., in their study of 7599 patients with stable chronic HF, showed that a baseline resting HR is associated with increased mortality, with every 10 bpm increase associated with respective increases of 8% for all-cause mortality and 10% for the composite end point of cardiovascular death and HF hospitalization, irrespective of the dose or usage of β-blockers and left ventricular ejection fraction.[10] The adverse cardiovascular impact of higher HR has been observed in patients with HF and preserved left ventricular systolic function.[66] The association of faster HR with all-cause and cardiovascular mortality in hypertension in elderly patients was observed in the Syst–Eur study by Palatini et al..[67] In this study, it was noted that a HR of ≥79 bpm in elderly patients with isolated systolic hypertension was associated with an 89% increase in the adjusted risk of mortality.[67]
A currently accepted normal HR range of 60–100 bpm is based on the New York Heart Association recommendations.[68] Within this HR range of 60–100 bpm, epidemiologic and clinical studies indicate a gradient association of HR with adverse cardiovascular outcomes, both in the general population, as well as in patients with cardiovascular disorders.[65] In the Framingham study, a sixfold increase in the relative risk of sudden death was seen in subjects in the top HR quintile when compared with those in the bottom quintile.[9] In the NHANES I epidemiologic follow-up study cohort, a resting HR of >84 bpm was associated with an increased risk of cardiovascular and noncardiovascular mortality in men and white women.[7] In a cohort of 33,781 men and women followed for a period of 22 years as part of the Chicago Heart Association Detection Project in Industry, a 12 bpm higher resting HR (one standard deviation above mean; mean HR range: -74.9–79.5 bpm across age groups 18–74 years) was a risk factor for all-cause, cardiovascular and coronary mortality in younger men and in middle-aged men and women.[69] In the BEAUTIFUL trial, a cohort of 10,917 patients with coronary artery disease, a left ventricular ejection fraction of <40% and a baseline resting HR of >70 bpm predicted a 34% increased risk of cardiovascular death, 53% increased risk of HF hospitalizations, and a 38% increased risk of hospitalization for MI. Above 65 bpm, every 5-bpm increase in baseline HR resulted in an 8% increase in cardiovascular death and a 16% increase in HF hospitalizations.[11,16] In the SHIFT cohort of 6505 patients with chronic HF with a left ventricular ejection fraction of ≤35% and a HR of >87 bpm (when compared with <70 bpm) was associated with a twofold higher risk of cardiovascular death and HF hospitalization with the risk increased by 3% with every beat increase from baseline HR, and 16% for every 5-bpm increase.[12,17]
A significant risk of adverse cardiovascular events thus exists within the accepted 'normal' HR range of 60–100 bpm, prompting suggestions for redefining what is normal HR and what is tachycardia.[14,15] Spodick suggested from his study that considering a HR of 50–90 bpm as normal limits of sinus HR would improve the threshold of
tachycardia sensitivity and bradycardia specificity.[68] Likewise, Palatini suggested a new threshold of 80–85 bpm to categorize normal from higher HR.[15] Irrespective of the new normal, slower HRs appear to be deterministic for healthy hearts.[14]
HR, although simple to measure, is heavily influenced by autonomic tone, body position, physical, psychological and environmental factors, and methods of measurement. Several methods of measurement have been adopted in clinical studies, including resting HR from peripheral pulse palpation or ECG, mean HR over 24 h, HRV, nocturnal/sleep HR and HR recovery following treadmill exercise testing.[13] Whether the prognostic significance of one measurement is better than the other remains to be proven. The following consensus recommendations aim to standardize the measurement of resting HR:
The patient should be allowed to sit for at least 5 min in a quiet room at a comfortable temperature;
HR should be measured over a 30-s period by pulse palpation;
At least two measurements should be taken in the sitting position;
Those subjects in whom orthostatic blood pressure measurement is performed, HR should be measured after each blood pressure reading;
The result may vary according to whether the HR is measured by a doctor, a nurse or an automatic device;
Patients performing self-blood pressure measurement should also collect HR data.[65]
With regard to the setting in which HR is measured, available data would indicate that HR recorded with ambulatory monitoring or self-measured at home provides little or no additional prognostic information to HR measured in the clinic.[65]
Although convincing evidence exists that elevated resting HR is associated with adverse cardiovascular outcomes, the underlying pathophysiology remains unclear. Proposed mechanisms include: increased myocardial work; higher mean blood pressure; increased arterial wall shear stress with resulting endothelial dysfunction and atherosclerosis; decreased arterial compliance and distensibility; disruption of vulnerable plaques; reduction in coronary perfusion; and increased arrhythmia vulnerability.[4] On the other hand, elevated HR could simply be a marker of autonomic imbalance, resulting in sympathetic overactivity and reduced vagal activity, facilitating adverse cardiovascular pathogenetic factors, such as insulin resistance, left ventricular hypertrophy, decreased capillary density, small vessel hypertrophy, platelet activation, increased hematocrit and decreased ventricular arrhythmia threshold.[4]
High Resting HR: A Modifiable Risk Factor or Just a Risk Predictor?HR reduction is a major determinant of clinical benefit in the management of several cardiovascular disorders. It is a risk factor temporally modifiable by genetics, environment, clinical conditions and drugs. The Paris Prospective Study of over 5000 healthy middle-aged men showed that an increase of >3 bpm in resting HR during a 5-year period was associated with a 19% increase in all-cause mortality, while a decrease of >4 bpm was associated with a 14% decreased mortality risk.[70] In a prospective study of over 29,000 healthy men and women, Nauman et al. found that the temporal increase in resting HR to >85 bpm from a baseline of <70 bpm over a 10-year period was associated with a 90% higher risk of ischemic heart disease mortality and 50% higher risk of all-cause mortality;[71] however, the major limitation of the study was the use of different techniques of HR measurement at baseline (manual pulse check) and during follow-up (automatic device recording). Cucherat, in a meta-regression analysis of randomized clinical trials of HR reduction in post-MI, showed that the beneficial effect of β-blockers and calcium-channel blockers in post-MI patients was related to resting HR reduction.[72] Every 10-bpm reduction in resting HR reduced the relative risk of cardiac death by 30%.[72] In patients with tachycardia-induced cardiomoyopathy, HR control, either by elimination of the culprit arrhythmia or simply by rate control, results in a complete reversal of left ventricular dysfunction.[14,73,74]
What would be an ideal resting HR to aim for? This remains an area of intense debate.[11,75,76] A randomized comparison of a strict (≤80 bpm at baseline) versus lenient (≤110 bpm) rate-control strategy in patients with atrial fibrillation showed no significant difference in outcomes.[76–78] A CRUSADE registry substudy that evaluated the relationship between presenting HR and in-hospital events in non-ST-segment elevation acute coronary syndromes found an increased risk of all-cause mortality and stroke in patients who, at presentation, had either
very low or very high resting HR.[79] Similarly, in patients with acute MI undergoing percutaneous intervention, a HR of >80 bpm was found to be associated with an increased risk of mortality.[80] At present, there is no consensus on a threshold resting sinus HR beyond which there is a significant increase in cardiac risk. However, based on the current evidence, a resting sinus HR of >70 bpm would be associated with a higher risk of long-term adverse cardiovascular outcomes.[11,12,16,17]
β-blockers and nondihydropyridine calcium antagonists remain the mainstay of pharmacotherapy for HR reduction in patients with coronary artery disease. By lowering resting and exercise HR, these agents reduce myocardial work and oxygen demand, and improve coronary blood flow, thereby limiting angina.[2] In addition to symptomatic benefits, pleiotropic effects and reduction in resting HR may play a role in the mortality and morbidity benefit associated with β-blockers in patients with HF and MI.[72,81–85] However, analysis of the placebo arm of the BEAUTIFUL trial showed that in patients with coronary artery disease and left ventricular dysfunction, despite a high percentage of β-blocker use (~90%), HR-mediated risk was found to be independent of β-blocker use.[11] Moreover, similar benefits have not been seen with β-blocker use in other patient populations, such as individuals with stable coronary artery disease or hypertension, or with risk factors for atherosclerosis.[86,87] A meta-analysis of randomized controlled trials evaluating β-blocker use in hypertension patients found that β-blocker-mediated HR reduction had an adverse impact on the risk of cardiac events and death.[86,88] A post-hoc analysis of the LIFE trial showed that in patients with hypertension and left ventricular hypertrophy, a higher in-treatment HR predicted increased risk of atrial fibrillation irrespective of whether the patient was randomized to atenolol or losartan.[89] The lack of efficacy of β-blockers is proposed to be due to reduced efficacy in lowering central aortic pressure, failure to improve endothelial function and left ventricular hypertrophy, weight gain, decreased exercise tolerance, and adverse metabolic effects including risk of developing diabetes and dyslipidemia.[88] Moreover, efficacy of β-blockers in reducing HR reduction is often limited by associated side effects and intolerance. In a meta-analysis of randomized controlled trials, the risk of treatment withdrawal was 80 and 41% greater with β-blockers compared with diuretics and renin–angiotensin–aldosterone system blockers, respectively.[90]
The development of ivabradine, a selective inhibitor of hyperpolarization-activated mixed sodium–potassium inward I f current in the sinus node pacemaker cells, offers promise in this regard.[18] Ivabradine provides pure sinus HR reduction, both at rest and during exercise, independent of autonomic effects, and without significant effects on myocardial contractility.[18]
Animal experiments have demonstrated that selective HR reduction with ivabradine favorably impacts cardiovascular pathophysiology above and beyond the reduction of myocardial oxygen consumption and potentiation of anti-ischemic effects. Several salutary effects, including protection against myocardial stunning,[91] reversal of cardiac remodeling with improvement in left ventricular systolic function,[92,93] reduction in diastolic dysfunction and reduction in myocardial fibrosis,[93,94] delayed time to onset of ventricular fibrillation,[95] and reduction in infarct size,[96] have been shown in experimental models.
Several clinical trials have demonstrated the cardiovascular beneficial effects of ivabradine. Borer et al., in a double-blind, placebo-controlled trial, showed that ivabradine, in a dose-dependent fashion, improved exercise tolerance and time to development of ischemia in patients with chronic stable angina.[97] The cardiovascular efficacy of ivabradine, as measured by extent of HR reduction, reduction of rate–pressure product (marker of myocardial oxygen consumption) and total exercise duration, has been demonstrated to be similar to β-blockers[98–100] and calcium-channel blockers.[101] Ivabradine has been shown to have synergistic effects when used with β-blockers[102] and calcium-channel blockers[103] in patients with stable coronary disease.
The BEAUTIFUL trial was a multicenter, double-blind, placebo-controlled, randomized study that evaluated the effects of ivabradine on cardiovascular mortality and morbidity in patients with ischemic cardiomyopathy.[16] A total of 10,917 patients with documented coronary artery disease and a left ventricular ejection fraction of <40% were randomized to placebo or ivabradine. Ivabradine decreased the mean HR by 6 bpm. Over a median follow-up of 19 months, there was no significant difference between the two groups on the primary end point, a composite of cardiovascular death, hospitalization for acute MI and HF hospitalization. However, in a prespecified cohort of more than 5000 patients with a baseline HR of ≥70 bpm, ivabradine improved coronary outcomes with a 36% reduction in fatal and nonfatal MI, and a 30% reduction in the need for coronary revascularizations,[16] suggesting that ivabradine can blunt higher HR-mediated adverse effects on diastolic coronary perfusion and myocardial oxygen demand.
A post-hoc analysis of the BEAUTIFUL trial, however, showed that in patients with limiting angina and a resting of HR >70 bpm, ivabradine did significantly improve the primary composite end point of cardiovascular mortality, MI and HF hospitalization.[104]
Whether ivabradine-induced reduction in resting HR improves mortality and morbidity in patients with stable coronary artery disease and preserved left ventricular systolic function is being evaluated in an ongoing trial, SIGNIFY (ISRCTN 61576291): a randomized, double-blind, placebo-controlled, international, multicenter study of more than 11,000 patients with stable coronary artery disease and a resting HR of ≥70 bpm.
The SHIFT trial was a randomized, double-blind, placebo-controlled trial that evaluated the impact of ivabradine (7.5 mg twice-daily) on cardiovascular outcomes in 6558 patients with symptomatic HF and a left ventricular ejection fraction of ≤35% on maximally tolerated medical therapy, including β-blockers.[17] All patients had a resting sinus HR of ≥70 bpm. Over a median follow-up of 22.9 months, it was noted that ivabradine had significantly reduced the risk of the primary composite end point (hospitalization for worsening HF or cardiovascular death) by 18%, an effect primarily driven by a 21% reduction in HF hospitalizations. The outcome improvements were observed irrespective of age, gender, etiology of HF or β-blocker use.
A post-hoc analysis of the SHIFT trial found that the magnitude of HR reduction by ivabradine beyond that achieved by a β-blocker, rather than background β-blocker dose, primarily determined effect on outcomes.[105] A subsequent subanalysis also noted that the effect of ivabradine on HF outcomes was greater in patients with a baseline HR of >75 bpm and that the best outcomes were seen when an in-treatment HR was <60 bpm or an in-treatment HR reduction of >10 bpm was achieved.[106]
Ivabradine is noted to have a good safety profile and is very well tolerated. It has no significant effects on ventricular repolarization and has not been shown to be proarrhythmic. Visual symptoms (phosphenes) were seen in 3% of patients in the SHIFT trial, but were transient in nature. Symptomatic bradycardia can also result, but the incidence is low.[107]
In summary, a combination of animal experimental data, as well as human data, from epidemiological studies and randomized clinical trials have proven that high resting sinus HR is an independent predictor of mortality and adverse cardiovascular outcomes, irrespective of the presence of structural heart disease. Although a 'safe' resting sinus HR for any particular individual may vary depending on demographic factors, as well as medical comorbidities, a resting HR of >70 bpm would be of concern. Healthy individuals with a resting HR of >70 bpm should be encouraged to adopt a healthier lifestyle. Special attention should be given to patients with coronary artery disease, hypertension, cardiomyopathy and HF with a resting HR of >70 bpm, since these patients are at risk for cardiovascular events. In these high-risk individuals, use of ivabradine, if available, should be considered in addition to standard therapy to reduce cardiovascular deaths and HF hospitalizations, and improve coronary outcomes. Except in the select populations mentioned above, we do not have convincing evidence that pharmacological reduction of resting sinus HR favorably affects hard clinical end points.
ConclusionST (resting HR >100 bpm) is commonly encountered in clinical practice. IST is a complex disorder with no clear etiology and often results in debilitating symptoms. Treatment involves a multidisciplinary approach combining lifestyle measures and pharmacotherapy, and can often be challenging. The selective I f current blocker, ivabradine, has emerged as a promising option in IST and may even be effective as monotherapy. Refractory cases can benefit from sinus node modification by catheter ablation.
Over the past several years, it has become clear that high resting HR within the normal range independently predicts all-cause and cardiovascular mortality, and other major adverse cardiac outcomes, both in the general population and in patients with structural heart disease. Although mechanisms remain less clear, it is apparent that slower HRs promote healthy hearts. Ivabradine-induced pure HR reduction has been shown to decrease cardiovascular mortality in patients with left ventricular dysfunction and HF. Whether high resting HR will be a modifiable risk factor or remains an epiphenomenon, in both the general population and those at risk of heart disease, needs further study.
HR, perhaps the most commonly measured vital sign, thus deserves closer attention than ever before. The definition of tachycardia, as we know it, needs an overhaul.[14,15,68]
Future Perspective
Ivabradine has been a big find in terms of pure HR reduction and the future holds promise in building upon the success of ivabradine and finding safe and effective pharmacological therapies for IST. HR threshold for risk of adverse cardiac outcomes will be well defined for different patient populations. Ability to favorably modify resting HR in individuals at risk of cardiovascular disease, as well as in patients with structural heart disease, will be clear. Future studies will also provide appropriate surveillance for at-risk individuals with higher resting sinus HR. Our opinion is that high resting HR will remain as much a marker for underlying substrate/illness as it will be a modifiable risk factor. We hope that definitions of tachycardia will change.
SidebarExecutive Summary
Inappropriate sinus tachycardia
Inappropriate sinus tachycardia (IST) is a syndrome of cardiac and extracardiac symptoms characterized by substantially fast sinus heart rate (HR) at rest (>100 bpm) or with minimal activity and disproportionate to physiologic demand.
Pathogenesis of IST is multifactorial and not well defined.
IST is a diagnosis of exclusion and extensive evaluation to identify secondary causes of sinus tachycardia should be performed.
Treatment of IST is indicated only in symptomatic individuals and can be challenging. A multidisciplinary approach is best for effective treatment of IST.
Medical therapy with β-blockers and nondihydropyridine calcium antagonists is often ineffective. Ivabradine, if available, can help in symptom control and improvement of quality of life. Catheter ablation remains an option, albeit with variable success, for the management of patients with IST and debilitating symptoms who have failed available pharmacotherapy and possible lifestyle and psychosocial modifications.
Long-term prognosis in IST appears to be benign.
Prognostic significance of elevated resting HR
High resting HR is a potent independent predictor of all-cause mortality and cardiovascular mortality at all ages in the general population, as well as in individuals with hypertension, myocardial infarction, diabetes mellitus and heart failure (HF).
In patients with HF and coronary disease, a resting HR of >70 bpm is associated with adverse cardiovascular prognosis and in these individuals, lifestyle and pharmacological measures should be initiated to lower the HR.
β-blockers and nondihydropyridine calcium antagonists are the mainstay of pharmacotherapy for HR reduction in coronary disease and heart failure. However, efficacy of these drugs is frequently limited by associated side effects and intolerance. Ivabradine, a selective I f inhibitor, provides pure HR reduction without affecting sympathetic activity or myocardial contractility.
HR reduction with ivabradine can reduce adverse cardiovascular events in patients with limiting angina and left ventricular dysfunction who are already on standard HF therapy.
The prognostic role of HR reduction in asymptomatic healthy individuals remains to be clinically proven.
High resting HR should be strongly considered in cardiovascular risk stratification. It may be time to redefine tachycardia.
References
1. Braunwald E. Control of myocardial oxygen consumption: physiologic and clinical considerations. Am. J. Cardiol.27(4),416–432 (1971).
2. Heusch G. Heart rate in the pathophysiology of coronary blood flow and myocardial ischaemia: benefit from selective bradycardic agents. Br. J. Pharmacol.153(8),1589–1601 (2008).
3. Levine HJ. Rest heart rate and life expectancy. J. Am. Coll. Cardiol.30(4),1104–1106 (1997).
4. Palatini P, Julius S. Elevated heart rate: a major risk factor for cardiovascular disease. Clin. Exp. Hypertens.26(7–8),637–644 (2004).
5. Heidland UE, Strauer BE. Left ventricular muscle mass and elevated heart rate are associated with coronary plaque disruption. Circulation104(13),1477–1482 (2001).
6. Jouven X, Empana JP, Schwartz PJ, Desnos M, Courbon D, Ducimetiere P. Heart-rate profile during exercise as a predictor of sudden death. N. Engl. J. Med.352(19),1951–1958 (2005).
7. Gillum RF, Makuc DM, Feldman JJ. Pulse rate, coronary heart disease, and death: the NHANES I epidemiologic follow-up study. Am. Heart J.121(1 Pt 1),172–177 (1991).
8. Heusch G. Heart rate and heart failure. Not a simple relationship. Circ. J.75(2),229–236 (2011).
9. Kannel WB, Kannel C, Paffenbarger RS Jr, Cupples LA. Heart rate and cardiovascular mortality: the Framingham Study. Am. Heart J.113(6),1489–1494 (1987).
10. Castagno D, Skali H, Takeuchi M et al. Association of heart rate and outcomes in a broad spectrum of patients with chronic heart failure: results from the CHARM (Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity) program. J. Am. Coll. Cardiol.59(20),1785–1795 (2012).
11. Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R. Heart rate as a prognostic risk factor in patients with coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a subgroup analysis of a randomised controlled trial. Lancet372(9641),817–821 (2008).
** Excellent article showing prognostic significance of resting heart rate in patients with coronary artery disease and left ventricular dysfunction.
12. Bohm M, Swedberg K, Komajda M et al. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet376(9744),886–894 (2010).
13. Gopinathannair R, Olshansky B. Resting sinus heart rate and first degree av block: modifiable risk predictors or epiphenomena? Indian Pacing Electrophysiol. J.9(6),334–341 (2009).
14. Gopinathannair R, Sullivan RM, Olshansky B. Slower heart rates for healthy hearts: time to redefine tachycardia? Circ. Arrhythm. Electrophysiol.1(5),321–323 (2008).
15. Palatini P. Need for a revision of the normal limits of resting heart rate. Hypertension33(2),622–625 (1999).
16. Fox K, Ford I, Steg PG, Tendera M, Ferrari R. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a randomised, double-blind, placebo-controlled trial. Lancet372(9641),807–816 (2008).
17. Swedberg K, Komajda M, Bohm M et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet376(9744),875–885 (2010).
** Randomized trial showing that ivabradine improves cardiovascular outcomes in patients with cardiomyopathy, symptomatic heart failure, and a resting heart rate of >70 bpm who are already on standard therapy.
18. Difrancesco D, Borer JS. The funny current: cellular basis for the control of heart rate. Drugs67(Suppl. 2),15–24 (2007).
19. Blomstrom-Lundqvist C, Scheinman MM, Aliot EM et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias – executive summary. A report of the
American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European society of Cardiology Committee for Practice Guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J. Am. Coll. Cardiol.42(8),1493–1531 (2003).
20. Codvelle MM, Boucher H. [Permanent sinus tachycardia without high frequency functional disorders]. Bull. Mem. Soc. Med. Hop. Paris54,1849–1852 (1939).
21. Wising P. Familial, congenital sinus tachycardia. Acta Medica Scandinavica108,299–305 (1941).
22. Bauernfeind RA, Amat YLF, Dhingra RC, Kehoe R, Wyndham C, Rosen KM. Chronic nonparoxysmal sinus tachycardia in otherwise healthy persons. Ann. Intern. Med.91(5),702–710 (1979).
23. Morillo CA, Klein GJ, Thakur RK, Li H, Zardini M, Yee R. Mechanism of 'inappropriate' sinus tachycardia. Role of sympathovagal balance. Circulation90(2),873–877 (1994).
24. Lopera G, Castellanos A, Moleiro F, Huikuri HV, Myerburg RJ. Chronic inappropriate sinus tachycardia in elderly females. Ann. Noninvasive Electrocardiol.8(2),139–143 (2003).
25. Shen WK. How to manage patients with inappropriate sinus tachycardia. Heart Rhythm2(9),1015–1019 (2005).
26. Olshansky B, Sullivan RM. Inappropriate sinus tachycardia. J. Am. College Cardiol. doi:10.1016/j.jacc.2012.07.074 (2012) (Epub ahead of print).
** Excellent review on inappropriate sinus tachycardia.
27. Femenia F, Baranchuk A, Morillo CA. Inappropriate sinus tachycardia: current therapeutic options. Cardiol. Rev.20(1),8–14 (2012).
28. Leon H, Guzman JC, Kuusela T, Dillenburg R, Kamath M, Morillo CA. Impaired baroreflex gain in patients with inappropriate sinus tachycardia. J. Cardiovasc. Electrophysiol.16(1),64–68 (2005).
29. Ho RT, Ortman M, Mather PJ, Rubin S. Inappropriate sinus tachycardia in a transplanted heart – further insights into pathogenesis. Heart Rhythm8(5),781–783 (2011).
30. Still AM, Huikuri HV, Airaksinen KE et al. Impaired negative chronotropic response to adenosine in patients with inappropriate sinus tachycardia. J. Cardiovasc. Electrophysiol.13(6),557–562 (2002).
31. Castellanos A, Moleiro F, Chakko S et al. Heart rate variability in inappropriate sinus tachycardia. Am. J. Cardiol.82(4),531–534 (1998).
32. Skeberis V, Simonis F, Tsakonas K, Celiker A, Andries E, Brugada P. Inappropriate sinus tachycardia following radiofrequency ablation of AV nodal tachycardia: incidence and clinical significance. Pacing Clin. Electrophysiol.17(5 Pt 1),924–927 (1994).
33. Madrid AH, Mestre JL, Moro C et al. Heart rate variability and inappropriate sinus tachycardia after catheter ablation of supraventricular tachycardia. Eur. Heart J.16(11),1637–1640 (1995).
34. Psychari SN, Theodorakis GN, Koutelou M, Livanis EG, Kremastinos DT. Cardiac denervation after radiofrequency ablation of supraventricular tachycardias. Am. J. Cardiol.81(6),725–731 (1998).
35. Emkanjoo Z, Alasti M, Arya A et al. Heart rate variability: does it change after RF ablation of reentrant supraventricular tachycardia? J. Intervent. Cardiac Electrophysiol.14(3),147–151 (2005).
36. Guo H, Wang P, Xing Y et al. Delayed injury of autonomic nerve induced by radiofrequency catheter ablation. J. Electrocardiol.40(4),355.e1–355.e4 (2007).
37. Chiale PA, Ferrari I, Mahler E et al. Differential profile and biochemical effects of antiautonomic membrane receptor antibodies in ventricular arrhythmias and sinus node dysfunction. Circulation103(13),1765–1771 (2001).
38. Chiale PA, Garro HA, Schmidberg J et al. Inappropriate sinus tachycardia may be related to an immunologic disorder involving cardiac beta andrenergic receptors. Heart Rhythm3(10),1182–1186 (2006).
39. Lowe JE, Hartwich T, Takla M, Schaper J. Ultrastructure of electrophysiologically identified human sinoatrial nodes. Basic Res. Cardiol.83(4),401–409 (1988).
40. Shen WK, Low PA, Jahangir A et al. Is sinus node modification appropriate for inappropriate sinus tachycardia with features of postural orthostatic tachycardia syndrome? Pacing Clin. Electrophysiol.24(2),217–230 (2001).
41. Frankel DS, Lin D, Anastasio N et al. Frequent additional tachyarrhythmias in patients with inappropriate sinus tachycardia undergoing sinus node modification: an important cause of symptom recurrence. J. Cardiovasc. Electrophysiol.23(8),835–839 (2012).
42. Winum PF, Cayla G, Rubini M, Beck L, Messner-Pellenc P. A case of cardiomyopathy induced by inappropriate sinus tachycardia and cured by ivabradine. Pacing Clin. Electrophysiol.32(7),942–944 (2009).
43. Romeo E, Grimaldi N, Sarubbi B et al. A pediatric case of cardiomyopathy induced by inappropriate sinus tachycardia: efficacy of ivabradine. Ped. Cardiol.32(6),842–845 (2011).
44. Lee RJ, Kalman JM, Fitzpatrick AP et al. Radiofrequency catheter modification of the sinus node for 'inappropriate' sinus tachycardia. Circulation92(10),2919–2928 (1995).
45. Ptaszynski P, Kaczmarek K, Ruta J, Klingenheben T, Wranicz JK. Metoprolol succinate vs. ivabradine in the treatment of inappropriate sinus tachycardia in patients unresponsive to previous pharmacological therapy. Europace15(1),116–121 (2013).
46. Killu AM, Syed FF, Wu P, Asirvatham SJ. Refractory inappropriate sinus tachycardia successfully treated with radiofrequency ablation at the arcuate ridge. Heart Rhythm9(8),1324–1327 (2012).
47. Calo L, Rebecchi M, Sette A et al. Efficacy of ivabradine administration in patients affected by inappropriate sinus tachycardia. Heart Rhythm7(9),1318–1323 (2010).
48. Kaplinsky E, Comes FP, Urondo LS, Ayma FP. Efficacy of ivabradine in four patients with inappropriate sinus tachycardia: a three month-long experience based on electrocardiographic, Holter monitoring, exercise tolerance and quality of life assessments. Cardiol. J.17(2),166–171 (2010).
49. Rakovec P. Treatment of inappropriate sinus tachycardia with ivabradine. Wien. Klin. Wochenschr.121(21–22),715–718 (2009).
50. Zellerhoff S, Hinterseer M, Felix Krull B et al. Ivabradine in patients with inappropriate sinus tachycardia. Naunyn Schmiedebergs Arch. Pharmacol.382(5–6),483–486 (2010).
51. Cappato R, Castelvecchio S, Ricci C et al. Clinical efficacy of ivabradine in patients with inappropriate sinus tachycardia: a prospective, randomized, placebo-controlled, double-blind, crossover evaluation. J. Am. Coll. Cardiol.60(15),1323–1329 (2012).
52. Boineau JP, Canavan TE, Schuessler RB, Cain ME, Corr PB, Cox JL. Demonstration of a widely distributed atrial pacemaker complex in the human heart. Circulation77(6),1221–1237 (1988).
53. Man KC, Knight B, Tse HF et al. Radiofrequency catheter ablation of inappropriate sinus tachycardia guided by activation mapping. J. Am. Coll. Cardiol.35(2),451–457 (2000).
54. Dravid SG, Hope B, Mckinnie JJ. Intracardiac echocardiography in electrophysiology: a review of current applications in practice. Echocardiography25(10),1172–1175 (2008).
55. Kalman JM, Lee RJ, Fisher WG et al. Radiofrequency catheter modification of sinus pacemaker function guided by intracardiac echocardiography. Circulation92(10),3070–3081 (1995).
56. Lesh MD, Kalman JM, Karch MR. Use of intracardiac echocardiography during electrophysiologic evaluation and therapy of atrial arrhythmias. J. Cardiovasc. Electrophysiol.9(Suppl. 8),S40–S47 (1998).
57. Marrouche NF, Beheiry S, Tomassoni G et al. Three-dimensional nonfluoroscopic mapping and ablation of inappropriate sinus tachycardia. Procedural strategies and long-term outcome. J. Am. Coll. Cardiol.39(6),1046–1054 (2002).
58. Diaz A, Bourassa MG, Guertin MC, Tardif JC. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur. Heart J.26(10),967–974 (2005).
59. Anselmino M, Ohrvik J, Ryden L. Resting heart rate in patients with stable coronary artery disease and diabetes: a report from the Euro Heart Survey on diabetes and the heart. Eur. Heart J.31(24),3040–3045 (2010).
60. Ho JE, Bittner V, Demicco DA, Breazna A, Deedwania PC, Waters DD. Usefulness of heart rate at rest as a predictor of mortality, hospitalization for heart failure, myocardial infarction, and stroke in patients with stable coronary heart disease (data from the Treating to New Targets [TNT] trial). Am. J. Cardiol.105(7),905–911 (2010).
61. Thackray SD, Ghosh JM, Wright GA et al. The effect of altering heart rate on ventricular function in patients with heart failure treated with beta-blockers. Am. Heart J.152(4),713.e9–13 (2006).
62. Gullestad L, Wikstrand J, Deedwania P et al. What resting heart rate should one aim for when treating patients with heart failure with a beta-blocker? Experiences from the Metoprolol Controlled Release/Extended Release Randomized Intervention Trial in Chronic Heart Failure (MERIT-HF). J. Am. Coll. Cardiol.45(2),252–259 (2005).
63. Maeder MT, Kaye DM. Differential impact of heart rate and blood pressure on outcome in patients with heart failure with reduced versus preserved left ventricular ejection fraction. Int. J. Cardiol.155(2),249–256 (2012).
64. Custodis F, Schirmer SH, Baumhakel M, Heusch G, Bohm M, Laufs U. Vascular pathophysiology in response to increased heart rate. J. Am. Coll. Cardiol.56(24),1973–1983 (2010).
65. Palatini P, Benetos A, Grassi G et al. Identification and management of the hypertensive patient with elevated heart rate: statement of a European Society of Hypertension Consensus Meeting. J. Hypertens.24(4),603–610 (2006).
** Good consensus article on clinical significance of elevated heart rate.
66. Kapoor JR, Heidenreich PA. Heart rate predicts mortality in patients with heart failure and preserved systolic function. J. Cardiac Fail.16(10),806–811 (2010).
67. Palatini P, Thijs L, Staessen JA et al. Predictive value of clinic and ambulatory heart rate for mortality in elderly subjects with systolic hypertension. Arch. Intern. Med.162(20),2313–2321 (2002).
68. Spodick DH. Normal sinus heart rate: sinus tachycardia and sinus bradycardia redefined. Am. Heart J.124(4),1119–1121 (1992).
69. Greenland P, Daviglus ML, Dyer AR et al. Resting heart rate is a risk factor for cardiovascular and noncardiovascular mortality: the Chicago Heart Association Detection Project in Industry. Am. J. Epidemiol.149(9),853–862 (1999).
70. Jouven X, Empana JP, Escolano S et al. Relation of heart rate at rest and long-term (>20 years) death rate in initially healthy middle-aged men. Am. J. Cardiol.103(2),279–283 (2009).
71. Nauman J, Janszky I, Vatten LJ, Wisloff U. Temporal changes in resting heart rate and deaths from ischemic heart disease. JAMA306(23),2579–2587 (2011).
72. Cucherat M. Quantitative relationship between resting heart rate reduction and magnitude of clinical benefits in post-myocardial infarction: a meta-regression of randomized clinical trials. Eur. Heart J.28(24),3012–3019 (2007).
73. Gopinathannair R, Sullivan R, Olshansky B. Tachycardia-mediated cardiomyopathy: recognition and management. Curr. Heart Fail. Rep.6(4),257–264 (2009).
** Concise review on tachycardia-mediated cardiomyopathy.
74. Khasnis A, Jongnarangsin K, Abela G, Veerareddy S, Reddy V, Thakur R. Tachycardia-induced cardiomyopathy: a review of literature. Pacing Clin. Electrophysiol.28(7),710–721 (2005).
75. Gopinathannair R, Sullivan RM, Olshansky B. Update on medical management of atrial fibrillation in the modern era. Heart Rhythm6(Suppl. 8),S17–S22 (2009).
76. Van Gelder IC, Groenveld HF, Crijns HJ et al. Lenient versus strict rate control in patients with atrial fibrillation. N. Engl. J. Med.362(15),1363–1373 (2010).
77. Groenveld HF, Crijns HJ, Van Den Berg MP et al. The effect of rate control on quality of life in patients with permanent atrial fibrillation: data from the RACE II (Rate Control Efficacy in Permanent Atrial Fibrillation II) study. J. Am. Coll. Cardiol.58(17),1795–1803 (2011).
78. Smit MD, Crijns HJ, Tijssen JG et al. Effect of lenient versus strict rate control on cardiac remodeling in patients with atrial fibrillation data of the RACE II (Rate Control Efficacy in Permanent Atrial Fibrillation II) study. J. Am. Coll. Cardiol.58(9),942–949 (2011).
79. Bangalore S, Messerli FH, Ou FS et al. The association of admission heart rate and in-hospital cardiovascular events in patients with non-ST-segment elevation acute coronary syndromes: results from 135,164 patients in the CRUSADE quality improvement initiative. Eur. Heart J.31(5),552–560 (2010).
80. Parodi G, Bellandi B, Valenti R et al. Heart rate as an independent prognostic risk factor in patients with acute myocardial infarction undergoing primary percutaneous coronary intervention. Atherosclerosis211(1),255–259 (2010).
81. Dulin BR, Haas SJ, Abraham WT, Krum H. Do elderly systolic heart failure patients benefit from beta blockers to the same extent as the non-elderly? Meta-analysis of >12,000 patients in large-scale clinical trials. Am. J. Cardiol.95(7),896–898 (2005).
82. Brophy JM, Joseph L, Rouleau JL. Beta-blockers in congestive heart failure. A Bayesian meta-analysis. Ann. Intern. Med.134(7),550–560 (2001).
83. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. BMJ318(7200),1730–1737 (1999).
84. Lechat P, Hulot JS, Escolano S et al. Heart rate and cardiac rhythm relationships with bisoprolol benefit in chronic heart failure in CIBIS II trial. Circulation103(10),1428–1433 (2001).
85. Kjekshus JK. Importance of heart rate in determining beta-blocker efficacy in acute and long-term acute myocardial infarction intervention trials. Am. J. Cardiol.57(12),F43–F49 (1986).
86. Bangalore S, Sawhney S, Messerli FH. Relation of beta-blocker-induced heart rate lowering and cardioprotection in hypertension. J. Am. Coll. Cardiol.52(18),1482–1489 (2008).
87. Bangalore S, Steg G, Deedwania P et al. Beta-blocker use and clinical outcomes in stable outpatients with and without coronary artery disease. JAMA308(13),1340–1349 (2012).
88. Bangalore S, Messerli FH, Kostis JB, Pepine CJ. Cardiovascular protection using beta-blockers: a critical review of the evidence. J. Am. Coll. Cardiol.50(7),563–572 (2007).
** Reviews the use of β-blockers in the management of cardiovascular disorders.
89. Okin PM, Wachtell K, Kjeldsen SE et al. Incidence of atrial fibrillation in relation to changing heart rate over time in hypertensive patients: the LIFE study. Circ. Arrhythm. Electrophysiol.1(5),337–343 (2008).
90. Bradley HA, Wiysonge CS, Volmink JA, Mayosi BM, Opie LH. How strong is the evidence for use of beta-blockers as first-line therapy for hypertension? Systematic review and meta-analysis. J. Hypertens.24(11),2131–2141 (2006).
91. Monnet X, Ghaleh B, Colin P, de Curzon OP, Giudicelli JF, Berdeaux A. Effects of heart rate reduction with ivabradine on exercise-induced myocardial ischemia and stunning. J. Pharmacol. Exp. Ther.299(3),1133–1139 (2001).
92. Mulder P, Barbier S, Chagraoui A et al. Long-term heart rate reduction induced by the selective I(f) current inhibitor ivabradine improves left ventricular function and intrinsic myocardial structure in congestive heart failure. Circulation109(13),1674–1679 (2004).
93. Becher PM, Lindner D, Miteva K et al. Role of heart rate reduction in the prevention of experimental heart failure: comparison between I f -channel blockade and beta-receptor blockade. Hypertension59(5),949–957 (2012).
94. Busseuil D, Shi Y, Mecteau M et al. Heart rate reduction by ivabradine reduces diastolic dysfunction and cardiac fibrosis. Cardiology117(3),234–242 (2010).
95. Vaillant F, Dehina L, Dizerens N et al. Ivabradine but not propranolol delays the time to onset of ischaemia-induced ventricular fibrillation by preserving myocardial metabolic energy status. Resuscitation doi: 10.1016/j.resuscitation.2012.07.041 (2012) (Epub ahead of print).
96. Heusch G, Skyschally A, Gres P, van Caster P, Schilawa D, Schulz R. Improvement of regional myocardial blood flow and function and reduction of infarct size with ivabradine: protection beyond heart rate reduction. Eur. Heart J.29(18),2265–2275 (2008).
97. Borer JS, Fox K, Jaillon P, Lerebours G. Antianginal and antiischemic effects of ivabradine, an I(f) inhibitor, in stable angina: a randomized, double-blind, multicentered, placebo-controlled trial. Circulation107(6),817–823 (2003).
98. Cucherat M, Borer JS. Reduction of resting heart rate with antianginal drugs: review and meta-analysis. Am. J. Ther.19(4),269–280 (2012).
99. Tardif JC, Ford I, Tendera M, Bourassa MG, Fox K. Efficacy of ivabradine, a new selective I(f) inhibitor, compared with atenolol in patients with chronic stable angina. Eur. Heart J.26(23),2529–2536 (2005).
100. Joannides R, Moore N, Iacob M et al. Comparative effects of ivabradine, a selective heart rate-lowering agent, and propranolol on systemic and cardiac haemodynamics at rest and during exercise. Br. J. Clin. Pharmacol.61(2),127–137 (2006).
101. Ruzyllo W, Tendera M, Ford I, Fox KM. Antianginal efficacy and safety of ivabradine compared with amlodipine in patients with stable effort angina pectoris: a 3-month randomised, double-blind, multicentre, noninferiority trial. Drugs67(3),393–405 (2007).
102. Tardif JC, Ponikowski P, Kahan T. Efficacy of the I(f) current inhibitor ivabradine in patients with chronic stable angina receiving beta-blocker therapy: a 4-month, randomized, placebo-controlled trial. Eur. Heart J.30(5),540–548 (2009).
103. Lopez-Bescos L, Filipova S, Martos R. Long-term safety and efficacy of ivabradine in patients with chronic stable angina. Cardiology108(4),387–396 (2007).
104. Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R. Relationship between ivabradine treatment and cardiovascular outcomes in patients with stable coronary artery disease and left ventricular systolic dysfunction with limiting angina: a subgroup analysis of the randomized, controlled BEAUTIFUL trial. Eur. Heart J.30(19),2337–2345 (2009).
105. Swedberg K, Komajda M, Bohm M et al. Effects on outcomes of heart rate reduction by ivabradine in patients with congestive heart failure: is there an influence of beta-blocker dose?:
findings from the SHIFT (Systolic Heart Failure Treatment with the I(f) Inhibitor Ivabradine Trial) study. J. Am. Coll. Cardiol.59(22),1938–1945 (2012).
106. Bohm M, Borer J, Ford I et al. Heart rate at baseline influences the effect of ivabradine on cardiovascular outcomes in chronic heart failure: analysis from the SHIFT study. Clin. Res. Cardiol.102(1),11–22 (2013).
107. Savelieva I, Camm AJ. I f inhibition with ivabradine: electrophysiological effects and safety. Drug Saf.31(2),95–107 (2008).
Website
201. Ivabradine versus beta-blockers in the treatment of inappropriate sinus tachycardia.
http://clinicaltrials.gov/ct2/show/NCT01657136
Papers of special note have been highlighted as:
** of considerable interest
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Future Cardiol. 2013;9(2):273-288. © 2013 Future Medicine Ltd.