incidence, predictors, and outcome of plaque prolapse after stent implantation in patients with...
TRANSCRIPT
Incidence, Predictors, and Outcome of Plaque Prolapse after Stent Implantation in Patients
with Acute Myocardial Infarction: An Intravascular Ultrasound Analysis
Young Joon Hong, MD, PhD; Myung Ho Jeong, MD, PhD, FACC, FAHA, FESC, FSCAI;
Youngkeun Ahn, MD, PhD, FACC, FSCAI; Doo Sun Sim, MD; Jong Won Chung, MD; Jung
Sun Cho, MD; Nam Sik Yoon, MD; Hyun Ju Yoon, MD; Jae Youn Moon, MD; Kye Hun Kim,
MD, PhD; Hyung Wook Park, MD, PhD; Ju Han Kim, MD, PhD; Jeong Gwan Cho, MD, PhD,
FACC; Jong Chun Park, MD, PhD; Jung Chaee Kang, MD, PhD
The Heart Center of Chonnam National University Hospital, Chonnam National University Research Institute of Medical Sciences, Gwangju, Korea

● Coronary angiography
-- provides only simple, planar projections of three-
dimensional coronary lumen anatomy.
-- is limited to detect intrastent plaque prolapse (PP).
● Previous studies have shown that
-- PP is not a rare phenomenon.
-- PP has been detected frequently by intravascular
ultrasound (IVUS).
Background (I)
● It has been known that several pre-intervention IVUS
factors and aggressive stenting procedure have been
associated with PP.
● Some studies have demonstrated that PP was associated
with stent thrombosis.
● However, data on the characteristics of PP in patients
with acute myocardial infarction (AMI) are lacking.
Background (II)

Objectives
● to assess the incidence, predictors, and outcome of PP
after stent implantation for infarct-related arteries in
AMI patients.

● a total of 310 patients with a first AMI
- 125 ST segment elevation and 185 non-ST segment
elevation MI
- From January 9, 2001 to July 31, 2007
- who underwent pre-intervention IVUS within 24 hours from
symptom onset
- were stented successfully
- had post-intervention IVUS imaging
Patient Population (I)
Patient Population (II)
● Exclusion
- prior MI, subacute or late stent thrombosis, restenosis
after stenting, coronary artery bypass graft failure, patients
studied with IVUS more than 24 hours after symptom
onset,
and patients in whom adequate IVUS images could not be
obtained
● Identification of infarct-related arteries
- electrocardiographic findings
- left ventricular wall motion abnormalities on left ventricular
angiogram or echocardiogram
- coronary angiographic findings

Laboratory Analysis● Venous blood samples were obtained within 24 hours after
stenting.
● The blood samples were centrifuged, and serum was
removed and stored at -70°C until the assay could be
performed.
● Absolute creatine kinase-MB (CK-MB) levels were
determined by radioimmunoassay (Dade Behring Inc., Miami,
Florida).
● Cardiac-specific troponin I (cTnI) levels were measured by a
paramagnetic particle, chemiluminescent immunoenzymatic
assay (Beckman, Coulter Inc., Fullerton, California).

IVUS Imaging
● All IVUS examinations were performed before PCI after
intracoronary administration of 200 µg nitroglycerin
● Commercially available IVUS system (Boston Scientific
Corporation/SCIMed, Minneapolis, MN)
● IVUS catheter was advanced distal to the target lesion, and
imaging was performed retrograde to the aorto-ostial
junction at an automatic pullback speed of 0.5 mm/sec

IVUS Analysis (I) ● according to the American College of Cardiology Clinical
Expert Consensus Document on Standards for Acqusition,
Measurement and Reporting of Intravascular Ultrasound
Studies
● using planimetry software (TapeMeasure, INDEC Systems
Inc., Mountain View, CA)
-- external elastic membrane (EEM) cross-sectional area
(CSA)
-- lumen CSA
-- plaque plus media (P&M) CSA: EEM CSA minus lumen CSA
-- plaque burden: P&M CSA divided by EEM CSA

Proximal Proximal ReferenceReference
LesionLesionSiteSite
Distal Distal ReferenceReference
EEMEEM
LumenLumen
P+MP+M
Max P+M Max P+M ThicknessThickness
Min P+M Min P+M ThicknessThickness
CaCa++++

IVUS Analysis (II) ● The lesion was the site with the smallest lumen CSA
-- if there were multiple image slices with the same minimum
lumen CSA
the image slice with the largest EEM and P&M was
measured
● Plaque morphology
-- Hypoechoic plaque: less bright compared with the
reference adventitia
-- Hyperechoic, noncalcified: as bright as or brighter than
the reference adventitia without acoustic shadowing
-- Calcified plaque: hyperechoic with shadowing
: lesion contained >90° of circumferential
calcium

IVUS Analysis (III) ● Coronary artery remodeling
-- was assessed by comparing the lesion site to the
reference EEM CSA
● Remodeling index (RI): the lesion site EEM CSA divided by
the average of the proximal and distal reference EEM CSA
-- Positive remodeling: RI >1.05
-- Intermediate remodeling: RI between 0.95 and 1.05
-- Negative remodeling: RI <0.95
● Thrombus
-- an intraluminal mass
-- having a layered or lobulated appearance
-- evidence of blood flow (microchannels) within the mass
-- speckling or scintillation
IVUS Analysis (IV) ● A ruptured plaque
-- contained a cavity that communicated with the lumen with
an overlying residual fibrous cap fragment.
-- a fragmented and loosely adherent plaque without a
distinct cavity and without a fibrous cap fragment was not
considered a plaque rupture.
-- rupture sites separated by a length of artery containing
smooth lumen contours without cavities were considered
to represent different plaque ruptures.
-- plaque cavity was measured and extrapolated to the
ruptured capsule area.

Example of Plaque Rupture with Thrombus
Thrombus
Ruptured plaque cavity
Thin fibrous cap

IVUS Analysis (V)
● At post-intervention
-- minimum stent CSA
-- Percent stent expansion: minimum stent CSA divided by
mean reference lumen CSA
-- PP was defined as tissue extrusion through the stent strut
at post-intervention
-- Volume of PP: subtracting lumen volume from stent
volume

Baseline Characteristics (I)
Plaque Prolapse (n=85)
No Plaque Prolapse (n=225)
p value
Age (yrs) 65±13 65±11 1.0
Male gender, # (%) 49 (58) 130 (58) 1.0
Clinical presentation, # (%) 0.081
Non-ST segment elevation MI 44 (52) 141 (63)
ST segment elevation MI 41 (48) 84 (37)
Diabetes mellitus, # (%) 31 (37) 80 (36) 0.9
Hypertension, # (%) 64 (75) 154 (68) 0.2
Smoking, # (%) 30 (35) 75 (33) 0.7
Family history of coronary artery disease, # (%)
18 (21) 34 (15) 0.2
Previous percutaneous coronary intervention, # (%)
3 (10) 9 (8) 0.8
Thrombolytic therapy, # (%) 11 (13) 21 (9) 0.4
Glycoprotein IIb/IIIa inhibitors, # (%) 20 (24) 44 (20) 0.4
Use of distal protection devices, # (%) 12 (14) 12 (5) 0.010
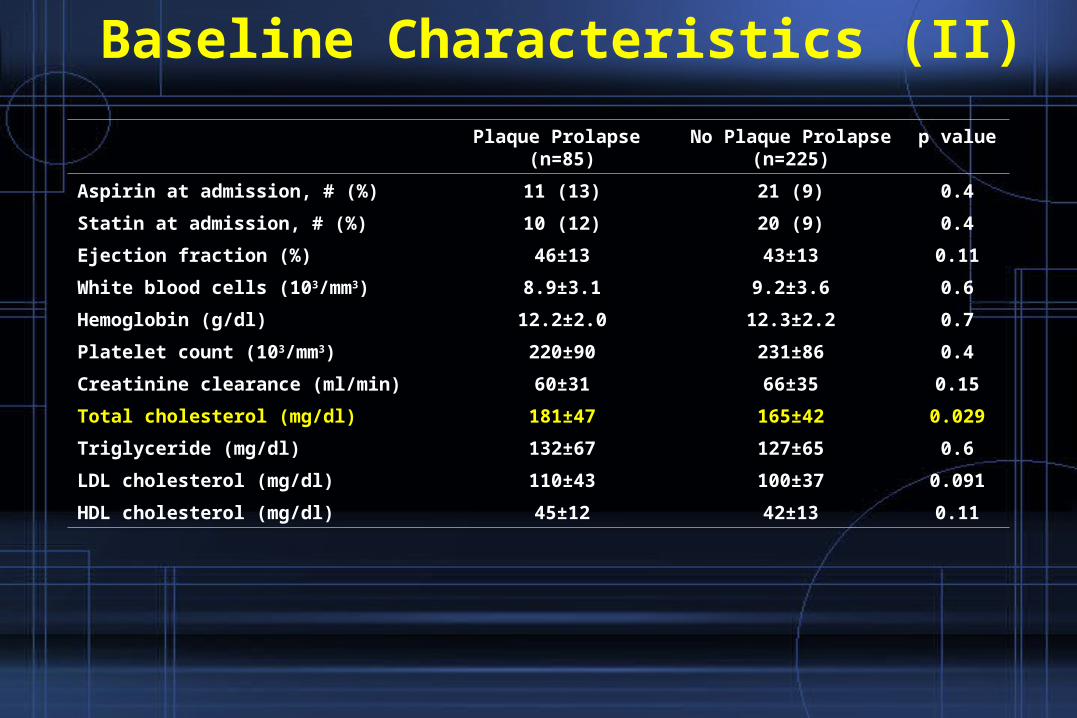
Baseline Characteristics (II)
Plaque Prolapse (n=85)
No Plaque Prolapse (n=225)
p value
Aspirin at admission, # (%) 11 (13) 21 (9) 0.4
Statin at admission, # (%) 10 (12) 20 (9) 0.4
Ejection fraction (%) 46±13 43±13 0.11
White blood cells (103/mm3) 8.9±3.1 9.2±3.6 0.6
Hemoglobin (g/dl) 12.2±2.0 12.3±2.2 0.7
Platelet count (103/mm3) 220±90 231±86 0.4
Creatinine clearance (ml/min) 60±31 66±35 0.15
Total cholesterol (mg/dl) 181±47 165±42 0.029
Triglyceride (mg/dl) 132±67 127±65 0.6
LDL cholesterol (mg/dl) 110±43 100±37 0.091
HDL cholesterol (mg/dl) 45±12 42±13 0.11

Coronary Angiographic Findings
Plaque Prolapse (n=85)
No Plaque Prolapse (n=225)
p value
Infarct-related artery, # (%) 0.024
Left main 0 (0) 5 (2)
LAD 36 (42) 131 (58)
LCX 14 (17) 28 (12)
RCA 35 (41) 61 (27)
Lesion location, # (%) 0.8
Ostium 1 (1) 3 (1)
Proximal 31 (37) 90 (40)
Middle 46 (54) 109 (48)
Distal 7 (8) 23 (10)
Multivessel disease, # (%) 41 (48) 112 (50) 0.8
Thrombus, # (%) 14 (16) 22 (10) 0.10
Calcium, # (%) 7 (8) 23 (10) 0.6
TIMI flow grade 0, # (%) 19 (22) 30 (13) 0.052

Procedural Results
Plaque Prolapse (n=85)
No Plaque Prolapse (n=225)
p value
Stent type, # (%) 0.15
Sirolimus-eluting stent 35 (41) 103 (46)
Paclitaxel-eluting stent 19 (22) 30 (13)
Bare-metal stent 31 (37) 92 (41)
No. of deployed stents, # (%) 1.5±0.6 1.1±0.3 <0.001
Stent diameter (mm) 3.28±0.40 3.24±0.46 0.7
Stent length (mm) 31±13 21±8 <0.001
Inflation pressure (mmHg) 15.3±2.9 14.1±2.6 0.001
Reference diameter (mm) 3.32±0.85 3.27±0.72 0.5
Pre-MLD (mm) 0.63±0.32 0.68±0.51 0.18
Lesion length (mm) 23±12 15±8 0.001

Intravascular Ultrasound Findings Plaque Prolapse
(n=85)No Plaque Prolapse
(n=225)p value
Reference
EEM CSA (mm2) 12.8±4.6 12.9±4.7 1.0
Lumen CSA (mm2) 8.3±3.0 8.3±3.1 0.9
P&M CSA (mm2) 4.6±2.6 4.5±2.6 1.0
Plaque burden (%) 35±11 34±11 0.7
Minimum lumen site
EEM CSA (mm2) 13.1±4.1 12.3±4.8 0.2
Lumen CSA (mm2) 2.5±1.5 2.8±1.3 0.063
P&M CSA (mm2) 10.6±4.2 9.4±4.3 0.040
Plaque burden (%) 79.5±13.0 75.2±10.6 0.003
IVUS lesion length (mm) 28±12 18±8 <0.001
Calcium arc (º) 114±76 195±81 <0.001
Calcium length (mm) 3.6±2.7 5.5±3.7 0.008
Superficial calcium, # (%) 51 (60) 158 (70) 0.087
Minimum stent CSA (mm2) 8.14±2.99 7.25±2.27 0.029
Stent expansion (%) 98±25 87±29 0.014
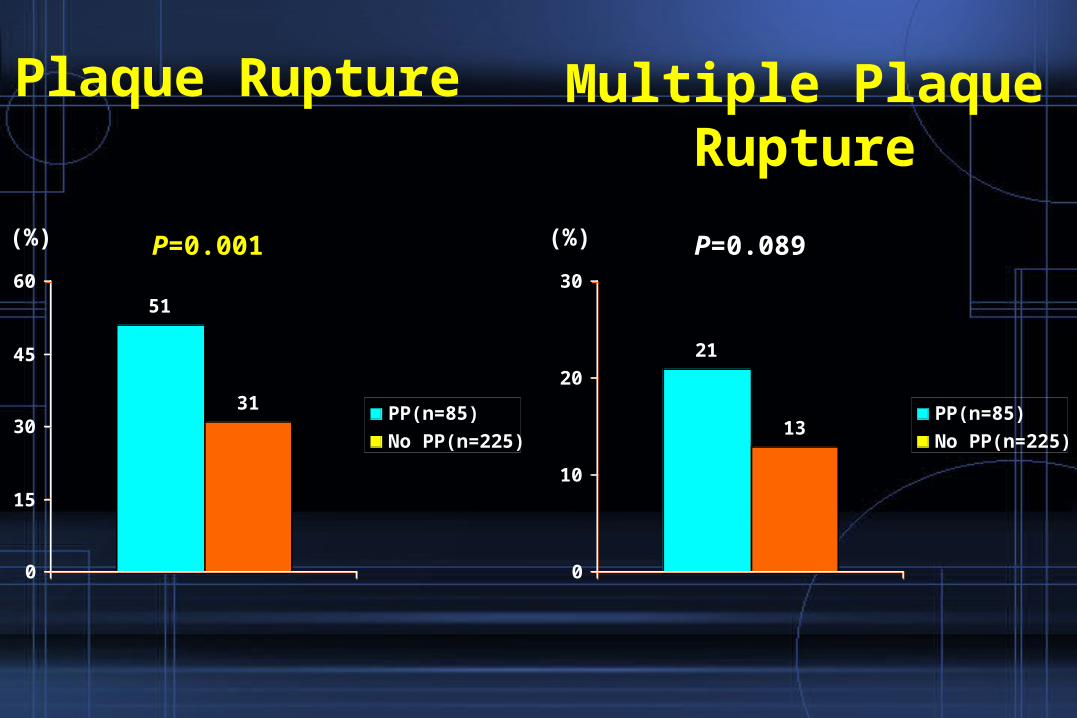
51
31
0
15
30
45
60
PP(n=85)
No PP(n=225)
P=0.001
Plaque Rupture
(%)
21
13
0
10
20
30
PP(n=85)
No PP(n=225)
(%) P=0.089
Multiple Plaque Rupture

3.1
2.5
0
1
2
3
4
5
PP(n=85) No PP(n=225)
P=0.008
Plaque Cavity Area(mm2)

40
21
0
10
20
30
40
50
PP(n=85)No PP(n=225)
P=0.001
Thrombus (%)

9
17
13
60
9
28
18
44
0
15
30
45
60
Hypoechoic Hyperechoic,noncalcified
Calcified Mixed
PP(n=85)
No PP(n=225)
(%)
P=0.044
Plaque Morphology

Remodeling Index
1.040.98
0
0.5
1
1.5
PP(n=85) No PP(n=225)
P=0.017
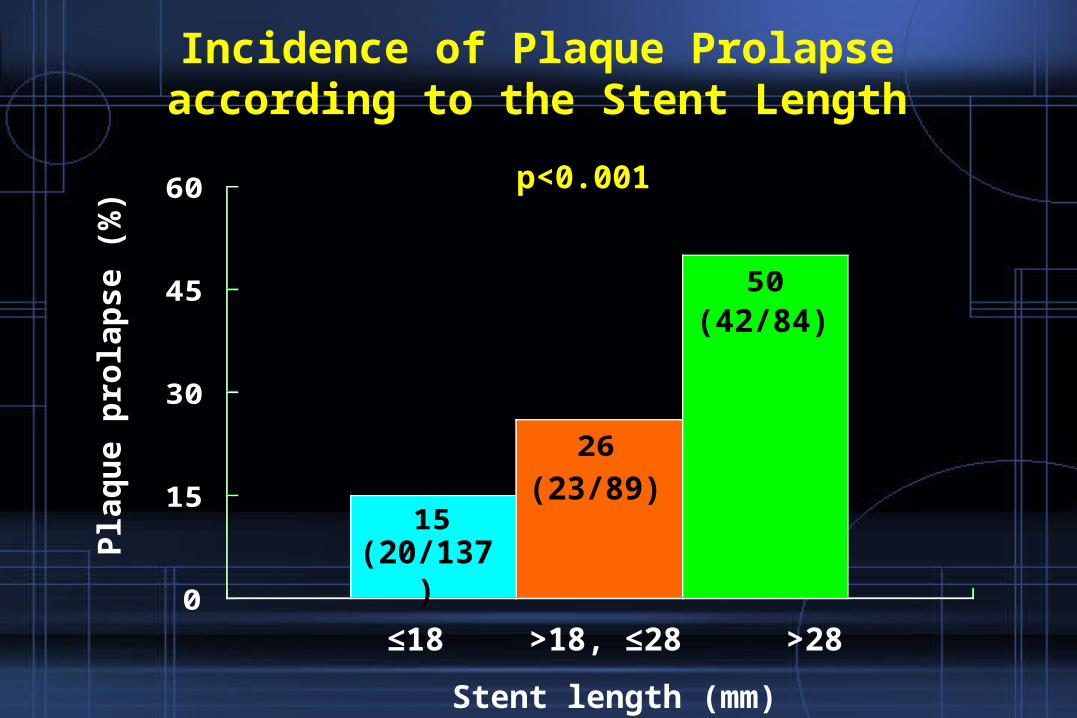
15
26
50
0
15
30
45
60
Stent length (mm)
≤18 >18, ≤28 >28
(20/137)
(23/89)
(42/84)
Pla
qu
e p
rola
pse
(%
)
p<0.001
Incidence of Plaque Prolapse according to the Stent Length

38
21
0
10
20
30
40
Plaque rupture (+)
(43/112)
(42/198)
Pla
qu
e p
rola
pse
(%
)
p=0.001
Plaque rupture (-)
Incidence of Plaque Prolapse according to the Presence/Absence of Plaque Rupture

36
28
19
0
10
20
30
40
Positive remodeling
(41/113)
(21/75)
(23/122)
Pla
qu
e p
rola
pse
(%
)
p=0.011
Intermediate remodeling
Negative remodeling
Incidence of Plaque Prolapse according to the Remodeling Pattern

Changes of Cardiac Enzymes at FU
12.3 16.3-4.9 -1.5
-60
-40
-20
0
20
40
60
80
Plaque prolapse
No plaque prolapse
CK-MB cTnI

Plaque prolapse (+)
Ste
nt
thro
mb
osi
s (%
)
p=0.3
Plaque prolapse (-)
30-Day Stent Thrombosis Rate
(2/85)
(2/225)
2.4
0.9
0
1
2
3
4
5

Thrombus (OR=1.84, 95% CI 1.08-3.13, p=0.026)
Multivariate Predictors of Post-PCI CK-MB Elevation
Plaque rupture (OR=1.95, 95% CI 1.10-3.46, p=0.023)
Plaque prolapse (OR=7.34, 95% CI 3.55-15.19, p<0.001)

Positive remodeling (OR=1.72; 95% CI 1.01-2.92, p=0.044)
Multivariate Predictors of PP
Stent length (OR=2.39; 95% CI 1.17-3.89, p=0.003)
Plaque rupture (OR=1.96; 95% CI 1.14-3.37, p=0.015)

Conclusions
The incidence of PP after stenting for infarct-related artery
was 27%.
Pre-intervention IVUS lesion characteristics – plaque rupture
and positive remodeling – and longer stent length predict
PP, and PP is associated with myonecrosis after stenting for
infarct-related artery in patients with AMI.