incidenceandriskfactorsofchronicdailyheadache in...
TRANSCRIPT

Incidence and Risk Factors of Chronic Daily Headachein Young Adolescents: A School Cohort Study
WHAT’S KNOWN ON THIS SUBJECT: Several studies haveinvestigated the prevalence of chronic daily headache (CDH) andanalyzed the risk factors for its persistence. However, theetiologic factors that lead to new-onset CDH remain unsettled inadolescents.
WHAT THIS STUDY ADDS: This study was the first incidence studyof CDH conducted in young adolescents. We reported theincidence rates and found that some risk factors for incidentchronic migraine and chronic tension-type headache weredifferent.
abstractOBJECTIVES: This study investigated the incidence and risk factors ofchronic daily headache (CDH) and its major subtypes in young ado-lescents.
METHODS: A field cohort of 3342 adolescents aged 13 to 14 was estab-lished in 3 middle schools in Taitung, Taiwan, from 2005 to 2007. Par-ticipants without CDH at baseline were annually followed up for 1 to 2years using the same questionnaires, including the Adolescent Depres-sion Inventory and Pediatric Migraine Disability Assessment. The neu-rologists made the headache diagnoses based on clinical interviewsand headache diaries. The person-time incidence rates and riskfactors of incident CDH and its subtypes (ie, chronic migraine [CM]and chronic tension-type headache [CTTH]) were calculated byusing Cox proportional hazards models.
RESULTS: The cohort completed 5586 person-years (PYs) of follow-up.Sixty-three subjects (21 boys/42 girls) developed incident CDH with anincidence rate of 1.13 per 100 PYs, including 37 with CM (0.66 per 100PYs) and 22 with CTTH (0.39 per 100 PYs). Thirty-three subjects (52%)had a baseline diagnosis of migraine. The independent risk factors forincident CDH included female gender, acute family financial distress,obesity, higher headache frequency, and a baseline diagnosis ofmigraine. A higher headache frequency was the only identical riskfactor for CDH, CM, and CTTH. A baseline diagnosis of migraine andobesity were significant predictors for both CM and CDH. Femalegender was a significant predictor for both CTTH and CDH.
CONCLUSIONS: Incident CDH was common in young adolescents. Somerisk factors for incident CM and CTTH were different. Pediatrics2013;132:e9–e16
AUTHORS: Shiang-Ru Lu, MD,a Jong-Ling Fuh, MD,b,c,d Shuu-Jiun Wang, MD,b,c,d Kai-Dih Juang, MS, MD,e,f Shih-Pin Chen,MD, PhD,b,d Yi-Chu Liao, MD, PhD,b,g and Yen-Feng Wang,MDb,d
aDepartment of Neurology, Kaohsiung Medical UniversityChung-Ho Memorial Hospital, Kaohsiung, Taiwan; Departments ofbNeurology and ePsychiatry, and cBrain Research Center,National Yang-Ming University School of Medicine, Taipei, Taiwan;dDepartment of Neurology, Neurologic Institute, Taipei VeteransGeneral Hospital, Taipei, Taiwan; and Departments of fPsychiatryand gNeurology, Taichung Veterans General Hospital, Taichung,Taiwan
KEY WORDSadolescence, incidence, migraine headache, tension-typeheadache, risk factors
ABBREVIATIONSADI—Adolescent Depression InventoryCDH—chronic daily headacheCI—confidence intervalCM—chronic migraineCTTH—chronic tension-type headacheHR—hazard ratiosICHD-2—International Classification of Headache Disorders, 2ndeditionICHD-2R—revision of ICHD-2IQR—interquartile rangesMINI-Kid—Mini-International Neuropsychiatric Interview for Chil-dren and AdolescentsPedMIDAS—Pediatric Migraine Disability AssessmentPYs—person-years
Dr Lu collected, analyzed, and interpreted the data and wasresponsible for drafting and revising the manuscript; Dr Fuhdeveloped the concept, designed the study, collected andanalyzed the data, revised the manuscript, and approved thefinal manuscript as submitted; Dr S.J. Wang developed theconcept, designed the study, collected and analyzed the data,drafted the initial manuscript, revised the manuscript, andapproved the final manuscript as submitted; Dr Juangdeveloped the concept, designed the study, and collected thedata; and Drs Chen, Liao, and Y.F. Wang collected and analyzedthe data.
(Continued on last page)
PEDIATRICS Volume 132, Number 1, July 2013 e9
ARTICLE
by guest on July 4, 2018www.aappublications.org/newsDownloaded from

Chronic daily headache (CDH), definedas $15 headache days per month for.3 months, is a worldwide health is-sue.1,2 The International Classificationof Headache Disorders, Second Edition(ICHD-2) and its revision (ICHD-2R) de-fine the following CDH subtypes: chronicmigraine (CM), chronic tension-typeheadache (CTTH), new daily-persistentheadache, and hemicrania continua.3,4
These subtypes are also applied toadolescents.
By examining the factors that contributeto incident (new-onset) CDH, somedeterminants may emerge as potentialtargets for prevention and treatment. Astudy in theUnitedStatesshowedthat the1-year incidence of CDHwas 3% in adults,and risk factors included obesity andbaseline headache frequency.5 In chil-dren and adolescents, the incidence andrisk factors of CDH are largely unknown.
This prospective survey aimed to in-vestigate the person-time incidencerate of CDH and its subtypes (ie, CM andCTTH) in young adolescents who hadbeen followed up for 1 or 2 years and toidentify the relevant risk factors forincident CDH, CM, and CTTH.
METHODS
Setting
This investigationwaspart of theTaitungCounty Adolescent Headache Survey(see Supplemental Information).6 Weselected 3 public middle schools inTaitung County: Tung-Hai, Shin-Sheng,and Chih-Pen. The seventh and eighthgraders at these schools were oursample population; they accounted for46% of adolescents aged 13 to 14 yearsin Taitung County attending middleschools and could be regarded asa community-based sample.
We estimated the required sample sizewas 3282 participants based on thepopulation size of 9336, an assumedincidenceof 1.2%with amarginof errorof 0.3%. To build a large baseline cohort
for the study of CDH incidence, werecruited all the seventh graders atShin-Sheng and all the seventh andeighthgradersat Tung-HaiandChih-Penmiddle schools in 2005 and continuedrecruiting all the seventh graders atTung-Hai and Chih-Pen middle schoolsin 2006 and 2007 (Fig 1A). Those witha diagnosis of CDH at baseline wereexcluded from the cohort. We then an-nually followed up on this cohort from2006 to 2009 while they were still atschool to determine if they developednew-onset CDH (ie, incident cases).Because students spend 3 years inmiddle school (grades 7–9), we couldperform 1 or 2 annual follow-ups dur-ing their middle school years.
The Institutional Review Board of theKaohsiung Medical University reviewedthe medical ethics of this study and theEducation Department of the TaitungCounty Government approved the studybefore it commenced.
Questionnaire
The participants answered the surveyquestionnaires in class by themselveswith the help of teachers and schoolnurses. The questionnaires contained 4parts (see Supplemental Information):
1. Sociodemographics: the collecteddata included age, gender, bodyweight and height, living arrange-ments, highest parental educationallevels, parental occupations, self-reported household economic sta-tus and acute family distress inthe past year, parent-child relations,and consumption of painkillers.
2. A validated headache question-naire for adolescents based onthe ICHD-2 and ICHD-2R was usedfor headache diagnoses.6
3. A validated depression question-naire, the Adolescent DepressionInventory (ADI), was used to surveydepressive symptoms in the previ-ous month. A score $19 was de-fined as depression.7
4. A validated Taiwanese version of thePediatric Migraine Disability Assess-ment (PedMIDAS) was used to as-sess headache disability during theprevious 3 months from grade I (nodisability) to IV (severe disability).8–10
Neurologic Evaluation
Within 3 weeks of the questionnairescreening, subjects who might haveCDH were selected (see SupplementalInformation). After obtaining thewrittenconsent forms from parents, our neu-rologists conducted neurologic exami-nations and semistructured interviewson these potential CDH cases at theirschools. The subjects were asked if theyhad had CDH in the past; only those whodid not have CDH at baseline but de-veloped it later were counted as in-cident CDH cases. The approximatestart and end dates of incident CDHwere estimated by using 1-monthsteps. They were asked, trying theirbest, to describe at least 2 headachephenotypes they had experienced. Theneurologists diagnosed each headachephenotype, determined the frequencyof attacks, and recorded the amount ofmedication usage. Obvious secondarycauses of headaches were excluded. Tofacilitate the diagnoses, the subjectswho were diagnosed as having CDHwere asked to keep a headache diaryfor 1 month. The headache diary andthe neurologists’ diagnosis were dis-cussed in a consensus meeting, andthe final diagnosis of CDH and its sub-types were made.
In this study, CDH was defined asheadache occurring at a frequency$15 days per month, with an averageof $2 hours per day, for .3 months.We shortened the headache durationcriterion from $4 hours to $2 hoursfor adolescents.11,12 CDH subtypeswere classified as CTTH based on theICHD-2 criteria3 and as CM based onthe ICHD-2R criteria,4 with the excep-tion that the number of days with
e10 Lu et al by guest on July 4, 2018www.aappublications.org/newsDownloaded from

probable migraine attacks was alsocounted as migraine days.11 Subjectswho met the criteria for CTTH throughphysician interview but CM based onthe headache diary, or vice versa,were classified as CM. CDH subjectswho did not fulfill the criteria for ei-ther CM or CTTH were classified as“unclassified CDH.” Medication over-use was considered an associated di-agnosis of CDH if the ICHD-2R criteriawere
met.13 A computer algorithm was used tomake migraine diagnoses according tothe ICHD-2 criteria, including migrainewithout aura, migraine with aura, andprobable migraine.3
Psychiatric Interview
Without knowledge of the headache di-agnoses, a board-certified psychiatrist(K.D. Juang) interviewedtheadolescents
with CDH on the same day of the neu-rologic evaluation using the structuredMini-International Neuropsychiatric In-terview for Children and Adolescents(MINI-Kid, version 1.01).14 The assessedpsychiatric disorders included de-pression and anxiety. The score in theMINI Suicidality Module was used tomeasure the suicidal risk (high risk ifthe score was $10, see SupplementalInformation).14
FIGURE 1Thediagnosticflowof thecurrentstudy. A, Therecruitmentandannual follow-upsof seventhandeighthgraders in3middleschools. B, Theresultsof thefirst andsecond annual follow-ups. Cohort 2005a: students recruited at baseline as eighth graders in 2005; Cohort 2005b, 2006, 2007: student recruited at baseline asseventh graders in 2005, 2006 and 2007, respectively.
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 e11 by guest on July 4, 2018www.aappublications.org/newsDownloaded from

The Diagnostic Process
The population of the 3 middle schoolswas 3577 adolescents (1834 boys and1743 girls, mean age 13.26 0.5 years)who were aged 13 (seventh graders,n = 2915) to 14 (eighth graders, n =662) during the recruitment period. Ofthese, 3391 (94.8%) adolescents (1720boys and 1671 girls, mean age 13.2 60.5 years) finished the baseline survey.Forty-nine subjects (1.45%) were di-agnosed as having CDH at the baselinesurvey (boys: 1.10% and girls: 1.80%,P = .095). After excluding these sub-jects, the incidence cohort consisted of3342 subjects (1701 boys and 1641girls, mean age 13.2 6 0.5 years) whowere seventh graders (n = 2734) andeighth graders (n = 608).
To ensure the consistency of diagnoses,the diagnostic processwas the same atboth the baseline survey and the annualfollow-up, including the questionnairesurvey, neurologic evaluation, psychi-atric interview for potential CDH sub-jects, and headache diary recording forincident CDH subjects, except thoseincident CDH subjects diagnosed in theprevious year would also be inter-viewed. The same strategies were ap-plied for prevalent and incident CDHcases. Those students who missed theannual follow-updue tosick leavewouldbe contacted by telephone.
Definition of Variables
The self-reported body heights andweights were crosschecked with therecords in the school nurse’s office tominimize the report bias. BMI was cal-culated as body weight divided by bodyheight squared (kg/m2). Obesity wasdefined according to the age- andgender-specific BMI criteria of the Tai-wan Department of Health.15 Lowerhousehold economic status was definedif it was “belowaverage” or “poor”; lowerparental educational level was definedasmiddle school diplomaor less for bothparents; lower parental occupational
level was defined as both parents beingskilled, semiskilled, or unskilled work-ers; acute family financial distress wasdefined as the presence of a tight hou-sehold budget or parental unemploy-ment that occurred in the past year.
Statistical Analysis
Data were analyzed by using SPSSversion 20, after sensitive personal in-formation had been masked. Continu-ousvariableswereexpressedasmeanswith standard deviations or medianswith interquartile ranges (IQR). Student’st, x2, Fisher’s exact, or Mann-Whitneytests were used for comparisons whenappropriate. For each participant, theperson-years (PYs) of follow-up werecounted from the baseline interview tothe last annual follow-up. The incidencerates of CDH and its subtypes were cal-culated and reported as the number ofnew cases per 100 PYs with 95% confi-dence interval (CI).
The potential risk factors for incidentCDH and its subtypes (see SupplementalInformation) were presented as relativerisks with 95% CI. Variables that wereassociated with incident CDH with a sig-nificance level of P , .25 in univariateanalysis andmissing answers for,10%of the participants were selectedfor a stepwise multivariate Cox pro-portional hazards analysis. Using1-month steps, time at entry was the dateof recruitment; time of exit was the lastannual follow-up for non-CDH subjects orthe self-reported date of CDH onset forincident cases. The independent pre-dictors for incident CDH and its subtypeswere presented as hazard ratios (HR)with 95% CIs. Two-tailed P values ,.05were considered significant.
RESULTS
Participants
Of the incidencecohort,567(293boysand274 girls) eighth graders and 2584 (1292boys and 1292 girls) seventh gradersfinished the first annual follow-up, and
2435 (1214 boys and 1221 girls) seventhgraders finished the second annualfollow-up (Fig 1B). As a whole, there were5586 PYs of follow-up. The participationrate for$1 annual follow-upwas 94.3%.Forty-one of the eighth graders and 150of the seventh graders were lost to thefirst annual follow-up, and 119 of theseventh graders were lost to the secondannual follow-up. The reasons for theloss to follow-up includedmigration anddropping out. The comparisons be-tween the participants and those lost tothe first or second annual follow-up areprovided in Supplemental Information.
Incidence Rate of CDH
During the follow-up period, 241 po-tential cases of new-onset CDH wereselected and interviewed by the neu-rologists. Of these cases, 63 adoles-cents (21 boys and 42 girls,mean age atbaseline 13.0 6 0.4 years) were di-agnosed with incident CDH. Most ofthem (n = 57, 90.5%) completed a head-ache diary for 1 month. Their medianheadache frequency during the past3 months was 16 days per month (IQR15–19), and median PedMIDAS scorewas 9 (IQR 2–15). Five (7.9%) incidentCDH subjects overused acute medi-cations. The person-time incidence rateof incident CDH was 1.13 per 100 PYs.Table 1 shows the age-, cohort-, school-,gender-, and subtype-specific incidencerates of CDH. Girls had a higher in-cidence rate of CDH than boys (1.51 vs0.75 per 100 PYs, P = .007).
CDH Subtype Classification
Of the 63 subjects with incident CDH, 37(58.7%) had CM with an incidence rateof 0.66 per 100 PYs, and 22 (34.9%) hadCTTH with an incidence rate of 0.39 per100 PYs (Table 1). Of the 22 incident CTTHsubjects, 7 (31.8%) also had episodicmigraine or probable migraine. Girlshad a higher incidence rate of CTTH thanboys (0.65 vs 0.14 per 100 PYs, P = .003).Four subjects (6.3%) had “unclassified
e12 Lu et al by guest on July 4, 2018www.aappublications.org/newsDownloaded from
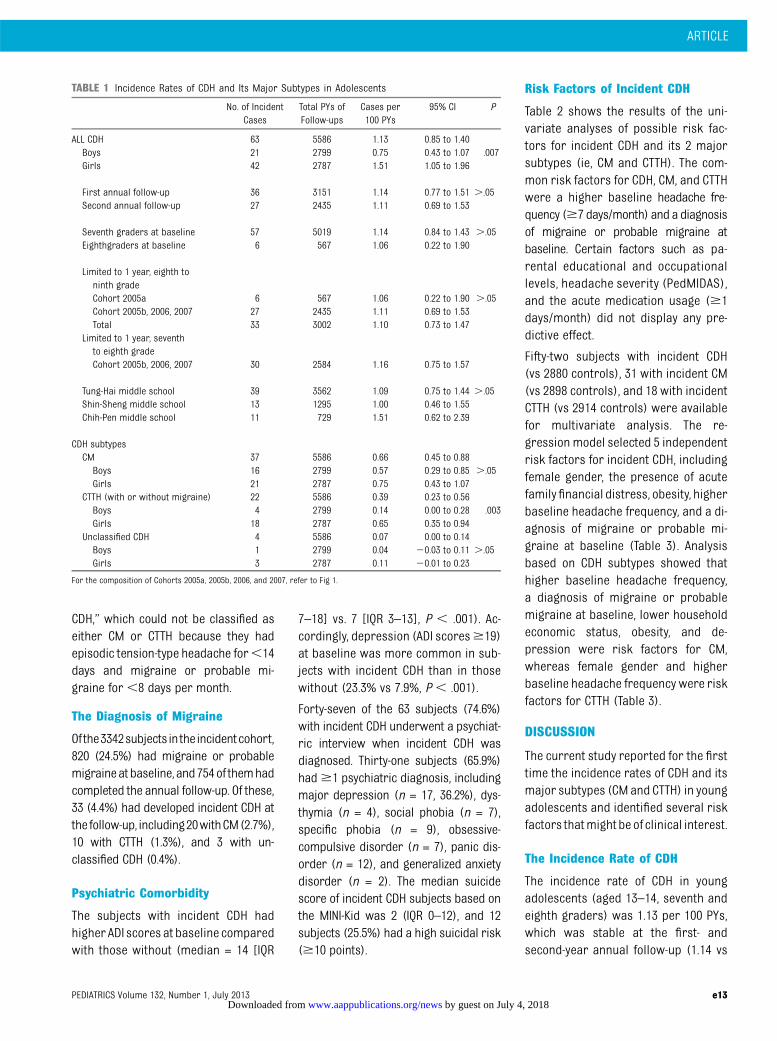
CDH,” which could not be classified aseither CM or CTTH because they hadepisodic tension-type headache for,14days and migraine or probable mi-graine for,8 days per month.
The Diagnosis of Migraine
Ofthe3342subjects intheincidentcohort,820 (24.5%) had migraine or probablemigraineatbaseline,and754of themhadcompleted the annual follow-up. Of these,33 (4.4%) had developed incident CDH atthefollow-up, including20withCM(2.7%),10 with CTTH (1.3%), and 3 with un-classified CDH (0.4%).
Psychiatric Comorbidity
The subjects with incident CDH hadhigher ADI scores at baseline comparedwith those without (median = 14 [IQR
7–18] vs. 7 [IQR 3–13], P , .001). Ac-cordingly, depression (ADI scores$19)at baseline was more common in sub-jects with incident CDH than in thosewithout (23.3% vs 7.9%, P , .001).
Forty-seven of the 63 subjects (74.6%)with incident CDH underwent a psychiat-ric interview when incident CDH wasdiagnosed. Thirty-one subjects (65.9%)had$1 psychiatric diagnosis, includingmajor depression (n = 17, 36.2%), dys-thymia (n = 4), social phobia (n = 7),specific phobia (n = 9), obsessive-compulsive disorder (n = 7), panic dis-order (n = 12), and generalized anxietydisorder (n = 2). The median suicidescore of incident CDH subjects based onthe MINI-Kid was 2 (IQR 0–12), and 12subjects (25.5%) had a high suicidal risk($10 points).
Risk Factors of Incident CDH
Table 2 shows the results of the uni-variate analyses of possible risk fac-tors for incident CDH and its 2 majorsubtypes (ie, CM and CTTH). The com-mon risk factors for CDH, CM, and CTTHwere a higher baseline headache fre-quency ($7 days/month) and a diagnosisof migraine or probable migraine atbaseline. Certain factors such as pa-rental educational and occupationallevels, headache severity (PedMIDAS),and the acute medication usage ($1days/month) did not display any pre-dictive effect.
Fifty-two subjects with incident CDH(vs 2880 controls), 31 with incident CM(vs 2898 controls), and 18 with incidentCTTH (vs 2914 controls) were availablefor multivariate analysis. The re-gression model selected 5 independentrisk factors for incident CDH, includingfemale gender, the presence of acutefamilyfinancial distress, obesity, higherbaseline headache frequency, and a di-agnosis of migraine or probable mi-graine at baseline (Table 3). Analysisbased on CDH subtypes showed thathigher baseline headache frequency,a diagnosis of migraine or probablemigraine at baseline, lower householdeconomic status, obesity, and de-pression were risk factors for CM,whereas female gender and higherbaseline headache frequency were riskfactors for CTTH (Table 3).
DISCUSSION
The current study reported for the firsttime the incidence rates of CDH and itsmajor subtypes (CM and CTTH) in youngadolescents and identified several riskfactors thatmight be of clinical interest.
The Incidence Rate of CDH
The incidence rate of CDH in youngadolescents (aged 13–14, seventh andeighth graders) was 1.13 per 100 PYs,which was stable at the first- andsecond-year annual follow-up (1.14 vs
TABLE 1 Incidence Rates of CDH and Its Major Subtypes in Adolescents
No. of IncidentCases
Total PYs ofFollow-ups
Cases per100 PYs
95% CI P
ALL CDH 63 5586 1.13 0.85 to 1.40Boys 21 2799 0.75 0.43 to 1.07 .007Girls 42 2787 1.51 1.05 to 1.96
First annual follow-up 36 3151 1.14 0.77 to 1.51 ..05Second annual follow-up 27 2435 1.11 0.69 to 1.53
Seventh graders at baseline 57 5019 1.14 0.84 to 1.43 ..05Eighthgraders at baseline 6 567 1.06 0.22 to 1.90
Limited to 1 year, eighth toninth gradeCohort 2005a 6 567 1.06 0.22 to 1.90 ..05Cohort 2005b, 2006, 2007 27 2435 1.11 0.69 to 1.53Total 33 3002 1.10 0.73 to 1.47
Limited to 1 year, seventhto eighth gradeCohort 2005b, 2006, 2007 30 2584 1.16 0.75 to 1.57
Tung-Hai middle school 39 3562 1.09 0.75 to 1.44 ..05Shin-Sheng middle school 13 1295 1.00 0.46 to 1.55Chih-Pen middle school 11 729 1.51 0.62 to 2.39
CDH subtypesCM 37 5586 0.66 0.45 to 0.88Boys 16 2799 0.57 0.29 to 0.85 ..05Girls 21 2787 0.75 0.43 to 1.07
CTTH (with or without migraine) 22 5586 0.39 0.23 to 0.56Boys 4 2799 0.14 0.00 to 0.28 .003Girls 18 2787 0.65 0.35 to 0.94
Unclassified CDH 4 5586 0.07 0.00 to 0.14Boys 1 2799 0.04 20.03 to 0.11 ..05Girls 3 2787 0.11 20.01 to 0.23
For the composition of Cohorts 2005a, 2005b, 2006, and 2007, refer to Fig 1.
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 e13 by guest on July 4, 2018www.aappublications.org/newsDownloaded from

1.11 per 100 PYs) and was similar be-tween those recruited as seventh andeighth graders (1.14 vs 1.06 per 100 PYs;Table 1). If we limited the period to 1year (ie, from seventh to eighth grade orfrom eighth to ninth grade), the in-cidence rates between different cohortswere similar (Table 1). Overall, thesedata were consistent despite of a varia-tion in the composition of the partic-ipants and the length of observation.
Risk Factors for Incident CDH
The current study identified 5 in-dependent risk factors for incidentCDH. Of these, obesity and higherheadache frequency were also pre-dictors for incident CDH in adults.5 Thissuggests both factors are importantfor the initiation of CDH in adults andyoung adolescents, and because bothfactors are modifiable, they might betargets for primary prevention of in-cident CDH.
In our previous prevalence study con-ducted in another school-based sample(seventh toninthgraders), thepredictors
for persistence of CDH included femalegender, acute medication overuse,chronic migraine, major depression,and anxiety disorder.12 Compared withthe current study, some risk factorswere common for both incident andprevalent CDH (eg, migraine and fe-male gender), and others were not (ie,medication overuse). It is unclear howthese factors interplay and contributeto CDH in young adolescents.
Several independent risk factors forincident CDH, CM, and CTTH found in thisstudy deserve further discussion.
1. High headache frequency: this wasthe only consistent risk factor forincident CDH, CM, and CTTH. Two lon-gitudinal studies also demonstratedthat a higher baseline headache fre-quency predicted the evolution ofCDH and transformed migraine fromepisodic headache.5,16 Higher head-ache frequency may indicate centralsensitization of nociceptive neuronsin the trigeminal pathway, thus pav-ing the way to headache chronifica-tion and the development of CDH.17
2. Migraine or probable migraine atbaseline: CM represents a naturalevolution from episodic migraine;a baseline diagnosis of migrainewas therefore a sine qua non andpredictor for CM and CDH in thisstudy. In our cohort, 2.7% of adoles-cents with migraine or probable mi-graine at the baseline developedincident CM in 1 to 2 years.
3. Obesity: the relationship betweenobesity and adult migraine has beenhighlighted in cross-sectional surveyswith mixed results.18–20 In youngmigraineurs, the role of obesity hasonly been evaluated in clinic-basedstudies. The prevalence of obesitywas not increased in children or ado-lescents with CM compared with pop-ulation norms,21,22 but obesity or BMIwere positively correlated with mi-graine frequency.21,23 Our study pro-vided the epidemiologic evidence inAsians that supports obesity as a riskfactor for adolescent CM and CDH.
4. Female gender: our study showedthat the incidence rates of CDH and
TABLE 2 Univariate Relative Risk (RR) for Incidence of CDH and Its Subtypes in Adolescents
Variable CDH Non-CDH Total CDH CM CTTH
(% at risk) (% at risk) RR (95% CI) P RR (95% CI) P RR (95% CI) P
Female gender 42/63 1524/3088 2.02 (1.20–3.40) .008 1.33 (0.70–2.54) .389 4.55 (1.54–13.43) .006(66.7%) (49.4%)
Lower household economic status 32/60 937/2988 2.45 (1.49–4.05) ,.001 2.86 (1.47–5.56) .002 1.95 (0.83–4.58) .125(53.3%) (31.4%)
Lower parental education level 8/44 401/2379 1.09 (0.51–2.34) .816 0.90 (0.31–2.58) .838 1.79 (0.57–5.60) .316(18.2%) (16.9%)
Lower parental occupation status 15/43 791/2176 0.94 (0.50–1.75) .843 0.74 (0.32–1.68) .469 2.05 (0.69–6.07) .197(34.9%) (36.4%)
Acute family financial distress 23/60 482/3065 3.23 (1.93–5.38) ,.001 3.46 (1.77–6.76) ,.001 2.42 (0.99–5.91) .052(38.3%) (15.7%)
Little parenting time 16/58 463/3066 2.10 (1.19–3.71) .010 2.07 (0.97–4.43) .061 1.73 (0.64–4.69) .285(27.6%) (15.1%)
Baseline headache $7 d/mo 11/63 108/3075 5.37 (2.88–10.02) ,.001 4.91 (2.09–11.54) ,.001 7.46 (2.80–19.88) ,.001(17.5%) (3.50%)
Migraine or probable migraine at baseline 33/63 721/3088 3.50 (2.15–5.69) ,.001 3.74 (1.97–7.10) ,.001 2.65 (1.15–6.11) .022(52.4%) (23.3%)
Depression (ADI $19) 14/60 239/3037 3.42 (1.91–6.14) ,.001 4.32 (2.11–8.86) ,.001 1.98 (0.59–6.72) .271(23.3%) (7.9%)
Higher PedMIDAS grade (grade II–IV) 5/63 166/3085 1.50 (0.61–3.69) .377 2.11 (0.76–5.89) .154 0.83 (0.11–6.13) .854(7.9%) (5.4%)
Acute medication usage $1 d/mo 12/62 390/3082 1.63 (0.88–3.05) .120 1.36 (0.57–3.26) .484 2.01 (0.74–5.41) .169(19.4%) (12.7%)
Obesity 15/63 502/3071 1.58 (0.89–2.80) .116 2.43 (1.23–4.80) .011 0.51 (0.12–2.16) .358(23.8%) (16.3%)
e14 Lu et al by guest on July 4, 2018www.aappublications.org/newsDownloaded from

CTTH were higher in girls than boys.In a similar vein, a cross-sectionaltwin study showed the prevalenceof CTTH increased in adolescent girlsbeginning at age 15, whereas it re-mained unchanged in adolescentboys.24 Whether sex hormones con-tribute to this phenomenon is un-known, and further investigation iswarranted.
5. Psychological and socioeconomic fac-tors: depression, lower householdeconomic status, and acute familyfinancial distress were predictorsfor incident CM or CDH in this study.In line with this, our previous lon-gitudinal surveys among youngadolescents aged 13 to 15 haddemonstrated depression as an im-portant factor for persistence of CDHat follow-up.12 The role of householdeconomy in adolescent CM had beenfeatured in 1 cross-sectional study25:low household income was corre-lated with CM in those without a fam-ily history of migraine, suggestinga role of social causation.25
The Diagnostic Issue of CDH, CM,and CTTH in Adolescents
The differences between adult and ad-olescent CDH are not well understood.
We shortened the duration criterion ofCDH to$2 hours in this study becauseyoung adolescents have shorter head-ache duration than adults and alsocounted the days with probable mi-graine attacks as migraine days. Theseadjustments had no impact on the in-cidence of CDH in general but increasedthe diagnostic rate of CM.11,12 Despitethis, the distinction between CM andCTTHwas not so clear-cut in some of ourCDH subjects owing to coexistence ofmigraine and tension-type headaches. Ifthe ICHD-2R criteria for CMwere appliedwithout modification, 5 of our CM sub-jects would be categorized as CTTH and3 as unclassified CDH, and the incidencerate of CM, CTTH, and unclassified CDHwould be 0.52, 0.48, and 0.13 per 100 PYs,respectively. The ICHD-2R criteria for CMmay undergo revision in the near future.
Limitations
Our study has limitations. First, althoughthe participation rate was high through-out thestudy, thesubjects lost to follow-upmay bias the results because they sharedsome characteristics with incident CDHcases (ie, lower household economicstatus, higher ADI scores, and migraineat baseline). Second, the cohort effectshould be considered. Because we
recruited subjects of different ages atdifferent timepoints, the difference in lifeexperience across the generations mighthave an impact on CDH incidence. Despitethat, we found the CDH incidence wasconsistent among the different cohorts(Table 1), indicating that the cohort effectwas not significant. Third, recall biaswas inevitable as all demographicsand headache features were self-reported by the participants. Nonethe-less, we have used various questioningtechniques and corroborated the clinicalinterview with the headache diary tovalidate the headache diagnoses. Fourth,type II errors could not be avoided whileanalyzing the risk factors for CDH sub-types because of the relatively smallnumber of cases of CM and CTTH. Fifth,because ethnic discrepancy was found incertain headache disorders, it is uncertainwhether the results of this study can beextrapolated to other ethnic groups.
CONCLUSIONS
Our study found that the incidence rateof CDH was 1.13 per 100 PYs in youngadolescents and underscores severalrisk factors associated with incidentCDH. Additional research is needed tounderstand the interactive relationshipof these factors in adolescent CDH.
TABLE 3 Stepwise Multivariate Cox Proportional Models of HR and 95% CIs for the Incidence of CDH, CM, and CTTH
Significant Risk Factors HR 95% CI P Factors Not Significant P
CDHBaseline headache $7 d/mo 4.06 1.94–8.49 ,.001 Lower household economic status .330Migraine or probable migraine at baseline 3.07 1.75–5.41 ,.001 Little parenting time .213Female gender 2.40 1.29–4.48 .006 Acute medication use $1 d/mo .253Acute family financial distress 2.32 1.32–4.10 .004 Depression .091Obesity 1.96 1.04–3.69 .038
CMMigraine or probable migraine at baseline 4.44 2.06–9.59 ,.001 Female gender .167Baseline headache $7 d/mo 2.89 1.08–7.76 .035 Acute family financial distress .444Depression (ADI $19) 2.47 1.08–5.62 .032 Little parenting time .426Obesity 2.41 1.13–5.14 .023 Acute medication usage $1 d/mo .336Lower household economic status 2.29 1.10–4.75 .026
CTTHBaseline headache $7 d/month 7.87 2.58–23.95 ,.001 Lower household economic status .629Female gender 3.37 1.11–10.24 .032 Acute family financial distress .315
Little parenting time .612Acute medication usage $1 d/mo .887Obesity .737Migraine or probable migraine at baseline .459Depression (ADI $19) .386
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 e15 by guest on July 4, 2018www.aappublications.org/newsDownloaded from

REFERENCES
1. Dodick DW. Clinical practice. Chronic dailyheadache. N Engl J Med. 2006;354(2):158–165
2. Stovner L, Hagen K, Jensen R, et al. Theglobal burden of headache: a documenta-tion of headache prevalence and disabilityworldwide. Cephalalgia. 2007;27(3):193–210
3. Headache Classification Subcommittee ofthe International Headache Society. TheInternational Classification of HeadacheDisorders: 2nd edition. Cephalalgia. 2004;24(suppl 1):9–160
4. Olesen J, Bousser MG, Diener HC, et al;Headache Classification Committee. Newappendix criteria open for a broader con-cept of chronic migraine. Cephalalgia.2006;26(6):742–746
5. Scher AI, Stewart WF, Ricci JA, Lipton RB.Factors associated with the onset and re-mission of chronic daily headache in a pop-ulation-based study. Pain. 2003;106(1-2):81–89
6. Wang SJ, Fuh JL, Juang KD, Lu SR. Migraineand suicidal ideation in adolescents aged 13to 15 years. Neurology. 2009;72(13):1146–1152
7. Huang CY, Hsu WY. A study of developing anadolescent depression inventory [in Chi-nese]. J Educ Psychol. 2003;26(1):167–190
8. Hershey AD, Powers SW, Vockell AL, LeCatesS, Kabbouche MA, Maynard MK. PedMIDAS:development of a questionnaire to assessdisability of migraines in children. Neurol-ogy. 2001;57(11):2034–2039
9. Hershey AD, Powers SW, Vockell AL, LeCatesSL, Segers A, Kabbouche MA. Developmentof a patient-based grading scale for Ped-MIDAS. Cephalalgia. 2004;24(10):844–849
10. Hung PH, Fuh JL, Wang SJ. Validity, re-liability and application of the taiwan ver-sion of the migraine disability assessmentquestionnaire. J Formos Med Assoc. 2006;105(7):563–568
11. Wang SJ, Fuh JL, Lu SR, Juang KD. Chronicdaily headache in adolescents: prevalence,impact, and medication overuse. Neurology.2006;66(2):193–197
12. Wang SJ, Fuh JL, Lu SR, Juang KD. Out-comes and predictors of chronic dailyheadache in adolescents: a 2-year longi-tudinal study. Neurology. 2007;68(8):591–596
13. Silberstein SD, Olesen J, Bousser MG, et al.The International Classification of HeadacheDisorders, 2nd Edition (ICHD-II)—revision ofcriteria for 8.2 Medication-overuse head-ache. Cephalalgia. 2005;25(6):460–465
14. Sheehan DV, Lecrubier Y, Sheehan KH et al.The Mini-International Neuropsychiatric In-terview (M.I.N.I.): the development and vali-dation of a structured diagnostic psychiatricinterview for DSM-IV and ICD-10. J Clin Psy-chiatry. 1998;59(suppl 20):22–33; quiz 34–57
15. Chen W, Chang MH. New growth charts forTaiwanese children and adolescents basedon World Health Organization standardsand health-related physical fitness. PediatrNeonatol. 2010;51(2):69–79
16. Bigal ME, Serrano D, Buse D, Scher A,Stewart WF, Lipton RB. Acute migrainemedications and evolution from episodic tochronic migraine: a longitudinal population-based study. Headache. 2008;48(8):1157–1168
17. Aurora SK, Kulthia A, Barrodale PM. Mech-anism of chronic migraine. Curr PainHeadache Rep. 2011;15(1):57–63
18. Bigal ME, Lipton RB. Obesity is a risk factorfor transformed migraine but not chronictension-type headache. Neurology. 2006;67(2):252–257
19. Mattsson P. Migraine headache and obesityin women aged 40-74 years: a population-based study. Cephalalgia. 2007;27(8):877–880
20. Winter AC, Berger K, Buring JE, Kurth T.Body mass index, migraine, migraine fre-quency and migraine features in women.Cephalalgia. 2009;29(2):269–278
21. Hershey AD, Powers SW, Nelson TD, et al;American Headache Society Pediatric Ado-lescent Section. Obesity in the pediatricheadache population: a multicenter study.Headache. 2009;49(2):170–177
22. Pakalnis A, Kring D. Chronic daily headache,medication overuse, and obesity in chil-dren and adolescents. J Child Neurol. 2012;27:577–580
23. Kinik ST, Alehan F, Erol I, Kanra AR. Obesityand paediatric migraine. Cephalalgia. 2010;30(1):105–109
24. Russell MB, Levi N, Saltyte-Benth J, Fenger K.Tension-type headache in adolescents andadults: a population based study of 33,764twins. Eur J Epidemiol. 2006;21(2):153–160
25. Bigal ME, Lipton RB, Winner P, Reed ML,Diamond S, Stewart WF; AMPP advisorygroup. Migraine in adolescents: associationwith socioeconomic status and family his-tory. Neurology. 2007;69(1):16–25
(Continued from first page)
www.pediatrics.org/cgi/doi/10.1542/peds.2012-1909
doi:10.1542/peds.2012-1909
Accepted for publication Apr 5, 2013
Address correspondence to Shuu-Jiun Wang, MD, The Neurologic Institute, Taipei Veterans General Hospital, Taipei, 112, Taiwan. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Lu has received research support from the Taiwan National Science Council and Kaohsiung Medical University, Taiwan. Dr Fuh isa member of a scientific advisory board of Eli Lilly and has received research support from the Taiwan National Science Council, Taipei-Veterans General Hospital,and Eli Lilly. Dr S.J. Wang has served on the advisory boards of Pfizer, Allergan, and Eli Lilly Taiwan. He has received speaking honoraria from local companies(Taiwan branches) of Pfizer, Eli Lilly, and Boehringer Ingelheim. He has received research grants from the Taiwan National Science Council, Taipei Veterans GeneralHospital, and Taiwan Headache Society. Dr Juang has indicated no financial relationships relevant to this article to disclose. Dr Chen has received researchsupport from the Taiwan National Science Council and Taipei Veterans General Hospital. Dr Liao has received research support from the Taiwan National ScienceCouncil and Taichung Veterans General Hospital. Dr Y.F. Wang received research support from Taipei Veterans General Hospital.
FUNDING: Supported in part by the Taiwan National Science Council (grants 100-2314-B-010-019-MY2 and 100-2314-B-010-018-MY3), Taipei-Veterans General Hospital(grants VGHUST101-G7-1-1, V101C-106, and V101E7-003), NSC support for the Center for Dynamical Biomarkers and Translational Medicine, National CentralUniversity, Taiwan (grant NSC 100-2911-I-008-001), the Brain Research Center at National Yang-Ming University, and a grant from Ministry of Education, Aim for theTop University Plan.
e16 Lu et al by guest on July 4, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2012-1909 originally published online June 17, 2013; 2013;132;e9Pediatrics
Yi-Chu Liao and Yen-Feng WangShiang-Ru Lu, Jong-Ling Fuh, Shuu-Jiun Wang, Kai-Dih Juang, Shih-Pin Chen,
School Cohort StudyIncidence and Risk Factors of Chronic Daily Headache in Young Adolescents: A
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/132/1/e9including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/132/1/e9#BIBLThis article cites 22 articles, 6 of which you can access for free at:
Subspecialty Collections
ubhttp://www.aappublications.org/cgi/collection/head_neck_injuries_sHead and Neck Injuriesdicine_subhttp://www.aappublications.org/cgi/collection/adolescent_health:meAdolescent Health/Medicinefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 4, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2012-1909 originally published online June 17, 2013; 2013;132;e9Pediatrics
Yi-Chu Liao and Yen-Feng WangShiang-Ru Lu, Jong-Ling Fuh, Shuu-Jiun Wang, Kai-Dih Juang, Shih-Pin Chen,
School Cohort StudyIncidence and Risk Factors of Chronic Daily Headache in Young Adolescents: A
http://pediatrics.aappublications.org/content/132/1/e9located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2013/06/12/peds.2012-1909.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 4, 2018www.aappublications.org/newsDownloaded from