incorporating behavioral health into the health planning process to improve value jack mahoney, md,...
TRANSCRIPT
Incorporating Behavioral Health Into the
Health Planning Process to Improve Value
Jack Mahoney, MD, MPH

2
About Pitney Bowes
80+ year legacy
Fortune 500 company
$5.9 billion global provider of integrated mail and document management solutions
global team of more than 35,000 employees
presence in more than 130 countries worldwide
more than 2 million customers

3
Mailstream
Printing
Create Produce Manage
Creative Services
DataManagement
Preparation &
Finishing
Distribute
Presort &Distribution
Store/Retrieve
Receive &
Integrate
Healthy, Productive Employees
CorporateResponsibility
ValuesCulture
ProgramsPurchasing
Health Plan Design
4
Optimizing Employee Health Benefits for a Healthier and More Productive Workforce
Rule 1: The health of your organization begins with your people.
Rule 2: To realize total value, you must understand total cost.
Rule 3: Higher costs don’t always mean higher value.
Rule 4: Health begins and ends with the individual.
Rule 5: Avoid barriers to effective treatment.
Rule 6: Carrots are valued over sticks.
Rule 7: Total value demands total teamwork.

5
On-site Clinics Wellness Programs
& Screenings Disability
Management
Workers Compensation
Safety
Crisis Management
Product Stewardship
Benefits Administration
Benefit Design
Funding / Underwriting
Vendor Sourcing & Management
Direct Delivery ConsultationMedical • Pharmacy Behavioral Health
Health Planning
Pitney Bowes Health Services Organization

6
Behavioral Health Integration
Benefit PlanManagement
and Design

7
Behavioral Health: PB Overview
Plan design carved out of all self-funded plans
• > 80% of population is self-funded exceeds parity
• unlimited in-network inpatient and outpatient services
• no deductible, co-insurance for in-network services
• specialist co-pays at PCP level

8
Enrollee Annual Cost Distribution
10%
50%
35%
5%
Nonusers Less than $1,000
$1,000 to $10,000 More than $10,000
Total CostParticipants
15%
75%
10%

9
Predictive Model Results
$1,000 to
$10,000
10%
50%
35%
5%
More than $10,000 Non Users
Up to$1,000

10
Predictive Model Results
$1,000 to
$10,000
10%
50%
35%
5%
More than $10,000 Non Users
Up to$1,000

11
Key Learning: Engage People in Managing Their Health
Remove access barriers to all health plans free or limited cost of preventive/screening
services eliminate front-end deductibles robust EAP services
• 8 session face-to-face free EAP– 3 sessions combined with unlimited telephonic for
Enterprise Services
• EAP utilization currently at 5%

12
Behavioral Health Integration
Benefit PlanManagement
and Design
Condition
Management

13
Predictive Model Results
$1,000 to
$10,000
10%
50%
35%
5%
More than $10,000 Non Users
Up to$1,000

14
Predictive Model Results
$1,000 to
$10,000
10%
50%
35%
5%
More than $10,000 Non Users
Up to$1,000

15
Key Predictors for Migration From Normal Spend to High-Cost Tier
Individuals with chronic conditions and low medication-compliance rates
asthma• more than 1 fill of albuterol in a 30-day period
diabetes• less than nine 30-day fills in a 12-month period
hypertension• less than nine 30-day fills in a 12-month period
depression• less than six 30-day fills in a 12-month period

16
chronic disease prevalenceis growing
RX is an integral partof managing
mostchronic
conditions
low possessionrates of targetmedications
is key predictorof future diseaseburden and cost
company’s futurehealth claims can
be reduced bykeeping employees
with chronic disease on their medications
Then:If: And: And:
How to keep employees taking their chronic disease medications?
Rx drugs are subject to
price elasticityof demand
Rx drug demand
elasticity is a function of
cost
medicationcompliance isa function of
drug access andaffordability
put target chronicdisease medicationson most affordable
tier to increasecompliance with
disease managementprogram
Then:If: And: And:
Pharmacy Benefit Design Decision
17
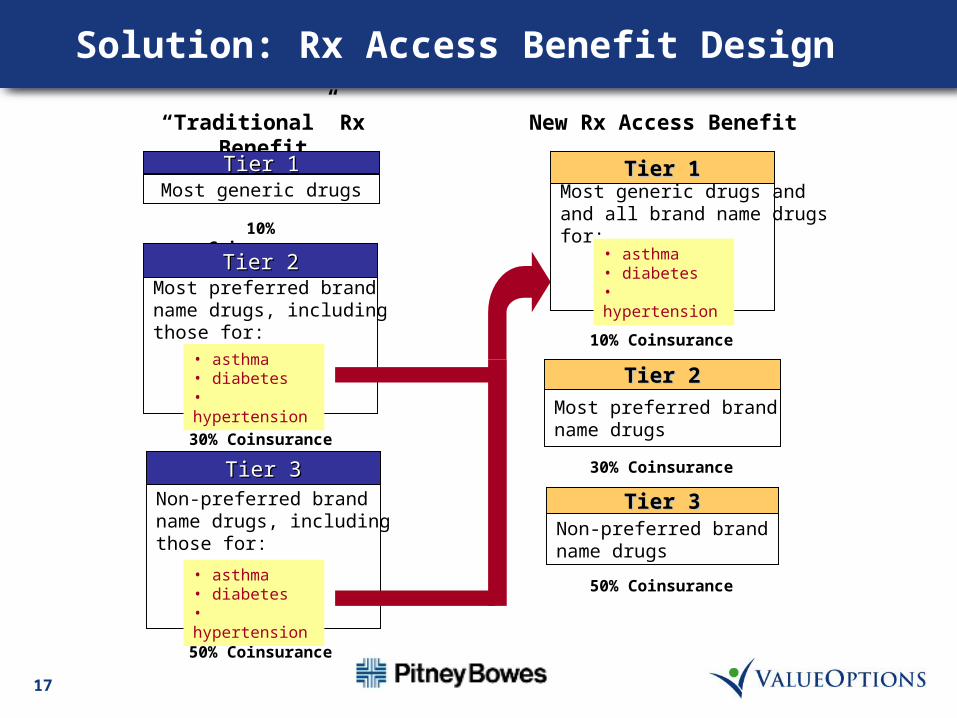
“Traditional” Rx Benefit New Rx Access Benefit
50% Coinsurance
Most generic drugsTier 1Tier 1
10% Coinsurance
50% Coinsurance
Non-preferred brandname drugs, includingthose for:
Tier 3Tier 3
• asthma• diabetes• hypertension
Most preferred brandname drugs
Tier 2Tier 2
Non-preferred brandname drugs
Tier 3Tier 3
10% Coinsurance
30% Coinsurance
Most generic drugs andand all brand name drugs for:
Tier 1Tier 1
• asthma• diabetes• hypertension
30% Coinsurance
Most preferred brandname drugs, includingthose for:
Tier 2Tier 2
• asthma• diabetes• hypertension
Solution: Rx Access Benefit Design

18
Depression and Mood Disorders
depression prevalence and costs significant for PB
• prevalence and cost equivalent to diabetes
• co-morbidity for many chronic conditions
• antidepressants second in “Top 25” prescription drug listing
• 2nd leading cause of short-term disability
inappropriate possession rates of medication identified by predictive modeling as indicator of future cost
• less than six 30-day scripts
19
prevalence• 37 per thousand
– 14% above national benchmark
• 1.45 admits per thousand– 9.5% above benchmark
• 277 office visits per thousand– 26% above national benchmark
Depression and Mood Disorders (cont.)

20
Depression and Mood Disorders (cont.)
Implementation issues if value-based pharmacy design implemented:
prescribing patterns for filled Rxs• 20% of Rx written by psychiatrists
– typically for 180 days
• 80% written by PMDs– majority (> 80%) not refilled
– significant compliance issues
care management• role of cognitive therapy
21
Depression and Mood Disorders (cont.)
mood disorder patients have high rates of co-morbidities by MDC• musculoskeletal• skin and breast• ENT• circulatory• metabolic• digestive• nervous system
comorbid with other target conditions• asthma: 13%• diabetes: 17%• cardiovascular: 19%

22
Mood Disorder Patients: Comorbidities
Mood Disorder Patients Compared to Total Active and Early Retiree Population
0%
25%
50%
75%
MD
C 1
MD
C 2
MD
C 3
MD
C 4
MD
C 5
MD
C 6
MD
C 7
MD
C 8
MD
C 9
MD
C 1
0
MD
C 1
1
MD
C 1
2
MD
C 1
3
MD
C 1
4
MD
C 1
5
MD
C 1
6
MD
C 1
7
MD
C 1
8
MD
C 1
9
MD
C 2
0
MD
C 2
1
MD
C 2
2
MD
C 2
3
MD
C 2
5
Mood Disorder Patients Actives and Early Retirees
% o
f P
op
ula
tio
n w
ith
MD
C D
iag
no
sis

23
Alternative Approach Building Foundation
reduce access barriers to behavioral healthcare• plan design
• EAP
• direct services
awareness/education program
work with managed care vendors to influence care delivery• eValue8
integrated disability management
no formulary change

24
Behavioral Health Integration
Benefit PlanManagement
and Design
Condition
Management
Health Plan

25
Health Plan Management for Quality
Quality Purchasing
used by business health coalitions and national employers to assess and manage the quality of available HMO/POS and PPO plans
eValue8 raises the bar for health care performance and moves the market to deliver greater value for the purchaser's health care dollar
gathers information on hundreds of benchmarks
standardized performance reports are prepared for comparison

26
Health Plan Management for Quality
Goal of eValue8™ quality health care administrative excellence consumer satisfaction cost-effective prices
27
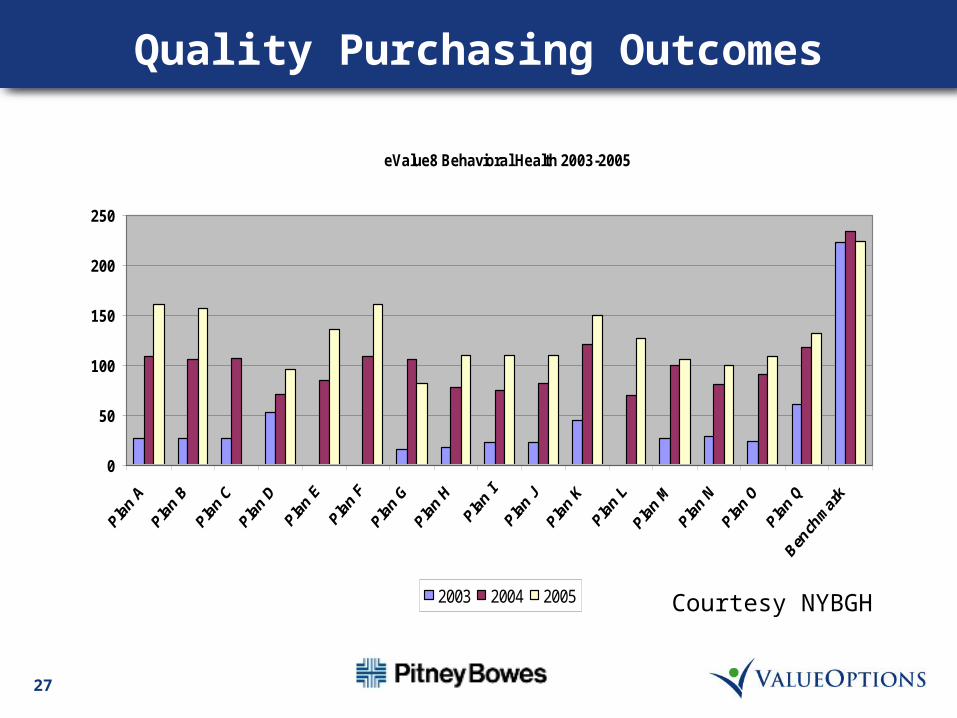
Quality Purchasing Outcomes
eValue8 Behavioral Health 2003-2005
0
50
100
150
200
250
2003 2004 2005 Courtesy NYBGH

28
Behavioral Health Integration
Benefit PlanManagement
and Design
Condition
Management
Health PlanDirect
Delivery

29
Depression and Mood Disorders
On-site Services depression awareness campaigns stress EAP
• EAP practitioner has scheduled time at all on-site clinics
• EAP practitioner available to management in all locations for critical incident/ER issues

30
Integrating Behavioral Health and Disability: Results
all behavioral health disability claims referred to Value Options for evaluation and assessment of work capacity
disability clients with secondary behavioral health diagnoses also referred
final work decision rests with PB disability department results
• 40% reduction in average duration of disability first six months• average duration of disability: 50-60 days, prior to Pitney
Bowes/Value Options program

31
Behavioral Health Integration
Benefit PlanManagement
and Design
Condition
Management
Health Plan
Direct Delivery
Consultation

32
Summary
behavioral health issues pervade all aspects of health planning• “carve-out” should not promote “silos”
integrated approach to client problems yields significant results
partnership of all parties essential for success