increased preoperative levels of plasma fibrinogen and d dimer in patients with renal cell carcinoma...
TRANSCRIPT

Urologic Oncology: Seminars and Original Investigations ] (2014) ∎∎∎–∎∎∎
http://dx.doi.org/10.1016/j1078-1439/r 2014 Elsev
* Corresponding authofax: þ90-212-635-1918.E-mail addresses: oners
(O. Sanli).
Original article
Increased preoperative levels of plasma fibrinogen and D dimer in patientswith renal cell carcinoma is associated with poor survival and adverse
tumor characteristics
Selcuk Erdem, M.D., Akin Soner Amasyali, M.D., Omer Aytac, M.D., Kadir Onem, M.D.,Halim Issever, M.D., Oner Sanli, M.D.*
Department of Urology, Istanbul Faculty of Medicine, Istanbul University, Istanbul, Turkey
Received 15 February 2014; received in revised form 10 March 2014; accepted 11 March 2014
Abstract
Background and objective: The relationship between renal cell carcinoma (RCC) and coagulation/fibrinolysis system has beendescribed in several studies. The aim of this study was to investigate the role of 4 different coagulation/fibrinolysis factors on the predictionof histopathologic and survival prognosis in patients with RCC.Patients and methods: Data from 128 patients who underwent surgical intervention between March 2006 and January 2011 for RCC
were evaluated in this prospective study. Blood samples were collected from all patients on the morning of the operation to measure theplasma fibrinogen, D-dimer, coagulation factor VII, and antithrombin 3 levels. The relationships of these factors in the demographic, clinical,and histopathologic outcomes were analyzed using the Student t, Mann-Whitney U, Kruskal-Wallis, and one-way analysis of variance tests.Receiver operating curve analyses were performed to determine the optimal cutoff level for fibrinogen and D dimer, both of which had astrong relation with the clinical and histopathologic parameters. Disease-free survival (DFS), cancer-specific survival (CSS), and overallsurvival (OS) were assessed using the Kaplan-Meier method. Multivariate Cox regression analyses (forward stepwise logistic regression)were performed to examine the independent prognostic values on survival outcomes.Results: Increased plasma fibrinogen and D-dimer levels were associated with tumor size (P ¼ 0.004 and 0.106), nuclear grade
(P o 0.001 and o0.001), TNM category (P o 0.001 and 0.029), and metastasis (P o 0.001 and 0.032). Both increased plasma fibrinogenand D-dimer levels predicted decreased DFS (P ¼ 0.027 and 0.04), CSS (P ¼ 0.007 and 0.043), and OS (P ¼ 0.014 and 0.001) rates basedon Kaplan-Meier analyses. Furthermore, multivariate analyses demonstrated that fibrinogen independently predicted poor DFS (hazard ratio[HR] ¼ 2.52; 95% CI: 1.04–6.31; P ¼ 0.029) and CSS (HR ¼ 3.89; 95% CI: 1.13–13.40; P ¼ 0.032), whereas D dimer had negativeindependent prognostic value on OS (HR ¼ 4.01; 95% CI: 1.54–10.50; P ¼ 0.005).Conclusions: Increased plasma fibrinogen levels accurately predict poor histopathologic and survival outcomes and may be an effective
independent prognostic factor in patients with RCC. Moreover, D dimer may serve as a copredictive factor in conjunction withfibrinogen. r 2014 Elsevier Inc. All rights reserved.
Keywords: Renal cell carcinoma; Fibrinogen; D dimer
1. Introduction
The reported incidence of organ-confined renal cellcarcinoma (RCC) has increased because of the routine use
.urolonc.2014.03.013ier Inc. All rights reserved.
r. Tel.: þ90-212-414-2000/þ90-212-413-1832;
[email protected], [email protected]
of cross-sectional imaging for a variety of diseases [1].Despite the identification of more renal masses and appro-priate surgical interventions, the development of metastasisis still a major concern in approximately 17% of patientswith incidental and 30% of patients with whole RCC [2,3].Currently, histopathologic parameters such as the Fuhrmannuclear grade (FNG), tumor size, and TNM staging havebeen used for prognosis prediction, but these parameters donot adequately provide a natural history of RCC. The use of
S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–102
biomarker data may improve the prediction of the overallprognosis and metastasis in these patient populations.
The coagulation pathway may play a role in cancerpathogenesis because the elevation of several coagulation/fibrinolysis factors is observed in patients with metastaticRCC [4]. This cancer-related coagulation cascade may bemediated by tissue factor (TF) on the surface of cancer cellsor by tumoral angiogenesis process [5,6]. Briefly, TF, whichis an initiator of the extrinsic coagulation pathway incarcinogenesis, is expressed on the surface of cancer cellsand stimulates the cancer-related coagulation cascade.Conversely, vascular endothelial growth factor (VEGF)-dependent angiogenesis is the most important biologicalprocess in RCC, and it has been demonstrated that angio-genesis and the coagulation cascade are closely relatedprocesses that stimulate each other during carcinogenesis[6]. TF is also stimulated by VEGF in endothelial cells,which results in the formation of thrombin and in clotformation, by converting soluble fibrinogen into insolublefibrin monomers [7]. These findings indicate that the factorsparticipating in the coagulation/fibrinolytic pathways arealso involved in regulating tumor angiogenesis.
Based on the close relation between RCC and thecoagulation/fibrinolysis system, 4 measurable key factorsmay be identified. (1) Fibrinogen, a glycoprotein synthesizedby hepatocytes, is a target molecule at the final step of thecoagulation cascade that is converted to fibrin monomers bythrombin and ultimately forms fibrin polymers. The role offibrinogen in carcinogenesis has been demonstrated in severalexperimental and clinical studies [8–10]. More importantly,recent evidence suggests that elevated plasma fibrinogen levelis an independent predictor of the adverse pathologic featuresencountered in RCC and is associated with poor survival [11–13]. (2) D dimer, the smallest fibrin(ogen) degradation product(FDP), which is the end result of plasmin-catalyzed digestionof fibrin(ogen), can be used as a marker of fibrinolytic systemactivity [10]. The routine assessment of plasma D-dimer levelsis crucial in diagnosing cancer-related or any-other-cause–related thromboembolic status and pulmonary embolism[14,15]. The relationship between increased plasma D-dimerlevels and carcinoma has been reported in several cancertypes, including RCC, but it has not been studied as aprognostic biomarker for RCC [16–19]. (3) Coagulationfactor VII (FVII), an enzyme that triggers the extrinsiccoagulation pathway, and its essential cofactor TF initiatekey pathogenetic mechanisms in cancer, including angio-genesis, cell migration, invasion, and survival [5,20–23]. (4)Antithrombin 3 (AT3) is a major plasma inhibitor ofcoagulating proteases, which primarily consist of thrombinand factor Xa [24]. The antiangiogenic and antitumor growthproperties of AT3 have been described previously [25,26].
In the present study, we prospectively evaluated therelationships of the plasma fibrinogen, D-dimer, FVII, andAT3 levels between histopathologic tumor characteristics andpatient survival. In addition, we determined whether thesefactors could be used as prognostic biomarkers for RCC.
2. Patients and methods
Between March 2006 and January 2011, 156 patientsunderwent curative or cytoreductive nephrectomy for theirrenal masses in a single tertiary academic center. Afterpreoperative staging evaluation with contrast-enhancedcomputed tomography (CT) or magnetic resonance imaging(MRI) scans, open or laparoscopic partial or radical neph-rectomy was performed at the treating surgeon's discretion.To eliminate the factors that influence the coagulation/fibrinolysis system, we excluded patients who receivedregular anticoagulation therapy or had other malignancybesides RCC (n = 20) and those with benign pathology (n =8). This study was approved by our local institutionalreview board.
Fibrinogen, D-dimer, FVII, and AT3 levels were assessedby collecting 2 ml of blood samples in a coagulation tube(9NC coagulation/fibrinolysis sodium citrate 3.2%,13 � 75 mm) from all patients on the morning of theoperation. The plasma fibrinogen, D-dimer, FVII, and AT3levels were quantified using the Stago STA-R Evolutiondiagnostic device (Diagnostica Stago UK Ltd, Theale, UK)and STA-Fib 2, STA-Liatest D-Di, STA-Stachrom AT III 3,and STA-Deficient VII reagents (Diagnostica Stago UKLtd, Theale, UK), respectively. The accepted normal rangefor each parameter was 200 to 400 mg/dl, 0 to 0.5 mg/ml,80% to 100%, and 70% to 130% for fibrinogen, D-dimer,AT3, and FVII, respectively.
In addition, blood samples were collected from 41 age-matched healthy controls who underwent surgery for benigndisease (benign prostatic hyperplasia, urinary stone disease,urinary incontinence, etc.) at the same center. These patientswere screened with a chest X-ray and at least 1 imagingmodality, such as ultrasonography, CT, or MRI.
The demographic, clinical, and histopathologic outcomeswere prospectively recorded for each patient. The patientswere pathologically staged using the 2010 TNM stagingclassification system [27]. The surveillance strategy follow-ing treatment included routine laboratory testing (serumcreatinine and estimated glomerular filtration rate), chestx-ray, and ultrasound, CT, or MRI every 3 to 6 months forthe first 2 years and then every 6 months until the fifth yearafter surgical intervention. Patients with distant metastasiswere referred to the oncology department for targetedtherapy consideration. Recurrence, metastasis, and survival(disease-free survival [DFS], cancer-specific survival [CSS],and overall survival [OS]) were prospectively documented.
DFS (i.e., the number of months from surgery to localrecurrence or metastasis; 8 patients were excluded owing topreoperative metastasis) and CSS (i.e., the number ofmonths from surgery to cancer-related death) were theprimary end points of the study. In addition, the secondaryend points included the OS (the number of months fromsurgery to death with any cause) and the relationshipsbetween histopathologic outcomes and coagulation/fibrinol-ysis factors.

Table 1The demographic, clinicopathologic, and follow-up parameters of patients
Patients no., n 128Age, y 58.66 � 11.31 (21–83)Male/female, n (%) 91/37 (75.7/24.3)
Operation type, n (%)Partial nephrectomyOpen 16 (12.5)Laparoscopic 10 (7.8)
Radical nephrectomyOpen 72 (56.2)Laparoscopic 30 (23.4)
Tumor side, n (%)Right 63 (49.2)Left 65 (50.8)
Pathologic tumor size, cm 7.91 � 4.81 (2–20)
Histologic subtypes, n (%)Clear cell 94 (73.4)Papillary 19 (14.8)Chromophobe 13 (10.1)Unclassifed 2 (1.5)
Fuhrman grade, n (%)Grade 1 2 (1.5)Grade 2 51 (39.8)Grade 3 52 (40.6)Grade 4 23 (17.9)
Pathologic T category, n (%)pT1a 27 (21.1)pT1b 35 (27.3)pT2a 15 (11.7)pT2b 6 (4.6)pT3a 43 (33.6)pT3b 2 (1.5)
TNM staging groups, n (%)Category 1 60 (46.9)Category 2 19 (14.8)Category 3 39 (30.5)Category 4 10 (7.8)
Metastasis, n (%)Preoperative 8 (6.3)Lung and bone 2Lung and liver 1Lung 3Bone 1Adrenal 1
Postoperative 21 (16.4)Lung, brain and bone 1Lung and brain 2Lung and bone 2Lung and liver 1Lung 8Liver 3Local recurrence 4
Median follow-up, mo 36.5 (1–88)
Status of patients, n (%)Alive 95 (74.2)With disease 10 (7.8)Disease free 85 (66.4)
Table 1Continued
Death 33 (25.8)Cancer related 19 (14.9)Non–cancer related 14 (10.9)
Fibrinogen (200–400 mg/dl) 438.7 � 195.8 (209–1,229)D dimer (0–0.5 mg/ml) 1.0 � 0.56 (0.1–3.42)Factor VII (%) 97.7 � 30.3 (13–200)Antithrombin 3 (%) 102.2 � 18.8 (40–186)
S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–10 3
2.1. Statistical analysis
The results from the Kolmogorov-Smirnov one-sampletest showed that fibrinogen and D dimer were not in anormal distribution, unlike FVII and AT3. The demo-graphic, clinical, and histopathologic parameters wereanalyzed using the Mann-Whitney U test and the Kruskal-Wallis one-way analysis of variance (ANOVA) test forfibrinogen and D dimer, whereas the Student t test and aone-way ANOVA test was used for FVII and AT3. Multiplecomparisons were examined using the z test and the Tukeytest for the Kruskal-Wallis and the one-way ANOVA tests,respectively.
Receiver operating curve (ROC) analyses were used todetermine the optimal cutoff values for the continuousplasma fibrinogen and D-dimer levels. The survival out-comes were analyzed using the Kaplan-Meier method, andcomparisons were made using the log-rank test. Thestatistically significant (P o 0.05) factors identified by theunivariate analyses were used as covariables in the multi-variate Cox regression analyses (forward stepwise logisticregression) to examine their independent prognostic valueon survival outcomes. The hazard ratios (HRs) with a 95%CI were reported as relative risks for each independentfactor.
3. Results
The demographic, clinicopathologic, and follow-upparameters of the study cohort are shown in Table 1.
In comparison with healthy controls, patients with RCChad significantly higher fibrinogen (374.5 vs. 332 mg/dl,P ¼ 0.002) and D-dimer (0.91 vs. 0.75 mg/ml, P ¼ 0.011)levels and lower FVII (97.68 � 30.25 vs. 112.1 � 26.19%,P ¼ 0.007) levels (Table 2). However, no significantchanges were observed in the AT3 levels between thegroups (102.16 � 18.76 vs. 103.39 � 13.13, P ¼ 0.696).
Based on the analysis of the histopathologic parameters,both the fibrinogen and D-dimer levels were significantlyelevated in patients with higher FNG (P o 0.001 vs.o0.001) and higher TNM categories (P o 0.001 vs.0.029) compared with patients with lower FNG and TNMcategories. The post hoc analysis (Kruskal-Wallis z test)revealed that FNG 4 had significantly higher levels of both

Table 2The analysis of the relation between coagulation factors and demographic, histopathologic, and clinical parameters
n Fibrinogen, mg/dl D dimer, mg/ml Factor VII (%) Antithrombin 3 (%)
Patients with RCC 128 374.5 (209–1,229) 0.91 (0.1–3.42) 97.68 � 30.25 102.16 � 18.76Controls 41 332 (218–468) 0.75 (0.19–1.32) 112.1 � 26.19 103.39 � 13.13P 0.002 0.011 0.007 0.696
SexMale 91 388 (209–1,229) 0.95 (0.1–3.42) 98.42 � 33.01 102.98 � 19.47Female 37 360 (223–1,202) 0.82 (0.22–2.37) 95.87 � 22.37 100.14 � 16.97P 0.743 0.612 0.667 0.439
Age, yo60 65 338 (219–1,229) 0.89 (0.13–2.32) 100.08 � 32.54 105.54 � 19.72Z60 63 413 (209–1,202) 1.03 (0.1–3.42) 95.21 � 27.75 98.67 � 17.18P 0.090 0.211 0.365 0.038
Operative sideRight 63 369 (209–1,202) 0.77 (0.1–3.42) 94.81 � 29.27 102.1 � 19.32Left 65 390 (215–1,229) 1 (0.19–2.51) 100.46 � 31.15 102.22 � 18.34P 0.475 0.075 0.292 0.971
Tumor size, cmr7 80 353 (209–1,013) 0.89 (0.1–2.51) 95.89 � 27.56 102.01 � 19.3547 48 440.5 (215–1,229) 1.02 (0.27–3.42) 100.67 � 34.38 102.40 � 17.93P 0.004 0.106 0.389 0.911
Histologic subtypesClear cell 94 390 (209–1,229) 0.975 (0.13–2.54) 97.55 � 27.50 101.42 � 19.41Papillary 19 387 (215–784) 0.75 (0.1–3.42) 97.90 � 19.16 99.89 � 18.74Chromophobe 13 338 (219–526) 0.82 (0.27–1.46) 98.53 � 36.51 109.23 � 13.49P 0.564 0.255 0.994 0.328
Fuhrman gradea
Grade 2 51 334 (219–769) 0.75 (0.13–3.42) 99.71 � 31.13 103.75 � 16.73Grade 3 52 361 (209–812) 0.91 (0.1–1.83) 95.73 � 30.99 102.46 � 21.35Grade 4 23 674 (305–1,229) 1.33 (0.58–2.54) 94.78 � 27.05 97.04 � 16.99P o0.001 o0.001 0.736 0.359
Pathologic T categorya
T1 62 337.5 (209–664) 0.86 (0.1–2.06) 96.71 � 27.95 104.15 � 20.06T2 21 390 (215–1,229) 1.0 (0.27–3.42) 103.76 � 33.82 107.19 � 18.53T3 45 493 (219–1,202) 1.04 (0.31–2.54) 96.18 � 31.90 97.07 � 16.04P o0.001 0.06 0.603 0.062
TNM stagingCategory 1–2 79 338 (209–769) 0.89 (0.1–3.42) 98.43 � 30.2 105.48 � 19.88Category 3–4 49 450 (219–1,229) 1.04 (0.31–2.54) 96.47 � 30.61 96.8 � 15.53P o0.001 0.029 0.723 0.01
MetastasisNo 99 353 (209–1,063) 0.89 (0.1–3.42) 98.96 � 31.79 103.08 � 19.50Yes 29 448.5 (254–1,229) 1.02 (0.22–2.51) 92.65 � 23.12 98.54 � 15.31P o0.001 0.032 0.345 0.272
Metastatic patientsPreoperative 8 440 (413–1,229) 0.97 (0.56–2.15) 89.11 � 26.41 98.89 � 17.72Postoperative 21 470.5 (254–1,202) 1.07 (0.22–2.51) 100.63 � 10.51 97.75 � 8.53P 0.437 0.657 0.249 0.865
SurvivalAlive 95 350 (209–812) 0.77 (0.1–3.42) 100.61 � 31.09 106.08 � 17.39Ex 33 450 (219–1,229) 1.23 (0.22–2.37) 89.24 � 26.34 90.85 � 18.19P o0.001 o0.001 0.063 o0.001
aPost hoc analysis.
S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–104
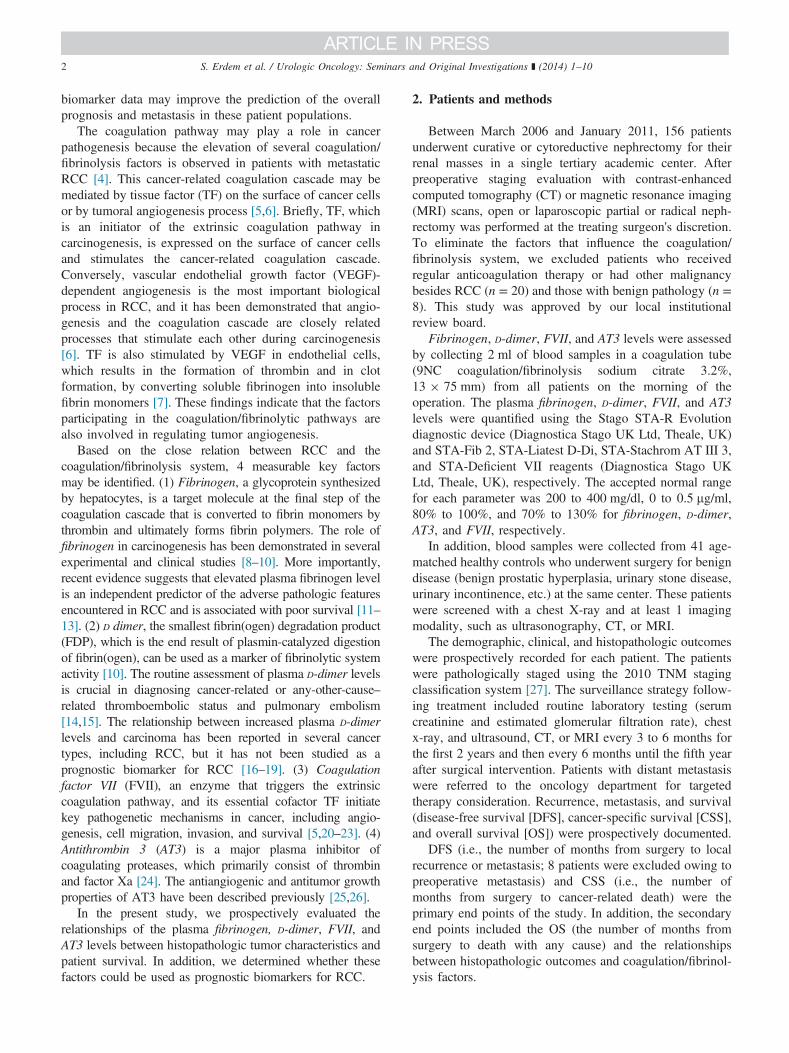
Fig. 1. The receiver operating curve (ROC) analyses of plasma fibrinogenand D-dimer levels. The optimal cutoff values are 343 mg/dl and 0.76 μg/mlfor fibrinogen (sensitivity ¼ 0.586, specificity ¼ 0.585, P ¼ 0.002) and D
dimer (sensitivity ¼ 0.609, specificity ¼ 0.585, P ¼ 0.011). (Colorversion of figure is available online.)
S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–10 5
fibrinogen and D dimer compared with FNG 2 and 3. Theadvanced pathologic T category was also associated withelevated fibrinogen levels (P o 0.001), and a post hocanalysis showed that the pT3-category tumors were signifi-cantly different from the pT1- and pT2-category tumors.Decreased AT3 levels were only associated with advancedTNM category (P ¼ 0.01), whereas FVII had no associ-ation with any histopathologic parameters.
The median fibrinogen (448.5 vs. 353 mg/dl,P o 0.001) and D-dimer (1.02 vs. 0.89 mg/ml, P ¼0.032) levels were significantly higher in metastatic patientscompared with nonmetastatic patients. Conversely, therewas no association between the plasma fibrinogen (P ¼0.437) and D-dimer levels (P ¼ 0.657) and preoperativelyand postoperatively detected metastases. FVII (P ¼ 0.345)and AT3 (P ¼ 0.272) were not associated with themetastatic status of the patients.
A total of 33 patients died, with a median follow-up of36.5 months. The patients who died had significantly higherpreoperative fibrinogen (450 vs. 350 mg/dl, P o 0.001) andD-dimer (1.23 vs. 0.77 mg/ml, P o 0.001) levels and lowerAT3 (106.08 � 17.39 vs. 90.85 � 18.19%, P ¼ 0.001)levels compared with the surviving patients.
The plasma fibrinogen and D-dimer levels were inves-tigated as independent predictors of survival because theyare closely related to clinicohistopathologic parameters. Forthis purpose, the ROC analyses were performed for bothfactors, and the optimum cutoff values were determined tobe 343 mg/dl and 0.76 mg/ml for fibrinogen (sensitivity ¼0.586, specificity ¼ 0.585, P ¼ 0.002) and D dimer(sensitivity ¼ 0.609, specificity ¼ 0.585, P ¼ 0.011),respectively (Fig. 1). According to these cutoff values, 53and 50 patients had decreased fibrinogen and D-dimer
levels, respectively, whereas 75 and 78 patients hadincreased fibrinogen and D-dimer levels, respectively.
The Kaplan-Meier analyses showed that the 5-yearDFS (88.1% vs. 72.4%, P ¼ 0.027), CSS (92.8% vs.70.9%, P ¼ 0.007), and OS (78.7% vs. 61.6%, P ¼0.014) rates were significantly lower in patients withincreased fibrinogen levels. In addition, increased D-dimerlevels were associated with significantly lower 5-year DFS(88.4% vs. 71.9%, P ¼ 0.04), CSS (90.5% vs. 72.6%, P¼ 0.043), and OS (88.7% vs. 55.3%, P ¼ 0.001) rates(Fig. 2).
Based on the univariate survival analysis, higher FNGand pathologic T category were also associated withdecreased DFS (P ¼ 0.034 and 0.014, respectively), CSS(P ¼ 0.002 and 0.003, respectively), and OS (P ¼ 0.002and 0.002, respectively) rates. Moreover, the clear cellhistologic subtype was associated with a lower DFS (P ¼0.026) rate, and a larger tumor size was associated withlower CSS (P ¼ 0.035) and OS (P ¼ 0.041) rates(Table 3).
Using multivariate Cox regression analyses for theprimary end points, it was found that increased fibrinogenlevels were an independent negative prognostic value forboth DFS (HR ¼ 2.52; 95% CI: 1.04–6.31; P ¼ 0.029)and CSS (HR ¼ 3.89; 95% CI: 1.13–13.40; P ¼ 0.032) aswell as increased FNG (HR ¼ 4.04; 95% CI: 1.51–10.81;P ¼ 0.005 and HR ¼ 6.38; 95% CI: 1.47–27.74; P ¼0.013) (Table 4). The clear cell histologic subtype (P ¼0.006) was also a negative independent prognostic factorfor DFS. However, increased D-dimer levels (HR ¼ 4.01;95% CI: 1.54–10.50; P ¼ 0.005), increased FNG (HR ¼2.14; 95% CI: 0.98–6.26; P ¼ 0.056), and a pathologic Tcategory higher than T1 (HR ¼ 2.4; 95% CI: 1.08–5.35;P ¼ 0.032) were identified as negative prognostic factorsfor OS.
4. Discussion
Angiogenesis, which is the development of abnormalnew blood vessels from existing vasculature, consists of themigration, proliferation, and differentiation of endothelialcells and is a prerequisite for the growth and metastasis oftumors [10]. However, VEGF, a major stimulator ofangiogenesis, plays a crucial role in the interaction betweenangiogenesis and the coagulation/fibrinolysis system [28].The stimulation of VEGF causes an increase in theproduction of TF by activated endothelial cells. Theexpression of TF and other procoagulant factors by tumorcells and the local activation of the coagulation cascadehave been reported in previous studies [6,29]. The for-mation of the TF/FVII complex is the first step of theextrinsic coagulation cascade. An experimental animalstudy demonstrated that the inhibition of the TF/FVIIcomplex blocks angiogenesis and tumor progression [30].Thus, it is possible that the extrinsic activation of the

Fig. 2. Kaplan-Meier charts of survival analyses. (A) Disease-free survival analyses of the patients stratified by fibrinogen and D dimer cutoff (343 mg/dl and0.76 μg/ml, respectively) levels. (B) Cancer-specific survival analyses of the patients stratified by fibrinogen and D-dimer cutoff (343 mg/dl and 0.76 μg/ml,respectively) levels. (C) Overall survival analyses of the patients stratified by fibrinogen and D dimer cutoff (343 mg/dl and 0.76 μg/ml, respectively) levels.(Color version of figure is available online.)
S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–106
coagulation cascade in patients with RCC results in adecrease of FVII by binding to TF. In parallel with thishypothesis, the present study found decreased FVII levels inpatients with RCC. However, the FVII levels were notassociated with FNG and metastatic status; consequently,we do not suggest that FVII is a suitable biomarkerfor RCC.
The concomitant activation of angiogenesis and thecoagulation cascade in RCC was indicated in an immuno-histochemical study by Verheul et al. [31]. In their study, theauthors demonstrated that VEGF, an angiogenesis marker,was expressed in 100% of the RCC specimens and thatfibrinogen, a coagulation marker, was detected near bloodvessels in 84% of the RCC cases. In addition, the authorsreported that fibrinogen adjacent to tumor cells was inde-pendently related to VEGF expression based on a multi-variate analysis. In another study, Sahni and Francis [28]found that VEGF specifically bound to fibrinogen with highaffinity, and fibrinogen-bound VEGF retained its functionalactivity on endothelial cell differentiation during angiogene-sis. Thus, there is some evidence that the interaction ofangiogenesis and tumor cells with the extracellular matrix issimultaneously regulated through secreted procoagulant andfibrinolytic agents. Meanwhile, fibrin(ogen) in the extracel-lular matrix acts as a “molecular bridge” between tumor cells,endothelium, and thrombocytes; fibrin(ogen)-covered plate-let/tumor microthrombi in circulation protect tumor cells
against the immune system and help tumor cells to migrateand stabilize at distant metastatic sites [8,9,32]. For thisreason, many authors have recently investigated the relation-ship between high plasma fibrinogen levels and adversepathologic features and survival.
In a well-designed experimental study, Palumbo et al. [9]investigated the role of fibrinogen on the carcinogenesis anddissemination of tumor cells. In their study, the authors foundthat the hematogenous pulmonary micrometastasis andlymph node metastasis of Lewis lung carcinoma werediminished in fibrinogen-deficient mice compared with thecontrol group. Meanwhile, the growth of primary or secon-dary tumors and angiogenesis was not different between thegroups. The same authors also documented that fibrinogenacts as a facilitating factor for the metastasis of circulatingtumor cells by promoting the sustained adhesion and survivalof these cells in the vasculature system [8]. Based on thetumor biological process, fibrinogen is one of the mostinvestigated coagulation factor in different cancer types suchas gastric, colorectal, pancreatic, ovarian, endometrial, andbreast [16,33–38].
Meanwhile, recent evidence suggests that there may be apossible relationship between hyperfibrinogenemia andadverse histopathologic features of RCC as well assurvival. In one such study, Xiao et al. [11] reported thathyperfibrinogenemia was associated with an increasedtumor category, lymph node metastasis and distant

Table 3Univariate survival analyses of patients grouped by demographic and histopathologic parameters and nominee biomarkers
Disease-free survival (n ¼ 120) Cancer-specific survival (n ¼ 120) Overall survival (n ¼ 128)
n 5-y DFS rates (%) χ2 P n 5-y CSS rates (%) χ2 P 5-y OS rates (%) χ2 P
SexMale 86 82.7 1.828 0.176 91 84.2 2.525 0.112 68.6 0.448 0.503Female 34 70.9 37 72.7 68.4
Age, yo60 61 80.8 0.283 0.595 65 82.2 0.251 0.617 76.5 3.594 0.058Z60 59 77.6 63 78.6 62.1
Pathologic T categoryT1 60 88.0 6.037 0.014 62 91.1 8.889 0.003 78.4 9.285 0.002T2-T3 60 69.7 66 69.3 53.6
Tumor size, cmr7 77 81.7 0.009 0.926 80 85.5 4.450 0.035 73.3 4.177 0.04147 43 78.7 48 71.1 61.2
Fuhrman gradeGrade 1–2 53 89.1 4.515 0.034 53 95.0 9.921 0.002 82.2 10.007 0.002Grade 3–4 67 70.8 75 69.3 59.4
Histologic subtypeClear cell 86 73.9 4.471 0.026 95 75.9 2.422 0.120 62.8 2.421 0.120Non–clear cell 34 93.4 33 92.3 84.8
Fibrinogen, mg/dlo343 52 88.1 4.901 0.027 53 92.8 7.247 0.007 78.7 5.987 0.014Z343 68 72.4 75 70.9 61.6
D dimer, mg/mlo0.76 48 88.4 4.217 0.04 50 90.5 4.104 0.043 88.7 11.186 0.001Z0.76 72 71.9 78 72.6 55.3
χ2 ¼ log-rank test.
S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–10 7
metastasis. Another Chinese group (Du et al. [12]),demonstrated that higher preoperative fibrinogen levelsare an independent negative predictor of DFS and OS inpatients with RCC, which is in parallel with advancedtumor category and distant metastasis. In a large-scaleEuropean cohort of patients (n ¼ 994), Pichler et al.proposed a cutoff value of 466 mg/dl (according to an ROCanalysis) for fibrinogen levels. The results from the multi-variate analyses in this study suggested that fibrinogenlevels higher than this value independently predicted poorCSS (HR ¼ 2.47; 95% CI: 1.49–4.11; P ¼ 0.001), DFS(HR ¼ 2.15; 95% CI: 1.44–3.22; P ¼ 0.001), and OS(HR ¼ 2.48; 95% CI: 1.80–3.40; P ¼ 0.001) rates witholder age, advanced pathologic T category and nucleargrade [12]. In line with these studies, the present studyrevealed that higher fibrinogen levels were significantlyassociated with poor histopathologic and clinical outcomessuch as larger tumor size, increased FNG, advanced pTcategory, metastatic progression, and death. The univariatesurvival analyses suggested that the patients with higherfibrinogen levels (4343 mg/dl) had significantly lowerDFS (median ¼ 12.5 vs. 20.5 mo, P ¼ 0.027), CSS(median ¼ 19 vs. 29 mo, P ¼ 0.007), and OS (median ¼12.5 vs. 20.5 mo, P ¼ 0.014) rates compared with patientswith lower fibrinogen levels. Furthermore, based on
multivariate analyses, increased fibrinogen levels remainedan independent negative prognostic factor for impairedDFS (HR ¼ 2.52; 95% CI: 1.04–6.31; P ¼ 0.029) andCSS (HR ¼ 3.89; 95% CI: 1.13–13.40; P ¼ 0.032) ratesin RCC as well as advanced FNG. Consequently, wepropose that preoperative plasma fibrinogen level is apromising survival prognostic factor that should be con-sidered in the follow-up of patients with RCC.
The contribution of immunotherapy on survival out-comes has been well described in patients with metastaticRCC. From this point of view, Casamassima et al. evaluatedseveral biohumoral parameters including fibrinogen topredict the immunotherapy response rate in metastaticRCC. They found that the median survival rate wassignificantly decreased in patients with hyperfibrinogenemiain comparison with their normal or lower counterparts(10 vs. 17 mo, P ¼ 0.01). Moreover, the authors reportedthat hyperfibrinogenemia was significantly related to dis-ease progression against immunotherapy in comparisonwith treatment response [39].
The other significant finding of the present study thatmerits to be mentioned is based on the increased D-dimerlevels and its relationship with poor histopathologic andsurvival outcomes in RCC. Elevated preoperative plasmaD-dimer levels were also associated with increased FNG,

Table 4Multivariate survival analyses
Disease-free survival (n ¼ 120) Cancer-specific survival (n ¼ 128) Overall survival (n ¼ 128)
Hazard ratio (95% CI) P Hazard ratio (95% CI) P Hazard ratio (95% CI) P
SexFemale 1 (reference) 0.02 1 (reference) 0.056 1 (reference) 0.304Male 2.48 (1.16–5.29) 0.42 (0.17–1.04) 1.42 (0.7–2.92)
Age, yo60 1 (reference) 0.862 1 (reference) 0.891 1 (reference) 0.065Z60 1.23 (0.57–2.63) 1.22 (0.49–3.03) 1.95 (0.95–3.98)
Pathologic T categoryT1 1 (reference) 0.284 1 (reference) 0.09 1 (reference) 0.032T2-T3 1.55 (0.60–3.96) 2.5 (0.78–8.33) 2.40 (1.08–5.35)
Tumor size, cmr7 – – 1 (reference) 0.268 1 (reference) 0.51447 1.61 (0.51–5.05) 1.37 (0.56–3.35)
Histologic subtypesNon–clear cell 1 (reference) 0.012 – – – –
Clear cell 6.36 (1.5–26.99)
Fuhrman gradeGrade 1–2 1 (reference) 0.005 1 (reference) 0.013 1 (reference) 0.056Grade 3–4 4.04 (1.51–10.81) 6.38 (1.47–27.74) 2.47 (0.98–6.26)
Fibrinogen, mg/dlo343 1 (reference) 0.029 1 (reference) 0.032 1 (reference) 0.143Z343 2.52 (1.04–6.31) 3.89 (1.13–13.40) 2.14 (0.81–4.16)
D dimer, mg/mlo0.76 1 (reference) 0.136 1 (reference) 0.114 1 (reference) 0.005Z0.76 1.92 (0.80–4.56) 2.43 (0.80–7.41) 4.02 (1.54–10.50)
S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–108
advanced pT category, metastatic progression, and death.Based on univariate analyses, higher D-dimer levels(40.76 mg/ml) were also associated with poor DFS(median ¼ 15 vs. 22 mo, P ¼ 0.04), CSS (median ¼21 vs. 25 mo, P ¼ 0.043), and OS (median ¼ 15 vs.23 mo, P ¼ 0.001) rates. However, based on multivariateanalyses, higher D-dimer levels predicted only decreased OSrates, which can not solely be related to cancer-specificcauses. In a clinical study investigating the role of anabnormal pretreatment coagulation profile on the responseto immunotherapy and survival outcomes in metastaticRCC, Tsimafeyeu et al. categorized the patients using boththe fibrinogen and D-dimer levels together with fibrinmonomer. The investigators concluded that hypercoagul-ability (i.e., increased fibrinogen and D-dimer levels in thepresence of fibrin monomer) predicted a poor immunother-apy response rate and OS among patients with metastaticRCC, which is similar to the study by Casamassima et al.[4,39]. In the present study, D dimer, as a FDP, was not apredictive factor based on multivariate DFS and CSSanalyses whereas fibrinogen strongly predicted poor out-comes for these primary end points. The possible explan-ation for this contrary finding may be related to the evidencereported by Palumbo et al. who found no reductionof hematogenous metastasis in plasminogen-deficient mice,
which indicates that plasmin-activated fibrinolysis and FDPsare not necessary for metastasis. Meanwhile, a deficiency infibrinogen significantly diminished hematogenous distantmetastases [8]. Despite, the plasma D-dimer levels was notfound to be an independent factor for DFS and CSS inmultivariate analyses, we believe that it may be used assupportive prognostic marker to make a prediction forborderline patients who have plasma fibrinogen level nearerto cutoff value.
According to the present study, it is rational to suggestthat patients with RCC with preoperative increasedfibrinogen level may need closer surveillance strategiesfor upfront metastases after surgery. However, this studyshould provide future directions on clinical approach withfurther studies such as whether patients with increasedpreoperative fibrinogen levels should have lower thresh-old to initiate targeted agents or whether they benefit fromanticoagulative agents (e.g., low-molecular-weight hepa-rin) to prevent future metastasis or thromboembolicevents. On the contrary, collecting sera samples frompatients and monitoring fibrinogen levels during follow-up would help to understand the effect of treatment onrelation between disease and coagulation system. More-over, preoperative fibrinogen level may be incorporatedinto prognostic systems and nomograms that combine

S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–10 9
independent factors to predict the prognosis in patientswith RCC [40–44].
The relatively small cohort of patients in comparisonwith those in the previous reports is a major limitation ofthe present study. Another negative aspect is the limitedduration of follow-up. On the contrary, the prospectivenature of the study is a major strength. We believe that thepresent study, along with previously reported studies,advocates the use of preoperative plasma fibrinogen levelsas a prognostic marker in patients with RCC. Moreover, theplasma D-dimer levels, not alone but in conjunction with theplasma fibrinogen levels, may be used as an adjuvantprognostic marker.
5. Conclusions
The coagulation/fibrinolysis system is closely associ-ated with RCC pathogenesis, which reflects histopatho-logic and survival outcomes. Preoperatively increasedfibrinogen levels independently predict decreased DFSand CSS rates in patients with RCC. For this reason,plasma fibrinogen levels may be used as a prognosticbiomarker for RCC prognosis. In addition, plasma D-dimerlevels may be another surrogate measure for the prognosisof patients with RCC in conjunction with plasma fibri-nogen levels.
References
[1] Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CACancer J Clin 2012;62:10–29.
[2] Bensalah K, Pantuck AJ, Crepel M, et al. Prognostic variables topredict cancer-related death in incidental renal tumours. BJU Int2008;102:1376–80.
[3] Kyoda Y, Kobayashi K, Hirobe M, et al. Evaluation of long-termoutcome for patients with renal cell carcinoma after surgery: analysisof cancer deaths occurring more than 10 years after initial treatment.Int J Clin Oncol 2014;19:146–51.
[4] Tsimafeyeu IV, Demidov LV, Madzhuga AV, Somonova OV,Yelizarova AL. Hypercoagulability as a prognostic factor for survivalin patients with metastatic renal cell carcinoma. J Exp Clin CancerRes 2009;28:30.
[5] Rickles FR, Patierno S, Fernandez PM. Tissue factor, thrombin, andcancer. Chest 2003;124:58S–68S.
[6] Versteeg HH, Peppelenbosch MP, Spek CA. Tissue factor signaltransduction in angiogenesis. Carcinogenesis 2003;24:1009–13.
[7] Wojtukiewicz MZ, Zacharski LR, Memoli VA, et al. Fibrinogen-fibrin transformation in situ in renal cell carcinoma. Anticancer Res1990;10:579–82.
[8] Palumbo JS, Kombrinck KW, Drew AF, et al. Fibrinogen is animportant determinant of the metastatic potential of circulating tumorcells. Blood 2000;96:3302–9.
[9] Palumbo JS, Potter JM, Kaplan LS, Talmage K, Jackson DG, DegenJL. Spontaneous hematogenous and lymphatic metastasis, but notprimary tumor growth or angiogenesis, is diminished in fibrinogen-deficient mice. Cancer Res 2002;62:6966–72.
[10] Staton CA, Brown NJ, Lewis CE. The role of fibrinogen and relatedfragments in tumour angiogenesis and metastasis. Expert Opin BiolTher 2003;3:1105–20.
[11] Xiao B, Ma LL, Zhang SD, et al. Correlation between coagulationfunction, tumor stage and metastasis in patients with renal cellcarcinoma: a retrospective study. Chin Med J (Engl) 2011;124:1205–8.
[12] Du J, Zheng JH, Chen XS, et al. High preoperative plasma fibrinogenis an independent predictor of distant metastasis and poor prognosisinrenal cell carcinoma. Int J Clin Oncol 2013;18:517–23.
[13] Pichler M, Hutterer GC, Stojakovic T, Mannweiler S, Pummer K,Zigeuner R. High plasma fibrinogen level represents an independentnegative prognostic factor regarding cancer-specific, metastasis-free, as well as overall survival in a European cohort of non-metastatic renal cell carcinoma patients. Br J Cancer 2013;109:1123–9.
[14] Arpaia G, Carpenedo M, Verga M, et al. D-dimer before chemo-therapy might predict venous thromboembolism. Blood CoagulFibrinolysis 2009;20:170–5.
[15] Harrison KA, Haire WD, Pappas AA, et al. Plasma D-dimer: a usefultool for evaluating suspected pulmonary embolus. J Nucl Med1993;34:896–8.
[16] Dirix LY, Salgado R, Weytjens R, et al. Plasma fibrin D-dimerlevels correlate with tumour volume, progression rate and survivalin patients with metastatic breast cancer. Br J Cancer 2002;86:389–95.
[17] Yamamoto M, Yoshinaga K, Matsuyama A, et al. Plasma D-dimerlevel as a mortality predictor in patients with advanced or recurrentcolorectal cancer. Oncology 2012;83:10–5.
[18] Zhang PP, Sun JW, Wang XY, Liu XM, Li K. Preoperative plasma D-dimer levels predict survival in patients with operable non-small celllung cancer independently of venous thromboembolism. Eur J SurgOncol 2013;39:951–6.
[19] Diao D, Zhu K, Wang Z, et al. Prognostic value of the D-dimer test inoesophageal cancer during the perioperative period. J Surg Oncol2013 Jul;108:34–41.
[20] Furie B, Furie BC. The molecular basis of blood coagulation. Cell1988;53:505–18.
[21] Shoji M, Hancock WW, Abe K, et al. Activation of coagulation andangiogenesis in cancer: immunohistochemical localization in situ ofclotting proteins and vascular endothelial growth factor in humancancer. Am J Pathol 1998;152:399–411.
[22] Belting M, Ahamed J, Ruf W. Signaling of the tissue factorcoagulation pathway in angiogenesis and cancer. Arterioscler ThrombVasc Biol 2005;25:1545–50.
[23] Mueller BM, Ruf W. Requirement for binding of catalytically activefactor VIIa in tissue factor-dependent experimental metastasis. J ClinInvest 1998;101:1372–8.
[24] Bjork I, Olson ST. Anti-thrombin. A bloody important serpin.AdvExp Med Biol 1997;425:17–33.
[25] O'Reilly MS, Pirie-Shepherd S, Lane WS, Folkman J. Anti-angiogenic activity of the cleaved conformation of the serpin anti-thrombin. Science 1999;285:1926–8.
[26] Larsson H, Sjoblom T, Dixelius J, et al. Anti-angiogenic effects oflatent anti-thrombin through perturbed cell-matrix interactions andapoptosis of endothelial cells. Cancer Res 2000;60:6723–9.
[27] AJCC Staging Manual, Edge SB, Byrd DR, Comptom CC et al.editors. 7th ed Philadelphia: Springer 2009.
[28] Sahni A, Francis CW. Vascular endothelial growth factor bindsto fibrinogen and fibrin and stimulates endothelial cell proliferation.Blood 2000;96:3772–8.
[29] Dvorak HF, Nagy JA, Berse B, et al. Vascular permeabilityfactor, fibrin, and the pathogenesis of tumor stroma formation. AnnN Y Acad Sci 1992;667:101–11.
[30] Hembrough TA, Swartz GM, Papathanassiu A, et al. Tissue factor/factor VIIa inhibitors block angiogenesis and tumor growth through anonhemostatic mechanism. Cancer Res 2003;63:2997–3000.
[31] Verheul HM, van Erp K, Homs MY, et al. The relationship ofvascular endothelial growth factor and coagulation factor (fibrin and

S. Erdem et al. / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–1010
fibrinogen) expression in clear cell renal cell carcinoma. Urology2010;75:608–14.
[32] Nieswandt B, Hafner M, Echtenacher B, Mannel DN. Lysis of tumorcells by natural killer cells in mice is impeded by platelets. CancerRes 1999;59:1295–300.
[33] Yamashita H, Kitayama J, Kanno N, Yatomi Y, Nagawa H. Hyper-fibrinogenemia is associated with lymphatic as well as hematogenousmetastasis and worse clinical outcome in T2 gastric cancer. BMCCancer 2006;6:147.
[34] Tang L, Liu K, Wang J, Wang C, Zhao P, Liu J. High preoperativeplasma fibrinogen levels are associated with distant metastases andimpaired prognosis after curative resection in patients with colorectalcancer. J Surg Oncol 2010;102:428–32.
[35] Takeuchi H, Ikeuchi S, Kitagawa Y, et al. Pretreatment plasmafibrinogen level correlates with tumor progression and metastasis inpatients with squamous cell carcinoma of the esophagus. J Gastro-enterol Hepatol 2007;22:2222–7.
[36] Guo Q, Zhang B, Dong X, et al. Elevated levels of plasma fibrinogenin patients with pancreatic cancer: possible role of a distant metastasispredictor. Pancreas 2009;38:e75–9.
[37] Polterauer S, Grimm C, Seebacher V, et al. Plasma fibrinogen levelsand prognosis in patients with ovarian cancer: a multicenter study.Oncologist 2009;14:979–85.
[38] Seebacher V, Polterauer S, Grimm C, et al. The prognostic value ofplasma fibrinogen levels in patients with endometrial cancer: a multi-centre trial. Br J Cancer 2010;102:952–6.
[39] Casamassima A, Picciariello M, Quaranta M, et al. C-reactive protein:a biomarker of survival in patients with metastatic renal cellcarcinoma treated with subcutaneous interleukin-2 based immuno-therapy. J Urol 2005;173:52–5.
[40] Kattan MW, Reuter V, Motzer RJ, et al. A postoperativeprognostic nomogram for renal cell carcinoma. J Urol 2001;166:63–7.
[41] Frank I, Blute ML, Cheville JC, et al. An outcome prediction modelfor patients with clear cell renal cell carcinoma treated with radicalnephrectomy based on tumor stage, size, grade and necrosis: theSSIGN score. J Urol 2002;168:2395–400.
[42] Cindolo L, de la Taille A, Messina G, et al. A preoperative clinicalprognostic model for non-metastatic renal cell carcinoma. BJU Int2003;92:901–5.
[43] Raj GV, Thompson RH, Leibovich BC, et al. Preoperative nomogrampredicting 12-year probability of metastatic renal cancer. J Urol2008;179:2146–51:[discussion 2151].
[44] Karakiewicz PI, Suardi N, Capitanio U, et al. A preoperativeprognostic model for patients treated with nephrectomy for renal cellcarcinoma. Eur Urol 2009;55:287–95.