independent assessment committee report constituted under ... · hospital agreement between the...
TRANSCRIPT
1
IndependentAssessmentCommitteeReport
ConstitutedunderArticle8.01ofthe
CollectiveAgreement
Between
HumberRiverHospital
And
OntarioNurses’Association
June12,2016
2
June12,20162016Ms.SusanBlairOntarioNursesAssociationProfessionalPracticeSpecialistOntarioNurses'Association85GrenvilleStreet,Suite400Toronto,Ontario,M5S3A2Ms.MargCzausChiefNursingExecutiveHumberRiverHospital1235WilsonAve.Toronto,ON,M3M0B2DearMs.BlairandMs.Czaus,ThemembersoftheIndependentAssessmentCommitteehaveconcludedourreviewandrespectfullysubmittheReportoftheIndependentAssessmentCommitteethatwasconstitutedunderArticle8.01ofthecollectiveagreementbetweenHumberRiverHospitalandtheOntarioNursesAssociation.ThisreportcontainstheIndependentAssessmentCommittee’sfindingsandrecommendationsregardingtheProfessionalWorkloadComplaintsubmittedbyNursesfromtheHemodialysisUnitatHumberRiverHospital.TheprocessundertakenthroughanIndependentAssessmentCommitteeprovidesauniqueopportunityfordiscussionanddialoguebetweenallthepartiesregardingthecomplexissuesandconditionsthatunderlieaProfessionalWorkloadComplaint.TheCommitteehasmade18recommendationsinfiveareasregardingissuesthatimpacttheworkloadofRegisteredNurses.TheMembersoftheIndependentAssessmentCommitteeunanimouslysupportallrecommendationsinthisreport.TheCommitteehopesthattherecommendationswillassisttheHospitalandtheAssociationtofindmutuallyagreeableresolutionswithregardtonursingworkloadissuesintheHemodialysisUnit.
3

4
5
TableofContents
1. Introduction.......................................................................................................................................71.1.OrganizationoftheIndependentAssessmentCommitteeReport.................................................71.2.ReferraltotheIndependentAssessmentCommittee......................................................................71.3.JurisdictionoftheIndependentAssessmentCommittee.................................................................81.4.ProceedingsoftheIndependentAssessmentCommittee............................................................12Pre-Hearing................................................................................................................................12Hearing......................................................................................................................................14PostClosureofHearing..............................................................................................................16
2. PresentationoftheProfessionalResponsibilityWorkloadComplaint.................................172.1 InformationonHumberRiverHospitalandtheHemodialysisUnit............................................172.2 HistoryofStaffinginHemodialysisUnitsince2011.......................................................................172.2.1 Staffingin2011...............................................................................................................172.2.2 StaffingChangesfrom2011-2013....................................................................................182.2.3 StaffingChangesin2013/2014........................................................................................192.2.4 StaffingChangesin2015/2016........................................................................................192.2.5 CurrentStaffing...............................................................................................................202.3 WorkloadConcernsofRegisteredNursesandDiscussionsattheHospitalAssociationCommittee.....................................................................................................................................................212.4 MeetingsbetweenAssociationandHospitalPriortoIAC...................................................24
3 Discussion,AnalysisandRecommendations..............................................................................263.1 RegisteredNurseStaffingandSchedulingToEnsureAdequateandSafeRNStaffing.............263.2 PatientVolumes,TypesofTreatmentandScheduling..................................................................313.3 Documentation.....................................................................................................................................323.4 CommunicationandDecisionMaking..............................................................................................323.5 ProcessforManagementofProfessionalResponsibilityWorkloadReportForm(PRWRFs)..333.6 Recommendations:..............................................................................................................................33
4. Conclusion.......................................................................................................................................35

6
AppendicesAppendix1:LetterfromAssociationApril30,2014
Appendix2:EmployerGrievanceJune12,2014
Appendix3:LetterfromHospitalLegalCounselSeptember12,2014
Appendix4:LetterfromLegalCounselforAssociationSeptember25,2014
Appendix5:LetterfromLegalCounselforHospitalOctober4,2014
Appendix6:LetterfromIACChairOctober142014
Appendix7:LetterfromLegalCounselforAssociationOctober21,2014
Appendix8:LetterfromLegalCounselforHospitalOctober23,2014
Appendix9:LetterfromIACChairNovember4,2014
Appendix10:AgendaforIAC
Appendix11:InformationRequesttoHospital
Appendix12:AttendeesatIAC
Appendix13:RNandRPNStaffinginHemodialysisUnitinApril2016(MondaytoFriday)
Appendix14:RNandRPNStaffinginHemodialysisUnitinApril2016(SaturdayandSunday)
7
1. Introduction
1.1. OrganizationoftheIndependentAssessmentCommitteeReport
TheIndependentAssessmentCommittee(IAC)Reportispresentedinfiveparts:
1. IntroductionThissectionoutlinesthereferraloftheProfessionalWorkloadComplainttotheIAC,reviewstheIAC’s jurisdiction as outlined in the Collective Agreement, and summarizes the Pre-Hearing,HearingandPost-Hearingprocesses.2. PresentationoftheProfessionalResponsibilityWorkloadComplaintThissectionpresentsthecontextofpracticerelatingtotheprofessionalworkloadcomplaintintheHemodialysisUnitatHumberRiverHospital;summarizestherelevanthistoryleadingtothereferraloftheprofessionalworkloadcomplainttotheIAC;andreviewsthepresentationsbytheOntario Nurses’ Association (‘the Association’), Humber River Hospital (‘the Hospital’) at theHearing.3. Discussion,AnalysisandRecommendations4. SummaryandConclusions5. ReferencesandAppendices
ThesubmissionsandexhibitsoftheOntarioNurses’AssociationandHumberRiverHospitalareonfilewithbothparties.
1.2. ReferraltotheIndependentAssessmentCommittee
ThisReportaddressestheprofessionalworkloadcomplaintsofRegisteredNursesfromtheHemodialysisUnitatHumberRiverHospital.TheAssociationstatedthefollowingintheirpre-hearingsubmission:

8
“ONA submits this Professional Responsibility Complaint to be the result of the employer, assigning ahigh number of patients to individual RNs and groups of RNs. As perArticle 8 of theHospital CentralAgreementRNshavesubmitted180PRWRFstodocumentwhenhavebeenaskedtoperformmoreworkthanisconsistentwithpatientcare.”1
1.3. JurisdictionoftheIndependentAssessmentCommittee
The IAC is convened under the authority of Article 8.01 on Professional Responsibility in the CentralHospitalAgreementbetweentheOntarioNurses’AssociationandHumberRiverHospital.Article8.01states:2
8.01 The parties agree that patient care is enhanced if concerns relating to professional practice,
patient acuity, fluctuating workloads and fluctuating staffing are resolved in a timely andeffectivemanner.IntheeventthattheHospitalassignsanumberofpatientsoraworkloadtoanindividualnurseorgroupofnurses such that theyhave cause tobelieve that theyarebeingasked toperformmoreworkthanisconsistentwithproperpatientcare,theyshall
i) atthetimetheworkload issueoccurs,discussthe issuewithintheunit/programtodevelop
strategiestomeetpatientcareneedsusingcurrentresourcesii) If necessary, using established lines of communication as identified by the hospital, seek
immediateassistancefromanindividual(s)(whocouldbewithinthebargainingunit)whohasresponsibilityfortimelyresolutionofworkloadissues.
iii) Failingresolutionoftheworkloadissueatthetimeofoccurrenceoriftheissueisongoingthenurse(s)willdiscusstheissuewithherorhisManagerordesignateonthenextdaythattheManager (or designate) and the nurse are both working or within five (5) calendar dayswhichever is sooner. Complete the ONA/Hospital professional Responsibility WorkloadReport Form. The manager (or designate) will provide a written response on the
1SubmissiontotheIndependentAssessmentCommitteebyOntarioNurses’Association,2016,p.62CollectiveAgreementBetweentheHospitalandOntarioNurses’Association,Article8–ProfessionalResponsibility,March31,2014,p.23.
(a)
9
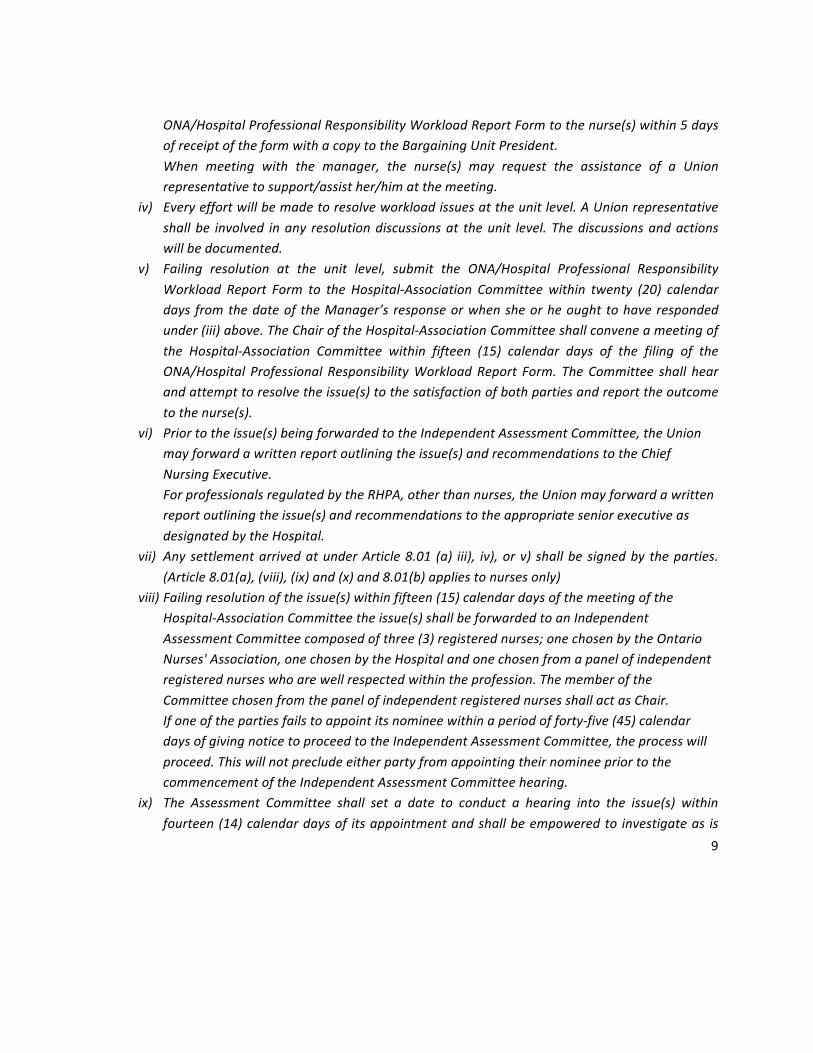
ONA/HospitalProfessionalResponsibilityWorkloadReportFormtothenurse(s)within5daysofreceiptoftheformwithacopytotheBargainingUnitPresident.When meeting with the manager, the nurse(s) may request the assistance of a Unionrepresentativetosupport/assisther/himatthemeeting.
iv) Everyeffortwillbemadetoresolveworkloadissuesattheunitlevel.AUnionrepresentativeshallbe involved inany resolutiondiscussionsat theunit level. Thediscussionsandactionswillbedocumented.
v) Failing resolution at the unit level, submit the ONA/Hospital Professional ResponsibilityWorkload Report Form to the Hospital-Association Committeewithin twenty (20) calendardays fromthedateof theManager’s responseorwhensheorheought tohaverespondedunder(iii)above.TheChairoftheHospital-AssociationCommitteeshallconveneameetingofthe Hospital-Association Committee within fifteen (15) calendar days of the filing of theONA/Hospital Professional ResponsibilityWorkloadReport Form. TheCommittee shall hearandattempttoresolvetheissue(s)tothesatisfactionofbothpartiesandreporttheoutcometothenurse(s).
vi) Priortotheissue(s)beingforwardedtotheIndependentAssessmentCommittee,theUnionmayforwardawrittenreportoutliningtheissue(s)andrecommendationstotheChiefNursingExecutive.ForprofessionalsregulatedbytheRHPA,otherthannurses,theUnionmayforwardawrittenreportoutliningtheissue(s)andrecommendationstotheappropriateseniorexecutiveasdesignatedbytheHospital.
vii) AnysettlementarrivedatunderArticle8.01 (a) iii), iv),orv) shallbesignedby theparties.(Article8.01(a),(viii),(ix)and(x)and8.01(b)appliestonursesonly)
viii) Failingresolutionoftheissue(s)withinfifteen(15)calendardaysofthemeetingoftheHospital-AssociationCommitteetheissue(s)shallbeforwardedtoanIndependentAssessmentCommitteecomposedofthree(3)registerednurses;onechosenbytheOntarioNurses'Association,onechosenbytheHospitalandonechosenfromapanelofindependentregisterednurseswhoarewellrespectedwithintheprofession.ThememberoftheCommitteechosenfromthepanelofindependentregisterednursesshallactasChair.Ifoneofthepartiesfailstoappointitsnomineewithinaperiodofforty-five(45)calendardaysofgivingnoticetoproceedtotheIndependentAssessmentCommittee,theprocesswillproceed.ThiswillnotprecludeeitherpartyfromappointingtheirnomineepriortothecommencementoftheIndependentAssessmentCommitteehearing.
ix) The Assessment Committee shall set a date to conduct a hearing into the issue(s) withinfourteen(14)calendardaysof itsappointmentandshallbeempoweredto investigateas is
10
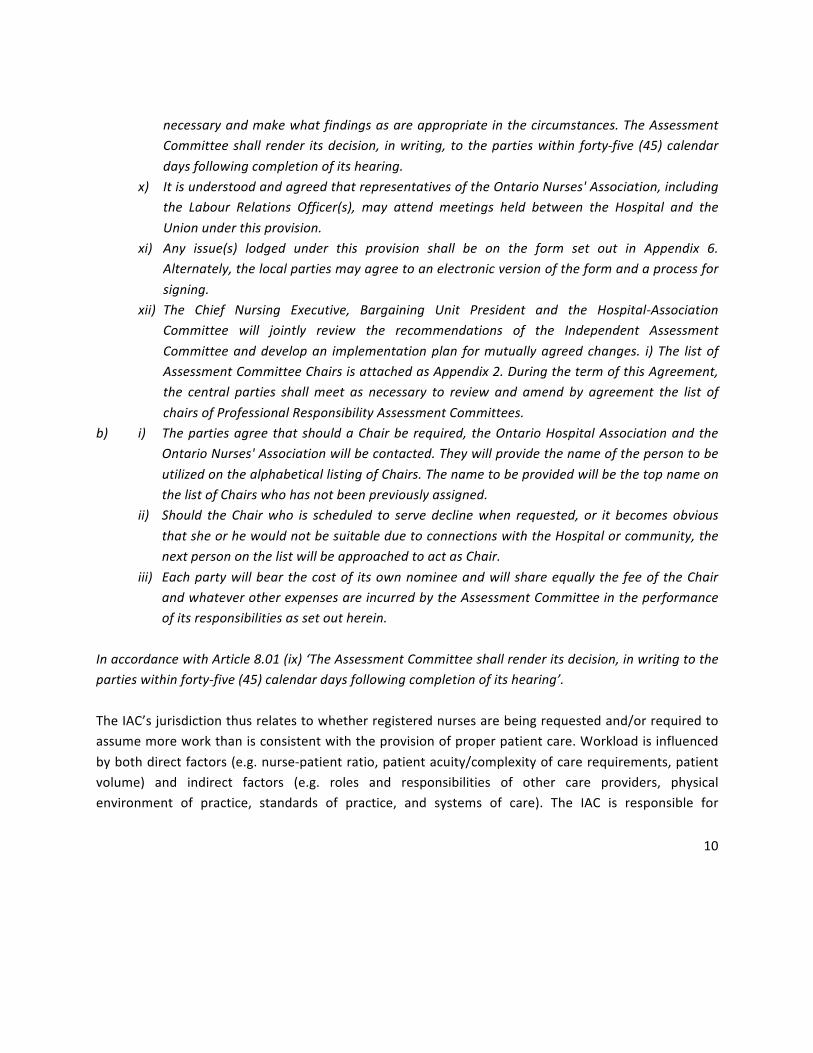
necessaryandmakewhatfindingsasareappropriateinthecircumstances.TheAssessmentCommitteeshall render itsdecision, inwriting, to thepartieswithin forty-five (45)calendardaysfollowingcompletionofitshearing.
x) ItisunderstoodandagreedthatrepresentativesoftheOntarioNurses'Association,includingthe Labour Relations Officer(s), may attend meetings held between the Hospital and theUnionunderthisprovision.
xi) Any issue(s) lodged under this provision shall be on the form set out in Appendix 6.Alternately,thelocalpartiesmayagreetoanelectronicversionoftheformandaprocessforsigning.
xii) The Chief Nursing Executive, Bargaining Unit President and the Hospital-AssociationCommittee will jointly review the recommendations of the Independent AssessmentCommitteeanddevelopan implementationplan formutuallyagreedchanges. i) The listofAssessmentCommitteeChairsisattachedasAppendix2.DuringthetermofthisAgreement,the central parties shallmeet as necessary to review and amend by agreement the list ofchairsofProfessionalResponsibilityAssessmentCommittees.
b) i) Thepartiesagree thatshouldaChairbe required, theOntarioHospitalAssociationandtheOntarioNurses'Associationwillbecontacted.TheywillprovidethenameofthepersontobeutilizedonthealphabeticallistingofChairs.ThenametobeprovidedwillbethetopnameonthelistofChairswhohasnotbeenpreviouslyassigned.
ii) Should the Chairwho is scheduled to serve declinewhen requested, or it becomes obviousthatsheorhewouldnotbesuitableduetoconnectionswiththeHospitalorcommunity,thenextpersononthelistwillbeapproachedtoactasChair.
iii) Eachpartywillbear thecostof itsownnomineeandwill shareequally the feeof theChairandwhateverotherexpensesareincurredbytheAssessmentCommitteeintheperformanceofitsresponsibilitiesassetoutherein.
InaccordancewithArticle8.01(ix)‘TheAssessmentCommitteeshallrenderitsdecision,inwritingtothepartieswithinforty-five(45)calendardaysfollowingcompletionofitshearing’.
TheIAC’sjurisdictionthusrelatestowhetherregisterednursesarebeingrequestedand/orrequiredtoassumemoreworkthanisconsistentwiththeprovisionofproperpatientcare.Workloadisinfluencedbybothdirectfactors(e.g.nurse-patientratio,patientacuity/complexityofcarerequirements,patientvolume) and indirect factors (e.g. roles and responsibilities of other care providers, physicalenvironment of practice, standards of practice, and systems of care). The IAC is responsible for

11
examining factors impactingworkload, and formaking recommendations to addressworkload issues.ConcernsoutsideofworkloadarebeyondthejurisdictionoftheIAC.In thematter of arbitration between Brantford General Hospital and the Ontario Nurses Associationboth parties acknowledged that while according to the collective agreement the IAC’s report is notbindingupontheparties,“thepartiesstressedto theboardthat theassociationandtheparticipatinghospitalsallfeelboundbythefindingsofsuchcommittees.”3TheIAC’sjurisdictionceaseswithsubmissionofitswrittenReport.Thefindingsandrecommendationsofthe IAC provide an independent external perspective to assist the Association and the Hospital toachievemutuallyagreeableresolutionstoworkloadissues.TheIACisnotanadjudicativepanel,anditsrecommendations are not binding. In accordance with Professional Responsibility Article 8 of theCollectiveAgreement,theIACwascomprisedofthreeRegisteredNurses.ThemembersoftheIndependentAssessmentCommitteewere:ChairpersonLeslieVincentFortheAssociationAngelaPreocaninFortheHospitalSylviaRodgers
3ArbitrationHearingBrantfordGeneralHospitalandOntarioNursesAssocation,September8,1986.

12
1.4. ProceedingsoftheIndependentAssessmentCommittee
Pre-Hearing
OnApril30,2014theAssociationnotifiedtheHospitalandtheIACChairinaletterthattheAssociationwas confirming an Independent Assessment Committee to investigate a complaint at Humber RiverHospitalandconfirmingtheChairasLeslieVincent,theAssociationnominee,AngelaPreocanin;andtheHospitalNominee,TrevaMcCumber.(Appendix1).TheIACmembersmetbyteleconferenceonMay21,2014anddiscussedthefollowingissues:
• OverviewoftheIACprocessandtimeframes;• ProposeddatesfortheIAC;• InformationrequirementsforthecommitteetoassistintheIAC’sprocessanddeliberations.
OnMay28,2014 the IACproposed to theHospitaland theAssociation that the IACbescheduled forNovember24-26,2014.TheAssociationagreedtothesedates,buttheHospitaldidnotreplyregardingtheiravailability.OnJune12,2014theHospitalfiledanEmployergrievance,statingthattheAssociationhadviolatedthecollectiveagreementarticles1,6and8.(Appendix2).OnJuly28,2014theIACchairagainaskedbothpartiesfortheiravailabilitytoholdtheIAConNovember24-26,2014. TheAssociationagreed;butnoresponsewasreceivedfromtheHospital.OnSeptember12,2014theIACchairrequestedthatbothpartiessubmittheirbriefstotheIACbyOctober31,2014.OnSeptember12,theHospital’s legalcounselsentalettertotheIACchairrequestingthattheIACbeadjourned until the grievance filed on June 12, 2014 has been properly resolved through arbitration.(Appendix3)OnSeptember25,thelegalcounselfortheAssociationsentalettertotheIACchairaskingthattheIACproceedonNovember24,2014.(Appendix4)On October 4 2014, legal counsel for the Hospital sent a letter to the IAC chair stating theirdisagreementwith the position byONA that the IAC should proceed, and stating their view that thegrievancebeheardpriortotheIAC.(Appendix5)
13
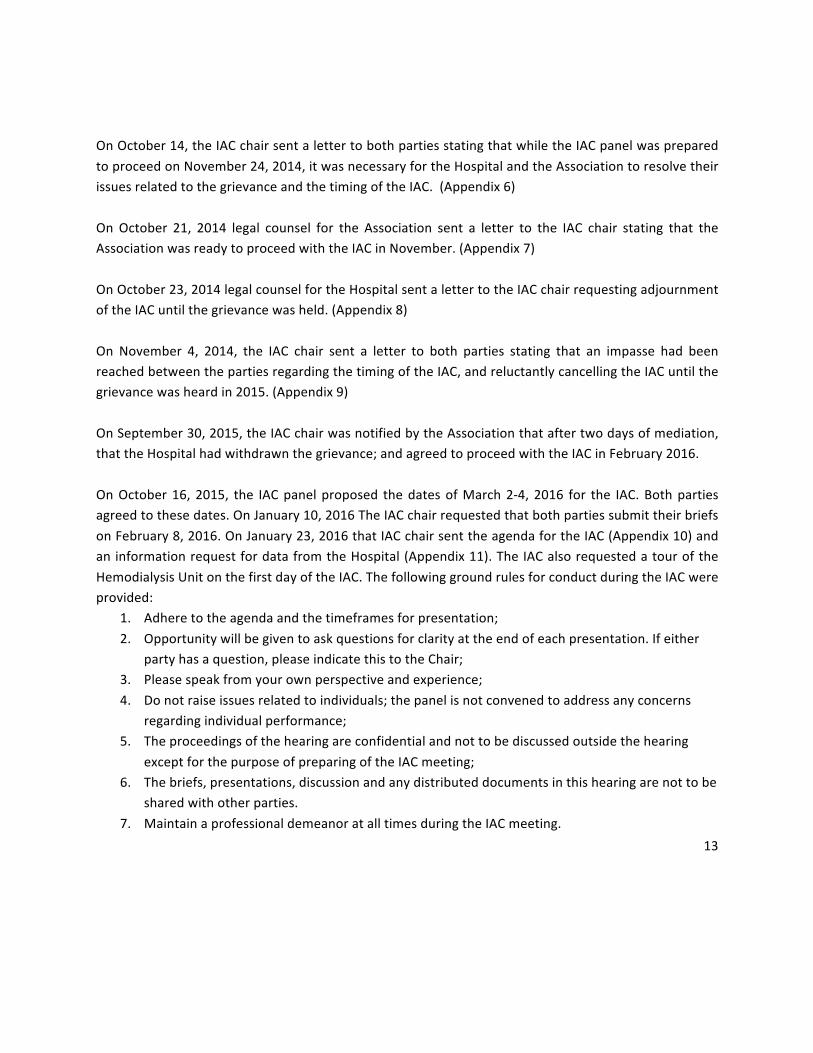
OnOctober14,theIACchairsentalettertobothpartiesstatingthatwhiletheIACpanelwaspreparedtoproceedonNovember24,2014,itwasnecessaryfortheHospitalandtheAssociationtoresolvetheirissuesrelatedtothegrievanceandthetimingoftheIAC.(Appendix6)OnOctober 21, 2014 legal counsel for the Association sent a letter to the IAC chair stating that theAssociationwasreadytoproceedwiththeIACinNovember.(Appendix7)OnOctober23,2014legalcounselfortheHospitalsentalettertotheIACchairrequestingadjournmentoftheIACuntilthegrievancewasheld.(Appendix8)On November 4, 2014, the IAC chair sent a letter to both parties stating that an impasse had beenreachedbetweenthepartiesregardingthetimingoftheIAC,andreluctantlycancellingtheIACuntilthegrievancewasheardin2015.(Appendix9)OnSeptember30,2015,theIACchairwasnotifiedbytheAssociationthataftertwodaysofmediation,thattheHospitalhadwithdrawnthegrievance;andagreedtoproceedwiththeIACinFebruary2016.OnOctober16, 2015, the IACpanelproposed thedatesofMarch2-4, 2016 for the IAC.Bothpartiesagreedtothesedates.OnJanuary10,2016TheIACchairrequestedthatbothpartiessubmittheirbriefsonFebruary8,2016.OnJanuary23,2016thatIACchairsenttheagendafortheIAC(Appendix10)andaninformationrequestfordatafromtheHospital(Appendix11).TheIACalsorequestedatouroftheHemodialysisUnitonthefirstdayoftheIAC.ThefollowinggroundrulesforconductduringtheIACwereprovided:
1. Adheretotheagendaandthetimeframesforpresentation;2. Opportunitywillbegiventoaskquestionsforclarityattheendofeachpresentation.Ifeither
partyhasaquestion,pleaseindicatethistotheChair;3. Pleasespeakfromyourownperspectiveandexperience;4. Donotraiseissuesrelatedtoindividuals;thepanelisnotconvenedtoaddressanyconcerns
regardingindividualperformance;5. Theproceedingsofthehearingareconfidentialandnottobediscussedoutsidethehearing
exceptforthepurposeofpreparingoftheIACmeeting;6. Thebriefs,presentations,discussionandanydistributeddocumentsinthishearingarenottobe
sharedwithotherparties.7. MaintainaprofessionaldemeanoratalltimesduringtheIACmeeting.
14
On February 22, 2016, the IAC met in preparation for the IAC meeting and to review the briefssubmittedbybothparties.OnFebruary25,2015, the IACchairwasnotifiedbytheHospitalnominee,TrevaMcCumber, thatshewasunfortunatelyunabletobepresentattheIAConMarch2-4.DespiteeffortsbytheHospitaltofindanalternatenominee,theIACwascancelledandrescheduledforMarch29-31,2016.ThenewnomineenamedbytheHospitalwasSylviaRodgers.OnMarch 28, 2016 the IAC chair was notified that the Hospital nominee was unable to attend theMarch 29-31, 2016 IAC due to family issues. The IAC was subsequently rescheduled for April 20-22,2016.ThepanelmetinpreparationfortheIAConApril20,2016priortothetouroftheHemodialysisunit.Priortothehearing,bothpartiesconfirmedwhowouldbeinattendanceatthehearing.
Hearing
Wednesday,April202016TheIACmetattheHospitalat1000HoursonMarch29,2016andweregreetedbyrepresentativesofthe Hospital and members of the Association. The IAC was provided with an extensive tour of theHemodialysisunit.ThetourservedtofamiliarizetheIACwiththeworkenvironmentandphysicallayoutoftheunit.ThefollowingindividualsfromtheHospitalwereonthetour:
• MelanieTremblay,Director,NephrologyProgram• DilshadPirani,Manager,Nephrology• JenniferDuteau,ClinicalPracticeLeader
ThefollowingindividualsfromtheAssociationwereonthetour:
• AnneGibb,RNHemodialysis• ElizabethAstillero,RNHemodialysis• MarianaMarkovic,ProfessionalPracticeSpecialist,LabourRelationsOfficer,ONA

15
Followingabreak,TheIAChearingconvenedat1300houraspertheagenda(Appendix10).ParticipantsandObserversontherespectivehearingdatesarelistedinAppendix12.Following introductionoftheIACCommitteemembersandrepresentativesoftheAssociationandtheHospital,theIACChairreviewed:
• ThejurisdictionalscopeoftheIAC,includingthepurposeoftheIAC;and• The ground rules for the Hearing procedure including confirmation that all participants
understoodandagreed.Ms.MarianaMarkovic, Professional Practice Specialist (PPS), presented on behalf of the Association.The Association’s presentation was based on their written Pre-hearing submission and supportingexhibitsaswellasasummaryofthe187ProfessionalResponsibilityWorkloadReportForms(PRWRFs)submittedbytheRegisteredNursesoftheHemodialysisUnitbetween2011and2016.Melanie Tremblay, Director of the Nephrology Program; Dilshad Pirani, Manager of the NephrologyProgram; and Jennifer Duteau, Clinical Practice Leader presented on behalf of the Hospital. TheHospital’spresentationwasbasedontheirwrittenpre-hearingsubmissionandsupportingexhibits.ThursdayApril21,2016TheIACChairresumedtheHearingat0900hours.MelanieTremblay,DilshadPiraniandJenniferDuteauprovidedtheHospital’sresponsetotheAssociation’ssubmission.MembersoftheHospitalparticipatedin the subsequent discussion. Ms. Markovic provided the Association’s response to the Hospital’ssubmission.OthermembersoftheAssociationalsoparticipatedinthesubsequentdiscussion.The IAC Chair adjourned the Hearing at approximately 1730 hours. Following adjournment of theHearing, the IACmet during the evening to review and synthesize the information provided, and toidentifykeyissuesrequiringadditionalclarificationandtheirrespectivequestionsforthefinaldayofthehearing.

16
Friday,April22,2016TheIACchairresumedthemeetingat0900hr.MembersoftheIACaskedfurtherquestionsinordertounderstanda rangeof issues inmoredetailandgaining furtherclarityof the issuesarising frombothparties’presentations.The IACChairconcludedthehearingbythankingMs.AngelaPreocanin,AssociationNomineeandMs.SylviaRodgersHospitalNominee;aswellasalltheparticipantsfortheirengagementandcontributionsintheHearingprocess.TheIACChairalsocommunicatedthehopethatthepartieswillbeabletomoveforward to seek resolution to the issues. The Chair also confirmed that IAC anticipated providing thefinalreportwithin45days.TheIACChairclosedtheHearingatapproximately1300hours.
PostClosureofHearing
TheIACmetinpersononMay2,2016.Atthismeeting,theIAChadextensivediscussionandreviewedthedraftreportandanalysis.Followingthemeeting,allIACmemberscontributedtothenextversionofthereportandrecommendations.ThereportwasfinalizedonJune2,2016.
17
2. PresentationoftheProfessionalResponsibilityWorkloadComplaint
2.1 InformationonHumberRiverHospitalandtheHemodialysisUnit
The Hemodialysis Unit at Humber River Hospital (HRH) is located in Toronto, Ontario. Humber RiverHospital isaregionalacutecarehospitalandservesacatchmentareaofmorethan850,000peopleinthe northwest Greater Toronto Area. In October 2015 the HRH moved into a new hospital at 1235Wilson Ave. in Toronto. The hospital has approximately 650 beds, employs approximately 3400employeesincluding1200RegisteredNurses(RNs)and300RegisteredPracticalNurses(RPNs).TheHemodialysisIn-CentreUnitisdividedintotheeastandwestwingswith61dialysisstations.Thereis a central patient care station in eachwingwith views of all dialysis stations. The unit services 350patients. There is an interprofessional team includingRNs,RPNs,physicians, socialworkers,dieticiansandpharmacists.Theunitoperates7daysaweek from0700-2300,with24-houroncall coverage foremergencytreatments.Onweekends,onlyhalftheunitisopen.Threetypesofservicesareprovided:
• Conventionalhemodialysis:4hourtreatments,3timesaweek• Shortdailyhemodialysis:patientsreceiving2-3hourtreatments,5-7timesperweek• AcutedialysisisperformedintheICU,Emergency,CardiacCareandin-patientunits
MostpatientsreceivetheirtreatmentintheIn-Centrewithexceptionofthosepatientsthataretooilltobemovedtothecentrefromtheirunitofcare.
2.2 HistoryofStaffinginHemodialysisUnitsince2011
2.2.1 Staffingin2011
In2011,theHemodialysisUnitwaslocatedattheChurchStreetSiteofHumberRiverHospital.Theunithadtwowingswithatotalof61dialysisstations.Staffing:• TwoChargeNursesondaysandtwoonevenings; theChargeNurseshavenopatientassignment,
buttakeoneifnecessary
18
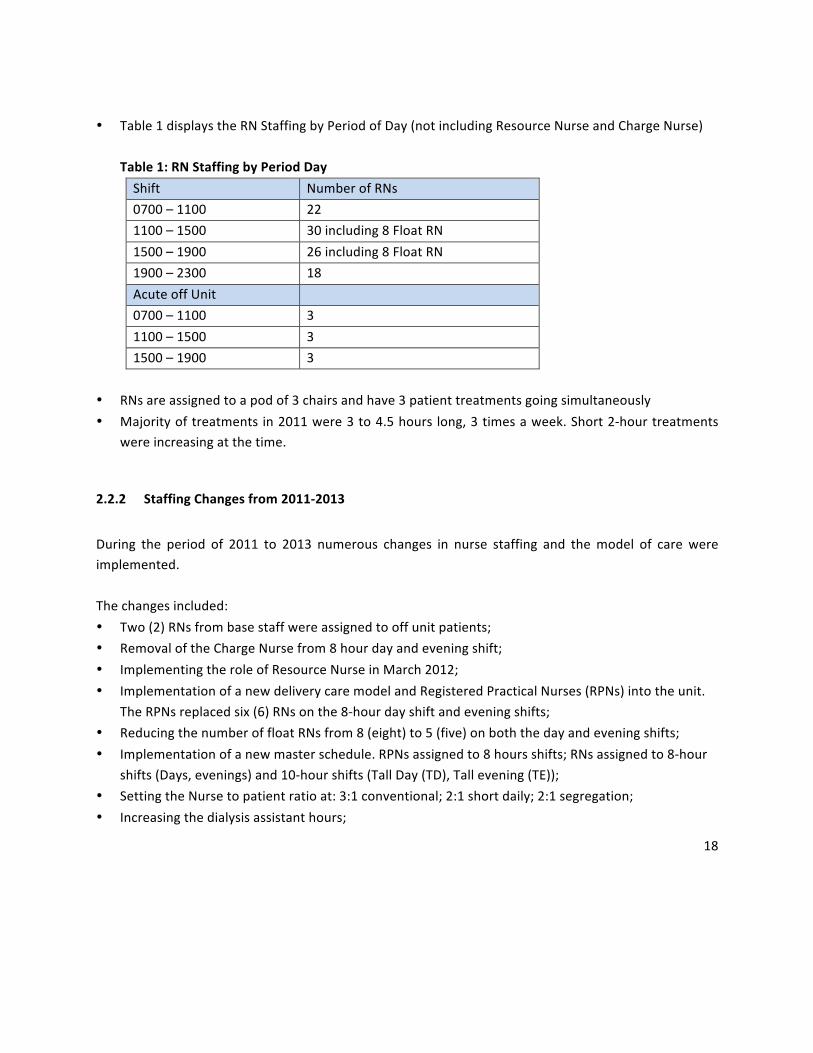
• Table1displaystheRNStaffingbyPeriodofDay(notincludingResourceNurseandChargeNurse)Table1:RNStaffingbyPeriodDayShift NumberofRNs0700–1100 221100–1500 30including8FloatRN1500–1900 26including8FloatRN1900–2300 18AcuteoffUnit 0700–1100 31100–1500 31500–1900 3
• RNsareassignedtoapodof3chairsandhave3patienttreatmentsgoingsimultaneously• Majorityoftreatmentsin2011were3to4.5hours long,3timesaweek.Short2-hourtreatments
wereincreasingatthetime.
2.2.2 StaffingChangesfrom2011-2013
During the period of 2011 to 2013 numerous changes in nurse staffing and themodel of care wereimplemented.Thechangesincluded:• Two(2)RNsfrombasestaffwereassignedtooffunitpatients;• RemovaloftheChargeNursefrom8hourdayandeveningshift;• ImplementingtheroleofResourceNurseinMarch2012;• ImplementationofanewdeliverycaremodelandRegisteredPracticalNurses(RPNs)intotheunit.
TheRPNsreplacedsix(6)RNsonthe8-hourdayshiftandeveningshifts;• ReducingthenumberoffloatRNsfrom8(eight)to5(five)onboththedayandeveningshifts;• Implementationofanewmasterschedule.RPNsassignedto8hoursshifts;RNsassignedto8-hour
shifts(Days,evenings)and10-hourshifts(TallDay(TD),Tallevening(TE));• SettingtheNursetopatientratioat:3:1conventional;2:1shortdaily;2:1segregation;• Increasingthedialysisassistanthours;
19
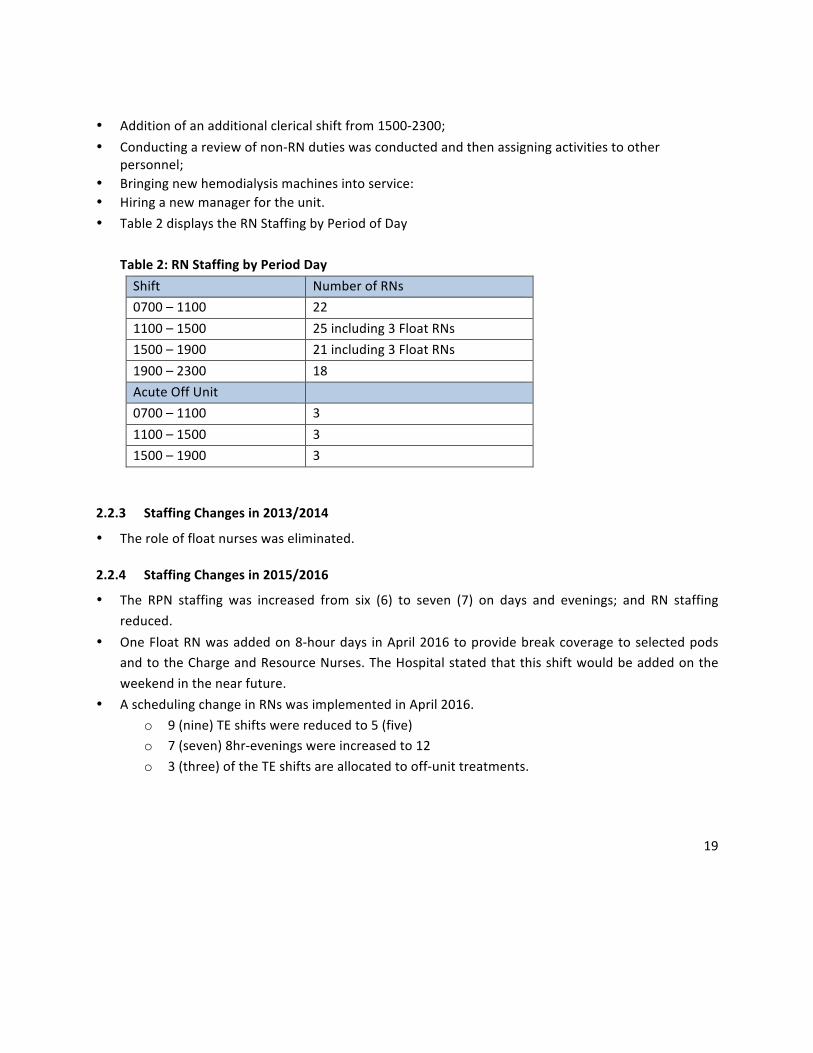
• Additionofanadditionalclericalshiftfrom1500-2300;• Conductingareviewofnon-RNdutieswasconductedandthenassigningactivitiestoother
personnel;• Bringingnewhemodialysismachinesintoservice:• Hiringanewmanagerfortheunit.• Table2displaystheRNStaffingbyPeriodofDay
Table2:RNStaffingbyPeriodDayShift NumberofRNs0700–1100 221100–1500 25including3FloatRNs1500–1900 21including3FloatRNs1900–2300 18AcuteOffUnit 0700–1100 31100–1500 31500–1900 3
2.2.3 StaffingChangesin2013/2014
• Theroleoffloatnurseswaseliminated.
2.2.4 StaffingChangesin2015/2016
• The RPN staffing was increased from six (6) to seven (7) on days and evenings; and RN staffingreduced.
• OneFloatRNwasaddedon8-hourdays inApril2016toprovidebreakcoveragetoselectedpodsandtotheChargeandResourceNurses.TheHospitalstatedthatthisshiftwouldbeaddedontheweekendinthenearfuture.
• AschedulingchangeinRNswasimplementedinApril2016.o 9(nine)TEshiftswerereducedto5(five)o 7(seven)8hr-eveningswereincreasedto12o 3(three)oftheTEshiftsareallocatedtooff-unittreatments.
20
2.2.5 CurrentStaffing
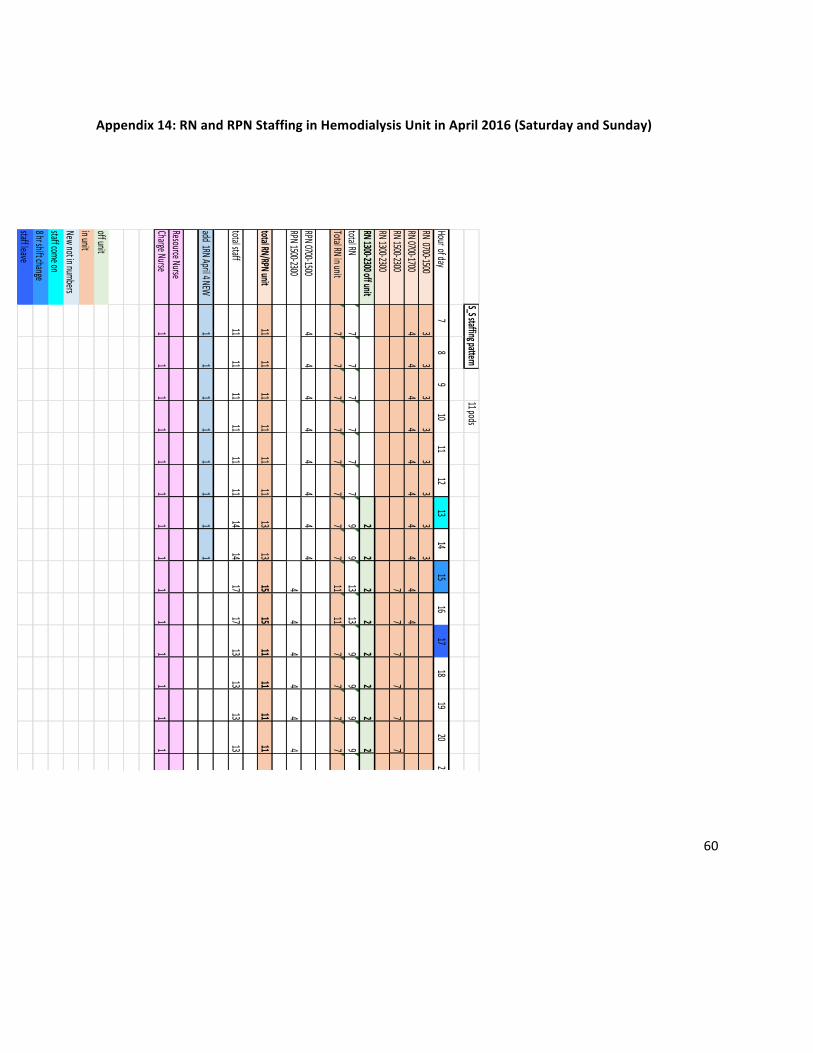
TheRNandRPNstaffareequallydividedacrossbothsidesoftheunit.EachnurseisassignedtoaPodof3stations.ThereisaChargeNurseandaResourceNurseonbothdayandeveningsshifts.TwoRNsareoncallatnight.AgraphicaldepictionoftheRNandRPNstaffingbyhourofday4onMondaytoFridayisincludedinAppendix13andSaturday-SundayinAppendix14.ThecurrentstaffingintheHemodialysisunitforRNsMondaytoFridayis:• 0700–1500:8RN• 0700–1700:6RN• 1500–2300:12RN• 1300–2300:5RN(2incentre;and3offunit)• 1(one)RNon8-hrdayshiftforbreakreliefThecurrentstaffingforRPNsMondaytoFridayis:• 0700–1500:7RPNs• 1500–2300:7RPNsOnweekends,thestaffingisreduced,asonlyonesideoftheunitisopen.ThecurrentstaffingintheHemodialysisunitforRNsonweekendsis:• 0700–1500:3RN• 0700–1700:4RN• 1500–2300:7RN• 1300–2300:2RN(foroffunit)• 1(one)8-hrRNtobeaddedonDayshiftforbreakrelief• ThereisoneChargeNurseondaysandeveningsThecurrentstaffingforRPNsonweekendsis:• 0700–1500:4RPNs• 1500–2300:4RPNs
4RNandRPNStaffingbyHourofDayonMondaytoFriday;andSaturday/SundayprovidedbyHumberRiverHospitalatIAConFriday,April22,2016.

21
Otherstaffincludes:• ClericalStaff:staggeredshiftswithcoveragefrom0600-2330.• DialysisTechnologists• DialysisAssistants• 1530-2330:1DA• HousekeepingAdditional,thefollowingstaffworkMondaytoFriday:• BodyAccessCoordinator• IndependentDialysisCoordinator• ClinicalPracticeLeaders• ClinicalInstructor• PatientCareManager• PatientServiceCoordinatorprovidesadditionalsupportafterhours
2.3 WorkloadConcernsofRegisteredNursesandDiscussionsattheHospitalAssociationCommitteeTherewere187ProfessionalResponsibilityWorkloadResponsibilityForms(PRWRFs)submittedbetween2011and2016.• 2011:21PRWRFs• 2012:75PRWRFs• 2013:61PRWRFs• 2014:19PRWRFs• 2015:4PRWRFs• 2016:7PRWRFsDuring thepresentation theAssociation stated that the nursingworkloadproblemsare as a result offollowingissues:• ProfessionalPracticeincludingpracticestandards,nurseleadership• Patientacuity• RNandRPNpractice• Fluctuatingworkload• Fragmentedandinterruptedcare• FluctuatingstaffingandRNstaffing• ExcellentCareforAllAct,2010.

22
TheAssociationprovided37recommendations5intheirbriefsubmissionforresolutionoftheworkload.TherecommendationscanbesummarizedunderRNandRPNstaffing,patientassignments, leadershipand leadershipaccountabilityandresponsibility,governancestructureengaging front linestaff; timelyand effective processes to resolve workload concern, education support; a fatigue managementprogram,documentationandmodelofcare.• RNandRPNstaffing:
o Basestaffingaccountsfortime/resourcesforconsultation;patientassessment;patientcareneeds; receiving report; documentation; replacement for orientation and professionaldevelopment
o RN/RPNstaffingmixo RPNroleclarityo RNsreplacedwithRNso Increasestaffingof4RNs/dayassignedtoroleofFloatNurseon11.25hr.tourso Adjust staffing to80/20RN toRPN ratio;Replace4RPNsoutof7working regular8hour
toursonDaysandEveningso Utilizebestpracticeguidelines/standardswithregardtostaffingandworkload
• Patientassignments:o UseofevidencebasedtoolsandtheThreeFactorframeworkinmakingdecisionsregarding
RPNstaffing;andsubsequentlyforpatientassignmentso Appropriate assignment of patients to RNs and RPNs; engagement of nursing staff in
assignmentdecisionso Patientassignmenttoolandpolicytobedevelopedandevaluated
• Leadershipandleadershipaccountabilityandresponsibility;• Governance structure engaging front line staff; engagement in planning, development of healthy
workenvironment;• Timely and effective processes to resolve concerns related to professional practice, acuity,
workloadsandstaffing;• Educationsupportanddedicatededucator;• Comprehensivefatiguepreventionandmanagementprogram;• Standardized documentation and handover (transfer of care) at end of patient runs and shift
change;and
5SubmissiontotheIndependentAssessmentCommitteebyOntarioNurses’Association,p.46-49.

23
• Modelofcaretoreducefragmentationofcare.TheAssociationstatedthattheincreasingpatientworkloadrequiresRegisteredNurses(RNs)toperformmore work than is consistent with proper patient care. During and following the presentation, theAssociationrespondedtoquestionsofclarificationfromboththeHospitalandIAC.Melanie Tremblay, Director of the Nephrology Program; Dilshad Pirani, Manager of the NephrologyProgram;andJenniferDuteau,ClinicalPracticeLeaderpresentedonbehalfoftheHospital.Thecontentof the Hospital’s presentation was based on their written pre-hearing submission. The presentationprovidedtheHospital’sviewon:• HospitalaccountabilitiestotheOntarioRenalNetwork;• Programleadership;• TransitionfromChurchsitetoWilsonsite;• ModelofCare;• Orientationofstaffandcompetenciesofstaff;• PatientschedulingandassignmenttonurseswithintheHemodialysisUnit;• Nursingworkloadthroughoutshifts;atchangeover.TheHospitalrecommendationsincluded:• AdditionalRNstaffforbreak/reliefsupport;hoursandshiftsbasedonunitactivity;• Schedulingtooptimizestaffutilizationandassessworkload;• Completeenvironmentalscanregardingstaffingandpatientpopulation;• RefiningPatientNeedsAssessmentTooltoidentifyRNonlyassignments;• A regular review process to assess and document patients for stability/predictability to support
patientassignmentstoappropriatestaffwithappropriateworkload;• ProcessesforstafftoupdatetheResourceNurseonsignificantchanges/eventsduringdialysis;• EstablishandmonitorstatisticstoreflectsignificanteventincludingtransferofcarefromRNtoRPN;
admissionofpatientspost-dialysis;numberofpatientsrequiringpost-dialysisobservations;numberof daily treatments, off unit treatments, urgent unplanned off unit treatments, cardiac arrests,circumstanceswhenstaffingnotadequate,replacingRNswithRPNsduetounavailability;
• Meetingregularlywithstafftoaddresstheirconcerns;• Establishingapracticecommittee;• ConsultationwithRPNAOreRPNrole;• WorkingwithunionpartnersretimelyaddressingofworkloadcomplaintsasperArticle8.01.
24
2.4 MeetingsbetweenAssociationandHospitalPriortoIAC
TherewereseveralmeetingsbetweentheAssociationandtheHospitalinanefforttoresolvetheissuesarisingfromthePRWRFs.InitiallythePRWRFSrelatedtotheHemodialysisunitwerediscussedintheHospitalAssociationCommittee(HAC).
OnFebruary3,2012,Ms.MarianaMarkovicnotifiedtheHospitalthattheAssociation’sintenttobringforththeissueofprofessionalresponsibilityrelatedtotheongoingproblemsidentifiedinthePRWRFs,andifnotresolved,torefertheissuestoanIndependentAssessmentCommittee.
AProfessionalResponsibilityCommitteemetonFebruary28,2012;April3,2012;June26,2012;November7,2012.Fourteenissueswereidentifiedanddiscussedduringthesemeetingsincludingstaffing,vacancies,overtime,equipment,rolesandresponsibilitiesofvariousteammembers,assignments,offunittreatments,patientvolumeandacuity.InformationwasprovidedbytheHospitaltotheAssociationonroledescriptions,staffing,sicktime,modelofcare,patienttreatments,educationsessionsandstaffmeetings.
FollowingtheNovember7meeting,theHospitalprovidedaLetterofUnderstandingtotheAssociationthatdetailedalistofimprovementstoaddressmostoftheprofessionalresponsibilityconcerns.ImprovementsidentifiedbytheHospitalwere:
• NewcaredeliverymodelimplementedinOctober2012toresolveRNsbeingpulledoffunitduringchangeovertodooffunittreatments.
• Patientassignmentschangedtoputallconventionaltreatmentsatmainpods;andshort(2hr.)treatmentsinexpansionC100.ThischangewastoresolveanRNpickingupa2nd2-hourpatient.
• Anewmasterscheduleasimplementedwithafloatnurseassignedperpodduringchangeover.• Theratioofstaffwastobe3:1forconventionaltreatments;2:1forshortdailytreatments;and
2:1forpatientsrequiringsegregation.• Anadditionaldialysisassistantshiftwasimplementedfrom1000-1800inordertoprovide
additionalsupportatchangeoverandforoff-unittreatments.• RoleofResourceNurseimplementedwithnopatientassignment.• Additionalclericalassociateshiftimplementedbetween1500-2300.• PatienttreatmentspotsassignedbytheResourceNursestobalanceworkloadassignmentsof
RNs.• Newdescriptionforfloatnursesimplementedwithnopatientassignment.• Non-nursingdutiesassignedtoclericalstaff,housekeeping,anddialysisassistants.

25
TheLetterofUnderstandingwasnotexecuted.
ItwasagreedtoestablishaHemodialysisUnitTaskForceandtermsofreferenceweredevelopedinJune2012.Thepurposeofthetaskforcewastodevelop,implementandevaluateeffectivestrategiestoaddressworkloadconcernsnotedundertheprofessionalresponsibilityconcernssubmittedsinceSeptember2011.Thestatedmeasureofsuccessofthetaskforcewastoidentifystrategieswithintheallocatedresourcestoensuretheachievementofpositivepatientoutcomes.6AccordingtotheminutesprovidedintheHospitalbrief,theTaskForcemetonfouroccasionsbetweenDecember2012andFebruary2013.7OnApril3,2013,theAssociationadvisedtheHospitalthattheunionwouldnotbecontinuingthetaskforcebecauseRPNswerebeingintroducedintotheunit.
OnJune18,2013,theAssociationadvancedtheProfessionalResponsibilityComplainttotheOntarioHospitalAssociationtoidentifythenextavailableIACchair.
TheHospitalfiledanemployergrievanceonJune12,2014.FollowingthegrievancefiledbytheHospital,bothpartiesparticipatedintwodaysofmediationonJanuary26,2015andSeptember29,2015.TheHospitalwithdrewthegrievanceonSeptember29,2015;andbothpartiesagreedtomeetonNovember2and3,andDecember18,2015;andsubsequentlyonFebruary2,2016.Theissuesdiscussedduringthesemeetingswere:
• November2-3,2015:Professionalpractice,patientacuity,fluctuatingworkloadandfluctuatingstaffing;
• December18,2015:RN/RPNassignment,modelofcare,rolesofRNandRPNoninterprofessionalteam,communication,breaksandeducationforRPN;
• February2,2016:reviewofprocessforassignments;breakassignmentsandacuitytoolfollow-up.
6TermsofReference–HemodialysisTaskForce,SubmissionsonBehalfoftheHumberRiverHospital,Tab9.
7DialysisTaskForceMeetingAgendasandMeeting,SubmissionsonBehalfoftheHumberRiverHospital,Tabs11-14.
26
3 Discussion,AnalysisandRecommendations
FiveissuesthatimpactonnursingworkloadintheHemodialysisunitwereidentifiedbytheIAC.Theissuesare:
1. RegisteredNurseStaffingandSchedulinga. DeterminingtheAssignmentofRNorRPNtoPatientstoensureadequateandsafeRN
Staffingb. SupportingConsultationandCollaborationamongNursingStaffc. NurseScheduling
2. PatientVolumes,TypesofTreatmentandScheduling3. Documentation4. CommunicationandDecisionMaking5. ProcessforManagementofProfessionalResponsibilityWorkloadReportForms
3.1 RegisteredNurseStaffingandSchedulingToEnsureAdequateandSafeRNStaffing
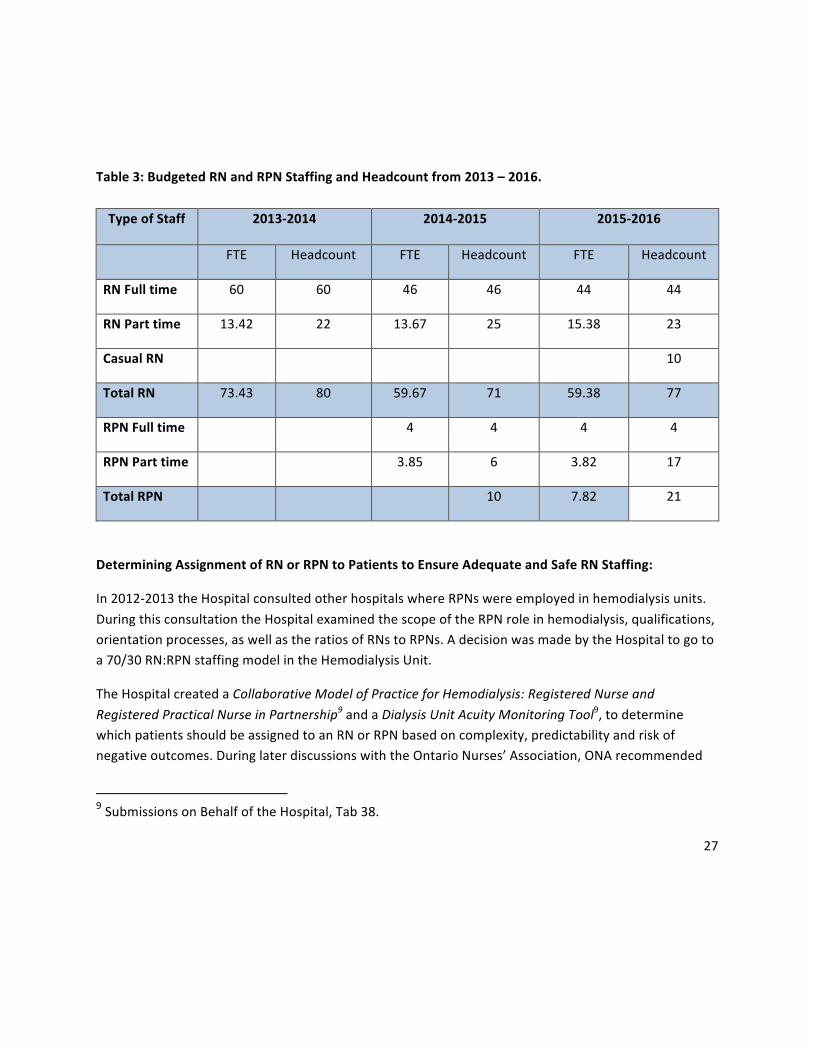
Nursestaffingisrecognizedasastructuralmeasureofqualityandadequacyofstaffinglevelsislinkedtopatientsafetyandqualityofcare.Ongoingevaluationofnursestaffingandoutcomesrelatedtopatientsafetyandqualityareessential.Since2011therehasbeensteadyerosionofRegisteredNurse(RN)staffcomplementintheHemodialysisunit,primarilyduetolayoffs,attritionandreplacementoffulltimepositionswithparttimepositions.DuringthesameperiodoftimetherehavebeenfrequentchangesinRNschedulingwithregardtothenumberofRNspershiftandthedurationofshifts.Inadditiontherehavebeenmanychanges,includinglayoffs,whichhavealteredthenumberoffullandparttimeRNsworkinginthehemodialysisunit.ThehospitalprovidedcomparativedataonRNbudgetedFTEsandheadcountfrom2013-20168,whichisreproducedinTable3.TotalRNFTEsdecreasedby14.05FTEsfrom73.43in2013to59.38in2016.Duringthesameperiod,theRPNstaffbudgetincreasedto7.82FTEs.Thisresultedinanetdecreasein6.23FTEsinRNstaffing(14.05less7.82),whilepatientvolumeshaveremainedthesameintheprevalentchronicdialysispatientsandincreasedintheacuteoffunitpatientpopulation.
8DataonRNandRPNBudgetedFTEs2013–2016,HumberRiverHospital,SubmittedtoIAConFriday,April22,2016.
27
Table3:BudgetedRNandRPNStaffingandHeadcountfrom2013–2016.TypeofStaff 2013-2014 2014-2015 2015-2016
FTE Headcount FTE Headcount FTE Headcount
RNFulltime 60 60 46 46 44 44
RNParttime 13.42 22 13.67 25 15.38 23
CasualRN 10
TotalRN 73.43 80 59.67 71 59.38 77
RPNFulltime 4 4 4 4
RPNParttime 3.85 6 3.82 17
TotalRPN 10 7.82 21
DeterminingAssignmentofRNorRPNtoPatientstoEnsureAdequateandSafeRNStaffing:
In2012-2013theHospitalconsultedotherhospitalswhereRPNswereemployedinhemodialysisunits.DuringthisconsultationtheHospitalexaminedthescopeoftheRPNroleinhemodialysis,qualifications,orientationprocesses,aswellastheratiosofRNstoRPNs.AdecisionwasmadebytheHospitaltogotoa70/30RN:RPNstaffingmodelintheHemodialysisUnit.
TheHospitalcreatedaCollaborativeModelofPracticeforHemodialysis:RegisteredNurseandRegisteredPracticalNurseinPartnership9andaDialysisUnitAcuityMonitoringTool9,todeterminewhichpatientsshouldbeassignedtoanRNorRPNbasedoncomplexity,predictabilityandriskofnegativeoutcomes.DuringlaterdiscussionswiththeOntarioNurses’Association,ONArecommended
9SubmissionsonBehalfoftheHospital,Tab38.
28
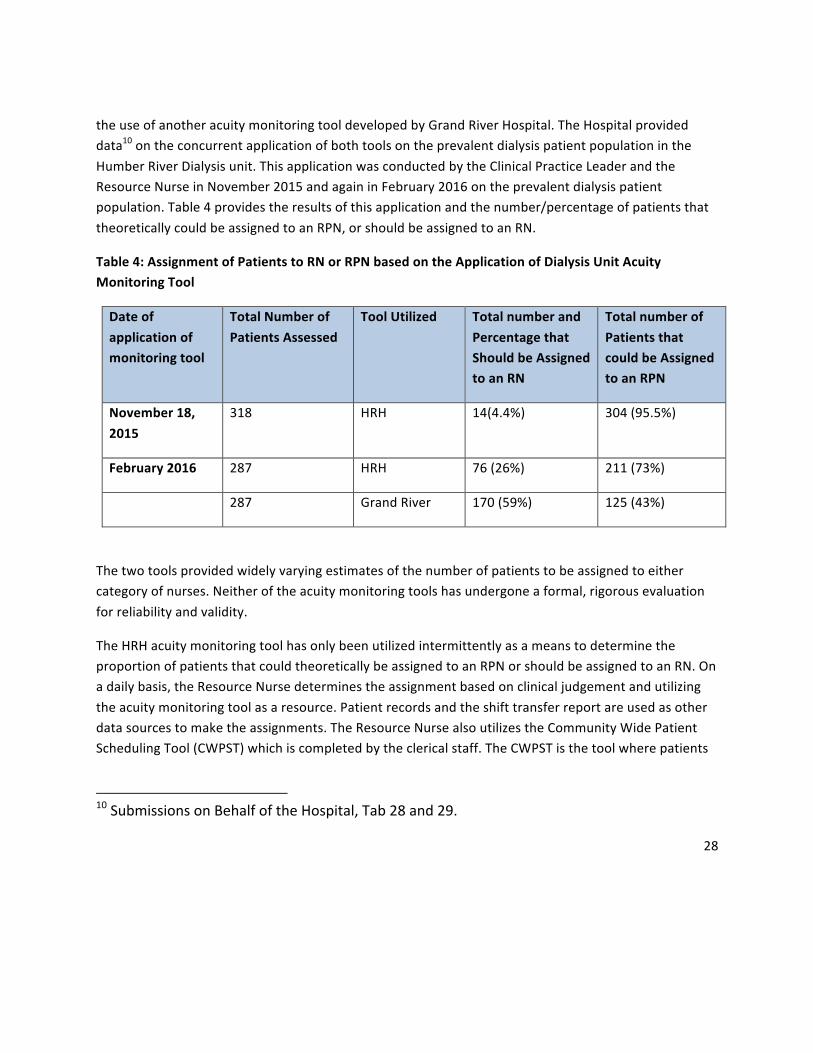
theuseofanotheracuitymonitoringtooldevelopedbyGrandRiverHospital.TheHospitalprovideddata10ontheconcurrentapplicationofbothtoolsontheprevalentdialysispatientpopulationintheHumberRiverDialysisunit.ThisapplicationwasconductedbytheClinicalPracticeLeaderandtheResourceNurseinNovember2015andagaininFebruary2016ontheprevalentdialysispatientpopulation.Table4providestheresultsofthisapplicationandthenumber/percentageofpatientsthattheoreticallycouldbeassignedtoanRPN,orshouldbeassignedtoanRN.
Table4:AssignmentofPatientstoRNorRPNbasedontheApplicationofDialysisUnitAcuityMonitoringTool
Dateofapplicationofmonitoringtool
TotalNumberofPatientsAssessed
ToolUtilized TotalnumberandPercentagethatShouldbeAssignedtoanRN
TotalnumberofPatientsthatcouldbeAssignedtoanRPN
November18,2015
318 HRH 14(4.4%) 304(95.5%)
February2016 287 HRH 76(26%) 211(73%)
287 GrandRiver 170(59%) 125(43%)
Thetwotoolsprovidedwidelyvaryingestimatesofthenumberofpatientstobeassignedtoeithercategoryofnurses.Neitheroftheacuitymonitoringtoolshasundergoneaformal,rigorousevaluationforreliabilityandvalidity.
TheHRHacuitymonitoringtoolhasonlybeenutilizedintermittentlyasameanstodeterminetheproportionofpatientsthatcouldtheoreticallybeassignedtoanRPNorshouldbeassignedtoanRN.Onadailybasis,theResourceNursedeterminestheassignmentbasedonclinicaljudgementandutilizingtheacuitymonitoringtoolasaresource.Patientrecordsandtheshifttransferreportareusedasotherdatasourcestomaketheassignments.TheResourceNursealsoutilizestheCommunityWidePatientSchedulingTool(CWPST)whichiscompletedbytheclericalstaff.TheCWPSTisthetoolwherepatients
10SubmissionsonBehalfoftheHospital,Tab28and29.
29
areassignedtostationandtimefortheirtreatment.OncetheResourceNursehasdeterminedthenurseassignments,thisinformationisaddedtotheCWPST.
Recentlynewpreandpostassessmentscreenswereaddedtothepatientrecord.TheelementsofthePostassessmentscreencontainsselectedindicatorsfromtheHRHacuitymonitoringtool.TheresultsofthepostassessmentscreenareautomaticallyaddedtotheCommunityWidePatientSchedulingToolforeachpatient,inanefforttoassisttheResourceNurseinmakingappropriateassignments.
Itisunknownifthesearethebestindicatorstoutilizeorifmoreordifferentindicatorsshouldbeaddedtobereflectiveofpatientcondition/reactionstotreatment.Forexample,shouldtheindicatorforcriticalresultsbemoresensitivetoanycriticalresultinthelast3months?Isthisthemostsuitabletimeframeforevaluation?DoestheResourceNursehavereadyaccesstoallthepertinentinformationonalmost300hemodialysispatientsandtheircurrentstatustomakethebestjudgementonnurse—patientassignmentsonadailybasis?
Theredidnotappeartoberegularandsystematicmonitoring/evaluationofnursestaffingandtheadequacyofRNstaffing.Theinfrequentuseofanon-validatedacuitytoolisinsufficient.WhiletheHospitalreportsdatatotheOntarioRenalNetworkfortheongoingmonitoringofhemodialysisprograms,theindicatorsarerelatedtopatientvolumes,typeofcare,timelinessandlocationofcare.Recentbenchmarkingstudy11conductedbytheHospitalin2016includedsomestaffingindicators(e.gnumberofnursesoneachshift,proportionofRNs/RPNs)butdidnotincludewhatmethods/toolsotherhemodialysisunitsutilizetodeterminenursestaffing.
SupportingConsultationandCollaborationamongNursingStaff
TheCollegeofNursesofOntarioPracticeGuidelineonRNandRPNPractice:theClient,theNurseandtheEnvironment12utilizesthreefactors(theclient,theenvironmentandthenurse)toguidedecisionmakingoncare-providerassignmentsandtheneedforconsultationandcollaboration.TheHRHCollaborativeModelforPracticeforHemodialysisstatesthatRNsandRPNswillconsultandcollaborateasnecessaryforpatientcare.
TheRPNsconsultRNsonaregularbasisalthoughtherehasbeennoevaluationofthedegree/frequencyofconsultation/collaborationwiththeexceptionofthemonitoringofTransferofAccountability.11SubmissionsonBehalfoftheHospital,Tab37
12CollegeofNursesofOntario.RNandRPNPractice:theClient,theNurseandtheEnvironment,2014
30
However,TOAonlyoccurswhentheconsultation/collaborationprocessisinsufficienttomeetpatientneeds,andthereforeisnotagoodmeasureofthetimeandworkloadinvolvedwithongoingconsultationandcollaborationamongRNsandRPNs.
EffectiveandtimelyconsultationandcollaborationbetweenRNsandRPNsisessentialtoprovidesafeandqualitypatientcare.Arguably,thepatientsintheHRHhemodialysisunitthatareassignedtoRNsaremorecomplexthanthoseassignedtoRPNs,astheRNsmustbeassignedtothosepatientswhoarelessstable,lesspredictableandathigherriskofnegativeoutcomes.Inaddition,RNsareassignedtoalloffunitpatients.TheRNsviewtheRPNsastheircolleaguesandunderstandtheirprofessionalaccountabilityandresponsibilitytosupporttheRPNSthroughconsultation,collaborationand/ortransferofaccountability.
However,thetimeinvolvedinconsultingandcollaborationwithRPNsisadditionalworkfortheRNs.ThiswasdescribedbytheRNsaschallenginggiventhecurrentavailabilityofRNsintheunitespeciallyduringbreaksandtimesofpatientturnover.Additionally,theRNmustcontinuethecareofherownpatients,whileconsultingwiththeRPN,possiblyresultingininterruptionsand/ordelaysincare.
NurseScheduling:
CurrentlytheRNsworkacombinationof8-hourand10-hoursshifts;withstarttimesof0700,1300or1500.AsaresultofthelengthandstarttimeofRNshifts,theRNstaffinghaspeaksandvalleysduringatypical18-hourworkday,rangingfrom14-23RNsatanyonetimeduringweekdays.ThetimeofgreatestoverlapofRNshiftsis1300-1700.DuringtheperiodsoflowerRNstaffingthereisalackofadequateRNcoverageorshiftbreaksandpatientturnover.ThereisfrequentdemandfortheChargeandResourceNursestoprovidepatientcare(breakcoveragefornurses,patientsrequiringobservationetc.),divertingthemawayfromtheirleadershiproles.Recentlyanewshiftfrom0700-1500wasaddedduringtheweekbecauseoftheneedtoprovidebreakcoveragefortheChargeNurseandResourceNurse,breakcoverageforthepodswithprivaterooms,andforpatientsrequiringobservationaftertreatment.Thegeographyofunitissuchthatsomepodsarenotvisiblefromthenursingstations,makingbreakcoveragechallenging.
Overthelast5years,thereappearstohavebeenlittleengagementofand/ordiscussionwiththenursingstaffregardinganyofthedecisionsregardingnursestaffing/schedulingbeforeorafterimplementation.Norwasitevidentthattherewasanysystematicevaluationbymanagementofthemanystaffingandschedulingchanges.
31
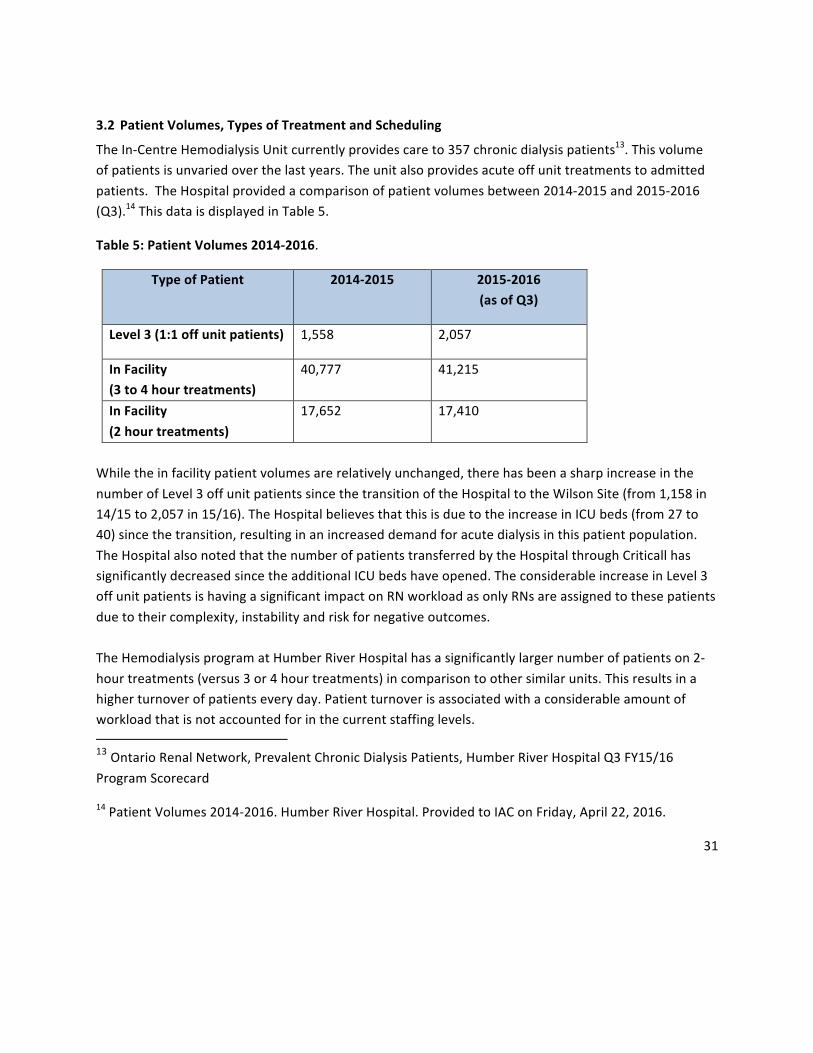
3.2 PatientVolumes,TypesofTreatmentandScheduling
TheIn-CentreHemodialysisUnitcurrentlyprovidescareto357chronicdialysispatients13.Thisvolumeofpatientsisunvariedoverthelastyears.Theunitalsoprovidesacuteoffunittreatmentstoadmittedpatients.TheHospitalprovidedacomparisonofpatientvolumesbetween2014-2015and2015-2016(Q3).14ThisdataisdisplayedinTable5.
Table5:PatientVolumes2014-2016.
TypeofPatient 2014-2015 2015-2016(asofQ3)
Level3(1:1offunitpatients) 1,558 2,057
InFacility(3to4hourtreatments)
40,777 41,215
InFacility(2hourtreatments)
17,652 17,410
Whiletheinfacilitypatientvolumesarerelativelyunchanged,therehasbeenasharpincreaseinthenumberofLevel3offunitpatientssincethetransitionoftheHospitaltotheWilsonSite(from1,158in14/15to2,057in15/16).TheHospitalbelievesthatthisisduetotheincreaseinICUbeds(from27to40)sincethetransition,resultinginanincreaseddemandforacutedialysisinthispatientpopulation.TheHospitalalsonotedthatthenumberofpatientstransferredbytheHospitalthroughCriticallhassignificantlydecreasedsincetheadditionalICUbedshaveopened.TheconsiderableincreaseinLevel3offunitpatientsishavingasignificantimpactonRNworkloadasonlyRNsareassignedtothesepatientsduetotheircomplexity,instabilityandriskfornegativeoutcomes.TheHemodialysisprogramatHumberRiverHospitalhasasignificantlylargernumberofpatientson2-hourtreatments(versus3or4hourtreatments)incomparisontoothersimilarunits.Thisresultsinahigherturnoverofpatientseveryday.Patientturnoverisassociatedwithaconsiderableamountofworkloadthatisnotaccountedforinthecurrentstaffinglevels.13OntarioRenalNetwork,PrevalentChronicDialysisPatients,HumberRiverHospitalQ3FY15/16ProgramScorecard
14PatientVolumes2014-2016.HumberRiverHospital.ProvidedtoIAConFriday,April22,2016.

32
Patientsarescheduledfortreatmentduringoneof3shiftsinthemorning,afternoonorevening.Eachtreatmentpodhas3chair/bedsandstarttimesare15minapart.Keepingtothescheduleforstarttimesisnotalwaysachievableduetomanyfactorsincludingpatientfactors(delayinarrivaltotheunit,accessissues)and/ordialysismachineissues.Asaresultnursingstaffarefrequentlygettingbehindjustastheystarttheshiftbecausedelaysarecommonandprobablyunavoidable.Thereisnotaspecificstandardforstarttimesspacingindialysisunits,andapparentlyvariesfrom15-30mindependingonthehospital.TheRNsnotedthatitisverychallengingtoadequatelyassesseachpatient,initiatetreatmentanddocumentcareduringthis45minutetimeframe.Documentationisfrequentlydeferredtolaterintheshift.
3.3 Documentation
HumberRiverHospitalcurrentlyusesMeditechfortheelectronichealthrecordforclients.NursesdothemajorityoftheirdocumentationinMeditech.Thepaperbasedpatientflowsheet(utilizedtorecordreadingsandotherinformationduringtreatmentfromthedialysismachines)wasdiscontinuedafterthemovetoWilsonsiteasthenewunithasIntegratedBedsideTerminals(IBTs)andacomputerstationwithineachpod.ItwasplannedthatnursescouldenterdatautilizingtheIBTSandthecomputerstations.However,theIBTsaretheentertainment/communicationdeviceforpatients,soinpracticaltermsarenotavailabletothenursingstaff.ThedialysismachinesnotinterfacedwithMeditech.Asaresult,nurseswereobservedbytheIACmemberswhileonatouroftheunittoberecordinginformation/dataonavarietyofinformalflowsheetsasameanstoretaindatafordocumentationintheelectronichealthrecord.Thisdocumentation“workaround”seemsunavoidableatthistimegiventhattheDialysismachinesarenotinterfacedwithMeditech.
Inaddition,thetightstarttimesandrapidpatientturnoverresultinlittleornotimefortimelyandappropriatedocumentationduringthefirsthoursofcare.
3.4 CommunicationandDecisionMaking
Theengagementofnursingstaffinameaningfulwayregardingtheirworkandworkconditionsisessentialincreatinganeffectiveworkenvironmenttosupporthighqualitypatientcare.
CommunicationwithstaffisbothformalandinformalintheHemodialysisUnit.Emailisrelieduponextensivelytocommunicateinformationtonursesincludingdecisionsregardingstaffing.Somechangesappeartobeimplementedattimeswithnoformalcommunication(e.g.schedulechanges).TheClinical

33
PracticeLeadersendsaweeklyemailtoallstaffwithclinicalandsafetyupdates,educationopportunitiesandotherinformationshefeelsthestaffmayrequire.Therewerenoinformationboardsforstaffintheunit.Performancedata(e.g.ORNreportcards)aresharedwithstaffintermittentlybutthisseemedtobeprimarilyverbal.Thestaffmeetingsareintermittentandshortinduration;andminutesarenotconsistentlydone.
Importantdecisionsonstaffingandschedulingappeartobemadebyleadershipwithlittleornoconsultationand/ordiscussionwithnursingstaff.TheHemodialysisTaskForcewasnotsustainedduetotheAssociation’swithdrawalfromthemeetings.Whiletherewasconsiderableengagementofstafftosupportthetransitiontoanewhospital,issuesofstaffingandworkloadwerenotdiscussedaspartofthetransitionplanning.
3.5 ProcessforManagementofProfessionalResponsibilityWorkloadReportForm(PRWRFs)
Duringtheperiodof2011to2016therewere187professionalresponsibilityworkloadreportformssubmittedbyRNstotheHospital.Duringthistimetherewasahaphazardprocessfortimelyreviewofformsandcommunicationbacktostaff.TheprocessforaddressingPRWRFs,asoutlinedinthecollectiveagreementwasnotconsistentlyfollowed.EffortsrelatedtotheHemodialysisTaskForce,establishedtoworkonworkloadissues,werenotsustained.Inthefallof2015andwinter2016,thepartiesdidmeetonthreeoccasions,butwerenotsuccessfulinreachinganagreementontheworkloadissues.
3.6 Recommendations:
TheIndependentAssessmentCommitteemakesthefollowingrecommendationsregardingworkloadissuesintheHemodialysisUnitatHumberRiverHospital.
RelatedtoRN/RPNAssignments:
1. Conductaformalevaluationoftheacuitymonitoringtoolsforreliabilityandvalidity.TheevaluationshouldminimallyincludetheacuitytooldesignedbyHumberRiverHospitalandthetooldesignedbyGrandRiverHospital.
2. DevelopasetofindicatorsforregularevaluationofRNstaffing;andwhichcanalsobecomparedwithotherhemodialysisunits.ThismayincludeRN/RPNhoursofcareperday,andratioofhourstopatienttreatments.
3. EvaluatethepostassessmentscreentodeterminetheutilityofthecurrentindicatorsindeterminingRNorRPNassignment;andreviseasnecessary.
4. InadditiontotheprospectiveuseoftheacuitymonitoringtoolinassigningpatientstoRNsandRPNs,conductaregularretrospective“realtime”auditofwhethertheassignmentswere
34
appropriate.ThiswouldprovidesomemeasureofevaluationoftheacuitytoolandtheabilityoftheResourceNursestomakeappropriateassignmentsbasedontheinformationavailabletothem.
5. DevelopamethodforquantifyingthenumberandtypeofconsultationsandcollaborationeffortsmadeonadailybasisbetweenRNsandRPNs.TheidentificationofwhyRPNsconsultRNswouldinformbothappropriatenessofpatientassignmentsandopportunitiesforimprovementincare.
RelatedtoNurseStaffing:6. Maintainthenewlyimplemented8-hrFloatRNshiftondaysforbreakcoverageofisolationrooms,
ChargeNurseandResourceNurse.7. IncreaseRNstaffingonadailybasisbyincreasingthenumberofRNsinafloatnurserole.This
staffingincreasewill:a. EnsureRNtimeandavailabilitytoengageineffectiveconsultationandcollaborationwith
RPNs;b. EnsurethattheRPNshavereadyaccesstoanRNduringbreaks;c. Provideadequatebreakcoverage;d. Alignstaffingwithpatientvolume,caredemandsandturnover;e. Allowforunplannedevents/delays(e.g.patientsrequiringobservation;accessissues;late
arrivalofpatientsfrominpatientfloors);f. Supporttimelydocumentationofcare;g. FreeuptheChargeNurseandResourceNursefrombreakcoverage;h. Sickcallcoverage.
ThiscouldbeaccomplishedbystartingtwoTEeveningshiftsearlierthanthecurrentstarttimeandbyadding2.8FTEsinadditionalRNhours,deployedtotheroleofFloatNurses.
a. AddTwofloatRNs;assigningonetoeachsideoftheunit;startingat1100(MondaytoFriday)
b. Add2FloatRNsonSaturdayandSundaywithstaggeredstarttimes.(e.g.oneat11,andonelater).
c. Starttwo(2)oftheTERNsatanearliertime(e.g.1200)8. ReviewtheFulltimeandParttimecomplementofRNstoensureadequatenumberofRNsavailable
toworkintheunit.RelatedtoPatientVolumesandScheduling:

35
9. Closelymonitorvolumeandtypeofpatientandstaffaccordingly(offunit,2hourtreatments).IncreasetheRNstaffingtosupporttheincreasedvolumeinacuteoffunitthathasbeenexperiencedposttransitiontoWilsonsite
10. Staggerstarttimes30minaparttoallownursesadequatetimeforassessment,initiationoftreatmentanddocumentation.
RelatedtoDocumentation:11. Ensurethereisadequatetimeintheshifttosupporttimelyandaccuratedocumentationofpatient
careintherecord.12. DevelopaninterfacebetweenthedialysismachinesandtheMeditechhealthrecord.13. Implementaflowsheetfornursesuntilinterfaceisachieved.
RecommendationsforCommunicationandDecisionMaking:
14. Createaregularstaffforumwhereissuesrelatedtostaffing,schedulingandotheroperationalissuesintheunitcanbediscussedwithleadership.
15. CreateaQualityBoardorotherareaforpostingofperformancedataonhemodialysisincludingpatientvolumes.
16. Ensurethatstaffarenotifiedofupcomingstaffmeetings,withanopportunitytocontributetotheagenda;agendasandminutesshouldbereadilyavailable.
17. Establishregularstaffhuddlesduringeachshifttosupporttimelydiscussionsofpatientflow,safetyconcerns,otherissuesofconcernetc.
RecommendationsreProcessforManagementofPRWRFs:
18. FormaSub-HACcommitteeforhemodialysisunittodiscussmonthlyifthereareworkloadcomplaintstoreview.
4. Conclusion
ThisreportcontainstheIndependentAssessmentCommittee’sfindingsandrecommendationsregardingProfessionalWorkloadComplaintsubmittedbyNursesfromtheHemodialysisUnitatHumberRiverHospital.TheprocessundertakenthroughanIndependentAssessmentCommitteeprovidesauniqueopportunityfordiscussionanddialoguebetweenallthepartiesregardingthecomplexissuesandconditionsthat
36
underlieaProfessionalWorkloadComplaint.TheCommitteehasmade18recommendationsinfiveareasregardingissuesthatimpacttheworkloadofRegisteredNurses.TheMembersoftheIndependentAssessmentCommitteeunanimouslysupportallrecommendationsinthisreport.TheCommitteehopesthattherecommendationswillassisttheHospitalandtheAssociationtofindmutuallyagreeableresolutionswithregardtonursingworkloadissuesintheHemodialysisUnit.

37
Appendix1:LetterfromtheAssociationApril30,2014.
ntoIACChair,October28,2013
April 30, 2014 Leslie Vincent SENT VIA EMAIL 716 Windermere Ave. Toronto, ON, M6S 3M1 Dear Ms. Vincent, Re: Humber River Hospital – Hemodialysis Unit, Professional Responsibility Complaint – Proceeding to an Independent Assessment Committee – Ontario Nurses’ Association, File No. 201202042 Thank you for accepting the request to chair the next IAC investigation and hearing. In accordance with Article 8.01 of the Central Hospital Agreement set out between Ontario Nurses’ Association (ONA) and Humber River Hospital (HRH), the Labour Management Committee (HAC) has met on a number of occasions and exchanged letters of communication several times in attempts to bring resolution to workload issues causing RNs working in the Hemodialysis Unit to believe that they are being asked to perform more work than is consistent with proper patient care. Ontario Nurses’ Association considers the unresolved workload issues to constitute Professional Responsibility concerns, as applied to regulated health professionals by the College of Nurses of Ontario (CNO) under the Regulated Health Professions Act (RHPA). The Association views the professional responsibility concerns of RNs to be a result of being assigned more work by the Employer than what is consistent with proper patient care. The RNs working in the Hemodialysis Unit at the HRH have identified workload issues and the work environment to make it difficult to provide safe quality patient care and to practice safely in accordance with the professional standards set out by the CNO for RNs. The effect of the workload and the working environment on RNs relates to professional practice, patient acuity, fluctuating workloads, and fluctuating staffing. Attempts at working towards resolution of workload issues that constitute professional practice concerns at HAC meetings with the Employer have been unproductive. The Employer is resolved to move forward to an IAC hearing to address the professional practice responsibility concerns that have been presented to them. The Association has no other recourse at this time but to forward this matter to a hearing before the Independent Assessment Committee. To this effect ONA respectfully submits this Professional Responsibility Complaint to the IAC.

38
Ms. Leslie Vincent Page 2 Humber River Hospital – Hemodialysis Unit, Professional Responsibility Complaint – Proceeding to an Independent Assessment Committee – ONA File 201202042
ONA’s Nominee is Angela Preocanin, RN, and her contact information is:
Angela Preocanin, RN 3257 Woodward Ave. Burlington L7N 2M7 Tel: 905-512-7413 Email: [email protected]
We are informed that the Employer’s Nominee is Treva McCumber, RN, DHSc, and her contact information is:
Treva McCumber, RN, DHSc Vice President, Transitions, Diagnostics & CNO Royal Victoria Regional Health Centre 201 Georgian Drive Barrie, ON L4M 6M2 Tel: 705-728-9090 Ext. 46000 Fax: 705-728-2408 Email: [email protected]
Once you have the information you require, it is our understanding that as the IAC Chair you will communicate with the two Nominees to set up a date for the hearing that is agreeable to both parties, the Employer and ONA. We thank you for your assistance in this matter. Sincerely, ONTARIO NURSES’ ASSOCIATION
Mariana Markovic Mariana Markovic Professional Practice Specialist Labour Relations Officer C:
Catherine Green, HRH, Manager Labour Relations Melanie Tremblay, HRH, Renal Program Director Scott Jarrett, HRH, Vice President of Patient Relations Reuben Devlin, HRH, President & CEO Mary Veneziano, Executive Administrative Assistant to the President & CEO and Board of Directors, on behalf of Paul Allison, HRH, Board of Directors Chair Micheal Howell, ONA, Local Coordinator and BUP Sheri Street, ONA, Servicing LRO Doug Anderson, ONA, Manager Provincial Services Team Beverly Mathers, ONA, Manager South District Service Team Valerie McDonald, ONA, Manager Labour Relations David McCoy, OHA, Manager Labour Relations Angela Preocanin, RN, ONA Nominee

39
Appendix2:EmployerGrievanceJune12,2014
From: Green, Catherine [email protected]: FW: ONA Grievance
Date: June 16, 2014 at 8:02 AMTo: Leslie Vincent ([email protected]) [email protected]: [email protected], Jarrett, Scott [email protected], Czaus, Margaret [email protected]
Hi Leslie
Please find attached an Employer Grievance which we sent to ONA on Friday concerning the Hemo IAC.
If you have any questions, please do not hesitate to contact me.
Thanks
Catherine Green RNManager, Labour RelationsTel. 416-747-3780Fax. 416-747-3758email: [email protected]
“Please note Humber River Hospital has moved to a new email address extension, @hrh.ca Please update your contact information. ThankYou.”

40
Appendix2:Page2ofEmployerGrievance

41
Appendix3:LetterfromHospital’sLegalCounselSeptember12,2014.
42
43
Appendix4:LetterfromLegalCounselforAssociationSeptember25,2014.

44
45
Appendix5:LetterfromLegalCounselofHospitalOctober4,2014
Hicks Morley Hamilton Stewart Stone LLP JASON GREEN77 King St. W., 39th FLoor, Box 371, TD Centre [email protected], ON M5K 1KB Direct: 416.864.7337Tel: 416.362.1011 Fax: 416.362.9680 Cell: 416.268.5180
Toionto File No. 631-490October 4, 2014
LcndonVIA EMAIL
Ms. Leslie VincentChair, lAG Panel716 Windermere AvenueToronto, Ontario M6S 3M1
Dear Ms. Vincent:
Re: Humber River Hospital and Ontario Nurses’ Association (ONA)Dialysis IAC
We are in receipt of Ms. Mcintyre’s letter of September 25, 2014 and can advise youthat the Hospital fundamentally disagrees with the position taken by ONA.
As you are likely aware, the Independent Assessment Committee (lAG) is a processdefined under Article 8 of the collective agreement between the Hospital and ONA. Tothe extent the Committee has any jurisdiction over workload concerns, it must be foundwithin the language of Article 8.
A review of that article makes it clear that an Independent Assessment Committeehearing is the final step in a thorough process that is designed to address workloadcomplaints that a nurse (or nurses as the case may be) genuinely believes negativelyimpacts proper patient care. These concerns are to be addressed by both the nurseand the Hospital at the earliest possible opportunity.
In order to achieve the goal of a timely resolution, the Article sets out a number ofmandatory steps that nurses must take in advancing their complaints. It is patently clearon the face of the language that an Independent Assessment Committee can only beconvened once the previous steps have been taken and no resolution of the workloadcomplaints achieved.
In the case of the workload complaints that ONA is attempting to place in front of thispanel, there are numerous breaches of the procedural requirements of Article 8. In theHospital’s view, these breaches are significant and prevent ONA from referring theworkload complaints to an IAC.

46
47
48
Appendix6:LetterfromIACChairOctober14,2014
Leslie Vincent RN Consultant 716 Windermere Ave., Toronto, ON, M6S 3M1
October 14, 2014
VIA EMAIL
Dear. Ms. McIntyre and Mr. Green,
I am in receipt of the letter from Ms. McIntyre, dated September 25, 2014; and the letter from Mr.
Green, dated October 3, 2014.
While the members of the Independent Assessment Committee are prepared to proceed with IAC
hearing on November 24-26, 2014, it is clear that the Hospital and the Association are at odds regarding
the timing of the IAC given the current grievance regarding the IAC process.
As I have previously communicated, I believe the Hospital and the Association need to resolve your
issues regarding the grievance and the timing of the IAC hearing. The IAC panel will not be deciding on
the merit of this grievance as we do not have this responsibility as our mandate; nor do I think we
should be placed in a position to be mediating between the two parties regarding this dispute.
I look forward to hearing the outcome of your discussions.
Sincerely,
Leslie Vincent
CC.
Mariana Markovic, Ontario Nurses Association
Doug Anderson, Ontario Nurses Association
Marg Czaus, Humber RIver Hospital
Treva McCumber, Hospital Nominee, IAC
Angela Preocanin, ONA Nominee, IAC
49
Appendix7:LetterfromLegalCounselforAssociationOctober31,2014.
50
Appendix8:LetterfromLegalCounselforHospitalOctober23,2014.

51
52
Appendix9:LetterfromIACChairNovember4,2014.
Leslie Vincent 716 Windermere Ave, Toronto, ON, M6S 3M1
Phone: 416-767-8773 E-mail: [email protected]
November 4, 2014. Ms. Mariana Markovic Ontario Nurses’ Association 85 Grenville Street, Suite 400 Toronto, Ontario, M5S 3A2 Mr. Jason Green Hicks Morley Hamilton Stewart Storie LLP 77 King St. W., 39th Floor, Box 371, TD Centre Toronto, ON, M5K 1K8
Dear Ms. Markovic and Mr. Green,
I am in receipt of letters from Ms. McIntyre, dated October 21, 2014; and Mr. Green, dated October 23, 2014. Despite considerable efforts encouraging the parties to resolve the procedural issues in dispute, we find ourselves at an impasse regarding the dates to convene the Independent Assessment Committee for the Hemodialysis Unit at the Humber River Hospital.
With regret, I am canceling the planned IAC dates of November 24-26, 2014 and will proceed to find a new date for the IAC in 2015. I would expect that we convene the IAC before the end of February 2015, and I will proceed to determine the availability of the IAC panel members.
Sincerely,
Chair, Independent Assessment Committee for Humber River Hospital Copy – Elizabeth J. McIntyre, Cavalluzzo Copy – Doug Anderson, Ontario Nurses Association Copy – Marg Czaus, Humber River Hospital Copy – Treva McCumber, Hospital Nominee Copy – Angela Preocanin – ONA Nominee

53
Appendix10:AgendaforIAC
Agenda
WednesdayApril20,2016
HolidayInn3450DufferinSt.Toronto,M6A2V1
RoomTBD
Time Item Participants
09:00–10:00 IACPanelPreparationMeeting IAC
10:00–12:00 Tour of Dialysis Unit at Humber River Regional
Hospital
IAC, HRRH and
ONA
13:00—13:15 IntroductionandReviewofProceedingsby
Chairperson
IACChair
13:15—14:45 OntarioNurses’AssociationSubmissionPresentation
Responsetoquestionsofclarificationfrom:• IndependentAssessmentCommittee• HumberRiverRegionalHospital
IAC, HRRH and
ONA
14:45—15:00 Break All
15:00—16:30 HumberRiverRegionalHospitalSubmission
Presentation
Responsetoquestionsofclarificationfrom• IndependentAssessmentCommittee• OntarioNurses’Association
IAC, HRRH and
ONA
16:30 ReviewofProcessforThursday,April21,2016
AdjournmentofHearing
IACChair

54
Agenda
ThursdayApril21,2016
HolidayInn3450DufferinSt.Toronto,M6A2V1
RoomTBD
Time Item Participants
09:00–12:00 Humber River Regional Hospital Response to OntarioNurses’AssociationSubmissionResponsetoquestionsfrom• IndependentAssessmentCommittee• OntarioNurses’Association• Discussion
IAC, HRRH and
ONA
12:00–13:00 LunchBreak All
13:00–16:00 OntarioNurses’AssociationResponsetoHumberRiverRegionalHospitalResponsetoquestionsfrom• IndependentAssessmentCommittee• HumberRiverRegionalHospital• Discussion
IAC, HRRH and
ONA
16:00-16:15 ReviewofProcessforFriday,April22,2016
AdjournmentofMeeting
IACChair
16:15
onwards
IndependentAssessmentCommitteeMeeting
IAC
55
Agenda
Friday,April22,2016
HolidayInn3450DufferinSt.Toronto,M6A2V1
RoomTBD
Time Item Participants
09:00—12:00 QuestionstobothPartiesbyIndependentAssessmentCommittee
IAC, HRRH andONA
12:00—12:30 Closing Remarks and Identification of Next Steps byChairperson
IACChair
12:30 ClosureofHearing All
12:30—14:30 IndependentAssessmentCommitteeMeeting IAC
56
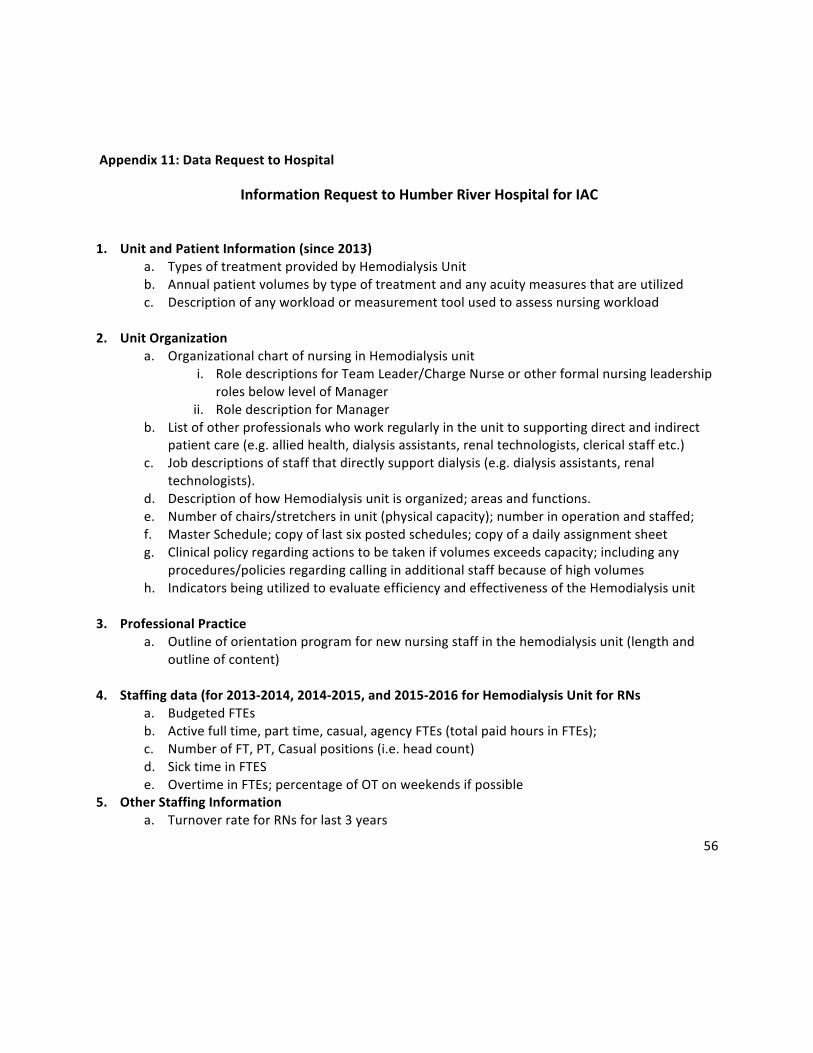
Appendix11:DataRequesttoHospital
InformationRequesttoHumberRiverHospitalforIAC
1. UnitandPatientInformation(since2013)a. TypesoftreatmentprovidedbyHemodialysisUnitb. Annualpatientvolumesbytypeoftreatmentandanyacuitymeasuresthatareutilizedc. Descriptionofanyworkloadormeasurementtoolusedtoassessnursingworkload
2. UnitOrganization
a. OrganizationalchartofnursinginHemodialysisuniti. RoledescriptionsforTeamLeader/ChargeNurseorotherformalnursingleadership
rolesbelowlevelofManagerii. RoledescriptionforManager
b. Listofotherprofessionalswhoworkregularlyintheunittosupportingdirectandindirectpatientcare(e.g.alliedhealth,dialysisassistants,renaltechnologists,clericalstaffetc.)
c. Jobdescriptionsofstaffthatdirectlysupportdialysis(e.g.dialysisassistants,renaltechnologists).
d. DescriptionofhowHemodialysisunitisorganized;areasandfunctions.e. Numberofchairs/stretchersinunit(physicalcapacity);numberinoperationandstaffed;f. MasterSchedule;copyoflastsixpostedschedules;copyofadailyassignmentsheetg. Clinicalpolicyregardingactionstobetakenifvolumesexceedscapacity;includingany
procedures/policiesregardingcallinginadditionalstaffbecauseofhighvolumesh. IndicatorsbeingutilizedtoevaluateefficiencyandeffectivenessoftheHemodialysisunit
3. ProfessionalPractice
a. Outlineoforientationprogramfornewnursingstaffinthehemodialysisunit(lengthandoutlineofcontent)
4. Staffingdata(for2013-2014,2014-2015,and2015-2016forHemodialysisUnitforRNs
a. BudgetedFTEsb. Activefulltime,parttime,casual,agencyFTEs(totalpaidhoursinFTEs);c. NumberofFT,PT,Casualpositions(i.e.headcount)d. SicktimeinFTESe. OvertimeinFTEs;percentageofOTonweekendsifpossible
5. OtherStaffingInformationa. TurnoverrateforRNsforlast3years

57
b. Jobpostinginformationorrequirementsc. Experienceprofile-Averageyearsofexperienceinunit;numberofjuniorstaff(lessthan2
years’experience)d. Numberandtypeofpositionspostedinthecurrentfiscalyear;andcurrentvacanciese. Numberofnursingstaffonmodifiedwork;orhavepermanentaccommodations
6. Other
a. Copyoflocalcollectiveagreement;
58
Appendix12:AttendeesattheIAC
AssociationAttendees:
MarianaMarkovic,RN,ProfessionalPracticeSpecialist,LRO,ONADanielleBisnar,LegalCounselforONAMikeHowellRN,BargainingUnitPresident,LocalCoordinatorSheriStreetRN,LabourRelationsOfficer,ONAElizabethAstilleroRN,HemodialysisAnneGibbRN,HemodialysisNadineCruickshankRN,ProfessionalPracticeSpecialist,LRO,ONAObserversVickiMcKenna,RN,ONA1stVicePresidentHospitalAttendees:
MargCzaus,ChiefNursingOfficerScottJarrett,VicePresident,PatientServicesKarenAdams,VicePresident,HumanResourcesandOrganizationalEffectivenessMelanieTremblay,Director,NephrologyDilshadPIrani,Manager,NephrologyMarisaVaglica,Director,ProfessionalPracticeJenniferDuteau,ClinicalPracticeLeaderSarahEvesandKathyrnBird,LegalCounselfortheHospital

59
Appendix13:RNandRPNStaffinginHemodialysisUnitinApril2016(MondaytoFriday)
M-Fstaffingpattern21pods
Hourofday7
89
1011
1213
1415
1617
1819
2021
22RN0700-1500
88
88
88
88
RN0700-17006
66
66
66
66
6RN1500-2300
1212
1212
1212
1212
RN1300-23002
22
22
22
22
2RN1300-2300offunit
xxxx
xxxx
xxxxx
33
33
33
33
33
totalRN14
1414
1414
1419
1923
2317
1717
1717
17TotalRNinunit
1414
1414
1414
1616
2020
1414
1414
1414
RPN0700-15007
77
77
77
7RPN1500-2300
77
77
77
77
totalRN/RPNunit21
2121
2121
2123
2327
2721
2121
2121
21
totalstaff21
2121
2121
2126
2630
3024
2424
2424
24
add1RNApril4NEW1
11
11
11
1
ResourceNurse1
11
11
11
11
11
11
11
1ChargeNurse
11
11
11
11
11
11
11
11
offunitinunitNewnotinnumbersstaffcomeon8hrshiftchangestaffleave
60
Appendix14:RNandRPNStaffinginHemodialysisUnitinApril2016(SaturdayandSunday)
S_Sstaffingpattern11pods
Hourofday7
89
1011
1213
1415
1617
1819
2021
22RN0700-1500
33
33
33
33
RN0700-17004
44
44
44
44
4RN1500-2300
77
77
77
77
RN1300-2300RN1300-2300offunit
22
22
22
22
22xx
totalRN7
77
77
79
913
139
99
99
9TotalRNinunit
77
77
77
77
1111
77
77
77
RPN0700-15004
44
44
44
4RPN1500-2300
44
44
44
44
totalRN/RPNunit11
1111
1111
1113
1315
1511
1111
1111
11
totalstaff11
1111
1111
1114
1417
1713
1313
1313
13
add1RNApril4NEW1
11
11
11
1
ResourceNurseChargeNurse
11
11
11
11
11
11
11
11
offunitinunitNewnotinnumbersstaffcomeon8hrshiftchangestaffleave