india and acute malnutrition in children veena shatrugna national institute of nutrition hyderabad...
TRANSCRIPT

India and Acute Malnutrition in Children
Veena Shatrugna
National Institute of NutritionHyderabad
India

-1- Absolute Weights – A 30 year trend (Mean in Kg)
Rural Rural Rural Rural NCHS Median 1977 1996 2003 2006 Values
Age F M F M F M F M F M
01+ 7.5 8.1 8.1 8.7 8.1 8.6 8.3 8.9 9.5 10.2
(219-920)
03 10.6 10.4 11.3 11.7 11.4 11.9 11.8 12.1 14.1 14.6 (218-916)
05 13.7 14.1 13.6 14.4 14.1 14.6 14.5 14.7 17.7 18.7
(229-747)
10 22.0 21.6 22.4 22.6 23.1 23.1 23.9 23.9 32.5 31.4
(304-734)
20-24 42.9 48.1 43.5 50.3 43.8 50.9 45.0 52.2 56.6 68.9
(509-3870)
>70** - - 39.1 47.3 41.5 49.2 40.6 49.0 - -
(161-178)
Source:** NNMB 1977, 1996, 2003, 2006

-2-
Absolute Heights – A 30 year trend (Mean in cm)
Rural Rural Rural Rural NCHS Median 1977 1996 2003 2006 Values
Age F M F M F M F M F M
01+ 71.9 73.1 72.8 75.0 73.8 75.3 74.0 75.7 74.3 76.1
(219-920)
3+ 85.8 86.4 88.4 90.1 89.8 91.1 89.9 91.1 93.9 94.9
(218-916)
05+ 99.6 100.5 100.4 102.1 102.5 103.2 102.4 102.6 108.4109.9
(229-747)
10+ 125.7 125.1 126.8 127.9 128.5 128.7 128.9 129.0 138.3137.5
(304-734)
20-24 151.2 163.4 151.5 164.0 151.1 163.3 152.0 164.2 163.7176.8
(509-3870)
>=70 147.9 162.3 147.9 161.0 146.8 160.0 145.5 159.9 -
(339-728)
Source: NNMB Reports, 1977, 1996, 2002, 2006



-3-
% DISTRIBUTION OF ADULTS ACCORDING TO BMI CLASSIFICATION 20 YEAR TREND
BMI 1974‑79* 1988‑90* 1996-97** 1993‑94*** 2002* CLASSES (RURAL) (RURAL) (RURAL) (URBAN) (RURAL) <18.5 (CED) F 51.8 49.3 47.7 36.7 38.9
M 55.6 49.0 45.5 42.8 36.6
(NORMAL) F 44.8 46.6 46.3 51.7 52.4
18.5‑25.0 M 42.1 48.3 50.4 51.8 57.2
(OBESE) F 3.4 4.1 6.3 11.6 8.7
>=25
M 2.3 2.7 4.1 5.5 6.2
* NNMB, 1991, quoted by N,Nadamuni Naidu et al, 1994.* Rural, 2002** NNMB, Rural surveys, 1996; *** NNMB Urban Surveys, 1994

- 4 a -
% DISTRIBUTION OF ADULTS ACCORDING TO BMI CLASSIFICATION - NNMB 2006
< 16 16-17 17-18.5 18.5-20 20-25 > 25< 16 16-17 17-18.5 18.5-20 20-25 > 25
(CED III) (CED II) (CED I) (Low Wt. (Normal) (Over wt.)(CED III) (CED II) (CED I) (Low Wt. (Normal) (Over wt.)
Normal)Normal)
Men 5.7 7.9 19.6 21.7 37.3 7.0
Women 8.0 9.0 19.0 18.7 34.4 9.1

- 4b -
Distribution (%) of Adults According to BMI Classification 10 year trend
BMI Males Males Females Females
1996 2006 1996 2006
<16.0 8.6 5.7 11.8 8.0
16.0-17.0 11.0 7.9 12.8 9.0
17.0-18.5 25.9 19.6 23.2 19.0
18.5-20.0 25.3 21.7 20.0 18.7
20.5-25.0 25.2 37.3 26.4 34.4
>25 4.1 7.0 6.0 9.1
Source: NNMB, 1996 & 2006(Rural)

- 5 - Thinness as a public health problem
Low prevalence (warning sign,
monitoring required): 5-9% of population with BMI <18.5
Medium prevalence
(poor situation): 10-19% of population with BMI <18.5
High prevalence
(serious situation): 20-39% of population with BMI <18.5
Very high prevalence
(critical situation): 40% of population with BMI <18.5

- 6 -Mean Birth Weights in different parts of the world
Region Region Mean Birth WeightMean Birth Weight (kg)(kg)
North America, Western Europe 3.5-3.6and Australia
Eastern Europe 3.1-3.3
Africa and East Asia 2.9-3.1
South Asia 2.7

- 7 - Mean Birth Weights and LBW in SEAR LBW LBW Country Country N N (<2500g) (<2500g) Birth weight Birth weight
(Kg)(Kg)
India 4307 33.0 2.63 Nepal Rural 2529 14.3 2.78 Urban 3629 22.3 2.76Sri Lanka 1851 18.4 2.84 Myanmar 3582 17.8 2.85Indonesia 1647 10.5 2.94Thailand 4124 9.6 3.00USA Afro-American 4614 10.6 3.14 Whites 16481 6.0 3.36 *Source: WHO, 1993.

- 8 - MATERNAL PARAMETERS (MEANS) ACCORDING TO BMI STATUSMATERNAL PARAMETERS (MEANS) ACCORDING TO BMI STATUS
BMI CLASSES N MOTHER'S (Wt, Kg.) BIRTH (Wt, Kg.) LBW (<2500 g)%
<16.0 81 35.4 2510 53.1 CED III
16.0-16.9 133 38.1 2573 41.4 CED II
17.0-18.4 460 40.9 2653 35.9 CED I 18.5-19.9 553 44.1 2771 27.7(NORMAL) 20.0-24.9 717 49.6 2812 26.4(NORMAL) 25.0-29.9 68 60.6 2972 14.7(OBESE) > 30 5 75.5 2972 20.0 (OBESE) TOTAL 2017 45.2 2742 30.5
Source : NNMB Repeat Surveys (1991) , Quoted by Nadamuni Naidu et al, 1994.

- 9-Birth Weight and Socio-Economic Status
PoorPoor MiddleMiddle HighHighincomeincome incomeincome incomeincome
Height (cms) 151.5 154.2 156.3
Weight (kg) 45.7 49.9 56.2
Hb(g/dl) 10.9 11.1 12.2
Birth weight (kg) 2.70 2.90 3.13

-10-BIRTH WEIGHTS IN POOR AND WELL TO DO GROUPS INBIRTH WEIGHTS IN POOR AND WELL TO DO GROUPS IN
MADRAS AND COONORMADRAS AND COONOR
NN B.WT PREMATUREB.WT PREMATURELbs Kg (%)Lbs Kg (%)
1949SPEL.WARD 1269 7.12 3.2 -GEN.WARD 1179 6.3 2.8 -
1954SPEL.WARD 200 6.85 3.08 12.3 GEN.WARD 500 6.01 2.7 8.4
SOURCE : Varkki C, et al, 1955.

-11-Birth weights (kg) in poor after supplementation
1971 1972 No No No No
Supplementation Supplementation Supplementation SupplementationSupplementation Supplementation Supplementation Supplementation Food Folic acid Iron Iron+ Folic acid
2.704 3.028 2.920 2.570 2.650 2.899
Source : L.Iyengar, 1972.

-12 -
Attempts made to increase birth weights in poor socio-economic group
1. Iron
2. Folic acid3. Iron and Folic acid
4. Zinc5. Vitamin A6. N3 fats, fish oils 7. Micro nutrients 8. Reduction of activities

- 13 -
Distribution (%) of 1-5 years children according to nutritional status (Weight for age) by sex-Gomez classification
Nutrition Grades* Nutrition Grades* Boys Girls Pooled
(n=2011) (n=1957) (n=3968)(n=2011) (n=1957) (n=3968)
NormalNormal 13.1 12.1 12.6
MildMild 45.5 45.5 45.5
Moderate Moderate 37.4 37.8 37.6
SevereSevere 4.0 4.6 4.3
* NCHS standards* NCHS standards
Source: NNMB 2005Source: NNMB 2005..

-14 a-
Distribution (%) of 1-5 years according to Weight for age – standard deviation (SD) classification by gender
Weight for age* Weight for age* Boys Girls Pooled
(n=2011) (n=1957) (n=3968)(n=2011) (n=1957) (n=3968)
Median Median 3.5 3.6 3.6
-1SD to-1SD to Median Median 11.4 10.1 10.8
-2SD to -1SD-2SD to -1SD 31.4 31.1 31.2
-3SD to-3SD to -2SD -2SD 38.2 37.7 37.9
<Median - 3SD<Median - 3SD 15.5 17.5 16.5
* NCHS standards* NCHS standards
Source: NNMB 2005.Source: NNMB 2005.

- 14b -
Distribution (%) of 1-5 years according to Weight for age – standard deviation (SD) classification by Age groups
Weight for age*Weight for age* < 1 1-3 3-5 < 1 1-3 3-5
Median Median 23.1 4.5 2.723.1 4.5 2.7
-1SD to Median -1SD to Median 26.726.7 11.5 10.9 11.5 10.9
-2SD to -1SD-2SD to -1SD 27.927.9 28.8 28.8 31.7
-3SD to-2SD -3SD to-2SD 16.2 16.2 35.0 35.0 39.9 39.9
<Median -3SD<Median -3SD 6.16.1 20.2 20.2 14.9 14.9
* NCHS standards* NCHS standardsSource: NNMB 2005.Source: NNMB 2005.

- 15 a -
Distribution (%) of 1-5 years children according to Height for age standard deviation (SD) classification by gender
Height for age* eight for age* Boys Girls Pooled
(n=2011) (n=1957) (n=3968)(n=2011) (n=1957) (n=3968)
Median Median 8.0 6.6 7.3
-1SD to Median 15.5 13.4 14.5
-2SD to -1SD 26.4 25.5 26.0
-3SD to -2SD 26.6 27.9 27.2
<Median - 3SD 23.5 26.6 25.0
* NCHS standards* NCHS standards
Source: NNMB 2005.Source: NNMB 2005.

- 15 b -
Distribution (%) of 1-5 years according to Height for age – standard deviation (SD) classification by Age groups
Height for age*Height for age* < 1 1-3 3-5 < 1 1-3 3-5
Median Median 28.3 9.4 6.228.3 9.4 6.2
-1SD to Median -1SD to Median 27.627.6 16.3 14.0 16.3 14.0
-2SD to -1SD-2SD to -1SD 25.525.5 23.0 23.0 28.228.2
-3SD to-2SD -3SD to-2SD 12.8 12.8 24.8 24.8 28.2 28.2
<Median -3SD<Median -3SD 5.75.7 26.5 26.5 23.5 23.5
* NCHS standards* NCHS standardsSource: NNMB 2005.Source: NNMB 2005.

-16 a -Distribution (%) of 1-5 years children according Weight for Height standard deviation (SD) classification by gender
Weight forWeight for HHeight * eight * Boys GirlsBoys Girls Pooled Pooled
(n=2457) (n=2399) (n=4856)(n=2457) (n=2399) (n=4856)
Median Median 10.8 10.8 13.2 13.2 12.0 12.0
-1SD to-1SD to Median Median 31.531.5 31.1 31.1 31.3 31.3
-2SD to -1SD-2SD to -1SD 41.841.8 41.6 41.6 41.7 41.7
-3SD to-3SD to -2SD -2SD 13.313.3 11.8 11.8 12.6 12.6
<Median - 3SD<Median - 3SD 2.52.5 2.3 2.3 2.4 2.4
* NCHS standards* NCHS standards
Source: NNMB 2005-06.Source: NNMB 2005-06.

-16 b -Distribution (%) of 1-5 years according to Weight for Height– standard deviation (SD) classification by Age groups
Weight for Height *Weight for Height * < 1 1-3 3-5 < 1 1-3 3-5
Median Median 23.5 11.7 12.223.5 11.7 12.2
-1SD to Median -1SD to Median 39.439.4 30.2 32.4 30.2 32.4
-2SD to -1SD-2SD to -1SD 24.124.1 43.6 43.6 39.9
-3SD to-2SD -3SD to-2SD 8.6 8.6 11.8 13.3 13.3
<Median -3SD<Median -3SD 4.44.4 2.6 2.6 2.2 2.2
* NCHS standards* NCHS standardsSource: NNMB 2005.Source: NNMB 2005.

ICMR Balanced diet for adults (1 Cu)ICMR Balanced diet for adults (1 Cu)
Cereals Pulses Veg Roots Flesh Milk Fats Sugar Nuts Fruits Condi- foods ments
460 40 40 60 - 150 25 30 - - -
-17 -

- 18 - Intake by age (> 70% of RDA)
Age Cereals Pulse L.V. Others R& T Milk Fat Sugar (yrs)
1-3 54 15 8 35 55 10 10 14
4 - 6 62 29 10 42 56 8 5 11
Male 58 29 15 39 56 8 3 1110-12 Female 67 30 15 37 55 7 3 12
Male 81 51 15 47 60 33 10 31 > 18 Female 77 39 10 50 56 37 27 50

- 19 -- 19 - Nutrient intakes ( >70% of RDA) by AgeNutrient intakes ( >70% of RDA) by Age
Age (yrs) Energy Protein Fat Calcium Iron Vitamin A
1-3 30 62 23 19 15 8 4 -6 31 73 30 28 15 10 7- 9 38 61 36 37 13 7.5 Male 45 50 54 24 9 9 10-12 Female 57 41 51 22 11 9
Male 55 40 65 32 10 1113-15 Female 70 39 58 25 15 9
Male 70 40 60 32 12 916-17 Female 70 43 62 35 14 10
Male 80 77 85 70 29 11 >18 Female 89 78 77 61 15 11

- 20 –
Other nutritional problems
Apart from stunting and under weight –
1.1. AnaemiaAnaemia - 60-90%
2.2. Iodine DeficiencyIodine Deficiency - endemic most parts of the country
3.3. Goitre Goitre - endemic in North East, sub Himalayan range, many tribal belts in central India
4.4. FluorosisFluorosis - endemic many parts of the country
-21 –21 –
According to Recommended Dietary GuidelinesAccording to Recommended Dietary Guidelines
60-65% Calories from Carbohydrates
25-30% from Fat
10-12% from Protein
Each of these calories, proteins and fats must be derived from as many foods as possible
In the rural area of India 80% of Calories are derived from from Cereals
Those with adequate calories from cereals have high iron intakes, but because almost All the calories come from cereals, the iron is not available…this population must derive its calories from other sources such as pulse, meat, vegetable, milk egg to use this iron.

- 22 -
• Children Only 30% have calorie adequacy (from cereals). They are deficient in all the other nutrient rich foods recommended for children.
• The WHO Recommendation
• Calories - 30-40% must come from fats (low volumes and energy densities)
• Vitamin A, calcium, iron - from milk, eggs, flesh foods, vegetables, fruit etc. (will also contribute additional calories),
• Cereals, pulse to be used to bridge the calorie gap.
• In India – it is reversed, cereal load has resulted in simple minded diagnosis of micronutrient deficiencies.

- 23 -
How did we reach this Cereal – Calorie Trap ?
RDA,
Consumption units
Minimum Wages
Poverty Line
Green Revolution---PDS The consumption unit story

- 24-- 24- RDA ICMR Balanced diet for adults (1 Cu)ICMR Balanced diet for adults (1 Cu)
Cereals Pulses Veg Roots Flesh Milk Fats Sugar Nuts Fruits Condi- foods ments
460 40 40 60 - 150 25 30 - - -

- 25 -- 25 -
Coefficient for computing calorie requirement of different groupsCoefficient for computing calorie requirement of different groups**
Group Cu-Units
Adult male (sedentary worker) 1.0
Adult male (moderate worker) 1.2
Adult male (heavy worker) 1.6
Adult female (sedentary worker) 0.8
Adult female (moderate worker) 0.9
Adult female (heavy worker) 1.2
Adolescents 12 – 21 years 1.0
Children 9 to 12 years 0.8
Children 7 to 9 years 0.7
Children 5 to 7 years 0.6
Children 3 to 5 years 0.5
Children 1 to 3 years 0.4
*Source: Gopalan et al (1991)

- 26 -- 26 -
Minimum Wages - Criteria
1. 3 consumption units * for one wage earner
2. 2700 cals per average Indian adult
3. ?? Clothing - 72 yards per annum per family
4. ?? House rent
5. ? Fuel, Lighting etc… - 20% of wages
6. ?? Education, Medical and other expenses

- 27- 27 - Since Minimum wages are based on caloriesSince Minimum wages are based on calories
Cheapest source of 2000 calories Cheapest source of 2000 calories
(Gm)(Gm) Cost (Rs.)Cost (Rs.)
Sugar 520 8.00
Rice 571.4 11.0
Oil 225 ml 18.0
Dals 500.0 22.0
Potato 2000 20.0
Sapota, banana 1740 25
Milk 3250ml 60
Chicken 2000 120
Dry fruits 400 200

- 28 -- 28 - Micironutrients essential for man Micironutrients essential for man
VitaminsVitamins Trace minerals Trace minerals
A.A. Micronutrients known to be essential for man and animalsMicronutrients known to be essential for man and animals
Vitamin A Thiamin Iron Selenium
Vitamin D Riboflavin Iodine Manganese
Vitamin K Nicotinic acid Zinc Chromium
Vitamin E Pyridoxine Copper CobaltEssential fatty acid Folic acid(-6 and -3)
Biotin (?) Vitamin B12
Pantothenic acid (?) Ascorbic acid
B. Micronutrients essential for animals and not yet established as essential for manB. Micronutrients essential for animals and not yet established as essential for man
Choline Silicon Molybdenum
p-Aminobenzoic acid Fluorine ArsenicNickel
Source: Narasinga Rao BS.

- 29 -- 29 - Phytonutrients for Health Promotion Phytonutrients for Health Promotion
Phytonutrient class
Carotenoids
Glucosinolates,
Isothiocyanates,
Indoles
Inositol phosphates
Phenolics, cyclic compounds
Phytoestrogens
Phytosterols
Polyphenols
Protease inhibitor
Saponins
Sulfides and thiols
Source: Beecher

- 30 -- 30 - Dietary antioxidants Dietary antioxidants
NutrientsNutrients Non-nutrients Non-nutrients
-Carotene-provitamin A Carotenoids (lycopene,xanthophyls)
Ascorbic acid-vitamin C Lutein, -and -carotenes (cryptoxanthine,
zeaxanthine)
Tocopherols Flavonoids (quercetin, myricetin,
quercetagatin, gossypetin)
Tocotrienols
Riboflavin
Sulfur amino acids Anthocyanins
Cysteine and methionine Isoflavones
Selenium Phenolic compounds (catechin) Indoles
Source: Narasinga Rao, BS.

- 31 -
Phytonutrients act synergistically with micronutrients – as part of an orchestra.
Example - -carotene, vitamin C, vitamin E and selenium act as Antioxidants with flavonoids, carotenoids and phenolic compounds.
An orchestra cannot be converted to a solo.
-carotene supplementation to prevent lung cancer did not lower rates of lung cancer – it increased it among high risk groups.
Single agents can be counter productive.

- 32 - Distribution (%) of children by protein –calorie adequacy status
Age (yrs)Age (yrs) % with adequate % with adequate % with adequate % with adequate
calories Vitamins Mineralscalories Vitamins Minerals
1-3 31.8 8.0 15.0
4-6 28.2 10.0 20.0
7-9 28.1 7.5 20.0
10-12 26.0 (B) 9.0 15.0
32.9 (G)
Source: NNMB Reports, 2002

-33 –
Mean intake of one Nutrient iron (mg) by levels of percentage RDA of energy
Details % RDA of energy IronMean ±SD (n)
Women
< 70 9.6 ± 7.50 (1081)(9.2 – 10.0)
70 – 100 13.2 ±8.07 (2567)12.9 - 13.5)
100 17.0 ±9.64 (2034)16.3 – 17.1)
Pooled 13.8 ±8.94 (5682)

-34 –
Mean intake of one nutrient iron (mg) by levels of percentage RDA of energy
Details % RDA of energy IronMean ±SD (n)
Children
1-6 yrs
< 70 5.9 ±4.57 (2898)
(5.7 – 6.1)
70 – 100 9.7 ± 6.46 (856)
(9.3 – 10.2)
100 14.0 ± 9.19 (234)
(12.9 – 15.2)
Pooled 7.2 ± 5.87 (3988)

- 35 -
Supplying additional iron would reduce anemia only if
iron is very deficient and only up to the point where
another factor becomes rate limiting. In the case of
poor societies, other factors- both nutritional and
environmental- are as important. Therefore,
management of nutritional anemia requires Health
and food (providing many nutrients, not just iron).
Instead of putting all nutrients into one food (cereal)
Cereal should be eaten with nutrient rich foods.

- 36 -- 36 -
Further addition of iron in these diets or iron supplements may cause iron overload known to have the following impacts on
1. Oxidative damage, diarrhea, in undernourished populations
2. Infections, like Malaria, TB, HIV,
3. Even deaths
What is required is sources of foods which make the iron available such as
1. Vitamin C rich foods
2. Small amounts of meat which provides haem iron
3. Fill the calorie gap with foods other than cereals
These increase the iron availability by 10 times.

-37 -37 -
Wheat flour fortification
To increase intakes of iron – using whole wheat flour (cereal) - iron availability is only – 1-2%
Other option - chemical addition to whole wheat flour
NaEDTA – to increase iron availability by 2-3 times
However, it increases viscosity of the flour
? Toxicity – and binding with other metal ions
Costly – four times
Ferrous sulfate - without EDTA low bioavailability
alters taste – with EDTA – iron amount have to be decreased net iron intake the same
Elemental iron – Low bioavailability
Fortification of flour in the West is carried out using MAIDA (refined flour)

- 38 -- 38 -
Options – whole country to switch to Refined flour (MAIDA) or
Tolerate Toxicity of EDTA
Safe levels to be calculated in undernourished populations
Intake should not be more than 2.5 mg / kg body weight
At this level of EDTA it does not provide adequate iron for children
No studies on the use of fortified flour in children

- 39 -- 39 -
St.John’s study (Kurpad)
Role of school lunch programme on anemia status of school children
Government school children – given the usual vitamin A and anti-helmenthic
Had the regular school lunch programme (cooked rice, dal, some vegetables)
No iron tablets were distributed
Anemia reduced from 60% to 20%
Important role of providing food on Anemia

- 40 -- 40 -
Millions of tons of cereals will be processed so that a
few mg quantities of a nutrient is added– and only
1-5% is available to humans
Need to re-look at strategy
Studies done in the following countries did not show improvements in haemoglobin after the distribution of iron fortified wheat flour.
SrilankaBangladeshThailandMoroccoIvory coast
India

- 41 –41 –
The National Anemia Prophylaxis Programme
Iron tabletsIron tablets – distributed under medical supervision.
Health care may be accessed (differences between Pemba and Nepal study)
Iron Fortified Wheat Flour – may leave Governments and people complacent.
Research on the relative safety of iron supplements as tablets or elixirs and fortified foods in areas endemic for malaria and other intracellular infections are not known.

- 42 -- 42 -15th ILC - Dr.Aykroyd’s Recommended Diet (1957)
gr.
Cereals- 14 oz - 420
Pulses 03oz - 90
Vegetables 10 oz - 300
Milk 10 oz - 300
Sugar/ 02oz - 60
Oil / ghee 02oz - 60
Fruits 02 oz - 60
Fish / meat 03 oz - 90
Eggs 01 oz - 30

- 43 - - 43 - Average Intake of Nutrients (per day) (Boys and Girls)
Age (yrs)
1 – 3 4 - 6
Mean RDA Mean RDAMean RDA Mean RDA
Protein (g) 20.2 22.0 28.7 30.0
Total fat (g) 10.7 25.0 12.7 25.0
Energy (Kcal) 719 1240 1020 1690
Calcium (mg) 245 400 272 400
Iron (mg) 5.7 12 8.6 18
Vit.A (µg) 129 400 166 400
Thiamin (mg) 0.5 0.6 0.7 0.9
Riboflavin (mg) 0.3 0.7 0.4 1.0
Niacin (mg) 5.2 8.0 7.9 11.0
Vit.C (mg) 17 30 25 40
Free folic acid (µg) 20.3 30 28.8 40

- 44 -- 44 -
Nutrition Rehabilitation Centre (National Institute of Nutrition Rehabilitation Centre (National Institute of Nutrition) Nutrition)
Average intake in hospital of a 7 kg child
Bread 40 gmsRice 50 gmsMilk 500 mlOil 20 mlDal 25 gmssugar 10 gmsBanana 1Eggs 1
1100 cal, 35 gms protein
Approximate cost of a 1000 Kcal diet – Rs 15 /-

- 45 -- 45 -
Rehabilitation diet for undernourished children
Diet - as close to the home diet as possible
Routine Diet at Nutrition ward for children
6 AM Milk8.30 am Khichri11 AM Bread and Milk / egg1.30pm Lunch Rice, Dal,etc4pm Milk / Egg7pm Dinner Rice Dal etc10pm Milk
Extra milk given during night if required

- 46 -- 46 -
The need to provide regular food, familiar as close to home food as possible vs high density packaged food.
1. Problems of processed food which is not produced locally.
2. Half the children of this country will require this
3. Assured supply for years is hard to imagine
4. Local populations will learn to trust only packaged food
5. Women will forget how to feed their children
6. Local employments of millions of women will be affected

- 47 -47 -
Iron content (mg) of common foods in 100g of edible portion
CerealCereal Iron (mg)Iron (mg)Bajra 8.0
Jowar 4.1
Ragi 3.9
Rice, raw, hand pounded 3.2
Rice, bran 35.0
Rice, flakes 20.0
Rice, puffed 6.6
Wheat, bulgar (parboiled) 4.9
Wheat, whole 5.3
Wheat flour (whole) 4.9
Wheat flour (refined) 2.7
Wheat germ 6.0
Wheat bread (brown) 2.2

Pulses Iron (mg)
Bengal gram dhal 5.3
Bengal gram roasted 9.5
Cow pea 8.6
Horse gram whole 6.77
Lentil 7.58
Moth beans 9.5
Rajmah 5.1
Soya bean 10.4
Leafy VegetablesAmaranth polygonoides 27.3
Cauliflower greens 40.0
Manathakkali leaves 20.5
Mint 15.6
Mustard leaves 16.3
Parsley 17.9
Radish leaves table 18.0
- 48 -- 48 - Contd/-
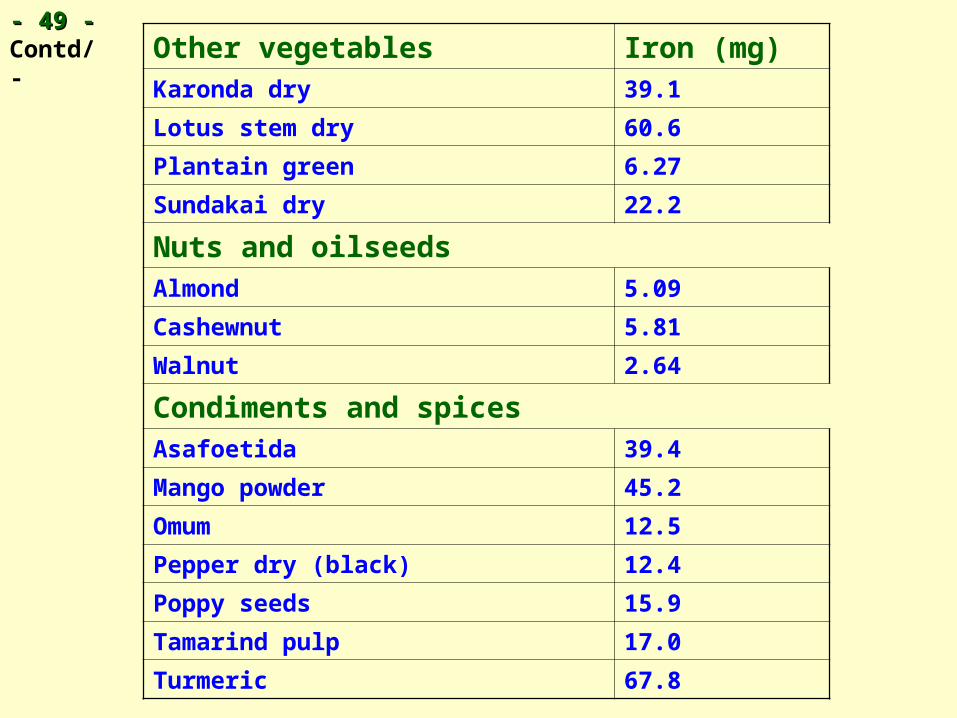
- 49 -- 49 -Contd/- Other vegetables Iron (mg)
Karonda dry 39.1
Lotus stem dry 60.6
Plantain green 6.27
Sundakai dry 22.2
Nuts and oilseedsAlmond 5.09
Cashewnut 5.81
Walnut 2.64
Condiments and spicesAsafoetida 39.4
Mango powder 45.2
Omum 12.5
Pepper dry (black) 12.4
Poppy seeds 15.9
Tamarind pulp 17.0
Turmeric 67.8

- 50 -- 50 -Contd/- Fruits Iron (mg)
Ambada 3.9
Apricot dry 4.6
Raisins 7.7
Seethaphal 4.31
Fishes and other sea foodsBombay duck dried 19.1
Chingri goda, dried 49.6
Crab muscle 21.2
Meat and poultryBeef meat 18.8
Liver sheep 6.3
Mutton muscle 2.5
Pork muscle 2.2