inegrated treatment concepts · web viewsupine training to roll over using resistance to pelvis and...
TRANSCRIPT

INEGRATED TREATMENT CONCEPTS
Copyright The Manual Therapy Institute 1998-2016

PNF for Orthopedics
The following information is based heavily on a course taken with the Institute for Physical Art presented by Vicky Saliba Johnson. All of their courses are highly recommended.
HistoryProprioceptive neuromuscular facilitation (PNF) is an approach to patient care that was originated in the mid 1940’s by Herman Kabat M.D. Margaret Knott joined him in his efforts to discover and define the approach in the late 1940’s. Once understood and defined, they began to teach PNF to graduate physical therapists at the Kaiser Kabat Institute, later to become Kaiser Rehabilitation Center in Vallejo. Dorothy Voss was one of the first students to complete the program. She then joined Maggie and together wrote the first and second edition of the PNF book. Maggie Knott at Kaiser taught PNF for 30 years.
Basic principlesWhile these principles serve as the foundation to the approach of PNF, they are easily integrated with the principles of other schools of manual therapy. The principles are meant to enhance one’s manual skills and create consistency, thus decrease potential for error.The underlying premise for the utilization of the basic principles is to enhance the postural response or movement patterns of the patient. The goal of treatment is to facilitate or “make easy” for the patient to achieve that movement or posture which has been identified to be in a state of dysfunction. The principles can be utilized with or without the patient’s cooperation as they are based on neuro-reflexive responses of the body.Success in the application of the principles to affect a desired response is dependant upon the patient. When considering the patient position, one should consider such factors as support, influence of tone, comfort and desired neuromuscular response.
1. Manual contact2. Therapist body position and mechanics3. Appropriate resistance4. Traction and approximation5. Quick stretch6. Verbal stimuli7. Visual stimuli8. Patterns of facilitation 9. Timing
2

Techniques
1. Rhythmic initiation- therapist passively performs desired movement first then becomes active-assisted.
2. Irradiation- slowly provide isometric contraction and feel for more proximal and central muscle firing.
3. Quick stretch- using appropriate resistance, perform quick stretch while soft tissue is elongated.
4. Isotonics- manual resistance in desired direction.
5. Reversals- resist in desired direction then immediately resist in opposite direction
6. Contract/relax
Activities
1. Anterior elevation/posterior depression (up and forward/ down and back) for UE.
3

2. Anterior elevation/ posterior depression for LE.
3. Supine training to roll over using resistance to pelvis and / or shoulder girdle.
4. Resisted bridge and approximation.
5. Resisted hooklying. Evaluate and treat.6. Resisted hip flexion, abduction, ER and extension, adduction and IR.7. Resisted sit to stand. Stick.8. Resisted gait.
4

9. Axial compression in: standing, sitting, ½ kneeling, standing one leg; other on chair/stool/PT hold 90 degrees.
10. Mirror, video, photo.Muscle imbalance
Muscle imbalance
There is a strong influence of Sahrmann and Kendall in the muscle imbalance approach to movement. The theory is that musculoskeletal problems are caused by motor control problems. Dominant muscles take over and are in need of muscle re-education. For example: wheels on a car are out of balance, which will wear them out unevenly and affect other parts of the car.A state of movement system balance exists when the path of the instantaneous center of rotation during active motion is consistent with the standard kinesiology for the joint for each axis of motion (example: IR, ER shoulder and hip).Equal and opposite forces (force couple) rotate a part around its axis. Change of one of the vectors alters the instantaneous center of rotation of the joint.
Why and how does this happen in the first place?1. Sustained postures2. Repeated micro trauma3. Macro trauma4. Neurological (we are wired a certain way)
Optimal/ideal postural resting alignment (the starting position) is a prerequisite for precise movement. Faulty initial alignment causes changes in the instantaneous center of rotation.(e.g. hinge point in lower cervical or lumbar spine). Alterations in muscle length and strength are factors in faulty joint alignment.If you move funny, it’s going to hurt OR if you are hurt, you are going to move funny.Repetitive movements and sustained positions will cause faults in the movement system elements (musculoskeletal, neurological, biomechanical), which lead to movement imbalance and therefore potential breakdown.
Abnormal or excessive associated movement is imposed on joints other than where movement should occur primarily. The body takes the path of least resistance for motion. Motion takes place where motion is available. Stabilizing structures of those joints are more flexible than those at the primary joint. Reduced flexibility of the proximal LE joints leads to “the tail wagging the dog”.Failure of trunk musculature to stabilize (recruit) properly will lead to faulty alignment. Central neuromuscular improper programming of movement can cause impaired function of peripheral tissue leading to pain syndromes.
5

Improving activation of motor unit firing pattern to speed up muscle contraction is necessary to provide better stabilization and joint protection (lumbar protection mechanism).Muscles that cross more than 1 joint (and therefore having more than 1 action) can loose flexibility as the length for desired single motion is obtained by simultaneously performing another motion (most often rotation)
Physical Therapy is a health profession whose primary purpose is the promotion of optimal human health and function through the application of scientific principles to prevent, identify, assess, corrector alleviate acute or prolonged movement dysfunction ( APTA House of Delegates 1978).
Guidelines for exercise prescriptionThe main purpose of these exercises is to achieve normal range and strength (recruitment) in muscles and to improve postural alignment.The exercises are designed to shorten muscles that are lengthened and to increase flexibility where muscles are shortened.
The emphasis is on precision in performance, which facilitates participation of muscle groups that have been less active because of substitution of synergistic muscles.Examples in upper quarter are the rhomboids vs traps and serratus, and in the lower quarter the PGM vs TFL
As the program incorporates RETRAINING of movement patterns as well as isolated muscle performance, a dynamic as well as static foundation is provided to reinforce alignment changes.The exercises are to be done relatively slowly to aid the precision and specificity that is required and minimize the participation of muscle groups that tend to overplay others.These exercises are to increase participation of relatively dormant musculature.Initially, neither the number of repetitions nor the completion of a motion is important. The emphasis is on how each movement is performed.Increases in repetitions or prolonged hold should be made gradually.This approach puts the responsibility for recovery in the patient’s hands. It is their job to comply with the program.
It is believed to be more important to strengthen what is weak, thereby effectively stretching what is short and tight (example: strengthening weak lower abdominals will effectively stretch short and tight lumbar paravertebrals and iliopsoas). We think that stretching is very important though, as it inhibits other synergistic tight muscles and allows better facilitation of weak muscles. We like to stretch for approximately 2 minutes.
6

Exercises to correct muscle imbalance should emphasize quality of movement rather than quantity.When prescribing exercises, the number of repetitions will vary per individual. A person who is only able to perform a low level program may initially perform 3 different exercises of 1 set of 3-5 reps. Progress as tolerated.It is better perform a few of the most important exercises several times per day instead of many exercises only once a day. The patient spends too much time with faulty movement patterns and therefore needs to perform the correct movement patterns regularly.
Imbalance syndromes
Lumbar Extension/Rotation Syndrome
The most common lumbar syndrome. Typical with recurrent LBP patients.
Signs and symptoms: usually unilateral or at least greater on one side. symptoms increased with extension and or rotation movements of the spine. noticeable in gait or running (tail wagging the dog) poor control and performance of core in preventing lumbopelvic
rotation/extension. functional or structural leg length discrepancy.
Key tests:
Standing: paravertebral muscular asymmetry. hyperlordotic and/or hinge point. increased symptoms when return from forward bending. Axial compression
Supine: Hip and knee flexion (marching): observe pelvic rotation and possible
extension. Hip abduction/lateral rotation from flexion (bent knee fall out): lumbar spine
and pelvis rotates within the first 50% of lower extremity motion. Both legs in extension increase symptoms.
Side-lying: Hip lateral rotation with slight hip and knee flexion (clam): observe pelvic
rotation. May need 1-2 pillows between knees and /or one under waist.
7

Prone: Knee flexion with or without hip extension: observe lumbar hyperextension
and/or rotation. Hip rotation with knee flexed: lumbopelvic rotation occurs within the first
50% of lower extremity motion.
Femoral anterior glide with medial rotation syndrome
The primary movement dysfunction is insufficient posterior glide and excessive medial rotation of the femur during hip flexion. An impaired PICR of the hip joint occurs displayed by upward and medial movement of the greater trochanter during hip flexion. There is impairment of the hip flexor lateral rotators to counteract the hip flexor medial rotators. The stiffness of the hip extensors and the posterior hip joint structures and the excessive flexibility of the anterior hip joint structures as the result of maintained hip extension create a path of least resistance of anterior glide.
Symptoms and signs: Groin pain with hip flexion. Often seen in runners, dancers. Functional or structural leg length discrepancy. Asymmetric hamstring muscles, medial shorter than lateral and/or medial
hamstrings recruited over lateral. Short TFL/ ITB. Hip medial rotation with gait and /or seated knee extension. posterolateral displacement of tibia.
Key tests
Postural assessment: posterior tilt, hip extension, and medial rotation; knee hyperextension, decreased gluteal definition.
Ober test
Thomas test
8

Craig’s test Patient prone. Knee at 90 degrees. Internally rotate hip. Palpate greater trochanter when it reaches parallel or its most lateral position. 8-15 degrees is normal, greater is anteversion and less is retroversion.
Active SLR test for AGMRPatient lies supine with both legs in extension. The therapist passively raises the leg while using the thumb to monitor the inguinal crease. The patient is asked to hold the leg in this position while the therapist lets go. The test is positive if the femur glides anteriorly and medially rotates.
Dominant hamstringDuring prone hip extension: Patient prone and performs hip extension. If the hamstring muscle contraction is evident earlier than the gluteus maximus muscle contraction, then the hamstring is considered dominant.
During seated knee extension: patient performs seated knee extension. Look for hip medial rotation, which would be indicative of a dominant medial hamstring
9

Single leg ¼ squatHave patient do single leg stance and observe from medial rotation of the hip/femur
With patient in quadruped, the pelvis on involved side appears higher at less than 90 degrees of hip flexion and increased lumbar flexion. Femur does not glide posterior or flex easily during backward rocking.
10

Muscle strength testingPosterior Gluteus MediusPatient in sidelying. The lower leg is flexed at hip and knee to maintain the pelvis and back in good alignment. The pelvis is rotated slightly forward, which places the gluteus medius in the best anti gravity test position. It is important to differentiate the posterior gluteus medius because straight abduction often grades normal when the posterior gluteus medius is weak.With the knee extended, the upper leg is placed in abduction, slight flexion and slight external rotation at the hip joint. Do not allow the pelvis to rotate backwards as this will allow the tensor fascia latae and the gluteus minimus to become active in abduction. Even though the pressure may be properly directed against the gluteus medius, the specificity of the test will then be greatly diminished.Weakness of the gluteus medius may become apparent by the patient’s inability to hold the precise testing position, or by the tendency of the muscle to cramp, or by an attempt to rotate the pelvis backwards to substitute with the tensor fascia latae and the gluteus minimus.Therapist applies pressure against the leg near the ankle in the direction of adduction and slight flexion.
IliopsoasPatient is supine. Therapist stabilizes the opposite iliac crest. The leg is slightly abducted, slightly externally rotated and then flexed. Therapist provides pressure against the anteromedial aspect of the tibia, in the direction of extension and slight abduction. This is directly opposite the line of pull of the psoas major from the origin of the lumbar spine to the insertion on the lesser trochanter of the femur.
11

Hip flexor strength testing in sitting
Intrinsic External RotatorsObturator internus and externus, superior and inferior gemelli, quadratus femoris and piriformisTest with the hip in extension as well as with the hip in 90 degrees flexion. Ideally you would like the external rotator strength to be equally strong in hip flexion and hip extension. If they test stronger in hip extension than in hip flexion, it means that the gluteal mm is taking a bigger role in hip external rotation than it should.
Gluteus maximus
12

Hamstrings (medial and lateral) Patient prone. Medial hamstrings: thigh and lower leg medially rotated and knee less than 90 degrees flexion. Lateral hamstrings: thigh and lower leg laterally rotated and knee less than 90 degrees.
Corrective exercises
Marching exercise with blood pressure cuff for biofeedback.Place the cuff under the lumbar spine while patient in hooklying. Pump cuff up to 40 mmHG. Have patient draw umbilicus in and up so that the pressure increases to 50 mmHG. Make sure patient performs a tilt and not a shear. When the patient can do this 10 times holding for 10 seconds each then progress to marching. Alternately lift one leg then the other slowly while maintaining the gauge between 50-60 mmHg.
Clam progression
Phase IPt sidelying. Slowly laterally rotate the top leg. Keep heels together. The motion is at the hip; do not let the pelvis or trunk move. Return to starting position.
13

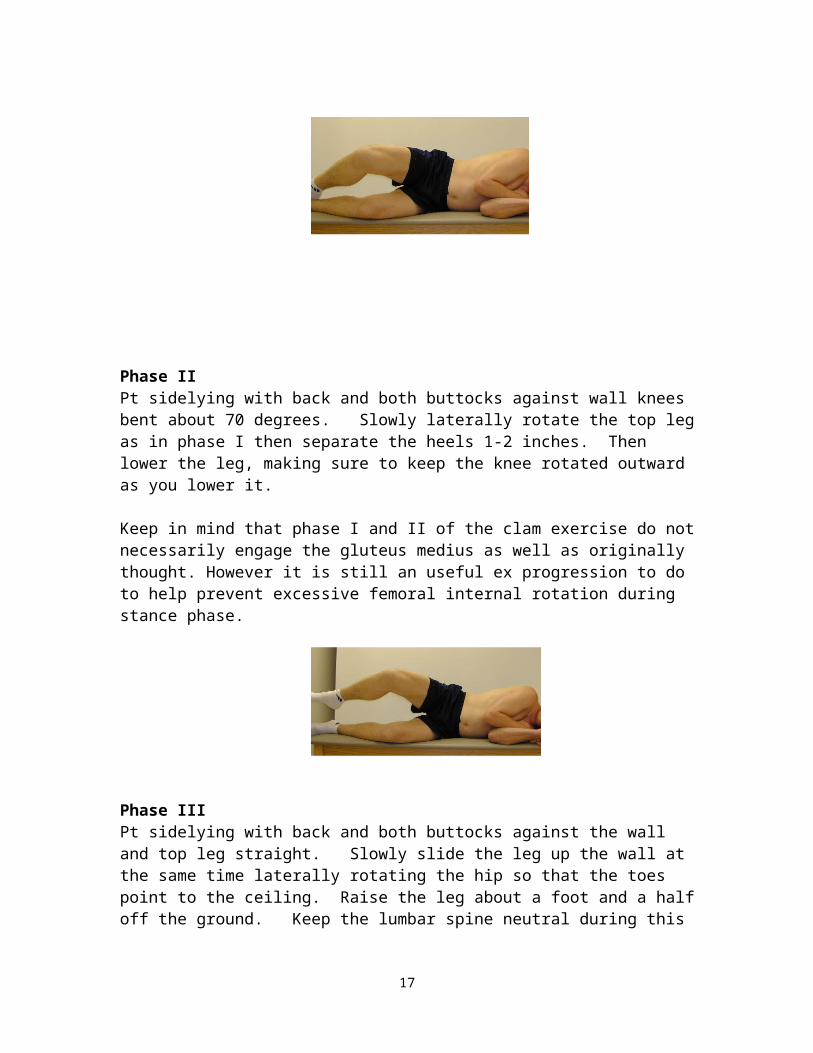
Phase IIPt sidelying with back and both buttocks against wall knees bent about 70 degrees. Slowly laterally rotate the top leg as in phase I then separate the heels 1-2 inches. Then lower the leg, making sure to keep the knee rotated outward as you lower it.
Keep in mind that phase I and II of the clam exercise do not necessarily engage the gluteus medius as well as originally thought. However it is still an useful ex progression to do to help prevent excessive femoral internal rotation during stance phase.
Phase IIIPt sidelying with back and both buttocks against the wall and top leg straight. Slowly slide the leg up the wall at the same time laterally rotating the hip so that the toes point to the ceiling. Raise the leg about a foot and a half off the ground. Keep the lumbar spine neutral during this movement. Keeping the leg rotated outward, slowly lower it to the floor.
14

Prone knee bend extension. Pillow under abdomen if needed, with cuff between pillow and abdomen if needed. Purpose: dissociate hip/low back motion in extension. Place cuff under abdomen. Pump cuff up to 70 mmHG. Have patient draw belly button in and up to decrease pressure gauge to 60-64 mmHG. Slowly bend knee to 90 degrees with slight lateral rotation, then just lift leg off table to about 10 degrees of hip extension. Have patient hold leg for 10 seconds. Do this 5 times and repeat on opposite side.
Standing, flatten back against wall while in squat position then slide your body to the upright position and maintaining a flat back.
Flatten back against wall, arms overhead, grab opposite elbow and sidebend.
15

Single leg quarter squatPurpose: strengthen hip abductors and external rotators. Patient stands with weight equally distributed over both feet. Patellae face anterior (knee over second toe). A mirror helps to give feedback. Shift weight to one foot and lift the other foot by flexing hip and knee. Keep the pelvis level (may need contraction of multifidus) and do not let the trunk lean to one side or rotate. While standing on the leg, make sure that the knee does not turn inward. Tighten gluteal musculature. When able, progress to quarter squat.
Sneaky lungesStagger stance. Step forward with involved leg. Raise heel up on rear foot and forward foot. Bring chest towards knee keeping knee of second toe then outstretch arms and return. Can be made more difficult with rubber /foam disc.
Golfer’s squat. Stand one leg keeping knee over second toe and place golf ball on floor using hip and knee flexion. Return upright then go back to pick up ball. Alternate hands.
Hip hinging Standing with stick and perform hip hinge and squat and sit to stand.
Bent knee fall out. Purpose: stretch adductors, strengthen abdominals, train to move thigh independently of pelvis. Patient supine. One leg straight. Pump cuff to 40, draw abdomen up and in to 50. The other leg with foot on floor, knee bent. Let the knee fall lout to the side, keeping needle between 50 and 60. Pull knee back in starting position.
16
Quadruped with stick and rock backwards
Quadruped with stick, arms and legs alternating
Sitting, extend knee with a few degrees of lateral rotation to treat dominant medial hamstring
17

Strengthening hip flexors-seatedActively lift knee to chest. When necessary, pull knee towards chest with both hands for the last few degrees. Maintain spinal neutral. Let go off the hands, and then slowly lower the knee down to the table. Repeat 5 times
Do not sit with legs crossed in hip flexion, medial rotation, adduction. If have to cross put lateral aspect of leg on opposite leg (hip lateral rotation)
Do not sleep with hip medially rotated, use pillows.
18

19