infections of the feet in diabetes -...
TRANSCRIPT

654 POSTGRADUATE MEDICAL JOURNAL December 1950
SIMONS, D. J., DAY, E., GOODELL, H., and WOLFF, H. G.(i943), Research Pubi. A. Nerv. and Ment. Dis., 23, 228.
SINKLER, W. (I887-88), Maryland journal, i8, i.SLATER, J. K. (1948), Edinb. Med. J., 5S, 173.SMITH, C. B. (I946), Canad. M. A. J., 54, 589.SOLTZ, S. E., BRICKNER, R. M., RILEY, H. A., and SALMON,
L. A. (I935), Bull. Neurol. 7nst. N. York, 4, 432.SPITZER, A. (I9OI), 'Ueber Migrane,' Jena.SPUEHLER, 0. (1946), Schweiz. Med. Wschr. 76, I259.VON STORCH, T. J. C. (1937), Nervenarzt, IO, 469.VON STORCH, T. J. C. (I937), New Eng. J. Med., 217, 247.VON STORCH, T. J. C. (1938), Y. Am. Med. Ass., III, 293.VON STORCH, T. J. C. (I941), Med. Clin. N. Am., 25, 13I7.VON STORCH, T. J. C. (I947), Amer. Practit., I, 63I.SUTHERLAND, A. M., and WOLFF, H. G. (I940), Arch. Neurol.
and Psychiat., 44, 929.THOMAS, W. A., and BUTLER, S. (1946), Am. _J. Med., I, 39.THOMAS, W. A., and BUTLER, S. (1946), Bull. N. York Acad.
Med., 22, 125.TILLGREN, N. (I947), Nord. Med., 33, 502.TILLGREN, N. (I947), Nord. Med., 34, 937.TILLGREN, N. (I947), Acta Med. Scand. (Suppl.), I96, 222.TILLIM, S. J. (i944), Ann. Int. Med., 20, 597.
TODD, R. B. (I854), 'Clinical Lectures on Paralysis, Diseases ofthe Brain and Other Affections of the Nervous System,'London, p. 28i.
TORDA, C., and WOLFF, H. G. (I945), Arch. Neurol. andPsychiat., 53, 329.
TROWBRIDGE, L. S., VON STORCH, T. .J. C., and MOORE,M. (I942), New Eng. J. Med., 227, 699.
UNGER, L. (1940), J. Alergy, 12, 197.VALLERY-RADOT, P., and BLAMOUTIER, P. (1927), Bull.
et Mem. Soc. Med. Hop. Paris, Si, 925.VILLEY, G., and BUVAT, J. F. (I937), Paris Med., I03, I89.VON WASSERMAN, A., NEISSER, A., and BRUCK, C. (I906),
Dtsch. Med. Wchschr., 32, 745.WEISMANN, S. (1924), 'Des Migraines,' Paris.WHITEHEAD, R. W., and McNIEL, E. E. (I935), Am. J.
Psychiat., 91, I275.WHITEHORN, J. C. (I944), Areh. Neurol. and Psychiat., 52, 197.WILSON, D. C. (l925), Clifton M. Bull., II, 71.WOLFF, A. A., and UNGER, L. (I944), Ann. Int. Med., 20, 828,-WOLFF, H. G. (1940), 'Modern Medical Therapy in General
Practice,' Baltimore.WOLFF, H. G. (I948), ' Headache and other Head Pain,' New York.WOLFF, H. G., IIARDY, J. D., and GOODELL, H. (1941), Y.
Clin. Invest., 2o, 63.
INFECTIONS OF THE FEET IN DIABETESWith Special Reference to Those Due to Gas-Forming Organisms
By E. C. B. BUTLER, F.R.C.S.The London Hospital
It is a common error to regard all infections ofthe feet occurring in diabetic patients as cases ofincipient gangrene. Most of these patients can besafely treated at home or in the out-patient de-partment. Only a minority need admission tohospital, and of these only a small proportion havetrue necrosis or require a major amputation. Theincidence of severe infection has been much re-duced since the introduction of penicillin.
Patients who require in-patient treatment mayfor convenience be divided into two groups,although the dividing line between the two is oftendifficult to determine.Group i consists of those patients who have
signs and symptoms of senile obliterative arterialdisease. The diabetic cases differ only in havinginfection as a constant feature.Group 2 consists of cases of diabetes com-
plicated by infection of the feet, the circulationbeinggood, the popliteal pulse being readily feltand oscillometer tests showing good pulsationbelow the knee.
Group IFollowing mild trauma an infection starts on
one or more toes and similar lesions may arise onthe heel or elsewhere on the foot. Under favour-able circumstances and treatment the infection will
resolve but in other instances it may spread or goon to necrosis, which in turn may remain localizedor involve the remainder of the foot.When spread of the infection occurs there is
little local reaction; formation of pus is unusualand there is no definite line of demarcation be-tween diseased and healthy tissue. On examina-tion, these patients are likely to show signs ofthrombosis in the femoral or popliteal vessels.Popliteal pulsation is absent, oscillometer readingsshow minimal or absent records below the kneeand the limb rapidly becomes blanched when ele-vated. Radiography may reveal widespreadmedial calcification of the main vessels.
TreatmentThe patient is best treated as an in-patient. A
swab from the infected area is sent to the laboratoryso that the invading organisms can be identifiedand their sensitivity established.
Staphylococcus aureus and haemolytic and non-haemolytic streptococci are commonly found; butgram-negative bacilli may also occur. Not in-frequently various types of anaerobic organismsare present and these may cause serious spreadinginfections. Some of these organisms are penicillinresistant and it is a wise precaution to learn with-out delay what drug or combination of drugs is
by copyright. on 14 June 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.302.654 on 1 Decem
ber 1950. Dow
nloaded from
BUTLER: Infections of the Feet in Diabetes
likely to prove effective should the infection be-come severe. The affected limb should be kept atroom temperature and rested on a soft pillow;care must be taken of both heels since pressurenecrosis is very liable to occur. Intermittentvenous occlusion has not in our experience beenhelpful in these cases, but active physiotherapy aidsthe circulation and helps to prevent the patientdeveloping further thrombosis. Local treatmentshould consist in removing any slough which ispresent or in cutting away any obviously necroticphalanx. It is a mistake to leave tenacious ad-herent sloughs on the ends of toes; underneaththese sloughs the infection persists and may spread.Formal amputation of toes through the metatarsophalangeal joints is contraindicated since it islikely to lead to a rapid spread of the infection, orto necrosis.
Local application of penicillin and sulphonamidepowder is not of great value in the presence ofnecrotic tissue; the powder tends to cake andpenetration is limited. Until the slough hasseparated hypertonic saline dressings or eusolcompresses are often useful. When there is noslough the part should be kept dry by means of aspirit dressing.A course of systemic penicillin may be valuable
in preventing cellulitis, but it is not necessary tocontinue penicillin therapy indefinitely in theabsence of an acute infection or while awaiting theseparation of necrotic areas.
In most cases the infection will subside and thenecrosis, if present, will remain limited to one toe.If the patient is fortunate the dead area willseparate spontaneously with, perhaps, slightjudicious aid.The indications for amputation in this group are
similar to those for patients with uncomplicatedsenile gangrene, namely spreading necrosis andintolerable pain. Fulminating infection is some-times an additional indication and is consideredlater.The average age of patients in this group was
64, the oldest being 78 and the youngest 5'. In
TABLE I
RESULTS IN i8 CASES WITH ABSENT POPLITEAL PULSATION
IAlive Dead
Above knee amputation .. 6 4 2*Below knee amputation .. o o oLocal removal of slough .. 6 6 oNo surgery .. .. 6 it
I8 15 3
* One heart failure, one gas infection.t Heart failure.
TABLE 2
RESULTS IN 22 CASES WITH POOR CIRCULATION BUT INWHOM NO NoTE WAS MADE OF THE POPLITEAL PULSATION
Alive Dead
Above knee amputation .. I I OBelow knee amputation .. o o oLocal surgery .. .. 9 7 2No surgery 1.. .. 2 12 0
22 20 2
* Both gas infections.
a similar series of arterio-sclerotic patients withgangrene the average age was 63.
Group 2. Cases with Popliteal Pulse PresentIn this group, since the blood supply is good,
infection rarely leads to gangrene except in thosecases where gas infection supervenes. Abscessformation is common and infection readily tracksup the layers of the foot causing sloughing of thetendons and fasciae. Osteomyelitis with sequestra-tion of the affected toes frequently occurs.A number of these patients also have diabetic
neuritis; this manifests itself by the presence ofperforating ulcers, commonly at the ball of the bigtoe. An X-ray invariably shows underlying in-fective arthritis with osteomyelitis of the adjacentbones.
In one of our cases the neuritis was so markedthat the patient developed a fracture of one of hermetatarsals without complaining of pain or dis-comfort. The healed fracture was discoveredwhen the foot was X-rayed for a perforating ulcer(Fig. i). A perforating ulcer may remain quiescentfor a long time save for a persistent painless dis-charge. Suddenly for no apparent reason infectionlights up and may prove the starting point of arapidly spreading cellulitis. We have also foundthat a small number of this group suffer from in-creasing blindness due to diabetic retinopathy.The double handicap of infected feet and im-pairment of vision is a hard burden. Every effortmust be made to avoid a major amputation on thesepatients as it is difficult for them to use crutches.In our experience both retinopathy and diabeticneuritis have occurred only in Group 2 cases,although it is possible that both complications mayarise in patients with arterio-sclerosis.
TreatmentOn admission to hospital a swab is taken from
the infected area. In this group chemotherapy islikely to be more valuable than in Group i, andan accurate bacteriological diagnosis is essential.Systemic penicillin may often be combined with acourse of sulphonamide and it is probable that in
December 1950by copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL
the future aureomycin will be a most valuableaddition in the more severe types of anaerobic in-fection. McKitterick and Root (1936) wereamong the first to emphasize that 'if the bloodsupply of a diabetic patient's foot is good enoughto form pus then it is good enough to tolerate.localsurgery.' This important statement should berememb( rAd.
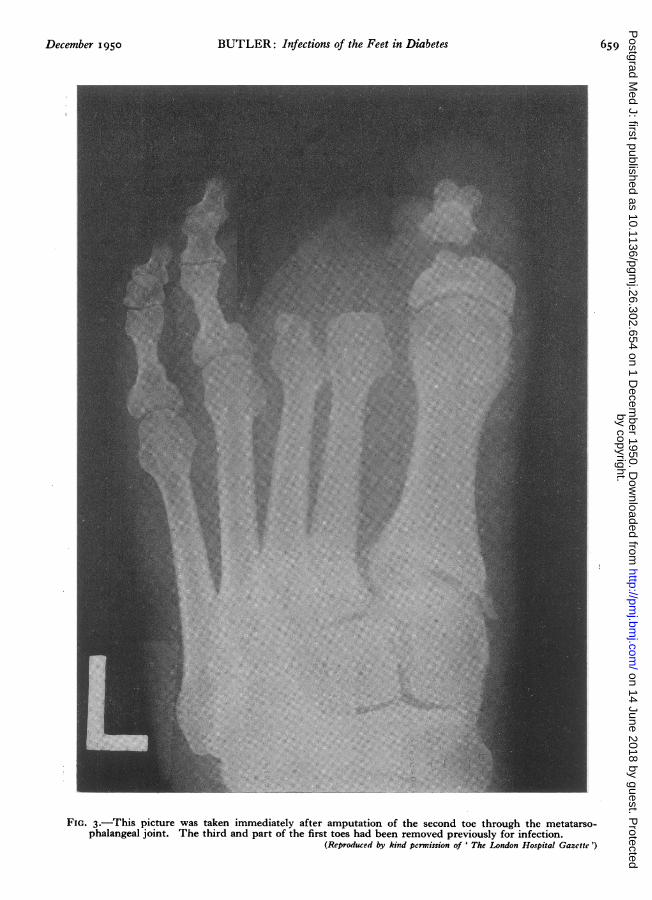
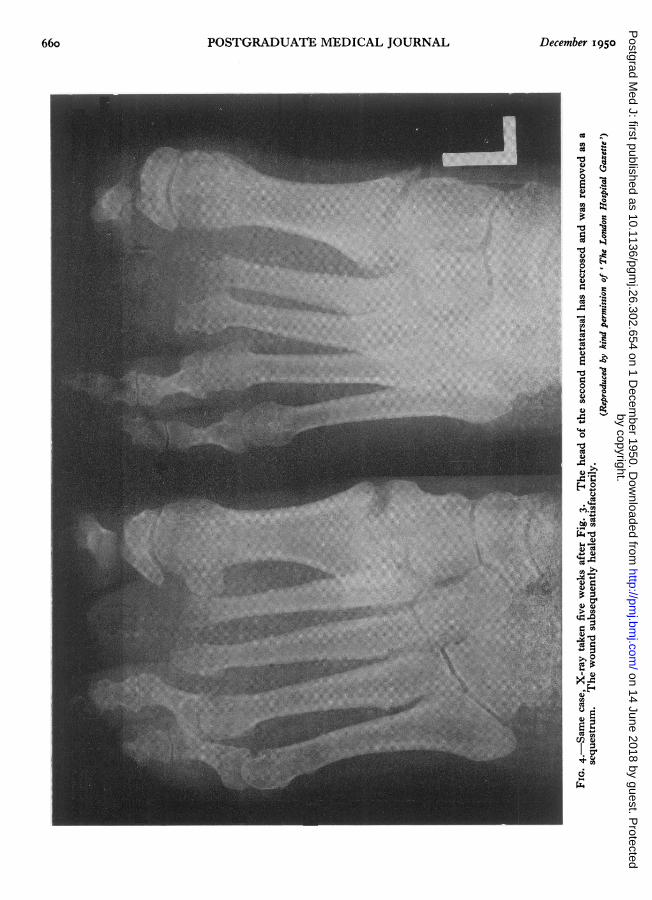
Abscesses should be drained freely in exactly thesame manner as in infections of the hand. Theincisions must be adequate. In the foot'the websbetween the toes commonly require drainage andthence the incisions may be prolonged on to thedorsum or sides of the foot. Drainage via the soleshould be avoided where possible. Necrotictendons and fascia must be completely excised ifthe wound is to heal; this may be done at a secondoperation if the field is obscured by pus. Incertain cases, once the acute phase is over, formalamputation of the diseased toes or metatarsals cansafely' be performed (Fig. 2). These wounds maybe sewn up confidently provided that all the dead'tissue has been removed. Systemic penicillinshould be continued until the wounds havehealed.When a toe has been amputated it is wise to
excise at the same time the head of the underlyingmetatarsal. If this is omitted the cartilage mayslough since a part of its blood supply derives fromthe excised joint (Figs. 3 and 4). In two cases wehave carried out amputation of the big toe andthree-quarters of the first metatarsal for perforatingulcers below the first metatarso-phalangeal jointswith osteomyelitis of the adjacent bones. Theyhave healed well. Walking has been satisfactorywith special surgical shoes. In cases where thefoot has become useless amputation at a higherlevel must be considered.
Syme's amputation has lately fallen into dis-repute in this country but we have found it asatisfactory procedure in certain of these patients.The late Dr. Leyton who was for many years incharge of the diabetic clinic at the London Hospitalwas always very insistent, in the light of his ex-perience, that his patients had as conservative anamputation as possible. We have followed histeaching in this matter. In cases of doubt it issafe to perform a below-knee amputation at thesite of election provided the oscillometer showsadequate pulsation in this region.The average age of Group 2 patients was 54;
the eldest was 67 and the youngest 32.
Gas Cellulitis and GangreneThis condition may be defined as infection of the
lower limbs in diabetic patients by gas-formingorganisms other than the clostridiae.
TABLE 3
RESULTS IN 25 CASES WITH PALPABLE POPLITEAL PULSE
Alive Dead
Above knee amputation .. o;Below knee amputation .. 4 2 2Syme's amputation .. 3 3 0Local surgery .. .. 8 8 oRemoval of metatarsal .. 3 2No surgery .. .. 6 6 o
25 21 4
Three of the deaths were due to gas infection and oneto cerebral haemorrhage.
BacteriologyA variety of organisms has been encountered.
Aerobic cultures have shown the common gram-positive cocci, but bacilli of the colon group arealso found in large numbers. Faecal strepto-cocci occurred in one case. Anaerobic cultures areusually disappointing. The most probable patho-gens responsible are anaerobic streptococci, faecalstreptococci and fusiform bacilli. Clostridial in-fection was not seen in all cases examined bacterio-logically.
SymptomsThese infections usually start from a previous
focus of infection such as a perforating ulcer;occasionally, however, they may arise de novo.The patients rapidly become very ill and in ful-minating cases death may occur in a few days. Onadmission there is high fever and a rapid pulse.The urine is loaded with sugar and containsacetone. The glycosuria tends to persist despitemassive doses of insulin. At first the cellulitis re-mains localized but soon spreads up the foot intothe leg. Gas is readily detected in the sub-cutaneous tissues and can be demonstrated radio-logically. If the disease is unchecked true gasgangrene develops, the muscles becoming necroticand putrid with bubbles of gas between the fibres.
In a short time the lower limb may become amass of stinking necrotic tissue. Death usually re-sults from a combination of severe diabetes,toxaemia and terminal bronchopneumonia. Bac-teraemia does not seem to occur; none of ourcases developed a positive blood culture.These severe infections may occur in either of
the two groups we have described; indeed themost severe cases have been in patients whoseblood supply has been adequate. The followingcase histories illustrate the aetiology of such in-fections and bring out the problems involved.
Case IWoman aged 55. Several months increasing
656 Decetnber 11950by copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from

BUTLER: Infections of the Feet in Diabetes
FIG. i.-The typical appearance of the bones and joint underlying a perforating ulcer of the big toe.Healed fractures of the fourth and fifth metatarsals also present.
(Reproduced by kind permission of ' The London Hospital Garzette')
December 1950 657by copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
.
':tI;
T
FIG. 2.-An X-ray of the same foot after amputation of three-quarters of the metatarsal, together with thebig toe. The wounds healed by first intention and the patient walked well with a special shoe.
(Reproduced by kind permission of ' The London Hospital Gazttte ')
658 December 1950by copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from
BUTLER: Infections of the Feet in Diabetes
FIG. 3.-This picture was taken immediately after amputation of the second toe through the metatarso-phalangeal joint. The third and part of the first toes had been removed previously for infection.
(Reproduced by kind permission of ' The London Hospital Gazette')
December I950 659by copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL December 1950
0
E ES
0 -
o
4)
Ca
(44)
C0)
'-
0h '0(.4
C)
4-)
od 1
4)-
0
(4
C4)4
0
1,0S
4.4
C)
C4E
'4.'4)
Ca
(4,
(4 4
> Ca
40
C124
6l
66oby copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from
rBJTLtR: Infectdons of the Feet in Diabetet
thirst. Three weeks painful toe. No previousdiagnosis of diabetes.
14.I2.38. Patient admitted to hospital, an illdehydrated woman with sugar and acetone inher urine. The popliteal pulse was felt; therewas an area of infected necrosis of her fifth righttoe. The diabetes was controlled with insulin.In spite of intermittent venous occlusion and acourse of sulphanilamide the infection spread andthe foot became gangrenous, gas being present.
26.12.38. Amputation of leg below knee withsuture of the flaps. Gas gangrene rapidly appearedin the stump and she died three days later.The post-mortem examination showed gas
gangrene with gas in the liver.Comment. Two mistakes were made in the
treatment of this patient. Amputation was per-formed far too near the site of infection and theflaps were sutured instead of being left open.
Case 2
Man aged 59. Two ,weeks painful heel follow-ing slight injury. No previous diagnosis ofdiabetes.
I4.II.43. Admitted to hospital with diffusecellulitis of the foot. The popliteal artery couldnot be felt. The urine was loaded with sugar andacetone.
15.JI.43. Gas infection was obvious; incisionswere made in the foot and leg, gas and pus wereliberated. A course of sulphonamide was com-menced. Culture showed a haemolytic strepto-coccus as well as staphylocossus aureus.
I6.II.43. The man died.Post-mortem report: Gangrene of leg; pan-
creatic calculi.Comment. It is difficult to see what further
could have been done. An emergency amputationmight have been carried out but would probablyhave proved fatal.
Case 3Female aged 68. Known to be diabetic. Ten
days malaise with pain in one foot.20.5.47. Admitted to hospital; temperature
1000, pulse I00. Urine full of sugar. There wasdiffuse cellulitis of one foot but the popliteal arterycould be felt. Cultures from the foot: Staphylo-coccus aureus. Anaerobic cultures: No growth.
Treatment. Penicillin; 200,000 Units was givenfour hourly.
25.5.47. Two large incisions made in foot andleg. Gas and pus liberated. Her condition im-proved considerably and a line of demarcationappeared below the knee.
i6.6.47. Amputation of the leg below the knee,flaps not sutured. For ten days she remain-'ed'wellthen her diabetes became uncontrolled, and
although the leg infection did not recur she diedof bronchopneumonia.No post-mortem examination.Comment. The gas infection was checked by
penicillin and surgery; unfortunately the diabetesrelapsed after removal of her gangrenous leg.
Case 4Man aged 57. Since 1947 had been treated in
hospital for severe diabetes with infections of thefeet; these had cleared up with chemotherapy anddrainage. For two weeks he had had a painfultoe.
30.8.48. On admission, an ill man with severediabetes, there was gross swelling of one foot ofwhich one toe was gangrenous. The diabeteswas not controlled with insulin. The poplitealpulse was palpable.
Treatment. Penicillin, one million units daily,in spite of which the cellulitis spread and gas be-came evident. Amputation was refused.
I8.9.48. Left leg drained by two large in-cisions; gas gangrene of muscles present. Culture:Staphylococcus aureus and streptococcus faecalis.B. coli also present. A blood transfusion wasgiven. After drainage his condition improved fora time but later relapsed.
21.9.48. Amputation performed through thethigh; flaps not sutured. Patient collapsed anddied two hours after operation.Post-mortem report: Toxaemia, diabetes.Comment. The infection was partially checked
by treatment; the optimum time for amputationwould have been when his condition improvedafter drainage. These patients are very ill andmajor operations are always hazardous.
Case 5Woman aged 45. Known diabetic for many
years. Controlled by insulin. Five years a per-forating ulcer under one big toe. One week in-creasing pain and swelling of big toe.On admission, 1948, ill woman. Temperature
I020, pulse Ioo. Severe glycosuria. One footwas sWollen with a perforating ulcer of the bigtoe. Her popliteal artery was palpable. X-rayshowed calcification of the vessels of the foot andleg and gas in the foot.
Treatment. Penicillin, 250,000 units three-hourly for four days. At the end of which timeno further spread had occurred. A large abscesswas drained on the dorsum of her foot. Culture:Staphylococcus aureus and anaerobic streptococci.Three weeks later a sequestrum was removedfrom her toe. She has remained well since.
Comment. This patient's infection fortunatelyresponded to penicillin; without this drug shemight well have lost her leg, if not her life,
b)ecember I1950 66iby copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL
Case 6Man aged 54. Two years known diabetic. Two
months infected toe; two weeks worse.On admission, I ill man with glycosuria and
cellulitis of one foot. His popliteal artery waspalpable. Culture from the foot: Non-haemolyticstreptococcus.
Treatment. One million units of penicillindaily. Despite this therapy his infection spreadand he suffered intense pain. The odour of thefoot became very offensive although no actual gaswas demonstrated. A below-knee amputationwas carried out; secondary suture of. the flapsbeing carried out on the fifth day. The woundhealed without suppuration.
Comment. This case has been included as itshows the ideal treatment to be adopted.in suchcases whenever practicable. If the circulationbelow the knee had been poor, then a thigh am-putation would have taken the place of a below-knee one.From these case records it is obvious that we
are dealing with a very serious and often fatal in-fection. In many ways they resemble those casesof gas cellulitis seen after war wounds, although thebacteriology is not identical, but they are moreserious because they occur in old and debilitatedpatients. Moreover, a higher percentage terminatein true gas gangrene of muscle than did thosefollowing war injuries.
In our view the principles of treatment of suchcases should be:
i. The infection must, if possible, be controlledby large doses of penicillin. If there is no rapidresponse to this drug another antibiotic must beadded, aureomycin being the most promising at thepresent time.
2. Immediate surgical intervention is usuallyunwise, but as soon as pus has formed free drainagemust be carried out.
3. Emergency amputations before the infectionhas been controlled are dangerous and may befatal.
4. Should amputation be required the flaps mustnever be sutured, they should be loosely tied to-gether over a pack; secondary suture can be doneon or after the fifth day in favourable circum-stances.
5. Blood transfusions are valuable to counter-act the progressive anaemia which is usuallypresent.
There is no doubt that the cases treated withpenicillin showed greatly improved results.Although twb of these four cases died, in all theinfection was checked at least temporarily by acombination of chemotherapy and surgery. Itwas impossible to control the glycosuria in thesepatients until the infection had been overcome;the demand for insulin then fell dramatically.
TABLE 4
REsULTS OF NINE CASES OF GAS INFECTION
Sex liteal Chemotherapy Surgical ResultArtery Tramnt
Male, Not Sulphonamiide. Amputation Diedfelt thigh
Female' Felt Sulphonamide Amputation Diedleg
Male Felt Penicillin Amputation Diedthigh
Male Not Sulphonamide Drained Diedfelt
Female Felt Sulphonamide Amputation Livedthigh
FeMale Not Sulphonamide Drained Diedfelt
Female Felt Penicillin Amputation Diedleg
Male Felt Penicillin Ainputation Livedleg
Female Felt Penicillin Drained Lived
Conclusionsi. This paper is based on a series of 62 patients
treated as in-patients at the London Hospital.There were nine deaths, six from gas infection,two from cardiac failure and one from cerebralhaemorrhage.
2. Diabetic patients with infections of the feetcan be divided into two groups; those with arterio-sclerosis and those in whom the vascular supplybelow the knee is still good.
3. The treatment of the first group is that ofarterio-sclerosis in general, but infection is alwaysan added complication.
4. The treatment of the second group is basedon the usual surgical principles of the treatment ofsepsis. Gangrene is rare and local measures areoften successful.
5. The dangers of gas cellulitis and gangrene inboth groups have been discussed. Nine cases arereported with six deaths.
By courtesy of the' Editors of the.' London Hospital Gazette '
66:z December i95aby copyright.
on 14 June 2018 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.302.654 on 1 D
ecember 1950. D
ownloaded from