infectious myelopathy
TRANSCRIPT
INFECTIOUS MYELOPATHY
DR.SARATH MENON.R, MD(Med.),DNB(Med.),MNAMS
DM RESIDENT,
DEPT. OF NEUROSCIENCES
AIMS,KOCHI.
INTRODUCTION
Infections and secondary inflammatory changes
play an important role
Direct neuronal invasion
Molecular mimicry
Myelopathy- spinal cord dysfunction of any
etiology ,intrinsic or extrinsic
PRESENTATION
Acute transverse myelitis
Acute flaccid paralysis- AHC, motor roots
APPROACH
History & physical examinations
Tempo of illness
Exposure
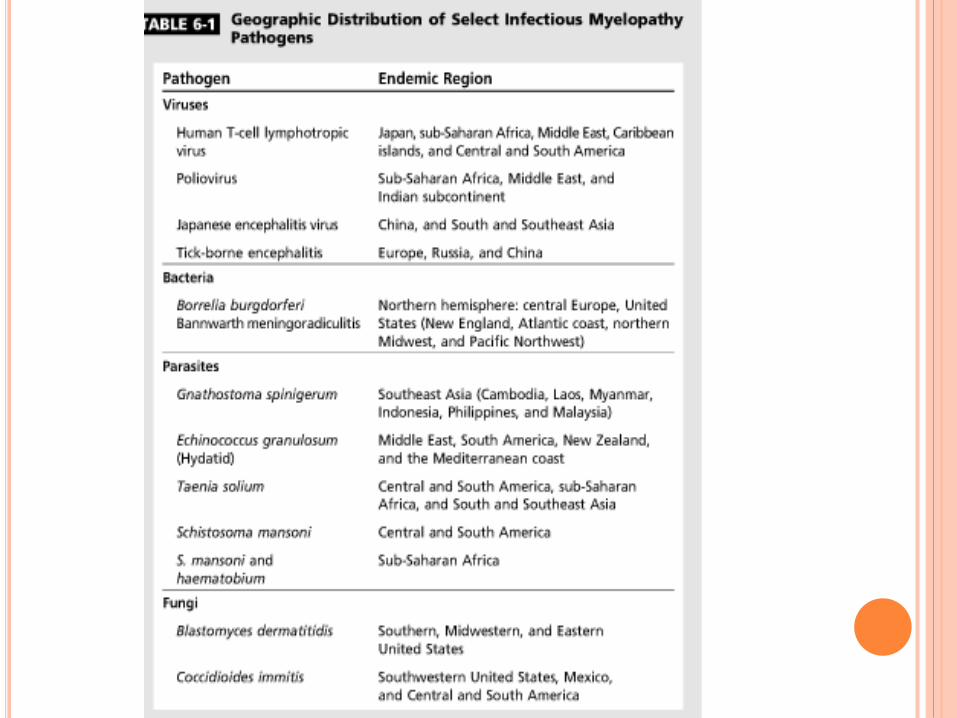
Demographic- endemicity
Host immune status
Ancillary test
Diagnosis & Rx

PARAINFECTIOUS ETIOLOGY
30 -60% infective myelopathy preceeded by
systemic infectious process
Molecular mimicry-
cross reactivity with host antigen in spinal cord
Usually 2-4 wks after infection
Dx- CSF IgG index,OCB
Serology & specific antigen in csf /serum
Rx-
Iv steroid
Refractory cases- IVIG,cyclophosphamide or
rituximab.
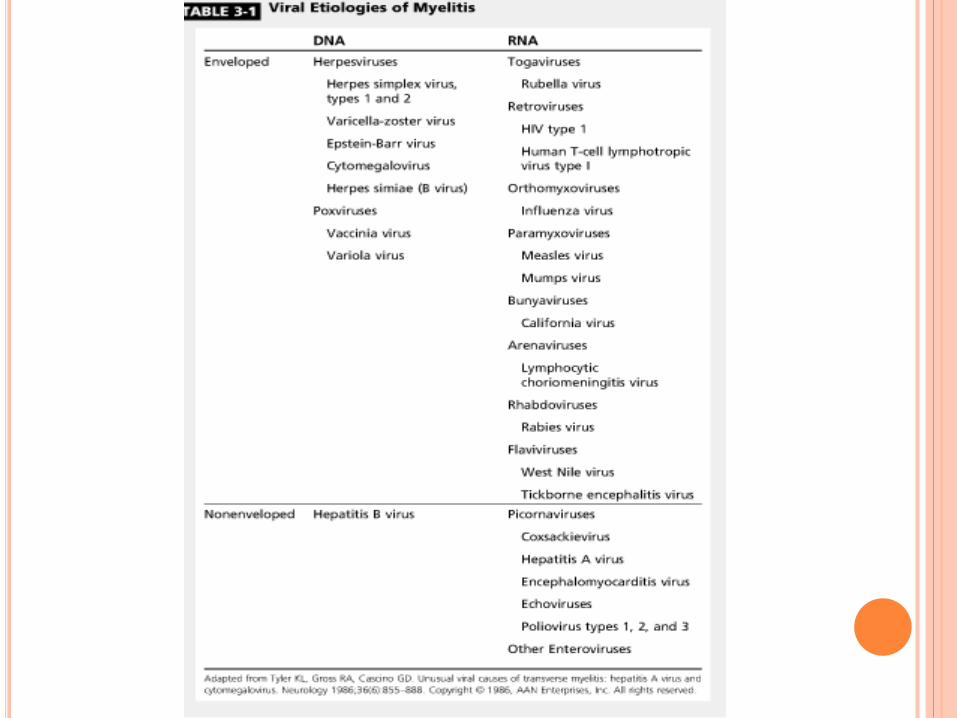
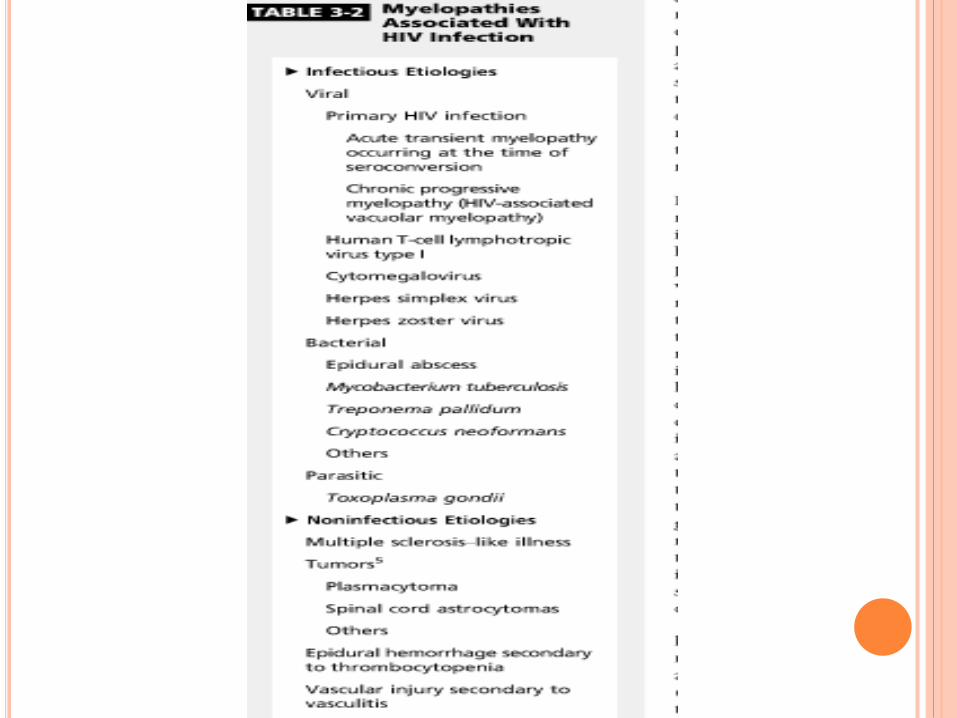
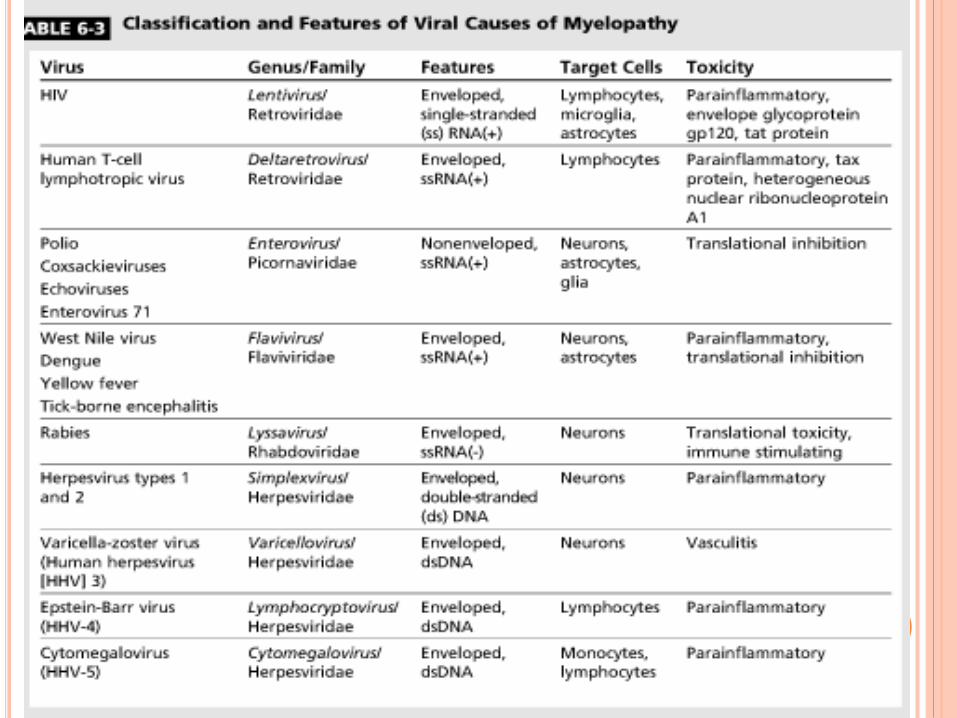
CAUSATIVE AGENTS
Viral
Bacterial
Parasitic
Fungal
RETRO VIRUSES- HIV
CNS – lymphocytes,microglia
Crosses BBB
Neurotoxicity by viral proteins
Chronic pro inflammatory state
CD4 < 200- HIV – vacuolar myelopathy
HIV –VACUOLAR MYELOPATHY
Slow progressive,painless myelopathy
LL weakness,gait difficulties,spasticity,erectile
dysfunction,mild paresthesia
Urge incontinence,urgency- later
Impaired proprioception
LL disproportionately affected.
Diagnosis of exclusion in HIV + pts.
Acute presentation,spinal level ,prominent pain ,UL
prominently involved- alternate diagnosis
D/D- oppurtunistic infection,neoplasms,VB12 def.
Imaging-
Usually normal.
Spinal cord atrophy
Findings similar SACD
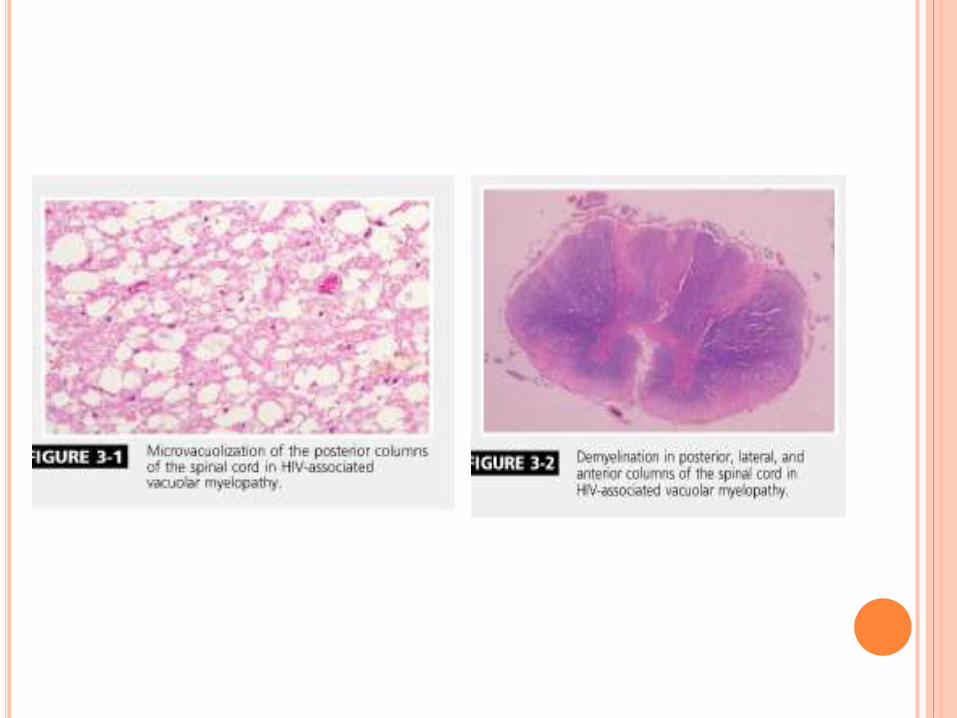
Microscopy-
spongy,vacuolation of myelin
lipid laden macrophages
Rx-
HAART reduced incidence
No response to ART,B12 or IVIG,steroids
13
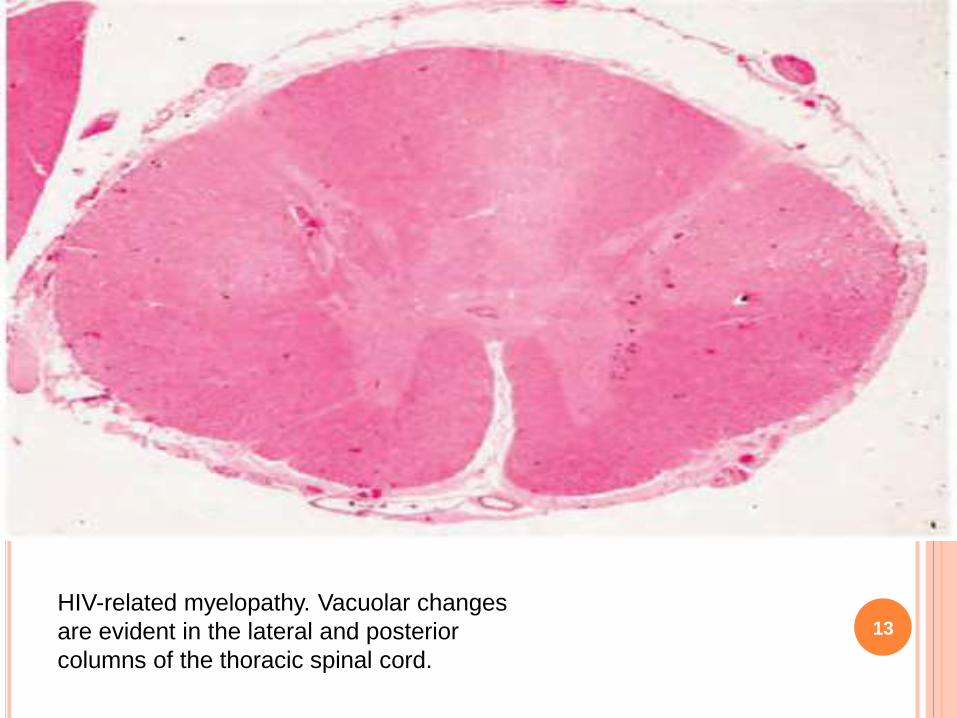
HIV-related myelopathy. Vacuolar changes
are evident in the lateral and posterior
columns of the thoracic spinal cord.
HTLV-1 (HAM/TSP)
4% HTLV-1 will develop
Female predominance
CD8 + Tcell neurotoxicity or molecular mimicry
Clinical features
- insidious ,slow progression
- LL spasticity
- prominent bladder/bowel involvement
- UL weakness insignificant
Diagnosis
- Clinical,demographic,serology
- csf- lymphocytic pleocytosis,OCB+
Confirmation- Western blot
PCR- peripheral blood- distinction & viral load
Imaging
-Focal T2 Hyperintensity in lower cervical cord
-contrast enhancement+
- close d/d to MS
- cervical/thoracic cord atrophy
TREATMENT
No effective clinical trials to date.
Steroids
INF-alpha, cyclosporine,azathioprine- effective
early – limited evidence
HAART
ENTEROVIRUSES
Ubiquitous RNA virus
Produce acute flaccid paralysis
Poliovirus
- AHC affection
- Subsaharan Africa,middle east,Indian subcontinent
- Fever,menigismus,asymmetric flaccid paralysis of LL
proximal > distal over 2 days
- Post polio syndrome
- Slow progressive recrudescence
- Severity of initial disease
ENTEROVIRUS 71- EV 71
AFP similar to polio
Asia –pacific
Children
Fever ,rash – paralysis over 3-5 days
Mri= T2 hyperintensity in lower brainstem,cerebellum
CSF- lymphocytic pleocytosis
No specific rx
IVIG -tried
FLAVIVIRUS- WEST NILE VIRUS
Polio-like paralysis
Mosquito vector
Fever—myelitis—over 2-8 days
Flaccid paralysis, respiratory,bladder +
Risk factor
Age > 50 yrs,immunosuppression
WNV – directly affect AHC
21
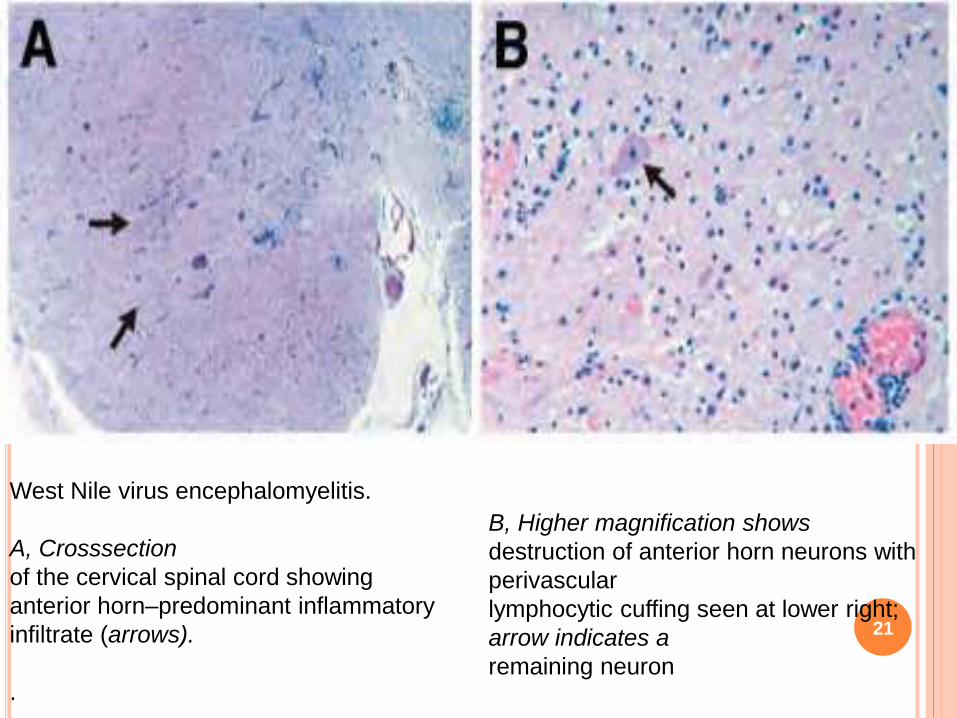
West Nile virus encephalomyelitis.
A, Crosssection
of the cervical spinal cord showing
anterior horn–predominant inflammatory
infiltrate (arrows).
.
B, Higher magnification shows
destruction of anterior horn neurons with
perivascular
lymphocytic cuffing seen at lower right;
arrow indicates a
remaining neuron
Diagnosis
-peripheral leukocytosis,thrombocytopenia,transaminitis
CSF- PMN /mononclear pleocytosis,elev.protein,sug-nl
- IgM –sensitive/specific
- serology
-Spinal cord imaging-normal
- Rx
- Supportive,no specific
- anecdotal- steroids
RABIES
2/3rd –furious/encephalitic,1/3rd –dumb/paralytic
Paralytic-
GBS like presentation—encephalopathy—death
Considered in exposure to animal bite esp.bat
PCR- Skin biopsy from nape of neck-specific
Serology
Virus amplification from skin,saliva,CSF
Supportive rx.
Prophylaxis
HERPES VIRUSES-HSV1&2
HSV1 &2 – myelitis
HSV-2 related myelitis-adults
Elsberg syndrome-reactivation of HSV-2
inflammation in dorsal roots + spinal cord = radiculomyelitis
C/f :
- subacute lower extremity weakness may ascend
- Numbness or tingling in lumbosacral dermatome
- Urinary retention
Acute necrotising myelopathy- severe form seen in
immunocompromised
Flaccid paraplegia+ areflexia
Diagnosis
- CSF-lymphocytic pleocytosis with raised protein
Necrotizing myelitis- PMN leukocytosis
CSF-PCR amplification of DNA
Imaging
- Spinal cord edema
- T2 hyperintensity+CE of radicular roots & cord
Rx
- Iv acyclovir x 14 days f/b oral acyclovir /valacyclovir
- Steroids –role uncertain
- Complete recovery is posssible
- 20% cases,recur

VZV
Myeloradiculitis on reactivation-immunocompromised
Necrotising vasculitis + demyelination
Zoster preceeds, cases with no rash
Asymmetric paraparesis + sensory loss- days to wks
CSF-
Mononuclear pleocytosis ,elevated protein
Anti-VZV IgM assay in CSF-sensitive
PCR- rapid
Imaging- T2 hyperintense in cord = dermatome
Rx
iv acyclovir + steroids
CMV
Imunocompromised- HIV – CD4<100cells/microL
Lumbosacral polyradiculomyelitis-
supf.meningitis-> nerve roots & spinal cord
Necrotizing myelitis
Imaging-
cord edema+root edema+ CE
meningeal thickening+clumping of roots
CSF-
PMN pleocytosis+elev.protein+ low sugar
Rx
IV ganciclovir+ foscarnet
Poor prognosis
EBV
Children / young adults
Immunocompromised –transplant
Spectrum – aseptic meningitis
meningoencephalitis
cranial/peripheral neuritis
GBS & myelitis
Myelitis- 2-3 weeks after primary infection
flaccid paraparesis,sensory level,bladder+
CSF-
mononuclear pleocytosis,elev.protein,sugar-nl

Serology –EBV DNA
CSF-EBV DNA PCR
Imaging-
T2hyperintensity+ce+nerve thickening
Rx
- Acyclovir-little effect on clinical course
- steroids
BACTERIAL- SYPHILIS
Meningovascular-cord infraction-endarteritis-rare
Tabes Dorsalis
Post antibiotic era- less incidence
c/f-
subacute/chronic – sensory ataxia+
loss of vibration,joint position
lancinating pain+
hyperreflexia,charcot joint,AR pupil
Imaging-
cord atrophy
non enhancing T2 hyperintensity-posterior cord
SYPHILIS-OTHER FORMS OF MYELOPATHY
Hypertrophic pachymeningitis
Spinal cord Gumma
AHC
Syingomelia
Aortic aneurysm –sec AHC
Charcot vertebra-cord compression
SYHILITIC MENINGOMYELITIS
Current era, most common spinal cord d/s
Men-25-40 yrs
Avg.6yr after infection
Progressive spastic ,asymmetric paraparesis
Imaging-
T2 hyperintensity central cord +CE
DIAGNOSIS & RX
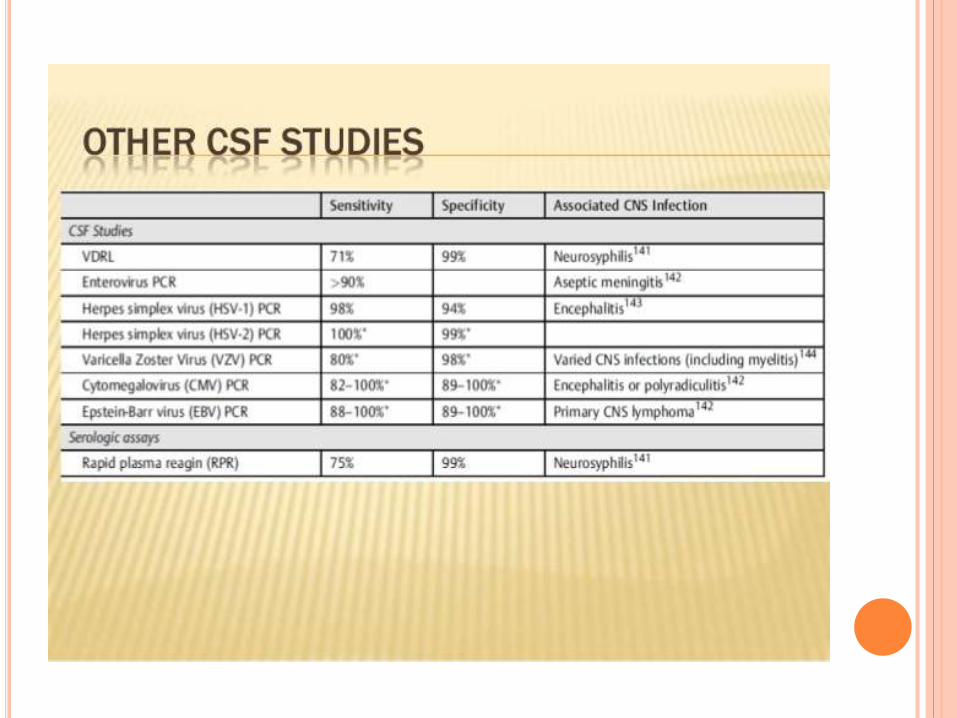
Peripheral serology+ CSF evaluation
VDRL & RPR- sensitive in early
TP-FAB- specific
CSF- mild inflammatory
- VDRL,FAB
Rx
Inj.Penicillin aqueous -12-24 mu q4h x 10-14 days
Jarisch-Herxheimer reaction
(iv steriods-premptively)
LYME DISEASE
Ixodes tick-endemic North America,Europe,Asia
Erythema migricans-initial lesion
Classic triad- facial palsy,aseptic meningitis,painful
radiculitis
Bannworth synd.-acute transverse myelitis-painful
Chronic,progressive myelopathy- other form
Diagnosis
-clinical history
-ELISA/Western blot
-CSf- Lyme specific IgM
-MRI- T2 hyperintensity+CE-root,meninges
Rx-
IV Ceftriaxone-14-28 days+ steroids
TUBERCULOSIS
MC myelopathy- Pott’s disease
Vertebral venous system
Anterior segment of thoracic & lumbar spine-collapse
Other forms-
- intramedullary/intradural tuberculomas-
(S/A myelopathic symptoms).
- granulomatous myeloradiculitis-
(rapid progressive rad.pain,paresthesia,flaccid
weakness,babinski+ ,bladder+)
- spinal artery vasculitis+ cord infarction
- ADEM
- Cord compression- vertebre,granulating tissue
DIAGNOSIS
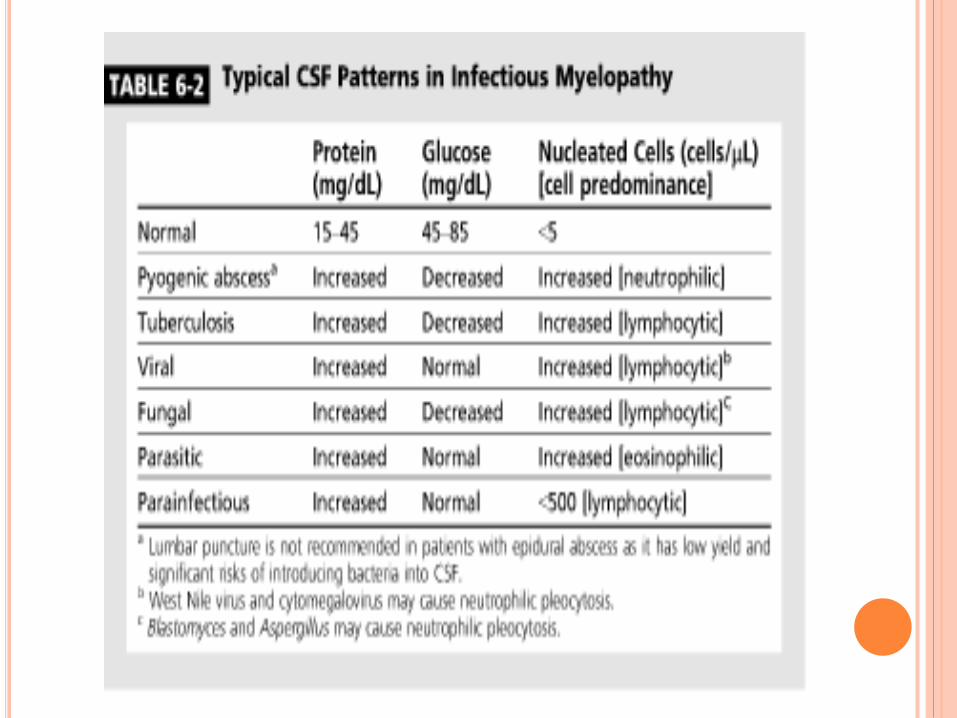
CSF- lymphocytic pleocytosis,low sugar,very high protein
AFB,TB cultures
Mantaux test- + in 40%
MRI (Pott’s)–T1 hypo +T2 hyper +CE
Vertebre collapse+ cord compression
Granulomatous myeloradiculitis-
CE+ meningeal thickening +spinal roots
Tuberculomas-
CE+ T1 hypointense ring +T2 hyperintense central
RX
2 month HRZE/S+ 7-10 Month HR
Vertebral disease- surgical option
Lumbar disease-better prognosis
PYOGENIC BACTERIA
Vertebral osteomyelitis- collapse+ epidural abscess
Intramedullary abscess- hematogenous seeding+
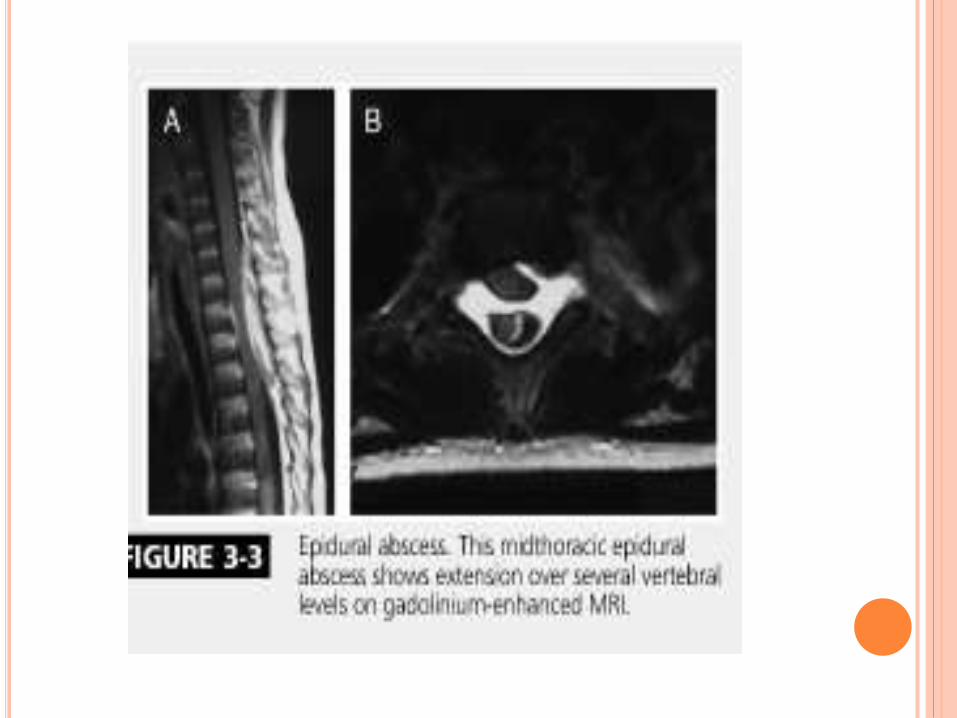
Epidural abscess
- osteomyelitis- hematogenous
- Local soft tissue,viscera,instrumentation ant.epidural
- Direct seeding- post.epidural
- Risk factors+
- Thoracic +
C/F-
- Focal back pain+ muscle spasms
- Fever
- MC- S.aureus > Streptococcus > GNB
Diagnosis-
ESR,CRP
Blood culture-+ 60%
Imaging
LP –contraindicated
Rx
- Drainage
- Iv antibiotics
OTHER BACTERIAL MYELOPATHY
Bartonella- myelitis & Brown –Sequard syndrome
Whipple disease-
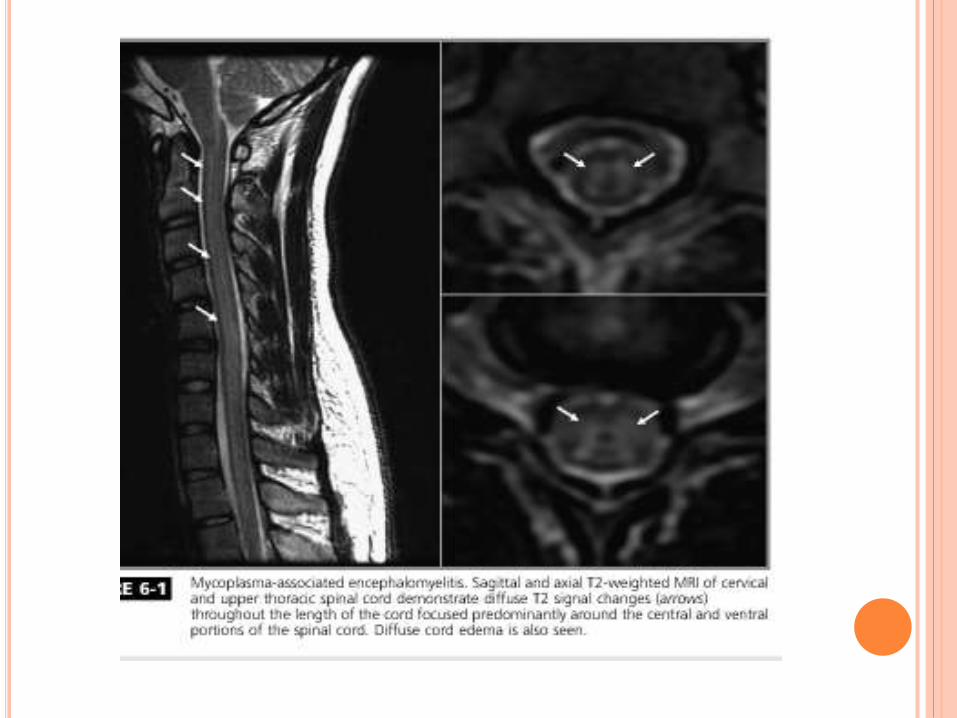
Parainfectious-
Mycoplasma
Pertussis
PARASITIC MYELOPATHIES
Schistosomiasis
Central America & Africa
Retrograde migration of eggs ffrom portal system to
epidural venous plexus
Subacute- low back ache- paraparesis-sensory level-
bladder/bowel++
T11 –L1 & Cauda equina
MRI-
-Cord enlargement
- intramedullary T2 hyperintensity
- lower thoracolumbar cord,conus,cauda CE
DIAGNOSIS
3 features
-Lower spinal cord or cauda
-Evidence of infection(ova in stool/urine,rectal
biopsy,serology)
-Exclusion of other causes
Peripheral Serology- ELISA,IF
CSF tests specific- Monoclonal antibodies or PCR
Tissue biopsy- gold standard
(avoided in CNS disease).
RX
Praziquantel
Concurrent steroids
Rarely, decompression- medically refractory
OTHER PARASITES
Toxoplasma gondii-
-Advanced HIV
-Parenchymal + spinal cord mass lesions
-Peripheral IgG+
- CSF-PCR(spf)
Rx-
pyrimethamine + sulfadiazine /clindamycin
folinic acid
NEUROCYSTICERCOSIS
1.2 %-5.8% cases involve spinal cord
Subarachnoid
Subarachnoid cysts migrate from basal cisterns
75% cases – intracranial NC
Csf- high proten + eosinophilia
Rx
- albendazole + steroids
- rarely,decompression.
HYDATID CYST-ECHINOCOCCUS
Spinal rare
Vertebrae,extradural or paraspinal
Cysts in other sites+
Large- mass effect,bony destruction,inflammatory
response
Imaging-cysts
Serology
Rx-
albendazole
surgical
Recurrence- norm
OTHER PARASITES
Gnathostoma spinigerum
Angiostrongylus cantonensis
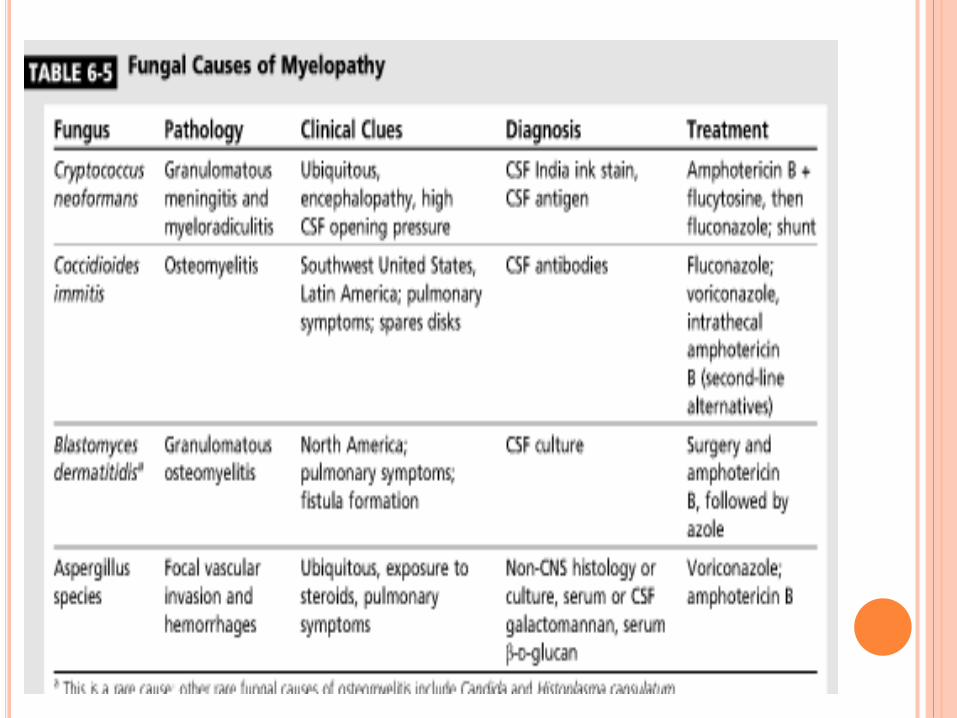
FUNGAL CAUSES
Immunocompromised
Aspergillus,cryptococcus
Spinal myelopathy
- epidural abscess
- c/c arachnoiditis
- intramedullary granulomas
- frank myelitis
- vasculitis + cord infarction.
APPROACH
Clinical –
- Onset- Acute vs Subacute Vs Chronic
- Progression
- Painful vs painless
- Sensory level
- Bladder/Bowel+
CSF analysis
Imaging
ACUTE FLACCID PARALYSIS
Polio
Enteroviruses
West NileV
Leukomyelitis-(Acute)
Herpes
CMV
Borellia- rare
EBV
Rabies
LEUKOMYELITIS (SUBACUTE-CHRONIC)
Treponema
Mycoplasma
Tuberculosis
HIV/HTLV-1

Thank you