influence of surgically implantable telemetry solutions on in-life and post-mortem toxicology...
TRANSCRIPT
Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
Contents lists available at SciVerse ScienceDirect
Journal of Pharmacological and Toxicological Methods
j ourna l homepage: www.e lsev ie r .com/ locate / jpha rmtox
Original article
Influence of surgically implantable telemetry solutions on in-life and post-mortemtoxicology endpoints
Theodore J. Baird a,⁎, Marc Bailie b, Daniel J. Patrick d, David Moddrelle c, Joshua Yoder a,David V. Gauvin a, Jill A. Dalton a
a Safety Pharmacology, MPI Research, Inc., 54943 North Main St., Mattawan, MI 49071-9399, USAb Integrated Nonclinical Development Solutions, Inc., 3005 Miller Avenue, Ann Arbor, MI 48103, USAc Xenometrics, LLC, P.O. Box 401, 17745 Metcalf Avenue, Stilwell, KS 66085, USAd Veterinary Pathology, MPI Research, Inc., 54943 North Main St., Mattawan, MI 49071-9399, USA
⁎ Corresponding author. Tel.: +1 269 668 3336x1336E-mail address: [email protected] (T.J. Bai
1056-8719/$ – see front matter © 2013 Elsevier Inc. Allhttp://dx.doi.org/10.1016/j.vascn.2013.02.006
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 5 June 2012Accepted 8 February 2013Keywords:CanineExternal telemetryForeign body responseHistopathologyImplanted telemetryToxicology
Introduction: Understanding the appropriate application of telemetry and other technologies fornonclinical investigation of functional safety issues in the context of ongoing toxicology evaluations is a cur-rent industry challenge. One major issue is related to the potential impact of surgical implantation of a telem-etry device on contemporarily established measures of drug toxicity, and potential for confoundingpathological issues related to the systemic and local response of the experimental animal to the presenceof a foreign body. This study was designed to evaluate the potential local and systemic impact of different im-planted telemetry devices with varying requisite degrees of surgical complexity on general toxicology studyendpoints. Methods: Sixteen male beagle dogs 1) no surgical instrumentation [n=4], 2) Jacketed External Te-lemetry (JET) with femoral artery blood pressure implant (PA-C10 LA) [n=4], or 3) fully implantable(DSI-D70-CCTP) devices [n=8], were assigned to experimental groups and evaluated within the context of a
standard repeat-dose toxicology design to determine the potential impact of these treatments on routinein-life and post-mortem toxicological endpoints. Results: Device implantation, regardless of the level of inva-siveness/complexity was without effect on any in-life safety parameter, including clinical chemistry and hema-tology, assessed in the experimental design. Histopathological findings were limited to the expected, primarilyminimal tomild localized effects characteristic of a foreign body reaction (fibrosis, inflammation) in the area im-mediately in contact with the body of the transmitter device and associated sites of ECG lead and pressure cath-eter interface with local tissues.Discussion: This study represents the first definitive evaluation of the influenceof variably invasive telemetry device implantation on standardized, essential toxicology endpoints in the con-text of a simulated repeated dose experimental design. The data suggest that, when carefully evaluated, thelocal effects of implanted telemetry devices can be managed in the context of a standard Investigational NewDrug (IND)-enabling toxicology study. This study provides support for the potential incorporation of unre-strained cardiovascular assessments via implanted or external telemetry into standard multi-dose toxicologystudies.© 2013 Elsevier Inc. All rights reserved.
1. Introduction
Telemetry solutions development for physiological monitoring inbasic research, as well as in support of efficacy and safety testing, hasbeen proliferative in recent years. Due to the high fidelity of signals,amenability to unrestrained and unanesthetizedmonitoring, and capac-ity for continuous and extended data collections, implantable telemetrydevices for cardiovascular assessment are the preferred methodologyfor use in definitive safety pharmacology investigations (Anon, 2001,2005; Bass, Vargas, & Kinter, 2004; Lindgren et al., 2008). Recentadvances in telemetry have also led to the development of several
; fax: +1 269 668 4151.rd).
rights reserved.
non-invasive telemetry systems for collecting electrocardiographic and(direct or indirect) blood pressure data.While these systems have obvi-ous potential for application in the context of both safety pharmacologyand repeated dose toxicity or combined functional safety/toxicity inves-tigations, it is clear that signal quality differences arise from the uniquemethods of application of these technologies within the researchenvironment (Baird et al., 2011; Harter, Holdsworth, Dalton, Gauvin, &Baird, 2009; McMahon et al., 2010), including such key variables as 1)the site and operating characteristics of the blood pressure sensor, and2) the orientation and type of lead employed for electrocardiography.In addition, surgically implanted blood pressure probes and ECG leadorientations which afford the highest signal to noise ratio, while beingthe preferredmethodology in traditional, stand-alone safety pharmacol-ogy studies (Baird et al., 2011; Henriques et al., 2010; Holzgrefe et al.,

Table 1Experimental design.
Group(subject numbers)
Surgery ECG leadplacement(device)
Blood pressure catheterplacement (device)
1 (6001–6004) − NA NA2 (6005–6008)a + Skin Lead II
(JET)Femoral Artery(PA-C10-LA)
3 (6009–6012)b + Lead II, EPI(D70-CCTP)
Internal Iliac Artery(D70-CCTP)
4 (6013–6016)b + Lead II, EPI(D70-CCTP)
Internal Iliac Artery(D70-CCTP)
+ Performed, − Not Performed.NA — not applicable.
a Animals were equipped with a jacketed external telemetry (JET) system with (skinsurface) multi-electrode configuration, and surgically implanted PA-C10-LA telemetrydevice with pressure catheter directed into the femoral artery.
b Animals were surgically implanted with a fully internalized telemetry device withsubcutaneous Lead II and Epicardial (EPI) electrode arrays and pressure catheter di-rected into the internal iliac artery.
149T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
2007), may be viewed as potentially confounding variables in researchinvestigations where collection of traditional toxicological (e.g., clinicalpathology, histopathology) endpoints is a core component.
Consequently, understanding the appropriate application of te-lemetry and other modern technologies for nonclinical investigationof functional (cardiovascular) safety issues in the context of ongoingtoxicology evaluations is a challenge currently presented to the in-dustry. Although not a new issue (Matsuzawa et al., 1997), this is aparticularly compelling topic in view of the rapid proliferation ofbiopharmaceuticals (Vargas et al., 2008) and other novel therapiesor diagnostic agents which support integration of safety and toxicol-ogy variables within a unified experimental design (Anon, 1997,2010a,b). Although the importance is increasingly recognized(Cavero, 2010; Guth et al., 2009; Leishman et al., 2012; Sarazan etal., 2011), systematic comparisons of alternative applications of cur-rent technology and associated differences in study design variablesremain largely unreported, both for the potential impact on function-al assay sensitivity and liabilities for confounding key toxicologicalendpoints (Baird et al., 2011; Prior, McMahon, Schofield, & Valentin,2009). The objective of this study, therefore, was to characterize thepotential interactions between alternative telemetric procedures uti-lized for functional (cardiovascular) safety and traditional drug toxic-ity evaluations towards establishing an accepted model defining theappropriate balance for integration of these key safety variables. Spe-cifically, the present experimental findings are hoped to provide con-text to understand definitively the influence of differing degrees ofsurgical sophistication in telemetry device implantation on routinelycollected in-life and post-life toxicology endpoints of interest in a ca-nine model. It is anticipated that this study also may be utilized as areference for guiding development of future protocols, particularlyas the above contribute to defining the nature of potential experi-mental design efficiencies, including animal welfare (3R's) concerns.
2. Methods
2.1. Animals
Animals were received from a USDA-approved laboratory animalvendor previously audited by staff veterinarianmembers of theMPI Re-search IACUC. Twenty-two male beagle dogs (Covance Research Prod-ucts, Kalamazoo, MI), 5–6 months of age, were qualified for studybased on pre-study physicals, clinical pathology, electrocardiographyevaluations and on the outcome of jacket acclimation sessionsconducted on at least three occasions prior to assignment to study. Inorder to model typical laboratory conditions and scheduling for toxicol-ogy investigations, animalswere allowed to acclimate to the general fea-tures of the testing environment for approximately 2 weeks prior to theinitiation of any study-specific procedures. Sixteen animals were ran-domly assigned to surgical treatment groups as indicated in Table 1.
2.2. Telemetry implants
There are various strategies currently available to facilitate the inte-gration of cardiovascular safety assessment (ICH S7A, B) as a componentwithin standard toxicology study designs. In general,methodologies uti-lized for this purpose are somewhat different than those contemporarilyused on stand-alone cardiovascular safety studies. The present experi-mental design was employed to evaluate the influence of two standardapproaches to telemetry-based recordings for cardiovascular systemevaluation. One technique employs the use of a minimally invasive,small scale telemetry implant to allow direct, systemic blood pressuredeterminations, used in conjunction with a jacketed external telemetrysystem for ECG recordings via externally applied (skin surface) elec-trodes. A second technique is more consistent with the approach usedin an independent cardiovascular safety pharmacology study design,and entails the full implantation of a more sophisticated telemetry
device similarly capable of direct arterial blood pressure determination,butwith options to enable ECG recording via differentially located sets ofinternal biopotential lead arrays (e.g., in the present experiment, subcu-taneous Lead II and base-apex epicardial). These different conditionswere included in the present study because there are known differencesin the sensitivity yielded by various non-invasive and implantable te-lemetry configurations for blood pressure and ECG evaluation (Guth etal., 2009; Henriques et al., 2010; Holzgrefe et al., 2007; McMahon,Mitchell, Klein, Jenkins, & Sarazan, 2010). Typically the more invasiveimplantation procedures, for example for ECG lead placement (epicardi-al versus subcutaneous or skin surface lead), result in higher fidelity sig-nals with positive influences on assay sensitivity and mitigatingproperties with regard to errors in data analyses and/or study conclu-sions. The highly localized foreign body response to an internal implantis a well-characterized phenomenon andwould be expected to be pres-ent at specific sites of tissue/device interface, regardless of the implanta-tion technology employed. However, a key issue which remains to beaddressed is whether the utilization of alternative telemetric optionsfor data recording, which may vary considerably in terms of the levelof surgical invasiveness, has potential to differentially influence moreglobal indicators of systemic toxicity such as are reflected by outcomeson routine in-life, and particularly, post-life toxicology study endpoints.
Table 1 indicates the assignment of animals to experimental groups,including Group 1) no surgical instrumentation [n=4], Group 2)Jacketed External Telemetry (JET) with femoral artery blood pressureimplant (PA-C10 LA) [n=4], and Groups 3 and 4) fully implantable(DSI-D70-CCTP) devices [n=4/group]. The PA-C10-LA (DSI; Fig. 1a) isan implantable telemetry device with a significantly reduced physicalprofile and more limited features for data capture in relation to theD70-CCTP,whichmay be utilized to collect blood pressure concomitant-ly with ECGs obtained by a jacketed external telemetry (DSI-JET™)system. The D70-CCTP transmitter (Data Sciences International—DSI;Fig. 1b) is a telemetry device with two sets of bio-potential leads and1 pressure catheter capable of collecting electrocardiographicbiopotentials associated with different lead arrays (e.g., the aforemen-tioned subcutaneous and epicardial sources) andarterial blood pressure.Two groups (n=4/group) of dogs were instrumented with D70-CCTPdevices (Groups 3 and 4) in order to assess an adequate number of ani-mals, since minor variations in the more complex implantation proce-dure were expected a-priori, due to selected placements of multipleECG lead arrays, as well as the ground lead, pressure catheter, and trans-mitter body. Inclusion of two independent groups of these similarlyinstrumented animals was designed to allow for specific evaluation ofthe stability of surgical outcome, particularly as potential associatedcomplications might be expected to impact measured toxicology end-points. Some alternative telemetry data collection schedules were alsoinstituted in these animals, as part of other unrelated evaluations of

a
b d
c
Fig. 1. a–d: Devices for fully implantable telemetric blood pressure and ECG monitoring, (a: PA-C10-LA) or direct arterial blood pressure monitoring (b: D70-CCTP) combined withJacketed External Telemetry for ECG collection. Panels c and d illustrate surgical placement of the PA-C10-LA and D70-CCTP devices, respectively. Tissues in direct apposition toelements of the PA-C10-LA (c) and accordingly subject to specific evaluation to characterize localized foreign body response included those adjacent to the transmitter bodyand midpoint and terminus of the intra-arterial pressure catheter. Tissues in direct apposition to elements of the D70-CCTP (d) and accordingly subject to specific evaluation tocharacterize localized foreign body response included those adjacent to the transmitter body, the termini of the ground lead, subcutaneous leads (2), and epicardial leads (2),and midpoint and terminus of the intra-arterial pressure catheter.
150 T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
signal quality, necessitating the two independent groups. Accordingly,for the purposes of data presentation, and to compare variability in thetoxicology data, including specifically the expression of foreign body re-sponse with the multiple sites of tissue/device interface with theD70-CCTP telemetry unit, in a simulated toxicology study design utiliz-ing a typical number of experimental subjects per group (e.g., n=4/group), these similarly implanted animals are depicted as randomly al-located to independent groups (3 and 4) in tables and graphicalillustrations.
2.3. Surgical procedures
The PA-C10-LA telemetry device was surgically implanted (Fig. 1c)by trained veterinary surgeons under aseptic conditions according totest facility Standard Operating Procedures. Briefly, an incision wasmade over a femoral artery anda pocketmade sub-muscularly. The fem-oral artery was exposed, and via an arteriotomy, the pressure catheterwas introduced and secured internally. The transmitter was then placedinto the sub-muscular pocket and anchored in place with non-absorbable suture. All muscle and subcutaneous tissues were closedwith absorbable suture, and the skin closed with non-absorbable sutureand tissue adhesive.
The D70-CCTP devicewas surgically implanted (Fig. 1d) by the sameveterinary surgical staff according to test facility Standard OperatingProcedures. The pressure catheter was introduced into, and secured inplace within the internal iliac artery. One set of ECG leads was placedsubcutaneously in an approximate Lead II configuration (positive leadover the 3–4th intercostal space, negative lead in the vicinity of theright clavicle), while the remaining two leads were implanted on (pos-itive lead), or in close proximity to (negative lead) the epicardium,
oriented in a base-apex epicardial arrangement, and the ground leadplaced subcutaneously on the left thorax approximately at the level ofthe 5th intercostal space. Epicardial placement of the leads was com-pleted according to a general procedure previously described in thenon-human primate to optimize the amplitude and consistency ofECG component waveforms (Holdsworth, O'Donohue, Smith, & Baird,2011). Briefly, an incision was made over the 5th intercostal space, aleft thoracotomy performed, the pericardium incised, and a pericardial“cradle” created so that both the base and ventricular apex could be eas-ily visualized. The bio-potential leadswere tunneled to the 7th intercos-tal space and passed into the thorax. The bio-potential leads weretrimmed and tied to expose a loop of bare wire. The positive bio-potential lead was attached to the left ventricle near the ventricularapex with non-absorbable suture, and the negative bio-potential leadattached to the mediastinal aspect of the left ventricle near the base ofthe left ventricle with non-absorbable suture. The precise location ofthis lead was manipulated as necessary to optimize p-wave amplitude.A small incision was made on the left thorax at approximately the 9thintercostal space and a chest tube passed into the thorax. The lungswere hyper-inflated to remove any atelectasis and the ribs apposedwith stainless steel suture. The chest tube was attached to suction, allmuscle and subcutaneous tissues closed with absorbable suture, andthe skin incisions closed using skin staples.
To verify functionality of the surgical implants and optimization ofthe ECG based on lead arrangement, PA-C10-LA and D70-CCTP signalswere continuously monitored during surgery and following comple-tion of surgical procedures, prior to recovery. All surgical animalswere allowed a 14-day recovery following implantation, includingdaily post-operative incision checks and standardized medicationprotocol for postsurgical pain control.

151T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
2.4. In-life and post-life data collection procedures
Because JET, including the use of ECG surface leads, shirts, and jacketswas used in Group 2 animals at various points during the experiment, an-imals in all other experimental groups were also subjected to identicalprocedures (leads, shirts, jackets) at the same intervals in order to controlfor the possibility that differential treatment in this regard might impactin-life or post-life toxicology parameters (e.g., especially potentially labileand/or sensitive variables such as food consumption, bodyweight, clinicalobservations, etc.). Telemetry data corresponding to these intervals is notreported herein, as these are voluminous and not central to the essentialexperimental question of whether differentially invasive surgical proce-dures to enable telemetric data collection of cardiovascular parametersis associated with detectable change in routine toxicological endpointscollected using established/contemporary methods. Accordingly, the fullcomplement of these telemetry data will be presented elsewhere, withthe exception of the results of post-surgery/pre-dose, 24-hour, qualitativerhythm analyses, which are presented alongside the restrained, strip-chart ECG findings.
Animals in all experimental groups were administered vehicle (0.9%Sodium Chloride for Injection, USP) by oral gavage (5 mL/kg/dose)daily for 28 days to simulate the research environment for a traditional,repeated dose toxicology study. During the course of the study, animalswere periodically evaluated for routine in-life toxicity endpoints(Auletta, 2002), including cageside observations (a.m. and p.m., daily),detailed clinical observations (daily), veterinary physical examinations(pre-test and terminal), body weights (daily), food consumption (daily,reported weekly), electrocardiography (10-second strip-charts obtainedwith animals briefly restrained in right lateral recumbency prior to theinitiation of dosing, mid-term, and terminal), ophthalmoscopy (pre-testand terminal), and clinical pathology (hematology, clinical chemistry, co-agulation, urinalysis; pre-test, Day 15, and terminal). Veterinary physicalobservations, ophthalmoscopy, andqualitative electrocardiographic eval-uations were conducted byMPI Research staff veterinarians, a consultingophthalmoscopy specialist, and an independent, board-certified veteri-nary cardiologist, respectively. Blood samples were also collected onDays 1 and 28 prior to dosing and at seven discrete intervals through24 h post-dose to simulate sampling protocols typically employed to de-rive exposure data on repeated dose toxicology study designs.
Following completion of the dosing regimen and in-life toxicologyevaluations, the animals were euthanized by intravenous sodium pento-barbital solution injection followed by exsanguination. At necropsy, theanimals were examined for macroscopic abnormalities and a standardset of organ weights and tissues for canine toxicity studies (Auletta,2002) were collected. Microscopic examination of fixed hematoxylinand eosin-stained sections, using a four-step grading system, wasperformed by a board-certified veterinary pathologist. Beyond the rou-tine histopathological evaluations typically conducted on repeated dosetoxicology studies, and consistentwith the goals of this experimental de-sign, the histopathological response of local tissues in direct contactwiththe body of the transmitter device, arterial pressure catheter, and subcu-taneous and intrathoracic (epicardial) ECG leads also was carefully eval-uated. All ECG lead sections were embedded in methyl-methacrylatemedia and sectioned using an automated rotary microtome at 5 and8 μm thicknesses with a D-profile tungsten carbide knife.
3. Results
3.1. In-life toxicology data
All animals demonstrated a clinically unremarkable recovery fromthe surgical procedures. There were no changes in any in-life endpointsroutinely utilized to evaluate drug toxicity (detailed clinical observa-tions, veterinary physical observations, body weight, food consumption,ophthalmoscopy, electrocardiographic evaluations, or clinical pathologyassessments) on repeated-dose investigations, which could be
attributed to specific, group-dependent manipulation of the relative in-vasiveness of surgical instrumentation of the animals. Fig. 2a–b andTables 2–5 summarize the lack of significant, treatment group-basedvariability characterizing these observations, as detailed in the followingsections. Variations in all of these endpoints were characteristic of nor-mal biological heterogeneity in animals of this age and species, andclosely approximated the range of typical variation objectively verifiedby means of test facility historical control data (historical data notshown for veterinary physical observations, ophthalmoscopy, or qualita-tive electrocardiographic evaluations due to typical NAD [no abnormal-ities detected] status of all animals in the present experiment accordingto the results of independent reports supplied by the aforementioned in-ternal and expert contributors).
3.1.1. Detailed clinical and veterinary observationsA summary of incidence rates for various detailed clinical observa-
tions conducted over the course of the study is provided in Table 2.These detailed clinical observations findings were infrequently and/orsporadically observed, did not express in any treatment group-dependent manner, and represent common observations in animals ofthis species, and so are considered incidental to experimental treatments.Some additional detailed clinical and veterinary findings were identifiedthat reflected the routine jacketing procedures (Pickersgill & Burnett,2000), or were associatedwith surgical manipulations (e.g., dermal abra-sion and or skin discoloration in regions underlying the shirt/jacket appa-ratus, scar reflecting incision site healing). These findings did not expressin any compelling, systematic manner across experimental groups, didnot require any veterinary assistance or intervention, and accordinglywere considered incidental to experimental surgical manipulations. Theobvious exception was the presence of surgical scar(s), which wouldnot affect Group 1 control animals, and did express differentiallyaccording to the specific surgical procedures conducted in Group 2(PA-C10-LA implant) versus Group 3 and 4 (D70-CCTP implant) animals.
3.1.2. Food consumption and body weightDaily bodyweight (Fig. 2a) and correlated food consumption values
summarized byweek (Fig. 2b) were stable over the course of the study,coinciding with a lack of complications during and following thetwo-week post-surgery recovery period, regardless of the level of inva-siveness of the implantation procedure employed. Values recorded forboth parameters were reflective of those typically observed for theage, sex, breed, and supplier of beagle dogs used on this study.
3.1.3. Ophthalmoscopic examinationsOne animal in Group 3 was noted with a persistent pupillary
membrane affecting the left eye, both prior to the initiation of dosingand at the terminal ophthalmoscopic examination. There were noother ophthalmoscopic observations noted in any other animal dur-ing the course of the study. This finding accordingly is considered in-cidental to experimental surgical manipulations, representing aperiodically observed variant in animals of this age and species.
3.1.4. Qualitative electrocardiographic evaluationsBased on review of the restrained 10-second strip chart ECGs col-
lected prior to the initiation of dosing, mid-term, and terminally, all an-imals were in sinus rhythm or demonstrated sinus arrhythmia, both ofwhich are normal in dogs. One animal in the non-surgical control group(Group 1) demonstrated first degree AV block on themid-term and ter-minal ECGs. First degree AV block is a normal variant observed in dogs(Cools et al., 2011; Gauvin, Tilley, Smith, & Baird, 2009). Since this find-ing occurred in a Group 1 control animal it is likely indicative of apre-existing condition in this individual animal, and is clearly unrelatedto experimental surgical manipulations. All of the remaining electrocar-diograms were qualitatively within normal limits.
To determinemore definitively the implications of experimental sur-gical manipulations, particularly intrathoracic epicardial ECG lead array

0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
0
8
10
12
14
16 Group 1 (Non-Implanted) Group 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP)
Bo
dy
Wei
gh
t (k
g)
Time (Days on Study)
a
0 1 2 3 4 5
0
100
200
300
400
500
600 Group 1 (Non-Implanted) Group 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP)
Fo
od
Co
nsu
mp
tio
n (
Wee
kly
Avg
g/k
g/d
ay)
Time (Weeks on Study)
b
Fig. 2. a–b: Body weight and food consumption values. Body weights (a) were collectedand reported daily; food consumption values (b) were recorded daily and summarizedweekly.
152 T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
placement, on qualitative cardiac rhythms, a post-surgery, pre-dosesample of 24-hour continuous (external) telemetry recording was com-prehensively analyzed for each animal. Incidental findings observed atthis pre-dose interval, which corresponded to within one day of collec-tion of the pre-study manual/restrained ECGs discussed above, werelimited to rare and sporadic atrial premature contractions (APCs), ven-tricular premature contractions (VPCs), and rare and isolated instancesof atrio-ventricular block (2°AVB), all of which were found to be
Table 2Detailed clinical observations.
Observationa Group 1 (no implant) Group 2 (PA-C1
Emesis/vomitus 0/0 1/1Inappetence 0/0 0/0Injected sclera 3/2 0/0Lacrimation 0/0 5/1Soft feces 12/3 2/2
a Values represent the total number of observations/total number of animals affected at
distributed across animals in a random manner. The first degree AVblock observed in one Group 1 animal at mid-term and terminal inter-vals by manual/restrained ECG also was confirmed by analysis of exter-nal telemetry data. The total number of animals in any experimentalgroup expressing any arrhythmia was ≤2/4, with fewer than 5 totalcounts in 24 h for any individual animal. This number of rhythmvariants is so considerably lower as to be insignificant relative to therange of that previously reported in normal animals, those surgicallyinstrumented for left ventricular pressure telemetry (Cools et al.,2010), and even in animals similarly instrumented (e.g., Groups 3 and4) with epicardial leads (Baird et al., in press;O'Donohue et al., 2011).
3.1.5. Clinical pathology evaluationsHematology, clinical chemistry, and urinalysis data review were
conducted by an independent, board-certified clinical pathologist bycomparison of treatment group-averaged values (±Standard Devia-tion, SD), as well as by consideration of these values in relation tothe range of variation in test facility historical control data collectedin untreated animals of the same age, species, breed, of the same ap-proximate age (±2 weeks), and from the same vendor. Historicalcontrol reference values in Tables 3–5 (far right column in eachtable) are based on at least 115 individual determinations in indepen-dent animals.
3.1.5.1. Hematology. Table 3 summarizes hematology values (Mean±SD), by study interval, for all experimental groups. In addition, the farright columnof the table contains similar summary statistics characteriz-ing normal (untreated) animals of the same species, breed, and approx-imate (±2 weeks) age, and from the same vendor for comparison.Although both within-group and between-group variability was ob-served in hematology and coagulation parameters none of these varia-tions significantly deviated from the range of normal biologicalvariation typically observed in animals of this age and species, orexpressed in any manner suggestive of an effect of surgical treatment.There were no meaningful treatment-related effects on red cell mass(erythrocytes, hemoglobin, and hematocrit) in any of the groups,which is somewhat notable due to the substantial differences in thelevel of invasiveness of the procedures facilitating telemetry device im-plantation, and lack of surgical manipulation in animals assigned to thecontrol group. There were mild decreases in red cell mass in all groupsthat were similar in magnitude and were considered within an accept-able range for biologic variation and procedure-related losses (i.e. sched-uled blood draws). At termination in Group 3 there were mild increasesin neutrophils, monocytes, eosinophils, basophils, and “other cells”(large unstained cells) relative toGroup 1 and/or Group 2. Thesefindingsmay indicate a transient physiological stress response; however, the var-iationswere not observed in Group 4 animals treated identicallywith re-spect to surgical instrumentation, were small in magnitude, and valuesremained within expected historical ranges; hence these were not con-sidered biologically relevant. There were periodically other minor alter-ations among hematology analytes that were not consideredmeaningful due to their small magnitude, similarity to pretest values,and/or sporadic nature.
3.1.5.2. Clinical chemistry. Table 4 summarizes clinical chemistryvalues (Mean±SD), by study interval, for all experimental groups.
0-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP)
0/0 1/10/0 1/10/0 0/00/0 0/02/2 1/1
any point (including prior to the initiation of dosing).

Table 3Hematology.
Parametera Study interval Group 1 (no implant) Group 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP) Historical average
Leukocyte count (×103/μL) Pretest 10.33±2.822 9.93±1.069 10.58±1.471 13.50±3.045 10.93±2.014Day 15 8.50±1.503 10.48±0.971 10.75±2.258 9.13±0.699Term 9.13±1.821 8.93±1.147 13.53±3.815 9.53±0.957
Erythrocyte count (×106/μL) Pretest 6.535±0.538 7.383±0.478 7.530±0.444 7.260±0.293 6.78±0.524Day 15 6.585±0.763 7.088±0.761 7.168±0.209 7.025±0.245Term 6.703±0.747 6.930±0.409 6.860±0.426 6.830±0.416
Neutrophils (×103/μL) Pretest 5.950±2.231 6.423±0.931 6.698±1.207 9.105±3.101 7.22±1.875Day 15 4.780±0.519 7.010±1.355 7.025±1.683 5.525±0.605Termination 5.423±0.907 5.468±0.826 9.398±3.677 5.705±0.996
Lymphocytes (×103/μL) Pretest 3.505±1.719 2.670±0.420 2.868±0.449 3.180±0.149 2.804±0.635Day 15 2.850±0.915 2.550±0.420 2.675±0.512 2.625±0.465Term 2.925±0.988 2.675±0.457 2.950±0.592 2.875±0.450
Monocytes (×103/μL) Pretest 0.460±0.378 0.495±0.157 0.433±0.119 0.690±0.243 0.609±0.202Day 15 0.445±0.167 0.535±0.125 0.475±0.142 0.448±0.130Term 0.388±0.045 0.435±0.107 0.573±0.239 0.478±0.151
Eosinophils (×103/μL) Pretest 0.328±0.431 0.250±0.115 0.440±0.280 0.395±0.220 0.254±0.151Day 15 0.288±0.186 0.320±0.161 0.468±0.230 0.475±0.158Term 0.328±0.148 0.288±0.087 0.510±0.175 0.418±0.098
Basophils (×103/μL) Pretest 0.050±0.037 0.063±0.005 0.085±0.027 0.075±0.024 0.048±0.025Day 15 0.050±0.020 0.033±0.013 0.045±0.013 0.033±0.010Term 0.038±0.005 0.033±0.010 0.050±0.008 0.038±0.010
Other cells (×103/μL) Pretest 0.038±0.029 0.043±0.005 0.055±0.010 0.048±0.010 0.033±0.018Day 15 0.075±0.013 0.038±0.017 0.040±0.014 0.048±0.022Term 0.028±0.013 0.028±0.005 0.053±0.013 0.028±0.010
Hemoglobin (g/dL) Pretest 14.05±0.695 15.85±1.038 15.98±0.877 15.05±0.332 15.01±1.172Day 15 14.38±1.597 15.13±1.711 15.18±0.512 14.55±0.954Term 14.65±1.399 14.78±0.967 14.53±0.918 14.10±0.566
Hematocrit (%) Pretest 43.03±2.476 48.23±2.786 48.73±2.716 46.10±1.608 44.13±3.396Day 15 42.05±4.470 44.38±4.784 44.55±1.682 43.03±2.597Term 42.55±3.931 43.35±2.390 42.40±2.825 41.60±1.791
MCV (fl) Pretest 65.98±2.141 65.33±0.885 64.70±0.693 63.53±1.394 65.14±1.570Day 15 63.93±1.668 62.60±0.945 62.18±0.741 61.20±1.744Term 63.63±1.782 62.55±0.705 61.78±0.699 61.00±1.639
MCH (pg) Pretest 21.53±0.911 21.48±0.435 21.23±0.171 20.75±0.843 22.17±0.692Day 15 21.85±0.624 21.30±0.245 21.18±0.150 20.70±0.766Term 21.88±0.457 21.33±0.465 21.20±0.082 20.65±0.545
MCHC (g/dL) Pretest 32.65±0.332 32.85±0.332 32.80±0.216 32.65±0.733 34.03±0.660Day 15 34.20±0.216 34.00±0.271 34.05±0.370 33.78±0.310Term 34.38±0.263 34.05±0.465 34.33±0.299 33.83±0.250
Platelet count (×103/μL) Pretest 275.0±56.15 376.3±38.76 333.5±42.77 352.5±48.45 360.1±66.57Day 15 299.8±75.80 390.8±73.97 327.5±59.75 360.5±39.37Term 337.8±83.34 365.3±66.84 322.0±35.40 319.5±45.97
Absolute reticulocytes (×103/μL) Pretest 31.88±1.443 61.65±21.321 45.73±11.169 73.80±36.572 52.98±26.613Day 15 30.75±9.952 34.53±10.002 28.28±7.257 26.55±8.346Term 36.83±8.069 45.43±6.015 26.08±8.986 32.98±15.339
APTT (s) Pretest 10.75±0.733 10.85±0.451 10.45±0.129 11.00±0.490 10.45±0.975Day 15 10.85±0.619 10.95±0.656 10.75±0.532 10.93±0.618Term 10.58±0.608 10.88±0.866 11.03±1.090 10.88±0.591
Prothrombin time (s) Pretest 6.83±0.386 7.05±0.443 6.95±0.191 6.98±0.126 8.59±0.983Day 15 6.73±0.472 7.00±0.616 6.85±0.129 6.75±0.238Term 6.58±0.359 6.85±0.507 6.70±0.141 6.78±0.330
MCV —Mean Corpuscular Volume; MCH —Mean Corpuscular Hemoglobin; MCHC— Mean Corpuscular Hemoglobin Concentration; APTT — Activated Partial Thromboplastin Time.a Tabled values represent experimental group or test facility historical averages and associated standard deviations. Historical control values (far right column) are based on at
least 115 determinations in individual, untreated animals matched to the present experimental subjects on species, breed, supplier, age (±2 weeks), and sex.
153T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
In addition, the far right column of the table contains similar summa-ry statistics characterizing normal (untreated) animals of the samespecies, breed, and approximate (±2 weeks) age, and from thesame vendor for comparison. Clinical chemistry analytes displayedminor variability between treatment groups, and over time whichdid not depart significantly from the range of historical control valuesreported for each parameter.
3.1.5.3. Urinalysis. Table 5 summarizes urinalysis values (Mean±SD),by study interval, for all experimental groups. In addition, the far rightcolumn of the table contains similar summary statistics characterizingnormal (untreated) animals of the same species, breed, and approxi-mate (±2 weeks) age, and from the same vendor for comparison. Uri-nalysis analytes displayed minor variability between treatment groups,and over time which did not deviate significantly from the range of his-torical control values reported for each parameter.
3.2. Pathology data
Pathology data (organweights, macroscopic andmicroscopic evalua-tion—Tables 6–9) review was conducted by an independent, board-certified pathologist by comparison of treatment group-averaged values(±SD), and/or standardized four-step histopathology grading scale, aswell as by consideration of group and individual outcomes in relationto the range of variation in test facility historical control data collectedin untreated animals of the same age, species, breed, of the same approx-imate age (±2 weeks), and from the same vendor.With the exception oforgan weight values (expressed as average values±SD; paired organsrepresent average weight of the pair from any individual animal), tablesof the facility histopathology historical control database were too volu-minous to be includedwithin the presentmanuscript. However, detaileddescription of the nature of surgical-based and incidental and/or iatro-genic findings are detailed in the sections to follow, with references

Table 4Clinical chemistry.
Parametera Study interval Group 1 (no implant) Group 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP) Historical average
Sodium (mEq/L) Pretest 146.8±0.96 145.8±2.22 146.8±1.26 146.3±1.26 147.8±1.90Day 15 144.0±2.94 145.0±2.45 145.8±0.96 145.3±1.26Termination 144.5±1.73 144.3±1.71 144.5±1.29 145.5±0.58
Potassium (mEq/L) Pretest 4.90±0.283 4.55±0.208 5.03±0.299 4.75±0.370 4.65±0.333Day 15 4.73±0.320 4.63±0.206 4.55±0.058 4.70±0.115Termination 4.53±0.320 4.63±0.096 4.40±0.245 4.38±0.171
Chloride (mEq/L) Pretest 112.3±0.96 110.8±1.50 110.8±1.26 110.8±1.50 110.8±1.82Day 15 110.8±2.63 111.3±1.71 111.5±1.29 110.8±1.26Termination 109.8±0.96 110.0±1.15 110.0±1.63 110.5±1.29
Calcium (mg/dL) Pretest 10.55±0.208 10.28±0.320 10.63±0.171 10.53±0.250 11.08±0.425Day 15 10.38±0.250 10.18±0.320 10.38±0.320 10.60±0.316Termination 9.88±0.206 9.88±0.287 9.83±0.150 10.10±0.141
Phosphorus (mg/dL) Pretest 7.53±0.299 6.38±0.427 6.68±0.685 6.28±0.275 6.03±0.714Day 15 6.33±0.613 5.70±0.698 5.75±0.603 5.95±0.858Termination 5.48±0.359 5.28±0.499 5.10±0.668 4.93±0.550
Alkaline phosphatase (U/L) Pretest 86.3±15.04 85.8±14.75 79.5±4.80 78.5±29.44 80.0±25.02Day 15 70.0±13.69 60.5±7.14 56.8±2.22 54.3±22.97Termination 64.8±12.31 58.5±8.35 53.0±4.76 52.3±19.97
Total bilirubin (mg/dL) Pretest 0.13±0.050 0.20±0.000 0.13±0.050 0.15±0.058 0.18±0.039Day 15 0.15±0.058 0.18±0.050 0.13±0.050 0.13±0.050Termination 0.15±0.058 0.18±0.050 0.15±0.058 0.13±0.050
Gamma glutamyltrans-ferase (U/L) Pretest 4.0±0.82 4.0±0.00 4.0±1.15 4.0±0.82 3.5±1.03Day 15 4.8±0.50 5.0±1.41 4.8±1.50 5.5±1.00Termination 3.8±0.96 3.3±0.50 3.0±1.15 2.8±0.50
Aspartate aminotrans-ferase (U/L) Pretest 31.8±8.96 33.5±1.73 32.5±2.65 34.5±6.19 27.7±6.33Day 15 30.5±4.20 33.8±1.71 32.5±3.11 31.0±9.06Termination 34.3±5.19 35.5±2.65 33.5±5.26 37.8±7.23
Alanine aminotrans-ferase (U/L) Pretest 32.3±6.60 32.8±6.18 27.5±5.00 31.0±4.24 28.5±6.48Day 15 36.0±11.69 37.0±6.27 35.0±7.87 37.0±6.73Termination 38.5±18.36 39.0±7.87 36.3±6.40 48.3±16.82
Sorbitol dehydrogenase (U/L) Pretest 5.70±0.852 8.98±2.142 7.88±1.678 6.93±0.506 5.79±2.33Day 15 5.60±0.876 6.83±0.768 6.53±0.556 4.88±0.854Termination 5.38±1.258 6.55±1.038 5.60±0.424 6.83±2.323
Urea nitrogen (mg/dL) Pretest 12.5±0.58 12.8±1.50 10.5±1.29 11.3±1.71 12.6±2.11Day 15 14.5±3.70 13.5±1.91 11.5±1.29 14.8±4.27Termination 12.5±1.73 11.8±1.26 10.3±0.50 11.3±1.71
Creatinine (mg/dL) Pretest 0.48±0.096 0.58±0.150 0.50±0.000 0.53±0.050 0.60±0.91Day 15 0.63±0.050 0.63±0.096 0.63±0.050 0.68±0.050Termination 0.63±0.050 0.65±0.129 0.58±0.050 0.63±0.050
Total protein (g/dL) Pretest 2.95±0.191 3.25±0.238 3.15±0.058 3.13±0.050 6.00±0.396Day 15 2.95±0.173 3.00±0.141 3.03±0.050 3.03±0.222Termination 3.10±0.216 3.10±0.141 3.00±0.082 3.13±0.150
Albumin (g/dL) Pretest 2.58±0.171 2.68±0.222 2.68±0.222 2.53±0.050 3.16±0.225Day 15 2.73±0.206 2.88±0.250 2.75±0.265 2.73±0.150Termination 2.45±0.173 2.48±0.171 2.50±0.294 2.23±0.150
Globulin (g/dL) Pretest 2.58±0.171 2.68±0.222 2.68±0.222 2.53±0.050 2.854±0.392Day 15 2.73±0.206 2.88±0.250 2.75±0.265 2.73±0.150Termination 2.45±0.173 2.48±0.171 2.50±0.294 2.23±0.150
Albumin/globulin ratio Pretest 1.15±0.058 1.20±0.163 1.18±0.096 1.23±0.050 1.14±0.189Day 15 1.10±0.000 1.03±0.126 1.10±0.141 1.13±0.050Termination 1.28±0.126 1.25±0.129 1.23±0.171 1.40±0.141
Triglycerides (mg/dL) Pretest 30.8±3.30 37.8±3.77 38.0±7.62 33.0±4.97 24.3±5.24Day 15 32.8±4.57 36.5±1.73 29.5±6.76 31.5±4.80Termination 38.0±8.29 40.0±3.65 34.0±5.23 31.0±7.12
Cholesterol (mg/dL) Pretest 166.5±26.11 149.3±17.33 168.8±17.63 147.0±9.66 175.8±30.41Day 15 162.3±21.70 145.0±15.64 150.0±21.92 151.0±10.68Termination 159.3±19.55 129.8±12.28 156.0±16.06 140.8±3.20
Glucose (mg/dL) Pretest 84.8±5.74 88.5±3.42 87.3±8.66 75.5±6.24 94.9±8.31Day 15 90.0±6.27 92.0±2.16 87.3±3.59 78.3±10.81Termination 87.0±7.70 88.0±4.69 85.3±3.86 82.3±4.11
a Tabled values represent experimental group or test facility historical averages and associated standard deviations. Historical control values (far right column) are based on atleast 115 determinations in individual, untreated animals matched to the present experimental subjects on species, breed, supplier, age (±2 weeks), and sex.
154 T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
made to facility historical control data and literature, as necessary, toprovide context to individual results.
3.2.1. Organ weightsTable 6 summarizes organ weight values (Mean±SD), by study in-
terval, for all experimental groups. In addition, the far right column ofthe table contains similar summary statistics characterizing normal(untreated) animals of the same species, breed, and approximate age(±2 weeks), and from the same vendor for comparison. There wereno definitive organ weight changes between treatment groups. The
mean absolute and relative spleen weights for Groups 2, 3, and 4 weredecreased compared to Group 1; however, these differences in spleenweights exhibited no histopathologic correlate, remained within therange of historical control values, and accordingly were considered ofnobiological consequence. In addition, all organweight values observedin all groups of experimental animals closely approximated meanvalues, and were within the range of observed values of test facilityorgan weight historical control data derived from animals of this samespecies, from the same vendor, and of the same approximate age(Table 6; mean values for each endpoint represent N≥110).

Table 5Urinalysis.
Parametera Study interval Group 1 (no implant) Group 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP) Historical average
Volume (mL) Pretest 201.3±84.59 138.8±145.91 118.8±73.75 226.3±126.91 145.68±122.197Day 15 312.5±102.10 317.5±117.01 242.5±146.60 242.5±123.66Termination 241.3±54.06 260.0±109.85 186.3±119.89 217.5±69.58
Specific gravity Pretest 1.029±0.017 1.020±0.010 1.033±0.012 1.019±0.013 1.016±0.012Day 15 1.023±0.003 1.026±0.007 1.030±0.012 1.029±0.009Termination 1.024±0.005 1.024±0.014 1.030±0.010 1.027±0.012
pH Pretest 7.00±0.408 7.00±0.000 7.50±0.408 7.50±0.000 7.12±0.697Day 15 7.25±0.289 7.75±0.645 7.38±0.479 7.13±0.250Termination 7.13±0.250 7.38±0.479 7.13±0.250 7.13±0.250
a Tabled values represent experimental group or test facility historical averages and associated standard deviations. Historical control values (far right column) are based on atleast 115 determinations in individual, untreated animals matched to the present experimental subjects on species, breed, supplier, age (±2 weeks), and sex.
155T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
3.2.2. Macroscopic observations and organ/tissue microscopyTreatment group-dependent macroscopic and microscopic exam-
ination findings are presented in Tables 7–9. Figs. 3–8 illustrate vari-ous findings characteristic of the foreign body response engenderedby implantation of the telemetry devices.
3.2.2.1. Group 1 (no surgical implant). There were no definitivetreatment-related macroscopic or microscopic findings. A 1.0 cm in di-ameter yellow discoloration (focus) in the skin/subcutis overlying thescapular region of one Group 1 animal correlated to a subcutaneous ag-gregate of mineralization surrounded by a granulomatous reaction andfibrous connective tissue. This focus was consistent with calcinosiscircumscripta, an uncommon syndrome of ectopic idiopathic, dystro-phic, metastatic or iatrogenic mineralization characterized by deposi-tion of calcium salts in soft tissues (Legendre & Dade, 1974; Zwicker &Pack, 2011). It could not be determined if the jacket played a role inthe development of this lesion, however, no other jacketed animals inany of the other experimental groups had similar findings. A macro-scopically small thymuswas also present in this animal, which correlat-ed to amoderate degree of generalized lymphoid depletion. Thisfindingwas considered to be related to normal thymic involution in beagle dogsduring the period of 6 to 23 months of age (Ploermen, Ravesloot, & vanEsch, 2003). All other microscopic observations, including epididymalpolyarteritis and sperm granuloma, kidneymineralization, laryngeal ul-ceration, liver mononuclear cell infiltration, parathyroid cyst, pituitarycyst, and testicular unilateral hypoplasia, were considered to be inci-dental due to sporadic and/or infrequent expression, lack of treatmentrelation, or status as background histopathological findings in animalsof this species (Peckham, 2002).
3.2.2.2. Group 2 (PA-C10-LA implant). There were nomacroscopic find-ings. All tissues were grossly within normal limits. Treatment-related
Table 6Organ weights.
Weighta Group 1 (no implant) Group 2 (PA-C10-LA
Body (kg) 11.34±0.26 10.73±0.33Brain (g) 77.78±3.19 83.80±5.13Adrenal (g) 1.00±0.17 1.07±0.22Epididymides (g) 3.21±0.19 3.39±0.24Heart (g) 91.22±14.01 83.44±3.43Kidney (g) 65.61±11.70 58.67±7.73Liver (g) 291.01±19.22 295.08±39.44Lung w/bronchi (g) 100.87±8.62 96.98±5.59Pituitary gland (g) 0.076±0.015 0.075±0.014Salivary gland, mandibular (g) 5.90±0.49 5.26±0.18Spleen (g) 87.79±9.33 60.96±12.70Testes (g) 14.02±1.32 14.36±2.55Thymus (g) 6.66±5.66 6.21±1.70Thyroid/parathyroid gland (g) 1.31±0.42 0.92±0.18
a Tabled values represent experimental group or test facility historical average and associright column) are based on at least 110 determinations in individual, untreated animals matand sex.
microscopic findings were limited to the catheterized femoral arteryand PA-C10-LA transmitter body implant site.
The nature andmagnitude of histological vascular changes resultingfrom intra-arterial catheterizationwere similar in animals instrumentedwith either PA-C10-LA (Group 2) or D70-CCTP devices (Groups 3 and4).Catheterized femoral artery microscopic observations (Table 8,Figs. 4–6) consisted of a discontinuity in the internal elastic lamina in3 of 4mid catheter artery sections and 1 of 4 catheter tip artery sections.Neointima formation, characterized by a newly formed inner liningcomprised primarily of smooth muscle cells, was present in 4 of 4 midcatheter artery sections (3minimal, 1mild) and 3 of 4 catheter tip arterysections (all minimal). The apparent cause of the internal elastic laminadiscontinuity and neointima formation was the intraluminal pressurecatheter placement and/or presence, as no similar findingswere presentin the non-catheterized arterial sections examined.
JET transmitter body implant site microscopic observations(Table 7) consisted of an intramuscular cavity where the transmitterbody was located in vivo, surrounded by a minimal to mildchronic-active inflammatory reaction, consisting of lymphocytes,plasma cells, macrophages, fibroblasts, collagenous connective tissue,and small numbers of neutrophils and extravasated erythrocytes(hemorrhage). Within the overlying subcutis and dermis, the sutureutilized to secure the telemetry device in place was surrounded by amild degree of granulomatous inflammation which was typical ofsuture-related inflammation.
A mild degree of heart mesothelial cell hypertrophy/hyperplasiawas present on the atrium of Animal 6007 (Table 9). This lesionconsisted of villous epicardial proliferation which is commonly ob-served as an incidental finding in dogs. All other microscopic observa-tions, including kidney mineralization, liver mononuclear cellinfiltration, parathyroid cyst, and thymus lymphoid depletion, wereconsidered incidental due to sporadic and/or infrequent observation
) Group 3 (D70-CCTP) Group 4 (D70-CCTP) Historical average
10.81±0.45 10.58±0.59 10.11±5.6381.20±1.79 85.6±4.04 77.04±16.851.03±0.18 1.05±0.22 0.98±0.693.38±0.83 3.14±0.69 2.39±2.25
96.25±17.08 99.98±7.44 80.26±44.9562.41±6.36 53.14±4.08 52.16±25.26
290.80±31.87 287.97±36.90 276.10±181.2796.58±10.15 98.47±3.57 92.35±46.670.069±0.011 0.078±0.036 0.068±0.0365.19±0.24 5.76±1.17 5.15±2.90
64.18±8.81 63.62±6.08 57.81±50.1112.95±4.17 16.39±2.11 10.06±10.267.49±3.75 8.45±3.22 9.71±11.141.2±0.2 1.05±0.19 0.96±0.64
ated ranges (individual animal low-high recorded values). Historical control values (farched to the present experimental subjects on species, breed, supplier, age (±2 weeks),

Table 7Summary of local histopathology: site of transmitter body.
Site (observations)a Group 1 (no implant) Group 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP)
Bone, rib (ground lead location)Fibrosis − − +++++ (1/4) +++++ (2/4)Hemorrhage − − ++ (1/4) ++ (2/4)Chronic Inflammation − − +++ (1/4) +++ (2/4)
Implant Site (D70-CCTP, PA-C10-LA)Fibrosis NA − ++++ (1/4), +++++ (3/4) ++++ (2/4), +++++ (2/4)Hemorrhage NA − ++ (2/4) ++ (3/4)Chronic-active Inflammation NA ++ (1/4), +++ (1/4) +++ (4/4) +++ (4/4)Granulomatous Inflammation (suture site) NA +++ (3/4) +++ (1/4) −
(−) Not present (+) present, no grade (++) present, minimal (+++) present, mild (++++) present, moderate (+++++) present, severe.NA — not applicable/site not evaluated.
a The implant site (and surrounding tissues) of the PA-C10-LA (Group 2) and D70-CCTP (Groups 3, 4) transmitter body was preserved in fixative, embedded in methyl methac-rylate, and evaluated microscopically. Standard microscopic examinations of neutral buffered formalin (NBF) fixed hematoxylin and eosin-stained paraffin sections were performedon other tissues.
156 T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
of the lesions, lack of treatment relation, or status as background his-topathological findings in animals of this species (Peckham, 2002).
3.2.2.3. Groups 3 and 4 (D70-CCTP implant). Treatment-related macro-scopic findings were limited to a rib nodule and adhesions involvingthe heart and thoracic cavity. A pituitary cyst was also macroscopical-ly observed in one animal which was considered to be an incidentalfinding.
A tan rib nodule, approximately 2.0 cm in diameter, was presentin both of Animals 6012 and 6013, and corresponded to an antemor-tem swelling observation. This nodule surrounded the DSI transmitterground wire and involved the fifth rib and fourth to fifth intercostalsoft tissue. Microscopically, these nodules consisted of a central cavity(from where the wire was originally located) surrounded by a severedegree of fibrosis, mild chronic inflammation (lymphocytes, plasmacells, and macrophages), and minimal hemorrhage. Another tan ribnodule, approximately 2.0 cm in diameter, was present in Animal6016 and surrounded the DSI transmitter ground wire and involvedthe sixth rib and fifth to sixth intercostal soft tissue. Microscopically,this nodule consisted of a central cavity (left where the wire was orig-inally located) surrounded by a severe degree of fibrosis, a mild de-gree of chronic inflammation (lymphocytes, plasma cells, andmacrophages), and a minimal degree of hemorrhage.
In Animal 6009 there was a mild thoracic cavity adhesion involv-ing the thoracic wall and multiple lobes of the lung and pericardium;and a mild heart adhesion involving the thoracic wall and the epicar-dial lead in the apex of the heart. In Animal 6011 there was a mild ad-hesion involving the thoracic wall and the left apical lobe of lung.Microscopically, the lung lesions consisted of minimal to mild degreeof chronic-active inflammation involving the pleura. The heart adhe-sion in Animal 6009 microscopically correlated to a mild degree of fi-brosis surrounding the cardiac lead. A minimal degree of pleuralchronic-active lung inflammation was also present in Animal 6010.Both of these epicardial inflammatory lesions were consistent witha response in these animals to the cardiac and pericardiac leads. In
Table 8Summary of local histopathology: site of intra-arterial pressure catheter.
Site (observations)a Group 1 (no implant) Grou
Artery (mid catheter)Discontinuity of internal elastic lamina NA + (3Neointima formation NA ++
Artery (catheter tip)Discontinuity of internal elastic lamina NA + (1Neointima Formation NA ++
(−) Not present (+) present, no grade (++) present, minimal (+++) present, mild (++NA — not applicable/site not evaluated.
a The implant sites (and surrounding tissues) of femoral artery (Group 2; PA-C10-LA) thembedded in methyl methacrylate and evaluated microscopically.
Animal 6014 there was a mild thoracic cavity adhesion involvingthe pericardium and right and left ventricles near the epicardialleads, this adhesion microscopically correlated to a mild degree ofchronic-active heart epicardial inflammation surrounding the cardiaclead. This animal also had a minimal degree of chronic-active inflam-mation involving the lung pleura. In Animal 6016 there was a mildthoracic cavity adhesion between the left apical lung lobe and the5–6 intercostal thoracic wall, this adhesionmicroscopically correlatedto a mild degree of chronic active pleural inflammation on the lungswhich likely was related to the rib nodule inflammation around theDSI transmitter wire previously discussed.
The nature and magnitude of histological vascular changesresulting from intra-arterial catheterization were similar in animalsinstrumented with either PA-C10-LA (Group 2) or D70-CCTP devices(Groups 3 and 4). Catheterized femoral artery microscopic observa-tions (Table 8, Figs. 4–6) consisted of a discontinuity in the internalelastic lamina in 4 of 4 mid catheter artery sections (Group 3), andin 2 of 4 mid catheter artery sections and 2 of 4 catheter tip artery sec-tions (Group 4). In Group 3, neointima formation, characterized by anewly formed inner lining comprised primarily of smooth musclecells, was present in 4 of 4 mid catheter artery sections (all mild)and 3 of 4 catheter tip artery sections (all mild). In Group 4, similarevidence of neointima formation was present in 4 of 4 mid catheterartery sections (all mild) and 4 of 4 catheter tip artery sections (2minimal and 2 mild). The apparent cause of the internal elastic laminadiscontinuity and neointima formation was the intraluminal pressurecatheter placement and/or presence, as no similar findings were pres-ent in the non-catheterized arterial sections examined.
In Animal 6009 there was a minimal degree of chronic-active in-flammation involving the epicardium of the free wall of the ventricle(Table 9). Chronic-active inflammation, affecting the ventricle wasalso observed in animal 6014. A mild degree of chronic-active inflam-mation involving the atrium was present in Animals 6012 and 6016.Both of these epicardial inflammatory lesions were considered reac-tions to the cardiac and pericardiac leads present in these animals,
p 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP)
/4) + (4/4) + (2/4)(3/4), +++ (1/4) +++ (4/4) +++ (4/4)
/4) − + (2/4)(3/4) ++ (3/4) ++ (2/4), +++ (2/4)
++) present, moderate (+++++) present, severe.
e internal iliac artery (Groups 3 & 4; D70-CCTP) catheters were preserved in fixative,
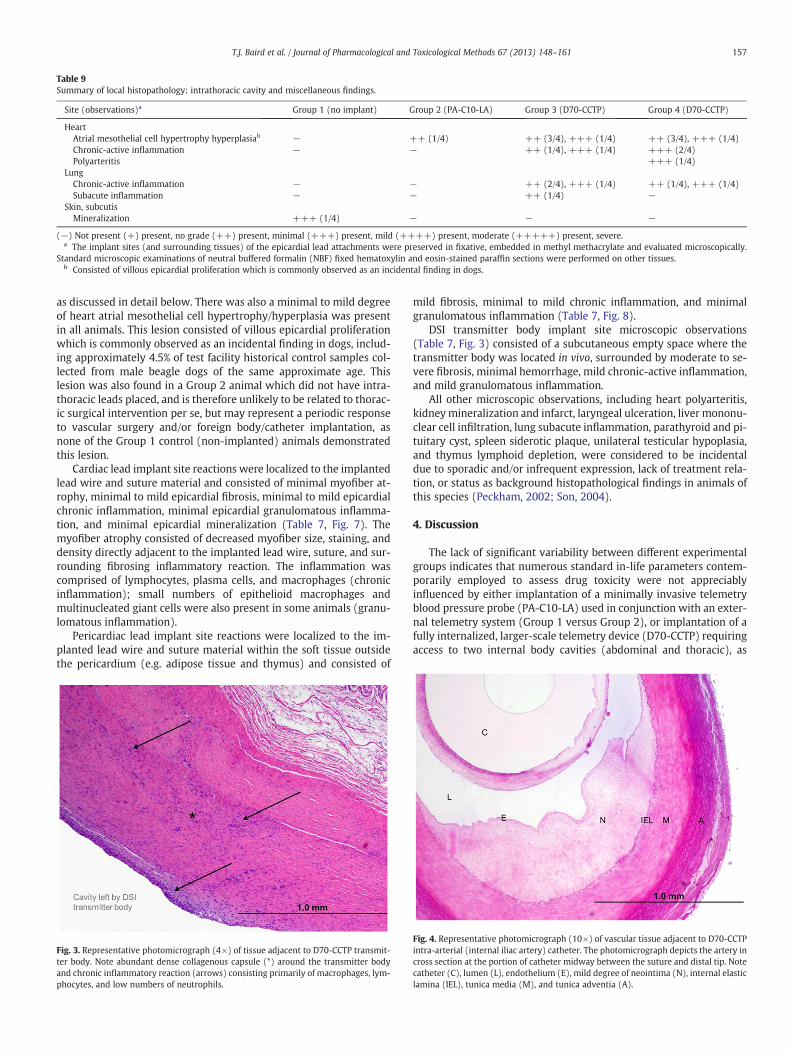
Table 9Summary of local histopathology: intrathoracic cavity and miscellaneous findings.
Site (observations)a Group 1 (no implant) Group 2 (PA-C10-LA) Group 3 (D70-CCTP) Group 4 (D70-CCTP)
HeartAtrial mesothelial cell hypertrophy hyperplasiab − ++ (1/4) ++ (3/4), +++ (1/4) ++ (3/4), +++ (1/4)Chronic-active inflammation − − ++ (1/4), +++ (1/4) +++ (2/4)Polyarteritis +++ (1/4)
LungChronic-active inflammation − − ++ (2/4), +++ (1/4) ++ (1/4), +++ (1/4)Subacute inflammation − − ++ (1/4) −
Skin, subcutisMineralization +++ (1/4) − − −
(−) Not present (+) present, no grade (++) present, minimal (+++) present, mild (++++) present, moderate (+++++) present, severe.a The implant sites (and surrounding tissues) of the epicardial lead attachments were preserved in fixative, embedded in methyl methacrylate and evaluated microscopically.
Standard microscopic examinations of neutral buffered formalin (NBF) fixed hematoxylin and eosin-stained paraffin sections were performed on other tissues.b Consisted of villous epicardial proliferation which is commonly observed as an incidental finding in dogs.
157T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
as discussed in detail below. There was also a minimal to mild degreeof heart atrial mesothelial cell hypertrophy/hyperplasia was presentin all animals. This lesion consisted of villous epicardial proliferationwhich is commonly observed as an incidental finding in dogs, includ-ing approximately 4.5% of test facility historical control samples col-lected from male beagle dogs of the same approximate age. Thislesion was also found in a Group 2 animal which did not have intra-thoracic leads placed, and is therefore unlikely to be related to thorac-ic surgical intervention per se, but may represent a periodic responseto vascular surgery and/or foreign body/catheter implantation, asnone of the Group 1 control (non-implanted) animals demonstratedthis lesion.
Cardiac lead implant site reactions were localized to the implantedlead wire and suture material and consisted of minimal myofiber at-rophy, minimal to mild epicardial fibrosis, minimal to mild epicardialchronic inflammation, minimal epicardial granulomatous inflamma-tion, and minimal epicardial mineralization (Table 7, Fig. 7). Themyofiber atrophy consisted of decreased myofiber size, staining, anddensity directly adjacent to the implanted lead wire, suture, and sur-rounding fibrosing inflammatory reaction. The inflammation wascomprised of lymphocytes, plasma cells, and macrophages (chronicinflammation); small numbers of epithelioid macrophages andmultinucleated giant cells were also present in some animals (granu-lomatous inflammation).
Pericardiac lead implant site reactions were localized to the im-planted lead wire and suture material within the soft tissue outsidethe pericardium (e.g. adipose tissue and thymus) and consisted of
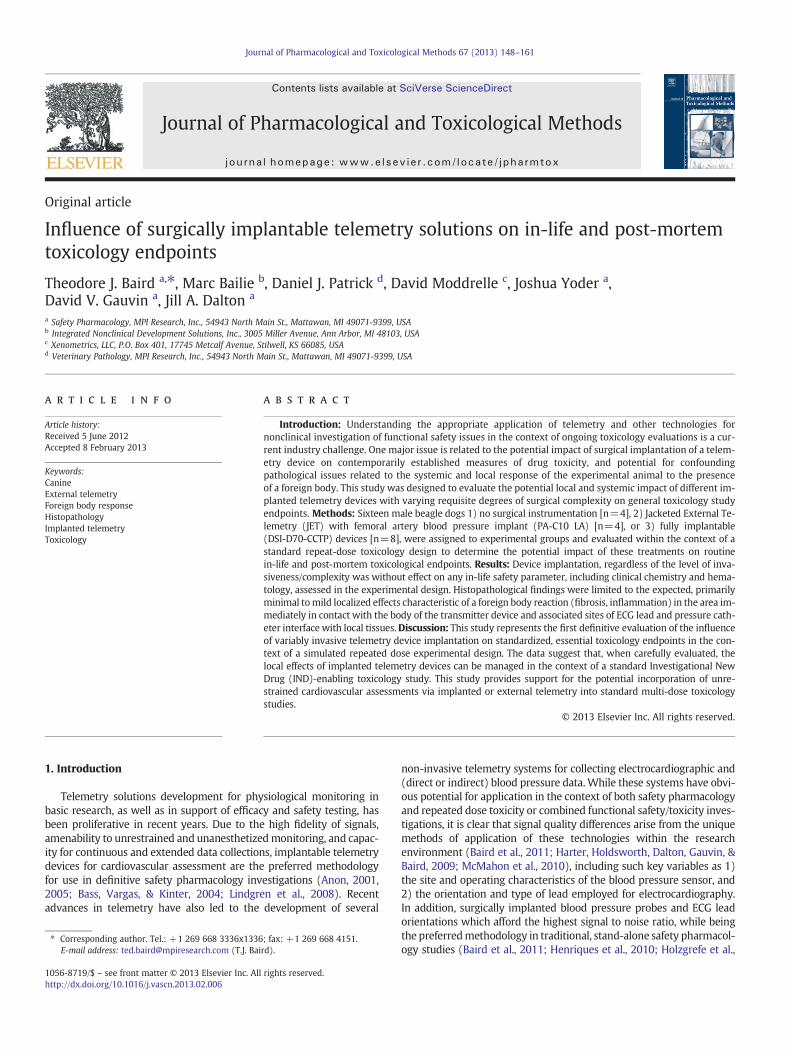
Fig. 3. Representative photomicrograph (4×) of tissue adjacent to D70-CCTP transmit-ter body. Note abundant dense collagenous capsule (*) around the transmitter bodyand chronic inflammatory reaction (arrows) consisting primarily of macrophages, lym-phocytes, and low numbers of neutrophils.
mild fibrosis, minimal to mild chronic inflammation, and minimalgranulomatous inflammation (Table 7, Fig. 8).
DSI transmitter body implant site microscopic observations(Table 7, Fig. 3) consisted of a subcutaneous empty space where thetransmitter body was located in vivo, surrounded by moderate to se-vere fibrosis, minimal hemorrhage, mild chronic-active inflammation,and mild granulomatous inflammation.
All other microscopic observations, including heart polyarteritis,kidneymineralization and infarct, laryngeal ulceration, liver mononu-clear cell infiltration, lung subacute inflammation, parathyroid and pi-tuitary cyst, spleen siderotic plaque, unilateral testicular hypoplasia,and thymus lymphoid depletion, were considered to be incidentaldue to sporadic and/or infrequent expression, lack of treatment rela-tion, or status as background histopathological findings in animals ofthis species (Peckham, 2002; Son, 2004).
4. Discussion
The lack of significant variability between different experimentalgroups indicates that numerous standard in-life parameters contem-porarily employed to assess drug toxicity were not appreciablyinfluenced by either implantation of a minimally invasive telemetryblood pressure probe (PA-C10-LA) used in conjunction with an exter-nal telemetry system (Group 1 versus Group 2), or implantation of afully internalized, larger-scale telemetry device (D70-CCTP) requiringaccess to two internal body cavities (abdominal and thoracic), as
Fig. 4. Representative photomicrograph (10×) of vascular tissue adjacent to D70-CCTPintra-arterial (internal iliac artery) catheter. The photomicrograph depicts the artery incross section at the portion of catheter midway between the suture and distal tip. Notecatheter (C), lumen (L), endothelium (E), mild degree of neointima (N), internal elasticlamina (IEL), tunica media (M), and tunica adventia (A).

Fig. 5. Representative photomicrograph (10×) of tissue adjacent to PA-C10-LAintra-arterial (femoral artery) catheter. The photomicrograph depicts the artery incross section at the portion of catheter midway between the suture and distal tip.Note catheter (C), layer of fibrin and erythrocytes (F) on surface of catheter, arteriallumen (L), endothelium (E), neointima (N), internal elastic lamina (IEL), tunicamedia (M), and tunica adventia (A). Also note discontinuity of internal elastic lamina(yellow arrow).
0
10
20
30
40
50
60
70
80
90
100
Per
cen
t (%
)
Percent Arterial Circumference Percent of Lumen Area
a
PA-C10-LA D70-CCTP
0
10
20
30
40
50
60
70
80
90
100
Per
cen
t (%
)
Percent Arterial Circumference Percent of Lumen Area
b
PA-C10-LA D70-CCTP
Fig. 6. a–b: Representation of the percent of arterial circumference or percent of lumenarea affected by neointima formation, as assessed at either the midpoint (a) or distaltip (b) of the arterial pressure catheter. Neointima formation was similar by eithermethod of assessment for both PA-C10-LA and D70-CCTP devices.
158 T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
applied in the present experiment (Groups 1 and 2 versus Groups 3and 4). Additionally, the lack of significant variability on thesein-life and post-mortem toxicology measures between animals in ex-perimental Groups 3 and 4 implies a stable and predictable surgicaloutcome, even with repeated application of a relatively invasive te-lemetry instrumentation protocol. Although there were local histo-pathological changes of a predictable nature observed in animals inGroups 2, 3, and 4 as a function of device implantation (foreignbody response), similar to results observed for in-life parameters,there were no significant differences in standard post-life endpointsas these are assessed on routine toxicology testing protocols.
This study represents the first definitive evaluation of the influ-ence of variably invasive telemetry device implantation on standard-ized, essential toxicology endpoints in the context of a simulatedrepeated dose experimental design. Perhaps somewhat surprisingly,there were no alterations in hematology, organ weights, macroscopicobservations, or microscopic histopathology indicative of a systemicchange in health status associated with surgical intervention and im-plantation with telemetry devices designed to persist in vivo for anextended period of time. Viewed alongside the post-life dataset, thepattern of ancillary in-life clinical and veterinary observational data,as well as body weight/food consumption, ophthalmology, electrocar-diography, and clinical pathology data, supports the interpretationthat surgical implantation of a telemetry device over a term consis-tent with the duration of this study did not confound the interpreta-tion of routinely assessed toxicology endpoints.
Although there were no biologically relevant systemic findings thatwould complicate interpretation of routinely collected in-life endpointsor organs/tissues, minimal to mild localized effects (fibrosis, chronicand/or granulomatous inflammation, etc.) were present in areas imme-diately in contactwith the body of the transmitter device and associatedsites of ECG lead and catheter interface with adjacent tissues. Becausethese findings were 1) predictable fromwell-characterized informationon the nature and development of foreign body response to biomate-rials such as those used in telemetry instrumentation, 2) highly local-ized to the direct interface of the tissue and device, and 3) minimal interms of severity of effect, these findings do not appear to complicate in-terpretation of routine toxicology study parameters such as those eval-uated in the course of the present investigation. Nevertheless, it seems
reasonable that the establishment of a historical dataset would serveto greatly facilitate contextual understanding of the nature ofdevice-related effects associated with different implantation proce-dures. This study represents an initial effort in this direction in the bea-gle dog. Possession of such reference data in all relevant species thatmight be employed on combined safety pharmacology/toxicologystudy designs (e.g., non-human primate, swine) would be expected tofacilitate data interpretation within individual laboratories employingsuch procedures.
The nature of the localized transmitter body, subcutaneous lead, andepicardial lead observations was similar to, and typical of, a well-contained, and biologically inconsequential foreign body tissue re-sponse (Anderson, Rodriguez, & Chang, 2008). Characteristics of the na-ture and magnitude of the vascular changes observed (intra-arterialinternal elastic lamina discontinuity and/or neointimal formation) inthis study have been reported with chronic implantation of similar de-vices (Authier et al., 2011), including those used with external teleme-try (McMahon et al., 2010). Similar to prior investigations, the presentstudy evaluations, which included specific assessment of differentiallylocated/invasive catheter sites (PA-C10-LA/femoral artery versus
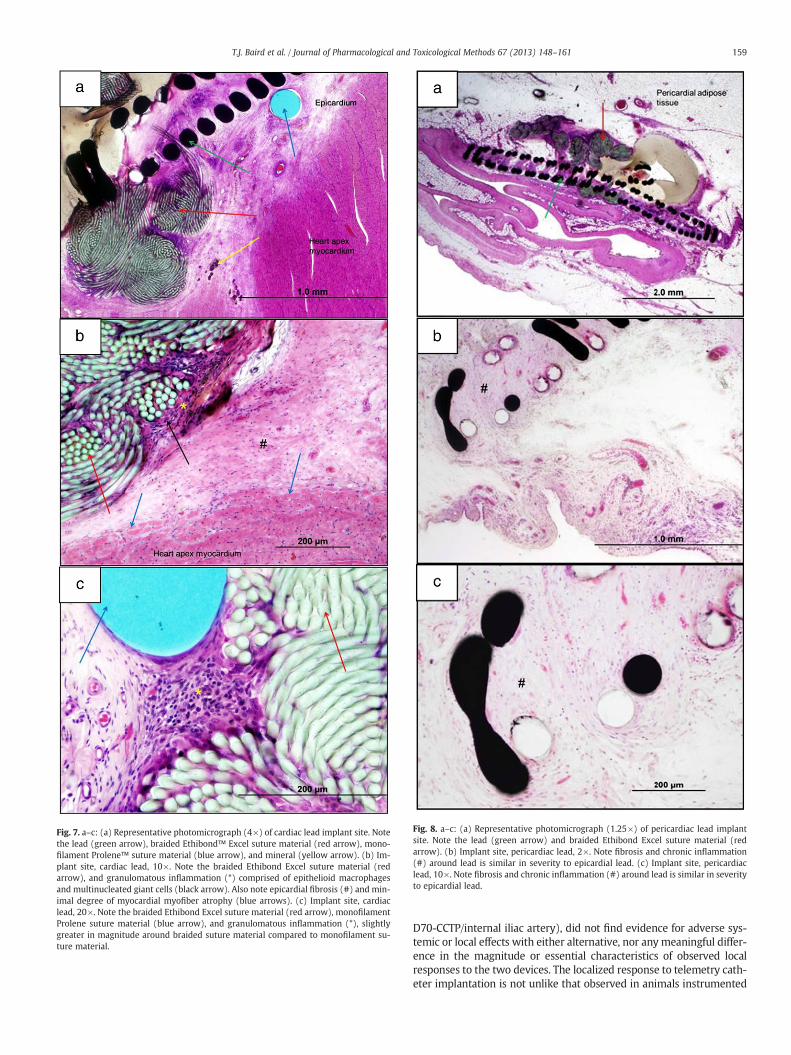
Fig. 7. a–c: (a) Representative photomicrograph (4×) of cardiac lead implant site. Notethe lead (green arrow), braided Ethibond™ Excel suture material (red arrow), mono-filament Prolene™ suture material (blue arrow), and mineral (yellow arrow). (b) Im-plant site, cardiac lead, 10×. Note the braided Ethibond Excel suture material (redarrow), and granulomatous inflammation (*) comprised of epithelioid macrophagesand multinucleated giant cells (black arrow). Also note epicardial fibrosis (#) and min-imal degree of myocardial myofiber atrophy (blue arrows). (c) Implant site, cardiaclead, 20×. Note the braided Ethibond Excel suture material (red arrow), monofilamentProlene suture material (blue arrow), and granulomatous inflammation (*), slightlygreater in magnitude around braided suture material compared to monofilament su-ture material.
Fig. 8. a–c: (a) Representative photomicrograph (1.25×) of pericardiac lead implantsite. Note the lead (green arrow) and braided Ethibond Excel suture material (redarrow). (b) Implant site, pericardiac lead, 2×. Note fibrosis and chronic inflammation(#) around lead is similar in severity to epicardial lead. (c) Implant site, pericardiaclead, 10×. Note fibrosis and chronic inflammation (#) around lead is similar in severityto epicardial lead.
159T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
D70-CCTP/internal iliac artery), did not find evidence for adverse sys-temic or local effects with either alternative, nor any meaningful differ-ence in the magnitude or essential characteristics of observed localresponses to the two devices. The localized response to telemetry cath-eter implantation is not unlike that observed in animals instrumented

160 T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
with chronic catheters designed to facilitate intravenous infusions(Gleason & Chengelis, 2000; Pickersgill & Burnett, 2000).
Although localized and benign histopathological changes of thetype commonly ascribed to “suture reaction” or local foreign body re-sponse were observed in animals instrumented with intrathoracic(epicardial) leads, these observations were not correlated in anymeaningful way with qualitative or quantitative electrocardiographicabnormalities, either as assessed from the evaluation of restrained,strip-chart ECGs (discussed herein, Section 3.1.4.), or based on subse-quent full review of 24-hour continuous telemetry recordings collect-ed following the second week of recovery from surgery. Incidentalfindings were limited to rare and sporadic atrial premature contrac-tions (APCs), ventricular premature contractions (VPCs), and rareand isolated blocked beats (2°AVB), which were found to be distrib-uted across animals in a random manner. Sinus pause was also rou-tinely observed in all animals. All of these “background” qualitativefindings previously have been described as occurring with greater rel-ative frequency in beagle dogs of the same age and sex as those eval-uated presently, including non-instrumented animals (Cools et al.,2011) and those with surgically placed (intrathoracic) epicardiallead arrays (Baird et al., in press; O'Donohue et al., 2011).
The present results have characterized, in the dog, the effects of var-iably invasive surgical implantation procedures with several alternativetelemetry device configurations in terms of the influence on a compre-hensive and representative sampling of toxicological endpoints of inter-est in contemporary drug safety evaluation. Results indicate a well-circumscribed and localized pattern of expected changes consistentwith foreign body reaction that result from in vivo utilization of such de-vices during the time-course of a typical repeated dose experimentdesigned to evaluate drug toxicity. The predictable nature of this re-sponse in the present experiment suggests the utility of establishingbackground historical data by similar efforts in other relevant speciesthat may be used to guide generalized tissue evaluation in toxicity stud-ies employing implantable telemetry for definitive cardiovascular evalu-ation. This effort would be analogous to that which has been formalizedfor infusion toxicology. With the present findings, such additional his-torical data will help support emerging alternative strategies for effec-tively characterizing diverse and sometimes challenging developmentprograms for new therapeutics.
Conflict of Interest
None of the authors have any financial or personal interests in MPIResearch, Inc., an independently owned contract research organiza-tion. Three authors (DVG, JAD, and TJB) are employed by the institu-tion in the capacity of Study Director.
References
Anderson, J. M., Rodriguez, A., & Chang, D. T. (2008). Foreign body reaction to biomate-rials. Seminars in Immunology, 20, 86–100.
Anon (2001). U.S. Department of Health and Human Services, Food and Drug Administra-tion, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluationand Research (CBER), Guidance for Industry. S7A: Safety Pharmacology Studies forHuman Pharmaceuticals (ICH S7A).
Anon (2005). U.S. Department of Health and Human Services, Food and Drug Administra-tion, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluationand Research (CBER), Guidance for Industry. S7B: The Non-clinical Evaluation of thePotential for Delayed Ventricular Repolarization (QT Interval Prolongation) byHuman Pharmaceuticals (ICH S7B).
Anon (1997). U.S. Department of Health and Human Services, Food and Drug Administra-tion, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluationand Research (CBER), Guidance for Industry. S6: Preclinical Safety Evaluation of Bio-technology Derived Pharmaceuticals. ICH S6.
Anon (2010a). U.S. Department of Health and Human Services, Food and Drug Administra-tion, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluationand Research (CBER), Guidance for Industry. S9: Nonclinical Evaluation for Antican-cer Pharmaceuticals (ICH S9).
Anon (2010b). U.S. Department of Health and Human Services, Food and Drug Adminis-tration, Center for Drug Evaluation and Research (CDER), Center for Biologics Evalua-tion and Research (CBER), Guidance for Industry. M3(R2): Non-Clinical Safety
Studies for the Conduct of Human Clinical Trials and Marketing Authorization forPharmaceuticals. ICH M3(R2).
Auletta, C. S. (2002). Acute, Subchronic, and Chronic Toxicology. In M. J. Derelanko,& M. A. Hollinger (Eds.), Handbook of Toxicology (2nd ed.). Boca Raton: CRCPress.
Authier, S., Moon, L. B., Stonerook, M., Fournier, S., Gervais, J., Maghezzi, S., et al. (2011).Evaluation of a novel ECG lead placement method in telemetered freely movingcynomolgus monkeys: Assessment of an intravascular biopotential lead. Journalof Pharmacological and Toxicological Methods, 64, 145–150.
Baird, T. J., O'Donohue, K. P., Posthumus, T. N., Abernathy, M. M., Glidewell, T., May, J. R.,et al. (2011). Influence of the local laboratory environment and selection of telem-etry application on quantitative ECG sensitivity. Journal of Pharmacological and Tox-icological Methods, 64, e42–e43.
Baird, T. J., O'Donohue, K., Posthumus, T., Eliel, M. W., Gauvin, D. V., & Dalton, J. A. (inpress). Comparison of Telemetry Derived Epicardial and Intravascular Electrocar-diogram Characteristics in Beagle Dogs. Journal of Pharmacological and ToxicologicalMethods.
Bass, A. S., Vargas, H. M., & Kinter, L. B. (2004). Introduction to nonclinical safety phar-macology and the safety pharmacology society. Journal of Pharmacological and Tox-icological Methods, 49, 141–144.
Cools, F., Janssens, S., Vanlommel, A., Teisman, A., Towart, R., & Gallacher, D. J. (2011). J.ECG arrhythmias in non-implanted vs. telemetry-implanted dogs: Need for screen-ing before and sufficient recovery time after implantation. Journal of Pharmacolog-ical and Toxicological Methods, 64, 60–67.
Cavero, I. (2010). Cardiovascular system assessment best practices: A Safety Pharma-cology Society meeting. Expert Opinion on Drug Safety, 9, 855–866.
Gauvin, D. V., Tilley, L. P., Smith, F. W. K., & Baird, T. J. (2009). Prevalence and types ofspontaneous cardiac arrhythmias recorded in three experimentally- anddrug-naïve laboratory species (canine, primate, swine) used in toxicology andsafety assessment studies. Journal of Pharmacological and Toxicological Methods,59, 57–61.
Gleason, T. R., & Chengelis, C. P. (2000). The ambulatory model in dog multidose infu-sion toxicity studies. In G. Healing, & D. Smith (Eds.), Handbook of Pre-clinical Con-tinuous Intravenous Infusion London: Taylor & Francis.
Guth, B. D., Bass, A. S., Briscoe, R., Chivers, S., Markert, M., Siegl, P. K. S., et al. (2009).Comparison of electrocardiographic analysis for risk of QT interval prolongationusing safety pharmacology and toxicological studies. Journal of Pharmacologicaland Toxicological Methods, 60, 107–116.
Harter, M., Holdsworth, D., Dalton, J., Gauvin, D., & Baird, T. (2009). Evaluation ofquantitative and morphological characteristics of the electrocardiogram asrecorded simultaneously by non-invasive and standard implantable telemetryin beagle dogs and cynomolgus monkeys. International Journal of Toxicology,28, 49.
Henriques, T. A., Beck, T. W., Douglas, C. L., Jones, H. M., Kremer, J. J., Kruzich, P. J., et al.(2010). Left thoracotomy surgical approach for chronic instrumentation in dogsand monkeys providing high quality electrocardiogram signals. Journal of Pharma-cological and Toxicological Methods, 62, 136–142.
Holdsworth, D. L., O'Donohue, K. P., Smith, F. W. K., Jr., & Baird, T. J. (2011). Incidence ofArrhythmia in Cynomolgus Monkeys Instrumented for Telemetry with Epicardial(EPI) ECG Lead Orientation. Journal of Pharmacological and Toxicological Methods,64, e44.
Holzgrefe, H. H., Cavero, I., Gleason, C. R., Warner, W. A., Buchanan, L. V., Gill, M. W.,et al. (2007). Novel probabilistic method for precisely correcting the QT intervalfor heart rate in telemetered dogs and cynomolgus monkeys. Journal of Pharmaco-logical and Toxicological Methods, 55(2), 159–175.
Legendre, A. M., & Dade, A. W. (1974). Calcinosis circumscripta in a dog. Journal of theAmerican Veterinary Medical Association, 164(2), 1192–1194.
Leishman, D. J., Beck, T. W., Dybdal, N., Gallacher, D. J., Guth, B. D., Holbrook, M., et al.(2012). Best practice in the conduct of key nonclinical cardiovascular safety as-sessments in drug development: Current recommendations from the SafetyPharmacology Society. Journal of Pharmacological and Toxicological Methods,65(3), 93–101.
Lindgren, S., Bass, A. S., Briscoe, R. B., Bruse, K., Friedrichs, G. S., Kallman, M. J., et al.(2008). Benchmarking safety pharmacology regulatory packages and best practice.Journal of Pharmacological and Toxicological Methods, 58, 99–109.
Matsuzawa, T., Masaharu, H., Nara, H., Yoshida, M., Tamura, S., & Igarashi, T. (1997).Current status of conducting function tests in repeated dose toxicity studies inJapan. Journal of Toxicological Sciences, 22, 375–382.
McMahon, C., Mitchell, A. Z., Klein, J., Jenkins, A. C., & Sarazan, R. D. (2010). Evaluationof blood pressure measurement using a miniature blood pressure transmitter withjacketed external telemetry in cynomolgus monkeys. Journal of Pharmacologicaland Toxicological Methods, 62, 127–135.
O'Donohue, K., Holdsworth, D., Tapp, R., Harter, M., May, J., Abernathy, M., et al.(2011). A step-wise approach to quantitative arrhythmia assessment: Amulti-species and multi-drug validation. Journal of Pharmacological and Toxico-logical Methods, 66, 189.
Peckham, J. C. (2002). Animal Histopathology. In M. J. Derelanko, & M. A. Hollinger(Eds.), Handbook of Toxicology (2nd ed.). Boca Raton: CRC Press.
Pickersgill, N., & Burnett, R. (2000). The non-ambulatory model in dog multidose infu-sion toxicity studies. In G. Healing, & D. Smith (Eds.), Handbook of Pre-clinical Con-tinuous Intravenous Infusion London: Taylor & Francis.
Ploermen, J. P., Ravesloot, W. T., & van Esch, E. (2003). The incidence of thymic B lym-phoid follicles in healthy beagle dogs. Toxicologic Pathology, 31(2), 214–219.
Prior, H., McMahon, N., Schofield, J., & Valentin, J. -P. (2009). Non-invasive telemetricelectrocardiogram assessment in conscious beagle dogs. Journal of Pharmacologicaland Toxicological Methods, 60, 167–173.

161T.J. Baird et al. / Journal of Pharmacological and Toxicological Methods 67 (2013) 148–161
Sarazan, R. D., Mittelstadt, S., Guth, B., Koerner, J., Zhang, J., & Pettit, S. (2011). Cardio-vascular function in nonclinical drug safety assessment: Current issues and oppor-tunities. International Journal of Toxicology, 30, 272–286.
Son, W. C. (2004). Idiopathic canine polyarteritis in control beagle dogs from toxicitystudies. Journal of Veterinary Science, 5(2), 147–150.
Vargas, H. M., Bass, A., Breidenbach, A., Feldman, H. S., Gintant, G. A., Harmer, A. R., et al.(2008). Scientific review and recommendations on preclinical cardiovascular safetyevaluation of biologics. Journal of Pharmacological and Toxicological Methods, 58, 72–76.
Zwicker, L. A., & Pack, L. (2011). What is your diagnosis? Calcinosis circumscripta. Jour-nal of the American Veterinary Medical Association, 239(5), 575–576.