inhaled anticholinergics for copd: breathing life into the debate manish khullar, bsc pharm interior...
TRANSCRIPT

Inhaled Anticholinergics for COPD: Breathing Life into the Debate
Manish Khullar, BSc PharmInterior Health Pharmacy Resident
October 31, 2013
Learning Objectives
• Become familiar with the clinical presentation and risk factors associated with COPD
• Describe the classification of COPD and various methods of classification
• Be able to explain the evidence for inhaled anticholinergics in the management of severe COPD

Our PatientID 81 year old male admitted to EKRH on October 7th, 2013CC/HPI SOB for 1 week that’s been getting progressively worse
Headache, fatigue and confusion for 3 days prior to admissionMorning prior to admission felt “unsteady on his feet” Mild, productive cough
Allergies Azithromycin (hives)
Social History Lives at home with spouseNo alcoholQuit smoking 30 + years ago

Our PatientPast Medical History Medications Prior to Admission
Hypertension Hydrochlorothiazide 12.5mg po daily
Hyperlipidemia Rosuvastatin 20mg po daily
COPD Salbutamol MDI 100mcg INH q4h prnSalmeterol 50mcg/Fluticasone 250mcg INH BIDBudesonide 0.5mg/2mL nebules INH BIDIpratropium 40-80mcg INH QID and PRN Tiotropium 18ug INH dailyPrednisone 10mg po x 3 days tapering by 2mg q3d during exacerbations Home oxygen prn

Our PatientPast Medical History Medications Prior to Admission
GERD Pantoprazole 40mg po daily
BPH Dutasteride 0.5mg po daily
Community Acquired Pneumonia
Moxifloxacin 400mg po daily x 10 days (Sept/Oct 2013) Doxycycline 100mg po BID x 7 days (May 2013)
Pseudomonal lung infection (June 2013)
Ciprofloxacin 500mg po BID x 14 days

Review of SystemsVitals T: 36.8 BP: 118/64 HR: 64 RR: 24 SaO2: 91% RA
CNS GCS x 15, A+O x 3, dizzy
HEENT Normal
RESP Shortness of breathProductive cough (yellow/green phlegm) WheezingFEV1 : 40% from
CVS Ø
GI Normal
GU SrCr: 70 eGFR: 94
MSK/DERM Weakness
ENDO Ø
HEME WBC: 12.2 Neuts: 6.6
LYTES Na: 136 K: 4.1 Cl: 96
Investigations
• Diagnostics:– Chest x-ray (upon admission):• Bibasilar atelectasis and scarring of the lungs

Current Problems and Medications COPD Exacerbation Prednisone 50mg po daily x 5 days
Suspected Pseudomonal Lung Infection
Ceftazidime 2 grams IV q8hTobramycin 570mg IV daily
Chronic COPD Salbutamol 0.5mg + Ipratropium 2.5mg/3mL nebules INH QID + PRNTiotropium 18mcg INH daily Salmeterol 50mcg/Fluticasone 250mcg INH BIDBudesonide 0.5mg/2mL nebules INH BID
Hyperlipidemia Atorvastatin 40mg po daily
BPH Tamsulosin SR 0.4mg po daily
VTE Prophylaxis Heparin 5000 units SC BID GERD Pantoprazole 40mg po daily

List of DRPs 1) JM is at risk of adverse effects of corticosteroids (headaches, nausea, infections,
throat irritation, oral thrush) secondary to receiving duplicate therapy and would benefit from reassessment of his COPD therapy
2) JM is at risk of adverse effects of inhaled anticholinergics (headaches, chest pain, respiratory tract infections, urinary retention, dry mouth) secondary to receiving duplicate therapy and would benefit from reassessment of his COPD therapy
3) JM is at risk of adverse effects without added benefit secondary to concomitant use of tiotropium and ipratropium and would benefit from reassessment of his COPD therapy
4) JM is at risk of adverse effects without added benefit secondary to concomitant use of budesonide and fluticasone and would benefit from reassessment of his COPD therapy

DRP Focus
• JM is at risk of adverse effects (headaches, chest pain, respiratory tract infections, urinary retention, dry mouth) without added benefit secondary to concomitant use of tiotropium and ipratropium and would benefit from reassessment of his COPD therapy

Background: Classification of COPD
• By Symptoms:COPD Stage Symptoms
Mild SOB when hurrying on the level or walking up a slight hill
Moderate SOB causing patient to stop after walking appox 100 m on level
Severe SOB from COPD resulting in patient being too breathless to leave the house, breathless when dressing or undressing or presence of chronic respiratory failure or clinical signs of right heart failure
Can Resp J 2008;15:1-8

Background: Classification of COPD
• By Lung Function: COPD Stage Spirometry (postbronchodilator)
Mild FEV1 > 80% predictedFEV1/FVC<0.7
Moderate 50% < FEV1 <80% predicted FEV1/FVC<0.7
Severe 30% < FEV1 <50% predictedFEV1/FVC<0.7
Very Severe FEV1 <30%FEV1/FVC<0.7
Can Resp J 2008;15:1-8
Clinical Presentation
• Chronic cough• Sputum production • Dyspnea • Wheezing and chest tightness
Can Resp J 2008;15:1-8

Back to Our Patient
• COPD stage=moderate-severe– PFT: FEV1 40% of predicted – SOB after walking 1 block – Frequent exacerbations (#/year unknown)– Chronic cough– Sputum production

Goals of Therapy
• Reduce mortality • Prevent/decrease morbidity (hospitalizations,
exacerbations) • Prevent disease progression • Reduce signs and symptoms• Prevent adverse events• Improve quality of life

Therapeutic Approach
Can Resp J 2008;15:1-8

Clinical Question #1
• In a patient with moderate-severe COPD, will combination ipratropium and tiotropium as compared to either alone reduce mortality, number of exacerbations, and improve quality of life and symptoms without increasing the risk of adverse events?

Literature SearchDatabases Medline, google scholar
Search Terms Pulmonary Disease, Chronic ObstructiveIpratropiumTiotropiumCombination Therapy
Results 1 Review article (Dec 2012)• Hand searched references 2 trials

Cole 2012
Ann of Pharmacotherapy 2012, 46(12):1717-21

Kerstjens et al 2007Design Randomized, double-blind, placebo controlled three way cross over
studyPopulation Inclusion:
Clinical diagnosis of COPD (FEV1/FVC < 70% and FEV1 < 60% predicted) > 40 years of ageSmoking history > 10 pack yearsExcluded:Patients with asthma, atopy, allergic rhinitis or an elevated blood eosinophil count Baseline:N=60; mean age 63; ~75% male; 21 current smokers; FEV1 ~40%; 100% on respiratory medication
Intervention Tiotropium 18mcg (placebo); and added on ipratropium 40mcg or fenoterol 200mcg
Primary Outcome
Peak FEV1 (highest FEV1 minus steady-state baseline FEV1)

Kerstjens et al 2007: Methodology

Results: EfficacyFenoterol* Ipratropium* Placebo
(Tiotropium only) Baseline FEV1
(% of predicted)1170mL(40.1)
1170mL(40.1)
1170mL(40.1)
Peak change in FEV1
315mL** 230mL** 178mL
*statistically significant versus placebo (p<0.0001) **Fenoterol statistically significant versus ipratropium (p<0.0001)

Results: SafetySide Effect Number of Participants Experienced
Headache Ipratropium (1), placebo (1)
Tachycardia 1 with fenoterol
Paresthesia 1 with fenoterol
Constipation 1 with placebo
Hypertension 1 with placebo
Study Limitations
• Methodology• Single day (2 doses)• Very short study• small sample size
• Clinically • FEV1 is a surrogate marker • Improvement in symptoms not reported• Patients in trial were not on B2 agonist + 2
anticholinergics at any one time?

Bottom Line of Study
“Add on therapy with fenoterol and ipratropium results in additional significant bronchodilation, although fenoterol was more effective as add-on therapy to maintenance tiotropium therapy in patients with COPD…”

Cazzola et al 2008Design Randomized, double blind, crossover design
Population Inclusion:Clinical diagnosis of COPD (FVC < 70%; FEV1 < 60% predicted)> 40 years of ageSmoking history > 10 pack yearsNo change in symptom severity/treatment in previous 4 wks No signs of respiratory tract infection in month prior to or during the trial Excluded:Patients with asthma, atopy, allergic rhinitis or an elevated blood eosinophil count, patients with BPHBaseline:N=30; age 69; ~80% male; 19/30 current smokers; FEV1 ~50%
Intervention Tiotropium 18mcg INH + salbutamol 600mcg INH vs tiotropium 18mcg INH + ipratropium 120mcg INH vs tiotropium 18mcg INH + placebo
Primary Outcome FEV1 improvement induced by salbutamol 600mcg, ipratropium 120mcg or placebo over tiotropium 18mcg

Cazzola et al 2008: Methodology
• 3-way crossover, double-blind treatment • Tiotropium for a 6 month period• 3 hours post-tiotropium dose, add on
treatment with one of the following:• Ipratropium 120mcg• Salbutamol 600mcg• Placebo
• Cumulative dose; 3 non-consecutive days • 1 puff, 1 puff, 2 puff, 2 puff regimen

Results
Figure 1. Mean dose-response curves to inhaled salbutamol, ipratropium or placebo 3 hours after inhaling tiotropium 18mcg
Results: Safety
• No adverse effects were reported throughout the trial…

Limitations• Methodology
• Single day /very short study• Sample size was small (30)• Used higher than normal doses; unknown significance at lower doses
• Clinically • FEV1 is a surrogate marker • Improvement in symptoms not identified
• Relevance to our patient?• The patient was currently on both inhaled and oral corticosteroids;
excluded patients who had either for at least 3 months • Excluded patients with BPH • Patients in trial were not on B2 agonist + 2 anticholinergics at any one
time?

Bottom Line of Study
“…there is not much difference in bronchodilation between adding higher than conventional doses of salbutamol or ipratropium to tiotropium in patients with stable COPD”

Summary of Evidence for Combination Anticholinergic Therapy
Outcomes Benefit
Mortality ?
Exacerbations ?
Disease Progression ?
Signs/symptoms ?
Reduce adverse events ?
Improve QOL ?

Clinical Question #2
• In a patient with moderate-severe COPD, is tiotropium as compared to ipratropium more effective at reducing mortality, number of exacerbations, hospitalizations and improving quality of life and symptoms without increasing the risk of adverse events?

Literature SearchDatabases Medline, google scholar
Search Terms Pulmonary Disease, Chronic ObstructiveIpratropiumTiotropium
Limits a. RCTs, english, humansb. meta-analyses
Results 14 RCTS• 1 RCT: head to head comparison • Excluded: non-relevant articles -cost-effectiveness ; pharmacoeconomics, drugs that are not of interest. 8 Meta-analyses • All MAs had multiple studies but only 1 RCT
comparing tiotropium vs ipratropium
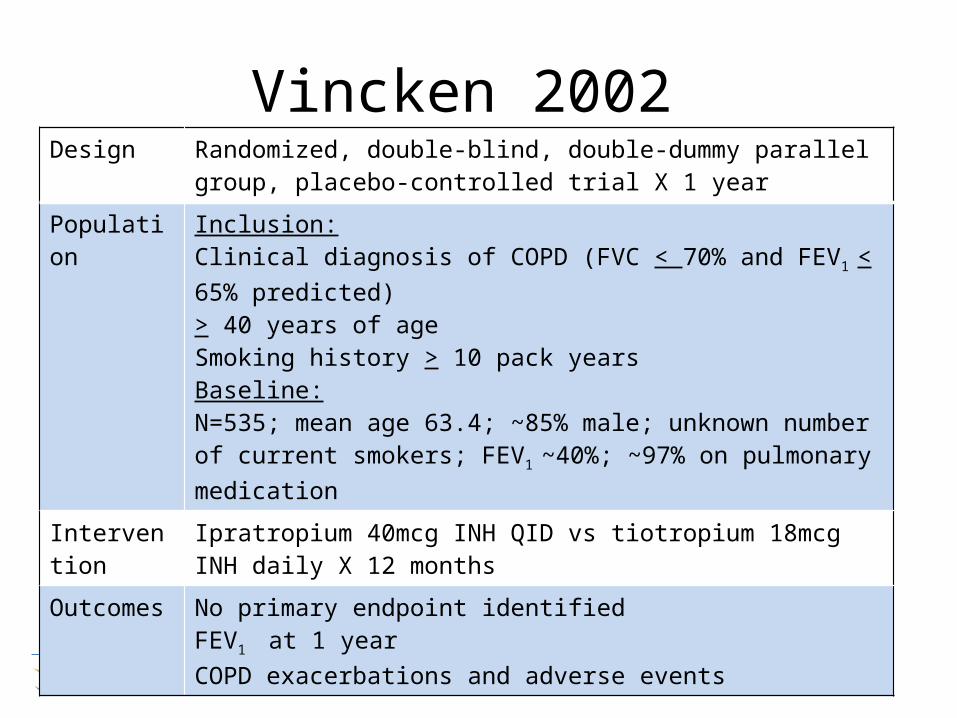
Vincken 2002 Design Randomized, double-blind, double-dummy parallel group, placebo-
controlled trial X 1 year Population Inclusion:
Clinical diagnosis of COPD (FVC < 70% and FEV1 < 65% predicted)> 40 years of ageSmoking history > 10 pack yearsBaseline:N=535; mean age 63.4; ~85% male; unknown number of current smokers; FEV1 ~40%; ~97% on pulmonary medication
Intervention Ipratropium 40mcg INH QID vs tiotropium 18mcg INH daily X 12 months
Outcomes No primary endpoint identifiedFEV1 at 1 year COPD exacerbations and adverse events

ResultsIpratropium
(n=179)Tiotropium
(n=356)P-value
FEV1 (at 1 year) Baseline: 1180mL
At 1 year: 1150mL
Baseline: 1250mL At 1 year: 1370mL
p<0.001
Hospitalizations 11.7% 7.3% P=0.11Exacerbations 46% 35% P=0.014
Meaningful increase in SGRQ*
35% 52% P=0.001
Withdrew due to adverse effects
12.8% (n=23)
10.1%(n=36)
P=0.089
Any treatment-related adverse related event
Dry mouth: 6.1%
Dry mouth: 12.1% -Mild, resolved during treatment in majority
of patients
P=0.03
*St. George’s Respiratory Questionaire

Study Limitations
• Methodology• Tiotropium n=356; Ipratropium n=179• 1 year study • Allocation concealment not defined (selection bias?)• Blinding of outcome assessment (detection bias?)• % of current smokers?
• Clinically • FEV1 is a surrogate marker • Patients in this trial were stable for 6 weeks prior to start of trial• Very small number of patients were on oral corticosteroids
(tiotroprium n=31; ipratropium n=19)• Participants were not on maximum dose of ipratropium (ie
320mcg/day)

Bottom Line of Study
“Tiotropium showed consistently greater efficacy across all of the aforementioned outcome measures compared to ipratropium….once daily administration of tiotropium should be considered as first-line maintenance treatment in patients with COPD”

Summary of Evidence: Tiotropium vs Ipratropium
Outcomes Benefit?
Mortality X
Exacerbations Y
Disease Progression ?
Signs/symptoms Y
Reduce adverse events Y
Improve QOL Y

Patient Specific Factors
• Tiotropium is once daily; Ipratropium is QID• Patient is already on multiple inhalers• Patient and wife appear to be confused with the approach to treatment and
inhaler use
• Tiotropium is expensive• Diagnosis of COPD (FEV1 < 0.65 and FEV/FVC <0.7) • Inadequate response to ipratropium after 3 months at 12 puffs daily • Must be prescribed by a respirologist to be covered by pharmacare• However, cost is not an issue for this patient
• Tolerability • Ipratropium is better tolerated• Tiotropium is associated with more dry mouth• Patient’s wife claims the patient seems to be doing better on tiotropium
(due to concomitant use?)

Alternatives for Symptom Management
• Short acting beta agonist• Salbutamol
• Anticholinergics• Ipratropium• Tiotropium• Combination ipratropium + tiotropium
• Long-acting beta-agonist– Salmeterol– Formoterol
• Inhaled corticosteroids

Therapeutic Recommendation
1) Discontinue ipratropium 40-80mcg INH QID and PRN
2) Discontinue budesonide 0.5mg/2mL nebules INH BID
3) Continue salbutamol 100mcg INH q4h prn4) Continue salmeterol 50mcg/fluticasone
250mcg INH BID5) Continue tiotropium 18mcg INH daily

What Actually Happened…
• Budesonide 0.5mg/2mL nebules INH BID was discontinued
• Physician, RT, patient and were unaware of how often the patient was using the combivent
• Physician wanted patient to remain on both anticholinergics
• Patient to have a diary and document use of each inhaler

Monitoring PlanEfficacy Degree of Change When
S: SOBAcute exacerbationsHospitalizations
AbsenceAbsenceAbsence
DailyOngoingOngoing
O: Vitals: RR, Sa02 Stable Daily
Toxicity Degree of Change When S: Headache
Dry mouthRespiratory tract infection Dyspepsia
PresencePresencePresence
Presence
OngoingOngoingOngoing
Ongoing O: Rash Presence Ongoing

Follow-up• Oct 10th:
• Patient improved clinically
• Oct 13th:• Patient continued to improve• Continued frequent inhaler use to control symptoms
• Oct 17th:• Course of antibiotics complete
• Oct 18th:• Medications were reconciled and plan was discussed with patient, physician and RT, with
physician and RT to follow-up with patient in community
• Oct 19th: • Patient discharged • New written care plan was provided
• Oct 29th:• Spoke with RT and patient is doing well and is improving and is no longer on ipratropium

Questions…
?