innovative clinical trial designs
TRANSCRIPT

Innovative Clinical Trial Designs: How to maximize the benefit?
Emad Shash, MBBCh., MSc., MD.
Medical Oncology Department
National Cancer Institute
Cairo University

What are we going to discuss today!Evidence
Based Medicine
Resources Utilization
Clinical Research
Innovation
• How are we used to perform clinical trials in Oncology?
• Does it fits in today’s needs?
• Integration of biology knowledge in shaping drug development
• New Clinical trial designs “Can they offer solution for accelerating drug development?”
• The supporting infrastructure role in clinical trial execution
Right PatientRight
Treatment
Right TimeCost
Effectiveness
Evolution Theory
Adaptation is always and should be according to Needs

Experimental design for Scurvy“James Lind 1716-1794”
12 classical SCURVY Sailors
Vinegar Diluted sulfuric acid Cider Sea Water Nutmeg & Garlic 2 Oranges & 1 Lemon
Normal diet + supplementation
(6 experimental groups)

Phases of Clinical Trials “what we are used to do”
Phase I
Drug given to 20-100 healthy volunteers (although patients in some cases)
Duration 1mth – 1 year
Cost $100K to $500K
Following studied here
• PK/PD
• Food interaction
• Safety
• Dose escalation/MTD
• Safety
• Early evidence of efficacy
Drug given to 100-500 patient volunteers
Duration 1 – 2 years
Cost $10M to $100M
Following studied here
• Efficacy
• Safety
• Establish dose for Phase III
Drug given to 1000-5000 patient volunteers
Duration 3 – 4 years
Cost $10M to $500M
Following studied here
• Confirmation of Efficacy
• Safety
Drug is launched in the market. 1000’s of patients
Many years
No specific amount
Additional post marketing testing of patients for drug
• Safety & Efficacy
• Support use of the approved indication
• Finding new therapeutic opportunities
• Extended use to different classes of patients
• 1000s of patients
Phase II Phase III Phase IV

Stages of drug development“Time & Money Consumption”
Source: “An Overview of the Drug Development Process”, by Ross Tonkens, M.D.
Phase I Phase IIIRESOURCES
≅15 Years≅30 M – 700 M

Continuous Decline in Healthcare & Research Spending

What are we going to discuss today!
Evidence Based
Medicine
Resources Utilization
Clinical Research
Innovation
• How are we used to perform clinical trials in Oncology?
• Does it fit our today’s needs?
• Integration of biology knowledge in shaping drug development
• New Clinical trial designs “Can they offer solution for accelerating drug development?”
• The supporting infrastructure role in clinical trial execution

Molecularly Targeted therapy Versus Conventional therapy
Patient
DrugBiomarker
Efficacy

Schwaederle M et al. JCO 2015
Better Biology Understanding & Treatment Outcome Optimization
Matching patients with drugs based on specific biomarkers
PubMed search
January 1, 2010, and December 31,
2012
570
phase II single-agent studies
32,149 patients

NSCLC Pathology: From Traditional View to more sub-molecular categorization

Advanced NSCLC: Evolution of Treatment
2000 - 2006 2006 - 2009 2010 2011 – 2017……..
EGFR mutation
ALK rearrangement
K-ras mutation
B-raf, HER2 mutation
ROS1, RET
Immunotherapy
Non-Squamous
Squamous
Targeting an Oncogenic Driver
EGFR mutation
Non-Squamous
Squamous
Non-Squamous
Squamous
NSCLC
Targeting EGFRTreating according histologyNSCLC

Time elapsed from discovery to practice change

The biomarker and drug development cycle
Patients-industry-Drug developers-
Translational researchers
Regulators
Payers
Analytical validation
Clinical validation
Clinical utility
Market access
Health care
delivery TR
Drug developers
Patients-Payers-Regulators-Industry
Time & Money Consumption while patients are waiting!!

Can we accelerate time? &
Still get the maximal benefit!

What are we going to discuss today!
Evidence Based
Medicine
Resources Utilization
Clinical Research
Innovation
• How are we used to perform clinical trials in Oncology?
• Does it fit in today’s needs?
• Integration of biology knowledge in shaping drug development
• New Clinical trial designs “Can they offer solution for accelerating drug development?”
• The supporting infrastructure role in clinical trial execution

Umbrella Trial
• Different targeted agents investigated in parallel in the same tumor type and within independent cohorts of patients
• Defined by specific molecular aberrations that could predict sensitivity to the investigational agent under assessment

Histology based clinical trial designTo evaluate multiple molecular aberrations

Le Tourneau et al. Lancet Oncol 2015Paoletti et al. CCO 2015
Molecularly targeted therapy based on tumor molecular profiling versus conventional therapy for advanced cancer (SHIVA) Trial: Proof-of-Concept

Le Tourneau et al. Lancet Oncol 2015
Molecularly targeted therapy based on tumor molecular profiling versus conventional therapy for advanced cancer (SHIVA) Trial: Proof-of-Concept
Molecularly targeted agent group (n=99)
Treatment at physician's choice group (n=96)
Age (years) 61 (54–69) 63 (54–69)
Sex
Female 60 (61%) 69 (72%)
Male 39 (39%) 27 (28%)
Previous lines of treatment 3 (2–5) 3 (2–5)
Royal Marsden Hospital score
0 or 1 51 (52%) 48 (50%)
2 or 3 48 (48%) 48 (50%)
Molecular pathway altered
Hormone receptor pathway 40 (40%) 42 (44%)
PI3K/AKT/mTOR pathway 46 (46%) 43 (45%)
RAF/MEK pathway 13 (13%) 11 (11%)

Adapted from: Le Tourneau et al. Lancet Oncol 2015
Molecularly targeted therapy based on tumor molecular profiling versus conventional therapy for advanced cancer (SHIVA) Trial: Proof-of-Concept
0 5 10 15 20 25
Breast adenocarcinoma
Colorectal cancer
Sarcoma
Adenocarcinoma of unknown primary
Non-adenoid cystic carcinoma salivary gland tumour
Neuroendocrine tumour
Cutaneous melanoma
Ependymoma
Germline tumour
Distribution By Tumor Type
Treatment at Physican Choice Moleculary Targeted Group
0
5
10
15
20
25
30
35
40
45
50
Hormone receptor pathway PI3K/AKT/mTOR pathway RAF/MEK pathway
Distribution By Molecular Abberation
Moleculary Targeted Group Physician Choice Group
Distribution of molecular alterations in the PI3K/AKT/mTOR pathway
Distribution of molecular alterations in the RAF/MEK pathway

Molecularly targeted therapy based on tumor molecular profiling versus conventional therapy for advanced cancer (SHIVA) Trial: Proof-of-Concept
Le Tourneau et al. Lancet Oncol 2015
Progression-free survival Intent to treat population
PI3K/AKT/mTOR pathway
RAF/MEK pathway

Molecularly targeted therapy based on tumor molecular profiling versus conventional therapy for advanced cancer (SHIVA) Trial: Proof-of-Concept
Le Tourneau et al. Lancet Oncol 2015
Progression-free survival Intent to treat population
PI3K/AKT/mTOR pathway
RAF/MEK pathway
• It is the first to test, with a randomized control, the idea of whether off-label use of commercial drugs for matched molecular biomarkers confers a clinical benefit.
• The results suggest that off-label use of molecularly targeted agents in this manner should be restricted.
• Instead, patients should be encouraged to participate in well-designed next-generation clinical trials that use an iterative and scientific approach to build on findings from trials such as SHIVA
• Irrespective of these limitations, SHIVA offers robust evidence for deficiencies in assigning therapy based on the various loose associations between biomarkers and inhibitors that are often provided in commercial clinical diagnostic reports.

Basket Trial
• Histology-independent trial design
• Patients with cancers of different histology enrolled in the clinical trial based on the presence of a specific molecular aberration

Histology-independentaberration-specific clinical trial design

EXAMPLE: NCI MPACT BASKET TRIAL
KummarS, et al., ASCO Annual Meeting 2014 poster
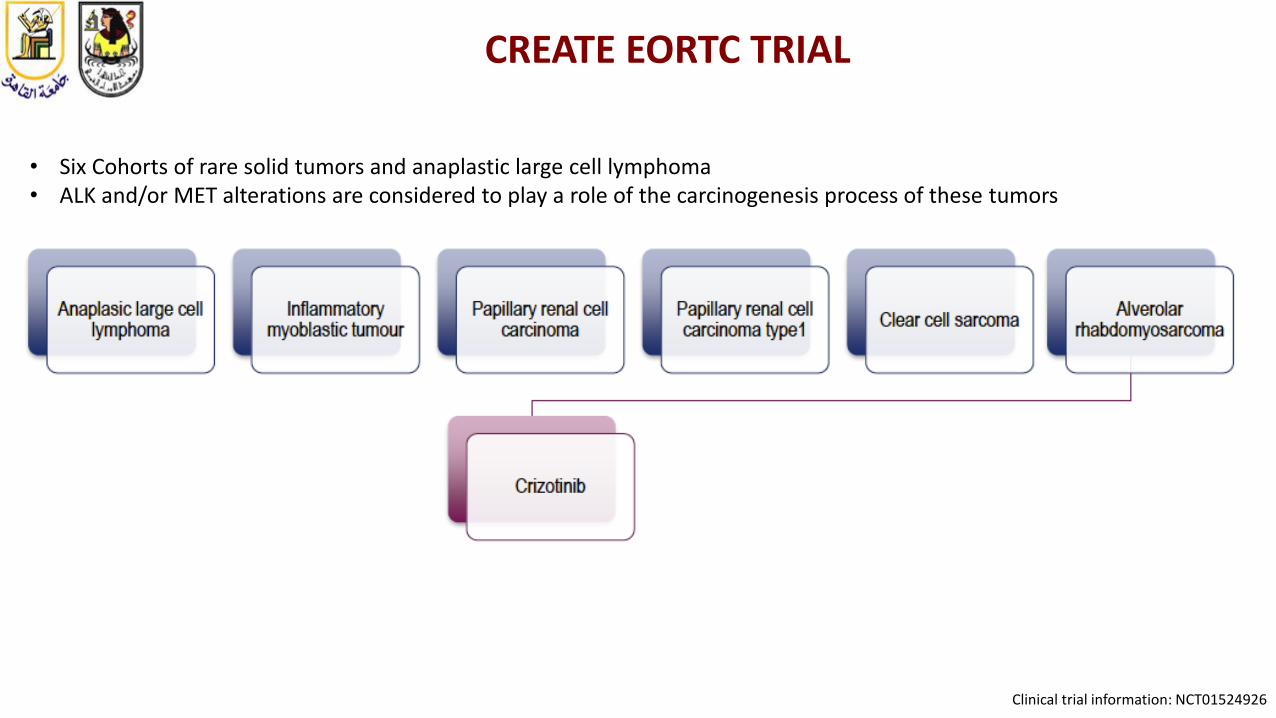
CREATE EORTC TRIAL
• Six Cohorts of rare solid tumors and anaplastic large cell lymphoma• ALK and/or MET alterations are considered to play a role of the carcinogenesis process of these tumors
Clinical trial information: NCT01524926

EORTC 90101 MET Driven (PRCC1 Cohort)
Schoffski et al. LBA AACR 2016

EORTC 90101 MET Driven (PRCC1 Cohort)
Schoffski et al. LBA AACR 2016

Basket of trials

BASKET TRIAL: PROS AND CONS
• Pros • Determining potential tumor efficacy of a single targeted agent in different
cancer types with the same gene abnormality
• Cons • Risk of overlooking the impact of tumor histology type. In fact, different
tumor responses by targeting the same mutation in several cancer types could be observed. (e.g. BRAF in melanoma versus BRAF in colorectal cancer: RR 50%-60% versus <5%)

ADAPTIVE TRIALS (1)
The principle of this trial is based on modifying parameters (dose, sample size, drug, schedule …) of a clinical trial evaluating a treatment in accord with observed outcomes in participants.

ADAPTIVE TRIALS (2)
Deepak et al. New Eng J Med 2016

ADAPTIVE TRIALS (3)
Deepak et al. New Eng J Med 2016

Park et al. New Eng J Med 2016
I-SPY 2
I-SPY 2 trialMulticenter, adaptive phase 2 trial of neoadjuvant therapy for:
• High risk clinical stage II or III breast cancer evaluated multiple new agents added to standard chemotherapy To assess the effects on rates of pathological
complete response

Park et al. New Eng J Med 2016
Neratinib (HKI-272; Puma Biotechnology)• an irreversible small-molecule inhibitor of the ErbB and the human
epidermal Growth factor receptor (HER) kinase family (epidermal growth Factor receptor, HER2, and HER4)
• It has shown promising activity against HER2-positive metastatic breast cancer.
• There is also evidence of preclinical activity against HER2negative tumor cells

Probability Distributions for SelectedBiomarker Signatures
Park et al. New Eng J Med 2016
Eligible women were categorized according to • 8 biomarker Subtypes on the basis of
• Human epidermal growth factor receptor 2 (HER2) status
• Hormone-receptor status• Risk according to a 70-geneprofile

Final Posterior and Predictive Probabilities of NeratinibEfficacy with Regard to 10 Biomarker Signatures
* The status of high-risk category 2 on the 70-gene profile was determined with the use of the MammaPrint assay
Park et al. New Eng J Med 2016

Final Posterior and Predictive Probabilities of NeratinibEfficacy with Regard to 10 Biomarker Signatures
* The status of high-risk category 2 on the 70-gene profile was determined with the use of the MammaPrint assay
Park et al. New Eng J Med 2016
• Neratinib reached the pre-specified efficacy threshold with regard to the HER2-positive, hormone-receptor–negative signature
• Neratinib added to standard therapy was highly likely to result in higher rates of pathological complete response than standard chemotherapy with trastuzumab among patients with HER2-positive, hormone-receptor–negative breast cancer.
ADAPTIVE TRIAL DESIGN: PROS AND CONS
• Pros• Faster evaluation of the drug
• Modification of drug, dosage and sample size during the trial according to the observed results
• Cons• Practical difficulties during the performance of the trial
• The clinicians are not familiar with the essential statistical part of this approach
• Active and dynamic follow-up of the trial is needed

WHAT ARE THE CHALLENGES OF THE NEW CLINICAL TRIAL DESIGNS?
• To show significant benefit in overall survival
• Rapidly evolving and not validated technics in use for tumor sequencing (NGS, circulating tumors cells, circulating tumor DNA…)
• High number of screened patients is needed
A strong infrastructure behind is needed to execute such trials with quality assurance

What are we going to discuss today!
Evidence Based
Medicine
Resources Utilization
Clinical Research
Innovation
• How are we used to perform clinical trials in Oncology?
• Does it fit our today’s needs?
• Integration of biology knowledge in shaping drug development
• New Clinical trial designs “Can they offer solution for accelerating drug development?”
• The supporting infrastructure role in clinical trial execution

The current fragmented approach of Drug & Biomarker related Development
Screening patients
Enrolling patients
Collecting tissue
Analyzing tissue
Collecting real-life data
Screening patients
Enrolling patients
Collecting tissue
Analyzing tissue
Collecting real-life data
Screening patients
Enrolling patients
Collecting tissue
Analyzing tissue
Collecting real-life data
Company A Company B Company C
QA/QC validated platforms & services
Collected data
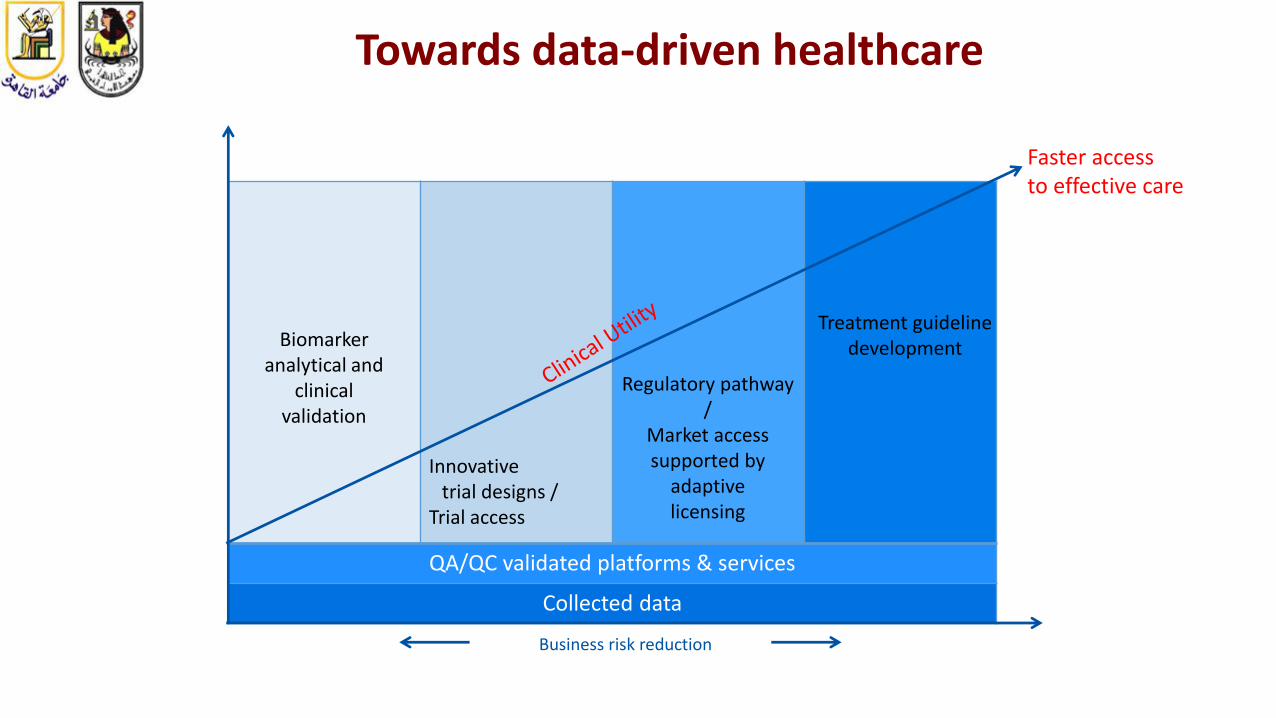
Towards data-driven healthcare
Faster access to effective care
Business risk reduction
Innovative trial designs /
Trial access
Regulatory pathway /
Market accesssupported by
adaptivelicensing
Biomarker analytical and
clinical validation
Treatment guideline development
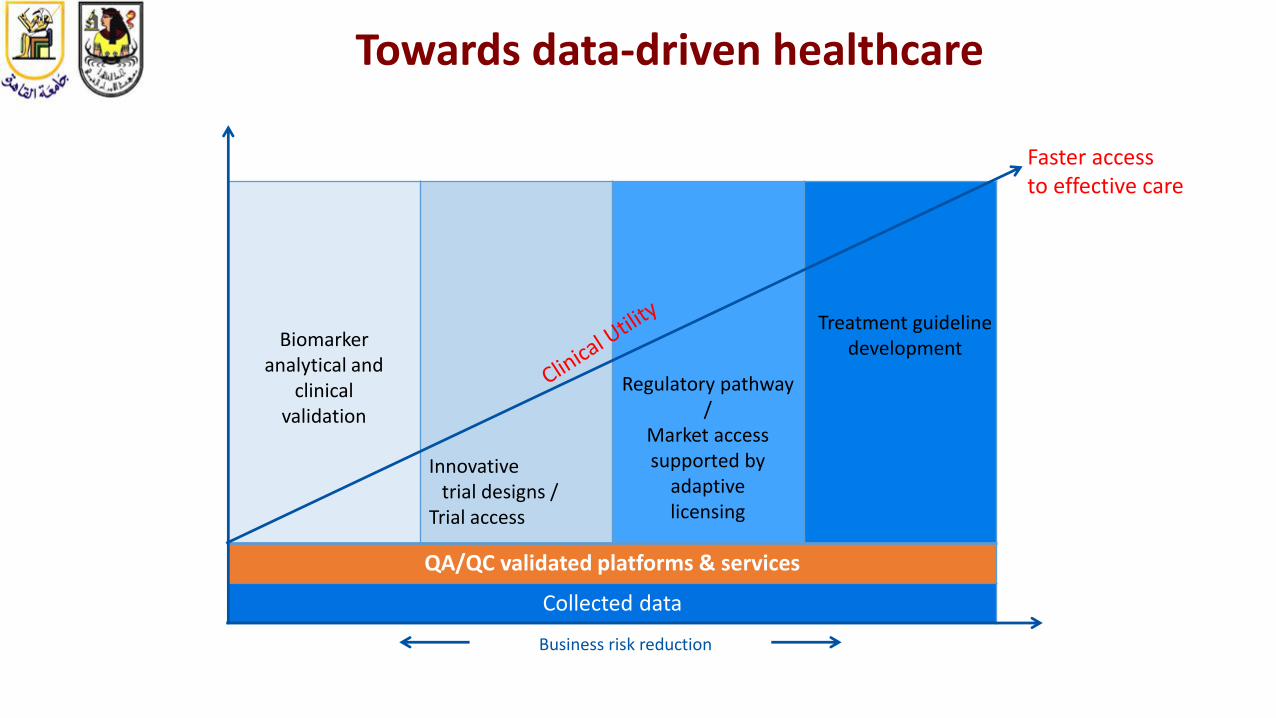
QA/QC validated platforms & services
Collected data
Towards data-driven healthcare
Faster access to effective care
Business risk reduction
Innovative trial designs /
Trial access
Regulatory pathway /
Market accesssupported by
adaptivelicensing
Biomarker analytical and
clinical validation
Treatment guideline development

• Clinical infrastructure
• Quality Assurance in RT(QART)
• Imaging• Translational Research Unit
• BiobankSample tool KEOSYS
platform
ORTA, VISTA, Safe,
PRISMA
QART
VODCA platform
EORTC Infrastructure as an “Example” supporting new generation clinical trials

Conclusion
• We need to adapt in our trials according to the accelerating needs
• Networking between institutions to render molecular tumor boardaccessible to the majority of centers and consequently to clinical trials and new drugs
• More collaboration with pharmaceutical companies due to the need of drugs (including off label drugs) with the different mechanisms of action to be used in precision medicine at the right time for the patient
• Validation Role of biomarkers and/or molecular imaging in determining mainly the negative predictive value of an evaluated drug
• We need the infrastructure that can support such complex trials

“In the long history of humankind (and animal kind, too) those who learned to collaborate and improvise most effectively have prevailed.”
Charles Darwin 1809-1882
Thank You