insights for care, partners for better health, pop up uni, 1pm, 2 september 2015
TRANSCRIPT
Speakers:
Dr Srikanth Bellary†, Clinical Director for Diabetes, Heart of England Foundation Trust
Farid Bidgoli, Associate Director of Market Access, MSD
Panel:
Hanno Ronte, Partner, Deloitte
Peter Pigden*, Patient Representative, Insights for Care
Declaration of Interests: None of the above participants have received an honorarium for this presentation †Honorariums and expenses have been provided previously for advisory services to MSD but not in relation to Insights for Care *Expenses have been provided to support attendance at the Insights for Care governance board meetings
August 2015 NOND‐1160089‐0000

For over 150 years, we have known that data can be used to transform
care
“The proposed [data gathering] would enable the mortality in hospitals, and also the mortality from particular diseases, injuries and operations, to be ascertained with accuracy, and these facts,
together with the duration of cases, would enable the value of particular methods of treatment and of special operations to be
brought to statistical proof” - Florence Nightingale, 1860
August 2015 NOND‐1160089‐0000

Nightingale identified that poor health, and not wounds, caused most military
deaths…use of her data reduced all-cause mortality from 42% to 2%
Evidence Based Policy ‘ Royal Commission on the Health of the Army’
Reduced rates of Infectious disease
All-cause mortality decrease : 42% to 2%
August 2015 NOND‐1160089‐0000

The Five Year Forward View identifies that data are central to achieving better
care in a financially sustainable way
• “Flat” funding with a need for transformational, disruptive change
• Evidence-based approach to future planning • New forms of care provision
‒ Evaluative component from establishment • Data assets to support system focus on integration of care
‒ Quality improvement / audits ‒ Research ‒ Risk stratification
August 2015 NOND‐1160089‐0000

Why Insights for Care?
August 2015 NOND‐1160089‐0000

Diabetes is an escalating national problem1
- 3.4 million patients to 5.6 million patients with Type 2 diabetes by 2035/36 in the UK - 9.8Bn to 16.9Bn of direct costs to the NHS by 2035/36 - 10% to 17% of NHS Expenditure
2010 2015 2020 2025 2030
5m
4m
3m
2m
1m
0m
9.5% 9.0%
8.5% 8.0%
English Diabetes Prevalence2
1. Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs, Diabetic Medicine, 2012 2. AHPO Diabetes Prevalence Model , November 2012
August 2015 NOND‐1160089‐0000

A pseudonymised data asset to provide a holistic view
of the whole pathway
Primary care Secondary Care
Pathology (LIMS)
E-prescribing
Nephrology
Diabetes
Imaging
Retinopathy
Solihull Community
CDS Administrative data
– Inpatient, outpatient,
A&E
Pathology results
Imaging activity and
scans
Retinal screening and
results
Community services
Inpatient prescriptions
Diabetes clinic specialist
database
Dialysis and other renal
specialist information
Other providers of care*
GP data
157 indiv idual
practices
– Indiv idual
engagement and data
agreements with each
practice
Pharmacy
Celesio Retail pharmacy
data
HE
FT
Info
rmati
cs
- P
seu
do
nym
isati
on
BCHC Birmingham City Council
Digital Health
Pro
vid
er
Syst
em
Pse
ud
on
ym
isati
on GP1
GP2
GPn
*On going discussions in relation to organisational participation in Insights for Care
August 2015 NOND‐1160089‐0000

Contributes:
Data access
Independence, scientific research credibility
Cross-setting relationships
Service redesign implementation
Contributes:
Project funding
Pharmaceutical expertise
Publication support
Contributes:
Technical expertise & capability
Information governance compliant trusted third party
Analysis & intellectual property
Project management
Insights for Care is a three-way Real World Evidence partnership
August 2015 NOND‐1160089‐0000
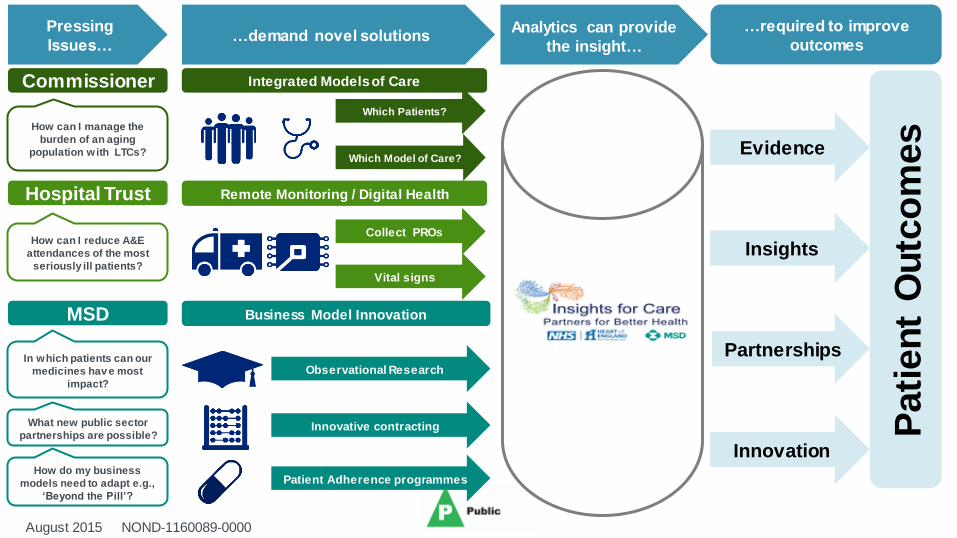
Commissioner
MSD
Hospital Trust
Pressing
Issues…
How can I manage the
burden of an aging
population with LTCs?
How can I reduce A&E
attendances of the most
seriously ill patients?
…demand novel solutions
Which Patients?
Remote Monitoring / Digital Health
Which Model of Care?
Observational Research
Innovative contracting
Evidence
Insights
Partnerships
Innovation
…required to improve
outcomes
Pati
en
t O
utc
om
es
Business Model Innovation
Collect PROs
Vital signs
Analytics can provide
the insight…
In which patients can our
medicines hav e most
impact?
How do my business
models need to adapt e.g.,
‘Beyond the Pill’?
What new public sector
partnerships are possible?
Integrated Models of Care
Patient Adherence programmes
August 2015 NOND‐1160089‐0000

Insights for Care can enable clinicians to do more by unlocking the
value of Real World Evidence
• My frustrations as a clinician in delivering care without adequate information and insight? ‒ What does my patient population actually look like? What is the local burden of disease and
demographic mix?
‒ How are my patients managed in primary care? How often to they visit their GP? What are their diagnoses and prescriptions?
‒ Who are my most vulnerable populations?
‒ Where can I make the biggest difference to my patients’ diabetes outcomes with new services?
‒ How can I demonstrate to my Trust and CCG that my new service intervention actually works?
August 2015 NOND‐1160089‐0000

Real World Evidence has the potential to address several key
limitations of classical clinical trials
• Currently, there are several limitations with clinical trials: ‒ Inclusion / exclusion criteria create an unrepresentative patient group (e.g., age groups, co-morbidities,
etc.)
‒ Cannot capture factors such as health professional behaviour, adherence to guidelines, etc.
‒ Limited ability to understand impact on long term outcomes
• Real World Evidence can address many of the above limitations:
‒ Provides insights into practical aspects of clinical care
‒ Allows design of care models that are appropriate for local communities (e.g., Retinal screening frequency, benefits of new therapies, hypoglycaemia, etc.)
‒ Allows resource investment to drive better outcomes through ongoing evaluation and improvement
August 2015 NOND‐1160089‐0000

It can help ensure patients living with diabetes have access to the most
appropriate treatment pathway…
• Risk stratification underpinned by analysis of patient demographic and clinical data can be used to ensure that treatment pathways are aligned with the current burden of a patient’s disease and its likely evolution
0%
5%
10%
15%
< 6.5 6.5 - 7.5
9.5 - 10.5
8.5 - 9.5
>10.5 7.5 - 8.5
Five-Year Mortality by baseline HbA1c
2008 2009 2010 2011 2012 2013 2014
0%
100%
98%
96%
Quartile 2
Quartile 1
Quartile 3
Quartile 4
Survival by IMD Quartile Hypothetical data, for Illustrative purposes only
August 2015 NOND‐1160089‐0000
HBA1C Year
Surv
ival
Mo
rtal
ity

…And that vulnerable groups of patients do not ‘slip through the net’
0%
25%
50%
75%
100%
45 + 40 - 45
15%
35 - 40
20%
75%
30 - 35
40%
25 - 30
50%
20 - 25
53%
15 - 20
54%
< 15
60%
Attend Education
Programme
Structured Education Attendance versus Index of Multiple Deprivation
• Attendance at structured education programmes drops off sharply for high-deprivation patient groups, identifying areas where new interventions have the potential to significantly improve outcomes
Key Target for New Interventions
Index modelled deprivation % o
f P
ts w
ith
Dia
be
tes
acce
ssin
g
stru
ctu
red
ed
uca
tio
n
Hypothetical data, for Illustrative purposes only

Insights for Care also has the potential to quantify the benefits of new
interventions
6
7
8
9
10
11
12
13
36 30 24 18 12 0 -12 -18 -24 -30 -36
Hb
A1c (
%) Median
Treated with single OAD Treated with multiple OAD
Q3
Q1
• We can track glycaemic durability in simplified Rx pathways – potentially allowing us to quantify the benefit of more intensive monitoring
Time to Transition to Insulin (Months)
Hypothetical data, for Illustrative purposes only
August 2015 NOND‐1160089‐0000

The IfC programme can also provide a range of organisational benefits
for Heart of England NHS Foundation Trust
• The Trust recognises key benefits for its community and development of services from the partnership: ‒ Deeper understanding of the community we serve
‒ Maximising the value of existing patient data to inform best care
‒ Tailoring of services to improve patient outcomes
‒ Improved future capacity planning and operational efficiency
‒ Greater research output for wide dissemination
‒ Improved Management against KPIs / targets
‒ Supporting professional development and attracting/retaining talent
August 2015 NOND‐1160089‐0000

The programme is underpinned by a robust governance framework…
• Insights for Care’s Information Governance processes and policies have been approved by the HEFT Caldecott Guardian and Board, and reviewed by Birmingham CrossCity CCG
• Our research protocol has been reviewed and received a favourable opinion by HEFT’s and MSD’s internal research ethics processes and by the HRA South East Coast Surrey Research Ethics Committee
• We have also received positive feedback on project Information Governance from the HRA Confidentiality Advisory Committee (CAG)
‒ The CAG confirmed “the data disclosed to Deloitte was not considered to constitute confidential patient information as the identity would not be ascertainable by those in receipt of and processing data”
• The CAG also gave positive feedback on the level of patient engagement in IfC, and
the general governance arrangements in place
August 2015 NOND‐1160089‐0000

…And a multi-channel approach to external communications
• Patient awareness posters displayed in all HEFT clinics commonly visited by diabetic patients, communal areas in HEFT and in participating GP surgeries
• Patient awareness / opt-out leaflets (with freepost envelopes) displayed all HEFT clinics commonly visited by diabetic patients and in participating GP surgeries ‒ Available in English and five most common monoglot languages in
HEFT catchment
• Patient helpline at HEFT to answer enquiries • Presence on HEFT and CCG websites* • HEFT and CCGs communicating IfC to all GPs (participating and not) to
provide awareness should their patients make enquiries Note: * In process
August 2015 NOND‐1160089‐0000

Lessons Learnt
Have a shared vision! Drive each other!
Early engagement across all organisations
Underpin the collaboration with strong governance
Strong project planning and communications
• Build broad stakeholder relationships • Align benefits to addressing organisational challenges and objectives • Organically grow from one disease area of interest
• Governance by design • Identify external expertise to support Caldecott guardians and IT • Patient and public engagement and involvement
• Strong project management with weekly progress calls • Strong clinical engagement • Resourcing commitment from all parties
August 2015 NOND‐1160089‐0000

Thank you!
Questions for the Panel
August 2015 NOND‐1160089‐0000