insulin & antidiabetic drugs peng qing. objectives be able to describe the insulin...
TRANSCRIPT

Insulin & Antidiabetic Drugs
Peng Qing

Objectives
Be able to describe the insulin preparations, the effects of insulin, clinical uses and adverse reactions of insulin.
Be able to list the major oral drug classes used and give example.

Background
Diabetes mellitus classification: 1. Type I. insulin-dependent diabetes mellitus (IDDM):
pancreatic B cell destruction (immune-mediated in most cases)
2. Type II. non-insulin-dependent diabetes mellitus (NIDDM): > 90%, defects of insulin secretion and action, insulin resistance.
3. Type 3, other;
4. Type 4, gestational diabetes mellitus

Insulin
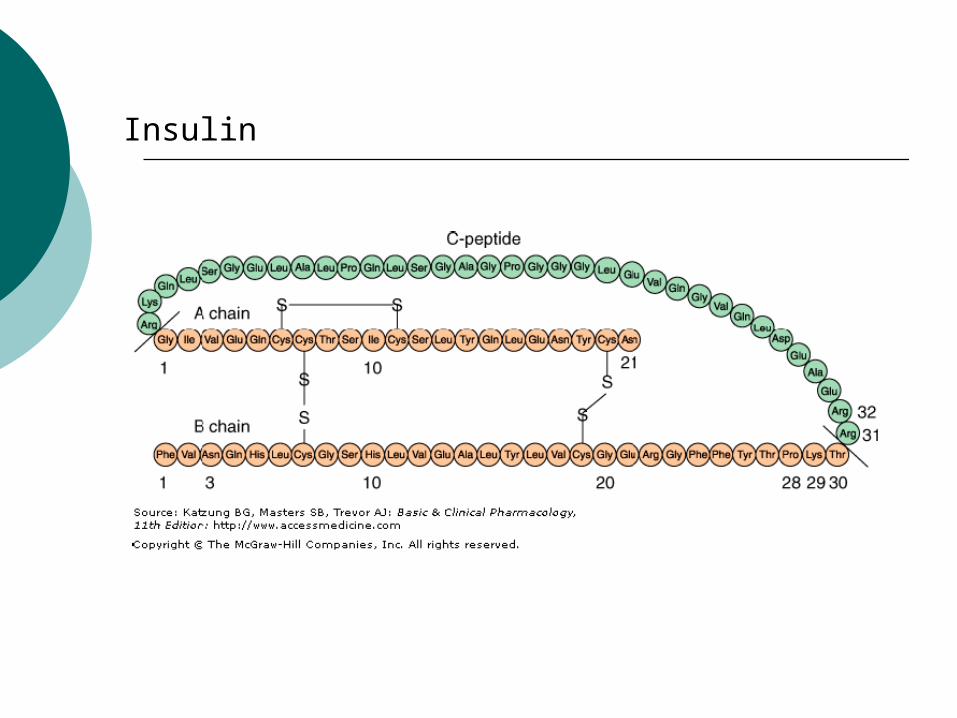
Small protein containing 51 amino acids arranged in two chains (A and B) linked by disulfide bridges.
Insulin and C-peptide are released from pancreatic B cells at a low basal rate and at a much higher stimulated rate in response to a variety of stimuli, especially glucose.
Insulin
Effects of Insulin on Its Targets
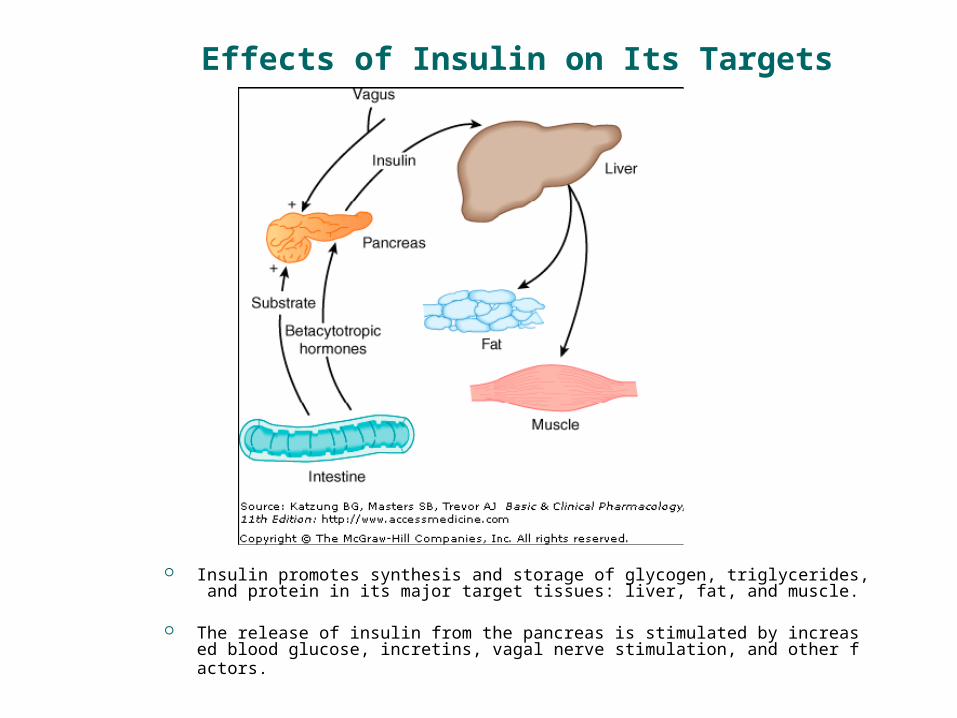
Insulin promotes synthesis and storage of glycogen, triglycerides, and protein in its major target tissues: liver, fat, and muscle.
The release of insulin from the pancreas is stimulated by increased blood glucose, incretins, vagal nerve stimulation, and other factors.


Principal types and duration of action of insulin preparations
Four principal types of injected insulins are available:
(1) rapid-acting, with very fast onset and short duration;(insulin aspart, insulin lispro)
(2) short-acting, with rapid onset of action; (Regular insulin )
(3) intermediate-acting; (protamine zinc insulin) (4) long-acting, with slow onset of action (Insulin gl
argine )

Pharmacokinetics
Insulin is a protein, which can be destructed by digestive enzyme. Oral adminstration is invalid.
Absorption is rapid when subcutaneous injection (i.h.)
Inactivation in liver and kidney.


Mechanism of Action
Insulin receptor on the membranes consists of two heterodimers( 异二聚体 ), each containing An α subunit, entirely extracellular and con
stitutes the recognition site. An β subunit, spans the membrane and co
ntains a tyrosine kinase( 激酶 ).

Phosphorylations results in multiple effects, including
-translocation of glucose transporters to the cell membrane with a resultant increase in glucose uptake;
- increased glycogen synthase activity and increased glycogen formation;
-multiple effects on protein synthesis, lipolysis, and lipogenesis; and enhance DNA synthesis and cell growth and division.

Clinical Uses
Therapy of all insulin deficient diabetes.1. IDDM (type 1)2. NIDDM (type 2) which cannot be controled by diet thera
py or oral hypoglycemic agents.3. Diabetes with acute or severe complication (Diabetic ke
toacidosis, hyperosmolar hyperglycemic syndrome).4. Diabetes accompanied severe infection, wasting diseas
e( 消耗性疾病 ), high fever, pregnance, trauma and operation.
5. Hyperkalemia.

Adverse Reactions
1.Hypoglycemia: most common complication of insulin therapy. relieved by
glucose administration
2.Insulin allergy: local or systemic urticaria results from histamine release fr
om tissue mast cells sensitized by anti-insulin IgE antibodies.

3.Insulin resistance: Acute resistance: induced by stress( 应激 ).
①insulin antagonist (eg, GC, adrenaline)↑; ②pH↓→ insulin-R↓; ③free fatty acid and ketone body in blood↑→ inhibit gluc
ose utilization. Chronic resistance:
①pro-receptor abnormality: anti-insulin antibodies;②receptor level change: number↓, or affinity↓③post-receptor abnormality: abnormal glucose transport
system or enzyme system in target cell. 4. Lipoatrophia at injection site( 脂肪萎缩 )
Oral Hypoglycemic Agents
Insulin sensitizerInsulin sensitizer
a-glucosidase inhibitorsa-glucosidase inhibitors
BiguanidesBiguanides
Insulin secretagoguesInsulin secretagogues

Insulin secretagogues :sulfonylureas
First-generation: tolbutamide( 甲苯磺丁脲 ; 甲糖宁 ; D860), chlorpropamide( 氯磺丙脲 )
Second-generation: glyburide( 格列本脲 ; 优降糖 ;降糖灵 ,glibenclamide), glipizide( 格列吡嗪 , 吡磺环己脲 ), glimepiride( 格列美脲 ); gliclazide( 格列齐特 , 达美康 )

Sulfonylureas
Mechanism of Action
-increase insulin release from the pancreas . -a reduction of serum glucagon levels
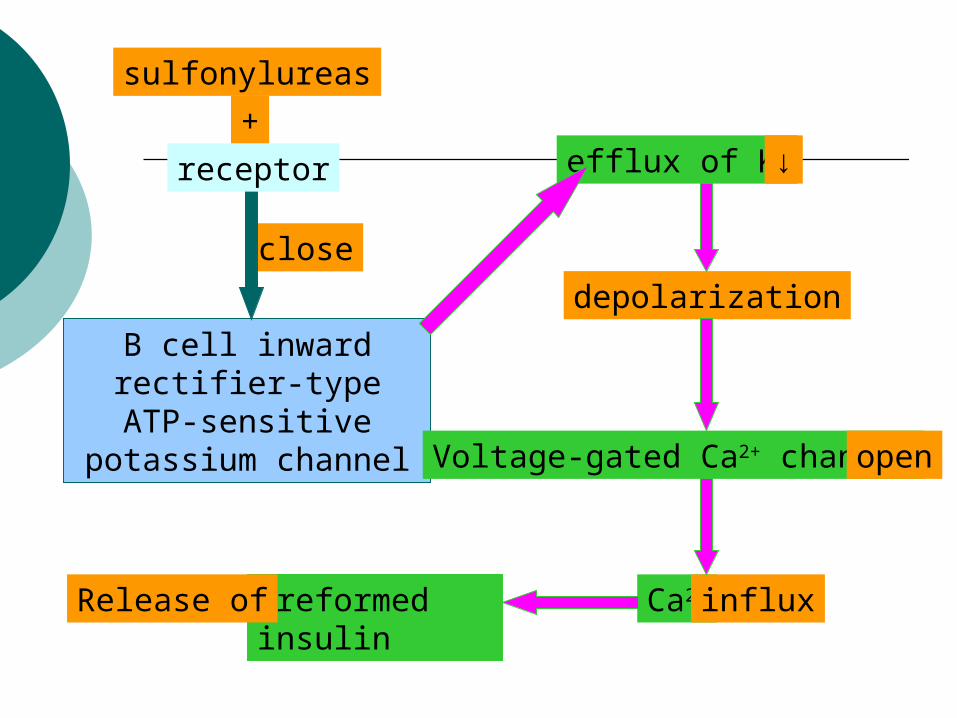
sulfonylureas
+
B cell inward rectifier-type ATP-sensitive potassium
channel
close
receptor
depolarization
Voltage-gated Ca2+ channel open
efflux of K+ ↓
Ca2+ influxpreformed insulinRelease of

Pharmacological Effects
1. Reduce blood glucose levels:
2. Stimulation of ADH secretion and potentiation of its action at the renal tubule → therapy of diabetes insipidus( 尿崩症 ).
3. Effects on blood coagulation: platelet adhesiveness↓, plasminogen( 纤溶酶原 ) synthesis↑
Clinical Uses
1. Type 2 diabetes with a functioning pancreas islet but invalid to diet therapy.
2. Diabetes insipidus( 尿崩症 ): chlorpropamide( 氯磺丙脲 )

Adverse Reactions
Cutaneous anaphylaxis( 皮肤过敏 ), gastrointestinal disorder, liver damage
Hematologic toxicity: leukopenia, blood platelet↓, hemolytic anemia
Persistent hypoglycemia
Contraindicated in patients with hepatic or renal insufficiency.

Insulin secretagogues: meglitinides
Repaglinide, the first member of the group, was approved for clinical use in 1998
modulate B-cell insulin release by regulating potassium efflux through the potassium channels.
has a very fast onset of action use in controlling postprandial glucose excursio
ns for type 2 diabetics.

Insulin Sensitizer
Insulin resistance Acquired: type 1 diabetes —— control bloo
d glucose Hereditary: type 2 diabetes —— insulin sen
sitizer Thiazolidinediones(Tzds, 噻唑烷酮类化合
物 ): rosiglitazone( 罗格列酮 ), pioglitazone( 吡格列酮 )

Pharmacological Effects
1. Tzds reduce insulin resistance2. Ameliorate lipid metabolism disturbance3. Prevent vascular complications in type 2 diab
etics4. Improve the function of pancreatic B cell

Mechanism of Action
Competitively activate peroxisome( 过氧化物酶 ) proliferator-activated receptor-γ(PPAR γ, nuclear receptor ) →
modulate the expression of the genes involved in lipid and glucose metabolism, insulin signal transduction, and adipocyte and other tissue differentiation.
Precautions and adverse effects
fluid retention, especially when used in combination with insulin or insulin secretagogues.
increased risk of heart failure Anovulatory women may resume ovulation and shoul
d be counseled on the increased risk of pregnancy.
hepatotoxicity
increased bone fracture in women.

Biguanides ( 双胍类 )
Metformin( 甲福明 , 二甲双胍 ), phenformin( 苯乙福明 ; 苯乙双胍 ; 降糖灵 )
Phenformin was discontinued in the USA because of its association with lactic acidosis and because there was no documentation of any long-term benefit from its use.
Not bound to plasma proteins, not metabolized, excreted by the kidneys as the active compound.

Mechanism of action remain elusive maybe includes: ①direct stimulation of glycolysis in tissues, wit
h increased glucose removal from blood; ②reduced hepatic gluconeogenesis; ③slowing of glucose absorption from the gastr
ointestinal tract④reduction of plasma glucagon levels.

Clinical Uses: 1. for patients whose hyperglycemia is due to i
neffective insulin action. Biguanides does not increase weight or provoke hypoglycemia.
Adverse Reaction: lactic acidosis gastrointestinal reaction(anorexia 食欲减退 , n
ausea, vomiting, abdominal discomfort, diarrhea),

Acarbose ( 阿卡波糖 )
α-glucosidase( 葡萄糖苷酶 ) inhibitors Mechanism: competed glycoside-hydrolase wit
h carbohydrate on the small intestine epithelium brush border → hydrolysis of carbohydrate↓→ delay the absorption of glucose.
Pharmacological Effect: lower the postprandial( 餐后 ) blood glucose levels.
Adverse Reactions: gastrointestinal discomfort.