insulin-like growth factor binding protein (igfbp) displacers: relevance to the treatment of renal...
TRANSCRIPT

Abstract Chronic renal failure (CRF) results in complexmetabolic and hormonal derangements, particularly inthe GH-IGF-IGFBP axis, which can be manifest in chil-dren as growth retardation. The decreased glomerular fil-tration rate (GFR) in CRF is associated with increasedplasma IGFBP levels, which may have an important rolein inhibiting the bioavailability of IGF-I. There is a largeliterature from both animal and human studies showingthat the administration of IGF-I can affect structure and function of normal and compromised kidneys. Wepropose an alternative therapeutic approach: activatingbound IGF by administering molecules that bind to theIGFBPs. In initial animal studies we used a mutant IGF,an IGF displacer, that binds to IGFBPs but not to IGF re-ceptors. In the rat this molecule activated the IGF systemand produced IGF-like effects in vivo, such as increasedkidney size, reduced serum creatinine, increased bonegrowth and increased body weight. Novel synthetic pep-tides have also been discovered which bind to specificIGFBPs, and we believe such molecules hold promise astherapeutic agents in renal disease.
Key words Insulin-like growth factor-I · Insulin-likegrowth factor binding proteins · Insulin-like growth factor binding protein displacers · Insulin-like growthfactor agonists · Insulin-like growth factor mimetics ·Renal failure
Introduction
The growth hormone (GH)–insulin-like growth factor(IGF-I) axis is a complex endocrine system that involvesthree peptide hormones, GH, IGF-I, and IGF-II, each withspecific receptors and binding proteins [1]. In the 1950sSalmon and Daughaday discovered a factor they subse-quently called “somatomedin” because it mediated the ac-tions of somatotrophin (GH), and was active in vitrowhere it could replicate some of the in vivo actions of GH.In the 1960s Froesch showed the presence of an “insulin-like” activity in serum that could not be inhibited by anti-insulin antibodies [2]. Further research in the 1970s and1980s determined that the Daughaday and Froesch “fac-tors” were in fact related peptides, structurally homolo-gous to insulin, and now known as IGF-I (formerly so-matomedin C) and IGF-II. The last decade has seen sixspecific IGF binding proteins (IGFBPs) purified, se-quenced and cloned. These IGFBPs have a high affinityfor IGF (but do not bind insulin) so that the IGF-I in bloodand in tissues is present largely bound to IGFBPs [1].
The IGFs, which can be synthesized by many tissues,including the kidneys, affect the metabolism, function,and growth of the kidney [3]. The past decade has alsoproduced evidence in humans that IGF-I improves renalfunction after acute renal failure (ARF) [4] and in chronicrenal failure (CRF) [5, 6]. In renal failure, there is an in-creased production and reduced renal clearance of IGF-BPs, resulting in increased blood IGFBP concentrations[7]. This excess IGFBP competes with IGF-I receptors forIGF-I, thereby reducing IGF bioactivity. By the use of anew class of molecule we have termed IGF displacers, itis possible to modify the total number of IGFBP bindingsites able to bind IGF-I, and increase IGF bioactivity invivo [8]. We have shown that IGF displacer moleculeswhen given to animals can affect renal structure and func-tion, and increase body weight. Because the IGFBPs arederanged in renal disease, it is possible that such IGF dis-placer molecules will be especially useful for treating pa-tients with renal failure, and related pediatric growth dis-orders.
V. Roelfsema · M.H. Lane · R.G. ClarkResearch Centre for Developmental Medicine and Biology, Faculty of Medicine and Health Science, University of Auckland,Auckland, New Zealand
R.G. Clark (✉)Research Centre for Developmental Medicine and Biology, Faculty of Medicine and Health Science, The University of Auckland, Private Bag 92019, Auckland, New Zealande-mail: [email protected].: +64-9-373-7599, Fax: +64-9-373-7497
Pediatr Nephrol (2000) 14:584–588 © IPNA 2000
R E V I E W A RT I C L E
Vincent Roelfsema · Mary H. Lane · Ross G. Clark
Insulin-like growth factor binding protein (IGFBP) displacers: relevance to the treatment of renal disease
Received: 12 April 1999 / Revised: 21 December 1999 / Accepted: 27 December 1999

585
IGF and IGF binding proteins
IGF-I and -II are bound by six different IGFBPs (IGFBP-1 to -6) with approximately 97% of the IGFs inserum being present in a bound form. The other IGF iseither in a bioactive free fraction (approximately 1%) orin an easily dissociable form [9]. Most IGF-I in the cir-culation is bound to IGFBP-3, which in turn complexeswith a third protein, the acid labile subunit (ALS), toform a 150-kDa moiety. This complex is too large toleave the circulation, prevents IGF from being degraded,and serves to store IGF in the circulation. A smallamount of the IGF in blood is bound to IGFBPs -1, -2, -4, -5 and -6, forming low molecular weight complexes(30–43 kDa) that can pass through capillaries [10]. IGF-BP-1 and -2 are also present in extravascular fluids suchas lymph and peritoneal fluid [11].
As shown in Fig. 1, the biological actions of IGFs aremediated through the membrane bound type I IGF recep-tor (IGF-1R). The IGFs bind the IGFBPs with higher af-finities than they bind the receptor; thus the IGF-I that isbound to IGFBP probably cannot directly activate theIGF-I receptor so the IGFBPs therefore regulate the ac-tivity of IGF-I [1]. In addition IGFBPs can be proteo-lysed or bind to the extracellular matrix, which lowersthe affinity of the IGFBP for IGF-I, and probably liber-ates IGF-I and therefore increases IGF activity [12, 13].In this article we propose (see Fig. 1) that the IGF boundto IGFBPs might also be activated by administering mol-ecules that bind to the IGFBPs. Since many componentsof the IGF system are expressed in the kidney and mayplay an important role in kidney physiology and patho-physiology [14], targeting the IGF system should im-prove kidney function in renal failure.
GH, IGF and IGFBP in renal failure
Chronic renal failure (CRF) causes many metabolic and hormonal derangements, including in the GH-IGF-IGFBP axis [7]. Because the kidneys have a significantrole in the clearance of GH from the circulation, serumlevels and serum half-life of GH in CRF are increased[15]. In children with CRF there is evidence for in-creased pulsatile release of GH [16], compared to normalchildren, resulting in a 2.5-fold increase in serum GH.While there is controversy as to whether total plasmaIGF levels are altered in CRF [7, 14], IGFBP-1, -2, -3, -4and -6 levels are increased, with levels increasing pro-gressively as renal function declines [17, 18]. Theamounts of intact IGFBP-3 are slightly decreased or nor-mal in CRF, but total IGFBP-3 levels are elevated due toproteolysis. The 29-kDa IGFBP-3 fragments have a 50-fold reduced affinity for IGF-I [19]. Since IGFBP-3 pro-tease activity is normal in CRF, the fragment accumula-tion appears to be due to reduced renal elimination [20].Serum IGFBP-4 concentrations are increased slightly inrenal failure; however, levels vary with nutritional status[21]. IGFBP-1 and -2 are increased the most in CRF andare inversely correlated with residual glomerular filtra-tion rate (GFR) [7]. In children the serum levels of IGF-BP-2, and to a lesser extent IGFBP-1, are correlated neg-atively with stature [22], suggesting that high IGFBPlevels contribute to the resistance to the metabolic andgrowth promoting properties of IGF-I that develop as re-nal failure progresses [23]. However, the beneficial ef-fects of GH in pediatric CRF and the efficacy of IGF-Ion renal function in CRF suggest that the hormone resis-tance may not be the major problem with the GH axis. Inanimals, increased IGFBP-1 levels have been shown toinhibit IGF-I as well as GH activity [24, 25], and the co-administration of IGF-I plus IGFBP-1 leads to an inhibi-tion of IGF activity [26]. Renal failure is a state of ex-cess IGFBPs, which are probably inhibitory, rather thana state of IGF deficiency. Therefore the use of IGF dis-placers to reduce IGFBP capacity might increase the bio-activity of the available IGF and improve or slow the de-cline in renal function in patients with CRF.
Animal studies
The normal kidney, and especially the damaged kidney,expresses IGF-I. This led to an examination of the roleof IGF-I in renal failure. Following acute renal failureIGF-I message and IGF binding sites are upregulated indamaged tubules, indicating that IGF-I may facilitatedifferentiation and act as a mitogen for tubular epithelialcells [27]. Furthermore, it has been demonstrated thatregeneration of damaged proximal tubular epithelia isaccelerated and recovery of normal renal function in-creased, when IGF-I was given to rats immediately afterischemic renal injury and that IGF-I treatment postinju-ry could reduce mortality [28–30].
Fig. 1 Schematic diagram of the mechanism of action of an IGFdisplacer compound. Interactions between IGF-I, IGFBPs, an IGFdisplacer (IGF-D) and the IGF type I receptor (IGF1-R) are illus-trated. IGFBPs bind IGF-I with high affinity so that normally littleIGF-I is available to bind to and activate IGF receptors. The intro-duction of an IGF displacer (IGF-D) will both prevent IGF-I bind-ing to an IGFBP and displace IGF-I that is bound to an IGFBP.The IGF-displacer will therefore act as an indirect IGF agonist byincreasing the amount of IGF-I that is available for binding to IGFreceptors
Initial studies testing IGF-I in animal models of CRFshowed no beneficial effect on renal function [31]. How-ever, more recent studies have suggested possible thera-peutic benefits of IGF-I in animals with CRF. Treatmentwith both IGF-I and GH has anabolic effects in rats withCRF, as seen by increases in food conversion efficiency,nitrogen retention, decreases in urinary potassium andprotein degradation, and enhanced long bone growth[32].
Clinical trials of IGF-I in renal failure
IGF-I has been tested as a possible therapeutic agent inCRF and end-stage renal disease (ESRD). In healthyadult men, recombinant human (rh) IGF-I rapidly in-creased GFR and renal plasma flow (RPF) by about30%, raising the hope that IGF-I would increase GFR inpatients with renal failure and postpone the need for dial-ysis therapy [33, 34]. Furthermore, rhIGF-1 has anaboliceffects which may improve nutritional status in CRF pa-tients. ESRD patients often suffer from protein-caloriemalnutrition, which in turn is associated with reduced se-rum IGF levels and reduced kidney mass. Clinically,malnutrition in such patients is a strong risk factor for in-creased morbidity and mortality [35]. In patients withmoderate renal failure, O’Shea et al. examined the effectof administering rhIGF-I (100 µg/kg b.i.d.) and noted animprovement in renal function and an increase in kidneysize over 4 days [36]. In a second, prolonged, study innine patients with ESRD, using the same dose of rhIGF-I,GFR increased by 23% after 4 days. However, in fivepatients treated with rhIGF-I for 13 and 27 days, therewas no long-term effect on inulin clearance or p-amino-hippurate (PAH) clearance and there were frequent andtroubling side effects [37]. The lack of a prolonged effectand the presence of side effects may have been related tothe large dose of IGF-I used, since prolonged therapy al-ters IGF-I bioavailability because of changes in the se-rum IGFBP profile [20]. Recently, Vijayan et al. showedin a prospective and double-blinded study that the abovementioned problems could be overcome by giving IGF-I(50 µg/kg/day) intermittently (4 days on treatment, 3 days off treatment), and that this treatment could im-prove renal function to that achieved by dialysis [5].
IGF displacers and renal function
Recently a new method of increasing the bioavailabilityof IGF-1 has been described. Two groups independentlymade two different human IGF-1 analogs (Leu24,59,60,ALA31hIGF-I [38], and Leu24Ala31hIGF-I) [8], which re-tain affinity for binding to the IGFBPs but show no ac-tivity on the IGF receptor. The idea is that displacementof some of the large pool of IGF-1 that is bound to IGF-BPs by an IGF displacer should elevate “free” levels ofIGF-1, and therefore increase IGF receptor activationand produce similar effects to the administration of IGF-
586
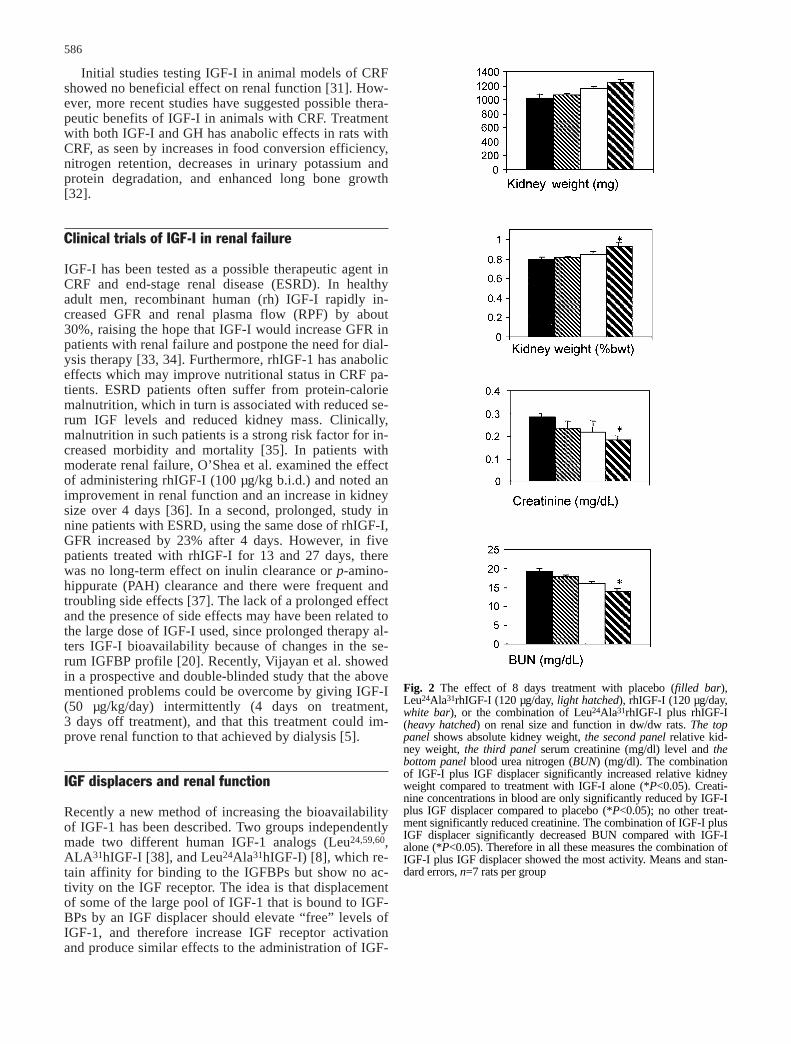
Fig. 2 The effect of 8 days treatment with placebo (filled bar),Leu24Ala31rhIGF-I (120 µg/day, light hatched), rhIGF-I (120 µg/day,white bar), or the combination of Leu24Ala31rhIGF-I plus rhIGF-I(heavy hatched) on renal size and function in dw/dw rats. The toppanel shows absolute kidney weight, the second panel relative kid-ney weight, the third panel serum creatinine (mg/dl) level and thebottom panel blood urea nitrogen (BUN) (mg/dl). The combinationof IGF-I plus IGF displacer significantly increased relative kidneyweight compared to treatment with IGF-I alone (*P<0.05). Creati-nine concentrations in blood are only significantly reduced by IGF-Iplus IGF displacer compared to placebo (*P<0.05); no other treat-ment significantly reduced creatinine. The combination of IGF-I plusIGF displacer significantly decreased BUN compared with IGF-Ialone (*P<0.05). Therefore in all these measures the combination ofIGF-I plus IGF displacer showed the most activity. Means and stan-dard errors, n=7 rats per group
since there is evidence that IGFBP-1 may have an im-portant role in inhibiting serum IGF-I bioavailability[39]. Particularly when phosphorylated, IGFBP-I has ahigher affinity for IGFs than membrane-bound IGF re-ceptors and the high levels of IGFBP-1 in CRF are nega-tively correlated with both linear growth and GFR. Fur-thermore IGFBP-1 levels normalize after a successful re-nal transplantation (reviewed in ref. [39]). The role ofthe other IGFBPs in children with renal failure is largelyunknown [18].
Novel peptides have now been discovered, usingphage displayed peptide libraries, which show remark-able specificity in that if they bind to IGFBP-1, they willnot bind to IGFBP-3, and vice versa [8]. One peptide, di-rected against IGFBP-1, has a defined NMR structure insolution, and therefore provides a lead to non-peptideIGF displacer mimetics. In the next decade, such non-peptide molecules may be useful as novel therapeutics inrenal failure. Because the problem in renal failure is nota deficiency of IGF-I, but a surfeit of IGFBPs, the dis-placer approach should lead to an improved safety to ef-ficacy profile, compared to treatment with IGF-I. In ad-dition IGF-I is a protein that must be injected; it is possi-ble that non-peptide IGF displacers will be made orallyactive. Research in this area will help discover both thefunction of the IGFBPs and their role in renal failure andother diseases where the IGFBPs are deranged.
Acknowledgements Professor Iain Robinson (MRC, Mill Hill)and Henry Lowman are acknowledged for their help, which en-sured the success of this project. Professor Erik Heineman and Dr.Greg Thomas are acknowledged for reading and commenting onthis manuscript.
References
1. Jones JI, Clemmons DR (1995) Insulin-like growth factors andtheir binding proteins: biological actions. Endocr Rev 16:3–34
2. Daughaday WH (1998) From sulfation factor to IGF-I, 40years of research on the regulation of cartilage growth. In:Takano K, Hizuka N, Takahashi S-I (eds) Molecular mecha-nisms to regulate the activities of insulin-like growth factors.Excerpta Medica, Amsterdam, pp 1–9
3. Flyvbjerg A, Orskov H (1994) Insulin-like growth factors andthe kidney. In: Baxter RC, Gluckman PD, Rosenfeld RG (eds)The insulin-like growth factors and their regulatory proteins.Excerpta Medica, Tokyo, pp 417–425
4. Franklin SC, Moulton M, Sicard GA, Hammerman MR, MillerSB (1997) Insulin-like growth factor I preserves renal functionpostoperatively. Am J Physiol 272:F257–F259
5. Vijayan A, Franklin SC, Behrend T, Hammerman MR, MillerSB (1999) Insulin-like growth factor I improves renal functionin patients with end-stage chronic renal failure. Am J Physiol276:R929–R934
6. Hammerman MR, Miller SB (1997) Effects of growth hor-mone and insulin-like growth factor I on renal growth andfunction. J Pediatr 131:S17–S19
7. Tonshoff B, Blum WF, Mehls O (1997) Derangements of thesomatotropic hormone axis in chronic renal failure. Kidney IntSuppl 58:S106–S113
8. Lowman HB, Chen YM, Skelton NJ, Mortensen DL, TomlinsonEE, Sadick MD, Robinson IC, Clark RG (1998) Molecular mim-ics of insulin-like growth factor 1 (IGF-1) for inhibiting IGF-1:IGF-binding protein interactions. Biochemistry 37:8870–8878
587
I (Fig. 1). To test this hypothesis we used two animalmodels of IGF deficiency, hypophysectomized rats anddwarf (dw/dw) rats. The effect of the administration ofIGF displacers on many parameters, including thegrowth and function of the kidney, were examined [8].
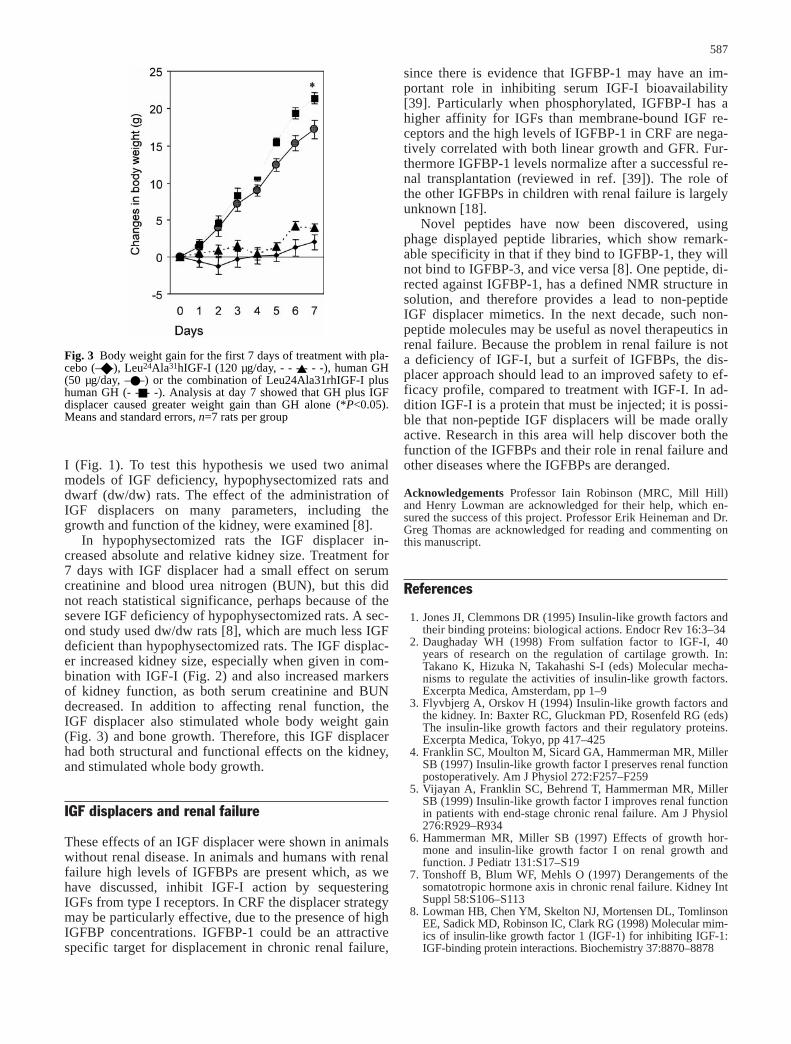
In hypophysectomized rats the IGF displacer in-creased absolute and relative kidney size. Treatment for7 days with IGF displacer had a small effect on serumcreatinine and blood urea nitrogen (BUN), but this didnot reach statistical significance, perhaps because of thesevere IGF deficiency of hypophysectomized rats. A sec-ond study used dw/dw rats [8], which are much less IGFdeficient than hypophysectomized rats. The IGF displac-er increased kidney size, especially when given in com-bination with IGF-I (Fig. 2) and also increased markersof kidney function, as both serum creatinine and BUN decreased. In addition to affecting renal function, the IGF displacer also stimulated whole body weight gain (Fig. 3) and bone growth. Therefore, this IGF displacerhad both structural and functional effects on the kidney,and stimulated whole body growth.
IGF displacers and renal failure
These effects of an IGF displacer were shown in animalswithout renal disease. In animals and humans with renalfailure high levels of IGFBPs are present which, as wehave discussed, inhibit IGF-I action by sequesteringIGFs from type I receptors. In CRF the displacer strategymay be particularly effective, due to the presence of highIGFBP concentrations. IGFBP-1 could be an attractivespecific target for displacement in chronic renal failure,
Fig. 3 Body weight gain for the first 7 days of treatment with pla-cebo (–◆–), Leu24Ala31hIGF-I (120 µg/day, - - -▲- - -), human GH(50 µg/day, –●–) or the combination of Leu24Ala31rhIGF-I plushuman GH (- -■- -). Analysis at day 7 showed that GH plus IGFdisplacer caused greater weight gain than GH alone (*P<0.05).Means and standard errors, n=7 rats per group
24. Rajkumar K, Barro D, Lewitt MS, Murphy LJ (1995) Growthretardation and hyperglycemia in insulin-like growth factorbinding protein-1 transgenic mice. Endocrinology 136:4029–4034
25. Cox GN, McDermott MJ, Merkel E, Stroh CA, Ko SC,Squires CH, Gleason TM, Russell D (1994) Recombinant hu-man insulin-like growth factor (IGF)-binding protein-1 inhib-its somatic growth stimulated by IGF-I and growth hormone inhypophysectomized rats. Endocrinology 135:1913–1920
26. Mortensen DL, Won WB, Siu J, Reifsnyder D, Gironella M,Etcheverry T, Clark RG (1997) Insulin-like growth factorbinding protein-1 induces insulin release in the rat. Endocri-nology 138:2073–2080
27. Matejka GL, Jennische E (1992) IGF-I binding and IGF-ImRNA expression in the post-ischemic regenerating rat kid-ney. Kidney Int 42:1113–1123
28. Miller SB, Martin DR, Kissane J, Hammerman MR (1992) In-sulin-like growth factor I accelerates recovery from ischemicacute tubular necrosis in the rat. Proc Natl Acad Sci USA89:11876–11880
29. Ding H, Kopple JD, Cohen A, Hirschberg R (1993) Recombi-nant human insulin-like growth factor-I accelerates recoveryand reduces catabolism in rats with ischemic acute renal fail-ure. J Clin Invest 91:2281–2287
30. Clark R, Mortensen D, Rabkin R (1994) Recovery from acuteischaemic renal failure is accelerated by des-(1-3)-insulin-likegrowth factor-1. Clin Sci 86:709–714
31. Miller SB, Hansen VA, Hammerman MR (1990) Effects ofgrowth hormone and IGF-I on renal function in rats with nor-mal and reduced renal mass. Am J Physiol 259:F747–F751
32. Hazel SJ, Gillespie CM, Moore RJ, Clark RG, Jureidini KF,Martin AA (1994) Enhanced body growth in uremic rats treat-ed with IGF-I and growth hormone in combination. Kidney Int46:58–68
33. Guler HP, Schmid C, Zapf J, Froesch R (1989) Effects of re-combinant insulin-like growth factor I on insulin secretion andrenal function in normal human subjects. Proc Natl Acad SciUSA 86:2868–2872
34. Hirschberg R, Brunori G, Kopple JD, Guler HP (1993) Effectsof insulin-like growth factor I on renal function in normalmen. Kidney Int 43:387–397
35. Hirschberg R, Adler S (1998) Insulin-like growth factorsystem and the kidney: physiology, pathophysiology, and ther-apeutic implications. Am J Kid Dis 31:901–919
36. O’Shea MH, Miller SB, Hammerman MR (1993) Effects ofIGF-I on renal function in patients with chronic renal failure.Am J Physiol 264:F917–F922
37. Miller SB, Moulton M, O’Shea M, Hammerman MR (1994)Effects of IGF-I on renal function in end-stage chronic renalfailure. Kidney Int 46:201–207
38. Loddick SA, Liu X-J, Lu Z-X, Liu C, Behan DP, ChalmersDC, Foster AC, Vale WW, Ling N, De Souza EB (1998) Dis-placement of insulin-like growth factors from their bindingproteins as a potential treatment for stroke. Proc Natl Acad SciUSA 95:1894–1898
39. Lee PDK, Giudice LC, Conover CA, Powell DR (1997) Insu-lin-like growth factor binding protein-1 – recent findings andnew directions. Proc Soc Exp Biol Med 216:319–357
588
9. Juul A, Flyvbjerg A, Frystyk J, Muller, Skakkebaek NE (1996)Serum concentrations of free and total insulin-like growth fac-tor-I, IGF binding proteins-1 and -3 and IGFBP-3 protease ac-tivity in boys with normal or precocious puberty. Clin Endo-crinol 44:515–523
10. Rabkin R, Fervenza FC, Maidment H, Ike J, Hintz R, Liu,Bloedow DC, Hoffman AR, Gesundheit N (1996) Pharmaco-kinetics of insulin-like growth factor-1 in advanced chronic re-nal failure. Kidney Int 49:1134–1140
11. Kale AS, Liu F, Hintz RL, Baker BK, Brewer ED, Lee PD,Durham SK, Powell DR (1996) Characterization of insulin-like growth factors and their binding proteins in peritoneal di-alysate. Pediatr Nephrol 10:467–473
12. Blat C, Villaudy J, Binoux M (1994) In vivo proteolysis of se-rum insulin-like growth factor (IGF) binding protein-3 resultsin increased availability of IGF to target cells. J Clin Invest93:2286–2290
13. Clemmons DR (1998) Role of insulin-like growth factor bind-ing proteins in controlling IGF actions. Mol Cell Endocrinol140:19–24
14. Feld S, Hirschberg R (1996) Growth hormone, the insulin-likegrowth factor system, and the kidney. Endocr Rev 17:423–480
15. Haffner D, Schaefer F, Girard J, Ritz E, Mehls O (1994) Meta-bolic clearance of recombinant human growth hormone inhealth and chronic renal failure. J Clin Invest 93:1163–1171
16. Tonshoff B, Veldhuis JD, Heinrich U, Mehls O (1995) Decon-volution analysis of spontaneous nocturnal growth hormonesecretion in prepubertal children with preterminal chronic re-nal failure and with end-stage renal disease. Pediatr Res 37:86–93
17. Tonshoff B, Blum WF, Mehls O (1996) Serum insulin-likegrowth factors and their binding proteins in children with end-stage renal disease. Pediatr Nephrol 10:269–274
18. Powell DR, Durham SK, Brewer ED, Frane JW, Watkins SL,Hogg RJ, Mohan S (1999) Effects of chronic renal failure andgrowth hormone on serum levels of insulin-like growth fac-tors-binding protein-4 (IGFBP-4) and IGFBP-5 in children: areport of the Southwest Pediatric Nephrology Study Group. J Clin Endocrinol Metab 84:596–601
19. Baxter RC, Skriver L (1993) Altered ligand specificity ofproteolysed insulin-like growth factor binding protein-3. Bio-chem Biophys Res Commun 196:1267–1273
20. Ike JO, Fervenza FC, Hoffman AR, Yeh I, Hintz RL, Liu F,Rabkin R (1997) Early experience with extended use of insu-lin-like growth factor-1 in advanced chronic renal failure. Kid-ney Int 51:840–849
21. Fouque D, Le Bouc Y, Laville M, Combarnous F, Joly MO,Raton P, Zech P (1995) Insulin-like growth factor-1 and itsbinding proteins during a low-protein diet in chronic renal fail-ure. J Am Soc Nephrol 6:1427–1433
22. Powell DR, Liu F, Baker BK, Lee PD, Hintz RL (1996) Insu-lin-like growth factor binding proteins as growth inhibitors inchildren with chronic renal failure. Pediatr Nephrol 10:343–347
23. Blum WF, Ranke MB, Kietzmann K, Tonshoff B, Mehls O(1991) Growth hormone resistance and inhibition of somato-medin activity by excess of insulin-like growth factor bindingprotein in uraemia. Pediatr Nephrol 5:539–544