integrating behavioral health and primary...
TRANSCRIPT

Integrating Behavioral Health and Primary Care
John H. Porcerelli, PhD, ABPP Department of Family Medicine & Public Health Sciences
Overview
1) Healthcare system & spending 2) Why behavioral health? 3) Patient-Centered Medical Home 4) Integration 5) WSU Training & pilot data 6) Unanswered Qs
2
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
1

Healthcare System
• 44 Million Americans w/out healthcare • Skyrocketing healthcare costs • 75% of healthcare costs – chronic illness • PC in the US is not comprehensive,
coordinated, accessible, or continuous – Fragmented dual health system
3
Spending in US
4
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
2
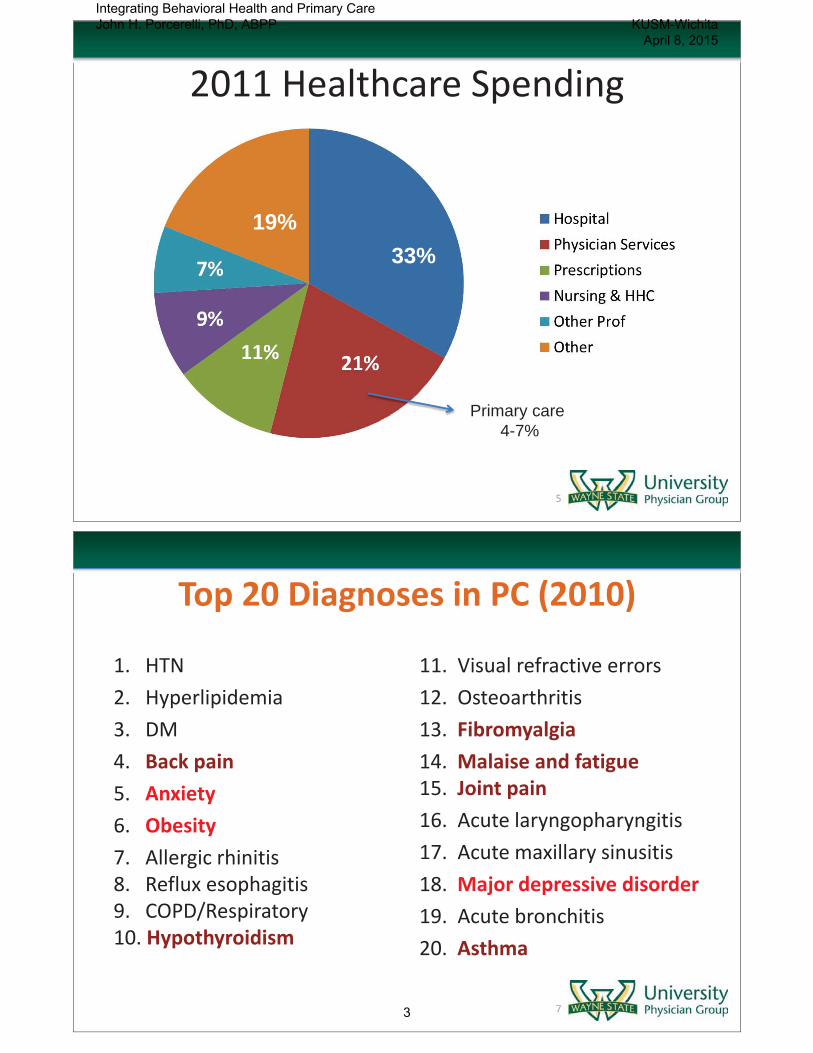
2011 Healthcare Spending
33% 19%
Primary care 4-7%
5
Top 20 Diagnoses in PC (2010)
1. HTN 2. Hyperlipidemia 3. DM 4. Back pain 5. Anxiety 6. Obesity 7. Allergic rhinitis 8. Reflux esophagitis 9. COPD/Respiratory 10. Hypothyroidism
11. Visual refractive errors 12. Osteoarthritis 13. Fibromyalgia 14. Malaise and fatigue 15. Joint pain 16. Acute laryngopharyngitis 17. Acute maxillary sinusitis 18. Major depressive disorder 19. Acute bronchitis 20. Asthma
7
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
3

Why Behavioral Health? • 84% of common physical complaints have no
identifiable organic etiology • 80% of people with behavioral health (BH) disorders
will see a PCP yearly • 50% of BH disorders are treated in PC • 59% of psychiatric prescriptions are written by PCPs • 30-50% of Pts referred by PCPs to BH specialists
don’t follow through • “Is anybody out there???”
• Psychotherapy : the least frequently used intervention for depression in PC
8
Why Behavioral Health? • Saves lives: When primary care practices used a care manager (MSW,
RN, or ψ) to help treat depression in older adults, Pts were 24% less likely to die compared with TAU (BMJ, 2013).
• Compliance: 20% Pts with DM2 and CVD suffer from depression. – They’re less likely to make lifestyle changes and adhere to medication regimens
(Arch Gen Psych, 2013).
• Medical $: Depression increases medical $ by 50-70%. When nurse
care managers monitored Pts with depression and DM2 or CVD – Pts had lower mean outpatient costs of $594 per person – 114 more depression-free days compared with Pts who received usual care (Arch
Gen Psych).
• Including mental health services in primary care practices may even reduce physician burnout.
9
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
4

Healthcare System
• Affordable Care Act (2010)
1. Better health of the population 2. Better patient care (quality, access, reliability)
3. Reduce costs
10
Patient Centered Medical Home
11
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
5

Evidence for the Effectiveness of PCMH
• PCMH Pilot (JAMA; 2008-2011) • 32 practices in Penn/29 comparison practices • No cost or utilization reductions
• PCMH Impact on Cost & Quality (PC-PCC; 2013-2014)
• Peer-reviewed journals (N=14) • State program evaluations (N=7) • Industry publication (N=7)
12
New Evidence
• Peer-reviewed: • 6/10 reductions in cost • 12/13 reductions in at least 1 utilization measure
• State reports (non peer-reviewed) • 7/7 reductions in cost • 6/7 at least one utilization measure
• Industry (non peer-reviewed) • 4/7 reductions in cost • 6/7 at least one utilization measure
13
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
6
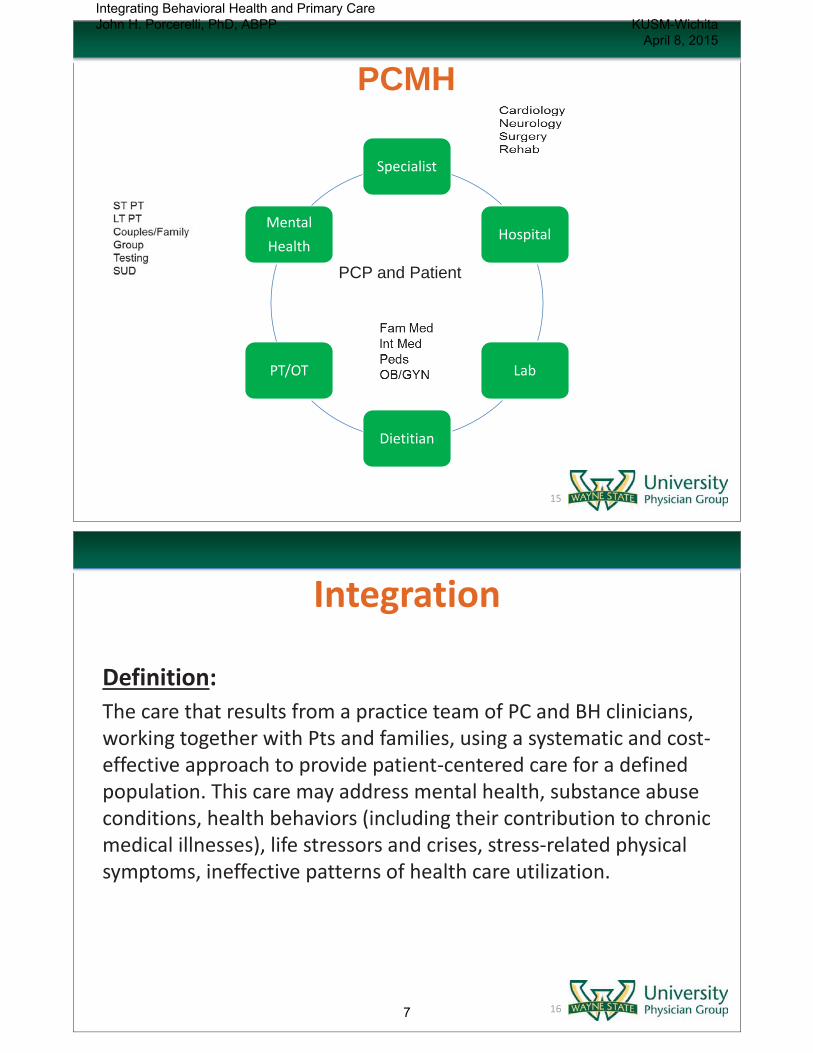
Specialist
Hospital
Lab
Dietitian
PT/OT
Mental Health
PCP and Patient
PCMH
15
Integration Definition: The care that results from a practice team of PC and BH clinicians, working together with Pts and families, using a systematic and cost-effective approach to provide patient-centered care for a defined population. This care may address mental health, substance abuse conditions, health behaviors (including their contribution to chronic medical illnesses), life stressors and crises, stress-related physical symptoms, ineffective patterns of health care utilization.
16
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
7

Agency for Healthcare Research & Quality (AHRQ)
• Elements of integrate behavioral health – Mental health care – Substance abuse care – Health behavior change – Life stressors and crises – Stress-related physical symptoms – Ineffective patterns of healthcare utilization – Teaching “bio-psycho-social” model
17
Inter-professional Training -Practicum/Internship-
Primary Care Health Psychology
UMass – PC Postdoc
MSU – PC Postdoc
18
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
8

WSU – Family Medicine • IJPM 2013
• Clinic huddle • Shadowing • Pull-ins, warm hand-offs • Co-counseling • Shared precepting • Feedback to PCPs (assessment, intervention) • Lectures • Video-observation & feedback • Home visits • Research
19
What Happens? Doctoral students & Family Medicine Residents
Family Medicine (2013)
Assessment Behavioral Intervention
Lifestyle Chronic Dis
Management Freq % Freq % Freq %
PCP 148/550 27 39/550 7 78/550 15
Psych 65/550 12 39/550 7 28/550 5
Both 227/550 41 80/550 15 61/550 11
Total 440/550 80 158/550 29 167/550 31
20
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
9

Education Extras!
Psychosocial Case
Conceptualization
Communication
Advice
Emotional Debriefing
Positive
Feedback
Medication Consultation/
Discussion
175/347
10/347
34/347
50/347
63/347
50% 3% 10% 14% 18%
Encounters (N = 347)
21
Unanswered Question
• Is behavioral health integration necessary? • Is it cost-effective?
– Artificial vs. real integration
• Reimbursement for behavioral health? • PC Health Professions Workforce
• Primary Care Health psychology (APA, ABPP)
• Social work (NASW: health, alc/tobacco/other)
• Nursing (NP – primary care)
22
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
10
Collaborative Practice • Interprofessional Collaborative Practice
• American Association of Colleges of Nursing • American Association of Colleges of Osteopathic Med • American Association of Colleges of Pharmacy • American Dental Education Association • Association of American Medical Colleges • Association of Schools of Public Health
23
Collaborative Practice
“Collaborative practice is the key to safe, high quality, accessible, patient-centered care.” Goal: To prepare all health professions students for deliberately working together with the common goal of building a safer and better patient-centered and community/population oriented U.S. healthcare system How care is delivered is as important as what care is delivered
24
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
11

ACGME (2011)
Multispecialty resident survey: Formal team training experiences with non-physicians is significantly related to greater resident satisfaction with learning and training experiences, less depression, anxiety, and sleep problems, and fewer serious medical errors
25
Core Competencies 1) Values/ethics for interprofessional practice
Respect the dignity and privacy of Pts while maintaining confidentiality in the delivery of team-based care
2) Roles/responsibilities Explain the roles and responsibilities of other care providers and how the team works together to provide care
3) Interprofessional communication Communicate consistently the importance of teamwork in patient-centered and community-focused care
4) Teams and teamwork Engage other health professionals – appropriate to specific care situations – in shared patient-centered problem solving
26
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
12

Key Areas Key areas integral to the future development of enhanced
primary care and the PCMH:
• Integrating services both inside and outside primary care practices. Examples include integrating behavioral and oral health into PCMHs and integrating PCMHs into Accountable Care Organizations (ACO) and various community based organizations and services;
• Providing financial support for enhanced primary care that helps control the total cost of care while maintaining or improving quality for patients;
• Developing the primary care health professions workforce to embrace all members of the team, including the patient and their family/caregiver;
• Engaging patients, consumers, and the public particularly in PCMH transformation and quality improvement activity; and
• Embracing the potential of technology to support this model of care.
27
Example 1: Routine Visit
• Presenting problems: “Just not feeling well”
Mrs B: age 49, BMI 42, HTN (145/95), DM2 (HA1c=9.2) • PCP: Inquired about changes in health over the last 4 months? • BH: Any life changes around that same time? • Pt: 74 yr-old mother living with her after stroke. • BH: PHQ-4=4 (depression/anxiety more than ½ the days); worsened in the last
month (“Mother is more demanding and will only use a cane vs. walker”) – Brief discussion of ambivalence & self-time / relaxation hand-out
• PCP: (1) reviewed meds, (2) referral specialist for home healthcare for mother, (3) BH assessment at follow-up
28
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
13

Example 2: ER Follow-up • Presenting problems: ER “Heart attack”
Mr A: age 27, single, truck driver • PCP: Woke up at 3am with palpitations, feared heart attack, ER • BH: Night before? Didn’t sleep well the night before; drank & got high with
new girl friend, hadn’t smoked pot since high school, “got a little paranoid” • PCP: Physical exam – normal; no Hx psych or sub abuse; + family Hx • BH: (Educ) The combination of sleep deprivation, alcohol/marijuana increased
his anxiety, interfered with sleep, and resulted in panic : Education about panic; hand-out; info about BH services • PCP: Follow-up
29
Example 3: ADHD? • Presenting problems:
Male: 22 yr old college senior – Needs Adderall for studying
• PCP: No Hx of ADHD or LD in elementary, middle or HS
• Pt: “Did so much better this semester using it to study”
• BH: GPA? (Pt: 3.4) Sleep hygiene? (Pt: terrible)
• PCP: Needs a full evaluation before he’ll prescribe medication
30
Integrating Behavioral Health and Primary Care John H. Porcerelli, PhD, ABPP KUSM-Wichita
April 8, 2015
14