integumentary system disease: part 1 · integumentary system disease: part i o principles and...
TRANSCRIPT

© Endeavour College of Natural Health endeavour.edu.au 1
NMDC221 Session 22:
Integumentary System Disease
Part I

© Endeavour College of Natural Health endeavour.edu.au 2
Topic Summary
Integumentary System Disease: Part I
o Principles and considerations in nutritional medicine
management of the integumentary system
o Review anatomy & physiology of the integumentary
system
Nutritional management & consideration of drug-nutrient
interactions for:
o Eczema & Dermatitis

© Endeavour College of Natural Health endeavour.edu.au 3
Integumentary System

© Endeavour College of Natural Health endeavour.edu.au 4
Integumentary System
o The integument (skin) is the largest organ of the body
when including its epidermal structures (nails, hair) it
constitutes the integumentary system
o It accommodates for protective and metabolic functions
in certain areas of the body
o Assists in homeostasis
(Tortora & Derrickson, 2009,p.170; Davidson & Haslett
2002,p.878)

© Endeavour College of Natural Health endeavour.edu.au 5
Integumentary System
Functions
o Protects the body from disease and personal injury
o Regulation of Body Fluids and Temperature
o Cutaneous Absorption
o Synthesis
o Sensory Reception
o Communication
o Vitamin D synthesis
(Tortora & Derrickson, 2009,p.170; Davidson & Haslett
2002,p.878)

© Endeavour College of Natural Health endeavour.edu.au 6
Nutrient Dosage Therapeutic Actions
Vitamin A
Beta-carotene
5,000-
10,000iu (up
to 20,000iu)
15-30mg
Antioxidant, photo-protective agent, immuno-
protective agent. Required for appropriate cell
differentiation, growth and development of epithelium
and keratin formation
Vitamin B1
Vitamin B3
Vitamin B5
Vitamin B6
50-200mg
100-200mg
50-500mg
50-200mg
Deficiency presents with skin lesions
Deficiency presents with skin peeling
Cofactor of CoA, aids wound healing
Alters PG species lines
Vitamin C 500-5000mg Combined with iron hydroxylate lysine and proline in
collagen formation. Antioxidant.
Vitamin E 100-1000iu Stabilize cell membranes, inhibits lipid peroxidation,
anti-inflammatory (LOX)
Nutrients for the Integumentary System
(Osiecki 7thed,p.3; Kohlmeier,2003,p.465; Mahan & Escott-Stump,2012,p.59)

© Endeavour College of Natural Health endeavour.edu.au 7
Integumentary System
Nutrient Dosage Therapeutic Actions
Lysine
Proline
Cysteine
500-3,000mg
500-2,000mg
200-500mg
Main structural amino acid components of collagen and
elastin
Biotin 0.5-15mg Combined with CoA is involved in the synthesis of amino
acids
Omega 3 1,000-5,000mg Deficiency presents in scaling and loss of cell
membrane integrity resulting in water loss. Anti-
inflammatory action
Copper 2-5mg Nutrient
Iron 15-80mg Combined with ascorbic acid hydroxylate lysine and
proline in collagen formation. Supports immune system
function.
(Osiecki 7thed,p.103,109; Kohlmeier,2003,p.350,356,404; Schlenker & Long, 2007;
Braun & Cohen,2010,p.677; Mahan & Escott-Stump,2012,p.41)

© Endeavour College of Natural Health endeavour.edu.au 8
Integumentary System
Nutrient Dosage Therapeutic Actions
Manganese 2-20mg Required for the activation of prolidase, stimulating the
utilization of proline, for collagen formation in human skin
cells.
Silica 20-30mg Deficient states present with reduced formation of collagen
and poor wound healing. Aid in eosinophil formation
Zinc 20-
100mg
Required for utilization of EFAs, inhibit lipid peroxidation,
immune system modulation, high concentrations present in
the epidermis.
(Osiecki 7thed,p.161; Muszyska et al. 2001; Seaborn & Nielsen, 2002; Mahan & Escott-
Stump,2012,p.111)

© Endeavour College of Natural Health endeavour.edu.au 9
Integumentary System
Vitamin C
o Vitamin C stimulates collagen synthesis and increases
healing (500-1000mg) with rapid use at wound sites.
o Oral vitamin C reduces lipid peroxidation and quashing
reactive oxygen species.
o Topical vitamin C protects from photo-oxidation
(Coulston, 2001)

© Endeavour College of Natural Health endeavour.edu.au 10
Integumentary SystemVitamin C
NF-kB plus AP-1 ratio play a key role in determining cell
survival or death after oxidative stress
UV-A irradiated cells respond to oxidative stress by
enhancing NF-kB binding activity.
Vitamin C exerts positive modulatory effects by
synergistically enhancing NF-kB activation in irradiated
keratinocytes
The ability of keratinocytes to accumulate Vitamin C can
prevent two effects of UV-B exposure:
o The increase of peroxide levels
o The induction of cell death
(Catani et al, 2005)

© Endeavour College of Natural Health endeavour.edu.au 11
Integumentary System
o “Human keratinocytes possess efficient systems to
maintain intracellular high levels of Vitamin C.
Keratinocytes transport inside the cytoplasm both the
reduced and oxidised form of Vitamin C and recycle the
reduced form through specific enzymatic systems. The
efficiency of systems involved in Vitamin C maintenance
is crucial to ameliorate the intracellular antioxidant state
in the skin” (Catani et al, 2005)

© Endeavour College of Natural Health endeavour.edu.au 12
The role of Vitamin C in keratinocytes to
counteract oxidative stress
1. Act directly by scavenging ROS generated by several
stresses
2. Prevent ROS mediated cell damage by modulating
gene expression
3. Regulate the commitment to keratinocytes
differentiation maintaining a balanced redox state
4. Promote cell cycle arrest and apoptosis in response to
DNA damage
(Catani et al, 2005)

© Endeavour College of Natural Health endeavour.edu.au 13
Integumentary System
Digestive Tract Dysfunction
o Research suggests a link between low stomach acid and
skin conditions with hypochlorhydria occurring in up to
87% of acne rosacea and 74% of eczema cases.
(Osiecki 2004,p.637)
o In vivo research found an inverse relationship between
low CYP2C activity, an isozyme of hepatic cytochrome
P450, and psoriasis. (Helsby et al. 1998)
o Phase II detoxification also plays a role in deactivating
allergen metabolites and increasing their excretion.
(Lutz et al. 2001)

© Endeavour College of Natural Health endeavour.edu.au 14
Eczema & Dermatitis

© Endeavour College of Natural Health endeavour.edu.au 15
Eczema / Dermatitis
Dermatitis is defined as inflammation of the dermal layer.
Eczema is derived from the Greek word meaning ‘boiling’.
This refers to the presentation of inflammation and weeping
of the skin.
These words are used interchangeably.
Dermatitis can be classified into;
o Eczematous (eczema)
o Non-eczematous (contact).
An assigned prefix denotes the perceived cause.
(Bennett, 1999; Kumar & Clark,2009,p.1282)

© Endeavour College of Natural Health endeavour.edu.au 16
Eczema / Dermatitis
Eczema / Dermatitis is characterized by;
o Redness, heat and inflammation.
o Pruritis with potential excoriation. Chronic scratching
leads to secondary thickening of the skin (lichenification).
o Oedema in the acute stages which separates the
keratinocyte (spongiosis) producing intradermal vesicles.
o Oozing with / without vesicles. Initially there may be
crusting followed by scaling & fissuring in chronic stages.
o Increased potential for secondary infection.
(Kumar & Clark 2009,p.1282)

© Endeavour College of Natural Health endeavour.edu.au 17
Eczema/Dermatitis
Presentation With Age
o Infantile Eczema: erythema, weeping or scaling around
the mouth & cheeks when the infant is a few months old
o Flexural / childhood eczema: facial eczema may persist
with presentation in skin folds of toddlers & older
children. Climatic factors exacerbate (sunlight, low
humidity).
o Adult eczema: continuation into adult life may involve the
flexures at the neck, elbow, wrist, ankle or knee and
possibly the limbs. Chronic eczematous changes are
common on the face, though any site may be involved.
(Kumar & Clark, 2009,p.1282)

© Endeavour College of Natural Health endeavour.edu.au 18
Eczema/Dermatitis
Atopic Endogenous Eczema
o Atopy is a predisposition to form allergen induced Th2
characterized by raised levels of IL-4 and IgE. This leads
to a generalized and prolonged hypersensitivity.
o Atopic individuals manifest one or more of a group of
diseases that includes asthma, hay fever, Urticaria, food
& other allergies, and eczema
o These atopic conditions tend to run true to type within
each family.
(Davidson & Haslett 2002)

© Endeavour College of Natural Health endeavour.edu.au 19
Eczema/Dermatitis
o Atopic eczema is an intrinsic hyper-reactivity to common
environmental factors, genetic predispositions or even a
potential for defective skin barrier function.
(Leung et al. 2004)
o May be caused by CD4-type T Helper 2 cells infiltrating
the skin and producing certain cytokines: IL-2 & IL-4 and
Interferon-gamma. Serum levels of IgE are raised.
(Kumar & Clark, 2009,p.1283; Ahuja, Land & Barnes 2003)

© Endeavour College of Natural Health endeavour.edu.au 20
Eczema/Dermatitis
o Reduced hypothalamic-pituitary-adrenal (HPA) axis
responsiveness has been found to present.
(Buske-Kirschbaum & Hellhammer 2003).
o Psychological stress increases eosinophils, while
reducing cortisol levels in atopic eczema patients,
compared to healthy controls. (Raap et al. 2003)
o Research has examined the role of food allergy, e.g.
cow's milk and hen's eggs, and inhaled allergens.
(Werfel & Breuer 2004).

© Endeavour College of Natural Health endeavour.edu.au 21
Eczema/Dermatitis
Atopic Eczema is characterized by the presentation of itchy
skin and at least 3 of the following:
o History of itch in skin creases (or cheeks if < 4 years)
o History of asthma/hay fever (or in first degree relative if <
4years). Atopy presenting in one or both parents
predisposes the infant to a greater chance of
presentation (20-50%)
o Dry skin (xeroderma)
o Visible flexural eczema (cheeks, forehead, outer limbs if
<4 years)
o Onset in first 2 years of life.
(Davidson & Haslett 2002)

© Endeavour College of Natural Health endeavour.edu.au 22
Eczema/Dermatitis
Vitamin C & Vitamin E
o A study found a small positive association between
maternal vitamin C intake during pregnancy and atopic
eczema in the 2nd year of life
o The same study found that maternal vitamin E intake
was negatively associated with eczema in the second
year
(Sheelagh et al, 2005)

© Endeavour College of Natural Health endeavour.edu.au 23
Eczema/DermatitisMaternal Diet
o A maternal diet during pregancy that had healthy
amounts of green and yellow vegetables, citrus fruit, and
β-carotene this may afford some protection against the
development of eczema in the infant.
o Conversely excessively high intakes of n-6 PUFA,
especially linoleic acid, during pregnancy may increase
the risk of childhood eczema
o Maternal intake of vitamin E, α-linolenic acid and
docosahexaenoic acid intake during pregnancy reduced
the chances of the development of infantile wheeze.
(Miyake et al. 2009, 820; Miyake et al. 2010, pp. 758, 764)

© Endeavour College of Natural Health endeavour.edu.au 24
Eczema/Dermatitis
Fish
o “Children's consumption of fish during the first year of life
was more important than maternal consumption of fish
during pregnancy in preventing eczema at 2 years of
age.”
(Øien et al. 2010, p.124)
Food Intolerance Triggers
o Kojima et al. 2003 found that “T-cells, especially those
expressing CLA, play an important role in food-induced
atopic eczema…hen’s egg is the most common cause of
food-related AD in early childhood” (p. 537)

© Endeavour College of Natural Health endeavour.edu.au 25
Eczema/Dermatitis
Food Additives and sensitives:-
Low Histamine Diet
o Removal of histamine foods from the diet Atopic eczema
(AE) patients led to a regeneration of the diaminoxidase-
producing jejunal enterocytes and therefore an increase
of enzyme activity.
o After two weeks on a histamine-free diet, participants
were challenged with histamine rich food.
o The participants “…reported an aggravation of eczema
as well as development of systemic reactions like flush,
headache, or dizziness…” (Maintz et al, 2006, p. 1110).
© Endeavour College of Natural Health endeavour.edu.au 26
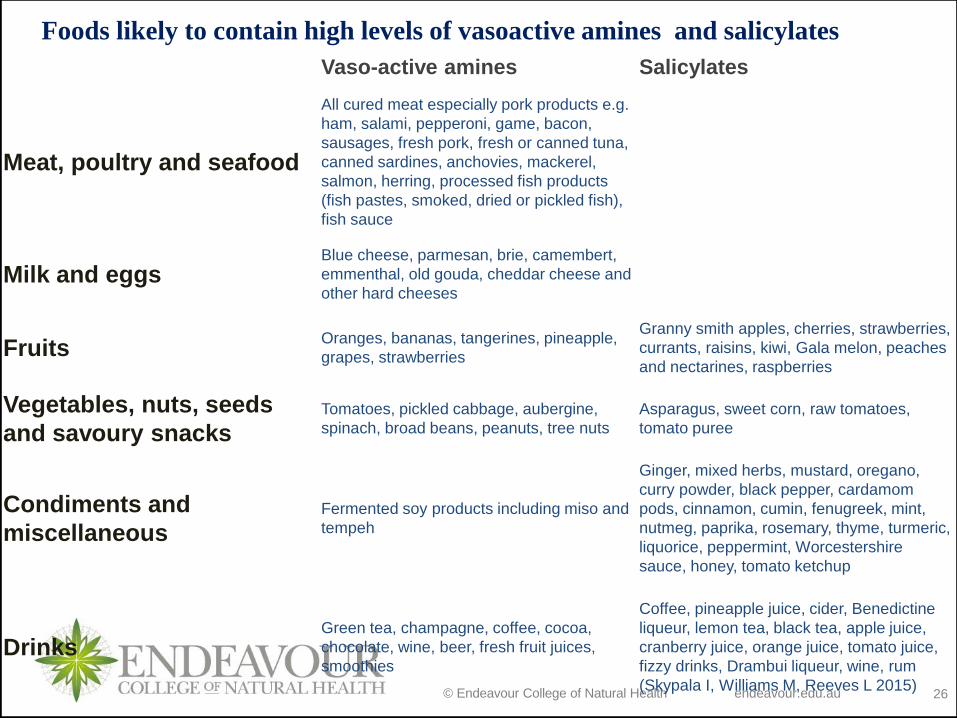
Vaso-active amines Salicylates
Meat, poultry and seafood
All cured meat especially pork products e.g.
ham, salami, pepperoni, game, bacon,
sausages, fresh pork, fresh or canned tuna,
canned sardines, anchovies, mackerel,
salmon, herring, processed fish products
(fish pastes, smoked, dried or pickled fish),
fish sauce
Milk and eggsBlue cheese, parmesan, brie, camembert,
emmenthal, old gouda, cheddar cheese and
other hard cheeses
FruitsOranges, bananas, tangerines, pineapple,
grapes, strawberries
Granny smith apples, cherries, strawberries,
currants, raisins, kiwi, Gala melon, peaches
and nectarines, raspberries
Vegetables, nuts, seeds
and savoury snacksTomatoes, pickled cabbage, aubergine,
spinach, broad beans, peanuts, tree nuts
Asparagus, sweet corn, raw tomatoes,
tomato puree
Condiments and
miscellaneousFermented soy products including miso and
tempeh
Ginger, mixed herbs, mustard, oregano,
curry powder, black pepper, cardamom
pods, cinnamon, cumin, fenugreek, mint,
nutmeg, paprika, rosemary, thyme, turmeric,
liquorice, peppermint, Worcestershire
sauce, honey, tomato ketchup
DrinksGreen tea, champagne, coffee, cocoa,
chocolate, wine, beer, fresh fruit juices,
smoothies
Coffee, pineapple juice, cider, Benedictine
liqueur, lemon tea, black tea, apple juice,
cranberry juice, orange juice, tomato juice,
fizzy drinks, Drambui liqueur, wine, rum
(Skypala I, Williams M, Reeves L 2015)
Foods likely to contain high levels of vasoactive amines and salicylates

© Endeavour College of Natural Health endeavour.edu.au 27
Eczema/Dermatitis
Discord/Nummular Eczema
o Presentation of irritant vesicles, demarcated scaly
patches that form plaques.
o Commonly affects the sides of the fingers, palms, the
toes or soles of the feet.
o Common in adults
o May be atopic/ non-atopic
o Staphyloccocus aureus infection commonly presents.
(Kumar & Clark,2009,p.1285)

© Endeavour College of Natural Health endeavour.edu.au 28
Eczema/Dermatitis
Seborrheic Eczema
o This condition is characterized by a red scaly rash and
inflammation (with little itch present).
o Overgrowths of Pityrosporum ovale yeast produces
inflammation and scaling in areas that are rich in
sebaceous glands. These include the scalp (dandruff),
central face, naso-labial folds, eyebrows and central
chest.
o An infantile form presents as ‘cradle cap.’ This may also
present on the torso and around the nappy area.
(Kumar & Clark,2009,p.1262; Davidson & Haslett, 2002)

© Endeavour College of Natural Health endeavour.edu.au 29
Seborrhoeic eczema
Seborrheic eczema, viewed 23rd Oct 2007
http://health.yahoo.com/media/mayoclinic/images/image_popup/ans
7_seb_dermatitis.jpg

© Endeavour College of Natural Health endeavour.edu.au 30
Eczema / Dermatitis Exogenous Eczema
Localized or unusual eczema presentation.
This may occur through;
o Direct irritation
o Allergic reaction (type IV hypersensitivity reaction)
Usually no personal or familial history of atopic disease.
( Kumar & Clark,2009,p.1286)

© Endeavour College of Natural Health endeavour.edu.au 31
Eczema / Dermatitis
Allergic contact
o Occurs through exposure to an irritant / chemical that
stimulates a cell mediated allergic immune reaction.
o T – lymphocytes are sensitized to the antigen some time
after the first contact. Langerhans cells in the dermis of
the skin present the Ag to T – lymphocytes. Sensitivity to
the antigen lasts for life. Second exposure stimulates a
magnified reaction.
(Kumar & Clark,2009,p.1286)

© Endeavour College of Natural Health endeavour.edu.au 32
Eczema / Dermatitis
Characteristics include;
o Intense pruritus (excoriation with scratching),
inflammation, heat, swelling.
o Pattern and distribution are suggestive of direct contact.
Ongoing irritation can see the symptoms spread.
Common irritants in allergic contact dermatitis include;
o Nickel (jewellery), Chromate (cement), Latex, Perfume,
Specific species of plants
(McKoy, 2009)

© Endeavour College of Natural Health endeavour.edu.au 33
Eczema/ Dermatitis
Irritant contact
o Non-specific inflammatory reaction that occurs after
repeated exposure to an irritant. There is no immune
system activation.
Characteristics include;
o Pain and inflammation with mild pruritus.
o There may be mild erythema to haemorrhage, crusting,
erosion, pustules, bullae, and oedema.
Common irritants include;
o Chemicals, soaps, plants, body fluid.
(McKoy, 2009)

© Endeavour College of Natural Health endeavour.edu.au 34
Eczema/ Dermatitis
Investigations
o Presentation of an unusual pattern of rash with clear-cut
demarcation or odd- shaped areas of erythema &
scaling.
o Exploration of history especially environmental changes
and the timing of those changes may indicate a cause.
o Skin patch test: back is most commonly used. Tested
substance is left on for 24 hours, removed & underlying
skin is examined.
o Causative agent may not be clearly defined.
(Kumar & Clark,2009,p1286; McKoy, 2009)

© Endeavour College of Natural Health endeavour.edu.au 35
Eczema/Dermatitis
Drug Risk Factors: Paracetamol
o Studies found that eczema rates were higher than
normal in 6-7 year olds that had no previous medical
history of asthma or rhino-conjunctivitis that had
paracetamol in their first year of life. This was thought to
reduce glutathione levels.
o Lowered glutathione is linked to chronic inflammation.
The healthy skin of eczema patients commonly presents
with chronic inflammatory markers = increased
cutaneous antioxidant defense levels
o Low glutathione favours a Th2 allergic pathway when an
allergen presents that sustains this reaction.
(Garcia-Marcos et al. 2010, p. 1040).

© Endeavour College of Natural Health endeavour.edu.au 36
Eczema/Dermatitis
Drug Risk Factors: Antibiotics
o Antibiotics taken in the first year of life is associated with
eczema presentation in 6-7 year old children with no
prior history of asthma or rhino-conjunctivitis.
(Garcia-Marcos et al. 2010, p. 1040)
o Children that had been in contact with antibiotics by 6
months old presented more frequently with flexural
eczema (Callard et al. 2002, p. 991)
o The “hygiene hypothesis” put forward for this is that gut
flora disruption causes an imbalance in Th1/Th2 and a
subsequent Th2 dominance
(Garcia-Marcos et al. 2010, p. 1040)

© Endeavour College of Natural Health endeavour.edu.au 37
Eczema/Dermatitis
Treatment Aims
o Identify & remove risk factors and triggers (allergens,
environment)
o Reduce inflammation in the skin
o Improve hydrochloric acid secretion
o Balance gut microbiome status
o Rebalance and regulate blood sugar levels
o Minimizing over heating of the skin
o Wearing cotton clothes
o Maintain hydration and moisture of the skin
(Stollery, 2007; Kumar & Clark,2009,p.1286; Sarris &
Wardle,2010,p.479)

© Endeavour College of Natural Health endeavour.edu.au 38
Eczema/Dermatitis
Nutrient Dosage Therapeutic Actions
Glutathione
Cysteine
Glutamine
Glycine
100-500mg
200-500mg
500-3000mg
4-30gm
Glutathione is able to stop the production of
cytokines when they are being produced in the
excessive amounts. Assists within liver phase 1
and 2 detoxification pathways.
Alpha
Linolenic Acid
(Omega 3)
1000-6000mg Alpha-Linolenic Acid (LNA) suppresses the
inflammatory response. This is due to its action on
enhancing PGE 3 response thereby down
regulating PGE 2 production. High PGE2 stimulate
mast cell hyper-excitability
Vitamin E 100-1000iu Due to its action as an antioxidant of lipid
peroxides or alternatively in diminishing PGE 2
activity.
(Coulston 2003; Jamison 2003; Pizzorno & Murray 2006,p.1093; Sarris & Wardle,2010,p.545)

© Endeavour College of Natural Health endeavour.edu.au 39
Eczema/Dermatitis
Nutrient Dosage Therapeutic Actions
Vitamin A 5000-10000iu Antioxidant, deficiency presents with increases in
the severity of atopic eczema.
Vitamin C 500-5,000mg Antioxidant, Collagen repair, stabilizing mast cell
hyper-excitability
Zinc 10-100mg Collagen Repair, enhances antioxidant activity
rebalances Th2 dominance
Lysine 300-3000mg Collagen Repair
Proline 500-1000mg Collagen Repair
Lactobacillus
rhamnosus
10-40 Billion Maternally from 36 weeks to post natal for 2 years
is linked to reduced presentation of atopy in
genetically predisposed individuals
(Wickens et al. 2008; Gropper et al. 2009,p.488; Sarris &Wardle, 2010,p.474)

© Endeavour College of Natural Health endeavour.edu.au 40
Eczema/Dermatitis
Drug Action Side Effects Interaction
Topical
Corticosteroids:
hydrocortisone,
methyl-
prednisolone,
betamethasone.
Anti-
inflammatory,
antipruritic,
immuno-
suppressant
action.
Skin atrophy, striae,
burning, dryness,
itching, loss of
pigmentation,
hirsutism, folliculitis.
Proportion is
systemically
absorbed
(dependent on the
size of area and the
frequency of
application) which
may result cortisol
excess symptoms.
Aloe vera: beneficial in
combination.
Green tea: concurrent
consumption has
presented with significant
skin lesion healing
Zinc & Biotin:
Co-administration of oral
doses have seen
reduced requirements for
topical applications of
corticosteroids.
(Stargrove et al, 2008,p.635; Bryant & Knight,2011,p.862)

© Endeavour College of Natural Health endeavour.edu.au 41
Eczema/Dermatitis
Drug Action Side Effects Interaction
Vitamin A
Analogue:
Alitretinoin
Topical retinoid
that binds to and
then stimulates
intracellular
retinoid
receptors. Anti-
inflammatory
and immuno-
modulatory
effects.
Skin irritation
– burning,
itching & heat.
Alitretinoin
CYP3A4 Inhibitors
Alitretinoin is metabolised by
cytochrome P450 3A4, so CYP3A4
inhibitors (grapefruit juice) can raise
plasma levels of alitretinoin.
Vitamin A
Patients should not take vitamin A
supplements or other retinoids while
being treated with alitretinoin, to avoid
the risk of hypervitaminosis A.
(Kumar & Clark, 2009)

© Endeavour College of Natural Health endeavour.edu.au 42
Eczema/Dermatitis
Drug Action Side Effects Interactions
Rituximab Antibody that destroys B
cells that have a specific
protein (CD20) on their
surfaces. Utilized in
conditions with overactive
or malfunctioning B cells.
Up to half of clients
experience fever.
Less commonly chills,
headache and
abdominal pain.
Severe side effects of
alterations of blood
levels of neutrophils,
white blood cells and
red blood cells.
None listed
(Hosli et al. 2008, p. 126)

© Endeavour College of Natural Health endeavour.edu.au 43
Eczema/Dermatitis
Other Topical Preparations
o Oatmeal baths to reduce itching
o Bath oils/ soap substitutes
o Emollients – changes in skin moisture reduces the
barrier function and allowing triggers and allergens to
penetrate the skin. Dry skin can increase itching which in
turn creates physical damage. Can potentially reduce the
requirement for corticosteroids
o Emollients can be used as soap alternatives.
o Occlusive treatment can be used if the site is wet,
exuding or inflamed. (Bennett, 1999)

© Endeavour College of Natural Health endeavour.edu.au 44
Class Discussion
6 year old boy
Presenting symptoms
o Eczema present in the creases of the elbows, knees,
ankles and webbing of the fingers. Eczema presents as
red, dry, slightly raised and weeping in the folds.
o It is very itchy and the child has been scratching it. He says
that it is far worse after a bath and in bed.
o Initially presented at 6 months old – the eczema was milder
and presented as a diffuse dry rash
o Was contained with steroid cream and oil additive in the
bathwater.
o Has flared up recently. Boy has started at a new school.

© Endeavour College of Natural Health endeavour.edu.au 45
Discussion
Medications / Supplements
o Hydrocortisone cream 1%
o Ego QV bath oil – fragrance free
Family History
o Mother: eczema, asthma as a child
o Father: eczema, nervous disposition
Past Medical History
o Infant: Natural birth, breastfed until 15 months old. Food
was introduced at 5 months. Fully vaccinated.

© Endeavour College of Natural Health endeavour.edu.au 46
Discussion
System Presentation
o Immune: Ran a high fever (39.5ºC) when he was 5.5
months old. It lasted for 6 hours. Was given Panadol &
the fever improved. There was no skin rash or URTI
symptoms.
o Has had a cold 4-5 times. Gets over them quickly, within
2-3 days. Only runny noses.
o GIT: craves fresh fruit: strawberries, oranges, rock
melon. Also craves dried fruits: dates, sultanas, figs.
Eats a varied diet.

© Endeavour College of Natural Health endeavour.edu.au 47
Discussion
Physical Examination Results
o Nails: pink, good capillary return, all fingers have moons,
white spots present on 2 fingers, soft, peel easily
o Skin: elbows & heels dry
o Tongue: pale & flabby, white coat, central crack, quiver
o Appearance: slim build, slightly agitated and fidgety
o Height: 98cm Weight: 20.5kg

© Endeavour College of Natural Health endeavour.edu.au 48
Discussion
Time Daily Dietary Intake
7am Muesli topped with fresh banana & yoghurt (pot set). Milk added.
10am Box sultanas
Rice crackers – cheese flavoured
12.30pm Vegetable pastie & tomato sauce
Apple
Orange juice
3.15pm Cheese & tomato sandwich (multigrain)
6pm Beef lasagne: beef, tomato, onion, mushroom, zucchini
Water: 500ml

© Endeavour College of Natural Health endeavour.edu.au 49
Group Discussion
o Cover the development of complementary diagnosis and
formulation of goals, application of goals to specific
actions, identifying the nutrients related to each action,
and developing a nutritional prescription.
o Consider individual nutrient dosage with clinical
decisions, integrative management of each condition
giving mechanisms of actions relevant for nutrient-drug
interactions.
o Discuss findings in the class with critical discussion.

© Endeavour College of Natural Health endeavour.edu.au 50
References
o Ahuja A, Land K, & Barnes CJ 2003, ‘Atopic dermatitis.’ South medical
journal, Vol. 96, No. 11, pp. 1068-1072 Viewed 23/03/11:
http://www.ncbi.nlm.nih.gov/pubmed/14632353
o Alan, C & Clemetson, B 1980, ‘Histamine and ascorbic acid in human
blood.’ The Journal of nutrition, Vol. 110, No. 4, pp. 662-668. Viewed
23/03/11: http://jn.nutrition.org/content/110/4/662.full.pdf+html
o Bennett, A 1999, Managing eczema and dermatitis.’ Nursing standard. Vol.
13. no. 42, pp. 67-72. Viewed 23/03/11:
http://proquest.umi.com.ezp01.library.qut.edu.au/pqdweb?index=0&did=436
50911&SrchMode=1&sid=1&Fmt=6&VInst=PROD&VType=PQD&RQT=309
&VName=PQD&TS=1300694374&clientId=14394
o Braun L, Cohen M. 2010. Herbs and Natural Supplements, An Evidence-
based Guide, 3rd ed. Churchill Livingstone Elsevier
o Bryant B & Knights K 2O11, Pharmacology for Health Professionals. 3RD ed.
Mosby Elsevier Australia

© Endeavour College of Natural Health endeavour.edu.au 51
References
o Buske-Kirschbaum, A. & Hellhammer, D.H. 2003, ‘Endocrine and immune
responses to stress in chronic inflammatory skin disorders’, Annuals of the
New York academy of science, Vol. 992, pp. 231-240.
o Callard, RE Hamvas, R Chatterton, C Blanco, C Pembrey, M Jones, R
Sherriff, A & Henderson, J 2002, ‘An interaction between the IL-4Rα gene
and infection is associated with atopic eczema in young children.’ Clinical
and experimental allergy, Vol 32, No. 7, pp. 990-993. Viewed 23/03/11:
http://onlinelibrary.wiley.com.ezp01.library.qut.edu.au/doi/10.1046/j.1365-
2222.2002.01414.x/full
o Catani MV 2005, ‘Biological role of vitamin C in keratinocytes.’ Nutrition
Reviews Washington, Vol. 63, No. 3; pp. 81-90.

© Endeavour College of Natural Health endeavour.edu.au 52
References
o Clark, C 2009, ‘New treatment for patients with chronic hand eczema.’
Clinical dermatology, Vol. 25, No. 1, pp. 6.Viewed 23/03/11:
http://find.galegroup.com.ezp01.library.qut.edu.au/gtx/retrieve.do?contentSe
t=IAC-
Documents&resultListType=RESULT_LIST&qrySerId=Locale%28en%2CUS
%2C%29%3AFQE%3D%28ti%2CNone%2C52%29New+treatment+for+pati
ents+with+chronic+hand+eczema+%3AAnd%3AFQE%3D%28da%2CNone
%2C4%292009%3AAnd%3AFQE%3D%28iu%2CNone%2C1%291%3AAnd
%3AFQE%3D%28pu%2CNone%2C20%29Clinical+Dermatology%3AAnd%
3AFQE%3D%28vo%2CNone%2C2%2925%24&sgHitCountType=None&in
PS=true&sort=DateDescend&searchType=AdvancedSearchForm&tabID=T
002&prodId=HRCA&searchId=R1¤tPosition=1&userGroupName=qut
&docId=A202706132&docType=IAC

© Endeavour College of Natural Health endeavour.edu.au 53
References
o Coulston, A Rock, C Monsen, E 2001, Nutrition in the Prevention and
Treatment of Disease, Academic Pree, London.
o Davidson, S Haslett, C 2002, Davidson’s Principles and Practice of
Medicine, 19th ed, Churchill Livingstone, United States.
o Garcia-Marcos L, Gonzalez-Dıaz C, Garvajal-Uruen AL, Pac-Sa MR,
Busquets-Monge RM, Suarez-Varela MM, Batlles-Garrido J, Blanco-Quiros
A, Varela A LS, Garcıa-Hernandez G, Aguinaga-Ontoso I. 2010, ‘Early
exposure to paracetamol or to antibiotics and eczema at school age:
modification by asthma and rhino conjunctivitis.’ Pediatric allergy and
immunology, Vol. 21, pp. 1036–1042.
o Groper, SS Smith, LJ & Groff, JL 2009, ‘Advanced nutrition and human
metabolism.’ 5th ed. Belmont, Wadsworth
o Helsby, N.A., Ward, S.A,, Parslew, R.A., Friedmann, P.S. & Rhodes, L.E.
1998, ‘Hepatic cytochrome P450 CYP2C activity in psoriasis: studies using
proguanil as a probe compound’, Acta Derm Venereol, vol. 78, no. 2, pp.
81-83.

© Endeavour College of Natural Health endeavour.edu.au 54
References
o Hosli, S Kostylina, S Yawalkar, G & Simon, N 2008, ‘Anti-CD20 (rituximab)
treatment improves atopic eczema.’
Journal of allergy and clinical immunology, Vol. 121, No. 1, pp. 122-
128.Viewed 23/03/11:
http://www.mdconsult.com.ezp01.library.qut.edu.au/das/article/body/237637
633-
2/jorg=journal&source=&sp=20366965&sid=0/N/626211/1.html?issn=0091-
6749
o Iciek, M Kwiecien, I & Włodek, L 2009, ‘Biological properties of garlic and
garlic-derived organosulfur compounds.’ Environmental and molecular
mutagenesis, Vol. 50, No. 3, pp. 247-265 Viewed 23/03/11:
http://onlinelibrary.wiley.com.ezp01.library.qut.edu.au/doi/10.1002/em.20474
o Jamison, J 2003, Clinical guide to nutrition and dietary supplements in
disease management, Churchill Livingstone, USA.

© Endeavour College of Natural Health endeavour.edu.au 55
References
o Kiuchi, F Iwakami, S Shibuya, M Hanaoka, F & Sankawa, U 1992, ‘Inhibition
of prostaglandin and leukotriene biosynthesis by gingerols and
diarylheptanoids.’I chemical and pharmaceutical bulletin. Vol. 40, no. 2, pp.
387-91.
o Kohlmeier, M 2003, Nutrient metabolism. Academic Press, New York.
o Kojima, H Shimojo, N Tomiita, M Nishimuta, T & Kohno, Y 2003, ‘The
expression level of cutaneous lymphocyte antigen on T-cells as a predictor
for the tolerance to hen’s egg-induced eczema.’ European journal of
pediatrics, Vol. 62 pp. 537–538. Viewed 23/03/11:
http://proquest.umi.com.ezp01.library.qut.edu.au/pqdweb?index=0&did=132
2856751&SrchMode=1&sid=1&Fmt=6&VInst=PROD&VType=PQD&RQT=3
09&VName=PQD&TS=1300691067&clientId=14394
o Kumar P & Clark M 2009, Clinical Medicine, 7th ed. Saunders Elsevier, UK

© Endeavour College of Natural Health endeavour.edu.au 56
References
o Lees & Bulleid, 1994, ‘The Role of Cysteine Residues in the Folding and
Association of the COOH-terminal Propeptide of Types I and I11
Procollagen.’ Journal of biological chemistry, Vol. 269, No. 39, pp. 24354-
24360.
o Lutz, W., Tarkowski, M. & Nowakowska, E. 2001, ‘Genetic polymorphism of
glutathione s-transferase as a factor predisposing to allergic dermatitis’,
Medical prevention, Vol. 52, No. 1, pp. 45-51.
o Mahan LK & Escott-Stump, S 2008, ‘Krause’s food and nutrition therapy.’
Saunders Elsevier, Missouri.
o Mahan LK & Escott-Stump, S 2012, ‘Krause’s food and nutrition therapy.’
Saunders Elsevier, Missouri.
o Maintz, L Benfadal, S Allam, J Hagemann, T Fimmers, R & Novak, N 2006,
‘Evidence for a reduced histamine degradation capacity in a subgroup of
patients with atopic eczema.’ Journal of allergy and clinical immunology, -
Vol. 117, No. 5 pp. 1100-1111

© Endeavour College of Natural Health endeavour.edu.au 57
References
o Martindale, S McNeill, G Devereux, G Campbell, D Russell, G & Seaton A
2005, ‘Antioxidant intake in pregnancy in relation to wheeze and eczema in
the first two years of life. ‘ American journal of respiratory and critical care
medicine. Vol. 171, No. 2, pp. 121-128. Viewed 23/03/11:
http://ajrccm.atsjournals.org/cgi/reprint/171/2/121
o Miyake, Y Sasaki, S Tanaka, K & Hirota Y 2010, ’Consumption of
vegetables, fruit, and antioxidants during pregnancy and wheeze and
eczema in infants.’ Allergy, Vol. 65, No. 6, pages 758–765.
o Miyake, Y Sasaki, S Tanaka, K Ohfuji, S & Hirota Y 2009, ’ Maternal fat
consumption during pregnancy and risk of wheeze and eczema in Japanese
infants aged 16–24 months: the Osaka Maternal and Child Health Study.’
Thorax, Vol. 64, pp. 815-821. Viewed 23/03/11:
http://thorax.bmj.com.ezp01.library.qut.edu.au/content/64/9/815#aff-3

© Endeavour College of Natural Health endeavour.edu.au 58
References
o Muszyska, A Woczyski, S & Paka, J, 2001, ‘The mechanism for
anthracycline-induced inhibition of collagen biosynthesis.’ European journal
of pharmacology, Vol. 411, no. 1-2, pp. 17-25.
Viewed 17/03/11:
http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6T1J-
420SJMJ-
&_user=2660300&_coverDate=05%2F31%2F2001&_rdoc=1&_fmt=high&_
orig=gateway&_origin=gateway&_sort=d&_docanchor=&view=c&_searchStr
Id=1681858377&_rerunOrigin=google&_acct=C000058449&_version=1&_u
rlVersion=0&_userid=2660300&md5=94437d378e812a10dcf4e122b18b0af
d&searchtype=a
o McCoy, K 2009, ‘Contact dermatitis.’ Merk professional manual online.
Viewed 23/03/11:
http://www.merckmanuals.com/professional/sec10/ch114/ch114c.html

© Endeavour College of Natural Health endeavour.edu.au 59
References
o Øien, T Storrø, O & Johnsen R 2010, ‘Do early intake of fish and fish oil
protect against eczema and doctor-diagnosed asthma at 2 years of age? A
cohort study.’ Journal of epidemiological community health, Vol 64, pp. 124-
129. Viewed 23/03/11:
http://jech.bmj.com.ezp01.library.qut.edu.au/content/64/2/124.full
o Osiecki, H 2006, The Physician's Handbook of Clinical Nutrition, 7th Ed,
BioConcepts Publishing QLD
o Osiecki H, 2004, ‘Research reveals conclusive association for skin disorder
patients’, Bioconcepts E-Newsletter, August.
o Pizzorno JE & Murray MT 2006, Textbook of Natural Medicine. 3rd ed.
Churchill Livingstone Elsevier
o Raap, U., Werfel, T., Jaeger, B., Schmid-Ott, G. 2003, ‘Atopic dermatitis and
psychological stress’, Hautarzt, vol. 54, no. 10, pp. 925-929.
o Sarris, J & Wardle, J 2010, Clinical Naturopathy. An evidence-based guide
to practice. Churchill Livingstone Elsevier

© Endeavour College of Natural Health endeavour.edu.au 60
Referenceso Schlenker, ED & Long, S, 2007, Williams essential of nutrition and diet
therapy. Mosby Elsevier, NSW.
o Seaborn, CD & Nielsen, FH, 2002, ‘Silicon deprivation decreases collagen
formation in wounds and bone, and ornithine transaminase enzyme activity
in liver.’ Biological Trace Element Research. Vol. 89, pp. 251-261.
o Skypala I, Williams M, reeves L, Meyer R, Venetr C, 2015. Sensitivity to
food additives, vaso-active amines and salicylates: a review of the
evidence. Clin Transl Allergy (2015) 5:34.
o Stargrove, MB Treasure, J & McKee, DL 2008 Herb, nutrient, and drug
interactions. Clinical implications and therapeutic strategies. Mosby
Elsevier, Missouri.
o Stollery, N 2007, ‘Photoguide: eczema.’ The Practitioner , Vol. 91. Viewed
23/03/11: http://find.galegroup.com.ezp01.library.qut.edu.au/gtx/retrieve.do?contentSet=IAC-
Documents&resultListType=RESULT_LIST&qrySerId=Locale%28en%2CUS%2C%29
%3AFQE%3D%28ti%2CNone%2C17%29PHOTOGUIDE+Eczema%3AAnd%3AFQE
%3D%28da%2CNone%2C4%292007%3AAnd%3AFQE%3D%28pu%2CNone%2C12
%29Practitioner%24&sgHitCountType=None&inPS=true&sort=DateDescend&search
Type=AdvancedSearchForm&tabID=T002&prodId=HRCA&searchId=R1¤tPosit
ion=1&userGroupName=qut&docId=A161213637&docType=IAC.

© Endeavour College of Natural Health endeavour.edu.au 61
References
o Tortora GJ & Derrickson, BH 2009, Principles of Anatomy and Physiology,
12th Ed, John Wiley & Sons, USA
o Werfel, T., Breuer, K. 2004, ‘Role of food allergy in atopic dermatitis’,
Current opinions on allergy and clinical immunology, Vol. 4, no. 5, pp. 379-
385.
o Wickens, K Black, PN Stanley, TV Mitchell, E Fitzharris, P Tannock, GW
Purdie,G & Crane, J 2008, ‘A differential effect of 2 probiotics in the
prevention of eczema and atopy: A double-blind, randomized, placebo
controlled trial.’ Journal of allergy and clinical immunology, Vol. 122, No. 4,
pp. 788-794. Viewed 23/03/ 11:
http://www.mdconsult.com.ezp01.library.qut.edu.au/das/article/body/237785
987-
5/jorg=journal&source=&sp=21124843&sid=0/N/665398/s00916749080131
95.pdf?issn=0091-6749

© Endeavour College of Natural Health endeavour.edu.au 62
References
o Atopic eczema, viewed 23rd Oct 2007
http://www.cleansleepcompany.co.uk/sitebuildercontent/sitebuilderpictures/1
0image001.jpg
o Seborrheic eczema, viewed 23rd Oct 2007
http://health.yahoo.com/media/mayoclinic/images/image_popup/ans7_seb_
dermatitis.jpg
o KW

© Endeavour College of Natural Health endeavour.edu.au 63
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and communicated to you by or on behalf of the Australian College of Natural Medicine Pty Ltd (ACNM) trading as Endeavour College of Natural Health, FIAFitnation, College of Natural Beauty, Wellnation - Pursuant Part VB of the Copyright Act 1968 (the Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act.
Do not remove this notice.