intensive insulin management and basal/bolus therapy
TRANSCRIPT
New Drugs and Devices: What is In
The Pipeline For Type 1 and Type 2
Diabetes
Steven V. Edelman, MD
Professor of Medicine
University of California San Diego School of Medicine
Veterans Affairs Medical Center
Founder and Director, Taking Control Of Your Diabetes, a 501(c)3
Not-for-Profit Organization
Type 1 Diabetes
Etiology
Screening and Prevention
Encapsulated islet cells
New glucagons
Artificial pancreas
SGLT1&2 inhibitors
Very smart apps
Pipeline Drugs And Devices Differ
Depending On What Type Of DiabetesType 2 Diabetes
Etiology
Screening and Prevention
Implantable GLP-1 RA
Oral GLP-1
Glucagon receptor antagonists
CGM for type 2 Diabetes
Most powerful therapy in type 2 diabetes!
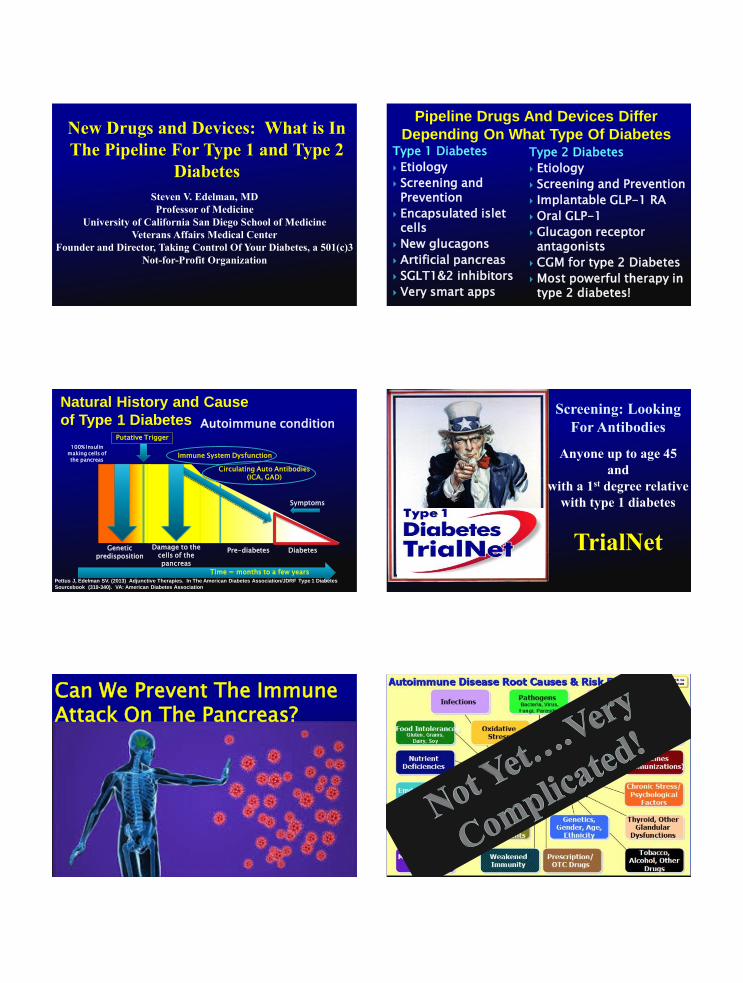
Natural History and Cause
of Type 1 Diabetes Autoimmune condition
Genetic predisposition
Damage to the cells of the pancreas
Pre-diabetes Diabetes
Time = months to a few years
100% Insulin making cells of the pancreas
Putative Trigger
Immune System Dysfunction
Circulating Auto Antibodies (ICA, GAD)
Symptoms
Pettus J, Edelman SV. (2013) Adjunctive Therapies. In The American Diabetes Association/JDRF Type 1 Diabetes
Sourcebook (319-340). VA: American Diabetes Association
Screening: Looking
For Antibodies
Anyone up to age 45
and
with a 1st degree relative
with type 1 diabetes
TrialNet
Can We Prevent The ImmuneAttack On The Pancreas?

Taken from Viacyte.com
Viacyte Device
Stem
Amylin
BLOOD VESSEL
CELLSMEMBRANE
Using the Devices in Mice Controls Blood Sugars
0
100
200
300
400
500
600
-42 -14 14 42 70 98 126 154 182 210 238
Blo
od
Glu
co
se (
mg
/dL
)
Time (days post-implant)
STZ
No STZ
Insulin implants
STZ VC-01 blood glucose control by graft stable 5+ months
after VC-01 explant,return of blood glucose topre-implant levels
9
Cell survival and differentiation into beta-cells 12 weeks after implant
Appears safe and well-tolerated
Encaptra device appears to be immune protective as designed
Need to optimize engraftment as it relates to the foreign body response to the device
STEP ONE: Demonstrated
Differentiation Into Beta Cells and
Potential for Prolonged Cell Survival
Both: 12-week PEC-Encap in
T1D patient Bottom: dark brown
= Nkx6.1 immunoreactivity
marks endocrine cells
PEC-Encap week 1
Age at Diagnosis of T1D
Beck RW, Tamborlane WV, Bergenstal RM, Miller KM, Dubose SN, Hall CA.
The T1D Exchange Clinic Registry. J Clin Endocrinol Metab. 2012; 97:4383-9.
You can get type 1 diabetes
at any age!

➢ The most missed diagnosis in diabetes
➢ Type 1 diabetes can occur at anyage
➢ Slower beta-cell destruction (may respond briefly to oral agents)
➢ Typically does not have features of the Metabolic Syndrome
➢ Blood test positive for type 1 diabetes (GAD auto antibodies)
Latent Autoimmune Diabetes in Adults
(LADA)
Gary Hall Jr.Olympic Gold MedalistWorld Record Holder
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes.
Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
Edelman SV, Henry RR. Diagnosis and management of type 2 diabetes.
12th Edition. Professional Communications, Inc., Greenwich, CT. 288 pages, 2014.
My Story with Type 1 Diabetes
Diagnosed at the age of 15
(1970) with the classic
symptoms
Thirst
Urination
Weight loss
Poor wound healing
Blurry vision
Fatigue
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fifth
Edition Professional Communications Inc., Greenwich, CT. , 2018.
My Story With Type 1 Diabetes
No one in my family had type 1 diabetes
I was sent home from the hospital on one shot of insulin a day (NPH/Reg)
Urine testing only
No A1c test
No pumps or pens
No insulin analogs
No CGM
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fifth
Edition Professional Communications Inc., Greenwich, CT. , 2018.
Banting and Best
University of Toronto, 1921
Jacobs. Diabetes Care. 1997; 20:1279.
Time (h)
22.00 3.00 7.00 8.00 9.00 10.00 11.00 12.00 13.00 14.00 15.00 16.00 17.00 18.00 19.00
1000
500
250
0
750
LisPro Regular
Serum Insulin Levels in Type 1 Diabetes
breakfast lunch dinner
Jacobs. Diabetes Care. 1997;20: 1279.
(mm
ol/
l)
Do
in
mg
/dL
15
10
5
0
Time (h)
22.00 3.00 7.00 8.00 9.00 10.00 11.00 12.00 13.00 14.00 15.00 16.00 17.00 18.00 19.00
*p < 0.05
Blood Glucose Levels
breakfast lunch dinner
Lispro Regular
Avg A1c=6.8
90
180
270

Subcutaneous Insulin Has A Very
Narrow Therapeutic Window
Too little insulin leads to postprandial hyperglycemia
Too much leads to hypoglycemia
Very difficult to get it just right
HypoglycemiaHyperglycemia
Insulin DoseEdelman SV. Taking control of your diabetes: a patient oriented book on diabetes. Fifth
Edition Professional Communications Inc., Greenwich, CT. , 2018.
Physiologic Insulin, Glucagon and
Amylin Secretion
LiverPancreas
Portal Vein
Systemic Circulation
InsulinAmylin
Glucagon
Beta Cell
Alpha Cell
Pettus J, Edelman SV. (2013) Adjunctive Therapies. In The American Diabetes
Association/JDRF Type 1 Diabetes Sourcebook (319-340). VA: American Diabetes Association
Inhaled Insulin (Afrezza)
Santos Cavaiola T, Edelman SV. Inhaled insulin: A breath of fresh air? A review of inhaled insulin. Clinical Therapeutics. 2014. 36(8)
Rapid on
Rapid off
• Better post meal glucose
values• Less delayed hypoglycemia
Faster Acting Aspart or Fiasp(addition of L-arginine and niacinamide for faster absorption)
Bode et al DTT Vol 19 2017
2 hour PG levels in
T1D onPump
therapy after a
standarized meal
comparing Aspart
(Novolog)with
Faster Aspert
(Fiasp)
Xeris ready-to-use liquid glucagon for
treatment of severe hypoglycemia
Translates to a strong value proposition:
Auto-injector delivery
◦ Ultra-compact design
◦ Simple, two-step operation
◦ Integrated safety features
Pre-filled syringe delivery preferred in some market segments
Superior caregiver/patient experience
◦ Reduced time to administration
◦ Increased likelihood of successful administration
◦ Reduced anxiety
Treatment of severe hypoglycemia –
as per current GEK labelIndication
• 0.5 and 1.0 mg of glucagon
• Pediatric and adult populationsDosing
• SC delivery
• SHL “Molly” auto-injector
− Auto-inject and auto-retract
− ‘Lock-out’ safety needle
– 1 - 2 second hold down time
(labeled at 5 seconds)
• Pre-filled syringe option also
available
Drug
Delivery
Devices
2 years at room temperatureStorage
Could a ready-to-use liquid glucagon
help address unmet need?
Lilly

Will There Be Adjustable Sizes? What is desirable: Contextual
awareness
Utilization of the sensors commonly found in today’s smartphones to tie BG to:
Location – GPS
Activity◦ Accelerometer
◦ Gyroscope
Time – day – date◦ Clock
◦ Calendar
Courtesy of
mHealthSys, Inc.
BG, blood glucose
Unmet needs – wireless sensor data
aggregation with multivariate
analytics• Wirelessly interfaced metabolic
sensors
• Aggregation and multivariate
analytics provide deeper insights Activity
BP
HR
Weight, body
fat
Courtesy of
mHealthSys, Inc.
Blood Glucose
Activity
Meals/Food Intake
Food intake
Activity
Glucose
BP, blood pressure; HR, heart rate
Courtesy of
mHealthSys, Inc.
Unmet needs –
automatic food recognition
Suggested portions
Estimate CHO, protein and fat
Recommended dose & testing schedule
Postprandial BG prediction
CHO, carbohydrate
Integrated system
Food type
Volume Carbs
Breaded 110 ml 11 g
Rice 120 ml 16.4 g
Salad 80 ml 2.6 g
Captured image
3D model
80 ml
120m
l
110 ml
Segmentation
CHO estimation Recognition
SaladRice
Breaded
Bolus Calculator
Smartphone server side
Plate detection
Mougiakakou S, et al. Diabetes Tech Ther 2015:17(Suppl. 1);A126 Abstract
285
Scan Your Plate With Your Smart Phone App!Basal/Bolus or MDI Insulin Regimen
With Rapid and Long-Acting
Analogs/Inhaled Insulin
4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
8:0012:008:00
Time
Insu
lin
Acti
on
GlulisineOr
AspartOr
FiaspOr
Lisproor
Inhaled InsulinU-100/U-300
Glargine/Detemir) Degludec
Adapted with permission from Leahy J. In: Leahy J, Cefalu W, eds. Insulin Therapy. New York: Marcel Dekker; 2002:87-112. Nathan DM.
N Engl J Med 2002;347:1342-1349.
BOLUS
Basal
Smart Pens For You MDI
(Multiple Daily Injection) Folks
Works On The
iPhone XI I
38
Artificial Panreas
Tandem t:slim G5/X2
Medtronic 630/670G/530G
OmniPod
Insulin Pumps
Edelman SV. Taking control of your diabetes: a patient oriented book on diabetes.
Fourth Edition Professional Communications Inc., Greenwich, CT. 544 pages, 2013.
530G/630G/670G
Enlite by Medtronic
Dexcom G4
& G5
Platinum
Continuous Glucose Monitoring Devices Currently Available In The United States

How CGM and Trending Information
Can Affect Our Decisions (CF/I:CHO)
Herrmann K, Frias JP, Edelman SV, Lutz K, Shan K, Chen S, Maggs D, Kolterman OG. Pramlintide improved measures of glycemic control and body
weight in patients with type 1 diabetes mellitus undergoing continuous subcutaneous insulin infusion therapy. Postgraduate Medicine. 123(3), 2013.
G5 Dexcom Now Connects Directly to the
Smart Phone and Apple Watch Smart Phone
Clarity App
Mean glucose value
Standard Deviation
Time in Range
24 hour multiday
profile
An Artificial Pancreas Is Coming Faster
Than We Thought Possible
BG
mg/dL
Time
180
70
50
Alarm –
impending
hypoNo response –
alarm plus insulin
reduction or
off/glucagon on if
needed
Alarm –
impending
hyper
No response – alarm plus
automated insulin push
to bring level below
threshold(glucagon off)
Resume preset basal rate
Minimize time
in “Red” zones
iLet • BigFoot • Tandem • Insulet • Medtronic
How does the Auto mode feature work?AUTOMATED BASAL INSULIN DELIVERY
Auto Mode:
▪ 48 hours before it kicks in▪ Delivers automated basal insulin
doses every 5 minutes▪ Automated basal target = 120 mg/dL▪ Temporary target of 150 mg/dL can
be used
Bolusing & Meals
▪ Must enter blood glucose (BG) readings and/or carbohydrate grams
670G
HYBTID
Closed Loop
Important to Understand
what it can and cannot do This is a basal rate modulator
Works well overnight
Still requires meal boluses, correction bolus, and many fingersticks
Diabetes tasks during the day are not decreased
There are more alarms
Glucose
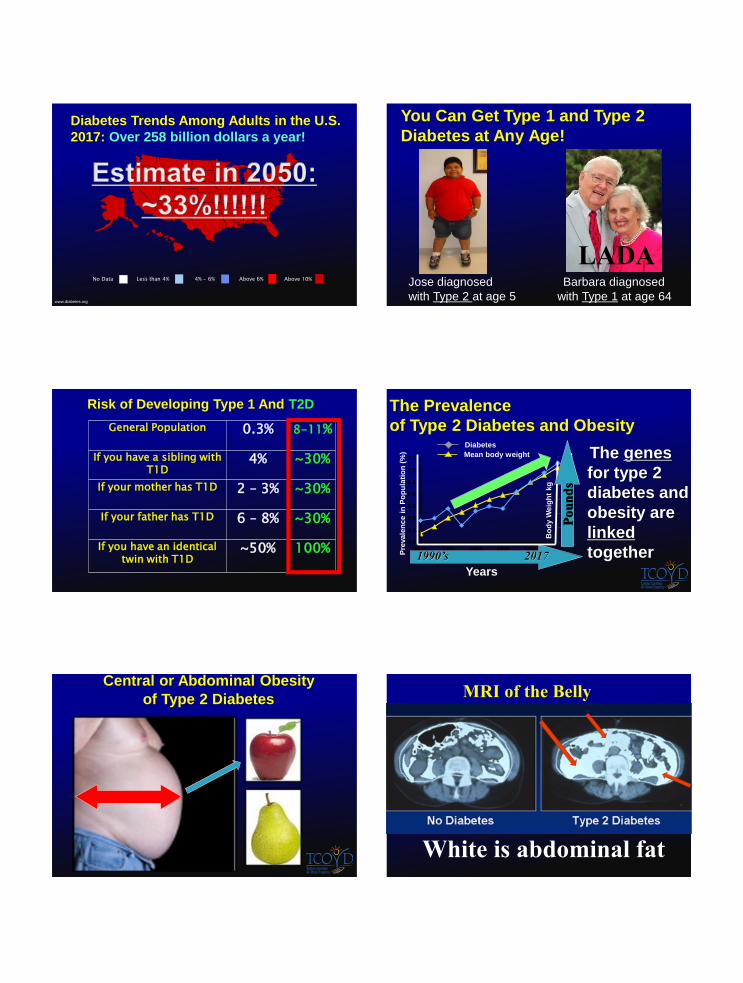
670G Study Subject Download
Average glucose = 153 (eA1c = 7.5%), 1% of readings < 70
mg/dl
D.I.Y.
SYSTEM
Old Medt.
Pump
iPhone
Riley Loop

Always in automode
Current BS-Blue
Predicted dotted line-Blue
How much insulin orange
(Example 6 extra units last hour)
Bars above and below baseline
Exercise targets
Cut out hypos almost completely
No lows at night
More time in range
iLet: Bionic Pancreas
2 ports for
insulin and glucagon
CGM Readings On and Off the Bionic Pancreas
Eversense
Implantable CGM (under FDA review)
“Other” Therapies for People
with Type 1 Diabetes
Symlin
Incretins (GLP-1 RA)*
SGLT-2 Inhibitors*
Inhaled Insulin
*Medications approved only type 2 diabetes at the current time

Sotagliflozin: First-in-Class Dual
SGLT1 and SGLT2 Inhibitor
SGLT1 is the primary transporter for absorption of glucose and galactose in the GI tract
SGLT2 is expressed in the kidney, where it reabsorbs 90% of filtered glucose
SGLT 1 SGLT 2
GI, gastrointestinal; SGLT, sodium-dependent glucose transporter Diabetes Care. 2015; 38(7):1181-8.
A1C and Hypoglycemia:T1D
Sotagliflozin significantly reduced mean A1C compared with placebo after 29 days with no increase in hypoglycemia
Change in A1C
-0.06
-0.55
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0
Placebo Sotagliflozin
Ch
an
ge
fro
m b
ase
lin
e (
%)
*
*P = 0.002 relative to
placebo
-0.4
-0.7
-0.8
-0.7
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0
Placebo Sotagliflozin
Ch
an
ge
fro
m b
ase
lin
e (
PP
D)
Change in number of hypoglycemic events (SMBG
≤70 mg/dL), per patient per day (PPD)
Multiple events for a patient were each counted
SMBG, self-monitoring of blood
glucose
Diabetes Care. 2015; 38(7):1181-8.
Body Weight T1D
Patients treated with sotagliflozin demonstrated weight loss compared with weight gain in the placebo group
0.5
-1.7
-2
-1.5
-1
-0.5
0
0.5
1
Placebo Sotagliflozin
Ch
an
ge
fro
m b
ase
lin
e (
kg
)
*
*P = 0.005 relative to placebo
Diabetes Care. 2015; 38(7):1181-8.
CGM Time in Target, Hyperglycemic,
and Hypoglycemic Ranges T1D
5.8
40.254
7.9
35.756.4
6.7
2568.2
<70 mg/dL
70–180 mg/dL
>180 mg/dL
Blood glucose
CGM
Sotagliflozin
% time in
ranges
Baseline
CGMDays –2 to –6
P=0.003
vs.
placebo
P=0.002
vs.
placebo
Treatment
CGMDays 3–27
8.5
35.
6
55
.
Placebo
% time in
ranges
Diabetes Care. 2015; 38(7):1181-8.
Phase 3 Program in T1DM Summary
inTandem program has the largest efficacy and safety database of an oral anti-diabetic agent for T1DM
Sotagliflozin significantly:
◦ Reduced A1C
◦ Reduced body weight
◦ Reduced blood pressure
◦ Reduced bolus insulin (leading to less hypoglycemia)
◦ Glucose variability (more time in range)
◦ Reduced severe hypoglycemia in the setting of optimized insulin setting
Benefit/risk profile favorable
◦ Additional A1C efficacy on top of insulin (consistent with SGLT 2 inhibition)
◦ Efficacy beyond A1C
◦ No increase in severe hypoglycemia, lower PPG, lower incidence of documented hypoglycemia (consistent with SGLT1 inhibition)
◦ DKA is manageable with appropriate care instructions
Type 2 Diabetes Trends Among
Adults in the U.S. 1990
Mokdad et al., Diabetes Care 2000;23:1278-83.
No Data Less than 4% 4% - 6% Above 6%
www.diabetes.org
Above 10%
Diabetes Trends Among Adults in the U.S.
2017: Over 258 billion dollars a year!
No Data Less than 4% 4% - 6% Above 6%
You Can Get Type 1 and Type 2
Diabetes at Any Age!
Barbara diagnosed
with Type 1 at age 64
Jose diagnosed
with Type 2 at age 5
LADA
Risk of Developing Type 1 And T2D
General Population 0.3% 8-11%
If you have a sibling with T1D
4% ~30%
If your mother has T1D 2 – 3% ~30%
If your father has T1D 6 – 8% ~30%
If you have an identical twin with T1D
~50% 100%72
73
74
75
76
77
78
4.0
4.5
5.0
5.5
6.0
6.5
7.0
7.5
1990 1992 1994 1996 1998 2000
The genes
for type 2
diabetes and
obesity are
linked
together
The Prevalence
of Type 2 Diabetes and Obesity
Pre
vale
nce i
n P
op
ula
tio
n (
%)
Diabetes
Mean body weight
Bo
dy W
eig
ht
kg
Years
1990’s 2017P
ou
nd
s
Central or Abdominal Obesity
of Type 2 Diabetes MRI of the Belly
White is abdominal fat

Diabetes in America.. NIH No. 95-1468. 1995:233-257.
Causes of Mortality in Patients With
Diabetes 20 years Ago:
The same Trend Exists in 2017
STROKE
Other
Pneumonia/
InfluenzaMalignant
Neoplasms
“Diabetes
complications”
10%
13%
13%
4% 5%
55%
Heart Disease
http://professional.diabetes.org/?loc=bb-dorg
Most Common Causes of Death in People With
Type 2 Diabetes: It is not eye, kidney or nerve
disease!
Geiss LS, et al. In: Diabetes in America, 2nd ed. 1995. Bethesda, MD: National Institutes
of Health; 1995:Chapter 11.
0
10
20
30
40
50
% of
Deaths
Ischemic
Heart
Disease
Other
Heart
Disease
Diabetes
related
Cancer Stroke Infection Other
Almost 80% do to any type
of heart disease and stroke
http://professional.diabetes.org/?loc=bb-dorg
Relatively New Class of Injectable
Medications for Type 2 Diabetes
GLP-1 RA Agonists
Improved control (A1c)
WEIGHT LOSS
Low risk of low blood glucose
LillyAstraZeneca NovoNordisk
Trulicity
Sanofi
Fixed Combinations Of Basal Insulin and GLP1-RA
Xultophy and Soliqua
Lancet Diabetes Endocrinol. 2014 Nov;2(11):856-8, 2017 PDR PIs
J
Two excellent diabetes medication in one pen!“Basal insulins that are super charged”
57 years of age BMI 32, drug naïve or metformin
DOD 6.3 years
A1c Oral Semaglutide (-0.7 to -1.9%) Dose ranging
A1c Injectable semaglutide -1.9%
A1cOral placebo -0.3%
Weight loss oral smeaglutide -6.9kg (highest dose)
Weight loss injectable semaglutide -6.4%
Mild to moderate GI side effects in both groups
ITCA 650—Medical Device To
Deliver Type 2 medication
Previously-approved GLP-1
therapeutic with demonstrated:
−Glycemic control
−Weight loss
−Safety
MEDICINE: EXENATIDE
Previously-approved delivery system
Small micropump
−Maintains stability at temps ≈37⁰C
−Maintains stability for > 12 months
TECHNOLOGY
Not yet approved by the FDA

Study SAVOR EXAMINE TECOS CAROLINA CARMELINA
DPP4-i saxagliptin
alogliptin sitagliptin linagliptin linagliptin
Comparator placebo placebo plcebo sulfonylurea placebo
N 16,500 5,400 14,000 6,000 8,300
Results 2013 2013 June 2015
2017 2017
✓ ✓ ✓
Large Non-Insulin CVOTs in T2DM
DPP-4 Inhibitors
Study LEADER ELIXA SUSTAIN 6
EXSCEL REWIND
GLP1-RA liraglutide lixisenatide semaglutide exenatide LR dulaglutide
Comparator placebo placebo placebo placebo placebo
N 16,500 14,000 6,000 5,400 8,300
Results 2016 2015 2016 2018 2019
✓ ✓✓
Large Non-Insulin CVOTs in T2DM
GLP-1 Receptor Agonists
Courtesy of Silvio Inzucchi MD, Yale University
✓
Study EMPA-REG CANVAS DECLARE NCT01986881
SGLT-2-i empaglifozin canagliflozin dapagliflozin ertugliflozin
Comparator placebo placebo placebo placebo
N 7300 4300 22,200 3900
Results Sept 2015 2017 2019 2020
Large Non-Insulin CVOTs in T2DM
SGLT-2 Inhibitors
Courtesy of Silvio Inzucchi MD, Yale University
✓ ✓
Investigatte Before Vilifying A Medication
(relative risk vs absolute risk)
(imbalance that is statistically significant)
Avandia (rosiglitazone): CAD Actos (pioglitazone): bladder cancer Insulin glargine (Lantus): breast cancer DPP-4 inhibitors: pancreatic cancer Onglyza (saxagliptin): hosp. for CHF Invokana (canagliflozin): amputation Ozempic (semaglutide) retinopathy/DME
Elvis
Abbott FreeStyle Libre: Now approved in the US
Waterproof
Lasts 10 days
12 hour warm up
Swipe to get a number
No calibration
Low Cost
swipe
Future Developments
Develop:
• A simple
• Easy to apply
• Low cost
• Disposable sensor
• Integrated into a
monitor or smart phone
Will give you a
glucose reading
every 5 minutes!

Natural History of Type 2 Diabetes Is Characterized by
Progressive Loss of Beta Cell Function
Macrovascular complications
Microvascular complications
Insulin resistance
Insulin secretion
Postprandial glucose
Fasting glucose
Progression of Dysglycemia
Prediabetes and Early Type
2 Diabetes: Generally
Asymptomatic
Diagnosis of Type 2
Diabetes Typically Delayed
Years to Decades
Progression to Type 2 Diabetes
Can be Prevented or Delayed
Adapted from Ramlo-Halsted BA, Edelman SV. Prim Care. 1999;26:771-789
Prediabetes Type 2 Diabetes
Completed diabetes prevention trials
Edelman, S. Diagnosis and Management of Type 2 Diabetes 10th Edition, Chapter 16.
Clinical study Treatment (3-4 years)Relative riskreduction
Finnish Diabetes Prevention Study Diet & exercise vs. control 58%
Diabetes Prevention ProgramDiet & exercise vs.placeboMetformin vs placebo
58%31%
STOP-NIDDM Acarbose vs. placebo 25%
Tripod Troglitazone in GDM 56%
XENDOS Orlistat vs. placebo 45%
DREAM Rosiglitazone vs. placebo 62%
ACT NOW Pioglitazone vs. placebo 72%
ORIGINInsulin glargine vs. placebo
28%
Developments In The Past
Decade For Type 2 Diabetes
DPP4 inhibitors (4 in the class)
SGLT2 Inhibitors (3 in the class)
GLP1-RA (5 in the class)
Several positive CVOT trials
Newer basal insulins
Fixed combinations of GLP1-RA & basal insulins
Insulin pumps for type 2 (Vgo and the T-Flex)
Inhaled insulin
Software programs and multiple apps
% o
f P
ati
en
tsa
Ach
ievin
g H
bA
1c <
7%
2003-20061
N=999
0
2007-20101,2
N=1444
2011-20142
N=2677
50
56.8%52.2% 50.9%
10
20
30
40
60
70
90
100
80
NHANES, National Health and Nutrition Examination Survey.aPatients with either Type 1 or Type 2 diabetes.
1. Ali MK et al. N Engl J Med. 2013;368:1613-1624. 2. Carls GS et al. 76th ADA Scientific Sessions. June 10–14, 2016. Poster 1515-P.
NHANES Data
ONLY ABOUT HALF OF PATIENTS ACHIEVE
HbA1c <7% WITH VIRTUALLY NO CHANGE
OVER THE LAST DECADE
NNO CHANGE IN THE LAST DECADE
HEDIS data from >1000 health plans covering >171 million lives (2014)
% o
f P
ati
en
ts A
ch
ievin
g H
bA
1c <
7%
2007 2008 2009 2010 2011 2012 2013 2014 2007 2008 2009 2010 2011 2012 2013 2014
HMO POPULATION MEDICAID POPULATION
ONLY ABOUT 40% OF PATIENTSa
ARE AT HbA1c <7%
ONLY ABOUT 30% OF PATIENTSa
ARE AT HbA1c <7%
0
50
10
20
30
40
60
70
80
90
100
% o
f P
ati
en
ts A
ch
ievin
g H
bA
1c <
7%
0
50
10
20
30
40
60
70
80
90
100
National Committee for Quality Assurance. http://www.ncqa.org/ReportCards/HealthPlans/StateofHealthCareQuality.aspx.
HEDIS, Healthcare Effectiveness Data and Information Set.aPatients with either Type 1 or Type 2 diabetes.
COMMERCIAL HMO AND MEDICAID
POPULATION RESULTS ARE EVEN WORSE
NO CHANGE IN 10 YEARS NO CHANGE IN 10 YEARS
HEDIS data from >1000 health plans covering >171 million lives in 2014
2005 2014
29.7% 31.1%OF ALL
PATIENTS
WITH
DIABETES*
OF ALL
PATIENTS
WITH
DIABETES*
% OF DIABETIC
PATIENTS WITH
VERY POOR GLYCEMIC
CONTROL
(HbA1c >9%)
IN THE US
National Committee for Quality Assurance. http://www.ncqa.org/ReportCards/HealthPlans/StateofHealthCareQuality.aspx.
*In a commercial HMO population that includes either Type 1 or Type 2 diabetes.
RATES OF VERY POOR GLYCEMIC CONTROL IN
DIABETES HAVE ALSO NOT IMPROVED

$110
$119
$130
$140
$151
$164
$180
$202
$224
$249
$274
$301 $331 $363
$0
$50
$100
$150
$200
$250
$300
$350
$400
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
MEDICAL COSTS OF T2D ARE
INCREASING IN THE US
* Includes medical costs of type 2 diabetes and related complications.
Total US Medical Costs for Diabetes From 2007 to
2020 (in billion US dollars)*
>$1000 cost burden
for every person in
US
Reference: UnitedHealth Group, The United States of Diabetes: Challenges and opportunities in the decade ahead. Working paper 5. November 2010.
DIABETES IS NOT A
RARE DISEASE AND
IT IS NOT AN
INEXPENSIVE
DISEASE
$
Steven V. Edelman, MDClinical Professor of Medicine
University of California, San Diego
Director, Taking Control of Your Diabetes
(TCOYD)
Type 2 Diabetes: Why Do
Clinical Trial Results
Disappear In Real World
Practice?
William Polonsky PhDPresident,g Behaviorall Diabetes Institute (BDI))
Clinical Professor of Medicine
University of California, San Diego
Diabetes Care (accepted for publication)
25%
REAL-WORLD RESULTS
PREDICTED UNDER TYPICAL
TRIAL CONDITIONSa
EXPLAINING
THE GAP
REAL
WORLDb
-1.04%
75%
-0.52%
GAP ADHERENCEc
Carls GS et al. 76th ADA Scientific Sessions. June 10–14, 2016. New Orleans, LA. Poster 117-LB.
BASELINE
CHARACTERISTICS,
ADDITIONAL DRUG
THERAPY
RCT, randomized clinical trial.aLinear regression model fitted to estimate the change in HbA1c 1 year after initiating GLP-1 RA or DPP-4i based on baseline and treatment characteristics. bOptum/Humedica SmartFile database (2007-2014) was used (GLP-1 RA 221 patients; DPP-4i 652 patients). Change in HbA1c measured from drug initiation to 365±90 days later. cMedical adherence classified as poorly adherent if percentage of days covered (PDC) <80%.
{
0
–1.2
–0.4
–0.8
–0.2
Ch
an
ge i
n H
bA
1c (
%)
–1.0
–0.6
–1.4
–1.6
POOR ADHERENCE IS THE KEY
CONTRIBUTOR TO THE EFFICACY GAP: GLP-1
RAs
Video of type 2 live longer
Get Type 2 Diabetes..And Live Longer Because Of It!
THANK
YOU!
[email protected] V. Edelman, MD
Professor of Medicine
University of California San Diego School of Medicine
Veterans Affairs Medical Center
Founder and Director, Taking Control Of Your Diabetes, a 501(c)3
Not-for-Profit Organization