interaction médicamenteuse 2015 · 2018. 3. 9. · anti-vitamink potentialisation des...
TRANSCRIPT

Interactions médicamenteuses
G Berkenboom
6/06/15

Médicaments retirés du marché
● Terfénadine (Triludan) Février 1998 ● Astémizole (Hismanal) Juillet 1999 ● Cisapride (Prépulsid) Janvier 2000 ● Cérivastatine Juillet 2001 ● Dompéridone (Motilium) Avril 2015
surveillance accrue
Complications léthales mais rares IMPACT ECONOMIQUE
Impact clinique surdosage/intolérance
● Intolérance aux statines ● Hémorragie sous anticoagulants,
antiagrégants ● Résistance aux antiagrégants ● Interaction pharmacodynamique
(insuffisance rénale, somnolence….)
Causes du problème
● Vieillissement de la poulation ● Explosion du nombre de prescriptions ● Risque d’interaction augmente de
manière exponentielle à partir de 4 médications

Drug availability
● Absorption ● Distribution ● Metabolism ● Elimination

P-glycoprotein transport system
● 2 types of transporters . Solute carrier transporters (facilitated or ion-coupled) OAT &OCT . ATP binding cassette (<ATP to pump across cell membranes) *P-gp
● Pgp* Responsible of elimination from hepatocytes into bile from renal tubular cells into urine

Date of download: 3/30/2015
Copyright © The American College of Cardiology. All rights reserved.
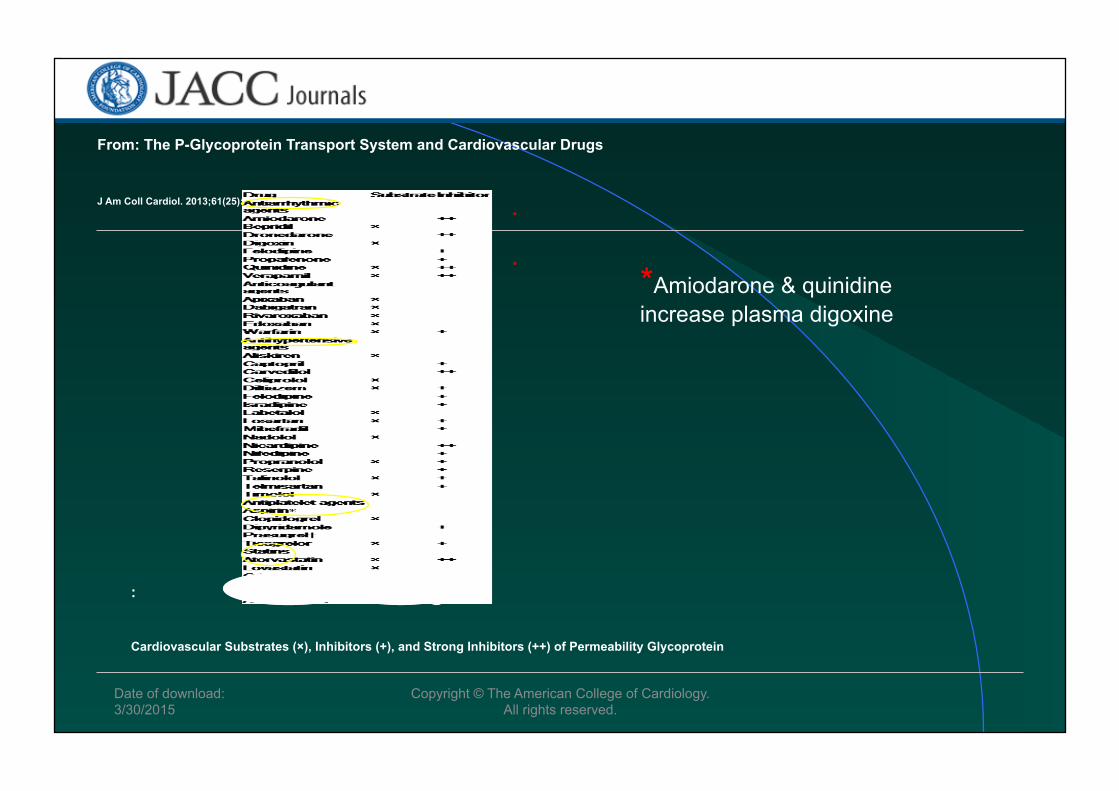
From: The P-Glycoprotein Transport System and Cardiovascular Drugs
J Am Coll Cardiol. 2013;61(25):2495-2502. doi:10.1016/j.jacc.2013.02.058
Structure of Permeability Glycoprotein Model of substrate transport by permeability glycoprotein (P-gp). (A) Substrate (magenta) partitions into the bilayer from outside the cell to the inner leaflet and enters the internal drug-binding pocket through an open portal. The residues in the drug-binding pocket (cyan spheres) interact with inhibitors and substrates in the inward-facing conformation. (B) Adenosine triphosphate (ATP) (yellow) binds to the nucleotide-binding domains, causing a large conformational change presenting the substrate and drug-binding site(s) to the outer leaflet/extracellular space.
Figure Legend:

Date of download: 3/30/2015
Copyright © The American College of Cardiology. All rights reserved.
From: The P-Glycoprotein Transport System and Cardiovascular Drugs
J Am Coll Cardiol. 2013;61(25):2495-2502. doi:10.1016/j.jacc.2013.02.058
Mechanisms of P-gp-Directed Efflux Permeability glycoprotein (P-gp) is found on the apical/luminal membrane of intestinal epithelial cells (A), the canalicular membrane of human hepatocytes (B), and the apical/luminal membrane of renal proximal tubule cells (C).
Figure Legend:

Complexity
● Same drugs can act as substrate and inhibitor (>< efflux) or inducer
● Drugs metabolized by CYP 450 are also substrates for P-gp (& OAT, OCT)!
Date of download: 3/30/2015
Copyright © The American College of Cardiology. All rights reserved.
From: The P-Glycoprotein Transport System and Cardiovascular Drugs
J Am Coll Cardiol. 2013;61(25):2495-2502. doi:10.1016/j.jacc.2013.02.058
Cardiovascular Substrates (×), Inhibitors (+), and Strong Inhibitors (++) of Permeability Glycoprotein
:
*
* *Amiodarone & quinidine increase plasma digoxine
dabigatran
● P-gp inhibition increases plasma dabigatran concentration ketoconazole 153% dronaderone 99% amiodarone 50% (report cases of hm shock)
● Atorva also a P-gp inhibitor but no increase in dabigatran action?

rivaroxaban
● Rifampicine (P-gp inducer) decreases rivaroxaban action
● Ritonavir (P-gp inhibitor) increases rivaroxaban action Amiodarone also (but to a lesser extent)
apixaban
● Ketoconazole 100% increase (true for all NOAC)
● Amiodarone minor increase

NOAC via dabiga apixa edoxa rivaro
atorva Pgp, Cyp +18% verapamil Pgp +12-180% +53% diltiazem Pgp +40% quinidine Pgp +50% +80% amioda Pgp +12-60% +10% +40% +10% Ketocon-azole
Pgp, Cyp +140% +100% ? +160%
erythro Pgp, Cyp +15-20% ? ? +30-50% HIV protease
Pgp, Cyp ? +100% ? +150%
Eur H J 2013;34:2094

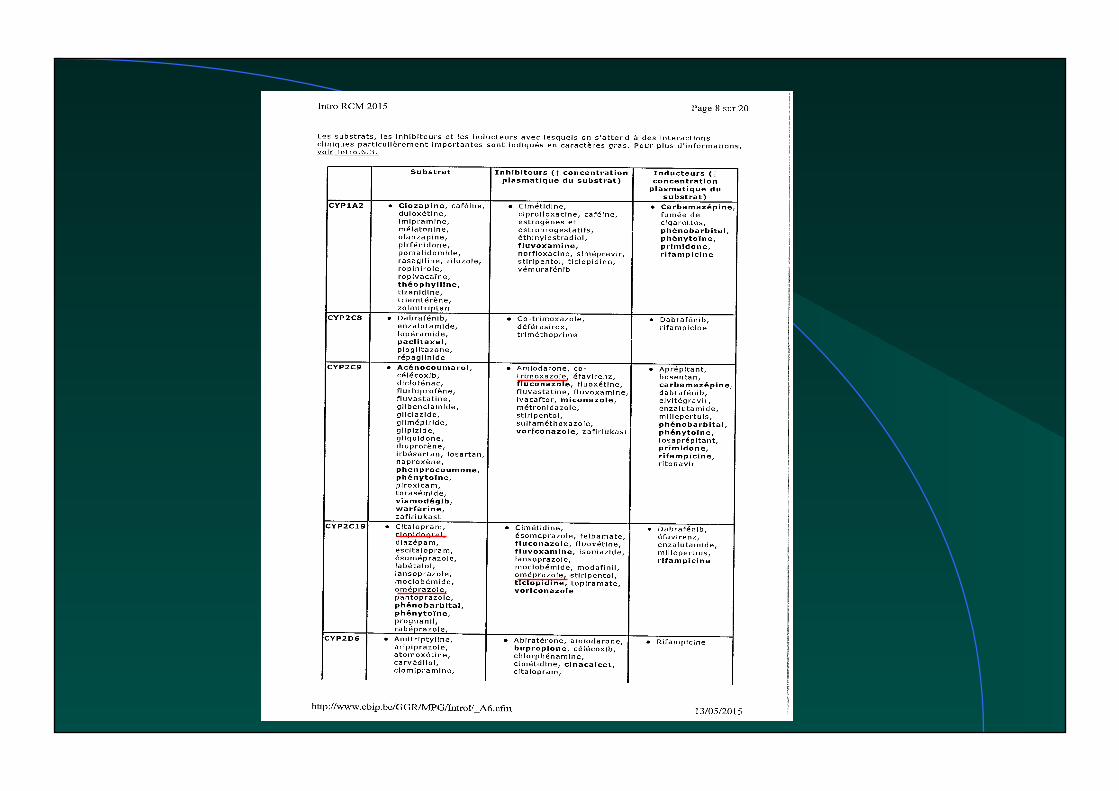
Anti-vitaminK ● Potentialisation des anticoagulants oraux:
.allopurinol, amiodarone, disopyramide, quinidine
.érythromycine, pénicillines, tétracyclines
metronidazole (Flagyl), cotrimoxazole <CYP2C9
fibrates (déplacement de liaison protéique)
.fluvastatine? Mais pas les autres statines? (prava et rosuva OK) AINS (à éviter!)
● Inhibiteurs:
Barbituriques, rifampicine (also for NOAC)
Date of download: 5/4/2015
Copyright © The American College of Cardiology. All rights reserved.
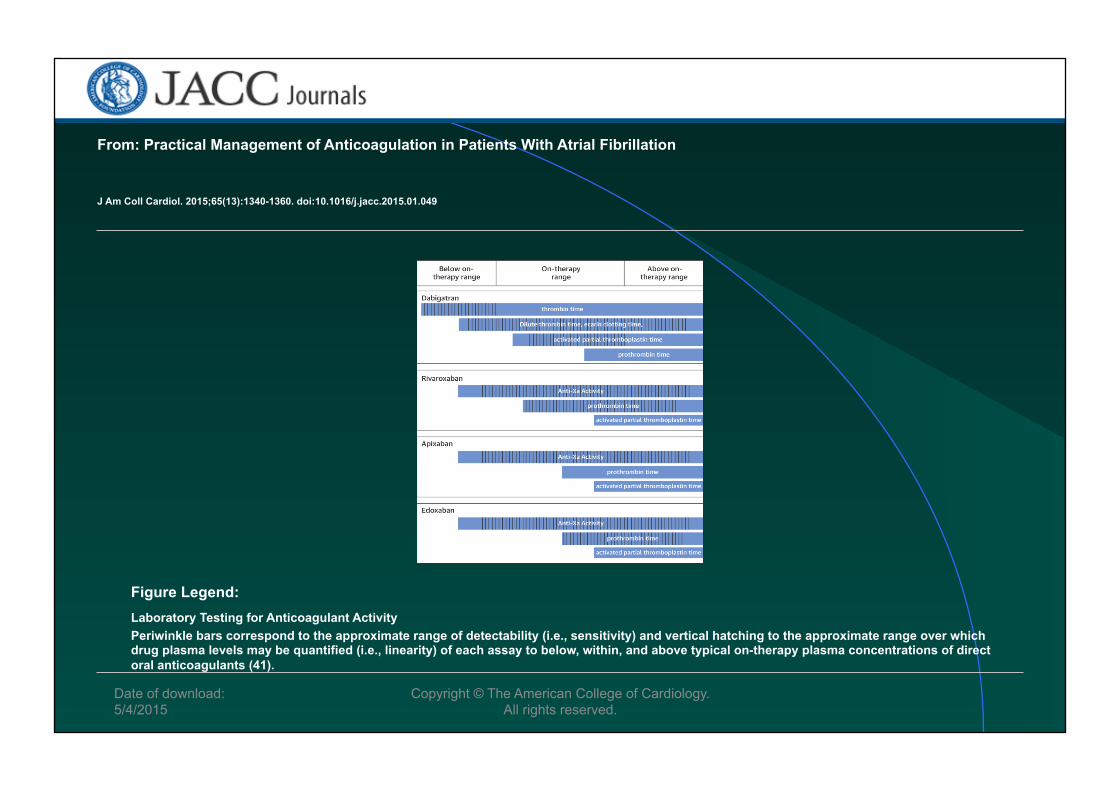
From: Practical Management of Anticoagulation in Patients With Atrial Fibrillation
J Am Coll Cardiol. 2015;65(13):1340-1360. doi:10.1016/j.jacc.2015.01.049
Laboratory Testing for Anticoagulant Activity Periwinkle bars correspond to the approximate range of detectability (i.e., sensitivity) and vertical hatching to the approximate range over which drug plasma levels may be quantified (i.e., linearity) of each assay to below, within, and above typical on-therapy plasma concentrations of direct oral anticoagulants (41).
Figure Legend:

Date of download: 5/4/2015
Copyright © The American College of Cardiology. All rights reserved.
From: Practical Management of Anticoagulation in Patients With Atrial Fibrillation
J Am Coll Cardiol. 2015;65(13):1340-1360. doi:10.1016/j.jacc.2015.01.049

Inhibition of Pgp digoxin
● Increase rate of av bloc ● Nicardipine>
verapamil>diltiazem>nifedipine ● Carvedilol, bisoprolol, propranolol (but
not atenolol, metoprolol, sotalol) ● Atorva

Clopidogrel response variability
● Activated platelets (advanced age, diabetes mellitus)
● Cyp 3A4: drug competition & decrease in the active metabolite
● Reduction into its active metabolite < genetic variation in Cyp 2C19 (hetero- homozygote) P-gp (overexpression)
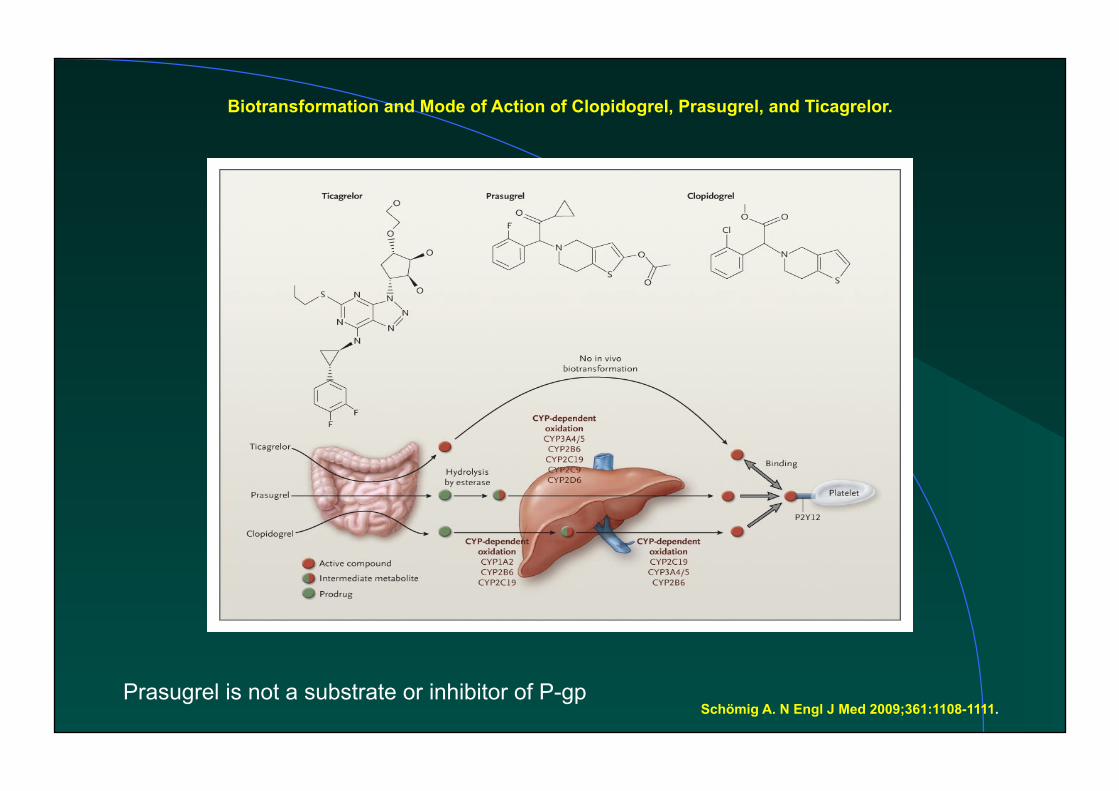
Biotransformation and Mode of Action of Clopidogrel, Prasugrel, and Ticagrelor.
Schömig A. N Engl J Med 2009;361:1108-1111. Prasugrel is not a substrate or inhibitor of P-gp
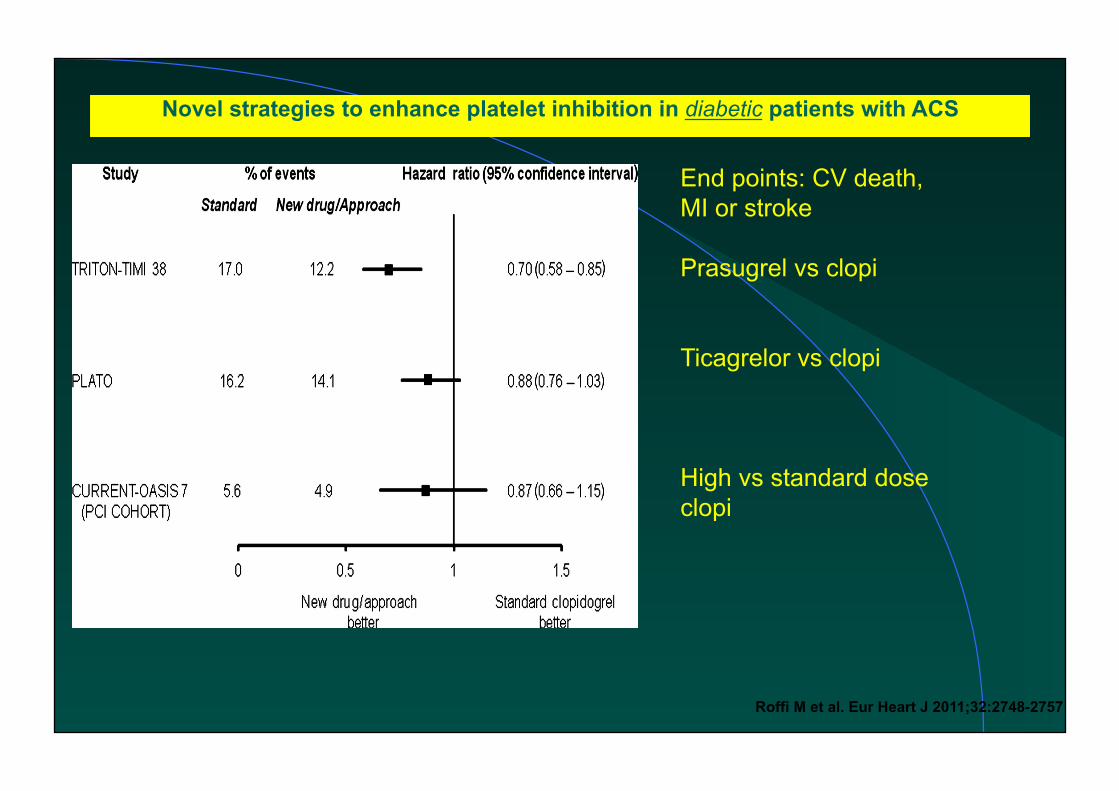
Novel strategies to enhance platelet inhibition in diabetic patients with ACS
Roffi M et al. Eur Heart J 2011;32:2748-2757
End points: CV death, MI or stroke Prasugrel vs clopi Ticagrelor vs clopi High vs standard dose clopi

Statin & drug interaction (1)
● < metabolization in gut wall & liver to hydrophilic metabolites readily excreted by kidney mainly CYP3A4 (genetic variability in expression of
cyto P450 isoenzymes) for lovastatin, simvastatin & atorvastatin (highly sensitive to inhibitor)
● Prava & rosuva: no significant metabolism (10% CYP2C9); cyclo & gemfibrozil can increase plasma conc by blocking their biliary excretion
CYP3A4 ● Substrats: .diltiazem, verapamil
.amiodarone, quinidine, disopyramide, lidocaine, propfénone .clopidogrel (pro-drogue) .losartan (aussi CYP2C9) .diazépam, alprazolam, midazolam .simvastatine, atorvastatine .digitoxine, éthynilestradiol, terfénadine, cyclosporine
● inhibiteurs: cimétidine, erythromycine, clarithromycine, tacrolimus, coticoides, HIV protease, tamoxifène, *pamplemousse tricycliques, omeprazole, ketoconazole
● inducteurs: barbituriques, rifampicine, dexamet *pamplemousse augmente biodisponibilité des statines

Interactions avec statines
● fluva: métabolisé par CYP2C9 biodisponibilité augmente avec: .Azoles .ritonavir .anti-H2; omeprazole
En pratique pour statine ● Cyclo, erythromycine, CCB, HIV protease:
augmentent conc plasmatique atorva lova simva risque de myopathie (CYP3A4)
● Si antagoniste du calcium: utliser prava ou fluva, rosuva ● Pamplemousse augmente la conc plasmatique: simva lova,
atorva (activité > 30% qd jus de pamplemousse pris pdt 3 j) ● statine et coumarine: interaction controversée? (surtout fibrates
potentialisent les anticoagulants) ● Fibrates peuvent aussi créer des myopathies et diminuent la
clairance hépatique des statines

Fibrates/statines
● Fibrates éliminés par reins; insuf rénale augmente risque de myopathies
● L ’augmentation des conc plasmatiques des statines se fait sans interaction avec le CYP3A4 (mais via OAT)
Interaction bien démontrée entre gemfibrozil (Lopid); le taux de
rabdomyolyse est nettement plus élevé avec la cériva (16 à 80 x) <synergie; En association (fibrate + statine), 1% des pts ont les CK X3
● En pratique si CKx > 5: stop statine

Therapeutic flow-chart for management of patients with statin-associated muscle symptoms.
Erik S. Stroes et al. Eur Heart J 2015;36:1012-1022
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.

Effects potentially involved in statin-related muscle injury/symptoms (Reproduced with permission from Needham and Mastaglia 2014).79 A number of statin-mediated effects have been proposed including reduced levels of non-cholesterol end-products of the mevalonate pathway; reduced
sarcolemmal and/or sarcoplasmic reticular cholesterol; increased myocellular fat and/or sterols; inhibition of production of prenylated proteins or guanosine triphosphate (GTP)ases; alterations in
muscle protein catabolism; decreased myocellular creatine; changes in calcium homeostasis; immune-mediated effects of statins and effects on mitochondrial function—see Figure 4 and Box
4.
Erik S. Stroes et al. Eur Heart J 2015;36:1012-1022
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Statines/toxicité musculaire
● Surtout molécules lipophiles: simva atorva lova
● Facteurs favorisant: insuf hépatique et éthylisme rénale infection aiguë hypothyroidie
âge (> 80 ans) polymédications
● En cas d ’insuf rénale: atorva est la statine de choix (élimination hépatique) Pour prava: si Cl créat < 60 ml/min: diminuer la dose de moitié
Statin high doses
● High doses seem beneficial in the early days after ACS but not in patients with stable symptoms
● Consider fct age, impact of long term therapy; if high risk: intensive strategy
● Large trials comparing different doses of the same statin, with 5 y fup & « hard » end points are needed

Cyclosporine ● Métabolisée par CYP3A4:
pamplemousse, vérapamil, diltiazem augmentent le taux plasmatique de cyclo
● Augmente risque de myopathie avec statines (simva, atorva..)
liposolubles, (prava, rosuva >< excrétion biliaire)
● Augmente taux de digoxine

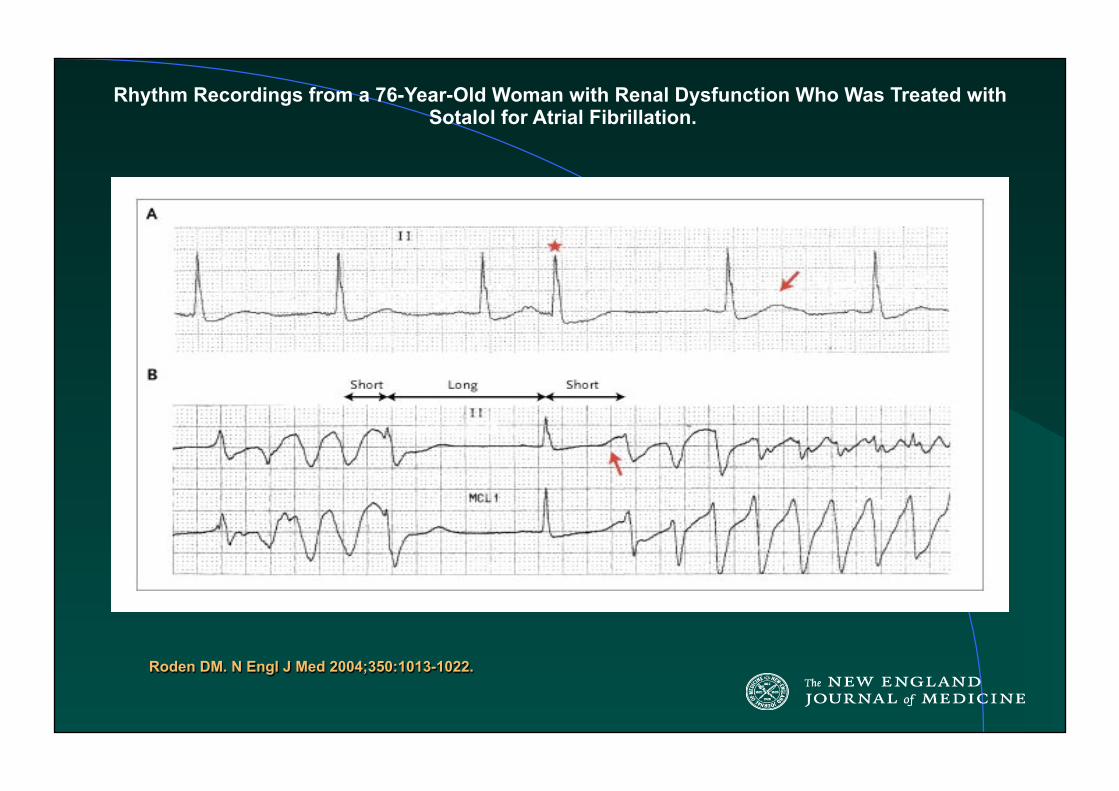
Rhythm Recordings from a 76-Year-Old Woman with Renal Dysfunction Who Was Treated with Sotalol for Atrial Fibrillation.
Roden DM. N Engl J Med 2004;350:1013-1022.
Drug-induced prolongation of the QT interval
● Antiarrhythmic drugs: Class 3: Sotalol, amiodarone, donaderone, ibutilide…. Class 1: disopyramide, quinidine, procainamide…
Discrepancies between the in vitro data (on action potential) & the risk of tdp
● Antidepressants, antipsychotics: nortryptyline, chlorpromazine, haloperidol, fluoxetine,risperidone
Risk factors for tdp
● Female ● Hypokaliemia, hypomagnesemia ● HF ● recent conversion from AF ● QT prolongation (subclinical) ● Ion channel polymorphisms ● Digitalis therapy

Terfenadine & CYP3A
● Biotransformed in fexofenadine (non cardioactive, but still antiH1) by CYP3A4
● In case of CYP3A4 inhibition (erythtromycin,
ketoconazole) or dowregulation (cirrhosis, HF…) or genetic factors…increased risk of tdp

Effects of a Drug on Whole-Organ Function.
Roden DM. N Engl J Med 2004;350:1013-1022.

Risk of acute renal failure with RAS inhibition
● Renal artery stenosis (bilateral) ● Decreased (absolute or effective)
arterial blood volume ● Use of nonsteroidal antiinflammatory
drugs ● Use of cyclosporine, tacrolimus
N Engl J Med 2002;3471256

(A) Adaptative mechanisms to renal hypoperfusion in compensated heart failure.
Ruggenenti P , Remuzzi G Eur Heart J 2011;32:2476-2478
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2011. For permissions please email: [email protected]
Take-home message
● Caution .with drug activity influenced by genetic polymorphism .with drugs having potent interactions on CYP3A4, P-gp
● List of drugs to avoid in cases long QT, Brugada.. are available: www.ncbi.nlm.nih.gov www.brugadadrugs.org
Take-home message (2)
● Cv drugs with narrow therapeutic indexes (antiarrhythmic, anticoagulant agents) can have large increase in concentrations (P-gp & Cyp3A4 inhibitors)
● Dose adjustment or use of alternative agents
● Special concerns with: erythromycin, azoles, amiodarone, quinidine, antidepressants and HIV protease inhibitors