interindividual variability of drug transport proteins: focus on
TRANSCRIPT


To my family


Investigations included in this thesis
This thesis is based on the following investigations, which will be referred to by the Roman numerals assigned below:
I mRNA expression of drug-transporting proteins along the human intestine and comparison with expression in Caco-2 cells Gunilla Englund, Fredrik Rorsman, Anders Rönnblom, Urban Karl-bom, Lucia Lazorova, Johan Gråsjö, Andreas Kindmark and Per Artursson
Submitted
II Genetic variation in the ATP-binding Cassette Transporter gene ABCG2 in a Swedish population.
Gunilla Bäckström, Jan Taipalensuu, Håkan Melhus, Helena Bränd-ström, Ann-Catrin Svensson, Per Artursson and Andreas Kindmark
European Journal of Pharmaceutical Sciences 18 (2003) 359–364
III Association between the number of coadministered P-glycoprotein inhibitors and serum digoxin levels in patients on therapeutic drug monitoring.
Gunilla Englund, Pär Hallberg, Per Artursson, Karl Michaëlsson and Håkan Melhus BMC Medicine (2004) 2:8
IV Differential expression of ABC transporters in colonic and rectal mu-cosa during active and inactive phases of ulcerative colitis
Gunilla Englund, Annica Jacobson, Fredrik Rorsman, Per Artursson, Andreas Kindmark and Anders Rönnblom
In manuscript
Reprints were made with the permission of the journals.


Contents
Introduction...................................................................................................11People respond differently to the same drug treatment ............................11
Physiological factors............................................................................13Genetic factors .....................................................................................13Environmental factors..........................................................................15Pathological factors .............................................................................16
Intestinal drug absorption and disposition................................................17Absorption ...........................................................................................17Excretion and reabsorption ..................................................................18Metabolism ..........................................................................................18
Transport proteins – The big picture ........................................................20Transport proteins in drug absorption and disposition ........................21
The ABC transporters Pgp and BCRP .....................................................24P-glycoprotein ..........................................................................................25
Expression and physiological role .......................................................25Important substrates.............................................................................26Pgp in drug absorption and disposition ...............................................26Interindividual variability ....................................................................27
Breast Cancer Resistance Protein.............................................................28Expression and physiological role .......................................................28Important substrates.............................................................................29BCRP in drug absorption and disposition............................................29Interindividual variability ....................................................................30
Investigations ................................................................................................31Aims of the thesis .....................................................................................31Expression of transporters along the human intestine..............................32
Background for investigation I ............................................................32Methodology........................................................................................32Expression of drug transporters along the intestine.............................34Comparisons of human intestine and Caco-2 cells ..............................35
Identification of sequence variation in the ABCG2 gene .........................38Background for investigation II...........................................................38Methodology........................................................................................38Genetic variation in the ABCG2 gene..................................................39
The Pgp-digoxin interaction: Effects of multiple Pgp inhibitors .............42Background for investigation III .........................................................42Methodology........................................................................................42Patients and co-administered drugs .....................................................43S-digoxin levels in relation to administration of Pgp inhibitors ..........43
Expression of intestinal ABC transporters in patients with ulcerative colitis ........................................................................................................47
Background for investigation IV .........................................................47Methodology........................................................................................47Patients.................................................................................................48Mucosal expression of ABC transporters in ulcerative colitis.............49Correlation between ABC transporters and cytokines.........................49
Conclusions...................................................................................................52
Summary of results and perspectives............................................................53
Acknowledgements.......................................................................................54
References.....................................................................................................55

Abbreviations
A Adenine ABC ATP binding cassette ANOVA Analysis of variance ASA Acetylsalicylic acid ATP Adenosine triphosphate BCRP Breast cancer resistance protein C Cytosine Caco-2 Human colon adenocarcinoma cells clone 2 Ct Treshold cycle CYP Cytochrome P450 DHPLC Denaturing high-performance liquid chromatography DNA Deoxyribonucleic acid ENT Equilibrative nucleoside transporter G Guanine GLM General linear model IBD Inflammatory bowel disease IL Interleukin MCT Monocarboxylic acid transporter MDCK Madin Darby canine kidney cells MDR Multi-drug resistance MRP Multidrug resistance protein NTCP Sodium/taurocholate cotransporting polypeptide OATP Organic anion transporter OCT Organic cation transporter PCA Principal component analysis P-creatinine Plasma concentration of cretinine PEPT Oligopeptide transporter Pgp P-glycoprotein 170 RNA Ribonucleic acid RT-PCR Reverse transcription polymerase chain reaction S-Digoxin Serum concentration of digoxin SLC Solute carrier SNP Single nucleotide polymorphism T Thymine TDM Therapeutic drug monitoring UC Ulcerative colitis


11
Introduction
People respond differently to the same drug treatment It is well established that patients respond in different ways to the same medication. In many cases, the variability is quite substantial with significant clinical implications. The differences in response can lead to drug-associated toxicity in some patients and to therapeutic failure in others. Apart from the personal suffering involved this result in a large health care burden (1-3).
This variability in responsiveness to drugs originates from differences in the pharmacodynamics and pharmacokinetics of the drug between individu-als, as well as from clinical heterogeneity of the underlying disease. The pharmacodynamic profile of a drug reflects the interaction between the pharmacologically active substance and receptors. The pharmacokinetics of a drug describes the concentration of drug that reaches the target site (see Box 1). Clinical heterogeneity of disease results from differences in the un-derlying disease mechanisms, despite similarities in clinical symptoms. The therapeutic range of a drug determines whether interindividual differences in drug response will lead to clinically important consequences.
In current medical practice, patients commonly receive standardized drug dosages, regardless of concomitant therapies, disease, genetics or relevant physiological factors. Research into the biological mechanisms underlying interindividual variability aims to better identify patients with exceptional genetic traits, disease conditions or risk of drug-drug interactions.
Pharmacodynamic and pharmacokinetic variability can arise from physio-logical, pathological, genetic or environmental differences among individu-als (Fig. 1). Differences in renal function and metabolic processes are well established causes of variability. Recently, transport proteins have been sug-gested as a source of interindividual variability (4-7). In this thesis, transport proteins were investigated with the aim of identifying factors that could po-tentially contribute to interindividual variability in drug absorption and/or disposition. The focus of the thesis was on two transport proteins from the ATP-binding cassette (ABC) superfamily: P-glycoprotein (Pgp) and Breast Cancer Resistance Protein† (BCRP).
In this thesis, Pgp is used as abbreviation for P-glycoprotein 170. The gene symbol ABCB1,and the name MDR1 are also frequently used in the literature. † The name BCRP is used for Breast Cancer Resistance Protein throughout this thesis. The gene symbol ABCG2 and the names MXR and ABCP also occur in the literature.

12
Drug response
Environment
Pathology
Genetics
Physiology
Pharmacokinetics Pharmacodynamics
Drug response
Environment
Pathology
Genetics
Physiology
Pharmacokinetics Pharmacodynamics
Fig. 1. Physiological, pathological, genetic and environmental factors all contribute to variability in pharmacokinetics and pharmacodynamics of drugs, which in turn result in variability in drug response.
Box 1. Pharmacokinetics‡
The concentration of a drug in the body is commonly described by Cmax (the highest observed concentration in blood/plasma/serum) and the AUC (the Area Under the plasma drug Concentration-time curve). The therapeutic range is the concentration range within which the drug therapy is likely to be successful; that is, a concentration high enough to give the de-sired effect but low enough to avoid toxicity. The drug concen-tration in the body will depend on the absorption, distribution, and elimination of the drug. Distribution and elimination are in-cluded in the term disposition.Bioavailability (F) is the fraction of a given dose that becomes available to the systemic circulation. The distribution refers to the transfer of the drug between blood and tissues and is de-scribed by the volume of distribution (V). Elimination refers to the irreversible loss of drug from the body, and includes metabolism and excretion. Elimination is described in terms of clearance (Cl).
‡ All pharmacokinetic definitions were adapted from ref (8).

13
Physiological factors Physiological differences among individuals result from differences in fac-tors such as gender, age and body composition, but also less obvious pa-rameters such as blood flow, gastrointestinal motility and intrinsic hepatocel-lular activity. Variability in drug response due to age can arise from differ-ences in metabolic capacity. For instance, the new-born and infants have different levels of several cytochrome P450 enzymes (CYP450) from those seen in adults (9). Age-related variability in drug response can also originate from the normal decline in renal blood flow and glomerular filtration with age (10). Gender-related differences in pharmacokinetics of drugs can, apart from differences in body composition, arise from differences in gastric emp-tying and in metabolic capacity (11, 12). Gender-related variability in drug response has been suggested to be clinically important for instance in the treatment of human immunodeficiency virus (HIV) infection (11).
In the intestine, the dissolution (13) and absorption (14) of a drug across the intestinal mucosa are influenced by physiological differences in gastric pH, ventricle emptying rate, and gastrointestinal motility. The site of drug release and absorption along the intestine represents a source of interindi-vidual variability in cases where the drug absorption is affected by pH-sensitive degradation, by metabolism or by active transport of the drug by enzymes or transporters with region-dependent expression. Investigation I of this thesis describes the regional expression along the human intestine of nine transport proteins. For all of these, transport of substances used as therapeutic agents have been described (see Table 1, page 20).
Genetic factors The human genome is made up of approximately 3 billion base pairs (15) and differences in the DNA sequence among individuals are estimated to occur in approximately every 1000th base pair (see Box 2). Pharmacogenet-ics is defined as the relationship between genetic variations and individual differences in drug response. Sequence alterations in genes encoding drug targets, genes involved in drug absorption and disposition (such as phase I and phase II enzymes and transport proteins) or genes with indirect effects on drug response all contribute to pharmacogenetic differences in drug re-sponsiveness (17).
The terms pharmacogenetics and pharmacogenomics are sometimes used interchangeably but strictly, pharmacogenetics address specific genes, whereas pharmacogenomics refers to the functions and interactions of all genes in a genome. The genetic definitions in this thesis were adapted from ref (16).

14
Pharmacogenetic studies of metabolic enzymes have been performed since the 1950s and several examples with clinical implications have been described, including thiopurine S-methyl transferase, CYP2D6 and N-acetyltransferase 2 (18). The genetic component of the metabolism of caf-feine, oxazepam and dextromethorphan was estimated to vary between 20% and close to 100% (19). Adverse drug reactions have been reported to occur more often with drugs that are metabolized by polymorphic enzymes (20), which suggest that pharmacogenetics could be useful in avoiding adverse drug reactions. The first genetic study suggesting a role for transport proteins in drug disposition was published in 2000 (21). In this thesis (InvestigationII), genetic variations were identified in the gene encoding BCRP, which is the ABC transporter expressed at highest levels in the jejunum of the human intestine (22).
Box 2. Genetic variation A mutation is an alteration in the nucleotide sequence. This al-teration can occur as the result of insertion or deletion of one or a few nucleotides, or as the result of point mutations, where one nucleotide replaces another. The resulting alternative form of the gene is called an allele. A gene for which more than one allele is commonly found in a population is said to be polymorphic. Sin-gle nucleotide mutations are the most common type of genetic variations. When a single nucleotide sequence variation is com-mon in a population (occurs at a frequency of >1%) it is defined as a single nucleotide polymorphism (SNP).
Most mutations are silent, and will not have any effects on the function of the genome. A mutation that occurs in the coding re-gion of the DNA sequence can be synonymous (resulting in a codon specifying the same amino acid) or nonsynonymous (re-sulting in a codon that specifies a different amino acid).
Studies on genetic variation have focused on the association be-tween SNPs and certain phenotypes. It is now recognized that specific phenotypes are preferentially associated with combina-tions of SNPs which are inherited together (23), i.e. haplotypes.The likelihood of certain loci being inherited together is de-scribed by the linkage disequilibrium, which is the nonrandom association of alleles in a population at nearby loci.

15
Environmental factors Environmental factors such as concomitant drug treatment, diet (24), inges-tion of herbal remedies (25), smoking (26), and alcohol intake (27) may con-tribute to interindividual variability in drug response. Several clinically im-portant interactions between food constituents and drugs have been de-scribed, affecting such factors as gastrointestinal transit time and formation of poorly soluble complexes (24). More recently, the effects of diet on in-duction and inhibition of drug-metabolizing enzymes and transport proteins have been described (28, 29).
It is exceedingly common for patients to receive more than one drug con-comitantly. In an American survey, more than seven percent of randomly selected individuals over 18 years of age took at least five prescription drugs during a given week (30), and in a Danish study, close to fifty percent of individuals over 70 years of age used two or more prescription drugs con-comitantly (31). This implies a risk for drug-drug interactions (1) (see Box 3). As drug-drug interactions often can be prevented (3, 32), identification of the mechanisms behind the interactions is extremely important. A vast num-ber of interactions with transport proteins have been described in vitro, but their relevance in vivo is poorly evaluated in many cases. Investigation III of this thesis evaluated the effects of treatment with multiple drugs in patients receiving therapeutics that can cause Pgp-mediated drug-drug interactions.
Box 3. Drug-drug interactions The administration of one drug can alter the effects of a second drug, a phenomenon known as drug-drug interactions. Drug-drug interactions can arise at the pharmacodynamic or the phar-macokinetic level. Pharmacokinetic interactions can occur due to effects on absorption, distribution, metabolism, binding to plasma proteins and excretion. Some pharmacokinetic drug-drug interactions are mediated by transport proteins. When two drugs bind to the same drug bind-ing site competitive inhibition may arise. The affinity for the binding site and the concentration of drug will be important for the effects. Some drugs affect the expression of transport pro-teins (up-regulation or down-regulation), which may alter the pharmacokinetics of concomitantly taken drugs. Transporter-mediated drug-drug interactions may also arise from indirect ef-fects, such as inhibition of ATPase activity or effects on mem-brane fluidity.

16
Pathological factors The state of disease itself can alter drug absorption, disposition and response. The dosage of a drug often requires modification in patients with pathologi-calally reduced organ function, such as chronic liver disease (33) or renal failure (34). It is now recognized that not only the direct effects on renal function is affected by renal failure, but also various enzymes and transport proteins (35). Patients with congestive cardiac failure, thyroid disorders (8) or gastrointestinal disorders (36) may also require dose adjustments for some drugs.
Permeability of the intestinal mucosa may be influenced by several condi-tions, including inflammation, hypoxia and stress (37). Inflammation is a component of many disease states, and several potential mechanisms that could contribute to variability in drug disposition have been linked with this condition. For example, serum albumin levels and the metabolic capacity of some enzymes can be decreased during an inflammatory response (38, 39). Investigation IV of this thesis was undertaken to determine whether the lev-els of apically situated ABC transport proteins are altered during intestinal inflammation in patients suffering from ulcerative colitis.

17
Intestinal drug absorption and dispositionAbsorptionThe oral route is preferred for administering drugs since it is convenient and many drugs are well absorbed by the gastrointestinal tract. An orally admin-istered drug given as a solid dosage form such as a tablet has to disintegrate and dissolve in the gastrointestinal canal, permeate through the intestinal epithelium and via the portal vein pass through the liver in order to be avail-able in the systemic circulation (Fig. 2).
Gut lumen
Gut mucosa
Liver
Systemic circulation
Gastrointestinal transitDisintegrationDissolutionPrecipitationDegradation (chemical, bacterial)Complex formation
MetabolismEfflux
MetabolismBiliary excretion
Gut lumen
Gut mucosa
Liver
Systemic circulation
Gastrointestinal transitDisintegrationDissolutionPrecipitationDegradation (chemical, bacterial)Complex formation
MetabolismEfflux
MetabolismBiliary excretion
Fig. 2. Several processes in the gut lumen, the gut mucosa and the liver influence the bioavailability of orally administered drugs.
Absorption in the intestine is assisted by the large surface area of the intestinal epithelium, which is greatly enhanced by the folds, villi and microvilli structures (40). The permeability of the intestine to a specific drug will affect the rate and extent of its intestinal absorption. Molecules can permeate cellular membranes by the transcellular (across the cells) or paracellular (between the cells) routes (Fig. 3).
Drugs following the paracellular route move by passive diffusion, whereas those following the transcellular route move by passive diffusion or carrier-mediated transport. The transcellular route is far more relevant to the permeation of drugs than the paracellular route because of the strict limit to the size of molecules able to pass the tight junctions between the cells and also, paracellular pores constitute only 0.1% of the total small intestinal surface area (41). A paracellular component has however to be considered for some low-permeability compounds (42). A combination of routes is likely to be involved in the absorption process of a drug.

18
Apical (luminal) side
Basolateral side
Intestinal lumen
1 2 3
3
3
Apical (luminal) side
Basolateral side
Intestinal lumen
1 2 3
3
3
Fig. 3. The most important route for drug transfer across the intestinal epithelium is the passive transcellular route (1). The paracellular route is of importance for a lim-ited number of small molecules (2). Carrier-mediated transcellular routes (3) can increase or decrease the permeability across the intestinal epithelium, and have been described for several therapeutic agents.
Excretion and reabsorption The intestine is an absorptive organ with an important role in forming a se-lective barrier to xenobiotics. Although the intestine is not generally re-garded as one of the eliminatory organs, ejection of xenobiotics into the in-testinal lumen has been demonstrated, e.g. for the drugs talinolol (43), pacli-taxel (44), and digoxin (45).
Enterohepatic circulation, which refers to biliary excretion and reabsorp-tion by the intestine, is an important way for the body to avoid loss of bile acids (46). Certain drugs can also be recycled by this system, which is an advantage when prolongation of the pharmacologic effect is required (46). Enterohepatic circulation of drugs can also imply problems with toxicity, as in the examples of methotrexate and irinotecan, for which gastrointestinal toxicity has been suggested to be enhanced due to biliary excretion (47).
MetabolismMetabolism of drugs takes place predominantly in the liver, but also occurs in other tissues, including the intestinal mucosa (48). For example, CYP3A4 (49) and CYP3A5 (50), which are involved in the metabolism of many drugs, are expressed at significant levels in the small intestine. Along with other Phase I enzymes (51), several Phase II enzymes, such as glucuronyl-transferase, N-acetyltransferase, sulfotransferase and glutathione-S-transferase (52), are also expressed in the intestinal mucosa.

19
The importance of the intestine in drug metabolism in general is debatable (53), but metabolism in this organ seems to significantly affect the bioavail-ability of compounds such as midazolam (54) and saquinavir (55). Pgp and CYP3A4 are co-localized in the intestinal villi, and several drugs are sub-strates for both CYP3A4 and Pgp (56). CYP3A4 and Pgp have therefore been suggested to work cooperatively to limit the bioavailability of certain drugs (57).

20
Transport proteins – The big pictureProteins with a transport function constitute a significant fraction of the membrane-bound proteins in the human body: 533 of the 20 000 – 30 000 human genes are estimated to encode transport proteins or ion channels (15). The most extensively studied human membrane transporter, P-glycoprotein, was first described in 1976 (58) but a great deal of effort has gone into the identification of new transporters within the last ten years (59, 60). A stan-dardized nomenclature system for transporters has been recommended by the Human Gene Nomenclature Committee (http://www.gene.ucl.ac.uk/nomen-clature), but more than one name is still in use for many transporters.
Transport proteins can translocate substances across plasma membranes or across intracellular membranes such as nuclear membranes or membranes encapsulating organelles. Among the plasma membrane transporters, two families dominate: the ABC transporters and the solute carriers (SLC). The ABC transporters consist of proteins that bind ATP and utilize the energy to drive the transport of various compounds across membranes (61). For the SLC transporters the transport process can be facilitated diffusion or secon-dary active transport, where energy from ion gradients is used (62, 63). Transport proteins are important as carriers of endogenous substances and nutrients, but they also carry xenobiotics such as toxic agents and drugs. For examples of transport proteins suggested to be involved in transport of drugs, see Table 1.
Transport proteins can be studied using a variety of in vitro and in vivomethods (see (64) for a review, and Box 4, for a brief overview). The lack of specific substrates and inhibitors and the fact that metabolism and multiple transport proteins can be involved makes interpretation of the results more challenging (65, 66). When using cell models it is also important to note the discrepancies between transporter expression in the cell line and the mod-elled tissue (for a discussion on comparison between the human intestine and the Caco-2 cells, see Investigation I of this thesis).
Table 1. Examples of transport proteins with therapeutic agents as substrates. Note that substrates for Pgp and BCRP are described in separate tables (pages 26 and 29).
Gene Alias Examples of transported therapeutic agents
ABCC2 MRP2, cMOAT Ampicillin, grepafloxacin, methotrexate, vinblastine, ritonavir, pravastatin, acetaminophen
ABCC3 MRP3, cMOAT-2 Doxorubicin, vincristine, methotrexate, cisplatin, mor-phine-3-glucuronide
SLC15A1 PEPT1 Ampicillin, cefadroxil, captopril, enalapril, valacyclovir SLC16A1 MCT1 Benzoic acid, salicylic acid, pravastatin SLCO2B1 OATPB Bensylpenicillin, fexofenadine, estrone-3-sulfate SLC22A1 OCT1 Acyclovir, cimetidine, ganciclovir, metformin SLC22A5 OCTN2 Actinomycin D, cimetidine, quinidine, verapamil

21
Box 4. Overview of methods to study transport proteins
In vitro modelsCell lines such as Caco-2 and MDCK are commonly used in studies of drug transport (67). Transfected cell lines are often used for mechanistic studies of specific transporters. Studies of transport proteins in cells include experiments where transport across semi-permeable inserts is determined, studies of drug up-take into cells or membrane vesicles and studies of ATPase ac-tivity. In vitro studies of drug transport can also be performed on excised segments from animal or human tissues mounted in Ussing chambers. The limited access to tissues and the limited viability of the tissues has restricted the use of this method (68).
Animal models Animal studies, and in particular studies of transgenic animals or knock-out animals (69-71), have been important in furthering our understanding of the role of transport proteins in drug absorption and disposition. There are also mutant models, where the animals are naturally deficient in a certain transport protein. Nonetheless, species differences are likely to exist and compensatory mecha-nisms can develop in gene-modified animals.
Clinical trials Clinical trials are required to determine the pharmacokinetic properties of drugs and to investigate the relevance to humans of any drug-drug interactions observed in vitro or in animal models. Human intestinal perfusion models provide an opportunity to study intestinal permeation more directly (72).
Transport proteins in drug absorption and disposition A high level of expression of transport proteins is observed in organs with excretory functions (i.e. liver and kidney) and in tissues with barrier func-tions (i.e. intestine, blood-brain barrier, maternal-fetal barrier, blood-testis barrier). The transport proteins can thus influence the absorption, distribu-tion and excretion of drugs (4). The effects on plasma and tissue concentra-tions will depend on the direction of transport (efflux versus uptake) and the localization of the transport proteins in the cellular membranes (apical or basolateral localization).

22
AbsorptionIn the small intestinal and colonic epithelia, transport proteins mediate both absorptive and excretory functions (73). They act as carriers of amino acids, peptides, sugars, bile acids/salts, metal ions, vitamins, phosphate, nucleo-tides, cholesterol, lipids/phospholipids and xenobiotics. Uptake transporters increase the bioavailability of several drugs, including ACE-inhibitors (74) and some -lactam antibiotics (75). The uptake of these drugs is mediated by the SLC transporters PEPT1 and MCT1, respectively.
The intestine has an important role in forming a selective barrier to ab-sorption. As a part of this role, efflux transporters translocate their substrates back into the intestinal lumen. Pgp, BCRP, and the Multidrug Resistance Protein 2 (MRP2 ) (76-78) are efflux transporters with suggested roles in limiting drug absorption. Inhibition of efflux transporters, for instance by concomitantly administered drugs, can increase the bioavailability of orally administered drugs (4). Active efflux in the intestine is hypothesized to be of importance for absorption only for low permeable drugs (Class III and IV according to the Biopharmaceutics Classification System (79)). Furthermore, potential effects on absorption can only be expected when the drug is given at doses low enough not to saturate the transport system.
DistributionThe distribution of drugs to certain organs and tissues is also influenced by uptake and efflux transporters. The accumulation of a drug in a certain tissue can be either advantageous (e.g. in a target organ (80)), or disadvantageous (e.g. if it leads to tissue toxicity (47)). The restriction of a drug from a cer-tain tissue can also be advantageous (e.g. in avoiding tissue toxicity (81)), or disadvantageous (e.g. in the therapeutic failure of multi-drug resistant ma-lignancies (82)). It is important to observe that an alteration in the distribu-tion of a drug can affect its plasma concentration.
Excretion The main organs for drug elimination, the kidney and the liver, both express a wide range of transporters (83). In the kidney, transporters play a key role in the reabsorption and secretion of many endogenous and xenobiotic com-pounds. Transporters expressed in the human kidney include members of OAT, OATP, MRP, OCT, ENT and PEPT (84) from the SLC superfamily, and Pgp (85) and BCRP (86) from the ABC superfamily. Transporters ex-pressed in the human liver include members of OATP, OAT, OCT, the sol-ute carrier family 10 (including NTCP) and the ABC superfamily (87). Both uptake processes across the sinusoidal membrane and transport from the
In this thesis, MRP2 is used as the abbreviation for Multidrug Resistance Protein 2. The gene symbol is ABCC2, and the names Multidrug Resistance-associated Protein 2 and cana-licular multispecific organic anion transporter, cMOAT, are sometimes used in the literature.

23
hepatocyte into the bile via the canalicular membrane is of importance for hepatobiliar excretion of certain drugs.

24
The ABC transporters Pgp and BCRP At present, 48 human ABC transporters have been identified. However, only a few of these have been fully characterized with regard to physiological function. The ABC transporters have been phylogenetically divided into seven sub-families (ABCA through ABCG). From an evolutionary point of view, the ABC transporters are well conserved among vertebrates (88) but also among non-eukaryotic species (89), supporting their essential role. A number of monogenic diseases are related to mutations in ABC protein-encoding genes; these include Dubin-Johnson syndrome (mutations in the gene encoding MRP2 (90)), type 3 progressive familial intrahepatic choles-tasis (mutations in the gene encoding MDR3 (91)), Tangier disease (muta-tions in the gene encoding CERP (92)) and cystic fibrosis (mutations in the gene encoding CFTR (93)).
A well-known impeding factor in cancer treatment is the development of cross-resistance to other agents on the exposure to one cytotoxic drug. This phenomenon is known as multi-drug resistance (MDR), and is partly ex-plained by overexpression of ABC transporters (82). Both Pgp (58) and BCRP (60, 94, 95) were identified because of their role in transporting cyto-toxic agents in multi-drug resistant cancer cells. Much research has focused on the identification of substances which inhibit the function of Pgp (and more recently also BCRP), and thereby enable the chemotherapeutic treat-ment (96). For brief background data on Pgp and BCRP, see Table 2.
Table 2. Background data on Pgp and BCRP.
Pgp BCRP
Year of discovery 1976 1998 Year of cloning 1987 1998
Number of PubMed records* 9275 466 Number of substrates† 275 53
Chromosome localization 7q21 4q22 Number of exons 28 16
Gene size 100kb 66kb Amino acids 1280 655 Protein size 170 kDa 72 kDa
* PubMed seach for publications (not including reviews) October 7th 2005, search terms “P-glycoprotein 170 or ABCB1 or MDR1 or Pgp or P-gp” and “Breast Cancer Resistance Protein or BCRP or ABCG2 or MXR or ABCP” † According to a summary of a search on the Transporter Database (http://133.9.194.61/tp-search/, accessed October 2005) established by Dr Sugiyama et al, The University of Tokyo.
Pgp and BCRP are also expressed in numerous non-malignant tissues and there is an overlap in tissue localization of the two transporters. The overall amino acid homology between Pgp and BCRP is only around 20% but de-
25
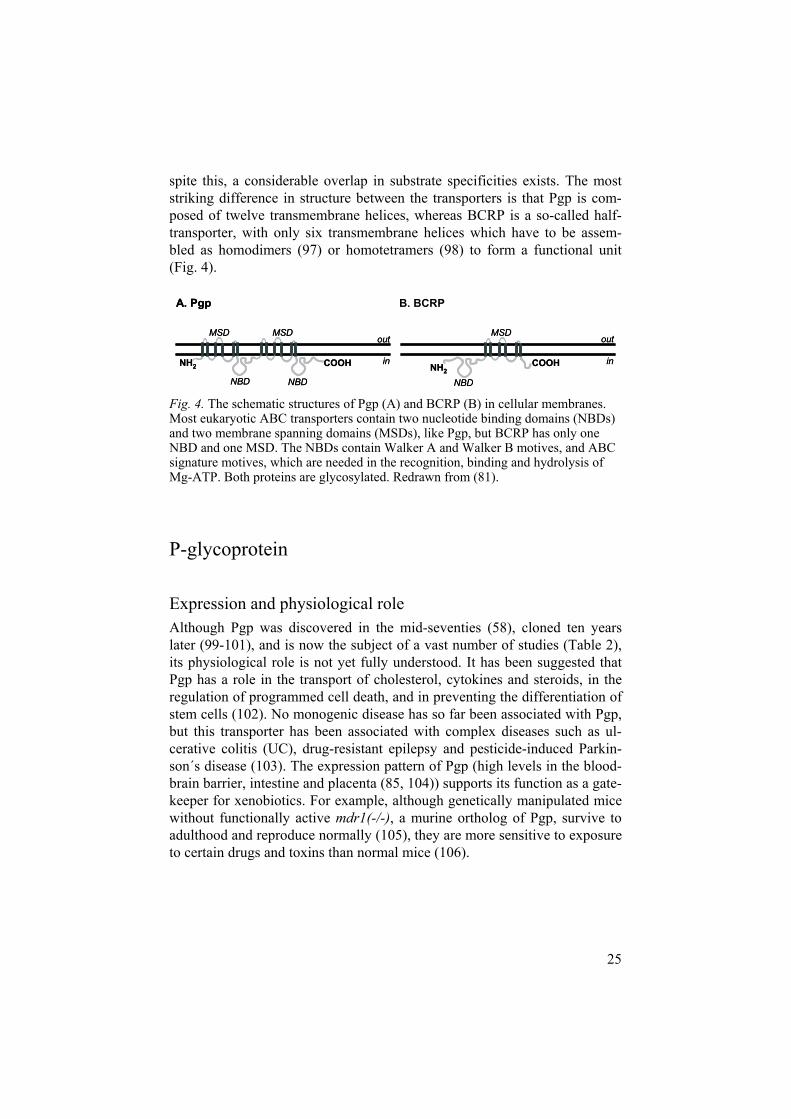
spite this, a considerable overlap in substrate specificities exists. The most striking difference in structure between the transporters is that Pgp is com-posed of twelve transmembrane helices, whereas BCRP is a so-called half-transporter, with only six transmembrane helices which have to be assem-bled as homodimers (97) or homotetramers (98) to form a functional unit (Fig. 4).
NH2COOH
out
in
NBD
MSD
NH2COOH
out
in
NBD
MSD
NH2 COOH
MSD MSD
NBD NBD
out
in
A. Pgp
NH2 COOH
MSD MSD
NBD NBD
out
in
A. Pgp B. BCRP
Fig. 4. The schematic structures of Pgp (A) and BCRP (B) in cellular membranes. Most eukaryotic ABC transporters contain two nucleotide binding domains (NBDs) and two membrane spanning domains (MSDs), like Pgp, but BCRP has only one NBD and one MSD. The NBDs contain Walker A and Walker B motives, and ABC signature motives, which are needed in the recognition, binding and hydrolysis of Mg-ATP. Both proteins are glycosylated. Redrawn from (81).
P-glycoprotein
Expression and physiological role Although Pgp was discovered in the mid-seventies (58), cloned ten years later (99-101), and is now the subject of a vast number of studies (Table 2), its physiological role is not yet fully understood. It has been suggested that Pgp has a role in the transport of cholesterol, cytokines and steroids, in the regulation of programmed cell death, and in preventing the differentiation of stem cells (102). No monogenic disease has so far been associated with Pgp, but this transporter has been associated with complex diseases such as ul-cerative colitis (UC), drug-resistant epilepsy and pesticide-induced Parkin-son´s disease (103). The expression pattern of Pgp (high levels in the blood-brain barrier, intestine and placenta (85, 104)) supports its function as a gate-keeper for xenobiotics. For example, although genetically manipulated mice without functionally active mdr1(-/-), a murine ortholog of Pgp, survive to adulthood and reproduce normally (105), they are more sensitive to exposure to certain drugs and toxins than normal mice (106).

26
Important substrates Pgp can transport a variety of structurally unrelated compounds, including amphipathic molecules that are neutral or weakly basic, and anionic charged compounds (107, 108). A vast number of therapeutic agents are substrates for Pgp. A brief overview of these is given in Table 3.
Table 3. Examples* of therapeutic agents transported by Pgp.
Substance class Substances
Analgesics Asimodaline, morhine, methadone Antiarrhythmics Quinidine Anticancer drugs Actinomycin D, daunorubicin, doxorubicin, etoposide, imatinib,
mitoxantrone, paclitaxel, tamoxifen, topotecan, vinblastine, vincristine
Antibiotics Clarithromycin, erythromycin, grepafloxacin, ketoconazole, rifampicin
Antidepressants Amitryptiline, clomipramine, fluoxetine Antiviral drugs Amprenavir, indinavir, nelfinavir, ritonavir, saquinavir Calcium channel blockers Diltiazem, nicardipine, nifedipine, nitrendipine, verapamil Cardiac glycosides Digoxin, digitoxin HMG-CoA reductase inhibitors
Atorvastatin, cerivastatin, pravastatin, simvastatin
Immunosuppressive drugs Cyclosporine A, tacrolimus Proton pump inhibitors Omeprazole, pantoprazole, Neuroleptics Chlorpromazine, haloperidol Steroids Dexamethasone, hydrocortisone, methylprednisolone,
prednisolone
* These examples were selected from the Transporter Database (http://133.9.194.61/tp-search/, accessed October 2005) established by Dr Sugiyama et al, The University of Tokyo.
Pgp in drug absorption and disposition In the early 1990s, the expression of Pgp in intestinal cell lines was demon-strated (109) and a role in limiting drug absorption was suggested (110). The effect of Pgp on the bioavailability of a number of drugs has now been dem-onstrated in both animal models and clinical trials. Animal studies, particu-larly those using mdr1(-/-) mice, provided good evidence for the involve-ment of Pgp in transport of certain drugs in the intestine (44, 111). The transport across the human intestinal mucosa of drugs such as digoxin (5, 45), cyclosporine A (7, 112) and talinolol (43, 113) appears to involve Pgp.
The significance of the effects of intestinal Pgp on drug absorption is con-troversial (114-116), and a more nuanced picture is now evolving (117), which takes into account the involvement of multiple transporters and meta-bolic enzymes as well as the varying of contributions of passive and Pgp-mediated permeation of the intestinal mucosa. The isolated effects of intesti-

27
nal transport proteins on drug absorption and bioavailability are difficult to determine in vivo, because of the interplay between metabolic enzymes and transporters (118), and due to difficulties in differentiating effects in the liver from those in the intestine (55). The expression of Pgp in the biliary cana-licular membrane of the hepatocytes makes Pgp important also in the secre-tion of drugs into bile (70, 111).
In some cases, Pgp efflux will counteract drug therapy by restricting the entrance of drugs to certain compartments, as established with cancer treat-ment (119) and suspected with HIV treatment (120). Pgp is expressed at high levels in the luminal membrane of the endothelial cells of the brain (121) where it has an important role in limiting toxicity and unwanted central nervous effects. The early experiments in mdr1(-/-) mice clearly demon-strated the protective role of Pgp in the blood-brain barrier (70), as the levels of ivermectin in the brain were approximately 100-fold higher in mice with-out functioning mdr1. In humans, an illustrative example of the action of Pgp in the blood-brain barrier is that of the interaction between loperamide and the Pgp inhibitor quinidine. Loperamide is an opioide, but is used clini-cally as an antidiarrheal because of the low concentration that reaches the brain. However, when Pgp efflux was inhibited, classical central nervous opioid effects resulted (122). Pgp also plays a protective role in other organs, including protection of the fetus against toxic agents (123).
Interindividual variability It has been suggested that Pgp significantly contributes to interindividual variability in drug bioavailability (7, 124). Age (125) and smoking (126) seem to be of minor importance for variability in Pgp expression, whereas dietary constituents (127), concomitant treatment with drugs and herbal remedies (128, 129), genetic variation (103) and certain disease conditions including inflammation (130), contribute to variability in Pgp expression and/or function. Differences in Pgp expression have also been suggested to be affected by gender (131, 132).
A number of drug-drug interactions, several of which are clinically im-portant, have been attributed to the actions of Pgp. The interactions between digoxin and quinidine (133), rifampin and digoxin (5), talinolol and digoxin (134), clarithromycin and digoxin (135), rifampin and talinolol (136), and rifampin and tacrolimus (137) are all suggested to be mediated by Pgp. Drug-drug interactions involving Pgp are assumed to be quantitatively more important at the blood-brain barrier as compared to the intestine, due to the large concentration gradient between the intestinal lumen and the circulating blood, and due to saturation of intestinal transporters on exposure of high concentrations of the drug in the intestinal lumen (138). Interactions between

28
intestinal Pgp and herbal remedies such as St John´s wort (128, 129) and between Pgp and food constituents such as grapefruit juice, green tea and rosemary extract have also been described (127).
In 2000, Hoffmeyer et al. reported genetic variations in the ABCB1 gene, and the association between a synonymous mutation in exon 26 (C3435T) and changes in digoxin plasma concentration (21). Numerous investigations of genetic variations in ABCB1 and their clinical consequences have been published. However, the impact of ABCB1 polymorphisms remains contro-versial (for a review on the functional implications of genetic variation in ABCB1, see (103)). Whereas some studies attribute effects on digoxin bioavailability (21), efficacy of HIV treatment (120) and the AUC of cyc-losporine (139) to a certain ABCB1 genotype, others show no association between sequence variations in ABCB1 and the pharmacokinetics of Pgp substrates (140-142).
Breast Cancer Resistance Protein
Expression and physiological roleBCRP has been detected in a large number of hematological malignancies and solid tumors, from which it effluxes cytotoxic agents and contributes to multi-drug resistance (143). BCRP is also found in the epithelial cells of the intestine, in placental syncytiotrophoblasts, in bile canalicular membranes (144), in the luminal surface of microvessel endothelia in the brain (145) and in the ducts and lobules of the breast (146). In contrast to most other half-transporters, which are expressed in intracellular membranes, BCRP is ex-pressed in the plasma membrane (147). In the intestine, BCRP is apically expressed, and it was therefore hypothesized that it would affect drug per-meability in a similar manner to that of Pgp (144).
A handful of endogenous substrates for BCRP have been identified: es-trone-3-sulfate, 17 -estradiol sulfate, 17 -estradiol 17-( -D-glucuronide)(148), folic acid (149) and protoporphyrin IX (150). However, as with Pgp the physiological role of BCRP is unclear. Its expression pattern in organs with a barrier function suggests a role in tissue defense (81). Similarly, its high expression in stem cells from various tissues indicates a role in cell differentiation (151). A physiological role in folate hemostasis (149) and in heme homeostasis (152) has also been suggested. No monogenic disease has yet been associated with BCRP. While Abcg2(-/-) mice survive to adulthood and reproduce normally in the absence of exposure to toxins (69, 71), they are more susceptible to toxins than normal mice (69, 153). These mouse strains show for instance enhanced sensitivity to dietary toxins and develop

29
phototoxic reactions on exposure to the chlorophyll-breakdown product pheophorbide (69).
Important substrates BCRP transports a variety of substances, although far fewer potential sub-strates have been investigated for BCRP than for Pgp. BCRP substrates in-clude molecules of either negative or positive charge, organic anions and conjugates of sulfate and glucuronide (154). Therapeutic agents transported by BCRP have mainly been identified among antitumor drugs (Table 4).
Table 4 Examples* of therapeutic agents transported by BCRP.
Substance class Substance
1-adrenoreceptor antagonists Prazosin Antibiotics Nitrofurantoin (155) Anticancer drugs Actinomycin D, daunorubicin, doxorubicin, etoposide,
flavopiridol, imatinib, irinotecan, methotrexate, mitoxan-trone, SN-38, tamoxifen, topotecan
Antiviral drugs Lamivudine HMG-CoA reductase inhibitors Cerivastatin, pitavastatin (156), pravastatin H2-receptor antagonist Cimetidine (157) Steroids Estradiol, estrone-3-sulfate, testosterone
* These examples were adapted from the Transporter Database (http://133.9.194.61/tp-search/, accessed October 2005) established by Dr Sugiyama et al, The University of Tokyo, where otherwise not noted. For additional sources, see the indicated references.
BCRP in drug absorption and disposition Effects of BCRP in drug absorption and disposition have been described in the intestine, the placenta, the liver, the blood-brain barrier and the mam-mary glands.
In mice, the bioavailability of topotecan was substantially increased and the hepatobiliary excretion was reduced upon inhibition of Bcrp1, the murine ortholog of human BCRP (77), and the oral bioavailability of the glycopro-tein IIb/IIIa antagonist ME3277 was limited by Bcrp1-mediated efflux in the intestine (158). Similarly, in humans, the oral bioavailability of topotecan increased when it was co-administered with GF120918, which is an inhibitor of both Pgp and BCRP (6). Bcrp1 is also involved in the excretion of the antibiotic nitrofurantoin into bile (155) and the accumulation of the 3-hydroxymethylglutaryl coenzyme A reductase inhibitor pitavastatin in bile (156). In these cases, the accumulation into bile was suggested to be advan-tageous for the therapeutic effects of these drugs.
The consequences of BCRP expression at the blood-brain barrier are not clear. BCRP seems to have little effect on the transport of the well character-ized BCRP substrate mitoxantrone across the blood-brain barrier (159), but

30
may affect penetration of the tyrosine kinase inhibitor imatinib into the brain (160). In the placenta, high expression of BCRP limits the penetration of its substrates into the fetus, as shown by the doubling of topotecan exposure in mice fetuses upon Bcrp1 inhibition (77). BCRP is expressed at high levels in mammary glands. Surprisingly, the localization of BCRP in mammary glands results in secretion of the BCRP substrates into milk, which is con-trary to its otherwise protective functions. In this way, the dietary carcino-gens aflatoxin B1 (153) and 2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine (PhIP) (146) and the drugs topotecan, cimetidine (146) and nitro-furantoin (155) are accumulated in milk.
Interindividual variability Because of its wide distribution in the body and its numerous functions, in-terest in determining genetic variation in the gene encoding BCRP, ABCG2,has been extensive. BCRP has been systematically screened for SNPs in different ethnic populations, including that described in Investigation II of this thesis, and more than 80 naturally occuring sequence variations have been described (161). Recent evaluations of possible associations between genetic variation in ABCG2 and drug absorption and disposition indicate that the bioavailability of topotecan (162) and the pharmacokinetics of diflo-motecan (163) and irinotecan (164) are associated with ABCG2 genotype.
BCRP has been suggested as a mechanistic explanation to the drug-drug interaction between methotrexate and pantoprazole or omeprazole (165). In cancer therapy, the pharmacokinetic drug-drug interaction between gefitinib and irinotecan, which is mediated by BCRP, has been suggested as a poten-tial strategy to increase the oral bioavailability of the poorly absorbed iri-notecan (166). Clinical trials are needed to confirm the role of BCRP in drug-drug interactions, and in vitro screens to identify BCRP substrates and inhibitors are warranted not only to identify chemosensitizers for combina-tion therapy in cancer treatment, but also to identify potential BCRP-mediated drug-drug interactions.
Food-drug interactions involving BCRP are conceivable, as BCRP trans-ports dietary derivatives such as glucuronidated forms of the flavonoid quercetin (167). However, the effects of food constituents on BCRP expres-sion or function are still to be evaluated in humans. The expression of BCRP is increased in mammary gland epithelium during late pregnancy and lacta-tion (146), which indicates some hormonal component in the regulation of BCRP. Gender differences in BCRP expression have also been suggested, after observations of higher BCRP expression in the liver for males (168). Expression of placental BCRP does not appear to be affected by smoking (126). The effects of disease on BCRP expression have not yet been evalu-ated. Investigation IV of this thesis was therefore performed in order to de-termine whether inflammatory conditions affect the expression of BCRP.

31
Investigations
Aims of the thesis The overall aim of this thesis was to identify factors affecting transport pro-teins which could contribute to variability in drug response. More specifi-cally, the goals were:
1. To determine the regional expression and co-localization of transport proteins, of known or potential importance for drug transport, along the human intestine. The aim was also to describe similarities and differ-ences in the expression of transporters between the commonly used invitro model Caco-2 and various regions of the human intestine.
2. To identify genetic variation in the gene encoding BCRP. 3. To evaluate a transporter-mediated drug interaction, namely the interac-
tion between Pgp and digoxin, in a clinical setting and to determine the effects of treatment with multiple Pgp inhibitors.
4. To investigate whether the expression of apically situated ABC trans-porters in the human intestine is affected by an inflammatory process, in this case ulcerative colitis.

32
Investigation I:
Expression of transporters along the human intestine
Background for investigation I The site of absorption of a drug can result in interindividual variability in bioavailability if the membrane permeability to that drug depends on carrier-mediated transport. Investigationr I of this thesis was undertaken to quantify the expression levels of nine transport proteins, known to transport drugs, along the human intestine. The levels of the ABC transporters Pgp, BCRP, MRP2, MRP3 and the SLC transporters PEPT1, MCT1, OATPB, OCTN2, and OCT1 were determined in human duodenum, ileum, jejunum and colon. The co-localization of multiple transporters is important to determine, as it is recognized that more than one transport protein often contribute to the net flux (66, 169). Investigation I also describes discrepancies and similarities in the expression of transporters between the most commonly used cell model in drug permeability screening, Caco-2 (170), and the human intestine, in-formation that is important for the interpretation of results from Caco-2 cells.
Methodology
Tissues and cells Biopsies from the duodenum, ileum and colon were obtained from 14 volun-teers (12 females and 2 males). Biopsies from these three intestinal locations were sampled from each individual during a single medical session. As the jejunum is an important region for drug absorption, the levels of transport proteins were also determined in this intestinal region in biopsies from 5 individuals undergoing right-sided hemicolectomy (for ethical and practical reasons, these could not be sampled from the same individuals offering duo-denal, ileal and colonic biopsies). Tissue samples with signs of inflammation or malignancy were excluded. Information on gender, age, concomitant drug treatment and disease was recorded. The study was approved by the Ethical Committee of the Medical Faculty, Uppsala University.
Caco-2 cells (American Tissue Culture Collection, VA, USA) were cul-tured as described elsewhere (67). Cells cultured on membrane inserts for 4, 14 and 21 days were investigated, as these culturing times are commonly used in transport experiments.

33
mRNA expression analysis All cells and tissues where kept in RNALater (Qiagen, Germany) until isola-tion of RNA with the RNeasy Mini kit (Qiagen) in accordance with the in-structions from the supplier, including DNase treatment. High RNA quality was confirmed for all samples using a Bioanalyzer 3000 (Agilent, CA, USA). RNA concentrations were determined using Nanodrop ND-1000 (NanoDrop Technologies, DE, USA).
Reverse transcription was performed for 1 µg of RNA using a cDNA High Capacity Archive kit (Applied Biosystems, CA, USA) and random hexamers as primers. Quantitative PCR was performed on an SDS 7000 system from Applied Biosystems using a Universal MasterMix (Applied Biosystems). The PCR conditions were 10 min at 95°C followed by 40 cy-cles of 15 s at 95°C and 1 min at 60°C. All assays were RNA-specific (span-ning exon-exon junctions) pre-designed TaqMan Gene Expression Assays from Applied Biosystems. Each TaqMan reaction was performed in tripli-cate, using 5,000 pg of RNA converted to cDNA in each well. Close to 100% PCR efficiency was confirmed for all transporters. 18S was selected as an internal reference for normalization of the input of the cDNA template (TaqMan Pre-Developed Assay Reagents, Applied Biosystems). Villin was used as a marker for differentiated enterocytes (171) and Musashi-1 was used as a marker for undifferentiated enterocytes (172), to ensure that the biopsies were comparable with respect to the content of epithelial cells.
Calculations and statistical considerations The relative transcript levels were determined using the comparative Ct method (the Ct method) or the relative standard curve method. Kruskal-Wallis tests followed by calculations of post-hoc probabilities for a two-sided test of significance were performed to determine whether the 18S-normalized expression levels (as Ct values) in the duodenum or colon dif-fered from those in the ileum. Probability values of less than 0.05 were con-sidered statistically significant. The statistical analysis was performed using Statistica 7.0 (StatSoft Scandinavia AB, Uppsala, Sweden). This comparison did not include the jejunum, as the jejunal biopsies were obtained from dif-ferent individuals and the assays were run on a separate occasion.
The differences in 18S-normalized expression levels between Caco-2 cells (4, 14 and 21 days on filter inserts) and the human duodenum, ileum and colon were determined. Principal Component Analysis (PCA) was per-formed to overview the similarities in transporter expression between Caco-2 cells and the human intestine, and the results are presented as score plots of the three significant principal components (t[1], t[2] and t[3]).

34
Expression of drug transporters along the intestine BCRP was the most prevalent ABC transporter transcript in all four regions of the human intestine (Fig. 5). Of the SLC transporters, PEPT1 was the most prevalent in the small intestinal regions, whereas MCT1 was the most prevalent in the colon (Fig. 5). The rank order of transcript prevalence was identical in the jejunum and the ileum (Fig. 5), which is an important obser-vation as the ileum is far easier to access.
0
0.5
1
1.5
2
MC
T1BC
RP
OC
TN2
Pgp
MR
P3O
ATPB
PEPT
1O
CT1
MR
P2
0
0.5
1
1.5
2
BCR
PPE
PT1
OC
TN2
Pgp
MC
T1M
RP2
MR
P3O
ATPB
OC
T1
0
0.5
1
1.5
2
2.5
3
3.5
BCR
PPg
pPE
PT1
OC
TN2
MR
P2O
ATPB
MC
T1M
RP3
OC
T1
0
0.5
1
1.5
2
2.5
BCR
P
Pgp
PEPT
1O
CTN
2M
RP2
OAT
PBM
CT1
MR
P3O
CT1
Expr
essi
on re
lativ
e to
vill
in
B. Jejunum
Expr
essi
on re
lativ
e to
vill
in
C. Ileum
A. Duodenum
Expr
essi
on re
lativ
e to
vill
in
D. Colon
Expr
essi
on re
lativ
e to
vill
in
0
0.5
1
1.5
2
MC
T1BC
RP
OC
TN2
Pgp
MR
P3O
ATPB
PEPT
1O
CT1
MR
P2
0
0.5
1
1.5
2
BCR
PPE
PT1
OC
TN2
Pgp
MC
T1M
RP2
MR
P3O
ATPB
OC
T1
0
0.5
1
1.5
2
2.5
3
3.5
BCR
P
Pgp
PEPT
1O
CTN
2M
RP2
OAT
PBM
CT1
MR
P3O
CT1
0
0.5
1
1.5
2
2.5
BCR
P
Pgp
PEPT
1O
CTN
2M
RP2
OAT
PBM
CT1
MR
P3O
CT1
Expr
essi
on re
lativ
e to
vill
in
B. Jejunum
Expr
essi
on re
lativ
e to
vill
in
C. Ileum
A. Duodenum
Expr
essi
on re
lativ
e to
vill
in
D. Colon
Expr
essi
on re
lativ
e to
vill
in
Fig. 5. Transcript prevalence (as an average of the transporter expression relative to the levels of the epithelial marker villin + SEM) of transporters in the human duode-num (A), jejunum (B), ileum (C) and colon (D). The transporters are arranged ac-cording to prevalence. Observe that the villin levels vary along the intestine, so that comparisons of expression levels relative to villin between the small intestine and colon should be avoided.
The expression of eight of the nine investigated transporters differed de-pending on the region of the intestine (Fig. 6). The only transporter for which no significant differences were observed between the different regions was OATPB. The expression of Pgp, BCRP, OCTN2 and MCT1 differed within the small intestine, but the differences were greater than 5-fold only

35
for Pgp. The expression of seven transcripts differed between the ileum and colon (Fig. 6). The most pronounced variation in regional expression was observed for MRP2 and PEPT1, with approximately 100-fold lower levels in the colon, and for MCT1, with 10-fold higher levels in the colon.
The interindividual variability in expression was fairly low in this study. Generally, the differences in transcript levels when comparing the individu-als with the highest versus lowest transcript levels were 2- to 5-fold. This is far lower than the reported variability of up to 65-fold in Pgp mRNA expres-sion (21) and 78-fold for BCRP (173).
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
0.0 0.5 1.0 1.5 2.0
Duodenum
Ileum
Colon
0.0 1.0 2.0 3.0 4.0
Duodenum
Ileum
Colon
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
OCTN2
MRP3
OATPB
Pgp
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
BCRP
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
PEPT1
0.0 0.5 1.0 1.5 2.0 2.5
Duodenum
Ileum
Colon
MRP2
0.0 0.5 1.0 1.5 2.0 2.5
Duodenum
Ileum
Colon
OCT1
0 5 10 15 20
Duodenum
Ileum
Colon
MCT1
**
***
***
***
***
***
***
*
**
**
*
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
0.0 0.5 1.0 1.5 2.0
Duodenum
Ileum
Colon
0.0 1.0 2.0 3.0 4.0
Duodenum
Ileum
Colon
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
OCTN2
MRP3
OATPB
Pgp
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
BCRP
0.0 0.5 1.0 1.5
Duodenum
Ileum
Colon
PEPT1
0.0 0.5 1.0 1.5 2.0 2.5
Duodenum
Ileum
Colon
MRP2
0.0 0.5 1.0 1.5 2.0 2.5
Duodenum
Ileum
Colon
OCT1
0 5 10 15 20
Duodenum
Ileum
Colon
MCT1
**
***
***
***
***
***
***
*
**
**
*
Fig. 6. The average values (calculated for 13-14 individuals) and standard deviations (SD) of regional expression levels relative to those in the ileum. OATPB was the only transporter with no significant differences between expression in the duode-num, ileum and colon. Transcript levels that were significantly different from the level in the ileum are indicated by * (p < 0.05), ** (p < 0.01) or *** (p < 0.001).
Comparisons of human intestine and Caco-2 cells In the comparison of human ileum and Caco-2 cells, greater than 5-fold dif-ferences were seen in the expression of OATPB (20-fold higher in Caco-2), BCRP (20-fold lower in Caco-2) and MRP2 (8-fold higher in Caco-2). It is important to consider these discrepancies if misinterpretation of permeability results from the Caco-2 model are to be avoided. In the estimation of simi-larity between Caco-2 cells and the human intestinal regions (Fig. 7), the

36
greatest similariteis were observed between the small intestinal segments and Caco-2, due to the greater similarity between Caco-2 and the small intestine in principal component 1, which explained 68% of the variation.
DuodenumIleumColonCaco-2 day 4Caco-2 day 14Caco-2 day 21
-6
-4
-2
0
2
4
6
-12 -10 -8 -6 -4 -2 0 2 4 6 8 10 12
t[2]
t[1]
-3
-2
-1
0
1
2
3
4
-12 -10 -8 -6 -4 -2 0 2 4 6 8 10 12
t[3]
t[1]
-3
-2
-1
0
1
2
3
4
-7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7
t[3]
t[2]
DuodenumIleumColonCaco-2 day 4Caco-2 day 14Caco-2 day 21
-6
-4
-2
0
2
4
6
-12 -10 -8 -6 -4 -2 0 2 4 6 8 10 12
t[2]
t[1]
-3
-2
-1
0
1
2
3
4
-12 -10 -8 -6 -4 -2 0 2 4 6 8 10 12
t[3]
t[1]
DuodenumIleumColonCaco-2 day 4Caco-2 day 14Caco-2 day 21
DuodenumIleumColonCaco-2 day 4Caco-2 day 14Caco-2 day 21
DuodenumIleumColonCaco-2 day 4Caco-2 day 14Caco-2 day 21
-6
-4
-2
0
2
4
6
-12 -10 -8 -6 -4 -2 0 2 4 6 8 10 12
t[2]
t[1]
-3
-2
-1
0
1
2
3
4
-12 -10 -8 -6 -4 -2 0 2 4 6 8 10 12
t[3]
t[1]
-3
-2
-1
0
1
2
3
4
-7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7
t[3]
t[2]
Fig. 7. The human intestinal regions (open symbols) the Caco-2 cells (closed sym-bols) were distinguishable by principal component analysis of the expression data. The principal component 1, t[1], explained 68% of the variation, and was dependent mainly on the expression of MRP2 and PEPT1. The second principal component, t[2], explained 22% of the variation and was dependent on OATPB and BCRP ex-pression, and principal component 3, t[3], explained only 5% of the variation and was primarily dependent on the expression of Pgp.
In order to study nine transporters in the limited tissue samples available from the volunteers, it was not possible to verify the results of this study on protein or functional levels. A clear relationship between mRNA and func-tionality exists for Pgp (174) and for PEPT1 (175), but the relationship is still to be established for several other transporters.
In conclusion, the expression of drug transporters along the intestine var-ied according to the intestinal region, although the levels within the small intestine were comparable for the majority of the investigated transporters. Pgp and BCRP had a similar distribution pattern along the intestine, with the highest levels in the proximal small intestine, and both Pgp and BCRP ex-

37
hibited statistically significant differences between the duodenum and the ileum, and between the ileum and the colon. As the combination of ex-pressed transporters is dependent on the region of the intestine, the effects of drug-drug interactions may vary depending on the site of absorption.

38
Investigation II:
Identification of sequence variation in the ABCG2 gene
Background for investigation II The hypothesis that genetic variation in the gene encoding BCRP, ABCG2,could be associated with variability in drug absorption and/or disposition in a similar way as suggested for Pgp, initiated study II of this thesis. This study aimed to identify genetic variation in the ABCG2 gene. At the onset of the study, no information regarding genetic variation in ABCG2 had been re-ported.
Methodology
Blood samples and DNA preparation Blood samples were obtained from 60 Swedish individuals who had served as controls in an independent study (176). DNA was isolated using the QIAamp DNA Blood Mini Kit (VWR International, PA, USA).
Identification of sequence variation Primer pairs (Interactiva, Germany) were designed to cover the coding re-gions, intron/exon boundaries and the 5´flanking (approximately 1000 base pairs and 3´flanking (approximately 600 base pairs) regions of the ABCG2 gene. PCR was performed using the ProofStart kit (VWR International, PA, USA) and a GeneAmp PCR system 9700 thermal cycler (Applied Biosys-tems, CA, USA). Prior to DHPLC screening, DNA from four individuals was pooled to allow for identification of individuals homozygous for rare alleles. For DHPLC screening, a Transgenomic WAVE system (Transge-nomic, NE, USA) was used under routine conditions (177). The tempera-tures for partial denaturation (Tm) were calculated using WAVEmaker ver-sion 4.0 and the Stanford algorithm (available from http://insertion.stanford.edu)) and confirmed empirically. When necessary because of non-uniform melting, two temperatures were selected for the screening.
Direct sequencing, using a Big Dye Terminator Cycle Sequencing kit (Applied Biosystems) and an ABI Prism 377 DNA Sequencer (Applied Biosystems), was performed for DNA in DHPLC pools where sequence differences were observed. For sequence alignment and amino acid sequence prediction, Sequence navigator (Applied Biosystems) and Strider 1.1 (178) were used. Each identified polymorphism was confirmed by cloning and dye

39
primer sequencing. Genotyping of the g.-19572_-19568delCTCA deletion was performed by electrophoresis on a 6% polyacrylamide gel, using an ABI 377 sequenator (Applied Biosystems) and data analysis was performed using GeneScan Analysis 3.1 and Genotyper 2.0 (Applied Biosystems). Allele frequencies of the sequence variations g.34G.A, g.8825C.A and g.-19202G.C were determined by direct sequencing using a 310 ABI Prism DNA Sequencer (Applied Biosystems).
StatisticsTests for Hardy–Weinberg equilibrium and linkage analysis were performed using Arlequin ver. 2.000 (179). Briefly, the haplotypic composition of the sample was estimated, and the linkage disequilibrium between a pair of loci was tested for using a likelihood-ratio test whose empirical distribution was obtained by a permutation procedure.
Genetic variation in the ABCG2 gene Eight sites of genetic variation were identified (see Table 5 and Fig. 8). The genetic variations speculated to be of greatest interest for future pharmaco-genetic studies were a CTCA deletion (g.-19572_-19569delCTCA) situated in the 5´flanking region, a G>C transversion (g.-19202G>C) in a CpG island region in the ABCG2 promotor, and non-synonymous alterations in exon two (g.34G>A) and in exon five (g.8825C>A, this sequence variation is now usually referred to as 421C>A) which result in amino acid changes of valine to methionine and glutamine to lysine, respectively.
Table 5. Identified sequence variation in the ABCG2 gene.
IDa Nucleotide sequence (5’ to 3’) Ref. sequenceb Alteration
AffectedDHPLC poolsc
Consequence
g.-19572_-19569 delCTCA
actcaCTCAcaaag actca____caaag 15 5’ flanking deletion
g.-19202G>C gtactGatcag gtactCatcag 5 CpG island SNP
g.-18845T>C tgagcTcgtcc tgagcCcgtcc 8 5’UTR SNP
g.-18604delA cggcaAggagg cggca_ggagg 1 5’UTR deletion
g.34G>A tcccaGtgtca tcccaAtgtca 2 Missense SNP Val12Met
g.8007G>A ttggaGggaaa ttggaAggaaa 3 Intronic SNP
g.8825C>A acttaCagttc acttaAagttc 4 Missense SNP Gln141Lys
g.44997G>A ttcttAaaatt ttcttGaaatt 9 Intronic SNP
a Sequence variantion ID in accordance with the nomenclature for sequence variation described at http://www.dmd.nl/mutnomen.html. b The reference sequence was defined as the genomic sequence deposited in GenBank with accession no. AC084732. Base one was defined as the “A” in the ATG-translation initiation of the ABCG2 gene. c The number of affected DNA pools out of a total of 15 pools. The number of affected DHPLC pools gives an indication of the mutation frequency.

40
In early studies of BCRP, it was noted that some drug-selected human (180) or murine (181) cell lines were resistant to doxorubicin and could transport the fluorescent dye rhodamine 123 while others could not. The source of this discrepancy was identified as a single nucleotide mutation in exon twelve, which led to an amino acid change in position 482 from argin-ine to threonine, glycine, methionine or serine. It was of particular interest to determine whether this variant commonly occurred in a healthy population, but this sequence variation was not observed in the studied population.
g.-19572_-19568delCTCAg.-19202G>Cg.-18845T>C
g.-18604delA g.34G>Ag.8007G>A
g.8825C>A
Translation start Walker A
Walker B TM 1, 2 TM 3, 4 TM 5, 6
g.44997G>A
g.-19572_-19568delCTCAg.-19202G>Cg.-18845T>C
g.-18604delA g.34G>Ag.8007G>A
g.8825C>A
Translation start Walker A
Walker B TM 1, 2 TM 3, 4 TM 5, 6
g.44997G>A
Fig. 8. Identified sequence variation in the ABCG2 gene. Black lines indicate in-tronic regions and white boxes the 16 exonic regions. Text in italics describes im-portant features encoded by the exons. TM indicates that the exon encode a trans-membrane region. Sequence variations that now have been associated with pharma-cokinetic parameters are indicated in bold.
The allele frequencies were determined for the sequence variation consid-ered to be most likely to affect BCRP expression or function. The deletion of CTCA was the more common allele in the studied population, occurring at a frequency of 54%. Of the single nucleotide variations, the G>C transversion in the CpG island occurred at a frequency of 5%, the G>A transition (Val12Met) at 2% and the C>A (Gln141Lys) transversion at 10%. Linkage disequilibrium was observed over the region between the CTCA deletion and the 421C>A (Gln141Lys) variation.
A number of studies have now been carried out to identify genetic varia-tions in ABCG2 (for a review, see (161)). Evaluation of the functional con-sequences of the sequence variation has revealed that the mRNA expression of BCRP is reduced for the 421C>A (Gln141Lys) variation (162, 182). Re-cently, studies linking genetic variation in ABCG2 to altered drug absorption and/or disposition have been performed. The 421C>A (Gln141Lys) variation has been associated with elevated plasma levels of the topoisomerase I in-hibitor diflomotecan after intravenous administration (163) and, in a pre-liminary study, has been associated with increased bioavailability of the

41
topoisomerase I inhibitor topotecan after oral administration (162). Pharma-cokinetic parameters for irinotecan and its metabolite SN-38 have been asso-ciated with the CTCA deletion (164), although no association between ABCG2 sequence variation and the pharmacokinetic parameters of SN-38 was observed in another investigation (183). Also, evaluation of ABCG2genotype in relation to pharmacokinetic parameters of the protease inhibitor nelfinavir revealed no apparent association (184).
In conclusion, genetic variations were identified in the ABCG2 gene. In recent studies some of these have been associated with interindividual vari-ability in drug absorption and/or disposition.

42
Investigation III:
The Pgp-digoxin interaction: Effects of multiple Pgp inhibitors
Background for investigation III Digoxin is commonly prescribed in the treatment of heart failure and atrial fibrillation despite its narrow therapeutic range and serious side affects. Di-goxin is not extensively metabolized in humans (185) and it has been sug-gested that Pgp is an important determinant of pharmacokinetics of digoxin after oral administration (5, 45, 133, 136). To evaluate the interaction be-tween digoxin and Pgp inhibitors in patients, we determined the relationship between the number of coadministered Pgp inhibitors and serum concentra-tions of digoxin (S-digoxin).
Methodology
PatientsAll patients at Uppsala University hospital who had their levels of digoxin determined via therapeutic drug monitoring (TDM) over the past three years were considered for this study. Patients were included if they were on oral digoxin treatment, their S-digoxin values were above the detection limit, steady state concentrations had been reached, the serum samples were meas-ured at trough, and information about concomitant treatment was available. The S-digoxin levels were determined by a fluorescence polarization immu-noassay (TDx®, Abbott Scandinavia AB, Sweden).
Classification of drugs The concomitantly administered drugs were classified as Pgp inhibitors when they demonstrated a clear inhibitory effect on Pgp in cellular transport assays, cellular uptake assays or animal models, as ascertained from a sys-tematic search of the literature in PubMed. Any effects of the concomitantly administered drugs on digoxin pharmacokinetics in vivo in humans were also documented. The Pgp inhibitors were then divided into two groups; 1) drugs with well documented interactions with digoxin in humans (these drugs were collectively designated “Class I Pgp inhibitors”) and 2) Pgp in-hibitors for which no significant effects on digoxin kinetics had been de-scribed in humans (these drugs were collectively designated “Class II Pgp

43
inhibitors”). Only substances administered orally were included in the classi-fication.
StatisticsAdjusted mean S-digoxin values were computed on the basis of the regres-sion estimates calculated with the General Linear Model using Proc GLM in SAS 8.02 (SAS Institute Inc., NC, USA), with the confounding factors at their mean values. Data were presented as mean values and standard errors (SE). Two models were used: one univariate and one multivariate, including the potential covariates age, sex, digoxin dose and total number of prescribed drugs for each individual (all continuous). In addition, subclass analysis in-cluding P-creatinine values and weight was performed.
Patients and co-administered drugs A total of 618 patients were included (for a summary of demographic data, see Table 6). 228 different drug substances were used by this group, and the median number of drugs was five for each patient.
Table 6. Demographic characteristics of the included patients.
Characteristic Median (range)
Age (years) 84 (24-99) P-creatinine (mmol/L) 100 (36-598)
Daily digoxin dose (mg) 0.13 (0.04-0.5) Number of administered drugs 5 (1-21)
Of the drugs used concomitantly with digoxin, eight were Pgp inhibitors with well documented effects on digoxin phamacokinetics, whereas thirteen drugs inhibited Pgp in vitro, but had no reported effects on digoxin pharma-cokinetics according to the PubMed search at the time of the study. The Class I drugs comprised amiodarone, atorvastatin, carvedilol, cyclosporine A, dipyridamole, quinidine, quinine and spironolactone. The Class II drugs included bromocriptine, flupenthixol, glibenclamide, isradipine, lansopra-zole, loperamide, medroxyprogesterone, omeprazole, pantoprazole, paroxet-ine, sertraline, simvastatin and terfenadine. Altogether, 47% of the patients took at least one Pgp inhibitor in addition to the treatment with digoxin.
S-digoxin levels in relation to administration of Pgp inhibitors The mean S-digoxin levels were significantly higher in the group receiving digoxin plus one or more Pgp inhibitors than in patients not taking Pgp in-hibitors (Fig. 9A, 1.55 0.04 nmol/L vs. 1.25 0.04 nmol/L, p < 0.001). Further, S-digoxin levels increased with the number of coadministered Pgp

44
inhibitors (Fig. 9B). The step-wise elevations in S-digoxin were even more pronounced in patients receiving Class I Pgp inhibitors alone (Fig. 9C).
0
0.5
1
1.5
2
2.5
0 1Number of P-gp inhibitors
***
0
0.5
1
1.5
2
2.5
0 1 2 3
Number of P-gp inhibitors
*** ***
**
S-D
igox
in(n
mol
/L)
Number of Pgp inhibitors
0
0.5
1
1.5
2
2.5
0 1 2 or 3
Number Class I P-gp inhibitors
*****
S-D
igox
in(n
mol
/L)
A B
C
S-D
igox
in(n
mol
/L)
Number of Pgp inhibitors
Number of Class I Pgp inhibitors
0
0.5
1
1.5
2
2.5
0 1Number of P-gp inhibitors
***
0
0.5
1
1.5
2
2.5
0 1 2 3
Number of P-gp inhibitors
*** ***
**
S-D
igox
in(n
mol
/L)
Number of Pgp inhibitors
0
0.5
1
1.5
2
2.5
0 1 2 3
Number of P-gp inhibitors
*** ***
**
S-D
igox
in(n
mol
/L)
Number of Pgp inhibitors
*** ***
**
S-D
igox
in(n
mol
/L)
Number of Pgp inhibitors
0
0.5
1
1.5
2
2.5
0 1 2 or 3
Number Class I P-gp inhibitors
*****
S-D
igox
in(n
mol
/L)
A B
C
S-D
igox
in(n
mol
/L)
Number of Pgp inhibitors
Number of Class I Pgp inhibitors
Fig. 9. The association between S-digoxin levels and the number of prescribed Pgp inhibitors. A) S-digoxin levels† were higher in patients also receiving one or more Pgp inhibi-tors ( 1; n = 290, S-digoxin mean ± SE 1.55 ± 0.04 nmol/L) than in patients not receiving a Pgp inhibitor (0; n = 328, S-digoxin mean ± SE 1.26 ± 0.04 nmol/L). B) S-digoxin levels† increased with the number of co-administered Pgp inhibitors. The adjusted S-digoxin levels were 1.26 ± 0.04, 1.51 ± 0.05, 1.59 ± 0.08 and 2.00 ± 0.25 nmol/L for patients receiving 0, 1, 2 and 3 Pgp inhibitors, respectively (n = 328, n = 204, n = 78 and n = 8 patients, respectively). C) The increase in S-digoxin levels† was even more pronounced in the group receiv-ing Class I Pgp inhibitors: 1.25 ± 0.04, 1.65 ± 0.07 and 1.83 ± 0.17 nmol/L for pa-tients taking 0, 1 or 2 Class I Pgp inhibitors, respectively (n = 328, n = 96 and n = 17, respectively). Significant differences are indicated by ** (p < 0.01) or *** (p < 0.001) †Adjusted for age, sex, digoxin dose and total number of prescribed drugs.

45
In patients receiving digoxin plus Class II inhibitors only, the trend to-wards higher digoxin levels with increasing numbers of Class II Pgp inhibi-tors was not statistically significant when the results were adjusted for age, sex, digoxin dosage and total number of prescribed drugs.
In 38 patients, the digoxin concentrations were higher than the recom-mended range (1.2 – 2.5 nmol/L at the time of the investigation). Patients with concentrations higher than the upper recommended concentration were more likely to be taking concomitant Pgp inhibitors than were patients with concentrations within the therapeutic range (68% vs. 47%, p = 0.01, Chi-square test).
The retrospective design of Investigation III is associated with several limitations. Lack of compliance and unreported usage of drugs are possible confounding factors. Only drugs reported on the day on which S-digoxin levels were measured could be included in the study. As digoxin is elimi-nated renally, it would have been ideal to have had measurements of creatinine clearance for all individuals. Creatinine clearance is not routinely determined, however, and the plasma concentrations of creatinine had to be used instead as an estimation of renal function. Another variable associated with digoxin concentration is body weight (or lean body mass). Surprisingly, body weight measurements were lacking for the majority of the patients, and only sub-group analysis of the individuals for whom this variable was known could be performed.
Dose, frequency of administration, bioavailability and clearance will all influence the measured S-digoxin levels. No conclusions can therefore be drawn concerning the tissue localization of the Pgp giving rise to the Pgp-digoxin interaction from this study. Both effects on bioavailability and renal clearance (135, 186, 187) contribute to the effects of the Pgp-digoxin inter-action. Pharmacokinetic interactions with digoxin can arise from mecha-nisms other than Pgp, such as changes in gut motility or pH or disturbance of digoxin metabolizing bacteria. Digoxin is also bound to red blood cells and serum albumin (188, 189) and displacement from these may also contribute to pharmacokinetic interactions involving digoxin. Furthermore, recent data suggests that transport mechanisms distinct from Pgp are involved in the translocation of digoxin across cellular membranes (189, 190).
In conclusion, S-digoxin levels increased with the number of co-administered Pgp inhibitors in this clinical study. The S-digoxin levels were 20% to 60% higher in individuals who were concomitantly taking Pgp in-hibitors. For a drug like digoxin which has such a narrow therapeutic range, such increases could result in safety concerns. In a study of men with a left ventricular ejection fraction of 45% or less who were treated with digoxin, serum digoxin concentrations > 1.5 nmol/L were associated with increased

46
mortality (191). Despite long clinical experience with heart glycosides such as digoxin and knowledge of several well-documented risk factors for asso-ciated toxicity (192), adverse drug reactions are still common in patients receiving the drug (32). We consider the evaluation of the effects of treat-ment with more than two drugs on digoxin levels to be particularly impor-tant, as situations like this are common in clinical practise.

47
Investigation IV:
Expression of intestinal ABC transporters in patients with ulcerative colitis
Background for investigation IV Inflammation is a component of many disease states. It is therefore impor-tant to understand the contribution of the inflammatory process to variability in drug absorption and/or disposition. In Investigation IV of this thesis, we determined the expression of the apically situated ABC transporters Pgp, BCRP and MRP2 in active and inactive phases of UC and compared these results with levels in controls. UC is the most common type of inflammatory bowel disease (IBD), with an incidence of 15 to 20 per 100 000 (193). The reasons for studying efflux transporters in IBD are two-fold: 1) To establish the etiopathological role of transport proteins in UC, since efflux transporters include nutritional and bacterial toxins as their substrates and 2) to improve understanding of drug-disease interactions and therapy failure, since several drugs used by patients with IBD are transported by ABC transporters.
Methodology
PatientsBiopsies from the distal sigmoid colon and rectum were obtained from pa-tients with inactive (n = 12) or active (n = 11) UC and from controls (n = 10). The controls were recruited among patients with normal mucosa who had been examined for anemia or rectal bleeding. The project was ap-proved by the Ethical Committee of the Medical Faculty, Uppsala Univer-sity, and all patients gave their informed consent to participate.
RNA isolation and RNA expression analysis RNA isolation and RNA expression analysis were performed as described for Investigation I, page 33. Ribosomal 18S (TaqMan Pre-Developed Assay Reagents, Applied Biosystems) was used as a reference transcript (internal standard) in the evaluation of content of villin, CD45, IL-1 and IL-6. As the intestinal mucosa is composed of heterogeneous cell populations, the RNA expression measurements represent an average expression from these differ-ent cell types. Therefore, two control genes were included: CD45 as a marker of leukocyte infiltration and villin as a marker of differentiated intes-tinal epithelial cells. As our primary interest in this study involved transport-

48
ers in the mucosal epithelial cells, the transcript levels of transporters were normalized to the villin expression levels.
Calculations and statistical considerations Relative transcript levels were determined using the comparative Ct method. The results were presented as the transcript levels relative to the levels in controls. The standard deviations of the relative transcript levels were calcu-lated from the standard deviation of Ct, using a first order Taylor series approximation. Kruskal-Wallis ANOVA by ranks followed by multiple comparisons was used for the comparison of the average transcript levels (p < 0.05 considered statistically significant). The statistical analysis was performed using Statistica 7.0 (StatSoft Scandinavia AB, Sweden). To con-trol for the potential confounding factors age, gender, disease duration and concomitant treatment with IBD drugs, we adjusted the group RNA expres-sion differences for putative group differences in these variables. A linear model was used to calculate individually adjusted values (the residuals from a model with RNA expression as dependent variable and the above covari-ates as predictors) and the Kruskal-Wallis test was applied on these adjusted values. For an evaluation of the co-variation between the expression of transporters and inflammatory markers, the Spearman rank correlation coef-ficients were calculated (p < 0.05 considered significant).
PatientsFor a summary of demographic and clinical features, see Table 7.
Table 7. Patient characteristics.
Control (n = 10)
UC Remission (n = 12)
UC Active (n = 11)
Sex (F = females, M = males ) F = 6, M = 4 F = 4, M = 8 F = 4, M = 7 Age (mean (range) in years) 57 (38-80) 51 (23-72) 47 (31-62)
Current smokers Not recorded 1 1 Patients with 5-aminosalicylate
high (> 2400 mg / day) - - 2
average (1600 – 2400 mg / day) - 2 1
low (< 1600 mg / day) - 1 3
local administration - - 1
Patients with sulfasalazine high (> 2.5 g / day) - 5 2
average (1.5-2.5 g / day) - 3 1
Patients with steroids high (> 40 mg / day) - - 2
average (15-35 mg / day) 1 1 - low (< 15 mg / day) - 1 -

49
Mucosal expression of ABC transporters in ulcerative colitis The levels of Pgp and BCRP were significantly reduced in inflamed tissues compared with non-inflamed tissues (Fig. 10). In the actively inflamed colon and rectum, the villin-normalized mRNA expression of Pgp was 22% and 34% of the values in control biopsies from the colon (Fig. 10A). The expres-sion levels of BCRP mRNA in inflamed tissues were even lower: the values were 11% (colon) and 16% (rectum) of those in control biopsies from the colon (Fig. 10B). The levels of MRP2 were very low in the colon and the rectum, with levels approximately 100-fold lower than those of Pgp and BCRP. No significant differences were observed in the MRP2 levels (Fig. 10C).
0
0.5
1
1.5
Control Remission Active
Exp
ress
ion
(rel
ativ
e to
con
trol)
B. BCRP
******0
0.5
1
1.5
Control Remission Active
Exp
ress
ion
(rel
ativ
e to
con
trol)
B. BCRP
******0
0.5
1
1.5
Control Remission Active
*****
Exp
ress
ion
(rel
ativ
e to
con
trol)
A. Pgp
0
0.5
1
1.5
Control Remission Active
*****
Exp
ress
ion
(rel
ativ
e to
con
trol)
A. Pgp
0
0.5
1
1.5
2
Control Remission Active
C. MRP2
Exp
ress
ion
(rel
ativ
e to
con
trol)
0
0.5
1
1.5
2
Control Remission Active
C. MRP2
Exp
ress
ion
(rel
ativ
e to
con
trol)
Fig. 10. The mRNA expression of Pgp (A), BCRP (B) and MRP2 (C) in control tissue and in tissue from UC patients in remission and during active inflammation (villin normalized expression relative to the levels in colon from control individuals + SEM). Filled bars = colonic tissues, open bars = rectal tissues. Statistically signifi-cant differences are indicated by ** (p < 0.01) and *** (p < 0.001).
The differences in Pgp and BCRP expression between inflamed and non-inflamed tissues remained significant when comparing the residuals from a linear model taking age, gender, disease duration and treatment with IBD drugs into account. As ABC transporters also exist in cell types other than epithelial cells, for example in leukocytes (194, 195), it was considered likely that the transporter levels in the inflamed tissues were overestimated when normalizing the expression data to the levels of the epithelial marker villin, as it was done in this study. On the other hand, the levels of transport-ers in inflamed tissues would be expected to be underestimated upon normal-izing to the total content of ribosomal 18S RNA.
Correlation between ABC transporters and cytokines Studies in rats and mice have suggested that pro-inflammatory cytokines mediate the effects of inflammation on the expression of metabolic enzymes and transporters, including Pgp, Bsep (Bile salt export pump) and members of the Mrp and Oatp families (196-199). The mucosal levels of the cytokines

50
IL-1 and IL-6 were therefore determined in this study. No significant corre-lations were observed betweeen IL-1 and ABC transporter expression. For IL-6, on the other hand, the levels correlated with the levels of all three in-vestigated ABC transporters (the Spearman rank correlations were signifi-cant at p < 0.05). Individuals with high IL-6 levels had low levels of Pgp and BCRP, whereas individuals with high MRP2 levels also exhibited high IL-6 levels (Fig. 11).
-2 -1 0 1 2 3
23
24
25
26
27A.
Expr
essi
on o
f IL6
(C
t)
Expression of Pgp ( Ct)
R = -0.66
-1 0 1 2 3 4 5 6
23
24
25
26
27B.
Expr
essi
on o
f IL6
(C
t)
Expression of BCRP ( Ct)
R = -0.64
6 7 8 9 1022
23
24
25
26
27
Expr
essi
on o
f IL1
6(
Ct)
Expression of MRP2 ( Ct)
C.
R = -0.65
-2 -1 0 1 2 3
23
24
25
26
27A.
Expr
essi
on o
f IL6
(C
t)
Expression of Pgp ( Ct)
R = -0.66
-2 -1 0 1 2 3
23
24
25
26
27A.
Expr
essi
on o
f IL6
(C
t)
Expression of Pgp ( Ct)
R = -0.66
-1 0 1 2 3 4 5 6
23
24
25
26
27B.
Expr
essi
on o
f IL6
(C
t)
Expression of BCRP ( Ct)
R = -0.64
-1 0 1 2 3 4 5 6
23
24
25
26
27B.
Expr
essi
on o
f IL6
(C
t)
Expression of BCRP ( Ct)
R = -0.64
6 7 8 9 1022
23
24
25
26
27
Expr
essi
on o
f IL1
6(
Ct)
Expression of MRP2 ( Ct)
C.
R = -0.65
6 7 8 9 1022
23
24
25
26
27
Expr
essi
on o
f IL1
6(
Ct)
Expression of MRP2 ( Ct)
C.
R = -0.65
Fig. 11. The correlation between Pgp (A), BCRP (B) and MRP2 (C) and the expres-sion of IL-6 in the colonic mucosa of individuals with active UC. The Spearman rank correlation coefficients are indicated in the graphs. These correlations were significant at p < 0.05.
Several therapeutic agents routinely used in IBD treatment are effluxed by ABC transporters, which could affect the local concentration of drug in the target tissue. Vectorial flux of 5-aminosalicylate has been suggested to be Pgp-mediated (200), sulphasalazine transport has been attributed to BCRP and MRP activity (201, 202) and cyclosporine is a modulator of several ABC transporters, including Pgp and BCRP (203). Steroids are important in the treatment of IBD, and it has been suggested that Pgp contributes to glu-cocorticoid resistance, which is an impeding factor in UC therapy (204). Several different steroids are effluxed by Pgp (205, 206) but it is now recog-nized that conjugated forms of steroids are also transported by BCRP (148).
Mice deficient in Pgp, mdr1a-/- mice, spontaneously develop colitis (207). This observation initiated an interest in the role of Pgp in tissue de-fense in IBD. Genetic variation in ABCB1 has recently been associated with susceptibility for UC (208). There are so far no reports on development of colitis in the Bcrp1-/- mice lines (69, 71) or in transport of bacterial toxins for BCRP, but such investigations would certainly be of interest.
Local drug delivery is common in IBD (209), and the concentration of drug reached in intestinal cells will be important for the responsiveness to treatment (200). Differences in expression of efflux transporters may lead to alterations in concentrations of drugs in the intestinal mucosa and changes in the absorption of substances that have to reach the systemic circulation to have an effect. The conclusions from this investigation were that Pgp and

51
BCRP are down-regulated in the intestinal mucosa during active phases of UC. This has potential implications for drug therapy, as well as for the fur-ther delineation of the pathogenesis of ulcerative colitis.

52
Conclusions
The results of this thesis emphasize the complex background to interindi-vidual variability of drug transporters. Physiological, genetic, environmental and pathological factors that could contribute to interindividual variability in responsiveness to certain drugs were described. Specifically, the conclusions from the investigations included in this thesis were that:
1. Many drug transporters are expressed in a region-dependent manner along the human intestine, although only minor differences in expression were observed within the small intestine. Large discrepancies between the Caco-2 model and the human ileum were observed for the transport-ers BCRP, OATPB and MRP2, and it is important to consider these in the interpretation of permeability data from this cell model.
2. Genetic variations of interest for pharmacogenetic studies were identi-fied in the ABCG2 gene. A CTCA deletion in the 5´flanking region, a G>C transversion in a CpG island region in the promotor and two non-synonymous alterations in exon two (34G>A) and five (421C>A, Gln141Lys) were considered to be of greatest interest. For these, the al-lele frequencies were determined and linkage disequilibrium was ob-served over the region between the CTCA deletion and 421C>A.
3. A large proportion of the patients undergoing drug level monitoring for digoxin were concomitantly taking one or more Pgp inhibitor(s). The se-rum concentrations of digoxin were significantly higher in patients with concomitant therapy with one or more Pgp inhibitor(s), and the concen-trations of digoxin increased with the number of administered Pgp in-hibitors. For drugs like digoxin which have a narrow therapeutic range increases of 20% to 60% in concentration, as observed in this study, are enough to raise safety concerns.
4. Expression of the ABC transporters Pgp and BCRP was significantly reduced in inflamed tissues from patients with UC. This could poten-tially affect the mucosal concentrations of several therapeutic agents used in IBD, as well as the systemic concentrations of drugs that are transported by these two ABC transporters.

53
Summary of results and perspectives
Studies of interindividual variability in drug response will continue to be important because of the severity and high frequency of adverse reactions in drug recipients (2, 210) and because serious drug-drug interactions and toxic reactions in some individuals have resulted in the withdrawal of approved drugs and prevented the approval of new drug entities (211). After identifi-cation of mechanisms of interindividual variability, the greater challenge will lie in predicting the substances and clinical circumstances for which these mechanisms will be of relevance.
The effects of transport proteins on drug plasma concentrations have not, to date, been as pronounced as the effects of some metabolic enzymes such as CYP2D6 (212). This may partly depend on the existence of parallel elimi-nation routes. However, less pronounced effects on drug plasma concentra-tion also require evaluation if individualization of pharmacotherapy is to be achieved. The measurement of smaller effects on concentration profiles will require greater stringency in the design of clinical studies. For instance, physiological, environmental or pathological differences may overshadow differences in pharmacogenetic studies, which may in part explain the dis-crepancies seen in the pharmacogenetic studies of Pgp (103). The concept of personalized medicine is currently very focused on genetics and, although genetics is a very important factor, other factors affecting interindividual variability also require consideration. The results of this thesis, with exam-ples of physiological, genetic, environmental and pathological factors that could potentially contribute to interindividual variability in drug response, emphasize the multifactorial nature of the issue of interindividual variability.

54
AcknowledgementsThe studies of this thesis were carried out at the department of Pharmacy and the department of Medical Sciences, at Uppsala University; the staffs at these depart-ments are gratefully acknowledged. This work was supported by the Swedish Foun-dation for Strategic Research, within the NNDD program. My participation in con-ferences and courses was made possible by travel grants from CD Carlssons stiftelse and Rektors Wallenbergmedel.
I wish to express my sincere gratitude to all of you that contributed to my thesis: My supervisors professor Per Artursson and professor Håkan Melhus, for giving me the opportunity to do a PhD on the topic I find the most interesting, and to Per for introducing me to the transporter field and for kindly sharing your research skills. To my supervisor Andreas Kindmark for being such an enthusiastic and warm person, and for your genuine and broad interest in research. To Anders Rönnblom and Fredrik Rorsman for a fruitful collaboration, and to An-ders for being one of the few persons I have met who is at the same time enthusiastic and realistic. To all nurses, assistants and doctors of the Department of Gastroen-terology at Uppsala University Hospital for excellent assistance with collecting the biopsies and for your at all times kind reception. To Urban Karlbom for your co-operation in Paper I. To Annica Jacobson, for all our discussions about research and everything else of interest, and for an inspiring time during our work with Paper IV. To Helena Brändström for introducing me to the secrets of molecular biology and for all your highly appreciated initiatives to coffee and lunch breaks. To Lucia Lazarova for sharing your knowledge in cell culturing.and for being such a considerate person. To Pär Hallberg for a good time during our work with Paper III. To Johan Gråsjö, Lars Berglund and Karl Michaëlsson for your constructive input in statistical matters. To past and present members of the “cell group”, especially to Eva Ragnarsson for always taking your time, to Elisabet Gullberg for being a very nice room mate, and to Helena Engman for being a tough teacher in cell culturing techniques. To Niclas Petri for your well-founded comments on my thesis. To Elin Grundberg for being a tough sparring partner and for your cheerfulness (even during early mornings). To my room mates, Elin, Helena, Richard, Calle, Fredrik, Turid, and Tijana for the good spirit and for all intriguing and unpredictable discussions (regardless of topic). To my family, for always supporting me, and particularly to my father, Göran, for taking such a great interest in my research. To my beloved husband, Tom, for your invaluable support during these years. No-one can be as encouraging as you and you are without doubt the best language re-viewer I know.

55
References
1. K. Fattinger, M. Roos, P. Vergeres, C. Holenstein, B. Kind, U. Masche, D. N. Stocker, S. Braunschweig, G. A. Kullak-Ublick, R. L. Galeazzi, F. Follath, T. Gasser, and P. J. Meier. Epidemiology of drug exposure and adverse drug reactions in two swiss departments of inter-nal medicine. Br J Clin Pharmacol 49: 158-67 (2000).
2. J. Lazarou, B. H. Pomeranz, and P. N. Corey. Incidence of adverse drug reactions in hospital-ized patients: a meta-analysis of prospective studies. Jama 279: 1200-5 (1998).
3. N. Moore, D. Lecointre, C. Noblet, and M. Mabille. Frequency and cost of serious adverse drug reactions in a department of general medicine. Br J Clin Pharmacol 45: 301-8 (1998).
4. A. Ayrton and P. Morgan. Role of transport proteins in drug absorption, distribution and excretion. Xenobiotica 31: 469-97 (2001).
5. B. Greiner, M. Eichelbaum, P. Fritz, H. P. Kreichgauer, O. von Richter, J. Zundler, and H. K. Kroemer. The role of intestinal P-glycoprotein in the interaction of digoxin and rifampin. JClin Invest 104: 147-53 (1999).
6. C. M. Kruijtzer, J. H. Beijnen, H. Rosing, W. W. ten Bokkel Huinink, M. Schot, R. C. Jewell, E. M. Paul, and J. H. Schellens. Increased oral bioavailability of topotecan in combination with the breast cancer resistance protein and P-glycoprotein inhibitor GF120918. J Clin Oncol20: 2943-50 (2002).
7. K. S. Lown, R. R. Mayo, A. B. Leichtman, H. L. Hsiao, D. K. Turgeon, P. Schmiedlin-Ren, M. B. Brown, W. Guo, S. J. Rossi, L. Z. Benet, and P. B. Watkins. Role of intestinal P-glycoprotein (mdr1) in interpatient variation in the oral bioavailability of cyclosporine. ClinPharmacol Ther 62: 248-60 (1997).
8. M. Rowlandand and T.N. Tozer. Clinical Pharmacokinetics, Concepts and Applications, 3rd edition. Williams & Wilkins: (1995).
9. M. J. Blake, L. Castro, J. S. Leeder, and G. L. Kearns. Ontogeny of drug metabolizing en-zymes in the neonate. Semin Fetal Neonatal Med 10: 123-38 (2005).
10. W. Muhlberg and D. Platt. Age-dependent changes of the kidneys: pharmacological implica-tions. Gerontology 45: 243-53 (1999).
11. M. Gandhi, F. Aweeka, R. M. Greenblatt, and T. F. Blaschke. Sex differences in pharmacoki-netics and pharmacodynamics. Annu Rev Pharmacol Toxicol 44: 499-523 (2004).
12. B. Meibohm, I. Beierle, and H. Derendorf. How important are gender differences in pharma-cokinetics? Clin Pharmacokinet 41: 329-42 (2002).
13. D. Horter and J. B. Dressman. Influence of physicochemical properties on dissolution of drugs in the gastrointestinal tract. Adv Drug Deliv Rev 46: 75-87 (2001).
14. M. Ashford. Bioavailability - physiochemical and dosage form factors. In:. Aulton, ME, ed. Pharmaceutics. The science of dosage form design. Second ed. London: Churchill Living-stone; 2002:234-252 (2002).
15. J. C. Venter, M. D. Adams, E. W. Myers, P. W. Li, R. J. Mural, G. G. Sutton, H. O. Smith, M. et al. The sequence of the human genome. Science 291: 1304-51 (2001).
16. A. E. Guttmacher and F. S. Collins. Genomic medicine--a primer. N Engl J Med 347: 1512-20 (2002).
17. W. E. Evans and H. L. McLeod. Pharmacogenomics--drug disposition, drug targets, and side effects. N Engl J Med 348: 538-49 (2003).

56
18. A. K. Daly. Pharmacogenetics of the major polymorphic metabolizing enzymes. Fundam Clin Pharmacol 17: 27-41 (2003).
19. W. Kalow, B. K. Tang, and L. Endrenyi. Hypothesis: comparisons of inter- and intra-individual variations can substitute for twin studies in drug research. Pharmacogenetics 8:283-9 (1998).
20. K. A. Phillips, D. L. Veenstra, E. Oren, J. K. Lee, and W. Sadee. Potential role of pharmaco-genomics in reducing adverse drug reactions: a systematic review. Jama 286: 2270-9. (2001).
21. S. Hoffmeyer, O. Burk, O. von Richter, H. P. Arnold, J. Brockmoller, A. Johne, I. Cascorbi, T. Gerloff, I. Roots, M. Eichelbaum, and U. Brinkmann. Functional polymorphisms of the human multidrug-resistance gene: multiple sequence variations and correlation of one allele with P- glycoprotein expression and activity in vivo. Proc Natl Acad Sci U S A 97: 3473-8 (2000).
22. J. Taipalensuu, H. Tornblom, G. Lindberg, C. Einarsson, F. Sjoqvist, H. Melhus, P. Garberg, B. Sjostrom, B. Lundgren, and P. Artursson. Correlation of gene expression of ten drug efflux proteins of the atp- binding cassette transporter family in normal human jejunum and in human intestinal epithelial caco-2 cell monolayers. J Pharmacol Exp Ther 299: 164-70. (2001).
23. L. R. Cardon and G. R. Abecasis. Using haplotype blocks to map human complex trait loci. Trends Genet 19: 135-40 (2003).
24. D. Fleisher, C. Li, Y. Zhou, L. H. Pao, and A. Karim. Drug, meal and formulation interactions influencing drug absorption after oral administration. Clinical implications. Clin Pharmacoki-net 36: 233-54 (1999).
25. A. Fugh-Berman. Herb-drug interactions. Lancet 355: 134-8 (2000). 26. S. Zevinand N. L. Benowitz. Drug interactions with tobacco smoking. An update. Clin Phar-
macokinet 36: 425-38 (1999). 27. A. G. Fraser. Pharmacokinetic interactions between alcohol and other drugs. Clin Pharma-
cokinet 33: 79-90 (1997). 28. R. J. Fontana, K. S. Lown, M. F. Paine, L. Fortlage, R. M. Santella, J. S. Felton, M. G. Knize,
A. Greenberg, and P. B. Watkins. Effects of a chargrilled meat diet on expression of CYP3A, CYP1A, and P-glycoprotein levels in healthy volunteers. Gastroenterology 117: 89-98 (1999).
29. G. K. Dresser, D. G. Bailey, B. F. Leake, U. I. Schwarz, P. A. Dawson, D. J. Freeman, and R. B. Kim. Fruit juices inhibit organic anion transporting polypeptide-mediated drug uptake to decrease the oral availability of fexofenadine. Clin Pharmacol Ther 71: 11-20 (2002).
30. D. W. Kaufman, J. P. Kelly, L. Rosenberg, T. E. Anderson, and A. A. Mitchell. Recent pat-terns of medication use in the ambulatory adult population of the United States: the Slone sur-vey. Jama 287: 337-44 (2002).
31. J. U. Rosholm, L. Bjerrum, J. Hallas, J. Worm, and L. F. Gram. Polypharmacy and the risk of drug-drug interactions among Danish elderly. A prescription database study. Dan Med Bull45: 210-3 (1998).
32. D. N. Juurlink, M. Mamdani, A. Kopp, A. Laupacis, and D. A. Redelmeier. Drug-drug interac-tions among elderly patients hospitalized for drug toxicity. Jama 289: 1652-8 (2003).
33. J. F. Westphal and J. M. Brogard. Drug administration in chronic liver disease. Drug Saf 17:47-73 (1997).
34. G. R. Matzke and R. F. Frye. Drug administration in patients with renal insufficiency. Mini-mising renal and extrarenal toxicity. Drug Saf 16: 205-31 (1997).
35. H. Sun, L. Frassetto, and L. Z. Benet. Effects of renal failure on drug transport and metabo-lism. Pharmacol Ther (2005).
36. R. L. Parsons. Drug absorption in gastrointestinal disease with particular reference to malab-sorption syndromes. Clin Pharmacokinet 2: 45-60 (1977).
37. D. C. Baumgart and A. U. Dignass. Intestinal barrier function. Curr Opin Clin Nutr Metab Care 5: 685-94 (2002).
38. K. W. Renton. Cytochrome P450 regulation and drug biotransformation during inflammation and infection. Curr Drug Metab 5: 235-43 (2004).

57
39. K. A. Slaviero, S. J. Clarke, and L. P. Rivory. Inflammatory response: an unrecognised source of variability in the pharmacokinetics and pharmacodynamics of cancer chemotherapy. Lancet Oncol 4: 224-32 (2003).
40. J. L. Madara. Epithelia: Biologic Principles of Organization. Textbook of Gastroenterology, 3rd edition II. Lippincott Williams & Wilkins: (1999).
41. H. Lennernas. Human intestinal permeability. J Pharm Sci 87: 403-10 (1998). 42. P. Matsson, C. A. Bergstrom, N. Nagahara, S. Tavelin, U. Norinder, and P. Artursson. Explor-
ing the role of different drug transport routes in permeability screening. J Med Chem 48: 604-13 (2005).
43. T. Gramatte and R. Oertel. Intestinal secretion of intravenous talinolol is inhibited by luminal R-verapamil. Clin Pharmacol Ther 66: 239-45 (1999).
44. A. Sparreboom, J. van Asperen, U. Mayer, A. H. Schinkel, J. W. Smit, D. K. Meijer, P. Borst, W. J. Nooijen, J. H. Beijnen, and O. van Tellingen. Limited oral bioavailability and active epithelial excretion of paclitaxel (Taxol) caused by P-glycoprotein in the intestine. Proc Natl Acad Sci U S A 94: 2031-5 (1997).
45. S. Drescher, H. Glaeser, T. Murdter, M. Hitzl, M. Eichelbaum, and M. F. Fromm. P-glycoprotein-mediated intestinal and biliary digoxin transport in humans. Clin Pharmacol Ther 73: 223-31 (2002).
46. M. S. Roberts, B. M. Magnusson, F. J. Burczynski, and M. Weiss. Enterohepatic circulation: physiologicalal, pharmacokinetic and clinical implications. Clin Pharmacokinet 41: 751-90 (2002).
47. Y. Kato, H. Suzuki, and Y. Sugiyama. Toxicological implications of hepatobiliary transport-ers. Toxicology 181-182: 287-90 (2002).
48. M. M. Doherty and W. N. Charman. The mucosa of the small intestine: how clinically relevant as an organ of drug metabolism? Clin Pharmacokinet 41: 235-53 (2002).
49. J. C. Kolars, K. S. Lown, P. Schmiedlin-Ren, M. Ghosh, C. Fang, S. A. Wrighton, R. M. Merion, and P. B. Watkins. CYP3A gene expression in human gut epithelium. Pharmacoge-netics 4: 247-59 (1994).
50. K. S. Lown, J. C. Kolars, K. E. Thummel, J. L. Barnett, K. L. Kunze, S. A. Wrighton, and P. B. Watkins. Interpatient heterogeneity in expression of CYP3A4 and CYP3A5 in small bowel. Lack of prediction by the erythromycin breath test. Drug Metab Dispos 22: 947-55 (1994).
51. X. Ding and L. S. Kaminsky. Human extrahepatic cytochromes P450: function in xenobiotic metabolism and tissue-selective chemical toxicity in the respiratory and gastrointestinal tracts. Annu Rev Pharmacol Toxicol 43: 149-73 (2003).
52. T. Prueksaritanont, L. M. Gorham, J. H. Hochman, L. O. Tran, and K. P. Vyas. Comparative studies of drug-metabolizing enzymes in dog, monkey, and human small intestines, and in Caco-2 cells. Drug Metab Dispos 24: 634-42 (1996).
53. J. H. Lin, M. Chiba, and T. A. Baillie. Is the role of the small intestine in first-pass metabolism overemphasized? Pharmacol Rev 51: 135-58. (1999).
54. M. F. Paine, D. D. Shen, K. L. Kunze, J. D. Perkins, C. L. Marsh, J. P. McVicar, D. M. Barr, B. S. Gillies, and K. E. Thummel. First-pass metabolism of midazolam by the human intestine. Clin Pharmacol Ther 60: 14-24 (1996).
55. P. J. Sinko, J. R. Kunta, H. H. Usansky, and B. A. Perry. Differentiation of gut and hepatic first pass metabolism and secretion of saquinavir in ported rabbits. J Pharmacol Exp Ther 310:359-66 (2004).
56. V. J. Wacher, C. Y. Wu, and L. Z. Benet. Overlapping substrate specificities and tissue distri-bution of cytochrome P450 3A and P-glycoprotein: implications for drug delivery and activity in cancer chemotherapy. Mol Carcinog 13: 129-34 (1995).
57. L. Z. Benet, C. L. Cummins, and C. Y. Wu. Unmasking the dynamic interplay between efflux transporters and metabolic enzymes. Int J Pharm 277: 3-9 (2004).
58. R. L. Juliano and V. Ling. A surface glycoprotein modulating drug permeability in Chinese hamster ovary cell mutants. Biochim Biophys Acta 455: 152-62 (1976).

58
59. R. Allikmets, B. Gerrard, A. Hutchinson, and M. Dean. Characterization of the human ABC superfamily: isolation and mapping of 21 new genes using the expressed sequence tags data-base. Hum Mol Genet 5: 1649-55. (1996).
60. L. A. Doyle, W. Yang, L. V. Abruzzo, T. Krogmann, Y. Gao, A. K. Rishi, and D. D. Ross. A multidrug resistance transporter from human MCF-7 breast cancer cells. Proc Natl Acad Sci U S A 95: 15665-70 (1998).
61. C. F. Higgins and K. J. Linton. The ATP switch model for ABC transporters. Nat Struct Mol Biol 11: 918-26 (2004).
62. M. A. Hediger, M. F. Romero, J. B. Peng, A. Rolfs, H. Takanaga, and E. A. Bruford. The ABCs of solute carriers: physiologicalal, pathologicalal and therapeutic implications of human membrane transport proteinsIntroduction. Pflugers Arch 447: 465-8 (2004).
63. A. Tsuji and I. Tamai. Carrier-mediated intestinal transport of drugs. Pharm Res 13: 963-77 (1996).
64. Y. Zhang, C. Bachmeier, and D. W. Miller. In vitro and in vivo models for assessing drug efflux transporter activity. Adv Drug Deliv Rev 55: 31-51 (2003).
65. U. I. Schwarz, D. Seemann, R. Oertel, S. Miehlke, E. Kuhlisch, M. F. Fromm, R. B. Kim, D. G. Bailey, and W. Kirch. Grapefruit juice ingestion significantly reduces talinolol bioavailabil-ity. Clin Pharmacol Ther 77: 291-301 (2005).
66. C. Tannergren, N. Petri, L. Knutson, M. Hedeland, U. Bondesson, and H. Lennernas. Multiple transport mechanisms involved in the intestinal absorption and first-pass extraction of fexofenadine. Clin Pharmacol Ther 74: 423-36 (2003).
67. S. Tavelin, J. Grasjo, J. Taipalensuu, G. Ocklind, and P. Artursson. Applications of epithelial cell culture in studies of drug transport. Methods Mol Biol 188: 233-72 (2002).
68. H. Lennernas. Human jejunal effective permeability and its correlation with preclinical drug absorption models. J Pharm Pharmacol 49: 627-38 (1997).
69. J. W. Jonker, M. Buitelaar, E. Wagenaar, M. A. Van Der Valk, G. L. Scheffer, R. J. Scheper, T. Plosch, F. Kuipers, R. P. Elferink, H. Rosing, J. H. Beijnen, and A. H. Schinkel. The breast cancer resistance protein protects against a major chlorophyll-derived dietary phototoxin and protoporphyria. Proc Natl Acad Sci U S A 99: 15649-54 (2002).
70. A. H. Schinkel, J. J. Smit, O. van Tellingen, J. H. Beijnen, E. Wagenaar, L. van Deemter, C. A. Mol, M. A. van der Valk, E. C. Robanus-Maandag, H. P. te Riele, and et al. Disruption of the mouse mdr1a P-glycoprotein gene leads to a deficiency in the blood-brain barrier and to increased sensitivity to drugs. Cell 77: 491-502 (1994).
71. S. Zhou, J. J. Morris, Y. Barnes, L. Lan, J. D. Schuetz, and B. P. Sorrentino. Bcrp1 gene expression is required for normal numbers of side population stem cells in mice, and confers relative protection to mitoxantrone in hematopoietic cells in vivo. Proc Natl Acad Sci U S A99: 12339-44 (2002).
72. H. Lennernas, O. Ahrenstedt, R. Hallgren, L. Knutson, M. Ryde, and L. K. Paalzow. Regional jejunal perfusion, a new in vivo approach to study oral drug absorption in man. Pharm Res 9:1243-51 (1992).
73. J. R. Kunta and P. J. Sinko. Intestinal drug transporters: in vivo function and clinical impor-tance. Curr Drug Metab 5: 109-24 (2004).
74. S. A. Adibi. The oligopeptide transporter (Pept-1) in human intestine: biology and function. Gastroenterology 113: 332-40 (1997).
75. B. E. Enerson and L. R. Drewes. Molecular features, regulation, and function of monocar-boxylate transporters: Implications for drug delivery. J Pharm Sci 92: 1531-44 (2003).
76. M. F. Fromm, H. M. Kauffmann, P. Fritz, O. Burk, H. K. Kroemer, R. W. Warzok, M. Eichel-baum, W. Siegmund, and D. Schrenk. The effect of rifampin treatment on intestinal expression of human MRP transporters. Am J Pathol 157: 1575-80. (2000).
77. J. W. Jonker, J. W. Smit, R. F. Brinkhuis, M. Maliepaard, J. H. Beijnen, J. H. Schellens, and A. H. Schinkel. Role of breast cancer resistance protein in the bioavailability and fetal penetra-tion of topotecan. J Natl Cancer Inst 92: 1651-6 (2000).

59
78. Y. Gotoh, H. Suzuki, S. Kinoshita, T. Hirohashi, Y. Kato, and Y. Sugiyama. Involvement of an organic anion transporter (canalicular multispecific organic anion transporter/multidrug re-sistance-associated protein 2) in gastrointestinal secretion of glutathione conjugates in rats. JPharmacol Exp Ther 292: 433-9. (2000).
79. H. Toyobuku, I. Tamai, K. Ueno, and A. Tsuji. Limited influence of P-glycoprotein on small-intestinal absorption of cilostazol, a high absorptive permeability drug. J Pharm Sci 92: 2249-59 (2003).
80. A. Tsuji. Tissue selective drug delivery utilizing carrier-mediated transport systems. J Control Release 62: 239-44 (1999).
81. E. M. Leslie, R. G. Deeley, and S. P. Cole. Multidrug resistance proteins: role of P-glycoprotein, MRP1, MRP2, and BCRP (ABCG2) in tissue defense. Toxicol Appl Pharmacol204: 216-37 (2005).
82. G. D. Leonard, T. Fojo, and S. E. Bates. The role of ABC transporters in clinical practice. Oncologist 8: 411-24 (2003).
83. H. Kusuhara and Y. Sugiyama. Role of transporters in the tissue-selective distribution and elimination of drugs: transporters in the liver, small intestine, brain and kidney. J Control Re-lease 78: 43-54 (2002).
84. W. Leeand R. B. Kim. Transporters and renal drug elimination. Annu Rev Pharmacol Toxicol44: 137-66 (2004).
85. A. T. Fojo, K. Ueda, D. J. Slamon, D. G. Poplack, M. M. Gottesman, and I. Pastan. Expression of a multidrug-resistance gene in human tumors and tissues. Proc Natl Acad Sci U S A 84:265-9 (1987).
86. P. A. Fetsch, A. Abati, T. Litman, K. Morisaki, Y. Honjo, K. Mittal, and S. E. Bates. Localiza-tion of the ABCG2 mitoxantrone resistance-associated protein in normal tissues. Cancer Lett(2005).
87. K. N. Faber, M. Muller, and P. L. Jansen. Drug transport proteins in the liver. Adv Drug Deliv Rev 55: 107-24 (2003).
88. M. Dean and T. Annilo. Evolution of the Atp-Binding Cassette (Abc) Transporter Superfamily in Vertebrates *. Annu Rev Genomics Hum Genet 6: 123-142 (2005).
89. P. Bouige, D. Laurent, L. Piloyan, and E. Dassa. Phylogenetic and functional classification of ATP-binding cassette (ABC) systems. Curr Protein Pept Sci 3: 541-59 (2002).
90. C. C. Paulusma, M. Kool, P. J. Bosma, G. L. Scheffer, F. ter Borg, R. J. Scheper, G. N. Tytgat, P. Borst, F. Baas, and R. P. Oude Elferink. A mutation in the human canalicular multispecific organic anion transporter gene causes the Dubin-Johnson syndrome. Hepatology 25: 1539-42 (1997).
91. J. M. de Vree, E. Jacquemin, E. Sturm, D. Cresteil, P. J. Bosma, J. Aten, J. F. Deleuze, M. Desrochers, M. Burdelski, O. Bernard, R. P. Oude Elferink, and M. Hadchouel. Mutations in the MDR3 gene cause progressive familial intrahepatic cholestasis. Proc Natl Acad Sci U S A95: 282-7 (1998).
92. S. G. Young and C. J. Fielding. The ABCs of cholesterol efflux. Nat Genet 22: 316-8 (1999). 93. J. R. Riordan, J. M. Rommens, B. Kerem, N. Alon, R. Rozmahel, Z. Grzelczak, J. Zielenski, S.
Lok, N. Plavsic, J. L. Chou, and et al. Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA. Science 245: 1066-73 (1989).
94. J. D. Allen, R. F. Brinkhuis, J. Wijnholds, and A. H. Schinkel. The mouse Bcrp1/Mxr/Abcp gene: amplification and overexpression in cell lines selected for resistance to topotecan, mi-toxantrone, or doxorubicin. Cancer Res 59: 4237-41. (1999).
95. K. Miyake, L. Mickley, T. Litman, Z. Zhan, R. Robey, B. Cristensen, M. Brangi, L. Greenber-ger, M. Dean, T. Fojo, and S. E. Bates. Molecular cloning of cDNAs which are highly overex-pressed in mitoxantrone-resistant cells: demonstration of homology to ABC transport genes. Cancer Res 59: 8-13. (1999).
96. C. H. Choi. ABC transporters as multidrug resistance mechanisms and the development of chemosensitizers for their reversal. Cancer Cell Int 5: 30 (2005).

60
97. K. Kage, S. Tsukahara, T. Sugiyama, S. Asada, E. Ishikawa, T. Tsuruo, and Y. Sugimoto. Dominant-negative inhibition of breast cancer resistance protein as drug efflux pump through the inhibition of S-S dependent homodimerization. Int J Cancer 97: 626-30. (2002).
98. J. Xu, Y. Liu, Y. Yang, S. Bates, and J. T. Zhang. Characterization of oligomeric human half-ABC transporter ATP-binding cassette G2. J Biol Chem 279: 19781-9 (2004).
99. P. Gros, J. Croop, and D. Housman. Mammalian multidrug resistance gene: complete cDNA sequence indicates strong homology to bacterial transport proteins. Cell 47: 371-80 (1986).
100. C. J. Chen, J. E. Chin, K. Ueda, D. P. Clark, I. Pastan, M. M. Gottesman, and I. B. Roninson. Internal duplication and homology with bacterial transport proteins in the mdr1 (P-glycoprotein) gene from multidrug-resistant human cells. Cell 47: 381-9 (1986).
101. K. Ueda, D. P. Clark, C. J. Chen, I. B. Roninson, M. M. Gottesman, and I. Pastan. The human multidrug resistance (mdr1) gene. cDNA cloning and transcription initiation. J Biol Chem 262:505-8 (1987).
102. U. Hoffmann and H. K. Kroemer. The ABC transporters MDR1 and MRP2: multiple functions in disposition of xenobiotics and drug resistance. Drug Metab Rev 36: 669-701 (2004).
103. C. Pauli-Magnus and D. L. Kroetz. Functional implications of genetic polymorphisms in the multidrug resistance gene MDR1 (ABCB1). Pharm Res 21: 904-13 (2004).
104. F. Thiebaut, T. Tsuruo, H. Hamada, M. M. Gottesman, I. Pastan, and M. C. Willingham. Cellular localization of the multidrug-resistance gene product P- glycoprotein in normal hu-man tissues. Proc Natl Acad Sci U S A 84: 7735-8 (1987).
105. A. H. Schinkel, U. Mayer, E. Wagenaar, C. A. Mol, L. van Deemter, J. J. Smit, M. A. van der Valk, A. C. Voordouw, H. Spits, O. van Tellingen, J. M. Zijlmans, W. E. Fibbe, and P. Borst. Normal viability and altered pharmacokinetics in mice lacking mdr1-type (drug-transporting) P-glycoproteins. Proc Natl Acad Sci U S A 94: 4028-33 (1997).
106. A. H. Schinkel, E. Wagenaar, L. van Deemter, C. A. Mol, and P. Borst. Absence of the mdr1a P-Glycoprotein in mice affects tissue distribution and pharmacokinetics of dexamethasone, di-goxin, and cyclosporin A. J Clin Invest 96: 1698-705 (1995).
107. A. Seelig. A general pattern for substrate recognition by P-glycoprotein. Eur J Biochem 251:252-61 (1998).
108. A. Seelig and E. Landwojtowicz. Structure-activity relationship of P-glycoprotein substrates and modifiers. Eur J Pharm Sci 12: 31-40 (2000).
109. J. Hunter, B. H. Hirst, and N. L. Simmons. Epithelial secretion of vinblastine by human intes-tinal adenocarcinoma cell (HCT-8 and T84) layers expressing P-glycoprotein. Br J Cancer 64:437-44 (1991).
110. J. Hunter, B. H. Hirst, and N. L. Simmons. Drug absorption limited by P-glycoprotein-mediated secretory drug transport in human intestinal epithelial Caco-2 cell layers. Pharm Res10: 743-9 (1993).
111. U. Mayer, E. Wagenaar, J. H. Beijnen, J. W. Smit, D. K. Meijer, J. van Asperen, P. Borst, and A. H. Schinkel. Substantial excretion of digoxin via the intestinal mucosa and prevention of long-term digoxin accumulation in the brain by the mdr 1a P-glycoprotein. Br J Pharmacol119: 1038-44. (1996).
112. G. Fricker, J. Drewe, J. Huwyler, H. Gutmann, and C. Beglinger. Relevance of p-glycoprotein for the enteral absorption of cyclosporin A: in vitro-in vivo correlation. Br J Pharmacol 118:1841-7. (1996).
113. U. I. Schwarz, T. Gramatte, J. Krappweis, R. Oertel, and W. Kirch. P-glycoprotein inhibitor erythromycin increases oral bioavailability of talinolol in humans. Int J Clin Pharmacol Ther38: 161-7 (2000).
114. X. Cao, L. X. Yu, C. Barbaciru, C. P. Landowski, H. C. Shin, S. Gibbs, H. A. Miller, G. L. Amidon, and D. Sun. Permeability dominates in vivo intestinal absorption of P-gp substrate with high solubility and high permeability. Mol Pharm 2: 329-40 (2005).

61
115. W. L. Chiou, S. M. Chung, T. C. Wu, and C. Ma. A comprehensive account on the role of efflux transporters in the gastrointestinal absorption of 13 commonly used substrate drugs in humans. Int J Clin Pharmacol Ther 39: 93-101. (2001).
116. W. L. Chiou, C. Ma, S. M. Chung, and T. C. Wu. An alternative hypothesis to involvement of intestinal P-glycoprotein as the cause for digoxin oral bioavailability enhancement by ta-linolol. Clin Pharmacol Ther 69: 79-81 (2001).
117. D. K. Meijer and H. Lennernas. EUFEPS conference on drug transporters at Copenhagen: integrative approaches in ADME research. Eur J Pharm Sci 26: 130-43 (2005).
118. L. Z. Benet, C. L. Cummins, and C. Y. Wu. Transporter-enzyme interactions: implications for predicting drug-drug interactions from in vitro data. Curr Drug Metab 4: 393-8 (2003).
119. R. Ralhan, R. K. Swain, S. Agarwal, J. Kaur, N. Nath, G. Sarkar, M. Mathur, and N. K. Shukla. P-glycoprotein is positively correlated with p53 in human oral pre-malignant and ma-lignant lesions and is associated with poor prognosis. Int J Cancer 84: 80-5 (1999).
120. J. Fellay, C. Marzolini, E. R. Meaden, D. J. Back, T. Buclin, J. P. Chave, L. A. Decosterd, H. Furrer, M. Opravil, G. Pantaleo, D. Retelska, L. Ruiz, A. H. Schinkel, P. Vernazza, C. B. Eap, and A. Telenti. Response to antiretroviral treatment in HIV-1-infected individuals with allelic variants of the multidrug resistance transporter 1: a pharmacogenetics study. Lancet 359: 30-6. (2002).
121. C. Cordon-Cardo, J. P. O'Brien, D. Casals, L. Rittman-Grauer, J. L. Biedler, M. R. Melamed, and J. R. Bertino. Multidrug-resistance gene (P-glycoprotein) is expressed by endothelial cells at blood-brain barrier sites. Proc Natl Acad Sci U S A 86: 695-8 (1989).
122. A. J. Sadeque, C. Wandel, H. He, S. Shah, and A. J. Wood. Increased drug delivery to the brain by P-glycoprotein inhibition. Clin Pharmacol Ther 68: 231-7 (2000).
123. J. W. Smit, M. T. Huisman, O. van Tellingen, H. R. Wiltshire, and A. H. Schinkel. Absence or pharmacological blocking of placental P-glycoprotein profoundly increases fetal drug expo-sure. J Clin Invest 104: 1441-7 (1999).
124. S. Masuda, M. Goto, M. Okuda, Y. Ogura, F. Oike, T. Kiuchi, K. Tanaka, and K. Inui. Initial dosage adjustment for oral administration of tacrolimus using the intestinal MDR1 level in liv-ing-donor liver transplant recipients. Transplant Proc 37: 1728-9 (2005).
125. S. S. Brenner and U. Klotz. P-glycoprotein function in the elderly. Eur J Clin Pharmacol 60:97-102 (2004).
126. D. Kolwankar, D. D. Glover, J. A. Ware, and T. S. Tracy. Expression and function of ABCB1 and ABCG2 in human placental tissue. Drug Metab Dispos 33: 524-9 (2005).
127. S. Deferme and P. Augustijns. The effect of food components on the absorption of P-gp substrates: a review. J Pharm Pharmacol 55: 153-62 (2003).
128. D. Durr, B. Stieger, G. A. Kullak-Ublick, K. M. Rentsch, H. C. Steinert, P. J. Meier, and K. Fattinger. St John's Wort induces intestinal P-glycoprotein/MDR1 and intestinal and hepatic CYP3A4. Clin Pharmacol Ther 68: 598-604 (2000).
129. A. Johne, J. Brockmoller, S. Bauer, A. Maurer, M. Langheinrich, and I. Roots. Pharmacoki-netic interaction of digoxin with an herbal extract from St John's wort (Hypericum perfora-tum). Clin Pharmacol Ther 66: 338-45 (1999).
130. M. Piquette-Miller, A. Pak, H. Kim, R. Anari, and A. Shahzamani. Decreased expression and activity of P-glycoprotein in rat liver during acute inflammation. Pharm Res 15: 706-11 (1998).
131. C. L. Cummins, C. Y. Wu, and L. Z. Benet. Sex-related differences in the clearance of cyto-chrome P450 3A4 substrates may be caused by P-glycoprotein. Clin Pharmacol Ther 72: 474-89 (2002).
132. E. G. Schuetz, K. N. Furuya, and J. D. Schuetz. Interindividual variation in expression of P-glycoprotein in normal human liver and secondary hepatic neoplasms. J Pharmacol Exp Ther275: 1011-8 (1995).

62
133. M. F. Fromm, R. B. Kim, C. M. Stein, G. R. Wilkinson, and D. M. Roden. Inhibition of P-glycoprotein-mediated drug transport: A unifying mechanism to explain the interaction be-tween digoxin and quinidine [seecomments]. Circulation 99: 552-7 (1999).
134. K. Westphal, A. Weinbrenner, M. Zschiesche, G. Franke, M. Knoke, R. Oertel, P. Fritz, O. von Richter, R. Warzok, T. Hachenberg, H. M. Kauffmann, D. Schrenk, B. Terhaag, H. K. Kroemer, and W. Siegmund. Induction of P-glycoprotein by rifampin increases intestinal se-cretion of talinolol in human beings: a new type of drug/drug interaction. Clin Pharmacol Ther68: 345-55 (2000).
135. S. Hirata, S. Izumi, T. Furukubo, M. Ota, M. Fujita, T. Yamakawa, I. Hasegawa, H. Ohtani, and Y. Sawada. Interactions between clarithromycin and digoxin in patients with end-stage re-nal disease. Int J Clin Pharmacol Ther 43: 30-6 (2005).
136. K. Westphal, A. Weinbrenner, T. Giessmann, M. Stuhr, G. Franke, M. Zschiesche, R. Oertel, B. Terhaag, H. K. Kroemer, and W. Siegmund. Oral bioavailability of digoxin is enhanced by talinolol: evidence for involvement of intestinal P-glycoprotein. Clin Pharmacol Ther 68: 6-12 (2000).
137. M. F. Hebert, R. M. Fisher, C. L. Marsh, D. Dressler, and I. Bekersky. Effects of rifampin on tacrolimus pharmacokinetics in healthy volunteers. J Clin Pharmacol 39: 91-6 (1999).
138. J. H. Lin. Drug-drug interaction mediated by inhibition and induction of P-glycoprotein. Adv Drug Deliv Rev 55: 53-81 (2003).
139. B. Chowbay, S. Cumaraswamy, Y. B. Cheung, Q. Zhou, and E. J. Lee. Genetic polymor-phisms in MDR1 and CYP3A4 genes in Asians and the influence of MDR1 haplotypes on cyclosporin disposition in heart transplant recipients. Pharmacogenetics 13: 89-95 (2003).
140. S. Drescher, E. Schaeffeler, M. Hitzl, U. Hofmann, M. Schwab, U. Brinkmann, M. Eichel-baum, and M. F. Fromm. MDR1 gene polymorphisms and disposition of the P-glycoprotein substrate fexofenadine. Br J Clin Pharmacol 53: 526-34 (2002).
141. T. Gerloff, M. Schaefer, A. Johne, K. Oselin, C. Meisel, I. Cascorbi, and I. Roots. MDR1 genotypes do not influence the absorption of a single oral dose of 1 mg digoxin in healthy white males. Br J Clin Pharmacol 54: 610-6 (2002).
142. N. von Ahsen, M. Richter, C. Grupp, B. Ringe, M. Oellerich, and V. W. Armstrong. No Influence of the MDR-1 C3435T Polymorphism or a CYP3A4 Promoter Polymorphism (CYP3A4-V Allele) on Dose-adjusted Cyclosporin A Trough Concentrations or Rejection In-cidence in Stable Renal Transplant Recipients. Clin Chem 47: 1048-52. (2001).
143. L. A. Doyle and D. D. Ross. Multidrug resistance mediated by the breast cancer resistance protein BCRP (ABCG2). Oncogene 22: 7340-58 (2003).
144. M. Maliepaard, G. L. Scheffer, I. F. Faneyte, M. A. van Gastelen, A. C. Pijnenborg, A. H. Schinkel, M. J. van De Vijver, R. J. Scheper, and J. H. Schellens. Subcellular localization and distribution of the breast cancer resistance protein transporter in normal human tissues. CancerRes 61: 3458-64. (2001).
145. H. C. Cooray, C. G. Blackmore, L. Maskell, and M. A. Barrand. Localisation of breast cancer resistance protein in microvessel endothelium of human brain. Neuroreport 13: 2059-63 (2002).
146. J. W. Jonker, G. Merino, S. Musters, A. E. van Herwaarden, E. Bolscher, E. Wagenaar, E. Mesman, T. C. Dale, and A. H. Schinkel. The breast cancer resistance protein BCRP (ABCG2) concentrates drugs and carcinogenic xenotoxins into milk. Nat Med 11: 127-9 (2005).
147. E. Rocchi, A. Khodjakov, E. L. Volk, C. H. Yang, T. Litman, S. E. Bates, and E. Schneider. The product of the ABC half-transporter gene ABCG2 (BCRP/MXR/ABCP) is expressed in the plasma membrane. Biochem Biophys Res Commun 271: 42-6 (2000).
148. M. Suzuki, H. Suzuki, Y. Sugimoto, and Y. Sugiyama. ABCG2 transports sulfated conjugates of steroids and xenobiotics. J Biol Chem 278: 22644-9 (2003).

63
149. I. Ifergan, A. Shafran, G. Jansen, J. H. Hooijberg, G. L. Scheffer, and Y. G. Assaraf. Folate deprivation results in the loss of breast cancer resistance protein (BCRP/ABCG2) expression. A role for BCRP in cellular folate homeostasis. J Biol Chem 279: 25527-34 (2004).
150. S. Zhou, Y. Zong, P. A. Ney, G. Nair, C. F. Stewart, and B. P. Sorrentino. Increased expres-sion of the Abcg2 transporter during erythroid maturation plays a role in decreasing cellular protoporphyrin IX levels. Blood 105: 2571-6 (2005).
151. S. Zhou, J. D. Schuetz, K. D. Bunting, A. M. Colapietro, J. Sampath, J. J. Morris, I. Lagutina, G. C. Grosveld, M. Osawa, H. Nakauchi, and B. P. Sorrentino. The ABC transporter Bcrp1/ABCG2 is expressed in a wide variety of stem cells and is a molecular determinant of the side-population phenotype. Nat Med 7: 1028-34. (2001).
152. P. Krishnamurthy, D. D. Ross, T. Nakanishi, K. Bailey-Dell, S. Zhou, K. E. Mercer, B. Sarkadi, B. P. Sorrentino, and J. D. Schuetz. The stem cell marker Bcrp/ABCG2 enhances hy-poxic cell survival through interactions with heme. J Biol Chem 279: 24218-25 (2004).
153. A. E. van Herwaarden, E. Wagenaar, B. Karnekamp, G. Merino, J. W. Jonker, and A. H. Schinkel. Breast cancer resistance protein (Bcrp1/Abcg2) reduces systemic exposure of the dietary carcinogens aflatoxin B1, IQ and Trp-P-1 but also mediates their secretion into breast milk. Carcinogenesis (2005).
154. M. J. Zamek-Gliszczynski, K. A. Hoffmaster, X. Tian, R. Zhao, J. W. Polli, J. E. Humphreys, L. O. Webster, A. S. Bridges, J. C. Kalvass, and K. L. Brouwer. Multiple mechanisms are in-volved in the biliary excretion of acetaminophen sulfate in the rat: role of Mrp2 and Bcrp1. Drug Metab Dispos 33: 1158-65 (2005).
155. G. Merino, J. W. Jonker, E. Wagenaar, A. E. van Herwaarden, and A. H. Schinkel. The breast cancer resistance protein (BCRP/ABCG2) affects pharmacokinetics, hepatobiliary excretion, and milk secretion of the antibiotic nitrofurantoin. Mol Pharmacol 67: 1758-64 (2005).
156. M. Hirano, K. Maeda, S. Matsushima, Y. Nozaki, H. Kusuhara, and Y. Sugiyama. Involve-ment of BCRP (ABCG2) in the biliary excretion of pitavastatin. Mol Pharmacol (2005).
157. P. Pavek, G. Merino, E. Wagenaar, E. Bolscher, M. Novotna, J. W. Jonker, and A. H. Schinkel. Human breast cancer resistance protein: interactions with steroid drugs, hormones, the dietary carcinogen 2-amino-1-methyl-6-phenylimidazo(4,5-b)pyridine, and transport of cimetidine. J Pharmacol Exp Ther 312: 144-52 (2005).
158. C. Kondo, R. Onuki, H. Kusuhara, H. Suzuki, M. Suzuki, N. Okudaira, M. Kojima, K. Ishi-wata, J. W. Jonker, and Y. Sugiyama. Lack of improvement of oral absorption of ME3277 by prodrug formation is ascribed to the intestinal efflux mediated by breast cancer resistant pro-tein (BCRP/ABCG2). Pharm Res 22: 613-8 (2005).
159. Y. J. Lee, H. Kusuhara, J. W. Jonker, A. H. Schinkel, and Y. Sugiyama. Investigation of efflux transport of dehydroepiandrosterone sulfate and mitoxantrone at the mouse blood-brain bar-rier: a minor role of breast cancer resistance protein. J Pharmacol Exp Ther 312: 44-52 (2005).
160. P. Breedveld, D. Pluim, G. Cipriani, P. Wielinga, O. van Tellingen, A. H. Schinkel, and J. H. Schellens. The effect of Bcrp1 (Abcg2) on the in vivo pharmacokinetics and brain penetration of imatinib mesylate (Gleevec): implications for the use of breast cancer resistance protein and P-glycoprotein inhibitors to enable the brain penetration of imatinib in patients. Cancer Res65: 2577-82 (2005).
161. T. Ishikawa, A. Tamura, H. Saito, K. Wakabayashi, and H. Nakagawa. Pharmacogenomics of the human ABC transporter ABCG2: from functional evaluation to drug molecular design. Naturwissenschaften 1-13 (2005).
162. A. Sparreboom, W. J. Loos, H. Burger, T. M. Sissung, J. Verweij, W. D. Figg, K. Nooter, and H. Gelderblom. Effect of ABCG2 Genotype on the Oral Bioavailability of Topotecan. Cancer Biol Ther 4: (2005).
163. A. Sparreboom, H. Gelderblom, S. Marsh, R. Ahluwalia, R. Obach, P. Principe, C. Twelves, J. Verweij, and H. L. McLeod. Diflomotecan pharmacokinetics in relation to ABCG2 421C>A genotype. Clin Pharmacol Ther 76: 38-44 (2004).

64
164. Q. Zhou, A. Sparreboom, E. H. Tan, Y. B. Cheung, A. Lee, D. Poon, E. J. Lee, and B. Chow-bay. Pharmacogenetic profiling across the irinotecan pathway in Asian patients with cancer. Br J Clin Pharmacol 59: 415-24 (2005).
165. P. Breedveld, N. Zelcer, D. Pluim, O. Sonmezer, M. M. Tibben, J. H. Beijnen, A. H. Schinkel, O. van Tellingen, P. Borst, and J. H. Schellens. Mechanism of the pharmacokinetic interaction between methotrexate and benzimidazoles: potential role for breast cancer resistance protein in clinical drug-drug interactions. Cancer Res 64: 5804-11 (2004).
166. C. F. Stewart, M. Leggas, J. D. Schuetz, J. C. Panetta, P. J. Cheshire, J. Peterson, N. Daw, J. J. Jenkins, 3rd, R. Gilbertson, G. S. Germain, F. C. Harwood, and P. J. Houghton. Gefitinib en-hances the antitumor activity and oral bioavailability of irinotecan in mice. Cancer Res 64:7491-9 (2004).
167. A. L. Sesink, I. C. Arts, V. C. de Boer, P. Breedveld, J. H. Schellens, P. C. Hollman, and F. G. Russel. Breast cancer resistance protein (bcrp1/abcg2) limits net intestinal uptake of quercetin in rats by facilitating apical efflux of glucuronides. Mol Pharmacol 67: 1999-2006 (2005).
168. G. Merino, A. E. van Herwaarden, E. Wagenaar, J. W. Jonker, and A. H. Schinkel. Sex-dependent expression and activity of the ATP-binding cassette transporter breast cancer resis-tance protein (BCRP/ABCG2) in liver. Mol Pharmacol 67: 1765-71 (2005).
169. H. Lennernas. Intestinal drug absorption and bioavailability: beyond involvement of single transport function. J Pharm Pharmacol 55: 429-33 (2003).
170. P. Artursson, K. Palm, and K. Luthman. Caco-2 monolayers in experimental and theoretical predictions of drug transport. Adv Drug Deliv Rev 46: 27-43 (2001).
171. A. B. West, C. A. Isaac, J. M. Carboni, J. S. Morrow, M. S. Mooseker, and K. W. Barwick. Localization of villin, a cytoskeletal protein specific to microvilli, in human ileum and colon and in colonic neoplasms. Gastroenterology 94: 343-52 (1988).
172. C. S. Potten, C. Booth, G. L. Tudor, D. Booth, G. Brady, P. Hurley, G. Ashton, R. Clarke, S. Sakakibara, and H. Okano. Identification of a putative intestinal stem cell and early lineage marker; musashi-1. Differentiation 71: 28-41 (2003).
173. C. P. Zamber, J. K. Lamba, K. Yasuda, J. Farnum, K. Thummel, J. D. Schuetz, and E. G. Schuetz. Natural allelic variants of breast cancer resistance protein (BCRP) and their relation-ship to BCRP expression in human intestine. Pharmacogenetics 13: 19-28 (2003).
174. J. Taipalensuu, S. Tavelin, L. Lazorova, A. C. Svensson, and P. Artursson. Exploring the quantitative relationship between the level of MDR1 transcript, protein and function using di-goxin as a marker of MDR1-dependent drug efflux activity. Eur J Pharm Sci 21: 69-75 (2004).
175. K. Naruhashi, Y. Sai, I. Tamai, N. Suzuki, and A. Tsuji. PepT1 mRNA expression is induced by starvation and its level correlates with absorptive transport of cefadroxil longitudinally in the rat intestine. Pharm Res 19: 1417-23 (2002).
176. M. Wadelius, K. Sorlin, O. Wallerman, J. Karlsson, Q. Y. Yue, P. K. Magnusson, C. Wade-lius, and H. Melhus. Warfarin sensitivity related to CYP2C9, CYP3A5, ABCB1 (MDR1) and other factors. Pharmacogenomics J 4: 40-8 (2004).
177. P. J. Oefner and P. A. Underhill. DNA mutation detection using denaturing High-Performance Liquid Chromatography (DHPLC), Current Protocols in Human Genetics (1998), John Wiley & Sons, Inc, 1998, pp. 7.10.1-7.10.11.
178. C. Marck. 'DNA Strider': a 'C' program for the fast analysis of DNA and protein sequences on the Apple Macintosh family of computers. Nucleic Acids Res 16: 1829-36. (1988).
179. S. Schneider, Roessli, D., and Excoffier, L. Arlequin: A software for population genetics data analysis. Ver 2.000. Genetics and Biometry Lab, Dept. of Anthropology, University of Ge-neva. (2000).
180. Y. Honjo, C. A. Hrycyna, Q. W. Yan, W. Y. Medina-Perez, R. W. Robey, A. van De Laar, T. Litman, M. Dean, and S. E. Bates. Acquired mutations in the mxr/bcrp/abcp gene alter sub-strate specificity in mxr/bcrp/abcp-overexpressing cells. Cancer Res 61: 6635-9. (2001).

65
181. J. D. Allen, S. C. Jackson, and A. H. Schinkel. A mutation hot spot in the bcrp1 (abcg2) multidrug transporter in mouse cell lines selected for Doxorubicin resistance. Cancer Res 62:2294-9. (2002).
182. C. Kondo, H. Suzuki, M. Itoda, S. Ozawa, J. Sawada, D. Kobayashi, I. Ieiri, K. Mine, K. Ohtsubo, and Y. Sugiyama. Functional analysis of SNPs variants of BCRP/ABCG2. Pharm Res 21: 1895-903 (2004).
183. F. A. de Jong, S. Marsh, R. H. Mathijssen, C. King, J. Verweij, A. Sparreboom, and H. L. McLeod. ABCG2 pharmacogenetics: ethnic differences in allele frequency and assessment of influence on irinotecan disposition. Clin Cancer Res 10: 5889-94 (2004).
184. S. Colombo, N. Soranzo, M. Rotger, R. Sprenger, G. Bleiber, H. Furrer, T. Buclin, D. Gold-stein, L. Decosterd, and A. Telenti. Influence of ABCB1, ABCC1, ABCC2, and ABCG2 hap-lotypes on the cellular exposure of nelfinavir in vivo. Pharmacogenet Genomics 15: 599-608 (2005).
185. E. Iisalo. Clinical pharmacokinetics of digoxin. Clin Pharmacokinet 2: 1-16 (1977). 186. J. M. Kovarik, L. Rigaudy, M. Guerret, C. Gerbeau, and K. L. Rost. Longitudinal assessment
of a P-glycoprotein-mediated drug interaction of valspodar on digoxin. Clin Pharmacol Ther66: 391-400 (1999).
187. J. Rengelshausen, C. Goggelmann, J. Burhenne, K. D. Riedel, J. Ludwig, J. Weiss, G. Mikus, I. Walter-Sack, and W. E. Haefeli. Contribution of increased oral bioavailability and reduced nonglomerular renal clearance of digoxin to the digoxin-clarithromycin interaction. Br J Clin Pharmacol 56: 32-8 (2003).
188. L. Liu, E. Mak, R. G. Tirona, E. Tan, P. M. Novikoff, P. Wang, A. W. Wolkoff, and K. S. Pang. Vascular binding, blood flow, transporter, and enzyme interactions on the processing of digoxin in rat liver. J Pharmacol Exp Ther 315: 433-48 (2005).
189. T. Mikkaichi, T. Suzuki, T. Onogawa, M. Tanemoto, H. Mizutamari, M. Okada, T. Chaki, S. Masuda, T. Tokui, N. Eto, M. Abe, F. Satoh, M. Unno, T. Hishinuma, K. Inui, S. Ito, J. Goto, and T. Abe. Isolation and characterization of a digoxin transporter and its rat homologue ex-pressed in the kidney. Proc Natl Acad Sci U S A 101: 3569-74 (2004).
190. T. Kodawara, S. Masuda, H. Wakasugi, Y. Uwai, T. Futami, H. Saito, T. Abe, and K. Inu. Organic anion transporter oatp2-mediated interaction between digoxin and amiodarone in the rat liver. Pharm Res 19: 738-43 (2002).
191. S. S. Rathore, J. P. Curtis, Y. Wang, M. R. Bristow, and H. M. Krumholz. Association of serum digoxin concentration and outcomes in patients with heart failure. Jama 289: 871-8 (2003).
192. T. Nakamura, M. Kakumoto, K. Yamashita, K. Takara, Y. Tanigawara, T. Sakaeda, and K. Okumura. Factors influencing the prediction of steady state concentrations of digoxin. Biol Pharm Bull 24: 403-8 (2001).
193. A. Ekbom. The epidemiology of IBD: a lot of data but little knowledge. How shall we pro-ceed? Inflamm Bowel Dis 10 Suppl 1: S32-4 (2004).
194. N. Albermann, F. H. Schmitz-Winnenthal, K. Z'Graggen, C. Volk, M. M. Hoffmann, W. E. Haefeli, and J. Weiss. Expression of the drug transporters MDR1/ABCB1, MRP1/ABCC1, MRP2/ABCC2, BCRP/ABCG2, and PXR in peripheral blood mononuclear cells and their re-lationship with the expression in intestine and liver. Biochem Pharmacol 70: 949-58 (2005).
195. J. S. Coon, Y. Z. Wang, S. D. Bines, P. N. Markham, A. S. Chong, and H. M. Gebel. Mul-tidrug resistance activity in human lymphocytes. Hum Immunol 32: 134-40 (1991).
196. G. Hartmann, H. Kim, and M. Piquette-Miller. Regulation of the hepatic multidrug resistance gene expression by endotoxin and inflammatory cytokines in mice. Int Immunopharmacol 1:189-99 (2001).
197. M. Buyse, G. Radeva, A. Bado, and R. Farinotti. Intestinal inflammation induces adaptation of P-glycoprotein expression and activity. Biochem Pharmacol 69: 1745-54 (2005).

66
198. G. Hartmann, A. K. Cheung, and M. Piquette-Miller. Inflammatory cytokines, but not bile acids, regulate expression of murine hepatic anion transporters in endotoxemia. J Pharmacol Exp Ther 303: 273-81 (2002).
199. M. Sukhai, A. Yong, A. Pak, and M. Piquette-Miller. Decreased expression of P-glycoprotein in interleukin-1beta and interleukin-6 treated rat hepatocytes. Inflamm Res 50: 362-70 (2001).
200. M. Schwab and U. Klotz. Pharmacokinetic considerations in the treatment of inflammatory bowel disease. Clin Pharmacokinet 40: 723-51 (2001).
201. E. Liang, J. Proudfoot, and M. Yazdanian. Mechanisms of transport and structure-permeability relationship of sulfasalazine and its analogs in Caco-2 cell monolayers. Pharm Res 17: 1168-74 (2000).
202. J. Van Der Heijden, M. C. De Jong, B. A. Dijkmans, W. F. Lems, R. Oerlemans, I. Kathmann, C. G. Schalkwijk, G. L. Scheffer, R. J. Scheper, and G. Jansen. Development of sulfasalazine resistance in human T cells induces expression of the multidrug resistance transporter ABCG2 (BCRP) and augmented production of TNFalpha. Ann Rheum Dis 63: 138-143 (2004).
203. M. Qadir, K. L. O'Loughlin, S. M. Fricke, N. A. Williamson, W. R. Greco, H. Minderman, and M. R. Baer. Cyclosporin A is a broad-spectrum multidrug resistance modulator. Clin Can-cer Res 11: 2320-6 (2005).
204. R. J. Farrell, A. Murphy, A. Long, S. Donnelly, A. Cherikuri, D. O'Toole, N. Mahmud, P. W. Keeling, D. G. Weir, and D. Kelleher. High multidrug resistance (P-glycoprotein 170) expres-sion in inflammatory bowel disease patients who fail medical therapy. Gastroenterology 118:279-88 (2000).
205. K. Dilger, M. Schwab, and M. F. Fromm. Identification of budesonide and prednisone as substrates of the intestinal drug efflux pump P-glycoprotein. Inflamm Bowel Dis 10: 578-83 (2004).
206. H. Saitoh, M. Hatakeyama, O. Eguchi, M. Oda, and M. Takada. Involvement of intestinal P-glycoprotein in the restricted absorption of methylprednisolone from rat small intestine. JPharm Sci 87: 73-5 (1998).
207. C. M. Panwala, J. C. Jones, and J. L. Viney. A novel model of inflammatory bowel disease: mice deficient for the multiple drug resistance gene, mdr1a, spontaneously develop colitis. JImmunol 161: 5733-44 (1998).
208. M. Schwab, E. Schaeffeler, C. Marx, M. F. Fromm, B. Kaskas, J. Metzler, E. Stange, H. Herfarth, J. Schoelmerich, M. Gregor, S. Walker, I. Cascorbi, I. Roots, U. Brinkmann, U. M. Zanger, and M. Eichelbaum. Association between the C3435T MDR1 gene polymorphism and susceptibility for ulcerative colitis. Gastroenterology 124: 26-33 (2003).
209. U. Klotz and M. Schwab. Topical delivery of therapeutic agents in the treatment of inflamma-tory bowel disease. Adv Drug Deliv Rev 57: 267-79 (2005).
210. J. Ebbesen, I. Buajordet, J. Erikssen, O. Brors, T. Hilberg, H. Svaar, and L. Sandvik. Drug-related deaths in a department of internal medicine. Arch Intern Med 161: 2317-23 (2001).
211. S. M. Huangand L. J. Lesko. Drug-drug, drug-dietary supplement, and drug-citrus fruit and other food interactions: what have we learned? J Clin Pharmacol 44: 559-69 (2004).
212. G. Alvan, L. Bertilsson, M. L. Dahl, M. Ingelman-Sundberg, and F. Sjoqvist. Moving toward genetic profiling in patient care: the scope and rationale of pharmacogenetic/ecogenetic inves-tigation. Drug Metab Dispos 29: 580-5 (2001).

