interlinking various personal health applications - … various...various personal health through...
TRANSCRIPT

Various Personal Health
through the WebApplications
Interlinking
Sukwha����������� ������������������ Kim,����������� ������������������ MD,����������� ������������������ PhD
Second Annual OSEHRA Summit & WorkshopSession: Open Source Technologies in Healthcare
Friday, September 6, 2013
Director,����������� ������������������ Department����������� ������������������ of����������� ������������������ Plastic����������� ������������������ Surgery,����������� ������������������ Seoul����������� ������������������ National����������� ������������������ University����������� ������������������ Hospital
“COPERNICAN REVOLUTION” DEMANDS A NEW BREED OF HEALTH INFORMATION SYSTEM
2Benson, T. (2009). Principles of Health Interoperability HL7 and SNOMED, Springer.
“The patient is the sole reason for healthcare activity, and so we should focus on meeting the patient’s needs. [...] Healthcare is changing from a paternalistic model to one of partnership between patients and healthcare professionals.”
“In the traditional healthcare model, care was based around discrete visits and episodes of care. [...] This model is disappearing fast, but we still rely on information systems that were originally conceived and designed for that environment.”
- Tim Benson
E-PATIENTS: HERE COMES HEALTH
3
- Dr. Tom Ferguson
• engaged when they seek to access their own health information
• enabled when they have access to their own health information
• equipped when they understand their own health information
• then empowered to achieve self-management of their care
1943-2006
Ferguson, T. (2007). e-Patients: How they can help us heal health care. Society for Participatory Medicine.
QUANTIFIED SELF: KNOW THYSELF
4
“Quantified Self is a collaboration of users and tool makers,who share an interest in self knowledge through self-tracking.”
The Quanti!ed Self; http://quanti!edself.com/
- Kevin Kelly - - Gary Wolf -

“DOES IT WORK FOR ME?” IS MORE IMPORTANT THAN “DOES IT WORK ON AVERAGE?”
5
• This guy measured his arithmetic speed daily:• how fast he does simple arithmetic problems, such as 3+4.• Several years ago, he discovered that butter — more precisely,
substitution of butter for port fat — made him faster.
- Prof. Seth Robert -
Seth’s Blog; http://blog.sethroberts.net/

DIFFERENT NEEDS, DIFFERENT PREFERENCES, AND DIFFERENT APPLICATIONS
6Gandhi, M. and Tecco, H. (2013). 2012 Digital Health Funding Report. Rock Health.

THERE IS NO ‘ONE-SIZE-FITS-ALL’ SOLUTION IN HEALTH CARE
7

THERE’S AN APP FOR THAT
8Estrin, D. and Sim, I. (2010). Open mHealth Architecture: An Engine for Health Care Innovation. Science Magazine, 330(6005):759-760.
“mHealth is emerging as
serving narrow, albeit valuable, needs, and thus coulda patchwork of incompatible applications
benefit from more coordinated development.”
(“apps”)
- Deborah Estrin and Ida Sim
LIQUIDITY OF DATA
9
“A prerequisite of Personal Health Records (PHR) systems is
- Tim Bensondata liquidity using open standards.”
Benson, T. (2009). Principles of Health Interoperability HL7 and SNOMED, Springer.

HOUR GLASS ARCHITECTURE
10Estrin, D. and Sim, I. (2010). Open mHealth Architecture: An Engine for Health Care Innovation. Science Magazine, 330(6005):759-760.
Mandl, K.D. and Kohane, I.S. (2009). No Small Change for the Health Information Economy. New England Journal of Medicine, 360(13):1278-1281.
“Flexibility is critical, since the system will have to function under new policies and in the service of new health care delivery mechanisms, and it will need to incorporate
emerging information technologies on an ongoing basis.”- Kenneth D. Mandl and Isaac S. Kohane

“ESCAPING THE EHR TRAP”
11Mandl, K.D. and Kohane, I.S. (2009). No Small Change for the Health Information Economy. New England Journal of Medicine, 360(13):1278-1281.
“Only a small subset of loosely coupled information technologies
- Kenneth D. Mandl and Isaac S. Kohane
need to be highly specific to health care. Many components can be generic.”
THE WORLD WIDE WEB IS THE MOST SUCCESSFUL DISTRIBUTED SYSTEM
12Jacobs, I. and Walsh, N. (2004). Architecture of the World Wide Web, Volume One. W3C.Costello, R.L. (2002). REST(Representational State Transfer). XML Technologies Course.
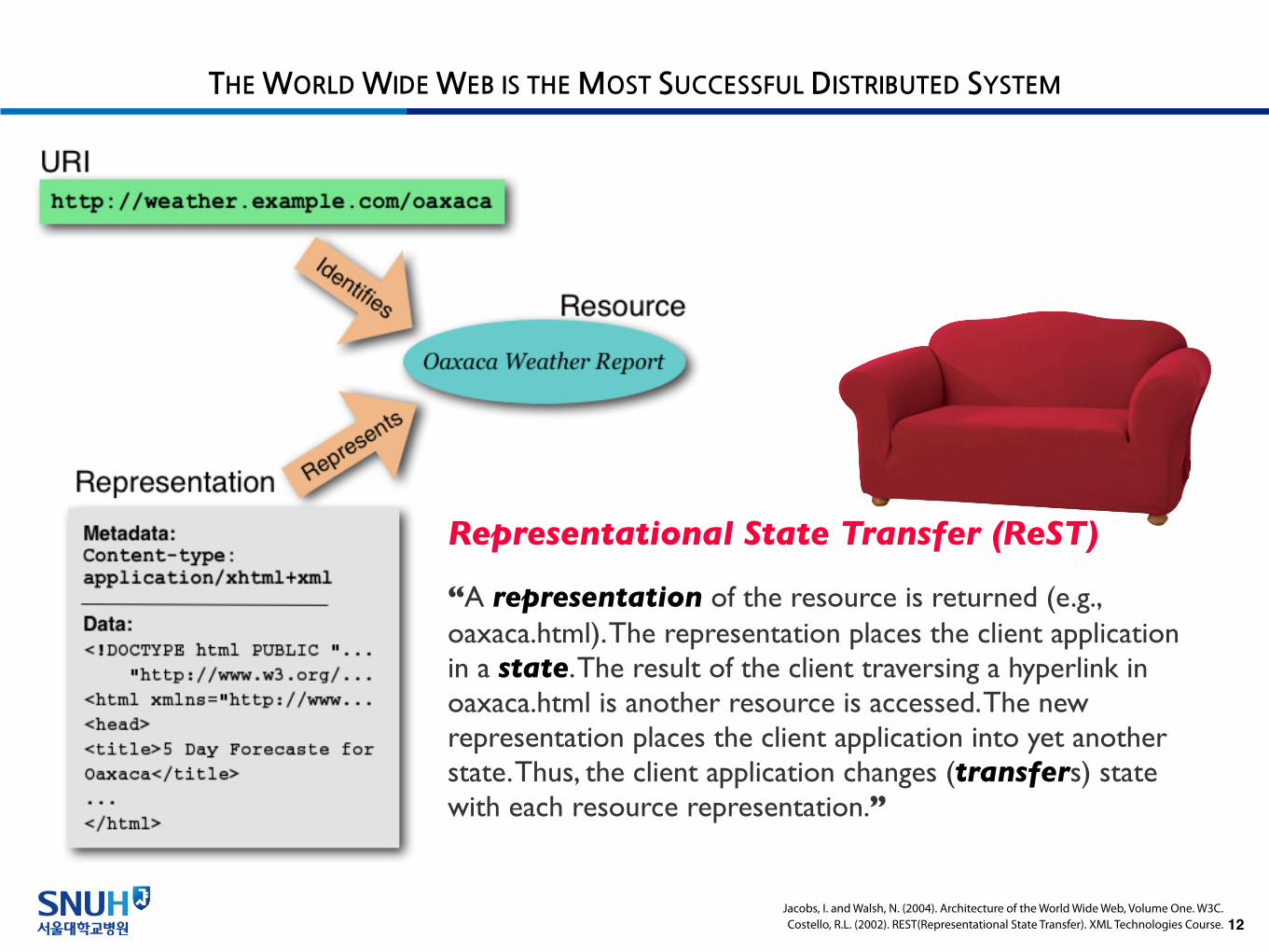
“A representation of the resource is returned (e.g., oaxaca.html). The representation places the client application in a state. The result of the client traversing a hyperlink in oaxaca.html is another resource is accessed. The new representation places the client application into yet another state. Thus, the client application changes (transfers) state with each resource representation.”
Representational State Transfer (ReST)
EXISTING OPEN SOURCE SOFTWARE & STANDARDS
13
APACHEHTTP SERVER
OAUTH
NOT ONLY OPEN SOURCE BUT ALSO OPEN STANDARDS
14Nicolas Rougier; http://www.loria.fr/~rougier/
“POSIX, an acronym for “Portable Operating System Interface”, is a family of standards specified by the IEEE for maintaining compatibility between operating systems. POSIX defines the application programming interface (API), along with command line shells and utility interfaces, for software compatibility with variants of Unix and other operating systems.”

OPEN STANDARDS FOR HEALTH INFORMATION INTEROPERABILITY
15
“Blue Button+ is a blueprint for the structured and secure transmission of personal health data on behalf of an individual consumer. It meets and builds on the view, download, and transmit requirements in Meaningful Use Stage 2 for certified EHR technology.”
HHS (2013). Introducing Blue Button +. HHS.gov/DigitalStrategy.ONC's Standards and Interoperability Framework (2013). Blue Button+ Implementation Guide.

THE RECOMMENDED STANDARD FOR REPRESENTING THE PATIENT HEALTH RECORD
16
“The Consolidated CDA is a XML-based standard that specifies the encoding, structure, and semantics of a clinical document. Blue Button adopts the requirements for sections and fields from Meaningful Use Stage 2.”
ONC's Standards and Interoperability Framework (2013). Blue Button+ Implementation Guide.
STANDARDIZED CODING SYSTEMS
17
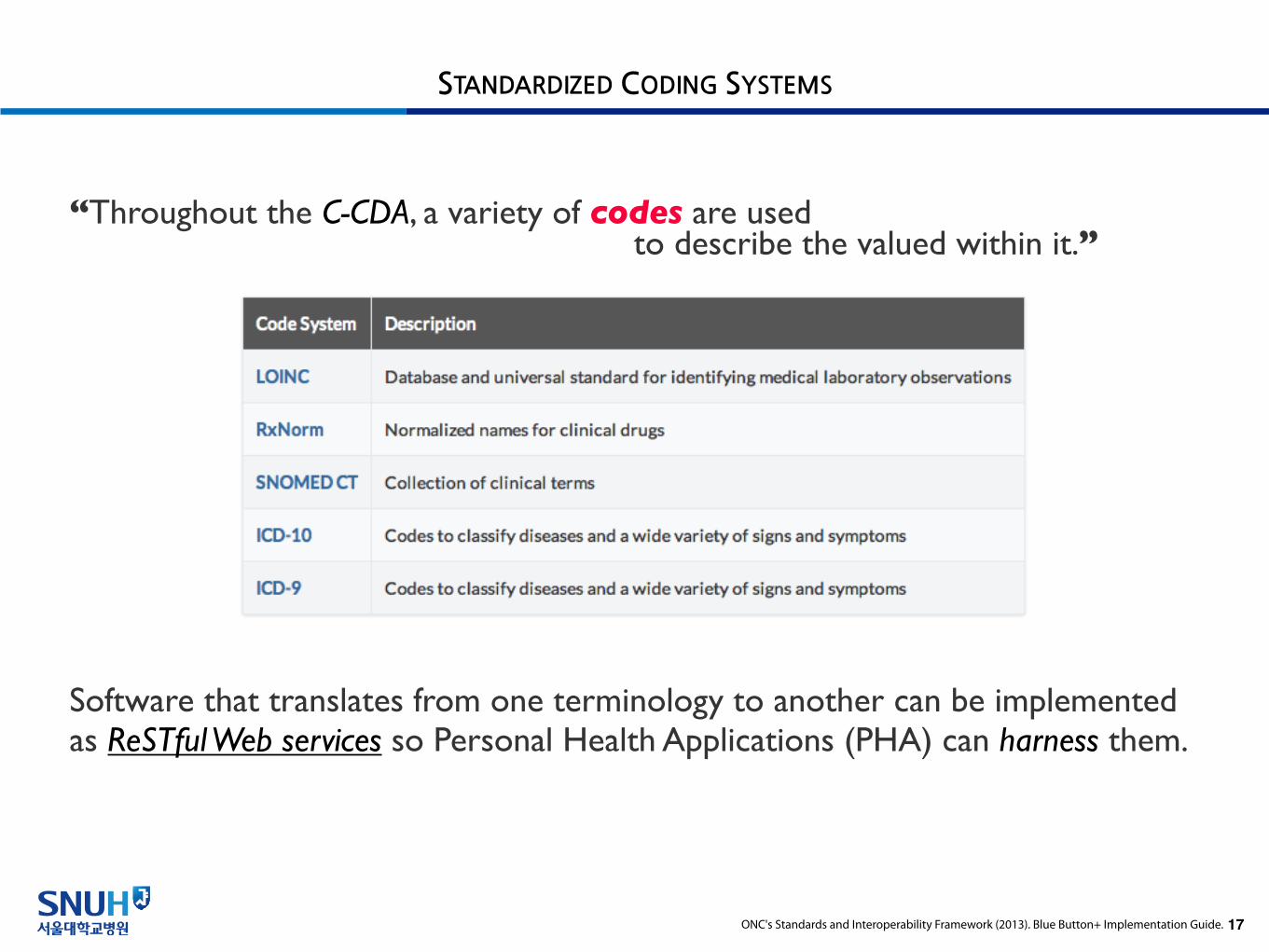
“Throughout the C-CDA, a variety of codes are usedto describe the valued within it.”
Software that translates from one terminology to another can be implemented as ReSTful Web services so Personal Health Applications (PHA) can harness them.
ONC's Standards and Interoperability Framework (2013). Blue Button+ Implementation Guide.
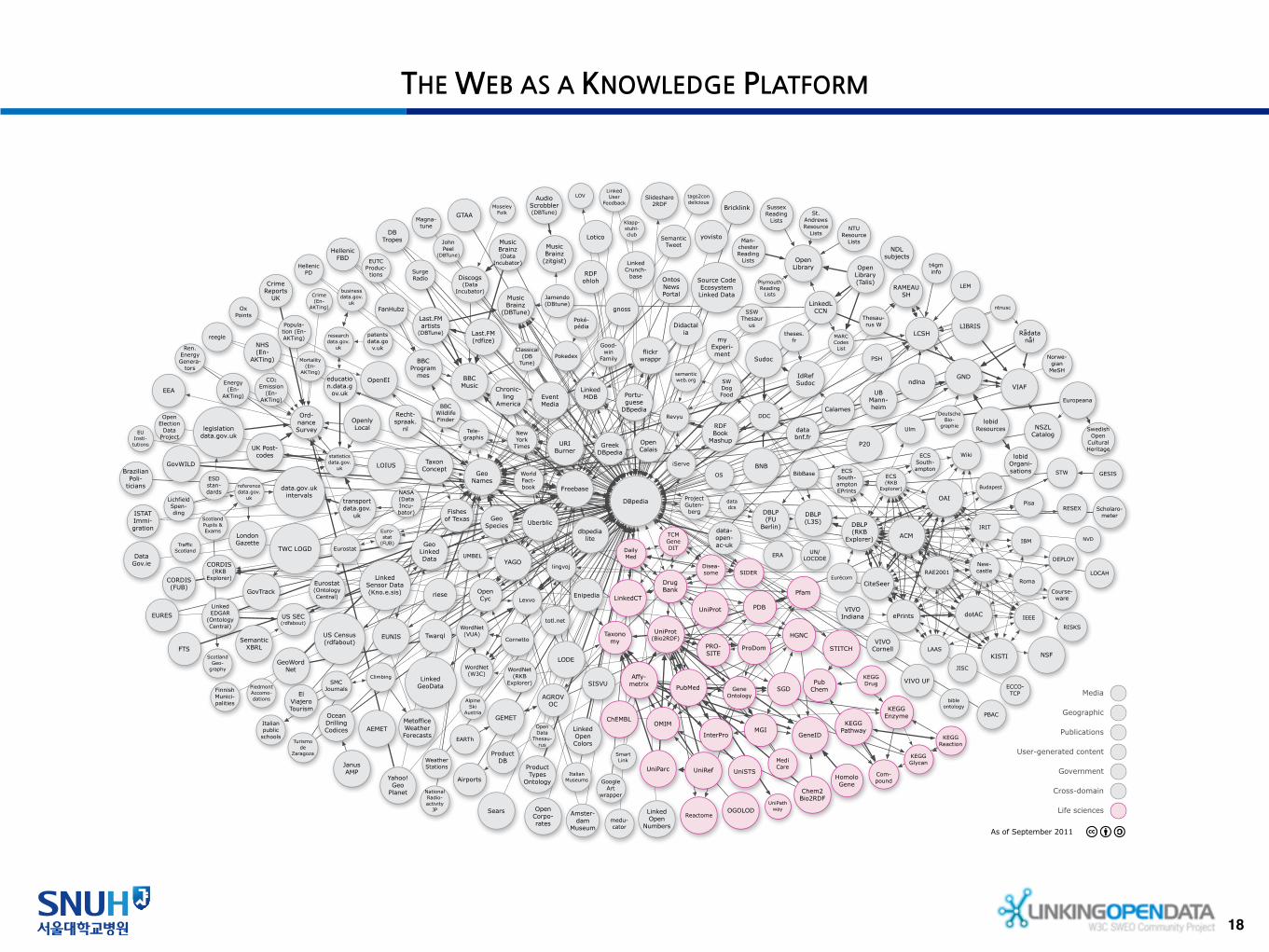
THE WEB AS A KNOWLEDGE PLATFORM
18
MusicBrainz
(zitgist)
P20
Turismo de
Zaragoza
yovisto
Yahoo! Geo
Planet
YAGO
World Fact-book
El ViajeroTourism
WordNet (W3C)
WordNet (VUA)
VIVO UF
VIVO Indiana
VIVO Cornell
VIAF
URIBurner
Sussex Reading
Lists
Plymouth Reading
Lists
UniRef
UniProt
UMBEL
UK Post-codes
legislationdata.gov.uk
Uberblic
UB Mann-heim
TWC LOGD
Twarql
transportdata.gov.
uk
Traffic Scotland
theses.fr
Thesau-rus W
totl.net
Tele-graphis
TCMGeneDIT
TaxonConcept
Open Library (Talis)
tags2con delicious
t4gminfo
Swedish Open
Cultural Heritage
Surge Radio
Sudoc
STW
RAMEAU SH
statisticsdata.gov.
uk
St. Andrews Resource
Lists
ECS South-ampton EPrints
SSW Thesaur
us
SmartLink
Slideshare2RDF
semanticweb.org
SemanticTweet
Semantic XBRL
SWDog Food
Source Code Ecosystem Linked Data
US SEC (rdfabout)
Sears
Scotland Geo-
graphy
ScotlandPupils &Exams
Scholaro-meter
WordNet (RKB
Explorer)
Wiki
UN/LOCODE
Ulm
ECS (RKB
Explorer)
Roma
RISKS
RESEX
RAE2001
Pisa
OS
OAI
NSF
New-castle
LAASKISTI
JISC
IRIT
IEEE
IBM
Eurécom
ERA
ePrints dotAC
DEPLOY
DBLP (RKB
Explorer)
Crime Reports
UK
Course-ware
CORDIS (RKB
Explorer)CiteSeer
Budapest
ACM
riese
Revyu
researchdata.gov.
ukRen. Energy Genera-
tors
referencedata.gov.
uk
Recht-spraak.
nl
RDFohloh
Last.FM (rdfize)
RDF Book
Mashup
Rådata nå!
PSH
Product Types
Ontology
ProductDB
PBAC
Poké-pédia
patentsdata.go
v.uk
OxPoints
Ord-nance Survey
Openly Local
Open Library
OpenCyc
Open Corpo-rates
OpenCalais
OpenEI
Open Election
Data Project
OpenData
Thesau-rus
Ontos News Portal
OGOLOD
JanusAMP
Ocean Drilling Codices
New York
Times
NVD
ntnusc
NTU Resource
Lists
Norwe-gian
MeSH
NDL subjects
ndlna
myExperi-ment
Italian Museums
medu-cator
MARC Codes List
Man-chester Reading
Lists
Lotico
Weather Stations
London Gazette
LOIUS
Linked Open Colors
lobidResources
lobidOrgani-sations
LEM
LinkedMDB
LinkedLCCN
LinkedGeoData
LinkedCT
LinkedUser
FeedbackLOV
Linked Open
Numbers
LODE
Eurostat (OntologyCentral)
Linked EDGAR
(OntologyCentral)
Linked Crunch-
base
lingvoj
Lichfield Spen-ding
LIBRIS
Lexvo
LCSH
DBLP (L3S)
Linked Sensor Data (Kno.e.sis)
Klapp-stuhl-club
Good-win
Family
National Radio-activity
JP
Jamendo (DBtune)
Italian public
schools
ISTAT Immi-gration
iServe
IdRef Sudoc
NSZL Catalog
Hellenic PD
Hellenic FBD
PiedmontAccomo-dations
GovTrack
GovWILD
GoogleArt
wrapper
gnoss
GESIS
GeoWordNet
GeoSpecies
GeoNames
GeoLinkedData
GEMET
GTAA
STITCH
SIDER
Project Guten-berg
MediCare
Euro-stat
(FUB)
EURES
DrugBank
Disea-some
DBLP (FU
Berlin)
DailyMed
CORDIS(FUB)
Freebase
flickr wrappr
Fishes of Texas
Finnish Munici-palities
ChEMBL
FanHubz
EventMedia
EUTC Produc-
tions
Eurostat
Europeana
EUNIS
EU Insti-
tutions
ESD stan-dards
EARTh
Enipedia
Popula-tion (En-AKTing)
NHS(En-
AKTing) Mortality(En-
AKTing)
Energy (En-
AKTing)
Crime(En-
AKTing)
CO2 Emission
(En-AKTing)
EEA
SISVU
education.data.g
ov.uk
ECS South-ampton
ECCO-TCP
GND
Didactalia
DDC Deutsche Bio-
graphie
datadcs
MusicBrainz
(DBTune)
Magna-tune
John Peel
(DBTune)
Classical (DB
Tune)
AudioScrobbler (DBTune)
Last.FM artists
(DBTune)
DBTropes
Portu-guese
DBpedia
dbpedia lite
Greek DBpedia
DBpedia
data-open-ac-uk
SMCJournals
Pokedex
Airports
NASA (Data Incu-bator)
MusicBrainz(Data
Incubator)
Moseley Folk
Metoffice Weather Forecasts
Discogs (Data
Incubator)
Climbing
data.gov.uk intervals
Data Gov.ie
databnf.fr
Cornetto
reegle
Chronic-ling
America
Chem2Bio2RDF
Calames
businessdata.gov.
uk
Bricklink
Brazilian Poli-
ticians
BNB
UniSTS
UniPathway
UniParc
Taxonomy
UniProt(Bio2RDF)
SGD
Reactome
PubMedPub
Chem
PRO-SITE
ProDom
Pfam
PDB
OMIMMGI
KEGG Reaction
KEGG Pathway
KEGG Glycan
KEGG Enzyme
KEGG Drug
Com-pound
InterPro
HomoloGene
HGNC
Gene Ontology
GeneID
Affy-metrix
bible ontology
BibBase
FTS
BBC Wildlife Finder
BBC Program
mes BBC Music
Alpine Ski
Austria
LOCAH
Amster-dam
Museum
AGROVOC
AEMET
US Census (rdfabout)
As of September 2011
Media
Geographic
Publications
Government
Cross-domain
Life sciences
User-generated content
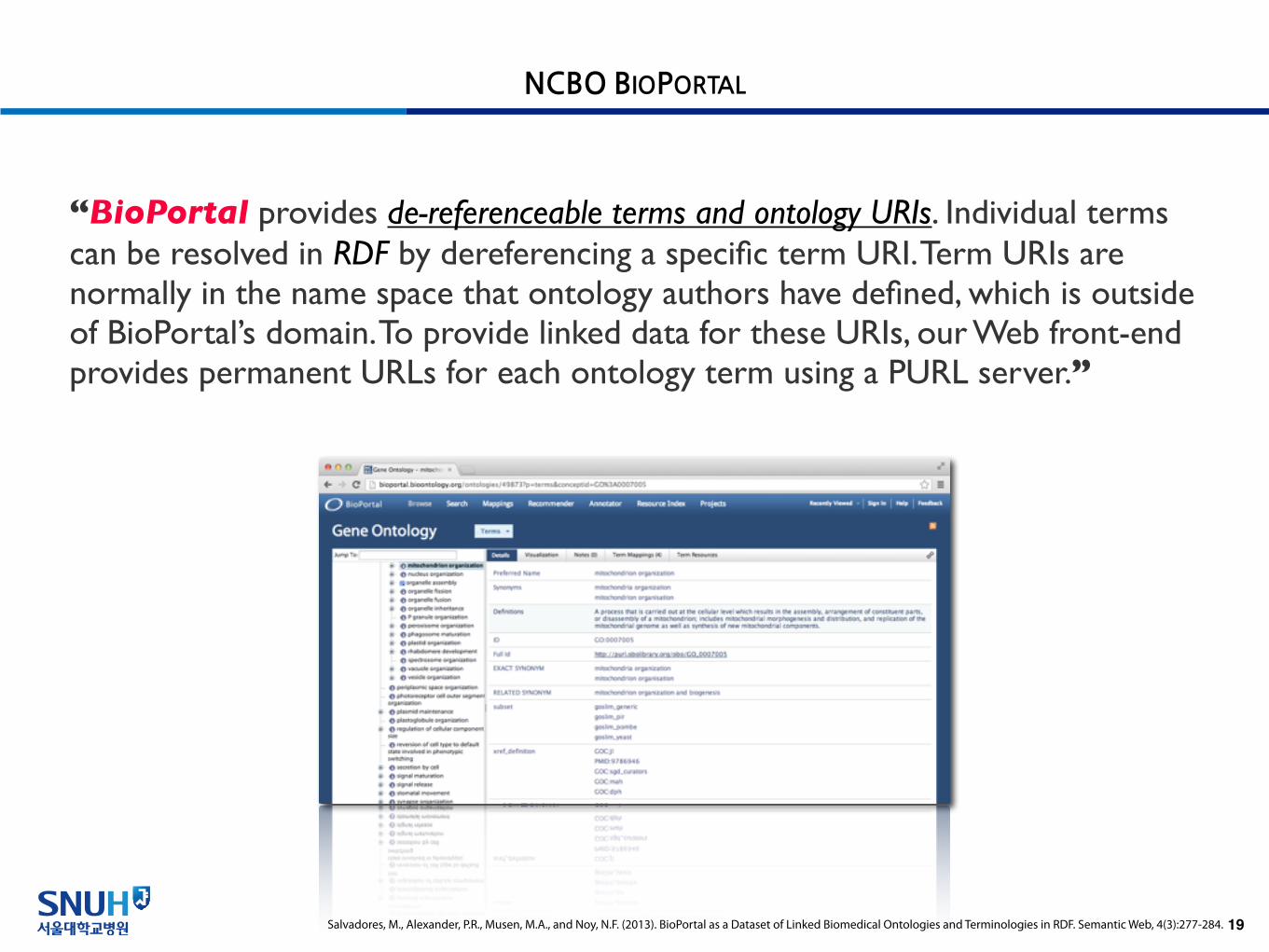
NCBO BIOPORTAL
19Salvadores, M., Alexander, P.R., Musen, M.A., and Noy, N.F. (2013). BioPortal as a Dataset of Linked Biomedical Ontologies and Terminologies in RDF. Semantic Web, 4(3):277-284.
“BioPortal provides de-referenceable terms and ontology URIs. Individual terms can be resolved in RDF by dereferencing a specific term URI. Term URIs are normally in the name space that ontology authors have defined, which is outside of BioPortal’s domain. To provide linked data for these URIs, our Web front-end provides permanent URLs for each ontology term using a PURL server.”

THE RECOMMENDED STANDARD FOR TRANSPORTING HEALTH INFORMATION
20ONC's Standards and Interoperability Framework (2013). Blue Button+ Implementation Guide.
“In alignment with Meaningful Use Stage 2 standards, Blue Button+ uses Direct protocols to securely transport health information from providers to third party applications. Direct uses SMTP, S/MIME, and X.509 certificates to achieve security, privacy, data integrity, and authentication of sender and receiver.”
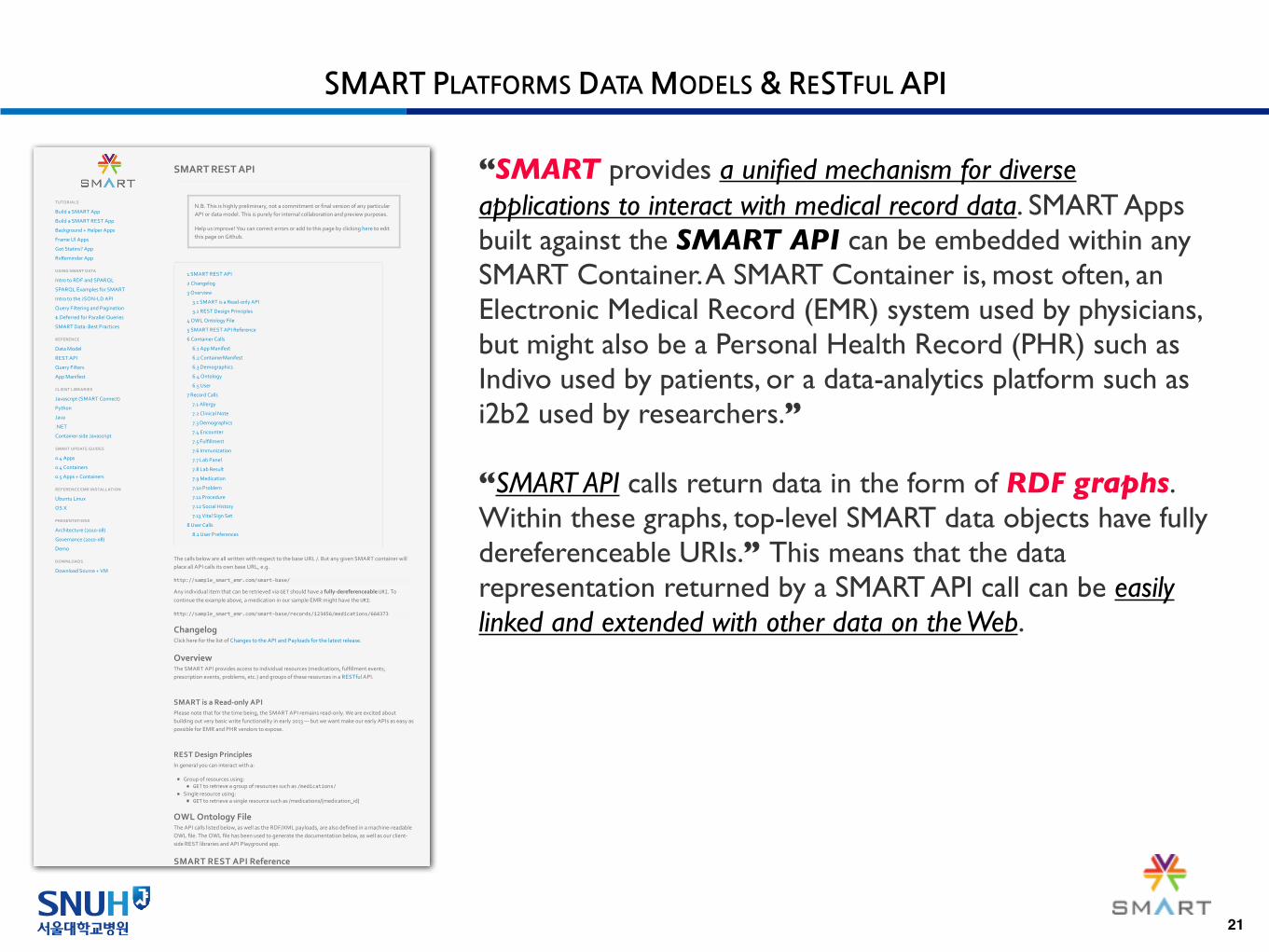
SMART PLATFORMS DATA MODELS & RESTFUL API
21
TUTORIALSTUTORIALS
Build&a&SMART&AppBuild&a&SMART&App
Build&a&SMART&REST&AppBuild&a&SMART&REST&App
Background&+&Helper&AppsBackground&+&Helper&Apps
Frame&UI&AppsFrame&UI&Apps
Got&Statins?&AppGot&Statins?&App
RxReminder&AppRxReminder&App
USING+SMART+DATAUSING+SMART+DATA
Intro&to&RDF&and&SPARQLIntro&to&RDF&and&SPARQL
SPARQL&Examples&for&SMARTSPARQL&Examples&for&SMART
Intro&to&the&JSONJLD&APIIntro&to&the&JSONJLD&API
Query&Filtering&and&PaginationQuery&Filtering&and&Pagination
$.Deferred&for&Parallel&Queries$.Deferred&for&Parallel&Queries
SMART&Data:&Best&PracticesSMART&Data:&Best&Practices
REFERENCEREFERENCE
Data&ModelData&Model
REST&APIREST&API
Query&FiltersQuery&Filters
App&ManifestApp&Manifest
CLIENT+LIBRARIESCLIENT+LIBRARIES
Javascript&(SMART&Connect)Javascript&(SMART&Connect)
PythonPython
JavaJava
.NET.NET
ContainerJside&JavascriptContainerJside&Javascript
SMART+UPDATE+GUIDESSMART+UPDATE+GUIDES
0.4&Apps0.4&Apps
0.4&Containers0.4&Containers
0.5&Apps&+&Containers0.5&Apps&+&Containers
REFERENCE+EMR+INSTALLATIONREFERENCE+EMR+INSTALLATION
Ubuntu&LinuxUbuntu&Linux
OS&XOS&X
PRESENTATIONSPRESENTATIONS
Architecture&(2010J08)Architecture&(2010J08)
Governance&(2010J08)Governance&(2010J08)
DemoDemo
DOWNLOADSDOWNLOADS
Download&Source&+&VMDownload&Source&+&VM
1&SMART&REST&API1&SMART&REST&API
2&Changelog2&Changelog
3&Overview3&Overview
3.1&SMART&is&a&ReadJonly&API3.1&SMART&is&a&ReadJonly&API
3.2&REST&Design&Principles3.2&REST&Design&Principles
4&OWL&Ontology&File4&OWL&Ontology&File
5&SMART&REST&API&Reference5&SMART&REST&API&Reference
6&Container&Calls6&Container&Calls
6.1&App&Manifest6.1&App&Manifest
6.2&ContainerManifest6.2&ContainerManifest
6.3&Demographics6.3&Demographics
6.4&Ontology6.4&Ontology
6.5&User6.5&User
7&Record&Calls7&Record&Calls
7.1&Allergy7.1&Allergy
7.2&Clinical&Note7.2&Clinical&Note
7.3&Demographics7.3&Demographics
7.4&Encounter7.4&Encounter
7.5&Fulfillment7.5&Fulfillment
7.6&Immunization7.6&Immunization
7.7&Lab&Panel7.7&Lab&Panel
7.8&Lab&Result7.8&Lab&Result
7.9&Medication7.9&Medication
7.10&Problem7.10&Problem
7.11&Procedure7.11&Procedure
7.12&Social&History7.12&Social&History
7.13&Vital&Sign&Set7.13&Vital&Sign&Set
8&User&Calls8&User&Calls
8.1&User&Preferences8.1&User&Preferences
SMART+REST+API
N.B.&This&is&highly&preliminary,¬&a&commitment&or&final&version&of&any&particularAPI&or&data&model.&This&is&purely&for&internal&collaboration&and&preview&purposes.
Help&us&improve!&You&can&correct&errors&or&add&to&this&page&by&clicking&here&to&editthis&page&on&Github.
The&calls&below&are&all&written&with&respect&to&the&base&URL&/.&But&any&given&SMART&container&willplace&all&API&calls&its&own&base&URL,&e.g.
http://sample_smart_emr.com/smart0base/
Any&individual&item&that&can&be&retrieved&via&GET&should&have&a&fully8dereferenceable&URI.&Tocontinue&the&example&above,&a&medication&in&our&sample&EMR&might&have&the&URI:
http://sample_smart_emr.com/smart0base/records/123456/medications/664373
ChangelogClick&here&for&the&list&of&Changes&to&the&API&and&Payloads&for&the&latest&release.
OverviewThe&SMART&API&provides&access&to&individual&resources&(medications,&fulfillment&events,prescription&events,&problems,&etc.)&and&groups&of&these&resources&in&a&RESTful&API.
SMART+is+a+Read8only+APIPlease¬e&that&for&the&time&being,&the&SMART&API&remains&readJonly.&We&are&excited&aboutbuilding&out&very&basic&write&functionality&in&early&2013&—&but&we&want&make&our&early&APIs&as&easy&aspossible&for&EMR&and&PHR&vendors&to&expose.
REST+Design+PrinciplesIn&general&you&can&interact&with&a:
Group&of&resources&using:GET&to&retrieve&a&group&of&resources&such&as&/medications/
Single&resource&using:GET&to&retrieve&a&single&resource&such&as&/medications/{medication_id}
OWL+Ontology+FileThe&API&calls&listed&below,&as&well&as&the&RDF/XML&payloads,&are&also&defined&in&a&machineJreadableOWL&file.&The&OWL&file&has&been&used&to&generate&the&documentation&below,&as&well&as&our&clientJside&REST&libraries&and&API&Playground&app.
SMART+REST+API+Reference
“SMART provides a unified mechanism for diverse applications to interact with medical record data. SMART Apps built against the SMART API can be embedded within any SMART Container. A SMART Container is, most often, an Electronic Medical Record (EMR) system used by physicians, but might also be a Personal Health Record (PHR) such as Indivo used by patients, or a data-analytics platform such as i2b2 used by researchers.”
“SMART API calls return data in the form of RDF graphs. Within these graphs, top-level SMART data objects have fully dereferenceable URIs.” This means that the data representation returned by a SMART API call can be easily linked and extended with other data on the Web.

OPEN SOURCE TOOLS AROUND OPEN STANDARDS
22
• C-CDA• SMART Platforms C-CDA Scorecard• NIST Validator Web App
• Direct Protocol• .Net Reference Implementation• Java Reference Implementation• NIST Validator Web App
• SMART Platforms ReSTful API• SMART App Javascript Libraries• SMART App Python Libraries• SMART App iOS Libraries• SMART App Java Libraries• SMART App .Net Libraries• SMART Container Javascript Libraries
• Indivo X ReSTful API• Indivo X App Python Libraries• Indivo X App iOS Libraries• Indivo X App Java Libraries
SMART C-CDA ScorecardSMART C-CDA Scorecard
Paste and go.<?xml version="1.0"?>
<?xml-stylesheet type="text/xsl" href="CDA.xsl"?><ClinicalDocument xmlns:xsi="http://www.w3.org/2001/XMLSchema-instance" xsi:schemaLocation="urn:hl7-org:v3 ../../../../../CDA%20Academy/ccda-schemas/ccda-schemas/infrastructure/cda/CDA_SDTC.xsd" xmlns="urn:hl7-org:v3" xmlns:cda="urn:hl7-org:v3" xmlns:sdtc="urn:hl7-org:sdtc"> <!--******************************************************** CDA Header******************************************************** --> <!-- CONF 16791 --> <realmCode code="US"/>
<!-- CONF 5361 --> <typeId root="2.16.840.1.113883.1.3" extension="POCD_HD000040"/>
<!-- US General Header Template --> <!-- CONF 5252 --> <templateId root="2.16.840.1.113883.10.20.22.1.1"/> <!-- *** Note: The next templateId, code and title will differ depending on what type of document is being sent. *** --> <!-- conforms to the document specific requirements --> <templateId root="2.16.840.1.113883.10.20.22.1.2"/>
<!-- CONF 5363 --> <id extension="Test CCDA" root="1.1.1.1.1.1.1.1.1"/>
<!-- CONF 5253 "CCD document" --> <code codeSystem="2.16.840.1.113883.6.1" codeSystemName="LOINC" code="34133-9" displayName="Summarization of Episode Note"/>
<!-- CONF 5254 --> <title>Primo Adult Health: Health Summary</title>
<!-- CONF 5256 --> <effectiveTime value="20121126000000-0000"/>
<!-- 5259 --> <confidentialityCode code="N" codeSystem="2.16.840.1.113883.5.25"/>
<!-- 5372 --> <languageCode code="en-US"/>
<!-- CONF 5266 --> <recordTarget>
<!-- CONF 5267 --> <patientRole>
<!-- CONF 5268--> <!-- Patient SSN recorded as an ID --> <id extension="123-456-7890" root="2.16.840.1.113883.4.1"/>
<!-- CONF 5271 --> <addr use="HP"> <!-- HP is "primary home" from codeSystem 2.16.840.1.113883.5.1119 --> <streetAddressLine>100 Marshall Lane</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22153</postalCode> <country>US</country> <!-- US is "United States" from ISO 3166-1 Country Codes: 1.0.3166.1 --> </addr>
<!-- CONF 5280 --> <telecom value="tel:+1(571)555-0189" use="HP"/> <!-- HP is "primary home" from HL7 AddressUse 2.16.840.1.113883.5.1119 -->
<!-- CONF 5283 --> <patient>
<!-- CONF 5284 --> <name use="L"> <!-- L is "Legal" from HL7 EntityNameUse 2.16.840.1.113883.5.45 --> <given>Nikolai</given> <family>Bellic</family> </name> <administrativeGenderCode code="M" codeSystem="2.16.840.1.113883.5.1" displayName="Male" codeSystemName="AdministrativeGender"/> <birthTime value="19330316"/> <maritalStatusCode code="M" displayName="Married" codeSystem="2.16.840.1.113883.5.2" codeSystemName="MaritalStatus"/> <religiousAffiliationCode code="1041" displayName="Roman Catholic" codeSystem="2.16.840.1.113883.5.1076" codeSystemName="ReligiousAffiliation"/> <raceCode code="2106-3" displayName="White" codeSystem="2.16.840.1.113883.6.238" codeSystemName="OMB Standards for Race and Ethnicity"/> <ethnicGroupCode code="2186-5" displayName="Not Hispanic or Latino" codeSystem="2.16.840.1.113883.6.238" codeSystemName="OMB Standards for Race and Ethnicity"/> <languageCommunication> <!-- CONF 5407: LanguageCode Code System 2.16.840.1.113883.1.11.11526 --> <languageCode code="en"/> <modeCode code="ESP" displayName="Expressed spoken" codeSystem="2.16.840.1.113883.5.60" codeSystemName="LanguageAbilityMode"/> </languageCommunication> </patient> </patientRole> </recordTarget> <author> <time value="20121126000000"/> <assignedAuthor> <!-- NPI 12345 --> <id extension="12345" root="2.16.840.1.113883.4.6"/> <code code="207QA0505X" codeSystem="2.16.840.1.113883.6.101" displayName="Adult Medicine" codeSystemName="NUCC"/> <addr> <streetAddressLine>1400 Main Street Ste G</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22150</postalCode> <country>US</country> </addr> <telecom use="WP" value="tel:+1(571)555-0179;ext=221"/> <assignedPerson> <name> <given>Raymond</given> <family>Boccino</family> <suffix>MD</suffix> </name> </assignedPerson> </assignedAuthor> </author> <dataEnterer> <assignedEntity> <id extension="678910" root="1.1.1.1.1.1.1.1.2"/> <code code="364SA2200X" displayName="Adult Health" codeSystem="2.16.840.1.113883.6.101" codeSystemName="NUCC"/> <addr> <streetAddressLine>1400 Main Street Ste G</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22150</postalCode> <country>US</country> </addr> <telecom use="WP" value="tel:+1(571)555-0179;ext=222"/> <assignedPerson> <name> <given>Mallory</given> <family>Bardas</family> <suffix>RN</suffix> </name> </assignedPerson> </assignedEntity> </dataEnterer> <custodian> <assignedCustodian> <representedCustodianOrganization> <id root="1.1.1.1.1.1.1.1.2"/> <name>Primo Adult Health</name> <telecom use="WP" value="tel:+1(571)555-0179"/> <addr> <streetAddressLine>1400 Main Street Ste G</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22150</postalCode> <country>US</country> </addr> </representedCustodianOrganization> </assignedCustodian> </custodian> <informationRecipient> <intendedRecipient> <!-- NPI 23456 --> <id extension="23456" root="2.16.840.1.113883.4.6"/> <informationRecipient> <name> <given>Bernard</given> <family>Crane</family> <suffix>MD</suffix> </name> </informationRecipient> <receivedOrganization> <name>Springfield Geriatric Associates</name> <telecom use="WP" value="tel:+1(571)555-0165"/> <addr> <streetAddressLine>202 County Line Rd</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22150</postalCode> <country>US</country> </addr> <standardIndustryClassCode code="207QG0300X" displayName="Geriatric Medicine" codeSystem="2.16.840.1.113883.6.101" codeSystemName="NUCC"/> </receivedOrganization> </intendedRecipient> </informationRecipient> <legalAuthenticator> <time value="20121126000000"/> <signatureCode code="S"/> <assignedEntity> <!-- NPI 12345 --> <id extension="12345" root="2.16.840.1.113883.4.6"/> <code code="207QA0505X" codeSystem="2.16.840.1.113883.6.101" displayName="Adult Medicine" codeSystemName="NUCC"/> <addr> <streetAddressLine>1400 Main Street Ste G</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22150</postalCode> <country>US</country> </addr> <telecom use="WP" value="tel:+1(571)555-0179;ext=221"/> <assignedPerson> <name> <given>Raymond</given> <family>Boccino</family> <suffix>MD</suffix> </name> </assignedPerson> </assignedEntity> </legalAuthenticator> <participant typeCode="IND"> <associatedEntity classCode="PRS"> <addr> <streetAddressLine>100 Marshall Lane</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22153</postalCode> <country>US</country> </addr> <telecom value="tel:+1(571)555-0189"/> <associatedPerson> <name> <given>Kathleen</given> <family>McReary</family> </name> </associatedPerson> </associatedEntity> </participant> <documentationOf> <serviceEvent classCode="PCPR"> <effectiveTime> <low value="19330316"/> <high value="20121126"/> </effectiveTime> <performer typeCode="PRF"> <assignedEntity> <!-- NPI 34567 --> <id extension="34567" root="2.16.840.1.113883.4.6"/> <code code="207RC0000X" codeSystem="2.16.840.1.113883.6.101" codeSystemName="NUCC" displayName="Cardiovascular Disease"/> <addr> <streetAddressLine>209 County Line Rd</streetAddressLine> <city>Springfield</city> <state>VA</state> <postalCode>22150</postalCode> </addr> <telecom use="WP" value="tel:+1(571)555-0155"/> <assignedPerson> <name> <given>Dwayne</given> <family>Forge</family> <suffix>MD</suffix> </name> </assignedPerson> </assignedEntity> </performer> <performer typeCode="PRF"> <functionCode code="PCP" displayName="Primary Care Physician" codeSystem="2.16.840.1.113883.5.88" codeSystemName="participationFunction"/> <assignedEntity> <!-- NPI 12345 --> <id extension="12345" root="2.16.840.1.113883.4.6"/> <code code="207QA0505X" codeSystem="2.16.840.1.113883.6.101"
Score me!
Your C-CDA's overallscore: 60%
Share your C-CDA with the SMART Community!Share your C-CDA with the SMART Community!P.S. We love works in progress :-)P.S. We love works in progress :-)
Collapse all Expand all TweetTweet 0
General 64% SNOMED CT, LOINC, and RxNorm codes validate against UMLS 0/5
points
Best Practice: Codes that claim to be from SNOMED CT, LOINC, and RxNorm should be present in UMLS2012AB.
Your Results:
3 of 68 codes weren't found in UMLS 2012ABYour code What now?
SNOMED CT:5962100 "Essential Hypertension" Check mapping
SNOMED CT:5582204 "Hyperlipidemia" Check mapping
SNOMED CT:49038010 "EKG" Check mapping
SNOMED CT, LOINC, and RxNorm codes match their displayName 3/3points
Best Practice: Codes in a C-CDA should assign a valid @displayName that reflects the meaning of the underlyingconcept. A best practice is to use preferred labels from UMLS.
Your Results:
1 of 61 codes didn't match their displayNameYour code Preferred
termWhat now?
SNOMEDCT:64572001
"Condition" "Disease" Seehttp://purl.bioontology.org/ontology/SNOMEDCT/64572001
Document uses sensible datetime precision 0/1points
Best Practice: C-CDA's datetimes should use ISO8601 strings to express appropriate precision.
Your Results:
1 issue.20121126000000-0000 Confirm this is the intended level of precision
Document uses official C-CDA templateIds whenever possible 5/5points
Best Practice: C-CDA's prescribed templateIds should be used whenever possible. Additional templateIdelements are allowed, but official C-CDA templateIds should always be present when they apply.
Physical units are valid UCUM expressions 3/3points
Best Practice: Any time a physical unit is used, it should be a valid UCUM expression
Lab Results 66% Lab Results coded with LOINC's top 2K codes 2/3
points
Best Practice: Lab results should be coded using LOINC. In pratice LOINC is huge, but 2000 codes cover 98%of real-world usage. This means that most results should be covered by the 2000+ most common LOINC codespublished by Regenstrief.
Your Results:
3 of 7 lab result codes weren't in the recommended value setNote: This may be normal, if this C-CDA document includes unusual labs for which no common LOINC codeexists. But look through the un-matched codes below to make sure you don't have a mapping error in your exportpipeline.
Recommended value set:
LOINC Top 2000 Codes
Your code The issue What now?
LOINC:18041-4
"Aortic valve Ejection [Time] byUS.doppler"
Not invalue set
Seehttp://purl.bioontology.org/ontology/LNC/18041-4
LOINC:18089-3
"AV Orifice Area US" Not invalue set
Seehttp://purl.bioontology.org/ontology/LNC/18089-3
LOINC:18844-1
"EKG impression Narrative" Not invalue set
Seehttp://purl.bioontology.org/ontology/LNC/18844-1
Medications100%
Medications coded with RxNorm SCD, SBD, GPCK, or BPCPK codes 3/3points
Best Practice: C-CDA medication lists should contain medications coded as RxNorm Semantic Clinical Drugs,Semantic Branded Drugs, and packs. This means prescribable products on the level of 'loratadine 10mg oraltablet'.)
Problems 83% Problems coded with HITSP's 16K SNOMED subset 2/3
points
Best Practice: Each problem in the problem list should be coded with a SNOMED code from the HITSP ProblemList valueset (OID 2.16.840.1.113883.3.88.12.3221.7.4).
Your Results:
4 of 8 problem codes weren't in the recommended value setsNote: This may be normal, if this C-CDA document includes unusual problems for which no appropriateSNOMED code exists. But look through the un-matched codes below to make sure you don't have a mappingerror in your export pipeline.
Recommended value sets:
HITSP Problem ListSNOMED CT CORE Problem List
Your code The issue What now?
SNOMEDCT:5962100
"EssentialHypertension"
Code notfound inUMLS2012AB
Check mapping
SNOMEDCT:5582204
"Hyperlipidemia" Code notfound inUMLS2012AB
Check mapping
SNOMEDCT:8957000
"Coronary ArteryDisease"
Obsolete Seehttp://purl.bioontology.org/ontology/SNOMEDCT/8957000
SNOMEDCT:238134004
"Generalizedobesity"
Not in valueset
Seehttp://purl.bioontology.org/ontology/SNOMEDCT/238134004
Problem statuses are internally consistent 3/3points
Best Practice: Each concern act should contain exactly one problem. If there is a status attached to the concernact as well as the problem, these should not contradict. A concern status of 'completed' is compatible with aproblem status of 'Resolved' or 'Inactive'. A concern status of 'active' is compatible with a problem status of'Active'.
Social History 0% Smoking Status Observations have the correct template ID 0/1
points
Best Practice: Smoking status observations should have template ID 2.16.840.1.113883.10.20.22.4.78
Structured Smoking Status Observations use correct SNOMED CT Codes N/A
Best Practice: Smoking Status obervations should be coded according to an explicit list of eight SNOMED CTCodes.
Only structured Smoking Status Observations are used N/A
Best Practice: Smoking status should be recorded in a discrete 'smoking status observation', not in the moregeneric, less-computable 'social history observation'.
Vitals 0% Vitals are represented using structured entries 0/5
points
Best Practice: Vitals in C-CDA should be represented with individual structured entries corresponding to BP,Heart Rate, etc.
Vitals are expressed with LOINC codes N/A
Best Practice: Vitals in C-CDA should be coded with LOINC. Specifically, with codes from the HITSP Vital SignResult value set.
Vitals are expressed with UCUM units N/A
Best Practice: Vitals in C-CDA should be represented with physical quantities that have appropriate UCUMcodes.
Your C-CDA.Beautiful.
Help improve the Scorecard!Four ways to help improve the SMART C-CDA Scorecard:1. Try out the Scorecard and tweet about it @SMARTHealthIT2. Share your sample C-CDA documents with the public3. Suggest new rubrics, or improvements to the existing ones4. Contribute code to improve the Scorecard
About the ScorecardThe SMART C-CDA Scorecard promotes best practices in C-CDA implementation by assessing keyaspects of the structured data found in invididual documents. It's a tool to help implementers gain visibilityinto how well and how often best practices are followed — and also to summarize progress with a roughquantitative assessment, highlighting improvements that can be made today.
Fills gaps and complements official validation toolsThe Scorecard runs alongside official C-CDA validation tools like the Transport Testing Tool provided byNIST and Model-Driven Health Tools. The official validation tools provide comprehensive assessment ofsyntactic conformance to the C-CDA specification, but they don't always enforce higher-level best practicesin C-CDA implementation. The Scorecard fills gaps and provides visibility into constraints missing from theofficial specifications, or features missing from the official validation tools. Our initial focus is on value setmembership for three key vocabularies used in C-CDA: LOINC, RxNorm, SNOMED CT.
Powered by SMART PlatformsVisit smartplatforms.org to learn more about the ONC-funded, SHARP III project.
© Harvard Medical School / Boston Children's Hospital, 2013. Source on GitHub.
Show me an example
Children’s Hospital Informatics Program
INDIVOHOME
RESEARCH &PUBLICATIONS
INDIVOCOLLABORATORS
LICENSE &TRADEMARK
DEVELOPERCOMMUNITY
TEAM &CONTACT INFO
INDIVO
CollaboratorsA number of research groups, non-profits, and for-profit companies have become Indivo EcosystemCollaborators. These groups are helping us develop and improve the Indivo ApplicationProgramming Interface (API), making the Indivo Platform extensible in many diverse use cases. Ifyou're interested in becoming an Indivo Ecosystem Collaborator, send us email.
Anvita HealthBiomedical Knowledge Engineering Laboratory, Seoul National UniversityChildhood Arthritis and Rheumatology Research Alliance (CARRA)Dossiai2b2Johnson and JohnsonLiveStrongMassachusetts Department of Public HealthMIT Media LabMyOscarOrange Research LabsRecombinant DataSHARP SMART Platforms ProjectSurescriptsThe Office of the National Coordinator for Health Information TechnologyTrialXTudiabetesNovartis
HEALTH 2.0 BLOGS ABOUT THEAPP CHALLENGE
Health 2.0 covers theSMART-Indivo App Challengeand its crowd-sourcing of appcreation.
SMART-INDIVO APPCHALLENGE
The SMART-Indivo AppChallenge has been posted tothe Health 2.0 DeveloperChallenge site.
O'REILLY RADAR COVERSINDIVO X USERS' CONFERENCE
Andy Oram from O’Reilly Mediaprovides insightful coverage ofthe Indivo X Users' Conference
INDIVO USERS' CONFERENCE:SLIDES AND RECAP
Slides from the 2012 Indivo XUsers' Conference are nowavailable! Click through for thelink, and a recap of the event.
More at our Blog.
© Children's Hospital Informatics Program
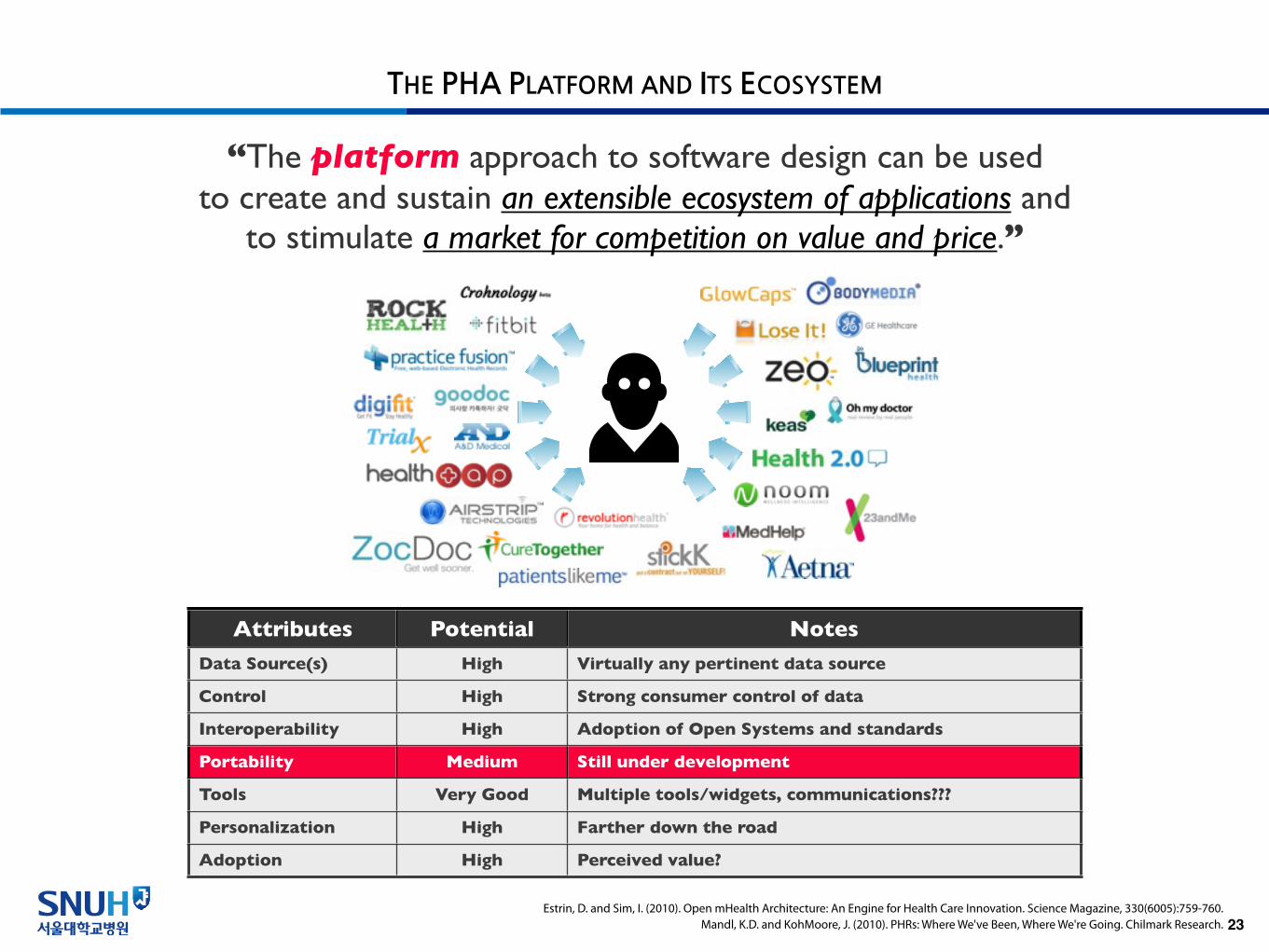
THE PHA PLATFORM AND ITS ECOSYSTEM
23
“The platform approach to software design can be used to create and sustain an extensible ecosystem of applications and
to stimulate a market for competition on value and price.”
Attributes Potential Notes
Data Source(s) High Virtually any pertinent data source
Control High Strong consumer control of data
Interoperability High Adoption of Open Systems and standards
Portability Medium Still under development
Tools Very Good Multiple tools/widgets, communications???
Personalization High Farther down the road
Adoption High Perceived value?
Estrin, D. and Sim, I. (2010). Open mHealth Architecture: An Engine for Health Care Innovation. Science Magazine, 330(6005):759-760.Mandl, K.D. and KohMoore, J. (2010). PHRs: Where We've Been, Where We're Going. Chilmark Research.

Thank You.