intermittent fasting for obesity treatmentthececonsultants.com/images/6_catenacci_fasting.pdf ·...
TRANSCRIPT

Intermittent Fasting for Obesity Treatment
Victoria A. Catenacci, MDAssociate Professor, Division of Endocrinology, Metabolism, and Diabetes
University of Colorado Anschutz Medical Campus
DisclosuresNo conflicts of interest to disclose
CASEMrs. D is a 42 yo female who presents to establish care, trying to lose weightPMH: gestational DMMeds: Mirena IUD, mviteWt 233 lbs, ht 5’4” (BMI = 40), BP 120/75, PE normalLabs: CBC, CMP, Lipids, TSH WNL, A1C 5.6%Enrolled in diabetes prevention program 6 months ago:– Daily caloric restriction (1200-1500 kcal/day)– Increased PA (300 min/week moderate intensity)– Self-monitoring strategies (calorie counting, food and PA logs)– Weekly group based-behavioral support

CASE After 3 months: wt 220 lbs (5% weight loss)After 6 months: wt 226 (3% weight loss) Doing well with exercise but reports increasing difficulty adhering to daily calorie goal…Open to weight loss medications in the future, but does not want to start yet… She has read about fasting for weight loss and is wondering if you would recommend this strategy?
Learning ObjectivesUpon completion of this program, the participant should be able to:
Understand common fasting paradigms for weight lossDescribe the current evidence base for time restricted feeding (TRF) and intermittent fasting (IMF) as treatments for overweight/obesity.
Humans evolved in environment where food was relatively scarce…
Mattson et al. Aging Research Reviews 39 (2017) 46-58
“Mammals have organs (liver, adipose tissue) that function as energy depots and enable fasting for various amounts of time depending on the species”
“Metabolic, endocrine, and nervous systems evolved in ways that allow maintenance of high levels of physical and mental performance when in a food-deprived/fasted state”

Hunting and Gathering in 2017….
• Smart phone “app” to record all ingestive events over 3 weeks.
• N = 156 (non-shift workers)
• Polar plot of aggregate data
• Most subjects ate frequently and erratically throughout wakeful hours.
• Only 5 hours (1AM to 6AM) where frequency of eating events declined.
≥5 kcals≥5kcals
• Representative scatter plot of ingestive events (n=11)
• Lack of clustering in breakfast-lunch-dinner temporal pattern.
• Median daily eating duration was 14.75 hours

Eat LessEat Less Often!
Fasting paradigms for weight loss are gaining popularity
“Male model Nicklas Kingoshares the regimen he used to take him from the grey suburbs of Copenhagen to the runways of Louis Vuitton in Paris…”

Cookbooks for Fasting???
Fasting Paradigms for Weight Loss*no clear consensus on terminology…
Time Restricted Feeding (TRF): food intake is restricted to a window of <8-10 hours/day.
Intermittent Fasting (IMF): recurring pattern of short fasting periods (16-48 hours) with little or no energy intake on fast days, with intervening periods of normal food intake.
Periodic Fasting (PF): periods of substantial energy restriction lasting 2-21 days, with intervening periods of normal food intake.
Mattson et al. Ageing Research Reviews 39 (2017) 46-58
Fasting Paradigms for Weight Loss*no clear consensus on terminology…
Time Restricted Feeding (TRF): food intake is restricted to a window of <8-10 hours/day.
Intermittent Fasting (IMF): recurring pattern of short fasting periods (16-48 hours) with little or no energy intake on fast days, with intervening periods of normal food intake.
Mattson et al. Ageing Research Reviews 39 (2017) 46-58
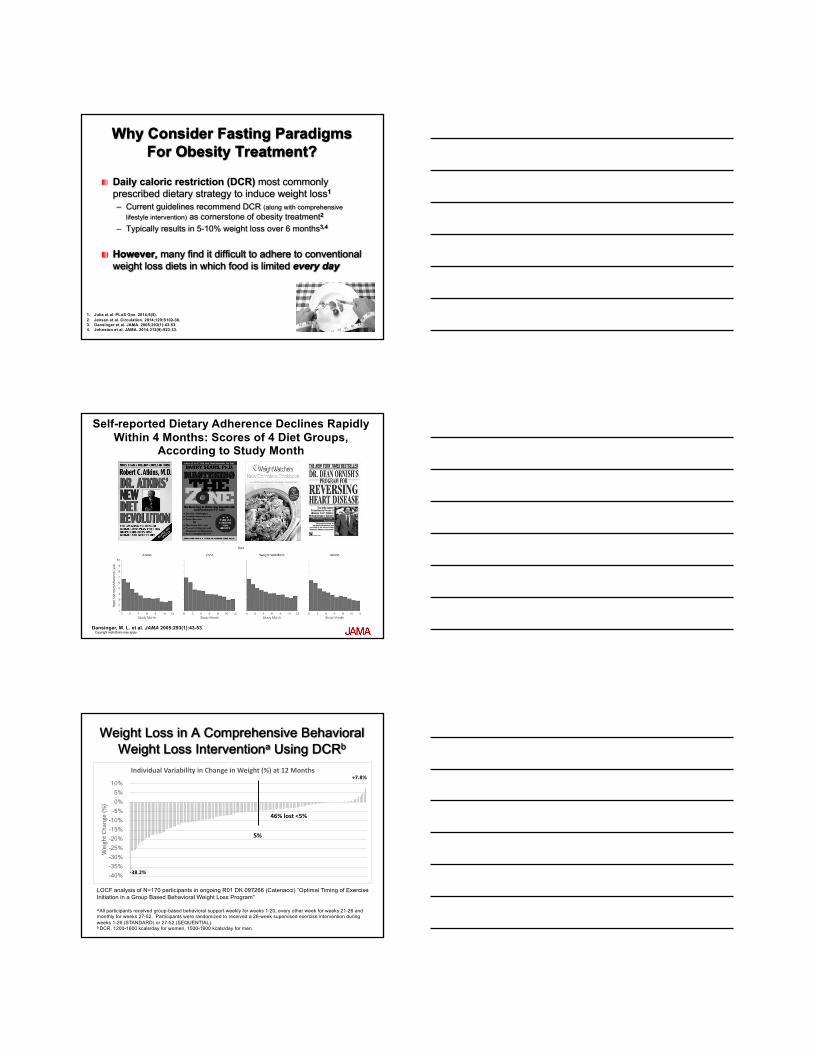
Why Consider Fasting Paradigms For Obesity Treatment?
Daily caloric restriction (DCR) most commonly prescribed dietary strategy to induce weight loss1
– Current guidelines recommend DCR (along with comprehensive lifestyle intervention) as cornerstone of obesity treatment2
– Typically results in 5-10% weight loss over 6 months3,4
However, many find it difficult to adhere to conventional weight loss diets in which food is limited every day
1. Julia et al. PLoS One. 2014;9(5). 2. Jensen et al. Circulation. 2014;129:S102-38. 3. Dansinger et al. JAMA. 2005;293(1):43-53. 4. Johnston et al. JAMA. 2014;312(9):923-33.
Copyright restrictions may apply.
Self-reported Dietary Adherence Declines Rapidly Within 4 Months: Scores of 4 Diet Groups,
According to Study Month
Dansinger, M. L. et al. JAMA 2005;293(1):43-53.
Weight Loss in A Comprehensive Behavioral Weight Loss Interventiona Using DCRb
LOCF analysis of N=170 participants in ongoing R01 DK 097266 (Catenacci) “Optimal Timing of Exercise Initiation in a Group Based Behavioral Weight Loss Program”
a All participants received group-based behavioral support weekly for weeks 1-20, every other week for weeks 21-26 and monthly for weeks 27-52. Participants were randomized to received a 26-week supervised exercise intervention during weeks 1-26 (STANDARD) or 27-52 (SEQUENTIAL). b DCR, 1200-1600 kcals/day for women, 1500-1900 kcals/day for men.
-40% -35% -30% -25% -20% -15% -10% -5% 0% 5%
10%
WeightC
hange(%
)
IndividualVariabilityinChangeinWeight(%)at12Months
46%lost<5%
5%
-38.2%
+7.8%

Weight Regain After Weight Loss
Adapted from Anderson et al. AJCN. 2001;74(5):579-84
2001 Meta-Analysis of US Dietary Weight Loss Studies
0
20
40
60
80
100
1 2 3 4 5
% of Lost Weight
Regained
Years after Weight Loss
# of Studies with Data Available13 20 10 8 8
77% of lost weight regained35% of lost
weight regained
Why Consider Fasting Paradigms For Obesity TreatmentCurrent dietary approaches only modestly effective
Important to consider and rigorously evaluate alternative dietary strategies as part of a range of dietary approaches that can be offered to individuals desiring weight loss.
Best approach for a given individual is likely to be the one they can adhere to over time…
Metabolic and Health Benefits of Fasting
Mattson et al. Ageing Research Reviews 39 (2017) 46-58
Patients ask about this…
Fasting Paradigms for Weight Loss*no clear consensus on terminology…
Mattson et al. Ageing Research Reviews 39 (2017) 46-58
Time Restricted Feeding (TRF): food intake is restricted to a window of <8-10 hours/day.
Animal Studies Suggest Weight Loss Benefit of TRF
Lean rodents: restricting feeding to 8 hour window during the active phase prevented adverse metabolic effects of a high fat diet (including weight gain, hyperinsulinemia, and hepatic steatosis)1
Diet-induced obese rodents: switching from ad libitum high fat diet to a time restricted high fat diet promoted weight loss (or weight stabilization) and improved glucose homeostasis and insulin sensitivity2
1. Hatori et al. Time-Restricted Feeding without Reducing Caloric Intake Prevents Metabolic Diseases in Mice Fed a High-Fat Diet. Cell Metabolism 2012;15:848-860.2.Chaix et al. Time-Restricted Feeding Is a Preventative and Therapeutic Intervention against Diverse Nutritional Challenges. Cell Metabolism 2014;20:991-1005.

Garaulet et al. Int J Obes, 2013
Importance of Meal Timing for Weight Loss• N=420 adults enrolled in 20 week weight loss program (Mediterranean diet +
cognitive behavioral techniques)• Age 42±11 yrs, BMI 31.4± 5.4 kg/m2, 49.5% female• Divided into Early (51%) and Late (49%) Eaters based on lunch time before and
after 1500 hours• No differences in EI, diet composition, estimated EE, appetite hormones, and
sleep duration
Gill et al. Cell Metab, 2015.
Time-Restricted Feeding Elicits Weight Loss
0 1224
• n=8 adults (BMI >25, eating window >14 hrs/day)• Asked to restrict eating to 10 hrs/d, no other dietary changes• Compliance assessed with smart phone app• 3.4 kg weight loss at 16 weeks, maintained at 1 year

Pilot Study of TRF as a Weight Loss InterventionCOMIRB 18-0487, PI Elizabeth Thomas
N=30 healthy adults with overweight/obesity randomized to TRF+RCD vs RCD alone– TRF = energy intake restricted to 10 hour/day window– RCD = standard reduced calorie diet (1200-1800 kcal/d)
12 week intervention, 6 month follow upOutcomes: body weight, DXA, energy intake/eating patterns (smart phone app),glucose variability (CGM), PA and sedentary behavior, [email protected]
Fasting Paradigms for Weight Loss*no clear consensus on terminology…
Intermittent Fasting (IMF): recurring pattern of short fasting periods (little or no energy intake on fast days), with intervening periods of normal food intake.
Alternate-day fasting (ADF)1-3 fast days/wk2 consecutive fast days/wk
Total (100%) energy restriction on fast day Partial (>75%) energy restriction on fast day
Mattson et al. Ageing Research Reviews 39 (2017) 46-58
Why is IMF Appealing? Dieters do not have to count and restrict calories every day1
Periodic nature of fasting may mitigate the constant hunger associated with DCR2
Less complicated: “this is the easiest diet I have ever been on, I just need to remember which days Ieat and which days I don’t!”
1Johnstone A. Int J Obes (Lond). 2015;39(5):727-33.2Horne BD et al. Am J Clin Nutr. 2015; 102:464-70

But don’t people just eat more on non-fast days?
Short-term (8-12 week) weight loss studies using self-reported measures of EI suggest individuals do not fully compensate on fed days for the calorie deficits on fast days
– Partial ADF (10 weeks)àEI on fed days 95±6% baseline requirements1
– Partial ADF (12 weeks)àEI on fed days 99±10% baseline requirements2
– Total ADF (8 weeks)àEI on fed days 103±13% baseline requirements3
Some studies suggest “carry-over” effect of IMF àreduction in energy intake of 23-32% on non-fasting days4,5
1Klempel et al. Nutr J. 2010;9:352Varady et al. Nutr J. 2013 12:146 3Catenacci et al. Obesity 2016;24(9):1874-834Harvie et al. Int J Obes (2011): 35(5)714-72720115Harvie et al. Int J Obes (2013) British J Nutr
What about Hunger? Total (100% energy restriction) ADF – Hunger (daily VAS 10AM, 12PM, 2PM, 4PM) increased from baseline
and did not decrease over 3 week study1
Partial (75% energy restriction) ADF – Hunger (daily 1-10 scale q 2h) increased at week 2 but no different
from baseline at week 8 of the intervention2
– Hunger (daily evening VAS scale) initially high but decreased by week 2 and remained low over 8 week intervention3
– Hunger (AUC fasting and postprandial VAS response to test meal) unchanged from baseline at week 84
1Heilbronn et al. Am J Clin Nutr 2005; 81:69-73.2Johnson et al. Free radical biology & medicine. 2007;42(5):665-743Klempel et al. Nutr J. 2010;9:354Hoddy et al. Clin Nutr. 2016; 35(6)1380-85
Is IMF Safe?
Pilot Study Design26 adults (6 men, 20 women), BMI ≥30 kg/m2, age18-55
– Randomized 1:1 to alternate-day fasting (ADF) or daily caloric restriction (DCR)
8 week intervention period (all food provided)
– ADF: Total (100%) energy restriction on fast days, ad libitum intake on fed daysa
– DCR: -400 kcal/dayb
a On fed days, ADF provided diet estimated to meet energy requirements plus 5-7 optional food modules (200 kcals) b Considered standard of care dietary weight loss intervention when study was designed in 2006
Catenacci et al, Obesity (2016) 24, 1874-1883

Is Fasting Safe?
BMP, CBC, heart rate, blood pressure, ECG, QEWP-R (binge eating behavior) and CES-D (depression) measured at baseline and week 8No changes in safety parameters, no adverse events over the 8 week study
N = 59, age 25-65, BMI 30-40 Underwent 8 week partial (75% ER) ADF (weight loss 4.2±0.3%)
Assessed with Multidimensional Assessment of Eating Disorder Symptoms (MAEDS) Assessed with Adverse Events Questionnaire
Current Evidence for IMF as a Weight Loss Strategy
Several studies1-13 suggest various IMF paradigms are safe and tolerable and produce 3-8% weight loss along with improvements in body composition and metabolic parameters in adults with overweight/obesity
However, limitations to current evidence base…
1Johnson et al, Free Radic Biol Med (2007);42(5):665-674, 2Varady et al, Am J Clin Nutr (2009);90:1138-43, 3Varady et al, Lipids Health Dis (2011);10:119-123, 4Harvie et al, 2011 Int J Obes (2011);35(5):714-727, 5Harvie et al, 2013 Br J Nutr(2013);110:1534-1547, 6Esghinia et al, J Diabetes Metab Disord (2013);12(1):4, 7Bhutani et al, Obesity (2013);21(7):1370-9, 8Klempel et al, Metabolism (2013):62:137-143, 9Varady et al, Nutr J (2013);12(1):146, 10Hoddy et al, Obesity (2014);22:2524-2531, 11Catenacci et al, Obesity (2016) 2;24(9):1874-83, 12Carter et al, Diabetes Res Clin Pract(2016):122: 106-112, 13Trepanowski et al, JAMA Int Med (2017);177(7):930-938

IMF Weight Loss Studies*Reference N Duration BMI (kg/m2) Intervention Groups Weight LossJohnson et al , 2007 9 8 weeks >30 ADF (80% ER on fast day) 8.0±1.5%
Varady et al, 2009 16 10 weeks 30-40 ADF (75% ER on fast day) 5.8±1.1%
Varady et al, 2011 60 12 weeks 25-40 ADF (75% ER on fast day)DCR (25% ER daily)EX (moderate intensity, 3x/wk)Control
5.2±1.1%5.0±1.4%5.1±0.9%-0.2±0.4%
Harvie et al, 2011 107 26 weeks 24-40 IER (492-542 kcal/d, 2 consecutive days/wk) CR (25% ER daily)
7.8±5.9%6.6±5%
Harvie et al, 2013 115 16 weeks(12 weeks weight loss,4 weeks maintenance)
24-45 IER (492-542 kcal/d, 2 consecutive days/wk) IER (492-542 kcal/d, 2 consecutive days/wk) + PFCR (25% ER daily)
6.2±4.6%5.7±3.9%4.3±4.6%
Esghinia et al, 2013 15 8 weeks ≥25 IMF (70-75% ER on fast day, 3days/wk) 7.1±1.4%
Bhutani et al, 2013 64 12 weeks 30-40 ADF (75% ER on fast day)EX (moderate intensity, 3x/wk)ADF + EX Control
3±1%1±0%7±2%0±0%
Klempel et al, 2013 32 10 weeks 30-40 ADF (75% ER on fast day), 45% FATADF (75% ER on fast day), 25% FAT
4.8±1.1%4.2±0.8%
Varady et al, 2013 32 12 weeks 20-30 ADF (75% ER on fast day)Control
6.8±1.0%0.3±1%
Hoddy et al, 2014 74 8 weeks 30-40 ADF (75% ER on fast day), LUNCHADF (75% ER on fast day) DINNERADF (75% ER on fast day) SMALL MEALS
3.5±0.4%4.2±0.5%4.6±0.6%
Catenacci et al, 2016 26 8 weeks ≥30 ADF (100% ER on fast day)DCR (-400 kcal/d)
8.8±0.9%6.2±0.9%
Carter et al, 2016 63 12 weeks ≥27(T2DM)
IER (70-85% ER, 2 consecutive days/wk) + EX (2000 steps)CR (35-45% ER daily) + EX (2000 steps)
6.2±3.0%5.6±4.4%
Trepanowski et al, 2017 100 52 weeks(26 weeks weight loss,26 weeks maintenance)
25-40 ADF (75% ER on fast day)DCR (25% ER daily)Control
6.8%, 6.0%6.8%, 5.3%(relative to control)
*Weight loss studies ≥8 weeks duration in individuals with overweight/obesity involving Alternate Day Fasting (ADF), Intermittent Fasting (IMF, 1-3 fast days/wk), or Intermittent Energy Restriction (IER, 2 consecutive fast days/wk) with ≥ 70% energy restriction (ER) on fast days.
IMF Weight Loss Studies*Reference N Duration BMI (kg/m2) Intervention Groups Weight LossJohnson et al , 2007 9 8 weeks >30 ADF (80% ER on fast day) 8.0±1.5%
Varady et al, 2009 16 10 weeks 30-40 ADF (75% ER on fast day) 5.8±1.1%
Varady et al, 2011 60 12 weeks 25-40 ADF (75% ER on fast day)DCR (25% ER daily)EX (moderate intensity, 3x/wk)Control
5.2±1.1%5.0±1.4%5.1±0.9%-0.2±0.4%
Harvie et al, 2011 107 26 weeks 24-40 IER (492-542 kcal/d, 2 consecutive days/wk) CR (25% ER daily)
7.8±5.9%6.6±5%
Harvie et al, 2013 115 16 weeks(12 weeks weight loss,4 weeks maintenance)
24-45 IER (492-542 kcal/d, 2 consecutive days/wk) IER (492-542 kcal/d, 2 consecutive days/wk) + PFCR (25% ER daily)
6.2±4.6%5.7±3.9%4.3±4.6%
Esghinia et al, 2013 15 8 weeks ≥25 IMF (70-75% ER on fast day, 3days/wk) 7.1±1.4%
Bhutani et al, 2013 64 12 weeks 30-40 ADF (75% ER on fast day)EX (moderate intensity, 3x/wk)ADF + EX Control
3±1%1±0%7±2%0±0%
Klempel et al, 2013 32 10 weeks 30-40 ADF (75% ER on fast day), 45% FATADF (75% ER on fast day), 25% FAT
4.8±1.1%4.2±0.8%
Varady et al, 2013 32 12 weeks 20-30 ADF (75% ER on fast day)Control
6.8±1.0%0.3±1%
Hoddy et al, 2014 74 8 weeks 30-40 ADF (75% ER on fast day), LUNCHADF (75% ER on fast day) DINNERADF (75% ER on fast day) SMALL MEALS
3.5±0.4%4.2±0.5%4.6±0.6%
Catenacci et al, 2016 26 8 weeks ≥30 ADF (100% ER on fast day)DCR (-400 kcal/d)
8.8±0.9%6.2±0.9%
Carter et al, 2016 63 12 weeks ≥27(T2DM)
IER (70-85% ER, 2 consecutive days/wk) + EX (2000 steps)CR (35-45% ER daily) + EX (2000 steps)
6.2±3.0%5.6±4.4%
Trepanowski et al, 2017 100 52 weeks(26 weeks weight loss,26 weeks maintenance)
25-40 ADF (75% ER on fast day)DCR (25% ER daily)Control
6.8%, 6.0%6.8%, 5.3%(relative to control)
*Weight loss studies ≥8 weeks duration in individuals with overweight/obesity involving Alternate Day Fasting (ADF), Intermittent Fasting (IMF, 1-3 fast days/wk), or Intermittent Energy Restriction (IER, 2 consecutive fast days/wk) with ≥ 70% energy restriction (ER) on fast days.
IMF Weight Loss Studies*: > 12 WeeksReference N Duration BMI (kg/m2) Intervention Groups Weight LossJohnson et al , 2007 9 8 weeks >30 ADF (80% ER on fast day) 8.0±1.5%
Varady et al, 2009 16 10 weeks 30-40 ADF (75% ER on fast day) 5.8±1.1%
Varady et al, 2011 60 12 weeks 25-40 ADF (75% ER on fast day)DCR (25% ER daily)EX (moderate intensity, 3x/wk)Control
5.2±1.1%5.0±1.4%5.1±0.9%-0.2±0.4%
Harvie et al, 2011 107 26 weeks 24-40 IER (492-542 kcal/d, 2 consecutive days/wk) CR (25% ER daily)
7.8±5.9%6.6±5%
Harvie et al, 2013 115 16 weeks(12 weeks weight loss,4 weeks maintenance)
24-45 IER (492-542 kcal/d, 2 consecutive days/wk) IER (492-542 kcal/d, 2 consecutive days/wk) + PFCR (25% ER daily)
6.2±4.6%5.7±3.9%4.3±4.6%
Esghinia et al, 2013 15 8 weeks ≥25 IMF (70-75% ER on fast day, 3days/wk) 7.1±1.4%
Bhutani et al, 2013 64 12 weeks 30-40 ADF (75% ER on fast day)EX (moderate intensity, 3x/wk)ADF + EX Control
3±1%1±0%7±2%0±0%
Klempel et al, 2013 32 10 weeks 30-40 ADF (75% ER on fast day), 45% FATADF (75% ER on fast day), 25% FAT
4.8±1.1%4.2±0.8%
Varady et al, 2013 32 12 weeks 20-30 ADF (75% ER on fast day)Control
6.8±1.0%0.3±1%
Hoddy et al, 2014 74 8 weeks 30-40 ADF (75% ER on fast day), LUNCHADF (75% ER on fast day) DINNERADF (75% ER on fast day) SMALL MEALS
3.5±0.4%4.2±0.5%4.6±0.6%
Catenacci et al, 2016 26 8 weeks ≥30 ADF (100% ER on fast day)DCR (-400 kcal/d)
8.8±0.9%6.2±0.9%
Carter et al, 2016 63 12 weeks ≥27(T2DM)
IER (70-85% ER, 2 consecutive days/wk) + EX (2000 steps)CR (35-45% ER daily) + EX (2000 steps)
6.2±3.0%5.6±4.4%
Trepanowski et al, 2017 100 52 weeks(26 weeks weight loss,26 weeks maintenance)
25-40 ADF (75% ER on fast day)DCR (25% ER daily)Control
6.8%, 6.0%6.8%, 5.3%(relative to control)
*Weight loss studies ≥ 8 weeks duration in individuals with overweight/obesity involving Alternate Day Fasting (ADF), Intermittent Fasting (IMF, 1-3 fast days/wk), or Intermittent Energy Restriction (IER, 2 consecutive fast days/wk) with ≥ 70% energy restriction (ER) on fast days.

IMF Weight Loss Studies*: > 16 per armReference N Duration BMI (kg/m2) Intervention Groups Weight LossJohnson et al , 2007 9 8 weeks >30 ADF (80% ER on fast day) 8.0±1.5%
Varady et al, 2009 16 10 weeks 30-40 ADF (75% ER on fast day) 5.8±1.1%
Varady et al, 2011 60 12 weeks 25-40 ADF (75% ER on fast day)DCR (25% ER daily)EX (moderate intensity, 3x/wk)Control
5.2±1.1%5.0±1.4%5.1±0.9%-0.2±0.4%
Harvie et al, 2011 107 26 weeks 24-40 IER (492-542 kcal/d, 2 consecutive days/wk) CR (25% ER daily)
7.8±5.9%6.6±5%
Harvie et al, 2013 115 16 weeks(12 weeks weight loss,4 weeks maintenance)
24-45 IER (492-542 kcal/d, 2 consecutive days/wk) IER (492-542 kcal/d, 2 consecutive days/wk) + PFCR (25% ER daily)
6.2±4.6%5.7±3.9%4.3±4.6%
Esghinia et al, 2013 15 8 weeks ≥25 IMF (70-75% ER on fast day, 3days/wk) 7.1±1.4%
Bhutani et al, 2013 64 12 weeks 30-40 ADF (75% ER on fast day)EX (moderate intensity, 3x/wk)ADF + EX Control
3±1%1±0%7±2%0±0%
Klempel et al, 2013 32 10 weeks 30-40 ADF (75% ER on fast day), 45% FATADF (75% ER on fast day), 25% FAT
4.8±1.1%4.2±0.8%
Varady et al, 2013 32 12 weeks 20-30 ADF (75% ER on fast day)Control
6.8±1.0%0.3±1%
Hoddy et al, 2014 74 8 weeks 30-40 ADF (75% ER on fast day), LUNCHADF (75% ER on fast day) DINNERADF (75% ER on fast day) SMALL MEALS
3.5±0.4%4.2±0.5%4.6±0.6%
Catenacci et al, 2016 26 8 weeks ≥30 ADF (100% ER on fast day)DCR (-400 kcal/d)
8.8±0.9%6.2±0.9%
Carter et al, 2016 63 12 weeks ≥27(T2DM)
IER (70-85% ER, 2 consecutive days/wk) + EX (2000 steps)CR (35-45% ER daily) + EX (2000 steps)
6.2±3.0%5.6±4.4%
Trepanowski et al, 2017 100 52 weeks(26 weeks weight loss,26 weeks maintenance)
25-40 ADF (75% ER on fast day)DCR (25% ER daily)Control
6.8%, 6.0%6.8%, 5.3%(relative to control)
*Weight loss studies ≥ 8 weeks duration in individuals with overweight/obesity involving Alternate Day Fasting (ADF), Intermittent Fasting (IMF, 1-3 fast days/wk), or Intermittent Energy Restriction (IER, 2 consecutive fast days/wk) with ≥ 70% energy restriction (ER) on fast days.
IMF Weight Loss Studies*: Food ProvidedReference N Duration BMI (kg/m2) Intervention Groups Weight LossJohnson et al , 2007 9 8 weeks >30 ADF (80% ER on fast day) 8.0±1.5%
Varady et al, 2009 16 10 weeks 30-40 ADF (75% ER on fast day) 5.8±1.1%
Varady et al, 2011 60 12 weeks 25-40 ADF (75% ER on fast day)DCR (25% ER daily)EX (moderate intensity, 3x/wk)Control
5.2±1.1%5.0±1.4%5.1±0.9%-0.2±0.4%
Harvie et al, 2011 107 26 weeks 24-40 IER (492-542 kcal/d, 2 consecutive days/wk) CR (25% ER daily)
7.8±5.9%6.6±5%
Harvie et al, 2013 115 16 weeks(12 weeks weight loss,4 weeks maintenance)
24-45 IER (492-542 kcal/d, 2 consecutive days/wk) IER (492-542 kcal/d, 2 consecutive days/wk) + PFCR (25% ER daily)
6.2±4.6%5.7±3.9%4.3±4.6%
Esghinia et al, 2013 15 8 weeks ≥25 IMF (70-75% ER on fast day, 3days/wk) 7.1±1.4%
Bhutani et al, 2013 64 12 weeks 30-40 ADF (75% ER on fast day)EX (moderate intensity, 3x/wk)ADF + EX Control
3±1%1±0%7±2%0±0%
Klempel et al, 2013 32 10 weeks 30-40 ADF (75% ER on fast day), 45% FATADF (75% ER on fast day), 25% FAT
4.8±1.1%4.2±0.8%
Varady et al, 2013 32 12 weeks 20-30 ADF (75% ER on fast day)Control
6.8±1.0%0.3±1%
Hoddy et al, 2014 74 8 weeks 30-40 ADF (75% ER on fast day), LUNCHADF (75% ER on fast day) DINNERADF (75% ER on fast day) SMALL MEALS
3.5±0.4%4.2±0.5%4.6±0.6%
Catenacci et al, 2016 26 8 weeks ≥30 ADF (100% ER on fast day)DCR (-400 kcal/d)
8.8±0.9%6.2±0.9%
Carter et al, 2016 63 12 weeks ≥27(T2DM)
IER (70-85% ER, 2 consecutive days/wk) + EX (2000 steps)CR (35-45% ER daily) + EX (2000 steps)
6.2±3.0%5.6±4.4%
Trepanowski et al, 2017 100 52 weeks(26 weeks weight loss,26 weeks maintenance)
25-40 ADF (75% ER on fast day)DCR (25% ER daily)Control
6.8%, 6.0%6.8%, 5.3%(relative to control)
*Weight loss studies ≥8 weeks duration in individuals with overweight/obesity involving Alternate Day Fasting (ADF), Intermittent Fasting (IMF, 1-3 fast days/wk), or Intermittent Energy Restriction (IER, 2 consecutive fast days/wk) with ≥ 70% energy restriction (ER) on fast days.
IMF Weight Loss Studies*: Comparison to DCR Reference N Duration BMI (kg/m2) Intervention Groups Weight LossJohnson et al , 2007 9 8 weeks >30 ADF (80% ER on fast day) 8.0±1.5%
Varady et al, 2009 16 10 weeks 30-40 ADF (75% ER on fast day) 5.8±1.1%
Varady et al, 2011 60 12 weeks 25-40 ADF (75% ER on fast day)DCR (25% ER daily)EX (moderate intensity, 3x/wk)Control
5.2±1.1%5.0±1.4%5.1±0.9%-0.2±0.4%
Harvie et al, 2011 107 26 weeks 24-40 IER (492-542 kcal/d, 2 consecutive days/wk) CR (25% ER daily)
7.8±5.9%6.6±5%
Harvie et al, 2013 115 16 weeks(12 weeks weight loss,4 weeks maintenance)
24-45 IER (492-542 kcal/d, 2 consecutive days/wk) IER (492-542 kcal/d, 2 consecutive days/wk) + PFCR (25% ER daily)
6.2±4.6%5.7±3.9%4.3±4.6%
Esghinia et al, 2013 15 8 weeks ≥25 IMF (70-75% ER on fast day, 3days/wk) 7.1±1.4%
Bhutani et al, 2013 64 12 weeks 30-40 ADF (75% ER on fast day)EX (moderate intensity, 3x/wk)ADF + EX Control
3±1%1±0%7±2%0±0%
Klempel et al, 2013 32 10 weeks 30-40 ADF (75% ER on fast day), 45% FATADF (75% ER on fast day), 25% FAT
4.8±1.1%4.2±0.8%
Varady et al, 2013 32 12 weeks 20-30 ADF (75% ER on fast day)Control
6.8±1.0%0.3±1%
Hoddy et al, 2014 74 8 weeks 30-40 ADF (75% ER on fast day), LUNCHADF (75% ER on fast day) DINNERADF (75% ER on fast day) SMALL MEALS
3.5±0.4%4.2±0.5%4.6±0.6%
Catenacci et al, 2016 26 8 weeks ≥30 ADF (100% ER on fast day)DCR (-400 kcal/d)
8.8±0.9%6.2±0.9%
Carter et al, 2016 63 12 weeks ≥27(T2DM)
IER (70-85% ER, 2 consecutive days/wk) + EX (2000 steps)CR (35-45% ER daily) + EX (2000 steps)
6.2±3.0%5.6±4.4%
Trepanowski et al, 2017 100 52 weeks(26 weeks weight loss,26 weeks maintenance)
25-40 ADF (75% ER on fast day)DCR (25% ER daily)Control
6.8%, 6.0%6.8%, 5.3%(relative to control)
*Weight loss studies ≥ 8 weeks duration in individuals with overweight/obesity involving Alternate Day Fasting (ADF), Intermittent Fasting (IMF, 1-3 fast days/wk), or Intermittent Energy Restriction (IER, 2 consecutive fast days/wk) with ≥ 70% energy restriction (ER) on fast days.

Attrition and AdherenceDrop out rates 0-40%Studies which report adherence suggest reasonable compliance with fast days (but rely on self-report…)– 80-98% of potential fast days achieved with partial ADF1-5
– 65-75% of potential fast days achieved with 2 consecutive fast days/wk6-7
Only 1 study using objective measure of EI8– Partial ADF vs DCR, targeted weekly energy restriction 25% in both groups – Actual energy restriction at 6 months: ADF 21±15%, DCR 24±16%, p = 0.65
1Varady et al Am J Clin Nutr (2009): 90:1138-432Klempel et al. Metabolism (2013) 63: 1367-143 3Varady et al. Nutr J. (2013) 12:146 4Bhutani et al. Obesity (2013) 21: 1370-13795Hoddy et al. Obesity (2014) 2524-25316Harvie et al. Int J Obes (2011): 35 (5) 714-727 7Harvie et al. British J Nutr (2013)110: 1534-47 8Trepanowski et al. JAMA Intern Med 2017;177(7): 930-938
“Comparison of Weight Loss Induced by IMF vs. DCR in Individuals with Obesity:
A 1-Year Randomized Trial”
R01 DK111622-01A1 (Catenacci) 9/15/17-6/30/22Co-Investigators
Dan Bessesen, MD Paul Maclean, PhD Ed Melanson, PhD Zhaoxing Pan, PhD
R01 DK111622 Overview
Pragmatic 1-year randomized trial designed to compare weight loss generated by IMF vs. DCR
150 healthy adults with obesity (18-55 yrs, BMI 30-45 kg/m2)Randomized 1:1 to IMF or DCREquivalent targeted weekly energy deficit (30%) Both groups receive behavioral support to compare IMF to current standard of care (DCR) in a robust fashionObjective measure of EI/EE (DLW intake-balance method)

Specific AimsAim 1. Compare changes in body weight (1⁰ outcome), body composition, and metabolic parameters (lipids, BP, HOMA-IR) induced by IMF and DCR.– Hypothesis: IMF will generate greater weight loss and improvements in
body composition and metabolic parameters at 1 year compared to DCR.
Aim 2. Evaluate the impact of IMF vs DCR on energy intake and dietary adherence.– Hypothesis: IMF will demonstrate greater degree of energy restriction and
better adherence to diet at 1 year.
Aim 3. Evaluate the impact of IMF vs DCR on components of energy expenditure and patterns of PA.– Hypothesis: REE will decrease less in IMF, changes in PAEE, MVPA, and
sedentary time will be similar at 1 year.
Aim 4 (Exploratory). Investigate predictors of weight loss within both groups.
Outcome MeasuresOutcomes by Study Week 0 13 26 39 52Body Weight (kg) xx xxx xxx xxx xxFat Mass (kg), Lean Mass (kg): DXA x x ? xMetabolic Parameters: Lipid Panel, HOMA-IR, BP x x ? xEI and TDEE: Doubly Labeled Water x x ? x7 Day Diet Records x x x xDietary Adherence, Effort, and Self-Efficacy: Monthly Likert Scale xx xxx xxx xxx xxHormones Related to Appetite: Leptin, Ghrelin, PYY, BDNF x x ? xREE: Indirect calorimetry x x ? xMVPA and Sedentary Time: ActivPAL x x x xQOL Measures, Mood State, Binge Eating Behaviors, Sleep x x x x
Dietary InterventionsIMF: Partial fast, 3 non-consecutive days/week
Fast days: calorie goal à75% deficit from baseline requirements Fed days: ad libitum, but encouraged to make healthy food choices
DCR: Moderate daily caloric restriction Every day: calorie goal à30% deficit from baseline requirements
Additional details…– Same targeted weekly energy deficit (30%) and dietary macronutrient content
(55% carbohydrate, 15% protein, 30% fat)– Dietary paradigms maintained for duration of 1 year study – Food NOT provided– Both groups receive comprehensive, high intensity group-based behavioral
support (weekly during weeks 0-13, every two weeks during weeks 14-52)

Why a Partial Fast?Match targeted weekly energy deficit – 30% energy restriction is standard of care for DCR– Options to achieve 30% weekly energy restriction with IMF
Total (100%) energy restriction 2 days/wkPartial (75%) energy restriction 3 days/wk
– 64/82 (78%) of individuals with obesity preferred partial fastConcerns about compliance/retention over 1 year– Decreases in subjective hunger in partial but not total fast
Acute effect of total vs partial ER1
– Short-term study suggests less compensation on post-fast day w/ partial vs complete fast resulting in similar 3 day energy defecit
Review of lay literature– Partial fast by far most commonly endorsed paradigm thus most
clinically relevant to study in large, pragmatic trial
1. Antoni et al, British Journal of Nutrition, (2016) 115, 951-959
Why NOT Provide Food?
Limits translatability of results– Most individuals do not have access to weight loss programs in
which food is provided
May bias results in favor of DCR– Food provision may increase ease of adherence to DCR but
does not reflect challenges faced in free-living conditions (accurately counting calories, choosing appropriate portion sizes)
– Food provision may model portion size and calorie control for DCR in a way that is not clinically replicable
Why maintain the same dietary paradigms for 1 year?
Weight loss with DCR typically plateaus at 6 monthsMany behavioral weight loss programs shift focus to weight loss maintenance at ~6 month mark.
However– Obtaining adherence and weight loss data over 1
year will help us understand when we should shift focus to weight loss maintenance with IMF.

Timeline: 6 cohorts of 25(Cohort 1 : 5/8/18)
Study Timeline Year 1 Year 2 Year 3 Year 4 Year 5
Planning and Final IRB approvals
Data Collection (n=~25 per cohort)
Cohort 1 (randomized 1:1 to IMF or DCR)
Cohort 2 (randomized 1:1 to IMF or DCR)
Cohort 3 (randomized 1:1 to IMF or DCR)
Cohort 4 (randomized 1:1 to IMF or DCR)
Cohort 5 (randomized 1:1 to IMF or DCR)
Cohort 6 (randomized 1:1 to IMF or DCR)
Data Analysis, Manuscripts
9/2017 9/2018 9/2019 9/2020 9/2021
For more information or to see if you qualify email [email protected]
Outstanding QuestionsDoes TRF enhance weight loss with a RCD?
Is IMF a durable weight loss strategy?
Does IMF or TRF have greater body composition or metabolic benefits?
Do adherence patterns differ between IMF and DCR?
Does IMF impact resting energy expenditure? Ability to exercise?
Can we predict who may respond more favorably to IMF?
What is the optimal frequency of fasting for weight loss? For weight loss maintenance?
What is the optimal energy restriction and macronutrient content on fast days?
Will individuals who self-select IMF do better than individuals who are randomly assigned?
CASE Mrs. D is a 42 yo female with BMI 40 trying to lose weight Lost 13 lbs over 3 months with daily calorie restriction and increasing PA regained 6 lbs over next 3 months.Difficulty adhering to the reduced calorie diet.She has read about fasting for weight loss and is wondering if you would recommend this strategy?

CASE Short-term studies suggest that TRF and IMF are safe and effective weight loss strategies, however well-designed long term studies have not been completed. Best diet for a given person is one they feel they can stick to over time…TRF: limit eating to 10 hour window, recommend starting window within 1-2 hours of waking (+RCD)IMF: 500 kcal/day (women), 600 kcal/day (men) on fast days (or no intake on fast days) 2-3 non-consecutive days/wk (consume as dinner meal)
Active Learning Question 1Time Restricted Feeding (TRF) is best defined as:
A. Short fasting periods (16-48 hours) with little or no energy intake on fast days with intervening periods of normal food intake.
B. Periods of substantial energy restriction lasting 2-21 days, with intervening periods of normal food intake.
C. Restricting food intake to a window of <8-10 hours/day.
Mattson et al. Ageing Research Reviews 39 (2017) 46-58
Active Learning Question 2Compared to standard daily caloric restriction, current evidence suggests that Intermittent Fasting (IMF):
A. Produces similar short-term weight loss and improvements in metabolic parameters in adults with overweight/obesity
B. Produces superior short-term weight loss and improvements in metabolic parameters in adults with overweight/obesity
C. Produces inferior short-term weight loss and improvements in metabolic parameters in adults with overweight/obesity
Trepanowski et al, JAMA Intern Med (2017);177(7):930-938Catenacci et al, Obesity (2016) 24, 1874-1883

AcknowledgementsCollaborators/Mentors
Edward Melanson, PhDWilliam T. Donahoo, MDJames O. Hill, PhDHolly R. Wyatt, MD Zhaoxing Pan, PhDPaul MacLean, PhDDaniel Bessesen, MD
Research StaffKristen Bing, RDLiza Weyland, MSDanielle Ostendorf, MSElizabeth Kealey, RDJared Scorsone
Grant SupportUL1 TR000154 (University of Colorado Clinical and Translational Science Institute)P30 DK048520 (Colorado Nutrition and Obesity Research Center)NIH R21 AT002617 (Donahoo)NIH F32 DK069020 (Catenacci) NIH K23 DK078913 (Catenacci)NIH R01 DK097266 (Catenacci)NIH R01 DK111622 (Catenacci)
Discussion