interpreting blood tests part 2 - simply revision - home · •acute viral hepatitis •autoimmune...
TRANSCRIPT
Interpreting Blood Tests
Part 2
Dr Andrew Smith
OutlinePrevious Talk:• Introduction• Which Tube!?!• FBCs• U+Es
This Week:• LFTs• Clotting• Extras• D-Dimers• Acute Phase Reactants• TFTs• Calcium, Phosphate and Alk Phos• Immunoglobulins• Batch Tests

Case 8• A 36 year old man is referred to you in AnE because he is noted to
be jaundiced. He has been feeling generally unwell recently, with
some D+V.
• His LFTs show the following: What’s useful to know?
Normal Values
ALP 34 30-150µmol/L
ALT 12 5-35iu/L
AST 7 5-35iu/L
ɣGT 12 <45iu/L
Bil 88 <20µmol/L
Alb 37 35-50g/L
Rest of bloods are normal
Unconjugated Bili: 70
Conjugated Bili: 18
Isolated hyperbilrubinaemia
Unconjugated
Haemolysis
Gilbert’s Syndrome
Neonatal
Drugs
Crigler-Najjar Syndrome
Conjugated
Dubin-Johnson Syndrome
Rotor Syndrome
Glycogen Storage Disease
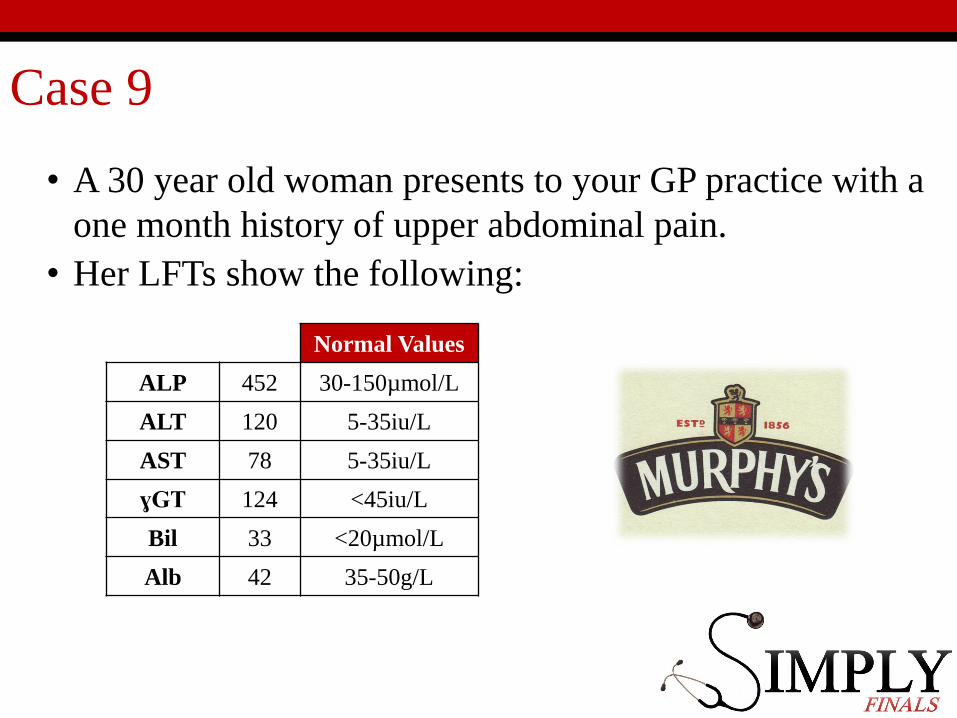
Case 9
• A 30 year old woman presents to your GP practice with a
one month history of upper abdominal pain.
• Her LFTs show the following:
Normal Values
ALP 452 30-150µmol/L
ALT 120 5-35iu/L
AST 78 5-35iu/L
ɣGT 124 <45iu/L
Bil 33 <20µmol/L
Alb 42 35-50g/L
Case 9
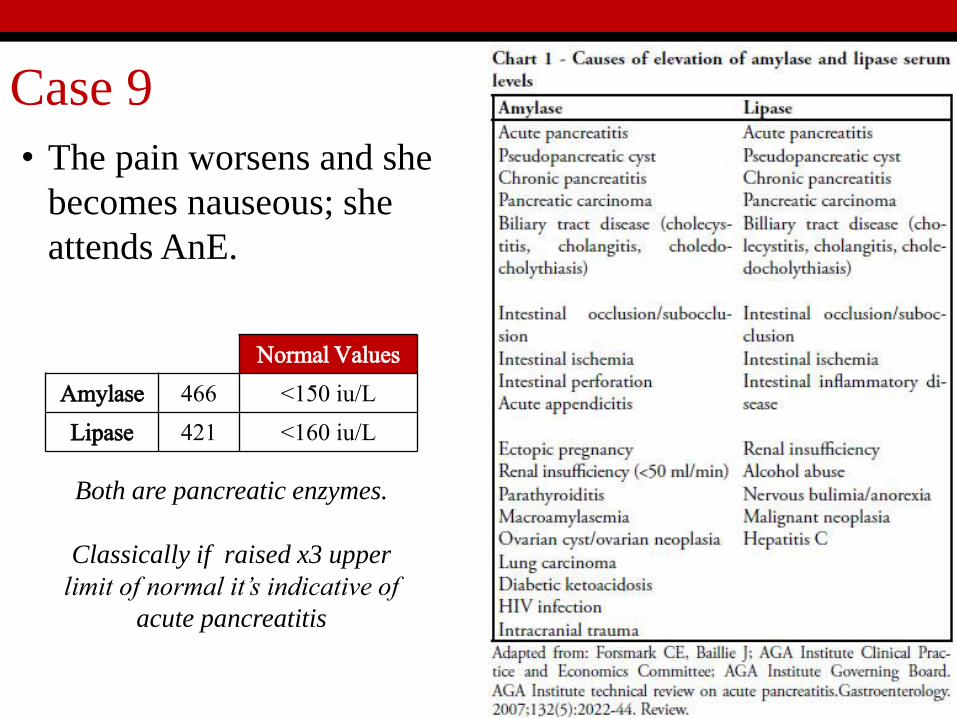
• The pain worsens and she
becomes nauseous; she
attends AnE.
Normal Values
Amylase 466 <150 iu/L
Lipase 421 <160 iu/L
Both are pancreatic enzymes.
Classically if raised x3 upper
limit of normal it’s indicative of
acute pancreatitis
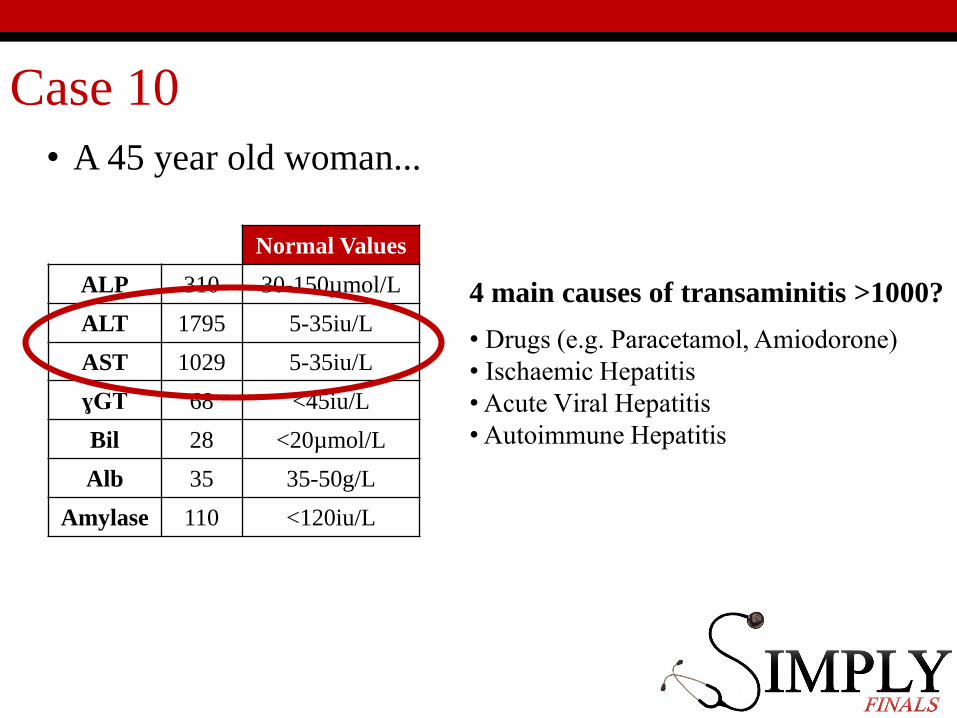
Case 10
• A 45 year old woman...
Normal Values
ALP 310 30-150µmol/L
ALT 1795 5-35iu/L
AST 1029 5-35iu/L
ɣGT 68 <45iu/L
Bil 28 <20µmol/L
Alb 35 35-50g/L
Amylase 110 <120iu/L
4 main causes of transaminitis >1000?
• Drugs (e.g. Paracetamol, Amiodorone)• Ischaemic Hepatitis•Acute Viral Hepatitis•Autoimmune Hepatitis
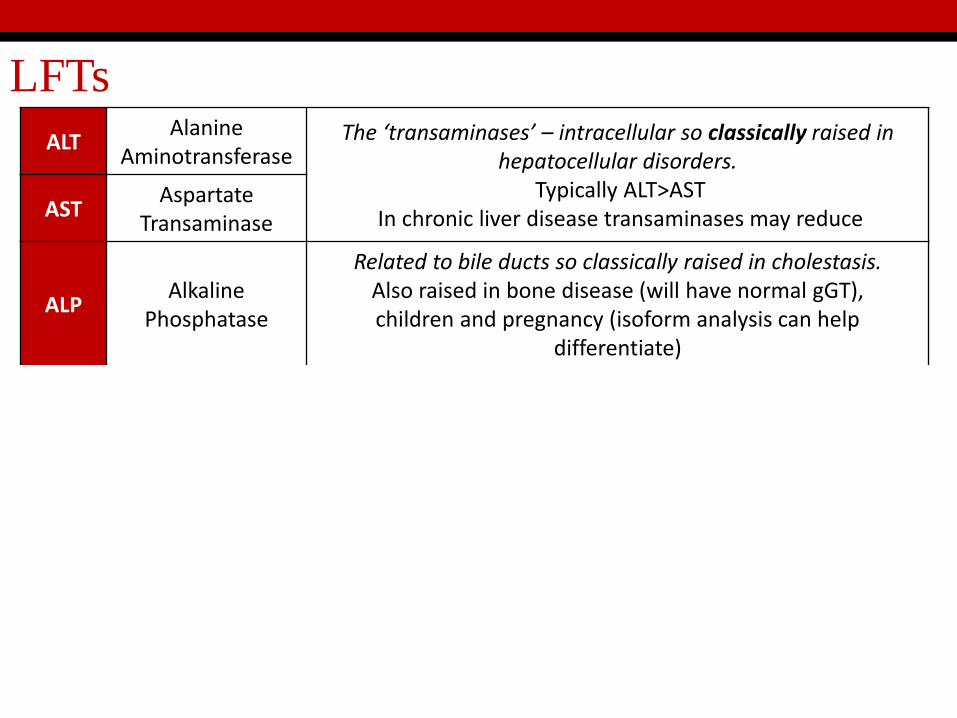
LFTs
ALTAlanine
AminotransferaseThe ‘transaminases’ – intracellular so classically raised in
hepatocellular disorders.Typically ALT>AST
In chronic liver disease transaminases may reduceASTAspartate
Transaminase
ALPAlkaline
Phosphatase
Related to bile ducts so classically raised in cholestasis.Also raised in bone disease (will have normal gGT),children and pregnancy (isoform analysis can help
differentiate)
ɣGTGamma glutamyltranspeptidase
Related to bile ducts.If raised with ALP suggests cholestasis.
If isolated rise, suggest enzyme induction (e.g. Alcohol)
Bil
BilirubinUnconjugated
(indirect)Conjugated
(direct)
Conjugated by liver enzymes and excreted in bile.Can be raised in all types of liver disease and there are extra-
hepatic causes.Ratio of indirect:direct bilirubin helps classify
Alb AlbuminMarker of hepatic synthetic function
(along with clotting factors) but has half life of around 20 days
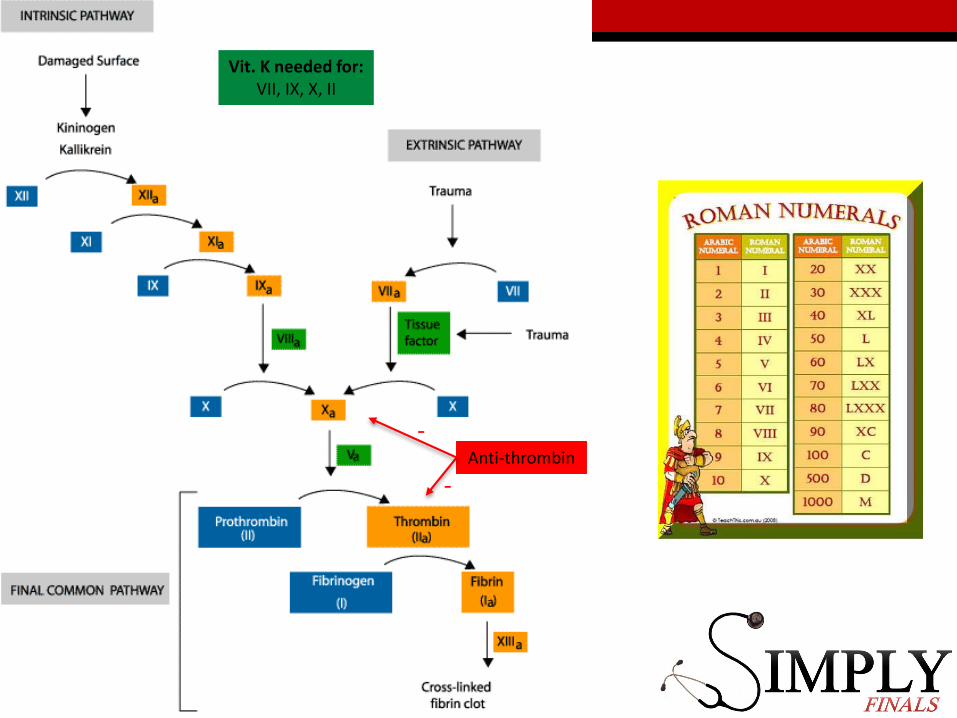
Anti-thrombin
-
-
Vit. K needed for: VII, IX, X, II
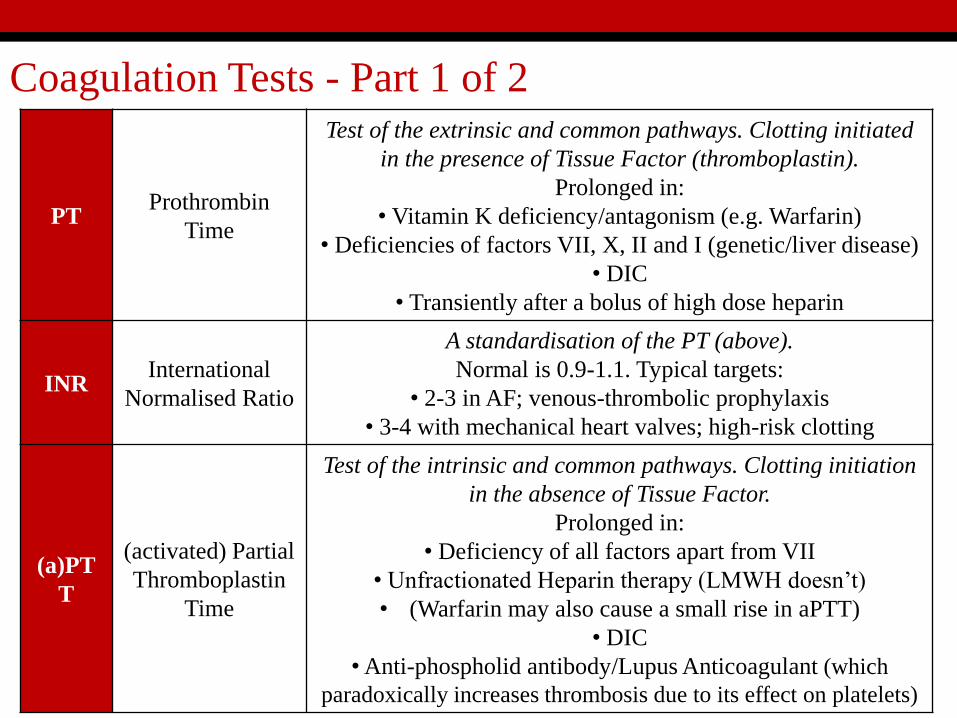
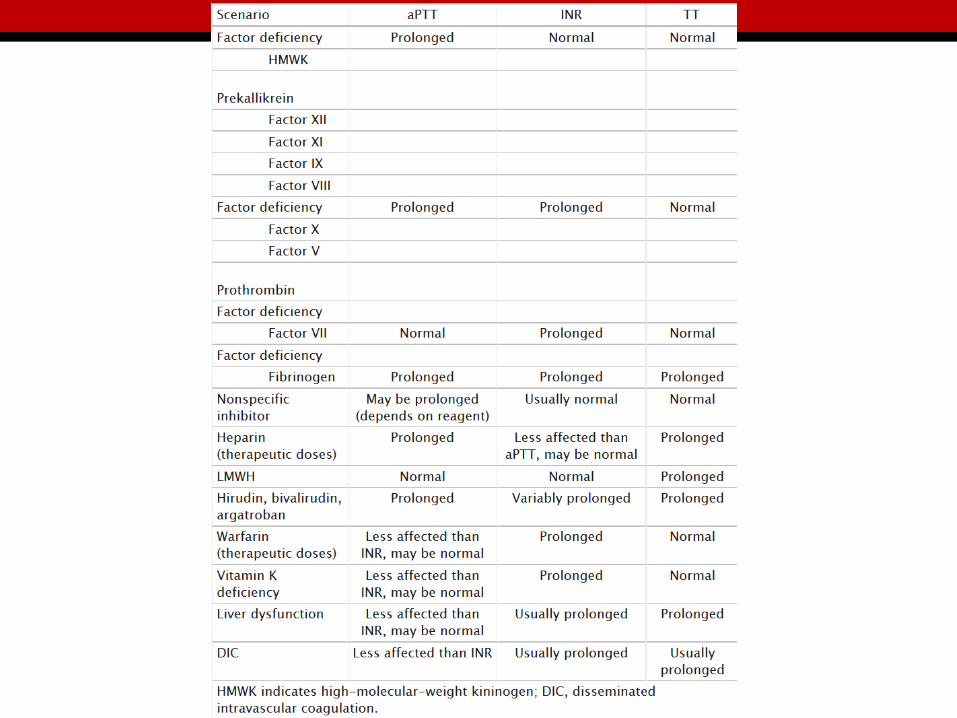
PTProthrombin
Time
Test of the extrinsic and common pathways. Clotting initiated
in the presence of Tissue Factor (thromboplastin).
Prolonged in:
• Vitamin K deficiency/antagonism (e.g. Warfarin)
• Deficiencies of factors VII, X, II and I (genetic/liver disease)
• DIC
• Transiently after a bolus of high dose heparin
INRInternational
Normalised Ratio
A standardisation of the PT (above).
Normal is 0.9-1.1. Typical targets:
• 2-3 in AF; venous-thrombolic prophylaxis
• 3-4 with mechanical heart valves; high-risk clotting
(a)PT
T
(activated) Partial
Thromboplastin
Time
Test of the intrinsic and common pathways. Clotting initiation
in the absence of Tissue Factor.
Prolonged in:
• Deficiency of all factors apart from VII
• Unfractionated Heparin therapy (LMWH doesn’t)
• (Warfarin may also cause a small rise in aPTT)
• DIC
•Anti-phospholid antibody/Lupus Anticoagulant (which
paradoxically increases thrombosis due to its effect on platelets)
Coagulation Tests - Part 1 of 2
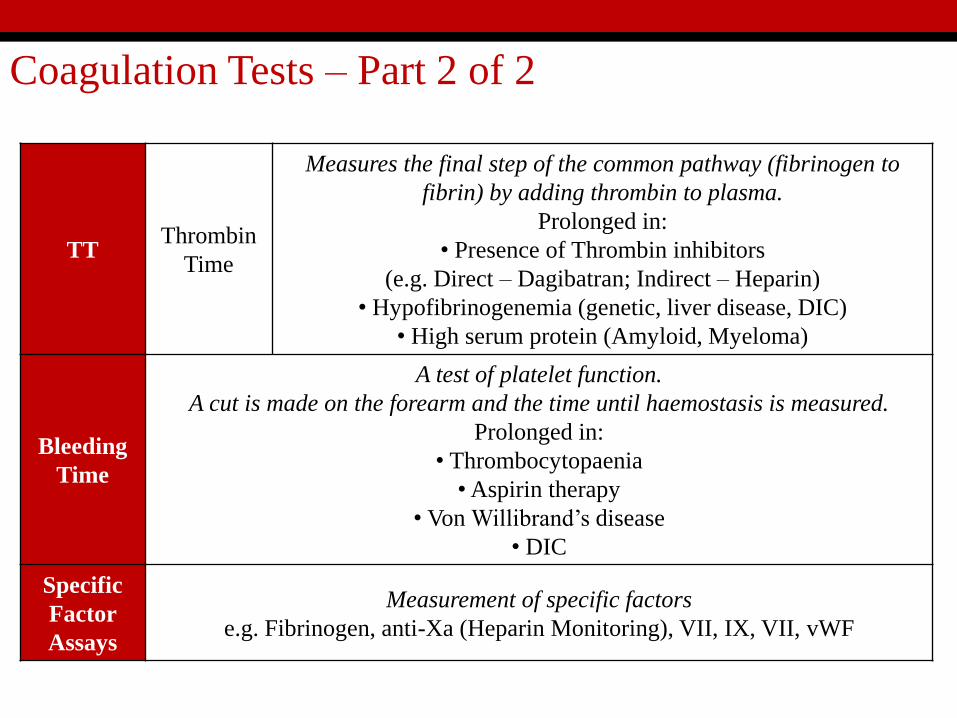
Coagulation Tests – Part 2 of 2
TTThrombin
Time
Measures the final step of the common pathway (fibrinogen to
fibrin) by adding thrombin to plasma.
Prolonged in:
• Presence of Thrombin inhibitors
(e.g. Direct – Dagibatran; Indirect – Heparin)
• Hypofibrinogenemia (genetic, liver disease, DIC)
• High serum protein (Amyloid, Myeloma)
Bleeding
Time
A test of platelet function.
A cut is made on the forearm and the time until haemostasis is measured.
Prolonged in:
• Thrombocytopaenia
•Aspirin therapy
• Von Willibrand’s disease
• DIC
Specific
Factor
Assays
Measurement of specific factors
e.g. Fibrinogen, anti-Xa (Heparin Monitoring), VII, IX, VII, vWF
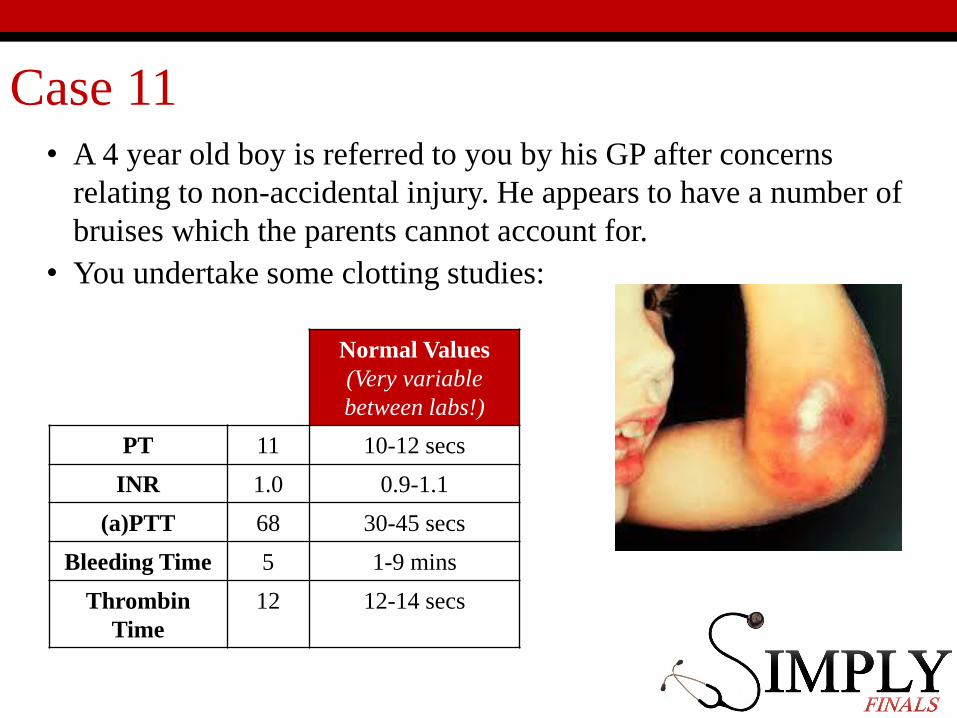
Case 11 • A 4 year old boy is referred to you by his GP after concerns
relating to non-accidental injury. He appears to have a number of
bruises which the parents cannot account for.
• You undertake some clotting studies:
Normal Values
(Very variable
between labs!)
PT 11 10-12 secs
INR 1.0 0.9-1.1
(a)PTT 68 30-45 secs
Bleeding Time 5 1-9 mins
Thrombin
Time
12 12-14 secs
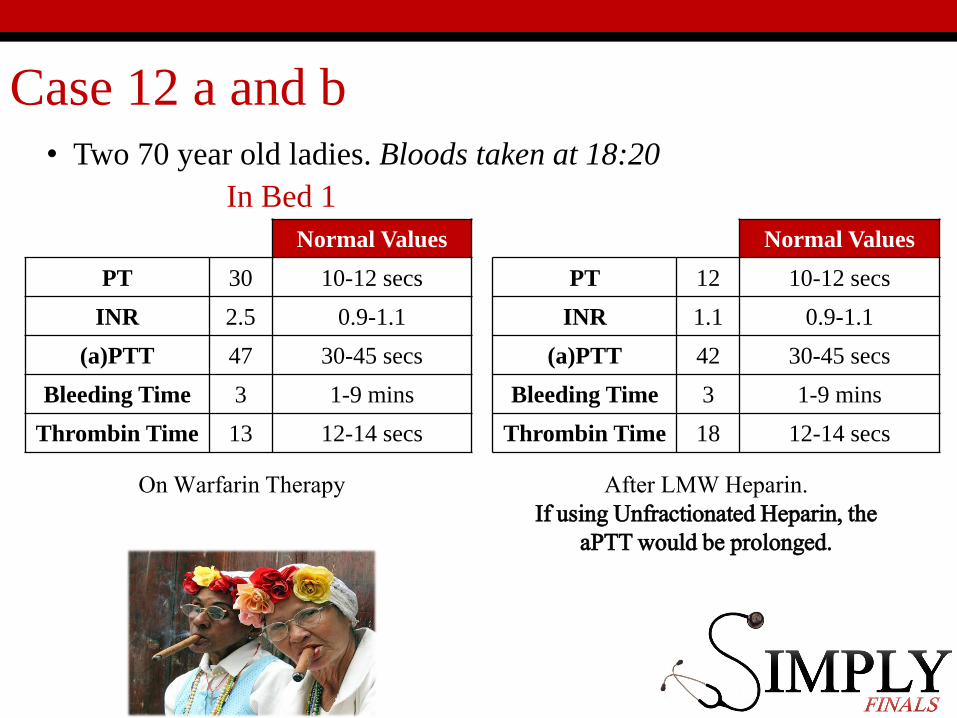
Case 12 a and b • Two 70 year old ladies. Bloods taken at 18:20
In Bed 1 In Bed 2
Normal Values
PT 30 10-12 secs
INR 2.5 0.9-1.1
(a)PTT 47 30-45 secs
Bleeding Time 3 1-9 mins
Thrombin Time 13 12-14 secs
Normal Values
PT 12 10-12 secs
INR 1.1 0.9-1.1
(a)PTT 42 30-45 secs
Bleeding Time 3 1-9 mins
Thrombin Time 18 12-14 secs
On Warfarin Therapy After LMW Heparin.If using Unfractionated Heparin, the
aPTT would be prolonged.
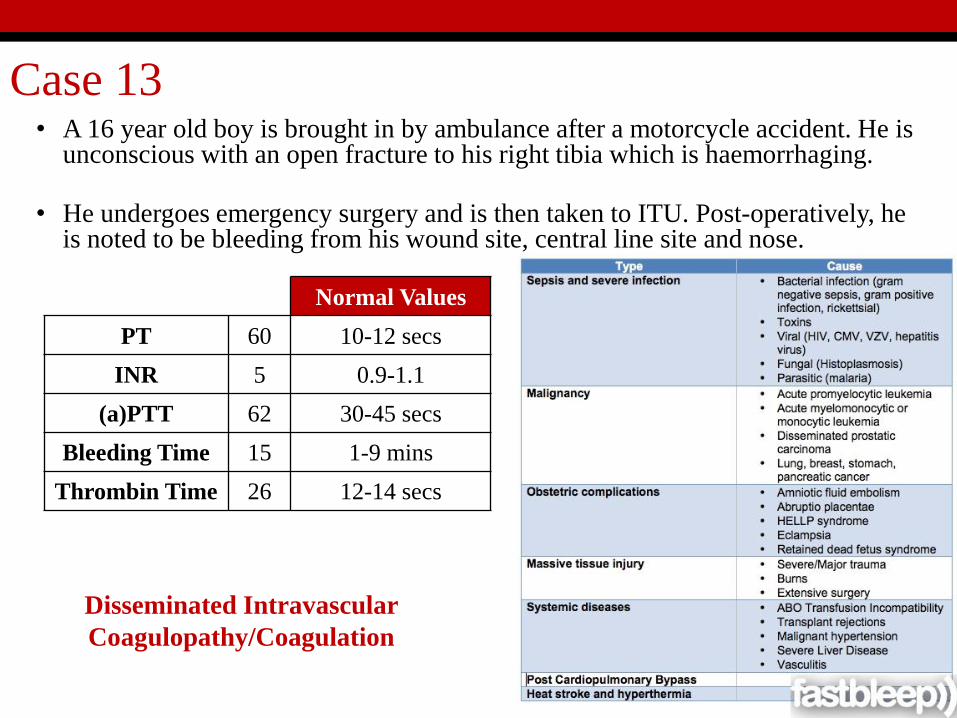
Case 13• A 16 year old boy is brought in by ambulance after a motorcycle accident. He is
unconscious with an open fracture to his right tibia which is haemorrhaging.
• He undergoes emergency surgery and is then taken to ITU. Post-operatively, he is noted to be bleeding from his wound site, central line site and nose.
Normal Values
PT 60 10-12 secs
INR 5 0.9-1.1
(a)PTT 62 30-45 secs
Bleeding Time 15 1-9 mins
Thrombin Time 26 12-14 secs
Disseminated Intravascular
Coagulopathy/Coagulation

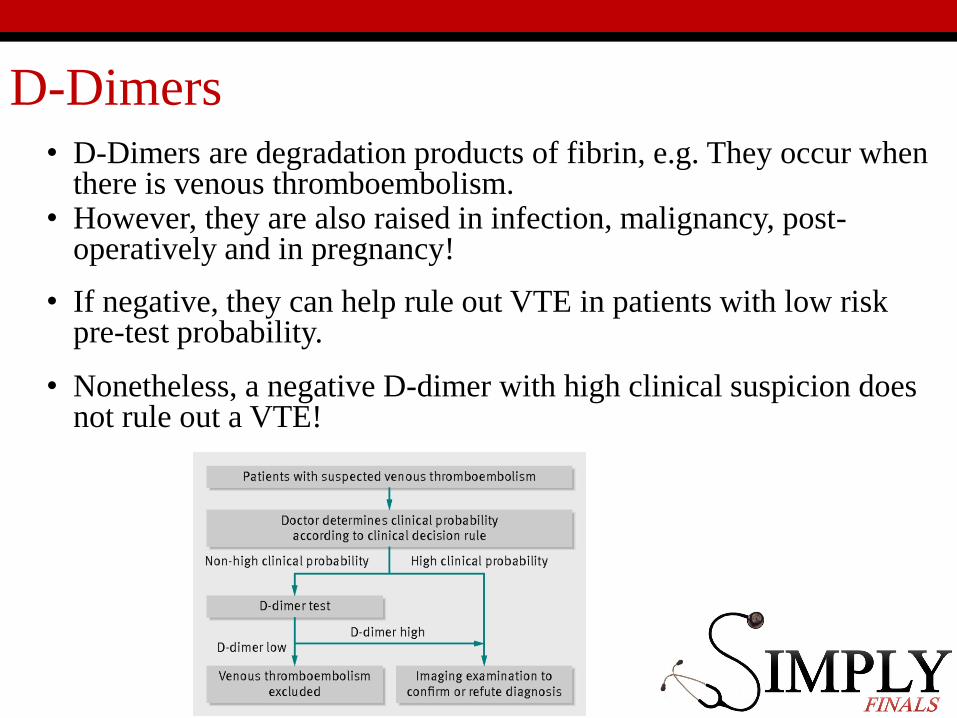
D-Dimers• D-Dimers are degradation products of fibrin, e.g. They occur when
there is venous thromboembolism.• However, they are also raised in infection, malignancy, post-
operatively and in pregnancy!
• If negative, they can help rule out VTE in patients with low risk pre-test probability.
• Nonetheless, a negative D-dimer with high clinical suspicion does not rule out a VTE!
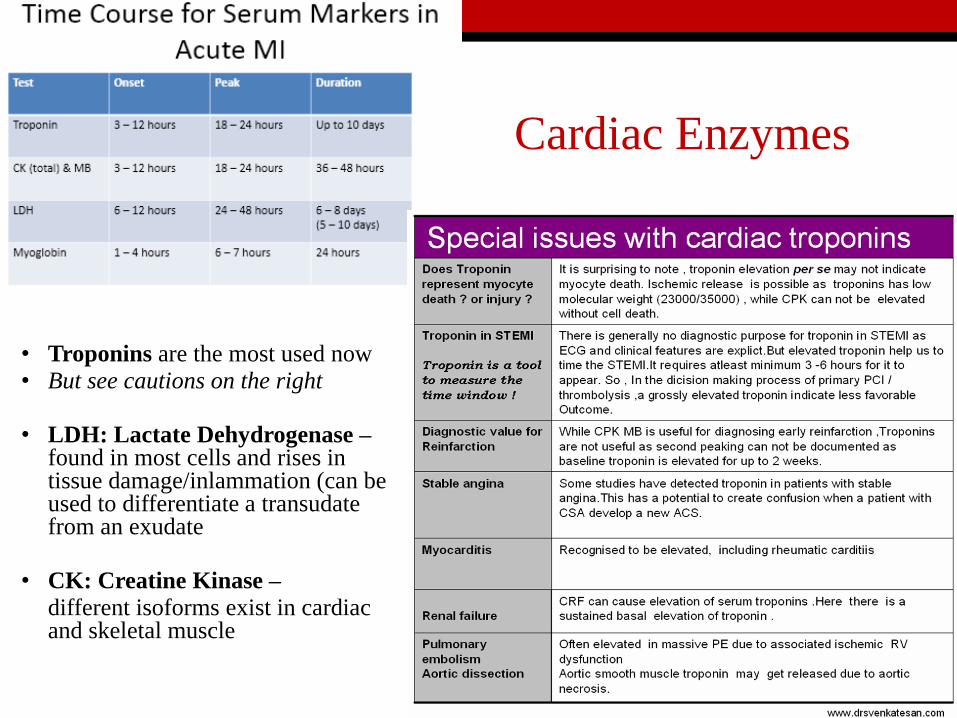
Cardiac Enzymes
• Troponins are the most used now• But see cautions on the right
• LDH: Lactate Dehydrogenase –found in most cells and rises in tissue damage/inlammation (can be used to differentiate a transudatefrom an exudate
• CK: Creatine Kinase –
different isoforms exist in cardiac and skeletal muscle
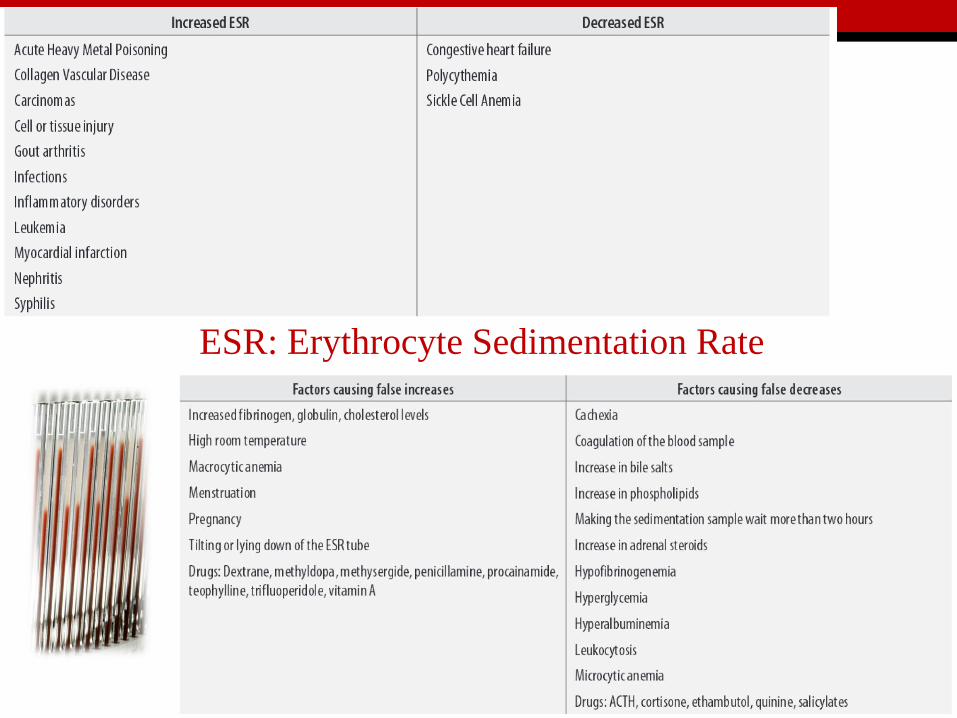
Inflammation/Acute Phase Reaction
ESR: Erythrocyte Sedimentation Rate
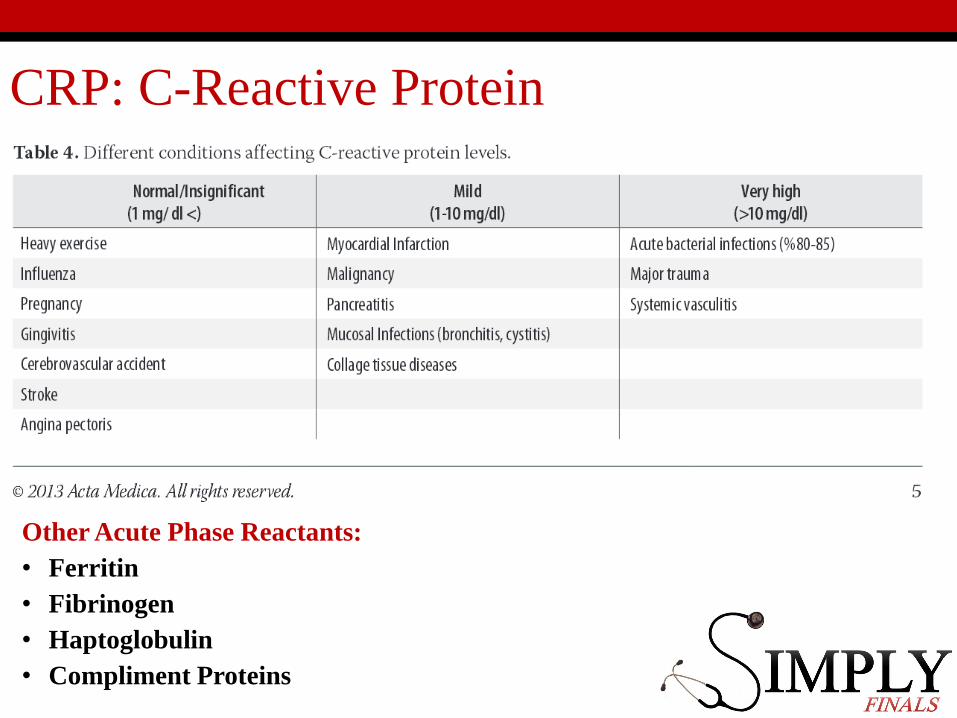
CRP: C-Reactive Protein
Other Acute Phase Reactants:
• Ferritin
• Fibrinogen
• Haptoglobulin
• Compliment Proteins
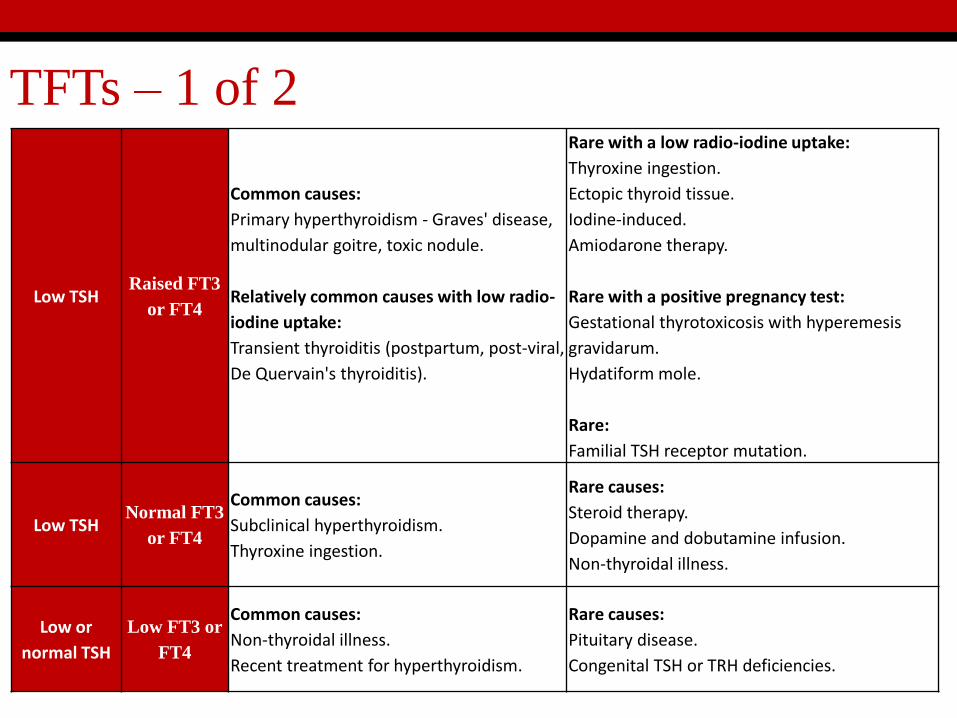
TFTs – 1 of 2
Low TSHRaised FT3
or FT4
Common causes:
Primary hyperthyroidism - Graves' disease,
multinodular goitre, toxic nodule.
Relatively common causes with low radio-
iodine uptake:
Transient thyroiditis (postpartum, post-viral,
De Quervain's thyroiditis).
Rare with a low radio-iodine uptake:
Thyroxine ingestion.
Ectopic thyroid tissue.
Iodine-induced.
Amiodarone therapy.
Rare with a positive pregnancy test:
Gestational thyrotoxicosis with hyperemesis
gravidarum.
Hydatiform mole.
Rare:
Familial TSH receptor mutation.
Low TSHNormal FT3
or FT4
Common causes:
Subclinical hyperthyroidism.
Thyroxine ingestion.
Rare causes:
Steroid therapy.
Dopamine and dobutamine infusion.
Non-thyroidal illness.
Low or
normal TSH
Low FT3 or
FT4
Common causes:
Non-thyroidal illness.
Recent treatment for hyperthyroidism.
Rare causes:
Pituitary disease.
Congenital TSH or TRH deficiencies.
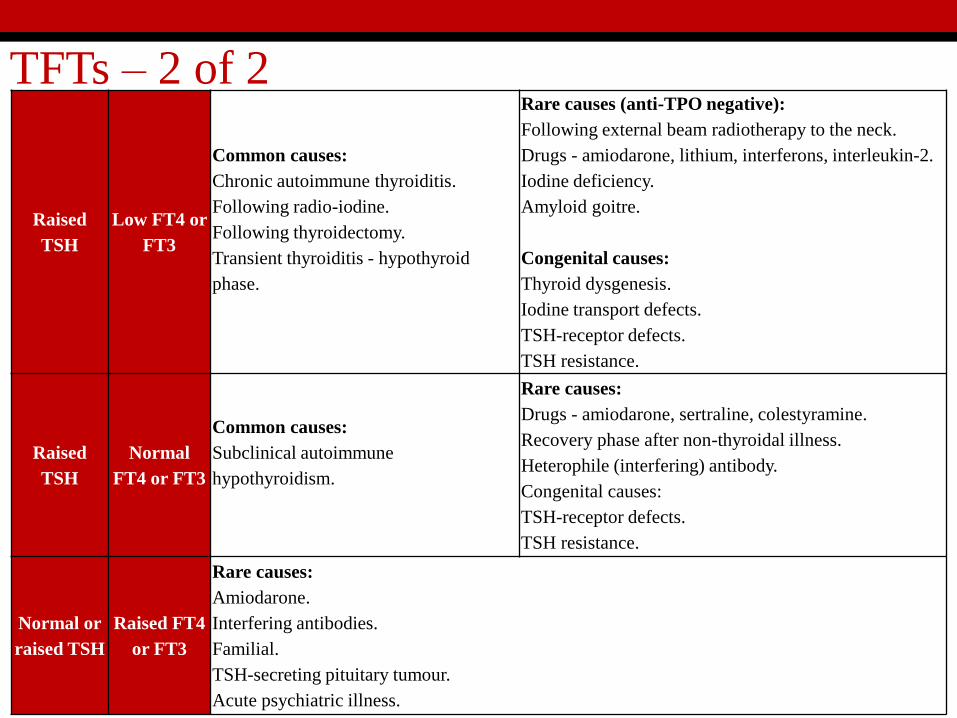
TFTs – 2 of 2
Raised
TSH
Low FT4 or
FT3
Common causes:
Chronic autoimmune thyroiditis.
Following radio-iodine.
Following thyroidectomy.
Transient thyroiditis - hypothyroid
phase.
Rare causes (anti-TPO negative):
Following external beam radiotherapy to the neck.
Drugs - amiodarone, lithium, interferons, interleukin-2.
Iodine deficiency.
Amyloid goitre.
Congenital causes:
Thyroid dysgenesis.
Iodine transport defects.
TSH-receptor defects.
TSH resistance.
Raised
TSH
Normal
FT4 or FT3
Common causes:
Subclinical autoimmune
hypothyroidism.
Rare causes:
Drugs - amiodarone, sertraline, colestyramine.
Recovery phase after non-thyroidal illness.
Heterophile (interfering) antibody.
Congenital causes:
TSH-receptor defects.
TSH resistance.
Normal or
raised TSH
Raised FT4
or FT3
Rare causes:
Amiodarone.
Interfering antibodies.
Familial.
TSH-secreting pituitary tumour.
Acute psychiatric illness.
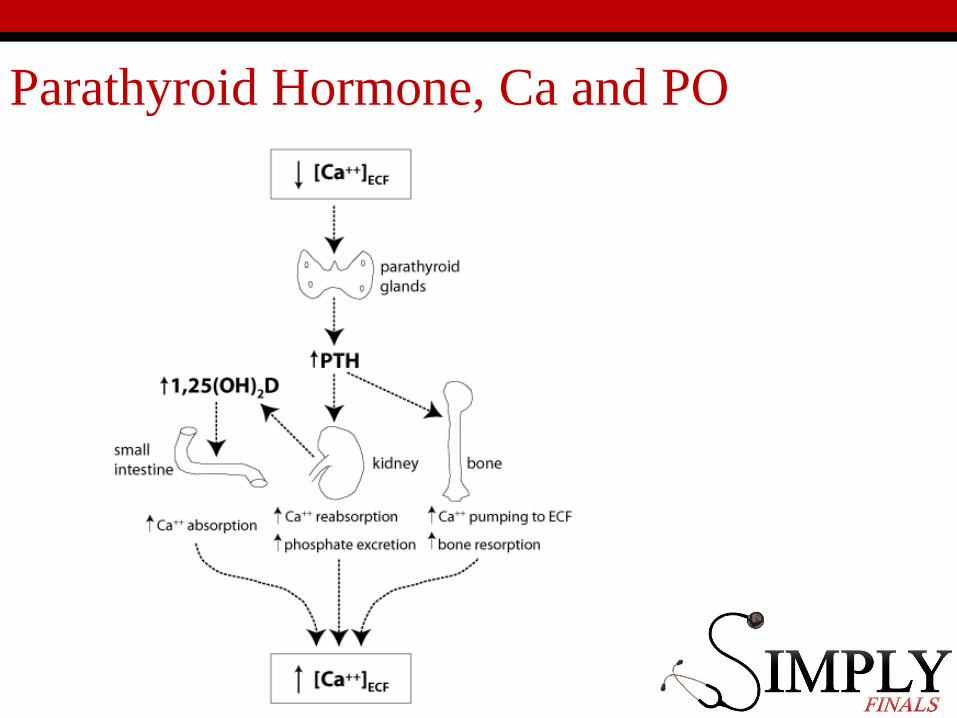
Parathyroid Hormone, Ca and PO
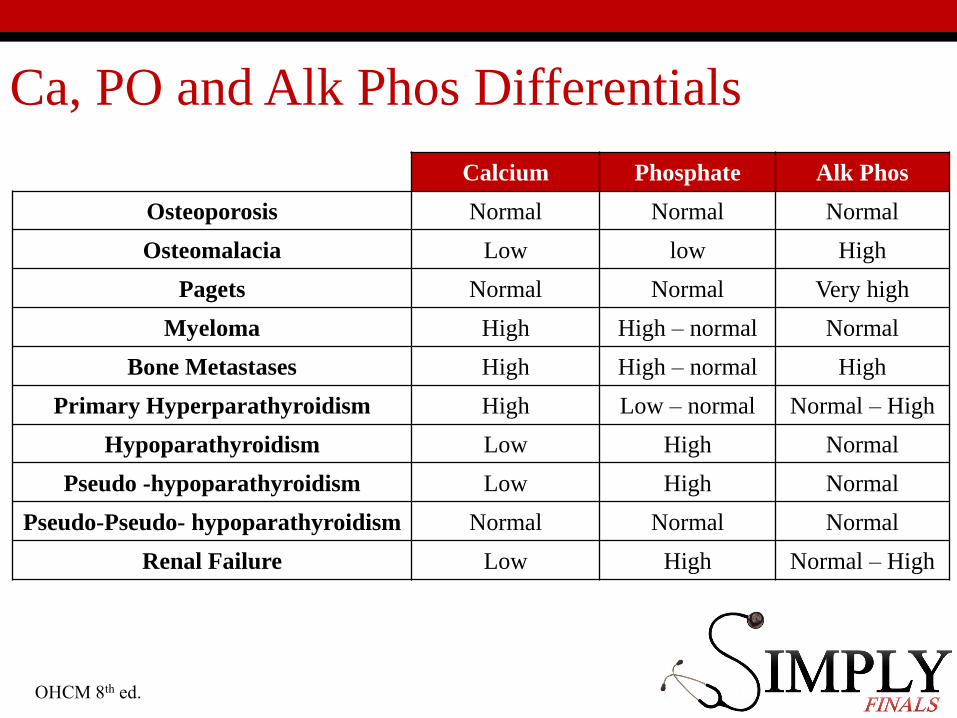
Ca, PO and Alk Phos Differentials
Calcium Phosphate Alk Phos
Osteoporosis Normal Normal Normal
Osteomalacia Low low High
Pagets Normal Normal Very high
Myeloma High High – normal Normal
Bone Metastases High High – normal High
Primary Hyperparathyroidism High Low – normal Normal – High
Hypoparathyroidism Low High Normal
Pseudo -hypoparathyroidism Low High Normal
Pseudo-Pseudo- hypoparathyroidism Normal Normal Normal
Renal Failure Low High Normal – High
OHCM 8th ed.
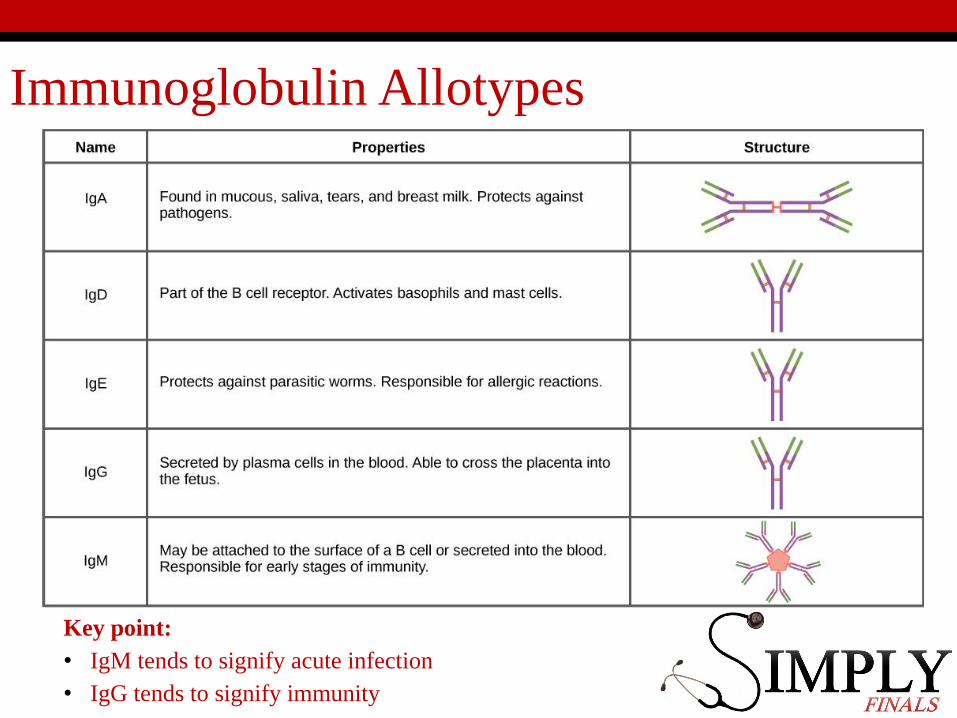
Immunoglobulin Allotypes
Key point:
• IgM tends to signify acute infection
• IgG tends to signify immunity
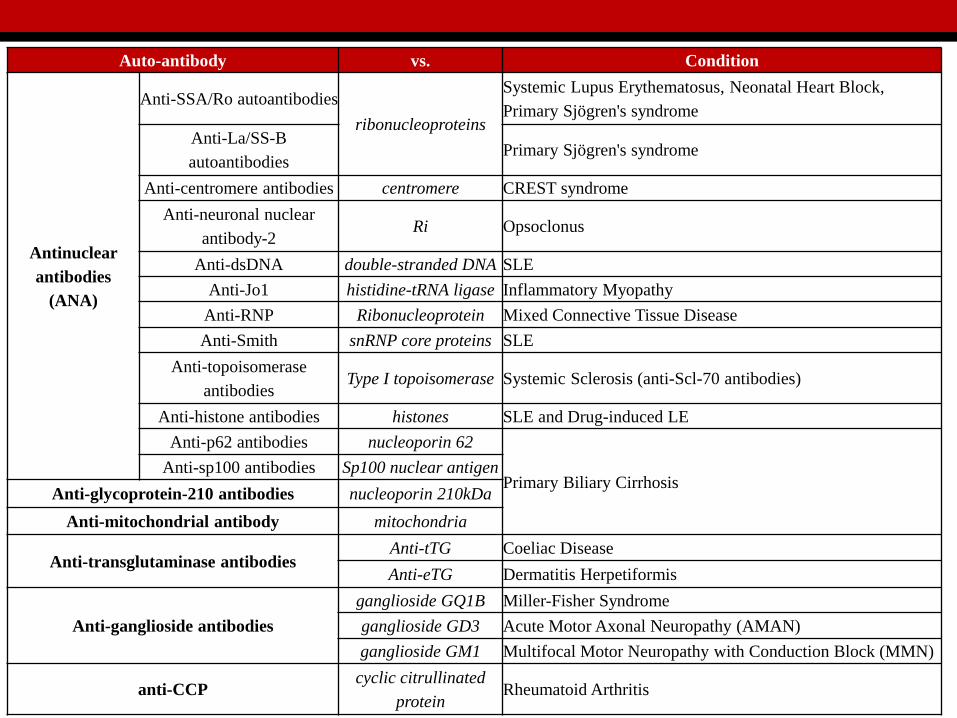
Auto-antibody vs. Condition
Antinuclear
antibodies
(ANA)
Anti-SSA/Ro autoantibodies
ribonucleoproteins
Systemic Lupus Erythematosus, Neonatal Heart Block,
Primary Sjögren's syndrome
Anti-La/SS-B
autoantibodiesPrimary Sjögren's syndrome
Anti-centromere antibodies centromere CREST syndrome
Anti-neuronal nuclear
antibody-2Ri Opsoclonus
Anti-dsDNA double-stranded DNA SLE
Anti-Jo1 histidine-tRNA ligase Inflammatory Myopathy
Anti-RNP Ribonucleoprotein Mixed Connective Tissue Disease
Anti-Smith snRNP core proteins SLE
Anti-topoisomerase
antibodiesType I topoisomerase Systemic Sclerosis (anti-Scl-70 antibodies)
Anti-histone antibodies histones SLE and Drug-induced LE
Anti-p62 antibodies nucleoporin 62
Primary Biliary CirrhosisAnti-sp100 antibodies Sp100 nuclear antigen
Anti-glycoprotein-210 antibodies nucleoporin 210kDa
Anti-mitochondrial antibody mitochondria
Anti-transglutaminase antibodiesAnti-tTG Coeliac Disease
Anti-eTG Dermatitis Herpetiformis
Anti-ganglioside antibodies
ganglioside GQ1B Miller-Fisher Syndrome
ganglioside GD3 Acute Motor Axonal Neuropathy (AMAN)
ganglioside GM1 Multifocal Motor Neuropathy with Conduction Block (MMN)
anti-CCPcyclic citrullinated
proteinRheumatoid Arthritis
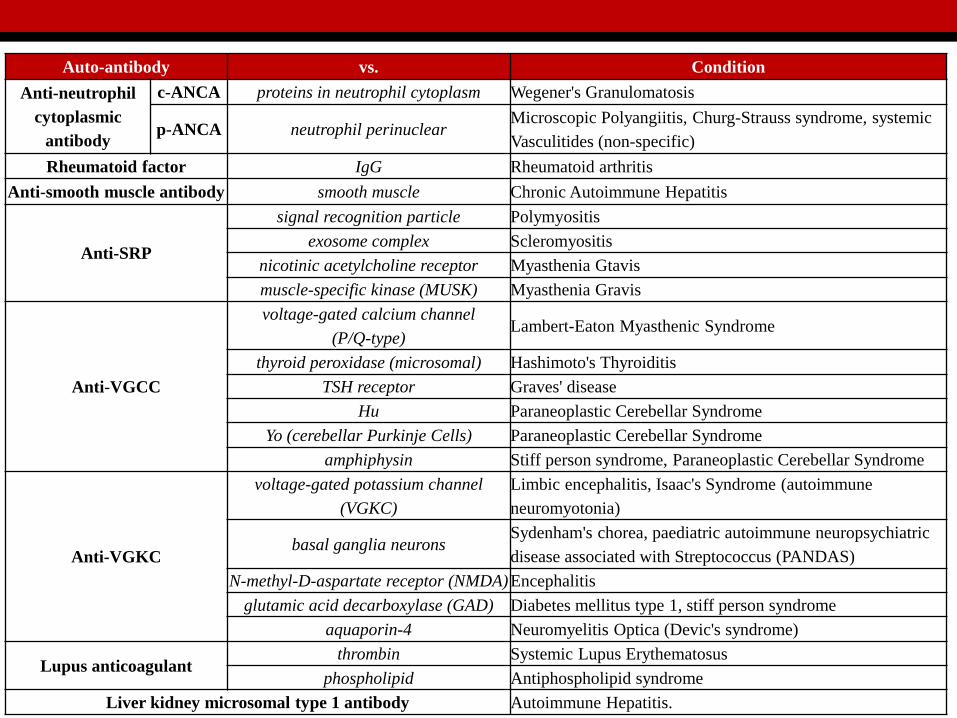
Auto-antibody vs. Condition
Anti-neutrophil
cytoplasmic
antibody
c-ANCA proteins in neutrophil cytoplasm Wegener's Granulomatosis
p-ANCA neutrophil perinuclearMicroscopic Polyangiitis, Churg-Strauss syndrome, systemic
Vasculitides (non-specific)
Rheumatoid factor IgG Rheumatoid arthritis
Anti-smooth muscle antibody smooth muscle Chronic Autoimmune Hepatitis
Anti-SRP
signal recognition particle Polymyositis
exosome complex Scleromyositis
nicotinic acetylcholine receptor Myasthenia Gtavis
muscle-specific kinase (MUSK) Myasthenia Gravis
Anti-VGCC
voltage-gated calcium channel
(P/Q-type)Lambert-Eaton Myasthenic Syndrome
thyroid peroxidase (microsomal) Hashimoto's Thyroiditis
TSH receptor Graves' disease
Hu Paraneoplastic Cerebellar Syndrome
Yo (cerebellar Purkinje Cells) Paraneoplastic Cerebellar Syndrome
amphiphysin Stiff person syndrome, Paraneoplastic Cerebellar Syndrome
Anti-VGKC
voltage-gated potassium channel
(VGKC)
Limbic encephalitis, Isaac's Syndrome (autoimmune
neuromyotonia)
basal ganglia neuronsSydenham's chorea, paediatric autoimmune neuropsychiatric
disease associated with Streptococcus (PANDAS)
N-methyl-D-aspartate receptor (NMDA)Encephalitis
glutamic acid decarboxylase (GAD) Diabetes mellitus type 1, stiff person syndrome
aquaporin-4 Neuromyelitis Optica (Devic's syndrome)
Lupus anticoagulantthrombin Systemic Lupus Erythematosus
phospholipid Antiphospholipid syndrome
Liver kidney microsomal type 1 antibody Autoimmune Hepatitis.
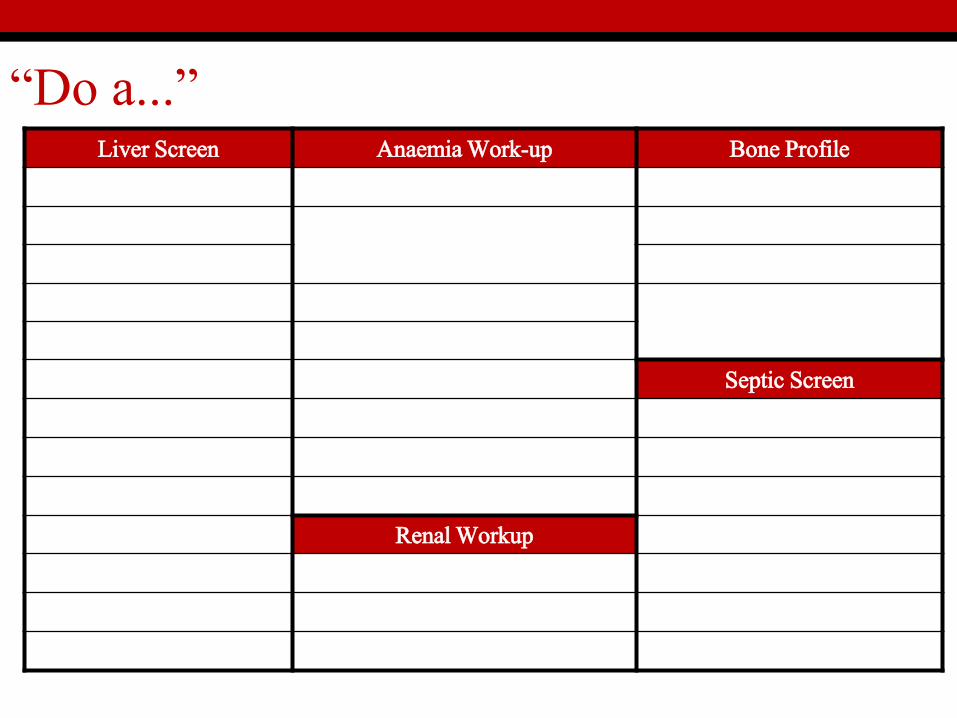
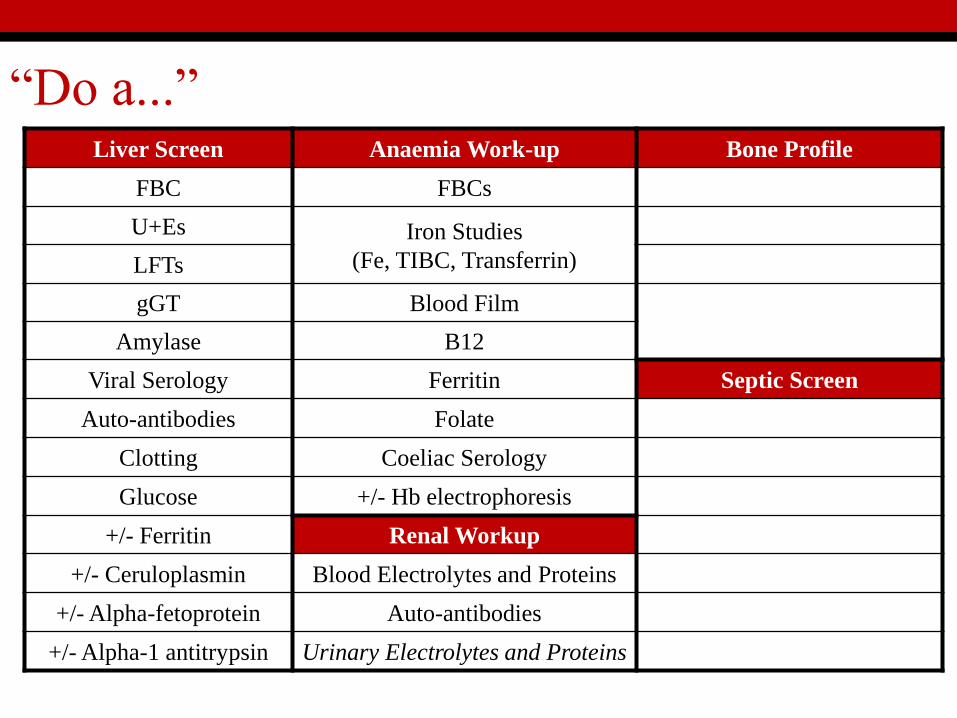
“Do a...”Liver Screen Anaemia Work-up Bone Profile
Septic Screen
Renal Workup
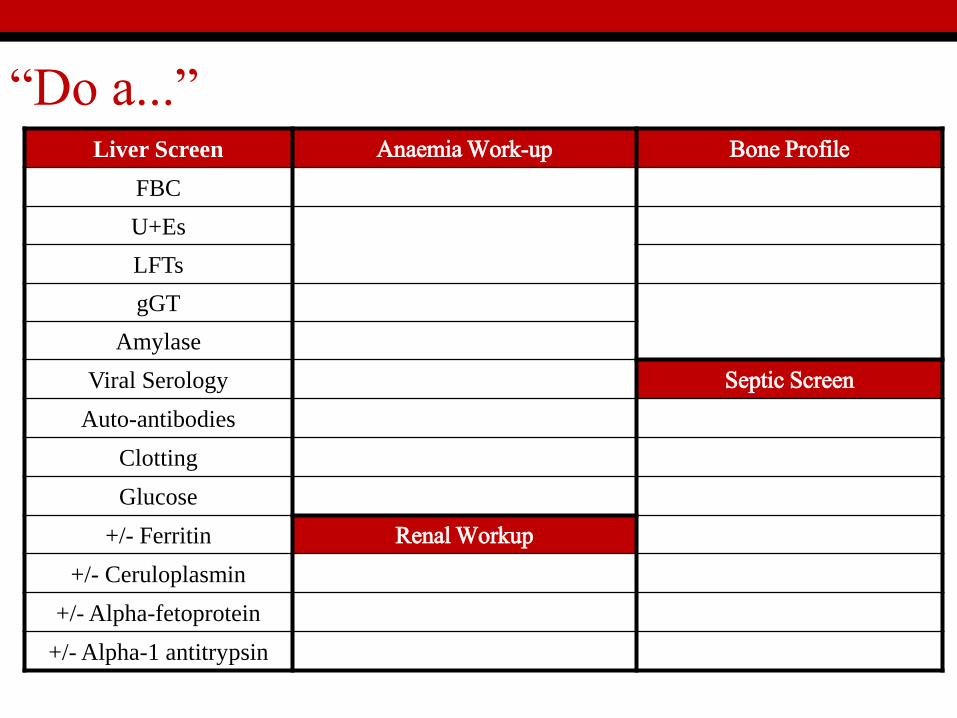
“Do a...”Liver Screen Anaemia Work-up Bone Profile
FBC
U+Es
LFTs
gGT
Amylase
Viral Serology Septic Screen
Auto-antibodies
Clotting
Glucose
+/- Ferritin Renal Workup
+/- Ceruloplasmin
+/- Alpha-fetoprotein
+/- Alpha-1 antitrypsin
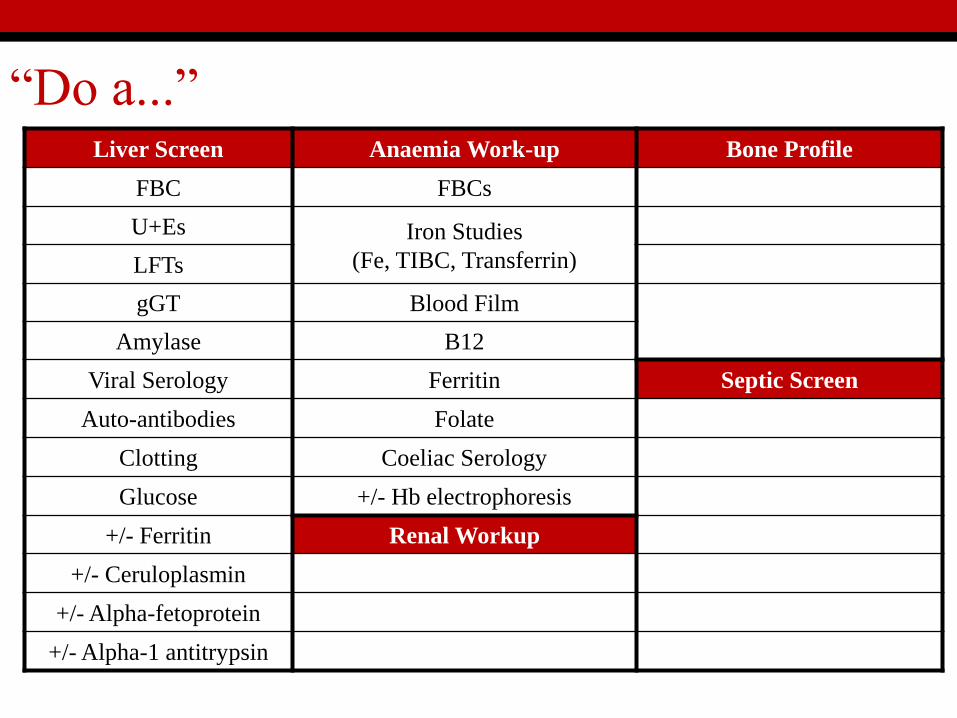
“Do a...”Liver Screen Anaemia Work-up Bone Profile
FBC FBCs
U+Es Iron Studies
(Fe, TIBC, Transferrin)LFTs
gGT Blood Film
Amylase B12
Viral Serology Ferritin Septic Screen
Auto-antibodies Folate
Clotting Coeliac Serology
Glucose +/- Hb electrophoresis
+/- Ferritin Renal Workup
+/- Ceruloplasmin
+/- Alpha-fetoprotein
+/- Alpha-1 antitrypsin
“Do a...”Liver Screen Anaemia Work-up Bone Profile
FBC FBCs
U+Es Iron Studies
(Fe, TIBC, Transferrin)LFTs
gGT Blood Film
Amylase B12
Viral Serology Ferritin Septic Screen
Auto-antibodies Folate
Clotting Coeliac Serology
Glucose +/- Hb electrophoresis
+/- Ferritin Renal Workup
+/- Ceruloplasmin Blood Electrolytes and Proteins
+/- Alpha-fetoprotein Auto-antibodies
+/- Alpha-1 antitrypsin Urinary Electrolytes and Proteins
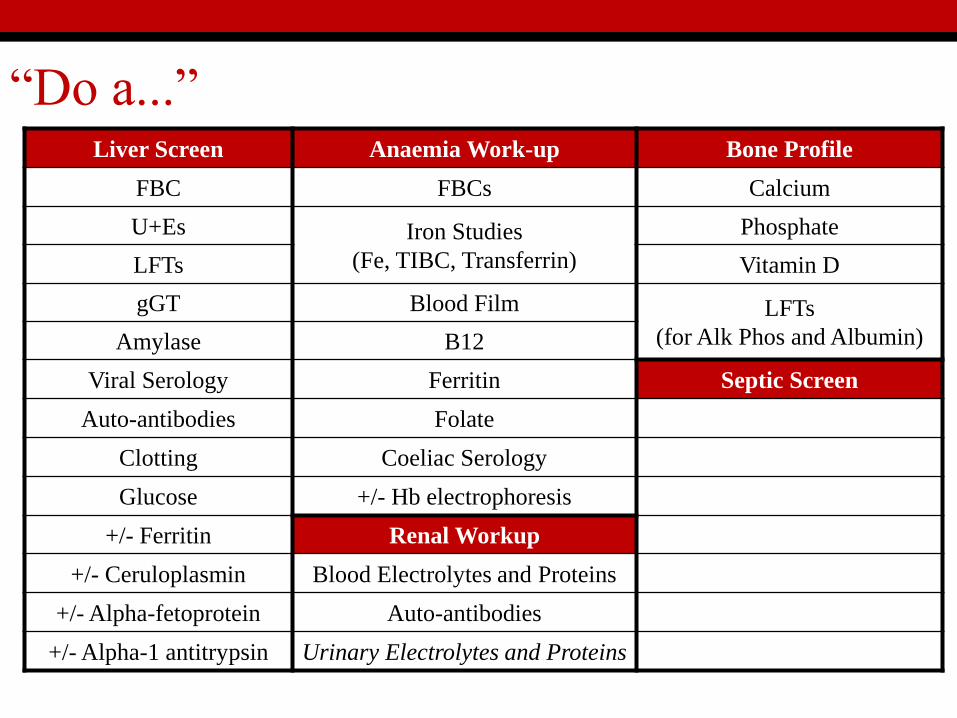
“Do a...”Liver Screen Anaemia Work-up Bone Profile
FBC FBCs Calcium
U+Es Iron Studies
(Fe, TIBC, Transferrin)
Phosphate
LFTs Vitamin D
gGT Blood Film LFTs
(for Alk Phos and Albumin)Amylase B12
Viral Serology Ferritin Septic Screen
Auto-antibodies Folate
Clotting Coeliac Serology
Glucose +/- Hb electrophoresis
+/- Ferritin Renal Workup
+/- Ceruloplasmin Blood Electrolytes and Proteins
+/- Alpha-fetoprotein Auto-antibodies
+/- Alpha-1 antitrypsin Urinary Electrolytes and Proteins
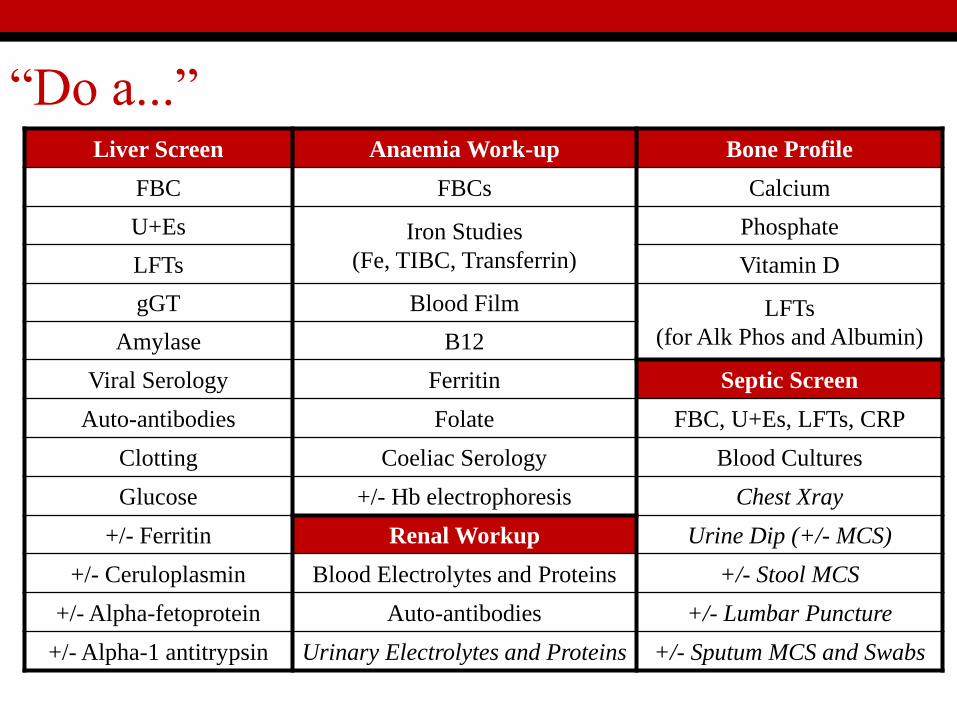
“Do a...”Liver Screen Anaemia Work-up Bone Profile
FBC FBCs Calcium
U+Es Iron Studies
(Fe, TIBC, Transferrin)
Phosphate
LFTs Vitamin D
gGT Blood Film LFTs
(for Alk Phos and Albumin)Amylase B12
Viral Serology Ferritin Septic Screen
Auto-antibodies Folate FBC, U+Es, LFTs, CRP
Clotting Coeliac Serology Blood Cultures
Glucose +/- Hb electrophoresis Chest Xray
+/- Ferritin Renal Workup Urine Dip (+/- MCS)
+/- Ceruloplasmin Blood Electrolytes and Proteins +/- Stool MCS
+/- Alpha-fetoprotein Auto-antibodies +/- Lumbar Puncture
+/- Alpha-1 antitrypsin Urinary Electrolytes and Proteins +/- Sputum MCS and Swabs
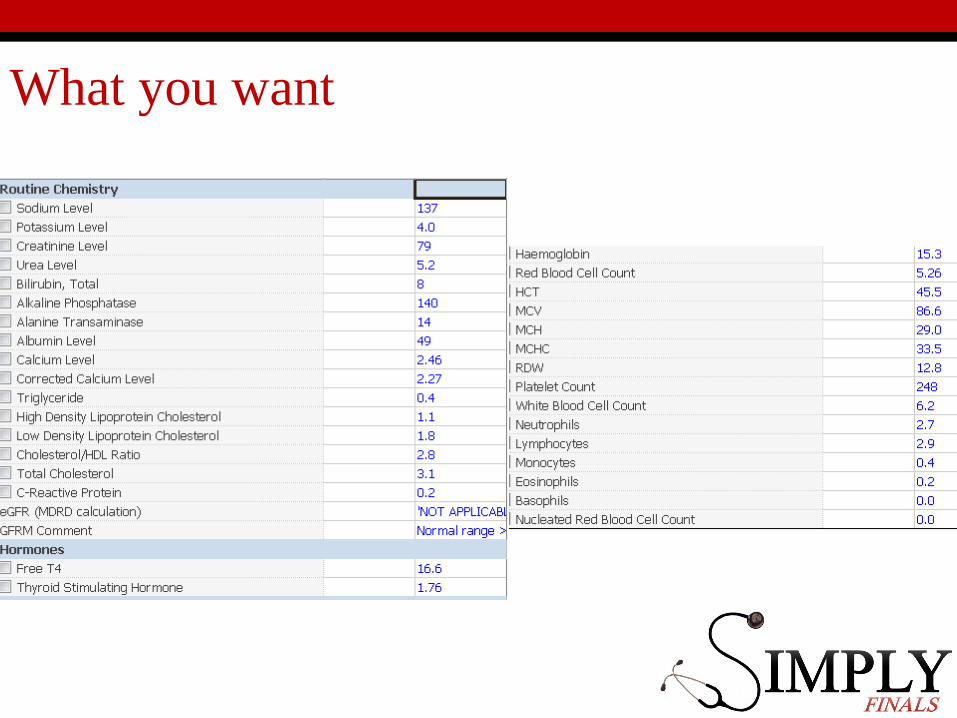
What you want
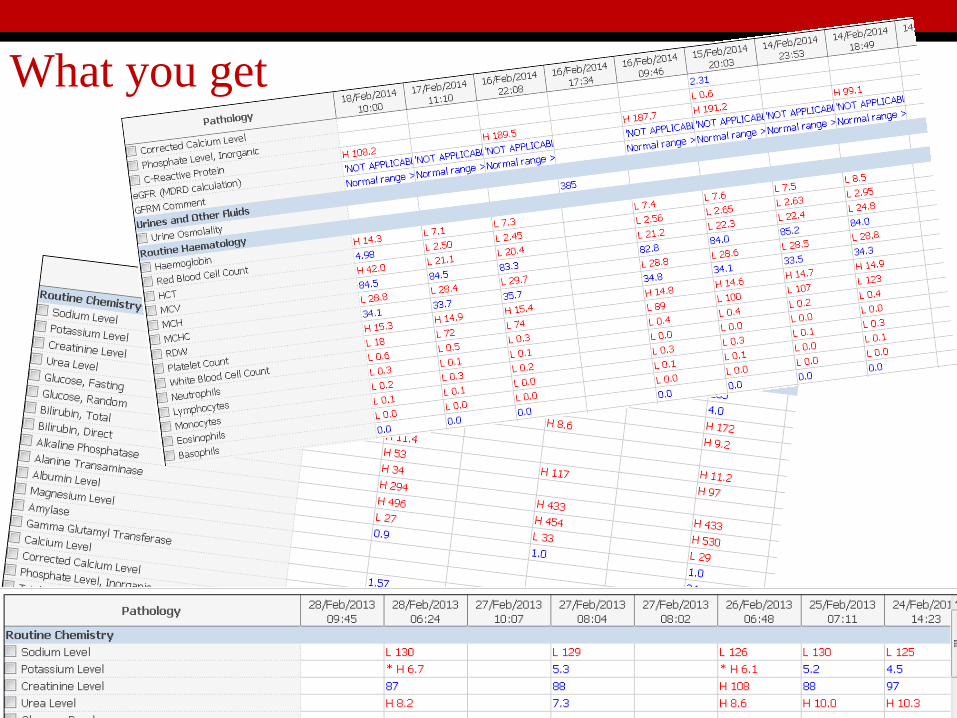
What you get
Thank-you
Any Questions?