interventions for paracetamol (acetaminophen)...
TRANSCRIPT
Interventions for paracetamol (acetaminophen) overdose
(Review)
Brok J, Buckley N, Gluud C
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2009, Issue 3
http://www.thecochranelibrary.com
Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
18AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
18ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
18REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
59DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Charcoal haemoperfusion versus no intervention (randomised trials), Outcome 1 Mortality. 61
Analysis 2.1. Comparison 2 Cysteamine versus no intervention (randomised trials), Outcome 1 Mortality. . . . . 62
Analysis 2.2. Comparison 2 Cysteamine versus no intervention (randomised trials), Outcome 2 Hepatotoxicity (aspartate
aminotransferase > 1000 IU/L). . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
Analysis 3.1. Comparison 3 Cysteamine versus dimercaprol (randomised trials), Outcome 1 Mortality. . . . . . 63
Analysis 3.2. Comparison 3 Cysteamine versus dimercaprol (randomised trials), Outcome 2 Maximum alanine
aminotransferase (IU/L). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Analysis 4.1. Comparison 4 Cysteamine versus methionine (randomised trials), Outcome 1 Mortality. . . . . . 64
Analysis 4.2. Comparison 4 Cysteamine versus methionine (randomised trials), Outcome 2 Hepatotoxicity (aspartate
aminotransferase > 1000 U/L). . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Analysis 5.1. Comparison 5 Methionine and supportive treatment versus supportive treatment (randomised trials),
Outcome 1 Mortality. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Analysis 5.2. Comparison 5 Methionine and supportive treatment versus supportive treatment (randomised trials),
Outcome 2 Hepatotoxicity (aspartate aminotransferase > 1000 U/L). . . . . . . . . . . . . . . . 65
Analysis 6.1. Comparison 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine (randomised trials),
Outcome 1 Mortality. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Analysis 6.2. Comparison 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine (randomised trials),
Outcome 2 Hepatotoxicity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Analysis 6.3. Comparison 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine (randomised trials),
Outcome 3 Any adverse event. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
Analysis 7.1. Comparison 7 Charcoal haemoperfusion in patients with fulminant hepatic failure (randomised trials),
Outcome 1 Mortality. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
Analysis 8.1. Comparison 8 5 h versus 10 h of charcoal haemoperfusion in patients with fulminant hepatic failure
(randomised trials), Outcome 1 Mortality. . . . . . . . . . . . . . . . . . . . . . . . . 68
Analysis 9.1. Comparison 9 Intravenous N-acatylcysteine versus ’placebo’ in patients with fulminant hepatic failure
(randomised trials), Outcome 1 Mortality. . . . . . . . . . . . . . . . . . . . . . . . . 68
68APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
72WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
72HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
72CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
72DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
73SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
73NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
73INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iInterventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
[Intervention Review]
Interventions for paracetamol (acetaminophen) overdose
Jesper Brok1, Nick Buckley2, Christian Gluud1
1Cochrane Hepato-Biliary Group, Copenhagen Trial Unit, Centre for Clinical Intervention Research, Department 3344, Rigshospitalet,
Copenhagen University Hospital, Copenhagen, Denmark. 2Professorial Medicine Unit, POWH Clinical School, University of NSW,
Randwick, Australia
Contact address: Jesper Brok, Cochrane Hepato-Biliary Group, Copenhagen Trial Unit, Centre for Clinical Intervention Research, De-
partment 3344, Rigshospitalet, Copenhagen University Hospital, Blegdamsvej 9, Copenhagen, DK-2100, Denmark. [email protected].
[email protected]. (Editorial group: Cochrane Hepato-Biliary Group.)
Cochrane Database of Systematic Reviews, Issue 3, 2009 (Status in this issue: Unchanged)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
DOI: 10.1002/14651858.CD003328.pub2
This version first published online: 19 April 2006 in Issue 2, 2006.
Last assessed as up-to-date: 21 February 2006. (Help document - Dates and Statuses explained)
This record should be cited as: Brok J, Buckley N, Gluud C. Interventions for paracetamol (acetaminophen) overdose. CochraneDatabase of Systematic Reviews 2006, Issue 2. Art. No.: CD003328. DOI: 10.1002/14651858.CD003328.pub2.
A B S T R A C T
Background
Poisoning with paracetamol (acetaminophen) is a common cause of hepatotoxicity in the Western World. Inhibition of absorption,
removal from the vascular system, antidotes, and liver transplantation are interventions for paracetamol poisoning.
Objectives
To assess the benefits and harms of interventions for paracetamol overdose.
Search strategy
We identified trials through electronic databases, manual searches of bibliographies and journals, authors of trials, and pharmaceutical
companies until December 2005.
Selection criteria
Randomised clinical trials and observational studies were included.
Data collection and analysis
The primary outcome measure was all-cause mortality plus liver transplantation. Secondary outcome measures were clinical symptoms,
(eg, hepatic encephalopathy, fulminant hepatic failure), hepatotoxicity, adverse events, and plasma paracetamol concentration. We used
Peto odds ratios and odds ratios with 95% confidence intervals (CI) for analysis of outcomes. Random- and fixed-effects meta-analyses
were performed.
Main results
Ten small and low-methodological quality randomised trials, one quasi-randomised study, and 48 observational studies were identified.
It was not possible to perform relevant meta-analyses of randomised trials that have addressed our outcome measures. Activated charcoal,
gastric lavage, and ipecacuanha are able to reduce the absorption of paracetamol, but the clinical benefit is unclear. Of these, activated
charcoal seems to have the best risk-benefit ratio. N-acetylcysteine seems preferable to placebo/supportive treatment, dimercaprol, and
cysteamine, but N-acetylcysteine’s superiority to methionine is unproven. It is not clear which N-acetylcysteine treatment protocol offers
the best efficacy. No strong evidence supports other interventions for paracetamol overdose. N-acetylcysteine may reduce mortality in
1Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

patients with fulminant hepatic failure (Peto OR 0.26, 95% CI 0.09 to 0.94, one trial). Liver transplantation has the potential to be
life saving in fulminant hepatic failure, but refinement of selection criteria for transplantation and long-term outcome reporting are
required.
Authors’ conclusions
Our results highlight a paucity of randomised trials on interventions for paracetamol overdose. Activated charcoal seems the best
choice to reduce absorption. N-acetylcysteine should be given to patients with overdose but the selection criteria are not clear. No N-
acetylcysteine regime has been shown to be more effective than any other. It is a delicate balance when to proceed to liver transplantation,
which may be life-saving for patients with poor prognosis.
P L A I N L A N G U A G E S U M M A R Y
Evidence on interventions for paracetamol (acetaminophen) overdose patients is weak
Poisoning with paracetamol (acetaminophen) is a common cause of hepatic injury. The evidence for all interventions for paracetamol
overdose is weak. Activated charcoal, gastric lavage, and ipecacuanha are able to reduce absorption of paracetamol if started within
one to two hours of paracetamol ingestion, but the clinical benefit is unclear. Activated charcoal seems to be the best choice if the
patient is compliant. N-acetylcysteine seems superior to no intervention and other antidotes (dimercaprol, cysteamine) and should be
administered to patients at significant risk of hepatic damage. However, N-acetylcysteine superiority to methionine is unclear. Liver
transplantation will clearly benefit patients with irreversible hepatic failure. However, identifying such patients early is problematic and
the long-term outcomes in this group of patients have not been reported. Other interventions have not shown any clinical benefit for
paracetamol overdose.
B A C K G R O U N D
Paracetamol (acetaminophen) is a mild analgesic and antipyretic
agent, which is used frequently worldwide (O’Grady 1997). In
therapeutic doses (500 mg to 1000 mg, three to four times per
day) it is known to have very few adverse events (Koch-Weser
1976). However, an overdosage can result in severe hepatotoxicity.
In general, a single dose of 150 mg/kg or more carries a risk of
liver damage, but smaller doses may also cause liver damage (
Kwan 2005). Currently paracetamol overdose is the leading cause
of acute liver failure in many countries (Lee 2004; Morgan 2005).
There are different types of interventions for paracetamol over-
dose. First, to inhibit absorption of the ingested paracetamol. Sec-
ond, to remove paracetamol from the blood after the drug is ab-
sorbed. Third, to prevent the conversion of paracetamol by cy-
tochrome P-450 2E1 to the hepatotoxic metabolite N-acetyl-p-
benzo-quinoneimine (NAPQI). Fourth, to detoxify NAPQI or to
prevent toxic effects due to this metabolite once it has been formed.
Fifth, only in severe cases, to treat fulminant hepatic failure.
Both gastric lavage, activated charcoal, and ipecacuanha (ipecac
syrup (an emetic)) may reduce paracetamol absorption within the
first few hours after ingestion (Underhill 1990; Buckley 1999a).
However, delaying these interventions wanes the potential benefi-
cial effect. Once absorbed, it has been suggested that paracetamol
can be removed from the blood with charcoal haemoperfusion (
O’Grady 1988; Higgens 1996).
Cimetidine has been suggested because it is an inhibitor of the cy-
tochrome P-450 that catalyses the activation of the toxic metabo-
lite NAPQI (Speeg 1995). However, Burkhart et al (Burkhart
1995) found no beneficial effect of adding cimetidine to N-acetyl-
cysteine in a quasi-randomised study.
Several antidotes (methionine, cysteine, cysteamine, and dimer-
caprol) that detoxify NAPQI have been assessed. Of these, cys-
teamine or methionine decreased the risk of developing liver dam-
age after a paracetamol overdose in randomised trials (Douglas
1976; Hamlyn 1981). In an observational study N-acetylcysteine
seemed equally effective as cysteamine and methionine and notice-
ably free of adverse effects (Prescott 1979). Ever since, N-acetyl-
cysteine has been accepted as the antidote of choice for paraceta-
mol overdose. Subsequently N-acetylcysteine was also found to
reduce mortality in patients with fulminant hepatic failure after
paracetamol overdose (Keays 1991).
Treatment with N-acetylcysteine is usually based on the patients’
paracetamol concentration. Different risk lines for hepatotoxicity
in graphs plotting concentration versus time are used to initiate
treatment. These ’nomograms’ are known as the high risk- (300
line), the probable risk- (200 line), and the possible risk-line (150
2Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

line) (Rumack 1975; Prescott 1979; Smilkstein 1991). If parac-
etamol levels are not available or not used, treatment is started if
more than 150 mg/kg (or more than 10 g) have been ingested.
The ultimate intervention for irreversible liver damage following
paracetamol overdose is liver transplantation. However, which cri-
teria to use for transplantation are debated (Bailey 2003). Further-
more, the decision to proceed to liver transplantation may have
to be taken in the context of a deliberate suicidal attempt, often
upon a background of mental illness and/or alcohol abuse (Bernal
1998).
This updated systematic review tries to assess the benefits and
harms of interventions for paracetamol overdose.
O B J E C T I V E S
To assess the benefits and harms of interventions for paracetamol
overdose.
M E T H O D S
Criteria for considering studies for this review
Types of studies
We included randomised trials examining interventions for parac-
etamol overdose regardless of sources of publication and language.
We expected that few randomised trials had been conducted.
Therefore, randomised trials with human volunteers, quasi-ran-
domised studies, and non-randomised studies were also included.
However, evidence of this kind has been reported under ’Ex-
ploratory analyses’ in the result section and was interpreted con-
servatively.
Several observational studies have evaluated the efficacy of N-
acetylcysteine and other antidotes. Inclusion criteria, number
of patients included, and outcome measures varied substantially
among the studies. Accordingly, we decided to specify four study
inclusion criteria regarding intervention with N-acetylcysteine and
other antidotes (Buckley 1999b) as follows:
(1) Consecutive, unselected patients with the majority of the pa-
tients not being referred from other centres for treatment.
(2) At least 20 patients.
(3) Mortality data or number of patients with an aspartate amino-
transferase (AST) or alanine aminotransferase (ALT) more than
1000 units IU/L.
(4) Data stratified by time from ingestion to antidote intervention.
Randomised trials or other studies examining interventions for
drug poisoning (which often included many patients who had
ingested paracetamol) were not included in this review.
Types of participants
Patients who have ingested a paracetamol overdose.
The definition of a paracetamol overdose is not a clear cut-off and
the risk depends on many factors eg, age, weight, co-morbidities,
medical treatment, etc. Patients are unlikely to develop hepatotox-
icity if they have ingested less than 150 mg/kg (Vale 2004) or less
than 10 g in adults (Buckley 1999a). However, the prediction of a
patient’s risk based on reported dose of paracetamol may be lim-
ited as patients or relatives are often unaware of the exact amount
ingested.
The plasma paracetamol concentration stratified by time from
ingestion indicates the risk of developing hepatotoxicity. This can
be used to define a paracetamol overdose and whether to initiate
treatment with antidotes. Three ’nomograms’ have been suggested:
• the high risk-line (300 line) that joins plots of 300 mg/L
of paracetamol at four hours and 10 mg/L at 24 hours
on semi-logarithmic graph (Smilkstein 1991).
• the probable risk-line (200 line) (200 mg/L at four hours
and 7 mg/L at 24 hours) (Rumack 1975; Prescott 1979).
• the possible risk-line (150 line) (150 mg/L at four hours
and 5 mg/L at 24 hours) (Smilkstein 1991).
Types of interventions
• Intervention with gastric lavage, ipecacuanha, or acti-
vated charcoal in any dose or duration compared with
placebo/no intervention or with each other.
• Intervention with charcoal haemoperfusion compared
with placebo/no interventions or other interventions
for paracetamol overdose.
• Intervention with antidotes (cimetidine, cysteamine,
methionine, dimercaprol, and N-acetylcysteine) com-
pared with each other, with placebo/no interventions,
or other interventions for paracetamol overdose.
• Different doses, durations, or way of administration
(peroral or intravenously) of N-acetylcysteine compared
with each other.
• Intervention with liver transplantation compared with
conservative treatment for paracetamol-induced hepatic
failure.
Co-interventions were allowed if received equally in the interven-
tions arms.
We did not want to examine other interventions for liver failure
(eg, different types of liver support) and secondary complications
to liver failure such as hepato-renal failure, hepatic encephalopathy,
and cerebral oedema.
Types of outcome measures
3Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Primary outcome measure:(1) Mortality plus liver transplantation.
Secondary outcome measures:(2) Clinical symptoms, ie, hepatic encephalopathy, fulminant hep-
atic failure, and renal failure.
(3) Hepatotoxicity (defined as number of patients with serum
aspartate aminotransferase or serum alanine aminotransferase >
1000 IU/L).
(4) Adverse events.
(5) Plasma paracetamol concentration (eg, plasma paracetamol
above a risk line (nomogram)), fall in plasma paracetamol versus
time, absorption of paracetamol measured as area under the curve
(AUC) of the plasma (or urine) concentration versus time curve.
Search methods for identification of studies
As described in ’Appendix 1’, we searched The Cochrane Hepato-Biliary Group Controlled Trials Register and Miscellaneous Database,The Cochrane Central Register of Controlled Trials (CENTRAL) in
The Cochrane Library , MEDLINE, EMBASE, and Science Ci-tation Index Expanded (Royle 2003). Trials were also identified
through manual searches of bibliographies in relevant articles,
hand searches of Liver International, Journal of Hepatology, Hepa-tology, Journal of Viral Hepatitis, Gastroenterology, and Gut. We also
wrote to authors of included trials and pharmaceutical companies.
Searches were performed by December 2005.
Data collection and analysis
JB and NB evaluated whether the trials fulfilled the inclusion crite-
ria and extracted data. Disagreements were resolved by discussion.
Excluded trials were listed with the reason for exclusion. We wrote
to the principal investigator of included trials to ask for relevant
data if such were not presented in the published reports.
Methodological quality
Randomisation and blinding were extracted as markers of method-
ological quality (Schulz 1995; Moher 1998; Kjaergard 2001; Jüni
2001; Als-Nielsen 2004). We assessed them as follows:
Allocation sequence generation
• Adequate if a computer, table of random numbers, coin
tossing, or similar was used to generate a sequence for
the allocation of patients.
• Unclear if the trial was described as randomised, but
the methods used for the allocation sequence generation
were not described.
• Inadequate if a system involving dates, names, admit-
tance numbers or similar were used for the allocation
of patients. These trials were classified as quasi-ran-
domised.
Allocation concealment
• Adequate if the allocation of patients involved a central
independent unit, sealed envelopes, on-site locked com-
puter, or identically appearing numbered drug bottles
or containers prepared by an independent pharmacist.
• Unclear if the trial was described as randomised, but the
methods used for the allocation sequence concealment
were not described.
• Inadequate if the allocation sequence was known to the
investigators who assigned participants eg, open table
of random numbers or similar.
Blinding
• Adequate if the trial claimed to be double blind and
ribavirin placebo tablets were used.
• Unclear if the trial claimed to be double blind but the
method of blinding was not described.
• Inadequate if the trial was not double blind.
Statistical methods
The analyses were performed in Review Manager version 4.2 (
RevMan 2003). Data were analysed by intention-to-treat includ-
ing all patients irrespective of compliance or follow-up.
Binary outcomes were expressed as odds ratios (OR) and con-
tinuous outcomes as weighted mean differences (WMD) with
95% confidence intervals (CI). Rare events (mortality plus liver
transplantation) were estimated by Peto odds ratio (Deeks 1998).
Data were analysed by both a random-effects model (DerSimonian
1986) and a fixed-effect model (DeMets 1987). If the results of
both analyses gave the same overall result regarding significance,
only the results of the fixed-effect model analysis is reported. Re-
gression analyses were performed to estimate funnel plot asymme-
try (Egger 1997). Heterogeneity was explored by chi-squared test
with significance set at P-value less than 0.10 and the quantity of
heterogeneity was measured by I2 (Higgins 2002).
We intended to assess the methodological quality of the included
trials in sensitivity analyses: adequate versus unclear or inadequate
generation of allocation sequence, allocation concealment, and
blinding.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
Search results
We identified 861 references through the electronic searches of
The Cochrane Hepato-Biliary Group Controlled Trials Register (n =
11), The Cochrane Hepato-Biliary Group Miscellaneous database (n
4Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

= 21), The Cochrane Central Register of Controlled Trials in TheCochrane Library (n = 44), MEDLINE (n = 252), EMBASE (n =
318), and Science Citation Index Expanded (n = 215). Of these ref-
erences, we excluded 797 clearly irrelevant references and dupli-
cates. Accordingly, this review includes data from 64 references on
10 randomised clinical trials, one quasi-randomised study, 30 ob-
servational studies in patients with paracetamol overdose, and 18
trials including healthy human volunteers. Details of these studies
are given in the table ’Characteristics of included studies’.
Randomised clinical trials
Prevention of absorption
One trial randomised patients to no intervention, activated char-
coal, ipecacuanha, or gastric lavage (Underhill 1990). However,
there are doubts about the quality of the randomisation in this
trial (see ’Methodological quality of included studies’).
Charcoal haemoperfusion
Two trials randomised patients with paracetamol-induced fulmi-
nant hepatic failure (O’Grady 1988) or acute paracetamol over-
dose (Gazzard 1974a) to charcoal haemoperfusion or no interven-
tion.
Antidotes
Three trials randomised patients to different antidotes (me-
thionine, cysteine, cysteamine and dimercaprol) (Douglas 1976;
Hughes 1977; Hamlyn 1981). One trial randomised patients to
different infusion rates of N-acetylcysteine (Kerr 2005). One trial
randomised patients with paracetamol-induced fulminant hepatic
failure to N-acetylcysteine or placebo (Keays 1991).
Other interventions
Two trials randomised patients to heparin (Gazzard 1974) or fresh
frozen plasma (Gazzard 1975) compared to no intervention.
Non-randomised studies or studies including human volun-
teers
Prevention of absorption
Five observational studies (Amitai 1987; Kirk 1991; Bond 1993;
Buckley 1999a; Montoya-Cabrera 1999), 15 randomised trials in-
cluding human volunteers (Levy 1976; Neuvonen 1983; Galinsky
1984; McNamara 1988; McNamara 1989; Rose 1991; Grierson
2000; Yeates 2000; Rangan 2001; Green 2001; Christophersen
2002; Saincher 1997; Sato 2003; Green 2004; Ly 2004), and two
non-randomised including human volunteers (Remmert 1990;
Hassig 1993) were identified. The interventions investigated were
activated charcoal, ipecacuanha, gastric lavage, or whole bowel ir-
rigation.
Charcoal haemoperfusion
We identified one observational study (Silk 1978) that inves-
tigated charcoal haemoperfusion for patients with paracetamol-
induced fulminant hepatic failure. One observational study (
Higgens 1996) investigated the efficacy of haemoperfusion for
acute paracetamol poisoning.
Antidotes
We identified one quasi-randomised trial (Burkhart 1995), 13
observational studies (Crome 1976; Prescott 1976; Smith 1978;
Prescott 1979; Vale 1981; Smilkstein 1988; Harrison 1990; Parker
1990; Smilkstein 1991; Spiller 1994; Buckley 1999b; Woo 2000;
Ayonrinde 2005), and one randomised trial including human vol-
unteers (Chen 1985) examining different antidotes (cysteamine,
methionine, dimercaprol, N-acetylcysteine, or cimetidine) for
paracetamol overdose.
Liver transplantation
Ten observational studies (O’Grady 1991; Mutimer 1994; Schiodt
1996; Anand 1997; Bernal 1998; Shakil 2000; Brandsaeter 2002;
Chung 2003; Gow 2003; Larson 2005) describe the course of pa-
tients with severe paracetamol-induced fulminant hepatic failure
potentially eligible for liver transplantation.
Risk of bias in included studies
Randomised clinical trials
All ten included trials had unclear or insufficient control of bias.
Generation of the allocation sequence was described and was ad-
equate in three randomised trials (Douglas 1976; Hamlyn 1981;
O’Grady 1988), and allocation concealment was adequate in five
randomised trials (Gazzard 1974a; Gazzard 1975; Hamlyn 1981;
Keays 1991; Kerr 2005). All randomised trials were conducted un-
blinded except one (Keays 1991), which used placebo, but failed
to mask the aroma.
In one trial, the control group was given supportive treatment
in a different hospital, which may seriously affect the value of
this comparison group and questions how the randomisation was
carried out (Underhill 1990).
Quasi-randomised studies
One study (Burkhart 1995) used odd/even months at hospitalisa-
tion to allocate patients to different interventions.
Observational studies
Ten observational studies (Smith 1978; Smilkstein 1988; Parker
1990; O’Grady 1991; Smilkstein 1991; Spiller 1994; Schiodt
1996; Buckley 1999a; Buckley 1999b; Montoya-Cabrera 1999)
were prospective. Seven observational studies (Crome 1976;
Prescott 1976; Silk 1978; Prescott 1979; Vale 1981; Kirk 1991;
Higgens 1996) were likely to be retrospective. Fourteen observa-
tional studies (Amitai 1987; Harrison 1990; Bond 1993; Mutimer
1994; Anand 1997; Bernal 1998; Gee 1998; Shakil 2000; Woo
2000; Brandsaeter 2002; Chung 2003; Gow 2003; Ayonrinde
2005; Larson 2005) were clearly retrospective.
Randomised trials in human volunteers
In all 16 trials the allocation concealment and the generation of
allocation sequence was not described. None of the trials was con-
ducted blinded.
Effects of interventions
5Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The few included randomised trials differed substantially in inclu-
sion criteria, interventions, and outcome measures. Therefore it
was only possible to perform one meta-analysis that had addressed
our outcome measures. Due to the amount of data from non-ran-
domised trials we have summarised the results under the heading
’Exploratory analyses of quasi-randomised studies, observational
studies, and randomised trials including human volunteers’. These
data should be interpreted with caution due to the increased risk
of bias.
Randomised clinical trials
Activated charcoal, gastric lavage and ipecacuanha
One trial (n = 60) found that activated charcoal was significantly
more effective in lowering the plasma paracetamol level than gas-
tric lavage (P = 0.013), ipecacuanha (P = 0.027), or supportive
treatment if given within four hours after ingestion (Underhill
1990). There was no significant difference (P = 0.081) between
gastric lavage and ipecacuanha, but gastric lavage and ipecacuanha
were more effective than supportive treatment.
Charcoal haemoperfusion
One trial (n = 16) found no clinically significant benefit of treat-
ment with charcoal haemoperfusion (Gazzard 1974a). The mean
cumulative amount of paracetamol removed was 1.4 g. One pa-
tient allocated to the haemoperfusion group died after ingesting
135 grams of paracetamol.
One trial found no significant difference in survival between 10
versus 5 hours of haemoperfusion in 53 patients with fulminant
hepatic failure (O’Grady 1988). Further, O’Grady et al found no
significant difference in survival between 10 hours of haemoper-
fusion versus no haemoperfusion in 32 patients with fulminant
hepatic failure and encephalopathy grade 4.
Cysteamine, methionine, and dimercaprol
Compared to no intervention, cysteamine had no significant effect
on mortality (Peto OR 0.53, 95% CI 0.05 to 5.22, two trials with
65 patients), but significantly decreased the risk of developing
hepatotoxicity (OR 0.17, 95% CI 0.06 to 0.53, two trials with 65
patients).
One trial (n = 40) found no significant difference between cys-
teamine, methionine, and no intervention in mortality (only one
patient died in the ’no intervention’ group) (Hamlyn 1981). Com-
pared to ’no intervention’, methionine significantly reduced the
number of patients with hepatotoxicity. No significant differ-
ence in hepatotoxicity was observed between methionine and cys-
teamine.
One trial (n = 52) found no significant difference between cys-
teamine and dimercaprol in mortality or hepatotoxicity (Hughes
1977). One patient receiving dimercaprol died.
All trials reported that most patients given cysteamine had nausea
and vomited during the therapy. Some patients also had severe
headaches, one had transient truncal rash, and one developed se-
vere malaise (Hamlyn 1981). One trial reported that 4/13 patients
given oral methionine needed additional metoclopramide to pre-
vent vomiting (Hamlyn 1981). Dimercaprol given as a deep in-
tramuscular injection was painful in all patients and 9/26 patients
developed severe abdominal pain (Hughes 1977).
N-acetylcysteine
One trial (n = 180) found no significant difference of initial in-
travenously dose of N-acetylcysteine over 60 min compared to 15
min on mortality (no deaths occurred) or hepatotoxicity (RR 0.75;
95% CI 0.22 to 2.56) (Kerr 2005). The 15 min infusion rate did
not significantly increase the risk of a specific adverse events (eg,
anaphylactoid reactions, gastrointestinal disorders, etc.) or drug-
related adverse events within two hours (RR 1.17; 95% CI 0.63
to 2.17), but significantly increased the number of patients with
occurrence of adverse events (RR 1.98; 95% CI 1.04 to 3.72).
One trial (n = 50) found that intravenous N-acetylcysteine com-
pared with placebo for paracetamol-induced fulminant hepatic
failure significantly reduced mortality (RR 0.65; 95% CI 0.43 to
0.99) (Keays 1991). No adverse events to N-acetylcysteine were
reported.
Other interventions
Two trials assessed heparin (Gazzard 1974) and fresh frozen plasma
therapy (Gazzard 1975) for patients with paracetamol overdose
without any finding of any significant clinical benefits.
Exploratory analyses of quasi-randomised studies
Cimetidine
One study (n = 107) found no significant effect of adding cime-
tidine to N-acetylcysteine on mortality (zero in both groups) and
hepatotoxicity (Burkhart 1995).
Exploratory analyses of observational studies
Activated charcoal
One study (n = 330) found that activated charcoal within 24 hours
significantly reduced the number of patients with paracetamol
concentration above the probable risk-line (Buckley 1999a). No
significant difference was observed in coma incidence and length
of hospital stay. Patients not receiving activated charcoal had a
significant longer time to presentation after ingestion. Subgroup
analyses indicate that activated charcoal is only beneficial if ad-
ministered within two hours.
One study (n = 122) found that activated charcoal within 16
hours significantly reduced the number of patients having a plasma
paracetamol concentration above the possible risk-line (Spiller
1994).
One study with 123 children found that activated charcoal within
two hours significantly reduced plasma paracetamol level (Kirk
1991).
On study with 14 children found that adding activated charcoal
to N-acetylcysteine significantly increased the half-life elimination
of paracetamol (Montoya-Cabrera 1999).
Ipecacuanha
One study with 455 children found that ipecacuanha significantly
reduced paracetamol concentration if vomiting occurred before 90
minutes. There was no significant reduction when ipecacuanha-
induced emesis occurred later than 90 minutes (Bond 1993).
6Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

One study with 123 children found that ipecacuanha within
one hour significantly reduced plasma paracetamol level (Kirk
1991). No significant difference on plasma paracetamol between
ipecacuanha and activated charcoal within two hours was ob-
served.
One study with 50 children found that ipecacuanha administered
early (at home) compared to late (at the hospital) decreased parac-
etamol concentration (Amitai 1987).
Gastric lavage
One study (n = 253) found that adding gastric lavage to activated
charcoal within 24 hours did not significantly reduce the number
of patients with paracetamol concentration above the possible risk
line or length of hospital stay (Buckley 1999a).
Haemoperfusion
One study (n = 79) found no significant difference on mortality
between charcoal haemoperfusion versus haemodialysis or versus
supportive therapy (Silk 1978).
One study found that charcoal haemoperfusion given within 42
hours compared to later than 42 hours after a paracetamol overdose
significantly reduced mortality (Higgens 1996).
Antidotes
We have presented the pooled results from all the studies (using
any of risk-line) (Table 1; Table 2; Table 3). We found that 21/107
(19%) on cysteamine, 31/197 (16%) on methionine, 418/2315
(18%) on N-acetylcysteine, and 52/90 (58%) given no interven-
tion developed hepatotoxicity. If any antidote was given within 10
hours, only 76/1153 (7%) developed hepatotoxicity compared to
392/1435 (27%) if antidotes were given later than 10 hours. A
total of 306/1614 (19%) given N-acetylcysteine orally developed
hepatotoxicity compared to 80/637 (13%) given N-acetylcysteine
intravenously. A total of 34/226 (15%) given N-acetylcysteine 980
mg/kg intravenously for 48 hours compared to 50/458 (11%) N-
acetylcysteine 300 mg/kg intravenously for 24 hours developed
hepatotoxicity. Pooling studies only using the 200 risk-line (prob-
able risk) did not change the above results significantly.
Table 1. Antidotes for paracetamol overdose
Cysteamine Methionine Dimercaprol N-acetylscysteine Supportive treatment
Treatment delay: 0 h
to 10 h
Mortality 0/97 (0%) 0/143 (0%) 1/26 (4%) 0/949 (0%) No data
Hepatotoxicity 4/61 (7%) 13/143 (9%) No data 58/949 (6%) No data
7Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
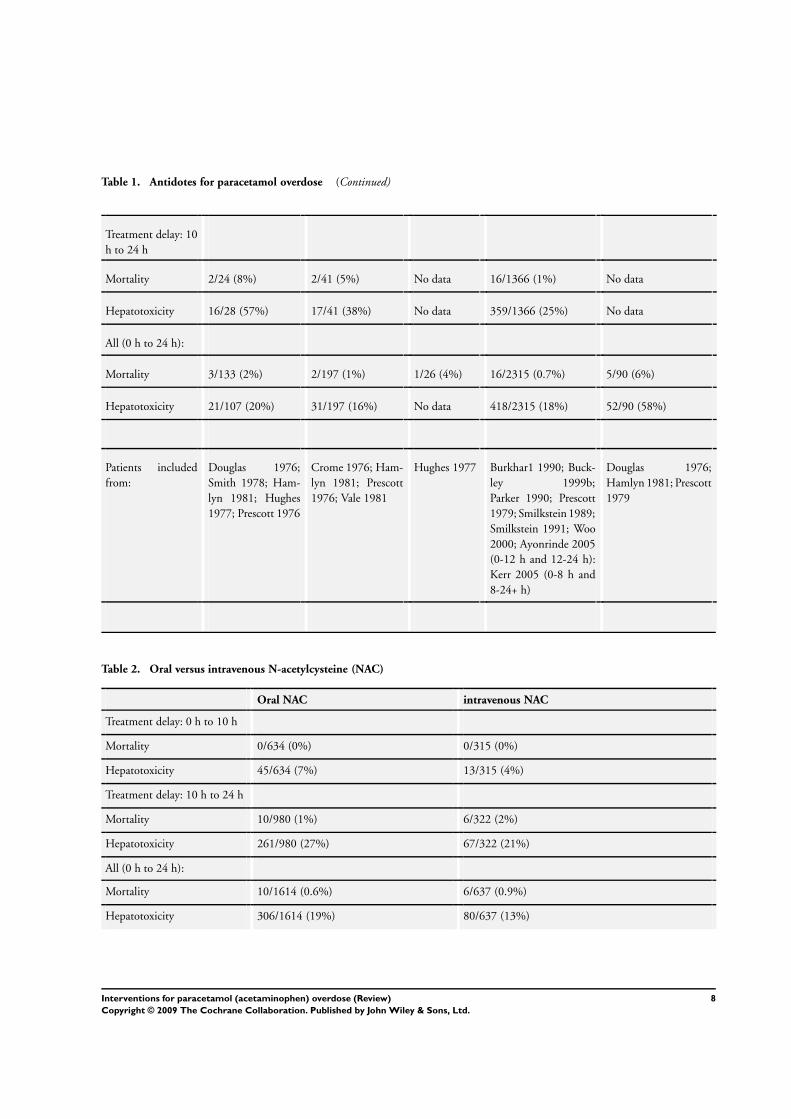
Table 1. Antidotes for paracetamol overdose (Continued)
Treatment delay: 10
h to 24 h
Mortality 2/24 (8%) 2/41 (5%) No data 16/1366 (1%) No data
Hepatotoxicity 16/28 (57%) 17/41 (38%) No data 359/1366 (25%) No data
All (0 h to 24 h):
Mortality 3/133 (2%) 2/197 (1%) 1/26 (4%) 16/2315 (0.7%) 5/90 (6%)
Hepatotoxicity 21/107 (20%) 31/197 (16%) No data 418/2315 (18%) 52/90 (58%)
Patients included
from:
Douglas 1976;
Smith 1978; Ham-
lyn 1981; Hughes
1977; Prescott 1976
Crome 1976; Ham-
lyn 1981; Prescott
1976; Vale 1981
Hughes 1977 Burkhar1 1990; Buck-
ley 1999b;
Parker 1990; Prescott
1979; Smilkstein 1989;
Smilkstein 1991; Woo
2000; Ayonrinde 2005
(0-12 h and 12-24 h):
Kerr 2005 (0-8 h and
8-24+ h)
Douglas 1976;
Hamlyn 1981; Prescott
1979
Table 2. Oral versus intravenous N-acetylcysteine (NAC)
Oral NAC intravenous NAC
Treatment delay: 0 h to 10 h
Mortality 0/634 (0%) 0/315 (0%)
Hepatotoxicity 45/634 (7%) 13/315 (4%)
Treatment delay: 10 h to 24 h
Mortality 10/980 (1%) 6/322 (2%)
Hepatotoxicity 261/980 (27%) 67/322 (21%)
All (0 h to 24 h):
Mortality 10/1614 (0.6%) 6/637 (0.9%)
Hepatotoxicity 306/1614 (19%) 80/637 (13%)
8Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
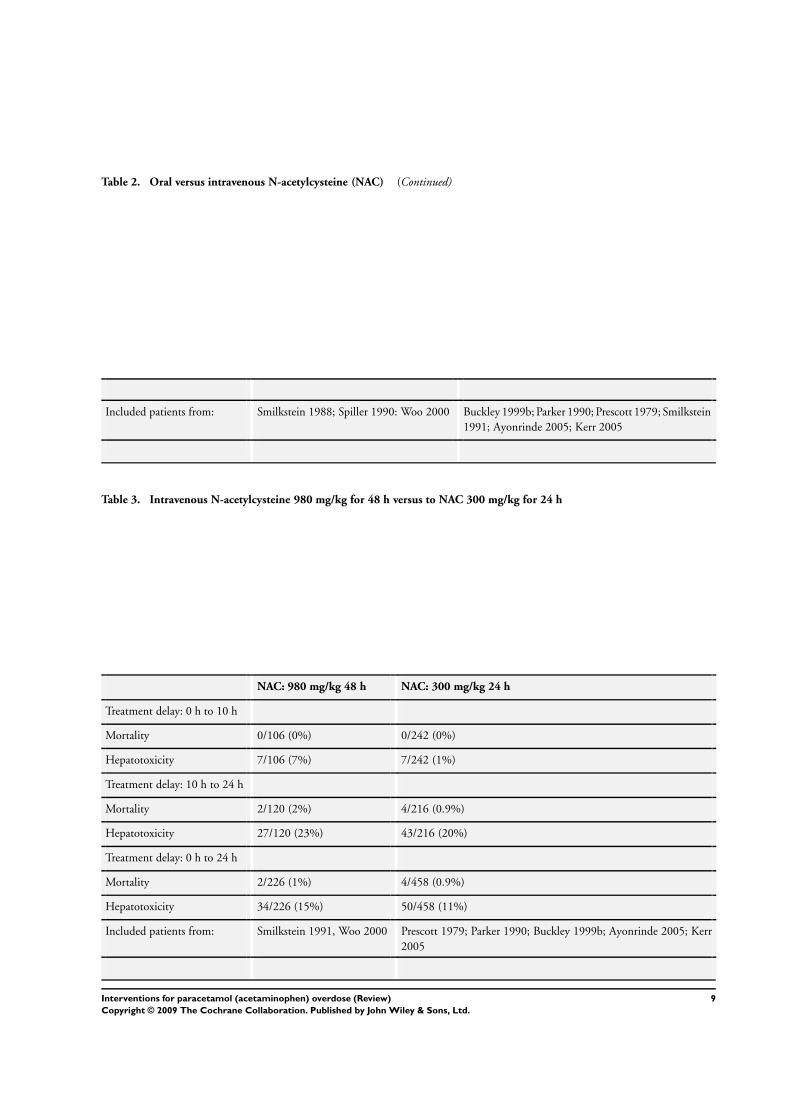
Table 2. Oral versus intravenous N-acetylcysteine (NAC) (Continued)
Included patients from: Smilkstein 1988; Spiller 1990: Woo 2000 Buckley 1999b; Parker 1990; Prescott 1979; Smilkstein
1991; Ayonrinde 2005; Kerr 2005
Table 3. Intravenous N-acetylcysteine 980 mg/kg for 48 h versus to NAC 300 mg/kg for 24 h
NAC: 980 mg/kg 48 h NAC: 300 mg/kg 24 h
Treatment delay: 0 h to 10 h
Mortality 0/106 (0%) 0/242 (0%)
Hepatotoxicity 7/106 (7%) 7/242 (1%)
Treatment delay: 10 h to 24 h
Mortality 2/120 (2%) 4/216 (0.9%)
Hepatotoxicity 27/120 (23%) 43/216 (20%)
Treatment delay: 0 h to 24 h
Mortality 2/226 (1%) 4/458 (0.9%)
Hepatotoxicity 34/226 (15%) 50/458 (11%)
Included patients from: Smilkstein 1991, Woo 2000 Prescott 1979; Parker 1990; Buckley 1999b; Ayonrinde 2005; Kerr
2005
9Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

One study (n = 98) in patients with paracetamol-induced fulmi-
nant hepatic failure found that N-acetylcysteine compared to no
intervention reduced mortality and the risk of coma significantly
(Harrison 1990).
Liver transplantation
Ten studies compared mortality among patients who had liver
transplantation to similar patients who did not. All studies used
almost the same criteria (Kings Hospital (O’Grady 1991)) for list-
ing patients for liver transplantation. The pooled results (Table 4)
show that 19/67 (28%) patients with transplantation and 121/180
(67%) patients without transplantation died.
Exploratory analyses of randomised trials including human
volunteers ingesting 1 g to 5 g of paracetamol
Activated charcoal
All trials, except one, found that activated charcoal given immedi-
ately, 30 min, or 60 min after a paracetamol ingestion, significantly
reduced the absorption. Two trials (Rose 1991; Christophersen
2002) found that activated charcoal given 120 min after ingestion
reduced absorption, but two trials (Yeates 2000; Green 2001) did
not support these findings (Table 5). One trial found activated
charcoal superior to ipecacuanha (Neuvonen 1983), and one study
found no significant difference (McNamara 1989).
Table 4. Liver transplantation for fulminant hepatic failure
Transplantation Supportive treatment Transpl. criteria Reference
2/6 (33%) mortality 7/8 (88%) mortality Kings College Hospital (KCH) and listed
for transplantation
O’Grady 1991
3/10 (30%) 6/7 (86%) Probably KCH and listed for transplan-
tation
Mutimer 1994
no data 6/10 (60%) KCH Schiodt 1996
no data 24/31 (77%) pH<7.3 Anand 1997
11/44 (25%) 20/24 (83%) KCH and listed for transplantation Bernal 1998
no data 10/14 (71%) KCH Shakil 2000
no data 16/32 (50%) KCH and listed for transplantation Brandsaeter 2002
10Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
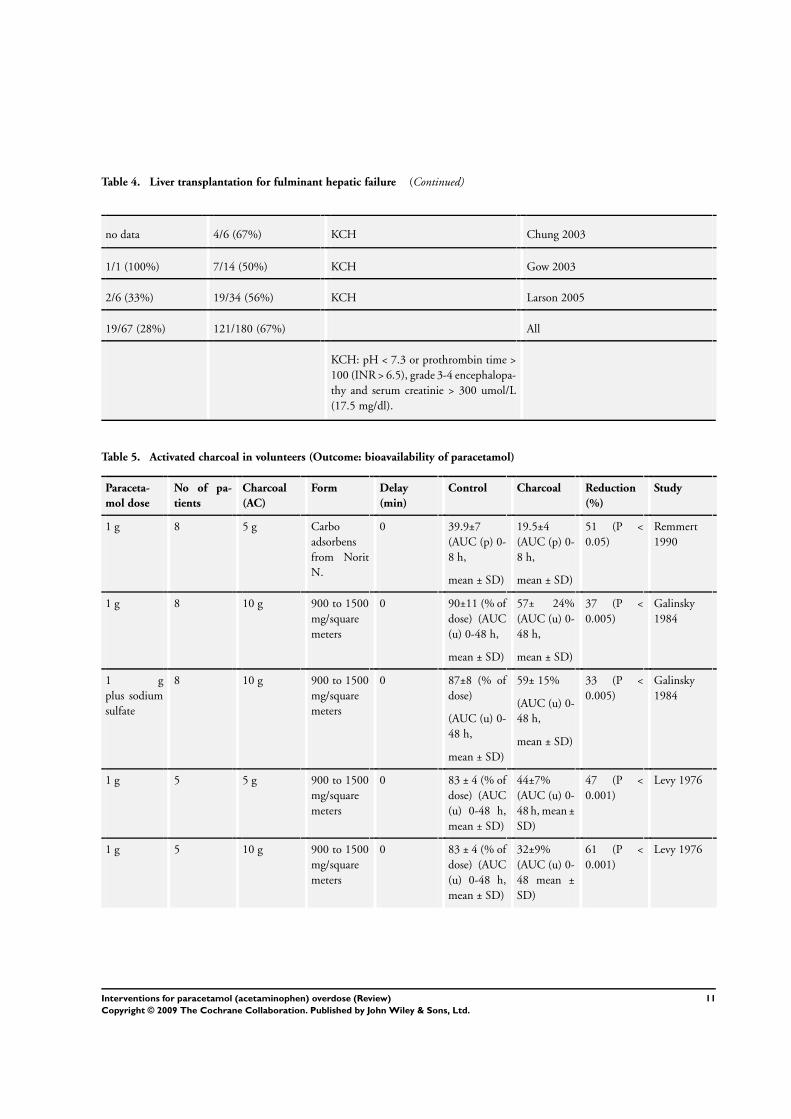
Table 4. Liver transplantation for fulminant hepatic failure (Continued)
no data 4/6 (67%) KCH Chung 2003
1/1 (100%) 7/14 (50%) KCH Gow 2003
2/6 (33%) 19/34 (56%) KCH Larson 2005
19/67 (28%) 121/180 (67%) All
KCH: pH < 7.3 or prothrombin time >
100 (INR > 6.5), grade 3-4 encephalopa-
thy and serum creatinie > 300 umol/L
(17.5 mg/dl).
Table 5. Activated charcoal in volunteers (Outcome: bioavailability of paracetamol)
Paraceta-
mol dose
No of pa-
tients
Charcoal
(AC)
Form Delay
(min)
Control Charcoal Reduction
(%)
Study
1 g 8 5 g Carbo
adsorbens
from Norit
N.
0 39.9±7
(AUC (p) 0-
8 h,
mean ± SD)
19.5±4
(AUC (p) 0-
8 h,
mean ± SD)
51 (P <
0.05)
Remmert
1990
1 g 8 10 g 900 to 1500
mg/square
meters
0 90±11 (% of
dose) (AUC
(u) 0-48 h,
mean ± SD)
57± 24%
(AUC (u) 0-
48 h,
mean ± SD)
37 (P <
0.005)
Galinsky
1984
1 g
plus sodium
sulfate
8 10 g 900 to 1500
mg/square
meters
0 87±8 (% of
dose)
(AUC (u) 0-
48 h,
mean ± SD)
59± 15%
(AUC (u) 0-
48 h,
mean ± SD)
33 (P <
0.005)
Galinsky
1984
1 g 5 5 g 900 to 1500
mg/square
meters
0 83 ± 4 (% of
dose) (AUC
(u) 0-48 h,
mean ± SD)
44±7%
(AUC (u) 0-
48 h, mean ±
SD)
47 (P <
0.001)
Levy 1976
1 g 5 10 g 900 to 1500
mg/square
meters
0 83 ± 4 (% of
dose) (AUC
(u) 0-48 h,
mean ± SD)
32±9%
(AUC (u) 0-
48 mean ±
SD)
61 (P <
0.001)
Levy 1976
11Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 5. Activated charcoal in volunteers (Outcome: bioavailability of paracetamol) (Continued)
5.6 g (80
mg/kg)
8 70 g (1g /kg)
plus cola
Char-
coAid 2000:
2000square
meters/g
0 298±83
mg*h/L
(AUC (u) 0-
6 h, mean ±
SD)
81±72
mg*h/L
(AUC (p) 0-
6 h, mean ±
SD)
73 (P <0.05) Rangan
2001
5.6 g (80
mg/kg)
8 70 g (1g /kg) Char-
coAid 2000:
2000square
meters/g
0 298±83
mg*h/L
(AUC (u) 0-
6 h, mean ±
SD)
77±85
mg*h/L
(AUC (p) 0-
6 h, mean ±
SD)
74 (P <0.05) Rangan
2001
1 g 6 50 g 1600 to
2000
mg/square
meters
5 100%
(AUC (p) 0-
24 h)
15% (range
1-30%)
85 (P <
0.01)
Neuvonen
1983
5 g 10 30g Super-
char: 3.150
square me-
ters/g
15 81±6%
(AUC (u) 0-
24 h, mean ±
SD)
42±10.2% 48 (P <
0.05)
Rose 1991
5 g 10 30 g Super-
char: 3.150
square me-
ters/g
30 81±6%
(AUC (u) 0-
24 h, mean ±
SD)
45±8% 44.1(P <
0.05)
Rose 1991
1 g 6 10 g 900 to 1500
mg/square
meters
30 100%
(AUC (u)0-
24 h)
40% (range
14-90%)
60 (P <
0.05)
Neuvonen
1983
1 g 5 10 g 900 to 1500
mg/square
meters
30 83 ± 4%
(AUC (u)0-
48 h, mean ±
SD)
57±7% 31.1 (P <
0.005)
Levy 1976
3 g 8 50 g Med Corp
Acta-Char:
950 square
meters/g
60 123
mg*h/ml
(AUC (p)0-
8 h) (A)
87 mg*h/ml
(AUC (p)0-
8 h) (A)
29 (A) (P <
0.05)
McNamara
1988
3.6 g (50
mg/kg)
12 50 g Carbomix:
2000 square
meters/g
60 190 mg*h/L
(95%
CI 119-235)
(AUC (p)0-
48 h)
539 mg*h/L
(95% CI
19.7-135)
66 (P <
0.05)
Christo-
phersen
2002
12Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 5. Activated charcoal in volunteers (Outcome: bioavailability of paracetamol) (Continued)
3 g 10 50 g Carbomix:
2000 square
meters/g
60 182 mg*h/L
(95% CI
143 to 221)
(AUC (b) 0-
48 h) SD:
19.5
92 mg*h/L
(95% CI 60
to 125) S.D:
16.3
43 (P <
0.05)
Yeates 2000
3 g 10 50 g 900 to1500
mg/square
me-
ters with ad-
ditional sor-
bitol
60 119
mg*h/ml
(AUC (p)0-
8 h) (A)
89 mg*h/ml
(A)
26 (A) (P <
0.05)
McNamara
1989
4 g 10 50g Charcodote:
?
60 221±122
mg*h/L
(AUC (p)0-
8 h)
154±71mg*h/L
67 (P <
0.001)
Green 2001
4 g 10 50g Charcodote:
?
60 258±122
mg*h/L
(AUC (p)0-
48 h)
206±120
mg*h/L
20 (P <
0.10)
Green 2004
3 g 10 50 g Carbomix:
2000 square
meters/g
120 182 mg*h/L
(95% CI
143 to 221)
(AUC (p) 0-
48 h) SD:
19.5
164 mg*h/L
(95%
CI 122 to
2-205) S.D:
20.75
1 (P > 0.05) Yeates 2000
3.6 g (50
mg/kg)
12 50 g Carbomix:
2000 square
meters/g
120 190 mg*h/L
(95%
CI 119-235)
(AUC (p)0-
48 h)
152 mg*h/L
(95% CI
53.8-116.2)
23 (P <
0.05)
Christo-
phersen
2002
4 g 10 50g Charcodote:
?
120 221±122
mg*h/L
(AUC (p)0-
8 h)
206±67
mg/l*h
15 (P >
0.05)
Green 2001
5 g 10 30 g Super-
char: 3.150
square me-
ters/g
120 81±6%
(AUC (u) 0-
24 h, mean ±
SD)
54±8% 33 (P <
0.05)
Rose 1991
13Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
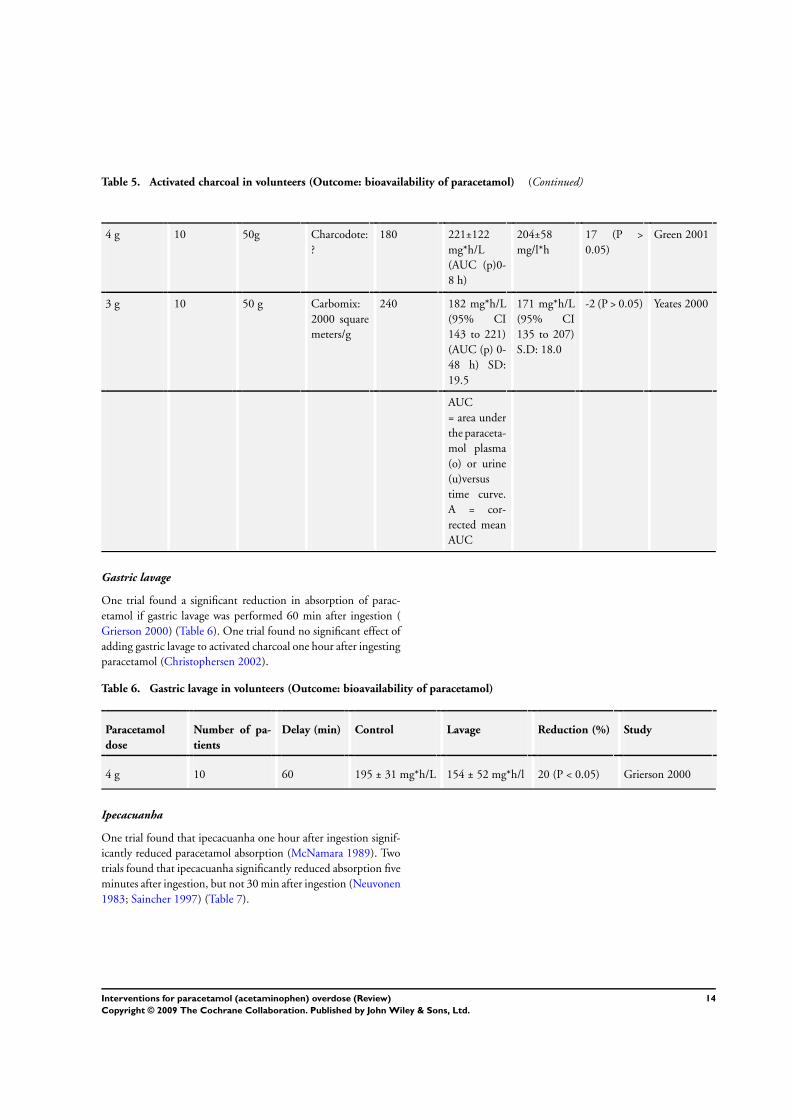
Table 5. Activated charcoal in volunteers (Outcome: bioavailability of paracetamol) (Continued)
4 g 10 50g Charcodote:
?
180 221±122
mg*h/L
(AUC (p)0-
8 h)
204±58
mg/l*h
17 (P >
0.05)
Green 2001
3 g 10 50 g Carbomix:
2000 square
meters/g
240 182 mg*h/L
(95% CI
143 to 221)
(AUC (p) 0-
48 h) SD:
19.5
171 mg*h/L
(95% CI
135 to 207)
S.D: 18.0
-2 (P > 0.05) Yeates 2000
AUC
= area under
the paraceta-
mol plasma
(o) or urine
(u)versus
time curve.
A = cor-
rected mean
AUC
Gastric lavage
One trial found a significant reduction in absorption of parac-
etamol if gastric lavage was performed 60 min after ingestion (
Grierson 2000) (Table 6). One trial found no significant effect of
adding gastric lavage to activated charcoal one hour after ingesting
paracetamol (Christophersen 2002).
Table 6. Gastric lavage in volunteers (Outcome: bioavailability of paracetamol)
Paracetamol
dose
Number of pa-
tients
Delay (min) Control Lavage Reduction (%) Study
4 g 10 60 195 ± 31 mg*h/L 154 ± 52 mg*h/l 20 (P < 0.05) Grierson 2000
Ipecacuanha
One trial found that ipecacuanha one hour after ingestion signif-
icantly reduced paracetamol absorption (McNamara 1989). Two
trials found that ipecacuanha significantly reduced absorption five
minutes after ingestion, but not 30 min after ingestion (Neuvonen
1983; Saincher 1997) (Table 7).
14Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 7. Ipecac in human volunteers (Outcome: bioavailability of paracetamol)
Paracetamol
dose
Number of
patients
Form Delay (min) Control Ipecacuanha Reduction (%) Study
3,9 g 10 30 mL 5 206 mg*h/L ±
48 (AUC (p)0-
6h, mean ± SD)
67 mg*h/L ± 37
(AUC (p)0-6h,
mean ± SD)
67 (P < 0.05) Saincher 1997
1 g 6 20 mL 5 55 mg*h/L 18 mg*h/L 65 (P < 0.01) Neuvonen 1983
1 g 6 20 ml 30 55 mg*h/L 54 mg*h/L 2 (P > 0.05) Neuvonen 1983
3,9 10 30 mL 30 206 mg*h/L ±
48 (AUC (p)0-
6h, mean ± SD)
183 mg*h/L ±
78 (AUC (p)0-
6h, mean ± SD)
11 (P > 0.05) Saincher 1997
3,9 10 30 mL 60 206 mg*h/L ±
48 (AUC (p)0-
6h, mean ± SD)
162 mg*h/L ±
47 (AUC (p)0-
6h, mean ± SD)
21 (P > 0.05) Saincher 1997
3 g 10 30 mL 60 120 (corrected
mean area under
the curve)
94 21 (P < 0.05) McNamara
1989
Whole bowel irrigation
One trial found that whole bowel irrigation (30 min after inges-
tion) had no significant reduction in absorption of paracetamol (
Ly 2004) (see Table 8). One trial found that whole bowel irrigation
(30 min after ingestion) had a significant reduction in absorption
of paracetamol if the ingested paracetamol dose was 4 g, but not
if the dose was 2 g (Hassig 1993).
Table 8. Whole bowel irrigation in volunteers (Outcome: bioavailability of paracetamol)
Dose Number of
patients
Type Delay (min) Control Bowel irriga-
tion
Reduction % Study
5 g (75
mg/kg)
10 ? 30 323 (95% CI
237-409)
(AUC (p) 0-6
h)
286 (95% CI
219-352)
(AUC (p) 0-6
h)
12 (P > 0.05) Ly 2004
Cimetidine
One trial found no statistical beneficial effect on plasma paraceta-
mol when ingesting cimetidine together with 750 mg paracetamol
(Chen 1985).
D I S C U S S I O N
Gastric lavage, activated charcoal, and ipecacuanha are able to re-
duce the absorption of paracetamol if given shortly after ingestion.
Activated charcoal seems to be the best choice to reduce parac-
etamol absorption but is less likely to be effective if given later
than two hours postingestion. N-acetylcysteine seems preferable to
15Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

placebo/supportive treatment, dimercaprol, and cysteamine, but
the superiority of N-acetylcysteine’s to methionine is unproven.
No N-acetylcysteine regimen has been shown to be more effective
than any other. Survival among patients with paracetamol-induced
fulminant hepatic failure seems higher if treated with N-acetyl-
cysteine; short-term survival is improved by liver transplantation
in those meeting transplant criteria, but long-term outcome data
are not available. There is no strong evidence supporting other
interventions for paracetamol overdose.
Our results highlight a lack of randomised trials on interventions
for paracetamol overdose, which is surprising as it is a very com-
mon type of drug poisoning. The included randomised trials were
small, the methodological quality was low, and most trials assessed
interventions not used today. Eg, no randomised trial has inves-
tigated the effect of the recommended antidote N-acetylcysteine
versus other antidotes or no intervention. More research to weight
up the benefits and risks of all interventions for paracetamol over-
dose are needed to confirm the established practice.
We included a several observational studies in explanatory analy-
ses, which raises some problems. There is no recommended search
strategy to identify observational studies within the Cochrane Col-
laboration. We tried to develop an extensive search strategy, but
we may not have been able to identify all relevant studies. Second,
there is no consensus within the Cochrane Collaboration on how
to assess the quality of observational studies. Furthermore, most
studies assessed surrogate outcomes indicating liver damage and
only few studies assessed important clinical outcomes. Accord-
ingly, the results of this review should be interpreted with caution.
Prevention of absorption
Only one randomised trial found activated charcoal to be more
effective than gastric lavage, ipecacuanha, or no intervention in
preventing the absorption of paracetamol (Underhill 1990). How-
ever, the number of patients included was small and the time inter-
val between ingestion and intervention in the different groups was
not clearly reported. The control group was given supportive treat-
ment in a different hospital which questions how the randomisa-
tion was carried out. Furthermore, the supportive treatment was
stopped early due to ethical reasons that may seriously affect the
value of the comparison group. Therefore, the value of this trial is
limited.
All the observational studies and studies in volunteers found that
activated charcoal, gastric lavage, or ipecacuanha, shortly after in-
gestion, are able to reduce the absorption of paracetamol. Whether
this translates into clinical benefits is not clear. Two studies sug-
gested that activated charcoal reduces the need for N-acetylcysteine
treatment (Spiller 1994; Buckley 1999a). Some results indicate
that activated charcoal may prevent absorption up to two hours
postingestion (Rose 1991; Buckley 1999a), but it may vary, eg,
depending on the dose of paracetamol, the gastric environment,
and additionally taken drugs. Through passive diffusion, activated
charcoal may also absorb paracetamol from the bloodstream which
may favour protracted use of activated charcoal compared with
gastric lavage or ipecacuanha (Rose 1991; Spiller 1994). Two stud-
ies found no benefits of adding gastric lavage to activated charcoal
(Buckley 1999a; Christophersen 2002).
The risk of adverse events has barely been reported. One well-
known complication from all the three interventions is aspiration
pneumonia (Liisanantti 2003). We identified one randomised trial
(Cooper 2005), which reported no significant increase of adverse
events in patients receiving activated charcoal for any drug over-
dose. Position statements on drug poisonings indicate that serious
adverse events seem to be fewer in activated charcoal compared
to ipecacuanha and gastric lavage (Chyka 2005; Krenzelok 2004;
Vale 2004). Accordingly, weak evidence indicates that activated
charcoal is currently the best choice to prevent absorption of parac-
etamol.
Haemoperfusion
Haemoperfusion has only been studied superficially and we found
no evidence to support or refute haemoperfusion for paracetamol
overdose and fulminant hepatic failure. Given the availability of
cheap and more effective alternatives, any plausible benefits of
haemoperfusion are unlikely to be justifiable on economic or risk-
benefit grounds.
Antidotes
Cysteamine, methionine, and dimercaprol
Two randomised trials found hepatoprotective effect of methion-
ine and cysteamine compared to no intervention (Douglas 1976;
Hamlyn 1981). No significant difference was observed between
the two antidotes, but a third trial found cysteamine superior to
dimercaprol (Hughes 1977). Douglas et al (Douglas 1976) had a
control group with a significant higher paracetamol concentration
before treatment which may limit the value of this comparison
group. Further, it must also be noted that data from four patients
were used in two trials (Douglas 1976; Hamlyn 1981). One ob-
servational study supports the beneficial effects of methionine and
cysteamine on hepatotoxicity (Prescott 1976). Overall cysteamine
therapy was associated with a high rate of nausea and vomiting.
Few adverse events were noticed in patients given methionine and
dimercaprol. Accordingly, methionine probably seems to be the
best choice of antidote among the three.
N-acetylcysteine
One randomised trial found that N-acetylcysteine increases sur-
vival in patient with paracetamol-induced fulminant hepatic fail-
ure (Keays 1991). However, no randomised trials have assessed the
effect of N-acetylcysteine in the acute treatment of paracetamol
overdose. One observational study found that N-acetylcysteine
16Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

compared to supportive treatment decreased the risk of hepato-
toxicity (Prescott 1979). Compared with cysteamine or methio-
nine there was no statistical difference, but these antidotes were
considered to have more adverse events. The study was small (n
= 200) and the comparison antidote and supportive groups were
historical control groups treated three and ten years earlier, respec-
tively. Accordingly, the risk of biased findings in this study is sub-
stantial (Sacks 1982; Deeks 2003). However, since this study was
published, N-acetylcysteine has been recommended as the drug
of choice. Historical data show that the overall mortality rate has
dropped from 3% (all poisonings (Clark 1973)) or 5 % (all above
the probable risk-line (Prescott 1979)) to 0.7% (Table 1) after the
introduction of N-acetylcysteine.
Pooling (Table 1) the patients from all the studies indicates that
N-acetylcysteine should be preferred over supportive treatment
and that early treatment (0 h to 10 h) is preferable compared to
late treatment (10 h to 24 h) irrespective the type of antidote.
However, the risk-line used for treating patients in all studies was
not uniform.
No randomised trials have demonstrated the optimal way of ad-
ministration and most beneficial dose of N-acetylcysteine. Pool-
ing (Table 2; Table 3) the results from the all the studies indi-
cates no clear difference between oral and intravenous N-acetyl-
cysteine administration or different intravenous protocols. How-
ever, one randomised trials found that slow initial infusion (60
minutes) of the 300 mg/kg intravenous protocol did not cause a
clinical important decrease in the number of adverse events. N-
acetylcysteine has never been compared to supportive treatment
in randomised trials or large observational studies. Therefore it
is difficult to quantify the risk of adverse events. Intravenous N-
acetylcysteine may induce anaphylactoid reactions and delivered
doses of N-acetylcysteine often vary from the intended which may
lead to inadvertent overdose and death (Mant 1984; Appelboam
2002; Bailey 2004; Ferner 2004). Oral N-acetylcysteine adminis-
tration often results in rashes, nausea, vomiting, and abdominal
pain. Accordingly, intravenous N-acetylcysteine seems to be as-
sociated with fewer more severe adverse events compared to oral
N-acetylcysteine, which frequently is associated with less severe
adverse events.
Most recommendations advise to measure the plasma paraceta-
mol concentration. If the plasma paracetamol is above a chosen
risk-line, N-acetylcysteine is advocated. If it is not possible to ob-
tain a plasma paracetamol concentration, N-acetylcysteine treat-
ment should be given if a potentially toxic dose has been ingested
(150 mg/kg). Other recommendations advise to initiate treatment
based on reported dose and not wait for blood samples. However,
paracetamol concentrations correlates weakly with reported parac-
etamol dose (Thomas 1997).
Both the 200 risk-line and the 150 risk-line are used as a direc-
tion for continued N-acetylcysteine intervention. Many factors
like alcoholism, eating disorder, or use of enzyme-inducing agents
increase the risk of paracetamol hepatotoxicity, and these patient
groups may need a lower threshold for treatment. After treatment
liver biochemistry should be checked (Vale 1995). If these vari-
ables are normal and the patient is asymptomatic, then he/she may
be discharged. If the patient has developed or is at risk of develop-
ing fulminant hepatic failure, N-acetylcysteine treatment should
be continued until recovery. It should be noticed that N-acetylcys-
teine and/or paracetamol overdose itself without evidence of liver
injury may increase the international normalised ratio (INR), and
management decisions should be based on the entire liver bio-
chemistry (Whyte 2000; Schmidt 2002).
Liver transplantation
Pooling the results from ten observational studies with 247 pa-
tients, in which King’s College Hospital criteria for liver transplan-
tation were used, indicates that transplantation improves survival
(Table 4). Overall 28% (19/67) of the patients with transplanta-
tion and 67% (121/180) of the patients without transplantation
died, but long-term outcomes were not assessed. Furthermore, de-
spite fulfilling King’s Hospital criteria, a substantial difference in
mortality rates in patients without transplantation were identified.
This difference may be because some studies reported the out-
come of patients that fulfilled King’s Hospital criteria at admission
whereas other reported the outcome of patients that fulfilled these
criteria during hospital stay.
N-acetylcysteine administration improves survival in patients with
fulminant hepatic failure, but no study has demonstrated when it
is beneficial to switch from late N-acetylcysteine administration
to liver transplantation. It is, therefore, difficult to choose between
N-acetylcysteine treatment and the risk of delaying transplanta-
tion which increases the patients’ risk of developing multi-organ
failure. Furthermore, the decisions to proceed to transplantation
may be taken in the context of contraindication like alcohol or
drug abuse, other diseases, age, graft availability, other recipients,
and patient/relative compliance. The King’s Hospital criteria are
widely used to list patients for liver transplantation. These criteria
have some limitations, eg, in some studies 50% of the patients
fulfilling the criteria survived without transplantation. Future re-
search may identify criteria of higher sensitivity and specificity
(eg, APACHE II) in predicting patients mortality risks and need
for transplantation (Mitchell 1988; Larson 2005). Even in liver
transplanted patients we found that 28% had short-term mortal-
ity. Accordingly, randomised trials in selected patient groups seems
needed.
Children
Children who unintentionally ingest a paracetamol overdose rep-
resent a difficult group of patients. They are rarely able to tell how
much and when they have ingested the drug. Furthermore, the
17Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

applicability of the recommended treatment line in young chil-
dren has never been proven due to the paucity of data (Vale 1995).
Therefore, treatment of children should be carried out with great
caution and more research is needed.
A U T H O R S ’ C O N C L U S I O N SImplications for practice
Although the evidence for how to treat patients with paracetamol
overdose is weak, the following recommendations seem reasonable:
Activated charcoal, gastric lavage, and ipecacuanha are interven-
tions that seem able to reduce the absorption of paracetamol if
the patients are treated within one to two hours postingestion.
Whether this translates into clinical benefits is unclear. If the pa-
tient is compliant, activated charcoal seems the best choice.
N-acetylcysteine should be given promptly to patients with parac-
etamol overdose, but the selection criteria are not clear. A poten-
tially toxic dose could be based on ingested dose (150 mg/kg or
more) or plasma paracetamol concentration above a chosen risk-
line. Furthermore, N-acetylcysteine should be given to all patients
with abnormal liver biochemistry or fulminant hepatic failure af-
ter paracetamol overdose. No N-acetylcysteine treatment regime
(1330 mg/kg orally. (72 hours), 980 mg/kg intravenously (48
hours), or 300 mg/kg intravenously (24 hours)) has been shown
to be more effective than any other.
Liver transplantation reduces the short-term mortality in patients
selected according to Kings Hospital criteria. However, the short-
term mortality among transplanted patients is still around 28%
and the long-term survival is not known. Moreover, a substantial
proportion of patients listed for transplantation survive with con-
servative therapy. Furthermore, making a decision to proceed to
transplantation in patients who have attempted suicide is a diffi-
cult task which may limit this therapeutic option.
Implications for research
Patients with a paracetamol overdose need to be studied in large
multicentre randomised trials with adequate methodology and
with relevant clinical outcome measures. The substantial fall in
mortality rate from paracetamol overdose since the introduction
of N-acetylcysteine means that it is unlikely that it would be con-
sidered ethical to randomise to N-acetylcysteine versus no inter-
vention. This review has demonstrated a number of topics that
need assessment in randomised trials, eg, N-acetylcysteine admin-
istered intravenously versus orally; N-acetylcysteine in one dose
versus other doses; activated charcoal versus no decontamination
or other methods for reducing paracetamol absorption; long-term
outcome of N-acetylcysteine versus N-acetylcysteine plus liver
transplantation in patients with fulminant hepatic failure. Fur-
thermore, adverse events in relation to the different interventions
should be reported systematically. New trials should be registered
(http://www.icmje.org/clin_trialup.htm) and reported according
to the CONSORT guidelines (www.consort-statement.org).
A C K N O W L E D G E M E N T S
We are indebted to Dimitrinka Nikolova and Sarah Klingenberg
for their helpful assistance. We also want to express our gratitude
to the Contact Editor and peer reviewers as well as Ronald L Koretz
for many helpful comments.
R E F E R E N C E S
References to studies included in this review
Amitai 1987 {published data only}
Amitai Y, Mitchell AA, McGuigan MA, Lovejoy FH. Ipecac-induced
emesis and reduction of plasma concentrations of drugs following
accidental overdose in children. Pediatrics 1987;80(3):364–7.
Anand 1997 {published data only}
Anand AC, Nightingale P, Neuberger JM. Early indicators of prog-
nosis in fulminant hepatic failure: an assessment of the King’s cri-
teria. Journal of Hepatology 1997;26(1):62–8. [MEDLINE: PMID:
9148024]
Ayonrinde 2005 {published data only}
Ayonrinde OT, Phelps GJ, Hurley JC, Ayonrinde OA. Paracetamol
overdose and hepatotoxicity at a regional Australian hospital: a 4-year
experience. Internal medicine journal 2005;35(11):655–60. [MED-
LINE: PMID: 16248859]
Bernal 1998 {published data only}
Bernal W, Wendon J, Rela M, Heaton N, Williams R. Use and out-
come of liver transplantation in acetaminophen induced acute liver
failure. Hepatology 1998;27(4):1050–5.
Bond 1993 {published data only}
Gond GR, Requa RK, Krenzelok EP, Normann SA, Tendler JD, Mor-
ris CL, et al.Influence of time to emesis on the efficacy of decontam-
ination using acetaminophen as a marker in a pediatric population.
Annals of Emergency Medicine 1993;22:1403–7.
Brandsaeter 2002 {published data only}
Brandsaeter B, Hockerstedt K, Friman S, Ericzon BG, Kirkegaard P,
Isoniemi H, et al.Fulminant hepatic failure: outcome after listing for
highly urgent liver transplantation-12 years experience in the nordic
countries. Liver Transplantation 2002;8(11):1055–62.
Buckley 1999a {published data only}
Buckley NA, Whyte IM, O´ Connell DL, Dawson AH. Activated
charcoal reduces the need for N-acetylcysteine treatment after ac-
18Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

etaminophen (paracetamol) overdose. Journal of Toxicology. Clinical
Toxicology 1999;37(6):753–7.
Buckley 1999b {published data only}
Buckley NA, Whyte IM, O´ Connell DL, Dawson AH. Oral or in-
travenous N-acetylcysteine: Which is the treatment of choice for ac-
etaminophen (paracetamol) poisoning. Journal of Toxicology. Clini-
cal Toxicology 1999;37(6):757–67.
Burkhart 1995 {published data only}
Burkhart KK, Janco N, Kulig KW, Rumack BH. Cimetidine as ad-
junctive treatment for acetaminophen overdose. Human & Experi-
mental Toxicology 1995;14(3):299–304.
Chen 1985 {published data only}
Chen MM, Lee CS. Cimetidine - acetaminophen interactions in
humans. British Journal of Clinical Pharmacology 1985;25:227–9.
Christophersen 2002 {published data only}
Christophersen AB, Levin D, Hoegberg LC, Angelo HR, Kampmann
JP. Activated charcoal alone or after gastric lavage: a simulated large
paracetamol intoxication. British Journal of Clinical Pharmacology
2002;53(3):312–7. [MEDLINE: PMID: 11874395]
Chung 2003 {published data only}
Chung PY, Sitrin MD, Te HS. Serum phosphorus levels predict clini-
cal outcome in fulminant hepatic failure. Liver Transplantation 2003;
9(3):248–53. [MEDLINE: PMID: 12619021]
Crome 1976 {published data only}
Crome P, Vale JA, Volans GN, Widdop B. Oral methionine in the
treatment of severe paracetamol overdose. Lancet 1976;2:829–30.
Douglas 1976 {published data only}
Douglas AP, Hamlyn AN, James O. Controlled trial of cysteamine
in treatment of acute paracetamol poisoning. Lancet 1976;2:111–5.
James OA. A controlled trial of cysteamine in the treatment of acute
paracetamol poisoning. Journal of Internal Medecine Research 1976;
4:118–22.
Galinsky 1984 {published data only}
Galinsky RE, Levy G. Evaluation of activated charcoal-sodium sul-
fate combination for inhibition of acetaminophen absorbtion and re-
pletion of inorganic sulfate. Journal of Toxicology. Clinical Toxicology
1984;22:21–30.
Gazzard 1974 {published data only}
Gazzard BG, Clarc R, Borirakchanyevat V, Willians R. A controlled
trial of heparin threrapy in the coagulation defect of paracetamol
induced hepatic necroses. Gut 1974;15:89–93.
Gazzard 1974a {published data only}
Gazzard BG, Willson RA, Weston MJ, Thompson RPH, Williams R.
Charcoal haemoperfusion for paracetamol overdose. British Journal
of Clinical Pharmacology 1974;1:271–5.
Gazzard 1975 {published data only}
Gazzard PG, Henderson JM, Williams R. Early changes in coagula-
tion following a paracetamol overdose. Gut 1975;16:617–20.
Gow 2003 {published data only}
Gow PJ, Smallwood A, Angus P. Paracetamol overdose in a liver trans-
plantation centre: An 8 year experience. Journal of Gastroenterology
and Hepatology 1999;14(8):817–21.∗ Gow PJ, Sood S, Angus PW. Serum phosphate as a predictor of
outcome in acetaminophen-induced fulminant hepatic failure. Hep-
atology 2003;37(7):211–2.
Green 2001 {published data only}
Green R, Grierson R, Sitar DS, Tenenbein M. How long after drug in-
gestion is activated charcoal still effective?. Journal of Toxicology. Clin-
ical Toxicology 2001;39(6):601–5. [MEDLINE: PMID: 11762668]
Green 2004 {published data only}
Green R, Sitar DS, Tenenbein M. Effect of anticholinergic drugs
on the efficacy of activated charcoal. Journal of Toxicology. Clinical
Toxicology 2004;42:267–72.
Grierson 2000 {published data only}
Grierson R, Green R, Sitar DS, Tenenbein M. Gastric lavage for
liquid poisons. Annals of Emergency Medicine 2000;35(5):435–9.
Hamlyn 1981 {published data only}
Hamlyn AN, Lesna M, Record CO, Smith PA, Path FRC, Watson
AJ. Methionine and cysteamine in paracetamol overdose, prospective
controlled trial of early therapy. The Journal of International Medical
Research 1981;9:226–31.
Harrison 1990 {published data only}
Harrison PM, Keays R, Bray GP, Alexander GJ, Williams R. Im-
proved outcome of paracetamol-induced fulminant hepatic failure
by late administration of acetylcysteine. Lancet 1990;335:1572–3.
Hassig 1993 {published data only}
Hassig SR, Linscheer WG, Murthy UK, Miller C, Banerjee A,
Levine L, et al.Effects of PEG-electrolyte (Colyte) lavage on serum
acetaminophen concentrations. A model for treatment of ac-
etaminophen overdose. Digestive Diseases and Sciences 1993;38(8):
1395–401.
Higgens 1996 {published data only}
Higgins RM, Goldsmith DJA, MacDiarmid-Gordon A, Taberner D,
Venning MC, Ackrill P. Treating paracetamol overdose by charcoal
haemoperfusion and long-hours high flux dialysis. The Quarterly
Journal of Medicine 1996;89:297–306.
Hughes 1977 {published data only}
Huges RD, Gazzard BG, Hanid MA, Trewby PN, Murray-Lyon IM,
Davis M, et al.Controlled trial of cysteamine and dimercaprol after
paracetamol overdose. BMJ (Clinical Research Ed.) 1977;2:1395.
Keays 1991 {published data only}
Keays R, Harrison PM, Wendon JA, Forbes A, Gove C, Alexander
GJM, et al.Intravenous acetylcysteine in paracetamol induced fulmi-
nant hepatic failure. British Medical Journal 1991;303:1026–9.
Kerr 2005 {published data only}
Kerr F, Dawson A, Whyte IM, Buckley N, Murray L, Graudins A,
et al.The Australasian Clinical Toxicology Investigators Collabora-
tion randomized trial of different loading infusion rates of N-acetyl-
cysteine. Annals of Emergency Medicine 2005;45(4):402–8. [MED-
LINE: PMID: 15795719]
Kirk 1991 {published data only}
Kirk M, Peterson J, Kulig K. Acetaminophen overdose in children:
a comparison of ipecac versus activated charcoal versus no gastroin-
testinal decontamination (abstract). Annals of Emergency Medicine
1991;20:472–3.
Larson 2005 {published data only}
Larson AM, Polson J, Fontana RJ, Davern TJ, Lalani E, Hynan LS,
et al.Acetaminophen-induced acute liver failure: results of a United
States multicenter, prospective study. Hepatology 2005;42(6):1364–
72. [: PMID: 16317692]
19Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Levy 1976 {published data only}
Levy G, Houston B. Effect of activated charcoal on acetaminophen
absorption. Pediatrics 1976;58:432–5.
Ly 2004 {published data only}
Ly BT, Schneir AB, Clark RF. Effect of whole bowel irrigation on the
pharmacokinetics of an acetaminophen formulation and progression
of radiopaque markers through the gastrointestinal tract. Annals of
Emergency Medicine 2004;43(2):189–95. [: PMID: 14747807]
McNamara 1988 {published data only}
McNamara RM, Aaron CK, Gemborys M, Davidheiser S. Sorbitol
catharsis does not enhance efficacy if charcoal in a simulated ac-
etaminophen overdose. Annals of Emergency Medicine 1988;17(3):
243–6.
McNamara 1989 {published data only}
McNamara RM, Aaron CK, Gemborys M, Davidheiser S. Efficacy of
charcoal carthartic versus ipecac in reducing serum acetaminophen
in simulated overdose. Annals of Emergency Medicine 1989;18(9):
934–8.
Montoya-Cabrera 1999 {published data only}
Montoya-Cabrera MA, Escalante-Galindo P, Nava-Juaez A, Terroba-
Larios VM, Teran-Hernandez JA. Evaluation of the efficacy of N-
acetylcysteine administrated alone or in combination with activated
charcoal in the treatment of acetaminophen overdose [Evaluacion de
la eficacia de la N–acetilcisteina administrada sola o conbinada con
carbon activado en el tratamiento de la sobredosis por acetaminofen].
Gaceta Medica de Mexico 1999;135(3):239–43.
Mutimer 1994 {published data only}
Mutimer DJ, Ayres RCS, Neuberger JM, Davies MH, Holguin J,
Buckels JAC, et al.Serious paracetamol poisoning and the results of
liver transplantation. Gut 1994;35:809–14.
Neuvonen 1983 {published data only}
Neuvonen PJ, Vartiainen M, Tokola O. Comparison of activated
charcoal and ipecac syrup prevention of drug absorbtion. European
Journal of Clinical Pharmacology 1983;24:557–62.
O’Grady 1988 {published data only}
O’Grady JG, Gimson AES, O Brian CJO, Pucknell A, Hughes RD,
Williams R. Controlled trial of charcoal haemoperfusion and prog-
nostic factors in fulminant hepatic failure. Gastroenterology 1988;94:
1186–92.
O’Grady 1991 {published data only}
O’Grady JG, Wendon J, Tan KC, Potter D, Cottam S, Cohen AT,
et al.Liver transplantation after paracetamol overdose. BMJ (Clinical
Research Ed.) 1991;303:221–3.
Parker 1990 {published data only}
Parker D, White P, Paton D, Routledge A. Safety of late acetylcys-
teine treatment in paracetamol poisoning. Human & Experimental
Toxicology 1990;9:25–7.
Prescott 1976 {published data only}
Prescott LF, Park J, Sutherland GR, Smith IJ. Cysteamine, methio-
nine, and penicillamine in the treatment of paracetamol poisoning.
Lancet 1976;2:109–13.
Prescott 1979 {published data only}
Prescott LF, Illinngworth RN, Chrichley JAJ, Stewart MJ, Adam RD,
Proudfoot AT. Intravenous N-acetylcysteine: the treatment of choice
for paracetamol poisoning. British Medical Journal 1979;2:1097–
1100.
Rangan 2001 {published data only}
Rangan C, Nordt SP, Hamilton R, Ingels M, Clark RF. Treatment
of acetaminophen ingestion with a superactivated charcoal-cola mix-
ture. Annals of Emergency Medicine 2001;37(1):55–8. [MEDLINE:
PMID: 11145772]
Remmert 1990 {published data only}
Remmert HP, Olling M, Slob W, van der Giesen WF, van Dijk
A, Rauws AG. Comparative antidotal efficacy of activated charcoal
tablets, capsules and suspension in healthy volunteers. European Jour-
nal of Clinical Pharmacology 1990;39:501–5.
Rose 1991 {published data only}
Rose SR, Gorman RL, Oderda GM, Klein-Schwarz W, Watson WA.
Simulated acetaminophen overdose: pharmokinetics and effective-
ness of activated charcoal. Annals of Emergency Medicine 1991;20
(10):1064–8.
Saincher 1997 {published data only}
Saincher A, Sitar DS, Tenenbein M. Efficacy of ipacac during the first
hour after drug ingestion in human volunteers. Journal of Toxicology.
Clinical Toxiclogy 1997;35:609–15.
Sato 2003 {published data only}
Sato RL, Wong JJ, Sumida SM, Marn RY, Enoki NR, Yamamoto
LG. Efficacy of superactivated charcoal administered late (3 hours)
after acetaminophen overdose. The American Journal of Emergency
Medicine 2003;21(3):189–91. [MEDLINE: PMID: 12811710]
Sato RL, Wong JJ, Sumida SM, Yamamoto LG. Adverse ef-
fects of superactivated charcoal administered to healthy volunteers.
Hawaii Medical Journal 2002;61(11):251–3. [MEDLINE: PMID:
12516788]
Schiodt 1996 {published data only}
Schiodt FV, Bondesen S, Petersen I, Dalhoff K, Ott P, Tygstrup N.
Admission levels of serum Gc-globulin: predictive value in fulmi-
nant hepatic failure. Hepatology 1996;23(4):713–8. [MEDLINE:
PPMID: 8666322]
Shakil 2000 {published data only}
Shakil AO, Kramer D, Mazariegos GV, Fung JJ, Rakela J. Acute
liver failure: clinical features, outcome analysis, and applicability of
prognostic criteria. Liver Transplantation 2000;6(2):163–9. [MED-
LINE: PMID: 10719014]
Silk 1978 {published data only}
Silk DBA, Williams R. Experiences in the treatment of fulminant
hepatic failure by conservative therapy, charcoal haemoperfusion, and
polyacrylonitrile haemodialysis. The International Journal of Artificial
Organs 1978;1:29–33.
Smilkstein 1988 {published data only}
Rumack BH, Peterson RC, Koch CG, Amara IA. Acetaminophen
overdose. Archives of Internal Medicine 1981;141:380–5.
Rumack BH, Peterson RG. Acetaminophen overdose. Pediatrics
1978;62 (suppl):898–901.
Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH. Efficacy of oral
N-acetylcysteine in the treatment of acetaminophen overdose. New
England Journal of Medicine 1988;319:1557–62.
Smilkstein 1991 {published data only}
Smilkstein MJ, Bronstein AC, Linden C. Acetaminophen overdose:
a 48-hour intravenous N-acetylcysteine treatment protocol. An-
20Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
nals of Emergency Medicine 1991;20:1058–63. [MEDLINE: PMID:
1928874]
Smith 1978 {published data only}
Smith JM, Roberts WO, Hall SM, White TA, Gilbertson AA. Late
treatment of paracetamol poisoning with mercaptamine. British
Medical Journal 1978;1(6109):331–3.
Spiller 1994 {published data only}
Spiller HA, Krenzelok EP, Grande GA, Safir EF, Diamond JJ. A
prospective evaluation of the effect of activated charcoal before oral
N-acetylcysteine in acetaminophen overdose. Annals of Emergency
Medicine 1994;23(3):519–23.
Underhill 1990 {published data only}
Underhill TJ, Greene MK, Dove AF. A comparison of the afficacy
of gastric lavage, ipecacuanha and activated charcoal in the emer-
gency management of paracetamol overdose. Archives of Emergency
Medicine 1990;7:148–54.
Vale 1981 {published data only}
Vale JA, Meredith TJ, Goulding R. Treatment of acetaminophen
poisoning. The use of oral methionine. Archives of Internal Medicine
1981;141(3 Spec No):394–6. [MEDLINE: 81132588]
Woo 2000 {published data only}
Woo OF, Mueller PD, Olson KR, Anderson IB, Kim SY. Shorter
duration of oral N-acetylcysteine therapy for acute acetaminophen
overdose. Annals of Emergency Medicine 2000;35(4):363–8.
Yeates 2000 {published data only}
Yeates PJA, Thomas HL. Effectiveness of delayed activated charcoal
administration in simulated paracetamol overdose. British Journal of
Clinical Pharmacology 2000;49:11–4.
References to studies excluded from this review
Alander 2000 {published data only}
Alander SW, Dowd MD, Bratton SL, Kearns GL. Pediatric ac-
etaminophen overdose: risk factors associated with hepatocellular
injury. Archieves of Pediatric and Adolescent Medicine 2000;154(4):
346–50.
Beckett 1989 {published data only}
Beckett GJ, Foster GR, Hussey AJ, Oliveira DBG, Proudfoot AT,
Prescott LF, et al.Plasma gluthathione S-transferase and F protein are
more sensitive than alanine aminotransferase as makers of paraceta-
mol-induced liver damage. Clinical Chemistry 1989;35(11):2186–9.
Beckett 1990 {published data only}
Beckett GJ, Donovan JW, Hussey AJ, Proudfoot AT, Prescott LF.
Intravenous N-acetylcysteine, hepatotoxicity and plasma glutathione
S-transferase in patients with paracetamol overdosage. Human &
Experimental Toxicology 1990;9(3):183–6. [MEDLINE: 90329304]
Bond 1999 {published data only}
Bond GR, Hite LK. Population-based incidence and outcome of
acetaminophen poisoning by type of ingestion. Academic Emergency
Medicine 1999;6(11):1115–20. [: PMID: 10569383]
Bray 1991 {published data only}
Bray GP, Mowat C, Muir DF, Tredger JM, Williams R. The effect
of chronic alcohol intake on prognosis and outcome in paracetamol
overdose. Human & Experimantal Toxicology 1991;10(6):435–8.
Brotodihardjo 1992 {published data only}
Brotodihardjo AE, Batey RG, Farrell GC, Byth K. Hepatotoxicity
from paracetamol selfpoisoning in western Sydney. The Medical Jour-
nal of Australia 1992;157:382–5.
Chamberlain 1993 {published data only}
Chamberlain JM, Gorman RL, Oderda GM, Klein-Schwartz W,
Klein BL. Use of activated charcoal in a simulated poisoning with
acetaminophen: a new loading dose for N-acetylcysteine?. Annals of
Emergency Medicine 1993;22(9):1398–402.
Chan 1993 {published data only}
Chan TYK, Chan AYW, Chritchley JAJH. Paracetamol poisoning
and hepatotoxicity in Chinese. Singapore Medical Journal 1993;34:
299–302.
Chan 1994 {published data only}
Chan TY, Critchley JA. Adverse reactions to intravenous N-acetylcys-
teine in Chinese patients with paracetamol (acetaminophen) poison-
ing. Human & Experimental Toxicology 1994;13 (8):542–4. [MED-
LINE: 95033433]
Chan 1996 {published data only}
Chan TY, Chan AY, Critchley JA. Factors responsible for continuing
morbidity after paracetamol poisoning in Chinese patients in Hong
Kong. Singapore Medical Journal 1996;37(3):275–7.
Dordoni 1973 {published data only}
Dordoni B, Willson RA, Thompson RPH, Williams R. Reduction of
absorption of paracetamol by activated charcoal and cholestyramine.
British Medical Journal 1973;3:86–7.
Gee 1998 {published data only}
Gee P, Ardagh M. Paediatric exploratory ingestions of paracetamol.
New Zealand Medical Journal 1998; Vol. 111, issue 1066:186–8.
James 2002 {published data only}
James LP, Wells E, Beard RH, Farrar HC. Predictors of outcome
after acetaminophen poisoning in children and adolescents. Journal
of Pediatrics 2002;140(5):522–6.
Levy 1985 {published data only}
Levy M, Oren R. Paracetamol overdosage in Jerusalem. Israel Journal
of Medical Sciences 1985;21 (1):36–9. [MEDLINE: 85130101]
Makin 1995 {published data only}
Makin AJ, Wendon J, Williams R. A 7-year experience of severe ac-
etaminophen-induced hepatotoxicity (1987-1993). Gastroenterology
1995;109(6):1907–16.
Oh 1980 {published data only}
Oh TE, Shenfield GM. Intravenous N-acetylcysteine for paraceta-
mol poisoning. The Medical Journal of Australia 1980;1(13):664–5.
[MEDLINE: 81030192]
Oren 1992 {published data only}
Oren R, Levy M. Paracetamol overdose in Jerusalem, 1984-89. Is-
rael Journal of Medical Sciences 1992;28(11):795–6. [MEDLINE:
93106742]
Perry 1998 {published data only}
Perry HE, Shannon MW. Efficacy of oral versus intravenous N-acetyl-
cysteine in acetaminophen overdose. Pediatrics 1998;132:149–52.
Prescott 1989 {published data only}
Prescott LF, Donovan JW, Jarvie DR, Proudfoot AT. The disposition
and kinetics of intravenous N-acetylcysteine in patients with parac-
21Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
etamol overdosage. European Journal of Clinical Pharmacology 1989;
37(5):501–6. [MEDLINE: 90092231]
Read 1986 {published data only}
Read RB, Tredger JM, Williams R. Analysis of factors responsible for
continuing mortality after paracetamol overdose. Human Toxicology
1986;5(3):201–6.
Riggs 1989 {published data only}
Riggs BS, Bronstein AC, Kulig K, Archer PG, Rumack BH. Acute
acetaminophen overdose during pregnancy. Obstetrics and Gynecol-
ogy 1989;74(2):247–53. [MEDLINE: 89314668]
Rivera-Penera 1997 {published data only}
Rivera-Penera T, Gugig R, Davis J, McDiarmid S, Vargas J, Rosenthal
P, et al.Outcome of acetaminophen overdose in pediatric patients
and factors contributing to hepatotoxicity. Pediatrics 1997;130(2):
300–4.
Schiodt 1997 {published data only}
Schiodt FV, Rochling FA, Casey DL, Lee WM. Acetaminophen tox-
icity in an urban county hospital. New England Journal of Medicine
1997;337(16):1112–7.
Schmidt 2002a {published data only}
Schmidt LE, Dalhoff K, Poulsen HE. Acute versus chronic alcohol
consumption in acetaminophen-induced hepatotoxicity. Hepatology
2002;35(4):876–82.
Singer 1995 {published data only}
Singer AJ, Carracio TR, Mofenson HC. The temporal profile of in-
creased transaminase levels in patients with acetaminophen-induced
liver dysfunction. Annals of Emergency Medicine 1995;26(1):49–53.
[MEDLINE: 95314041]
References to studies awaiting assessment
Dougherty 2000 {published data only}
Additional references
Als-Nielsen 2004
Als-Nielsen B, Gluud LL, Gluud C. Methodological quality and
treatments effects in randomised trials - a review of six emperical stud-
ies (abstract). 12th Cochrane Colloquium, Ottawa, Canada (http:
//www.cochrane.org/colloquia/abstracts/ottawa/); abstract book: O-
072: 2004.
Appelboam 2002
Appelboam AV, Dargan PI, Knighton J. Fatal anaphylactoid reaction
to N-acetylcysteine: caution in patients with asthma. Emergency
Medicine Journal 2002;19(6):594–5. [: PMID: 12421803]
Bailey 2003
Bailey B, Amre DK, Gaudreault P. Fulminant hepatic failure sec-
ondary to acetaminophen poisoning: a systematic review and meta-
analysis of prognostic criteria determining the need for liver trans-
plantation. Critical Care Medicine 2003;31(1):299–305.
Bailey 2004
Bailey B, Blais R, Letarte A. Status epilepticus after a massive intra-
venous N-acetylcysteine overdose leading to intracranial hyperten-
sion and death. Annals of Emergency Medecine 2004;44(4):401–6. [:
PMID: 15459624]
Chyka 2005
Chyka PA, Seger D, Krenzelok EP, Vale JA, American Academy of
Clinical Toxicology, European Association of Poisons Centres and
Clinical Toxicologists. Position paper: Single-dose activated char-
coal. Clinical Toxicology 2005;43(2):61–87. [MEDLINE: PMID:
15822758]
Clark 1973
Clark R, Borirakchanyavat V, Davidson AR, Thompson RP, Widdop
B, Goulding R, et al.Hepatic damage and death from overdose of
paracetamol. Lancet 1973;1(7794):66–70.
Cooper 2005
Cooper GM, Le Couteur DG, Richardson D, Buckley NA. A ran-
domized clinical trial of activated charcoal for the routine manage-
ment of oral drug overdose. QJM: Monthly Journal of the Association
of Physicians 2005;98(9):655–60. [MEDLINE: PMID: 16040667]
Deeks 1998
Deeks JJ, Bradburn MJ, Localio R, Berlin J. Much ado
about nothing: meta-analysis for rare events. Proceed-
ings of the Sixth Cochrane Colloquium, 1998. http:
//www.cochrane.org/docs/prizes.abstracts.htm#much (Accessed 22
February 2006).
Deeks 2003
Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et
al.International Stroke Trial Collaborative Group, European Carotid
Surgery Trial Collaborative Group. Evaluating non-randomised in-
tervention studies. Health Technology Assessment 2003; Vol. 7,
issue 27:1–173.
DeMets 1987
DeMets DL. Pratical aspects in monitoring: a brief review. Statistics
in Medicine 1987;6(7):753–60.
DerSimonian 1986
DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled
Clinical Trials 1986;7(3):177–88.
Egger 1997
Egger M, Davey GD, Schneider M, Minder C. Bias in meta-analysis
detected by a simple graphical test. BMJ (Clinical Research Ed.) 1997;
315:629–34.
Ferner 2004
Ferner RE, Langford NJ, Anton C, Hutchings A, Bateman DN,
Routledge PA. Random and systematic medication errors in routine
clinical practice: a multicentre study of infusions, using acetylcys-
teine as an example. British Journal of Clinical Pharmacology 2001;
52(5):573–7. [: PMID: 11736866]
Higgins 2002
Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-
analysis. Statistics in Medicine 2002;21:1539–58.
Jüni 2001
Jüni P, Douglas GA, Egger M. Assessing the quality of controlled
clinical trials. BMJ (Clinical Research Ed.) 2001;323:42–46.
Kjaergard 2001
Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality
and discrepancies between large and small randomized trials in meta-
analyses. Annals of Internal Medicine 2001;135(11):982–9.
22Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Koch-Weser 1976
Koch-Weser J. Acetaminophen. New England Journal of Medicine
1976;295(23):1297–300.
Krenzelok 2004
Krenzelok EP, McGuigan M, Lheur P, Manoguerra AS. Position pa-
per: Ipecac syrup. Journal of Toxicology. Clinical Toxicology 2004;42
(2):133–43. [MEDLINE: PMID: 15214617]
Kwan 2005
Kwan D, Bartle WR, Walker SE. Abnormal serum transaminases fol-
lowing therapeutic doses of acetaminophen in the absence of known
risk factors. Digestive Diseases and Sciences 1995;40(9):1951–5.
Lee 2004
Lee WM. Acetaminophen and the U.S. Acute Liver Failure Study
Group: lowering the risks of hepatic failure. Hepatology 2004;40(1):
6–9. [MEDLINE: PMID: 15239078]
Liisanantti 2003
Liisanantti J, Kaukoranta P, Martikainen M, Ala-Kokko T. Aspiration
pneumonia following severe self-poisoning. Resuscitation 2003;56
(1):49–53. [MEDLINE: PMID: 12505738]
Mant 1984
Mant TG, Tempowski JH, Volans GN, Talbot JC. Adverse reactions
to acetylcysteine and effects of overdose. British Medical Journal
(Clinical Research Ed.) 1984;289(6439):217–9. [: PMID: 6234965]
Mitchell 1988
Mitchell JR. Acetaminphen toxicity. New England Journal of
Medicine 1988;319:1601–2.
Moher 1998
Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al.Does
quality of reports of randomised trials affect estimates of intervention
efficacy reported in meta-analysis. Lancet 1998;352:609–13.
Morgan 2005
Morgan O, Griffiths C, Majeed A. Impact of paracetamol pack size
restrictions on poisoning from paracetamol in England and Wales:
an observational study. Journal of Public Health 2005;27(1):19–24.
[MEDLINE: PMID: 15637104]
O’Grady 1997
O’Grady JG. Paracetamol-induced acute liver failure. Journal of Hep-
atology 1997;26 (Suppl):41–6.
RevMan 2003
Copenhagen: The Nordic Cochrane Centre, The Cochrane Collab-
oration. Review Manager (RevMan). 4.2 for Windows. Copen-
hagen: The Nordic Cochrane Centre, The Cochrane Collaboration,
2003.
Royle 2003
Royle P, Milne R. Literature searching for randomized controlled
trials used in Cochrane reviews: rapid versus exhaustive searches.
International Journal of Technology Assessment in Health Care 2003;
19(4):591–603.
Rumack 1975
Rumack BH, Matthew H. Acetaminophen poisoning and toxicity.
Pediatrics 1975;55:871–6.
Sacks 1982
Sacks H, Chalmers TC, Smith H. Randomised versus historical con-
trols for clinical trials. Americal Journal of Medicine 1982;72:233–
40.
Schmidt 2002
Schmidt LE, Knudsen TT, Dalhoff K, Bendtsen F. Effect of acetyl-
cysteine on prothrombin index in paracetamol poisoning without
hepatocellular injury. Lancet 2002;360(9340):1151–2. [: PMID:
12387966]
Schulz 1995
Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of
bias. Dimensions of methodological quality associated with estimates
of treatment effects in controlled trials. JAMA 1995;273:408–12.
Speeg 1995
Speeg KV, Bay MK. Prevention and treatment of drug-induced liver
disease. Gastroenterology Clinics of North America 1995;24(4):1047–
64.
Thomas 1997
Thomas SH, Horner JE, Chew K, Connolly J, Dorani B, Bevan L, et
al.Paracetamol poisoning in the north east of England: presentation,
early management and outcome. Human & Experimantal Toxicology
1997;16(9):495–500. [: PMID: 9306135]
Vale 1995
Vale JA, Proudfoot AT. Paracetamol (acetaminophen) poisoning.
Lancet 1995;346(8974):547–52.
Vale 2004
Vale JA, Kulig K, American Academy of Clinical Toxicology, Euro-
pean Association of Poisons Centres and Clinical Toxicologists. Po-
sition statement: gastric lavage. Journal of Toxicology. Clinical Toxi-
cology 2004;42(7):933–43. [MEDLINE: PMID: 15641639]
Whyte 2000
Whyte IM, Buckley NA, Reith DM, Goodhew I, Seldon M, Dawson
AH. Acetaminophen causes an increased International Normalized
Ratio by reducing functional factor VII. Therapeutic Drug Monitoring
2000;22(6):742–8.∗ Indicates the major publication for the study
23Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
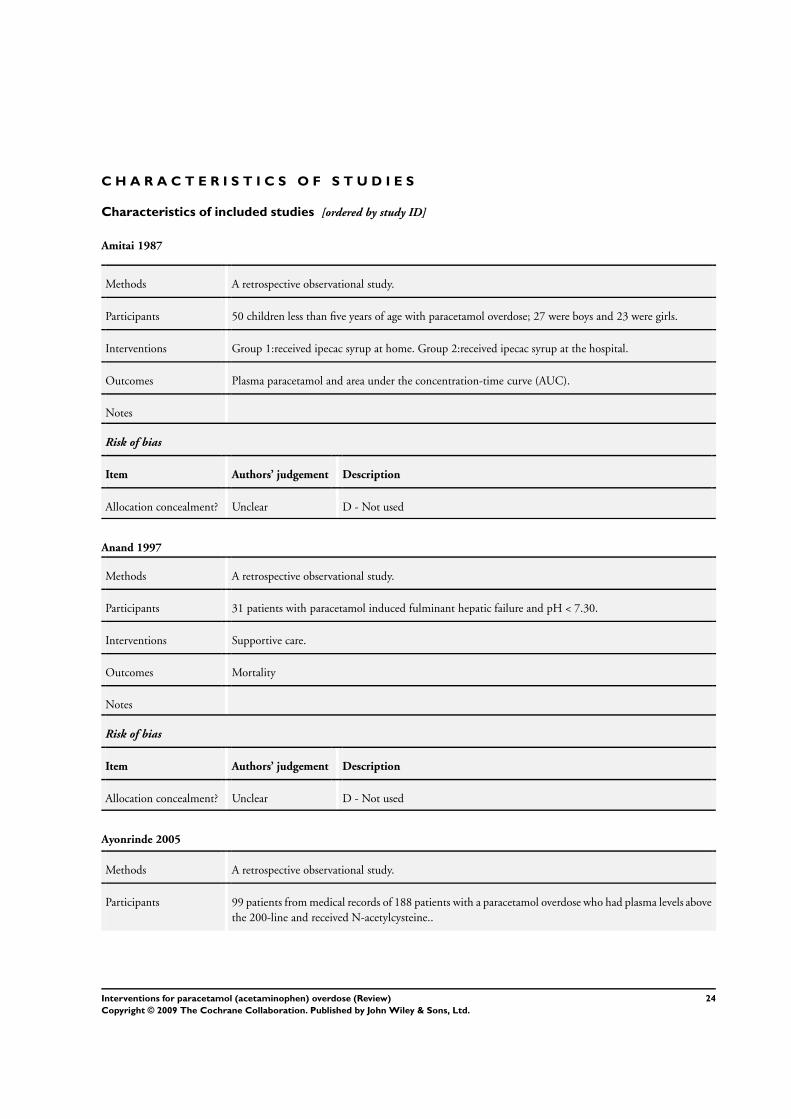
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Amitai 1987
Methods A retrospective observational study.
Participants 50 children less than five years of age with paracetamol overdose; 27 were boys and 23 were girls.
Interventions Group 1:received ipecac syrup at home. Group 2:received ipecac syrup at the hospital.
Outcomes Plasma paracetamol and area under the concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Anand 1997
Methods A retrospective observational study.
Participants 31 patients with paracetamol induced fulminant hepatic failure and pH < 7.30.
Interventions Supportive care.
Outcomes Mortality
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Ayonrinde 2005
Methods A retrospective observational study.
Participants 99 patients from medical records of 188 patients with a paracetamol overdose who had plasma levels above
the 200-line and received N-acetylcysteine..
24Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Ayonrinde 2005 (Continued)
Interventions N-acetylcysteine.
Outcomes Aspartate aminotransferase.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Bernal 1998
Methods A retrospective observational study.
Participants 124 patients eligible for liver transplantation due to paracetamol overdose.
Transplant criteria were serum creatinine > 300 µmol/L, prothrombin time of > 100 seconds, and grade
3 or 4 encephalopathy in patients with normal pH, or the single finding of pH < 7.3.
Interventions Intervention group:
received liver transplantation.
Control group:
received only supportive treatment.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Bond 1993
Methods A retrospective observational study.
Participants 644 paediatric patients (one to six years old) who ingested paracetamol and had high paracetamol con-
centration at four to 4.5 hours.
Interventions Patients received ipecac syrup.
25Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
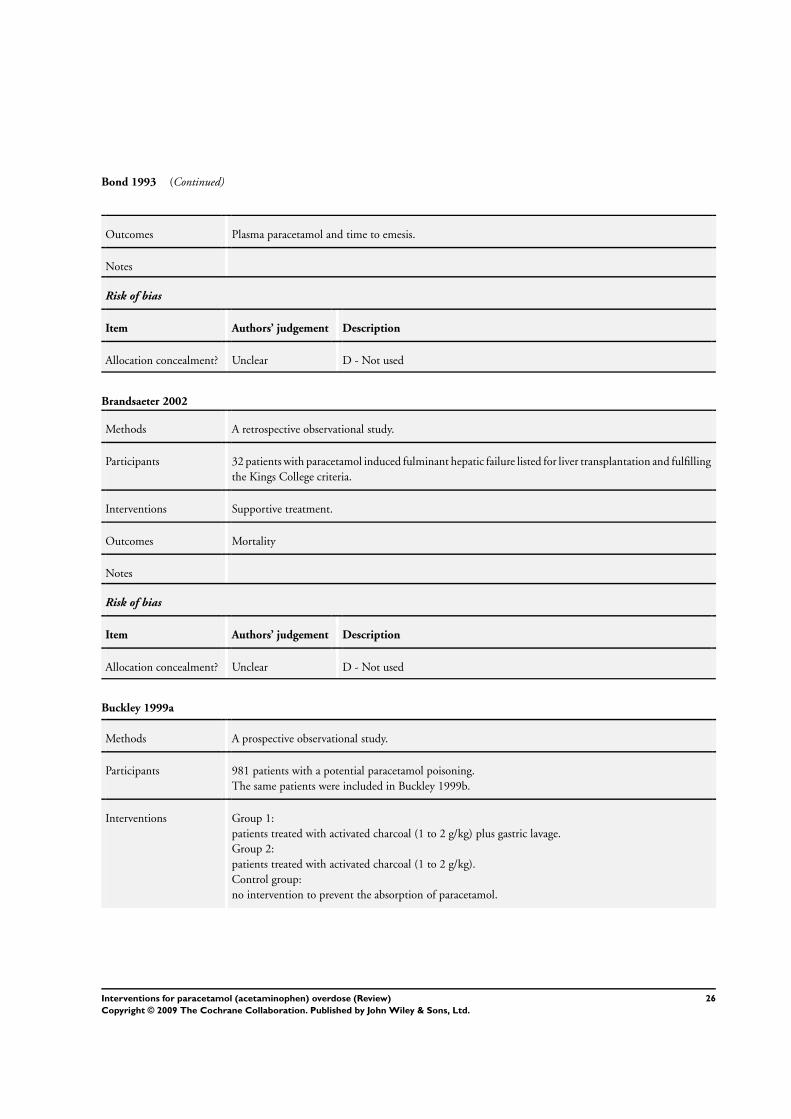
Bond 1993 (Continued)
Outcomes Plasma paracetamol and time to emesis.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Brandsaeter 2002
Methods A retrospective observational study.
Participants 32 patients with paracetamol induced fulminant hepatic failure listed for liver transplantation and fulfilling
the Kings College criteria.
Interventions Supportive treatment.
Outcomes Mortality
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Buckley 1999a
Methods A prospective observational study.
Participants 981 patients with a potential paracetamol poisoning.
The same patients were included in Buckley 1999b.
Interventions Group 1:
patients treated with activated charcoal (1 to 2 g/kg) plus gastric lavage.
Group 2:
patients treated with activated charcoal (1 to 2 g/kg).
Control group:
no intervention to prevent the absorption of paracetamol.
26Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Buckley 1999a (Continued)
Outcomes Mortality, plasma paracetamol concentration (ie, above the 150 and 200 risk-line).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Buckley 1999b
Methods A prospective observational study.
Participants 981 patients with a potential paracetamol poisoning;
86 patients had a paracetamol concentration above the probable risk line.
The same patients were included in Buckley 1999a.
Interventions Intervention group:
patients received activated charcoal (1 to 2 g/kg) if they arrived within four hours of ingestion.
Patients were given N-acetylcysteine. intravenously (300 mg/kg over 20 hours) if paracetamol concen-
tration was above the probable risk-line in the nomogram or if they had taken > 125 mg/kg and if the
serum concentration was not available within eight hours. Patients having a plasma concentration above
the possible risk-line in the nomogram were given NAC if the calculated half-life was > 4 hours.
Control group:
historical patients treated at other units given other doses of NAC.
Outcomes Mortality, acetaminophen plasma concentration (ie, above the 150 and 200 risk-line).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Burkhart 1995
Methods A quasi-randomised study.
Used odd/even months at hospitalisation to allocate patients to different interventions.
Participants 107 patients with paracetamol overdose according to the 150 risk line.
27Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
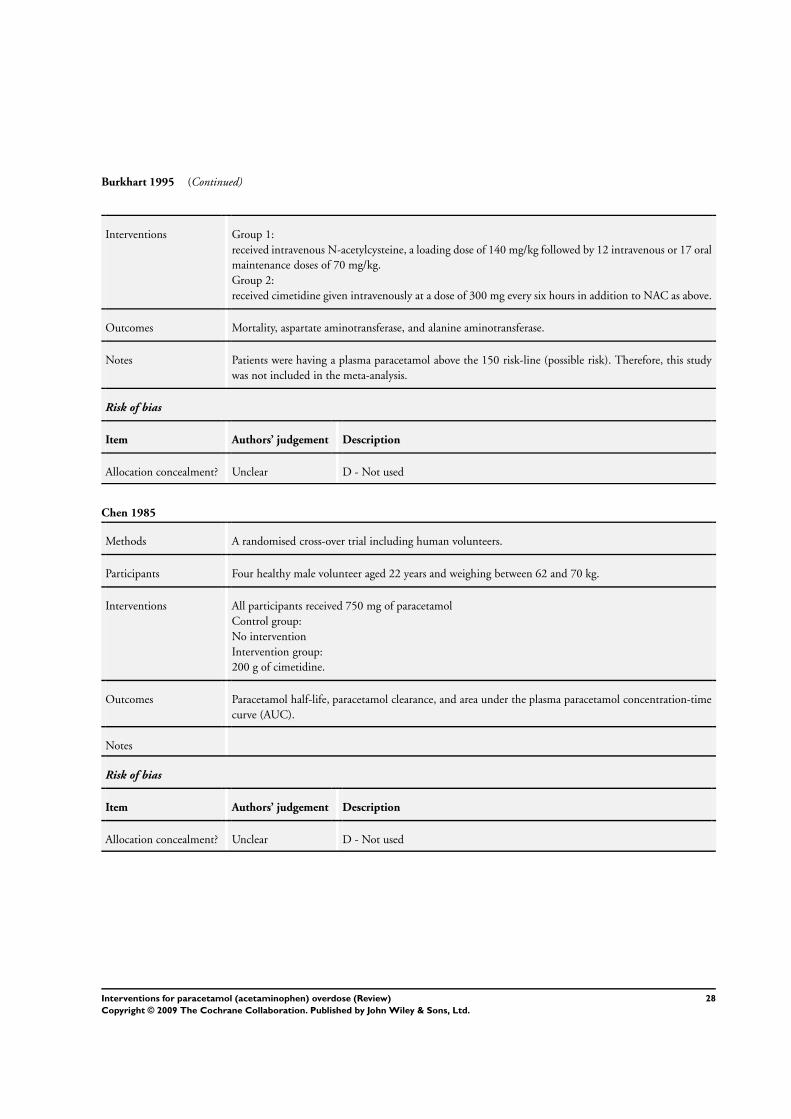
Burkhart 1995 (Continued)
Interventions Group 1:
received intravenous N-acetylcysteine, a loading dose of 140 mg/kg followed by 12 intravenous or 17 oral
maintenance doses of 70 mg/kg.
Group 2:
received cimetidine given intravenously at a dose of 300 mg every six hours in addition to NAC as above.
Outcomes Mortality, aspartate aminotransferase, and alanine aminotransferase.
Notes Patients were having a plasma paracetamol above the 150 risk-line (possible risk). Therefore, this study
was not included in the meta-analysis.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Chen 1985
Methods A randomised cross-over trial including human volunteers.
Participants Four healthy male volunteer aged 22 years and weighing between 62 and 70 kg.
Interventions All participants received 750 mg of paracetamol
Control group:
No intervention
Intervention group:
200 g of cimetidine.
Outcomes Paracetamol half-life, paracetamol clearance, and area under the plasma paracetamol concentration-time
curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
28Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
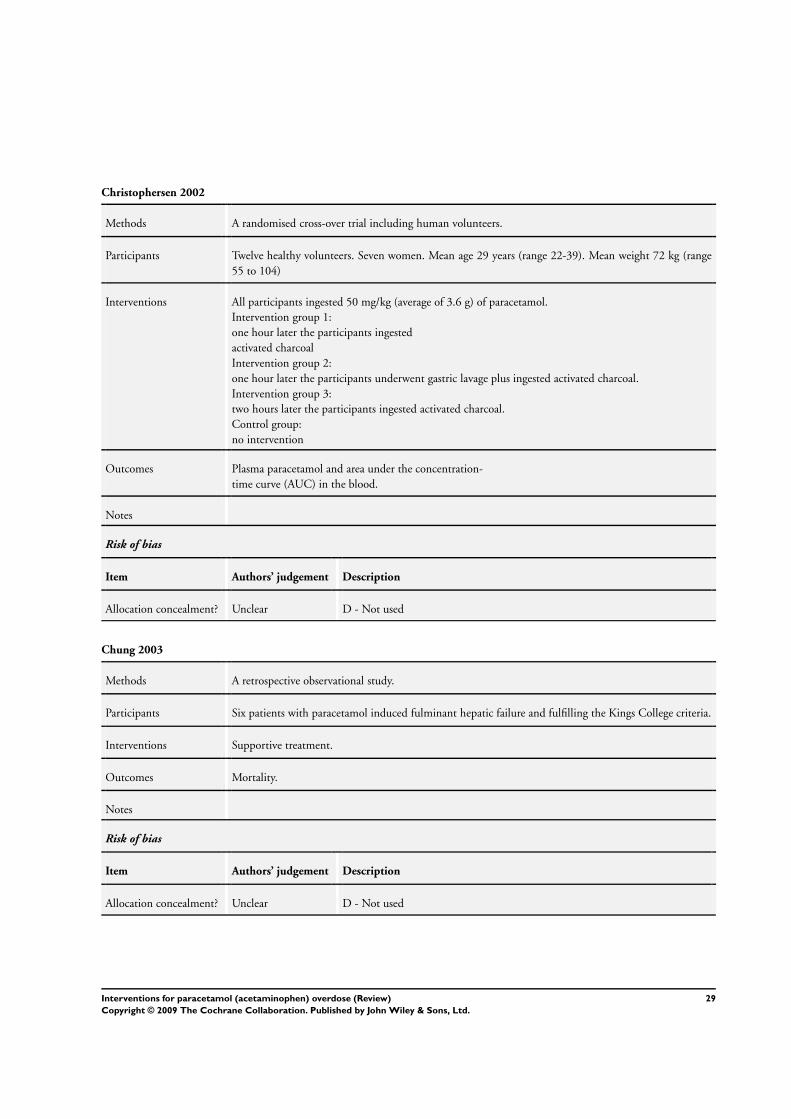
Christophersen 2002
Methods A randomised cross-over trial including human volunteers.
Participants Twelve healthy volunteers. Seven women. Mean age 29 years (range 22-39). Mean weight 72 kg (range
55 to 104)
Interventions All participants ingested 50 mg/kg (average of 3.6 g) of paracetamol.
Intervention group 1:
one hour later the participants ingested
activated charcoal
Intervention group 2:
one hour later the participants underwent gastric lavage plus ingested activated charcoal.
Intervention group 3:
two hours later the participants ingested activated charcoal.
Control group:
no intervention
Outcomes Plasma paracetamol and area under the concentration-
time curve (AUC) in the blood.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Chung 2003
Methods A retrospective observational study.
Participants Six patients with paracetamol induced fulminant hepatic failure and fulfilling the Kings College criteria.
Interventions Supportive treatment.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
29Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Crome 1976
Methods A retrospective observational study.
Participants 30 patients at risk of hepatic damage from paracetamol ingestion according to patient history.
Interventions Intervention group:
all patients received methionine (2.5 g orally every four hours up to a total dose of ten g).
Control group:
patients given supportive treatment at other units.
Outcomes Aspartate aminotransferase and bilirubin.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Douglas 1976
Methods A randomised clinical trial.
Control of bias:
- Allocation sequence generated by table of random numbers
- Allocation concealed not described
- No double blinding.
Participants 38 patients who were admitted to the hospital within 17 hours of paracetamol ingestion, and those plasma-
paracetamol was above the 200-line (probable risk-line).
Interventions Cysteamine group:
cysteamine was given as described by Prescott et al. (1973) except that it was dissolved in 5% dextrose
and injected, or added to 5% dextrose infusion, using a Millipore filter attached to a syringe.
Control group:
received supportive treatment: 5% dextrose, 2-3 litres daily, with added vitamins and potassium if necessary.
Outcomes Mortality, maximum aspartate aminotransferase, maximum serum bilirubin, maximum prothrombin
time, liver biopsy findings, maximum serum-ferritin, maximum serum bile, and adverse events.
Notes Douglas et al did not provide the time interval between ingestion of paracetamol and treatment in either
groups.
Four of the patients were also included in Hamlyn 1981 study.
Risk of bias
30Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Douglas 1976 (Continued)
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Galinsky 1984
Methods A randomised cross-over study including human volunteers.
Participants Eight healthy volunteers between 23 and 36 years weighing between 70 and 100 kg.
Interventions All participants ingested one gram of paracetamol
Intervention group:
ten grams of activated charcoal were consumed at the same time.
Control group:
no intervention.
Outcomes Plasma paracetamol and the area under the concentration-
time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Gazzard 1974
Methods A randomised clinical trial.
Control of bias:
- Generation of the allocation sequence: not described
- Allocation concealment: not described
- Blinding: no.
Participants 22 patients with a prothrombin time ratio of more than 2.2 after a paracetamol overdose.
Interventions Intervention group:
All patients received 300 ml of fresh frozen plasma every six hour until the prothrombin time had returned
to 1.25 or less. They also received heparin, given intravenously by pump infusion, to maintain a blood
heparin equivalent of 0.5/100 ml/mg.
Control group:
They received the same as the first group but without the heparin.
31Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
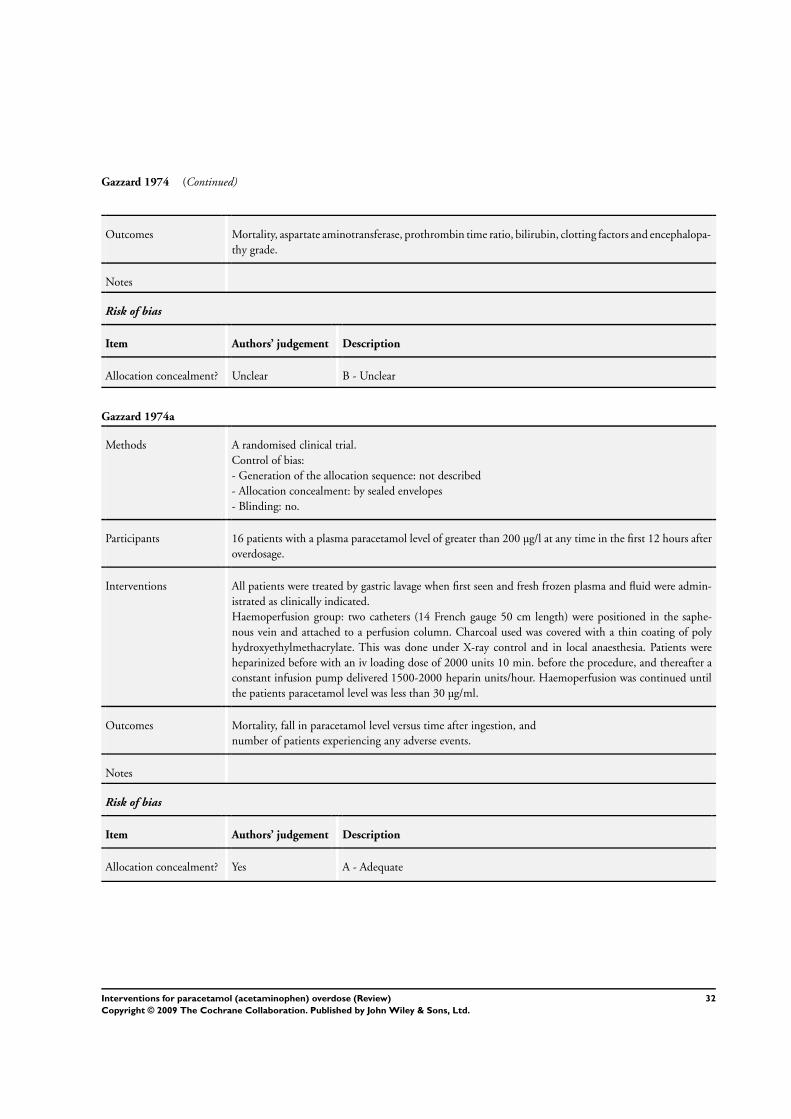
Gazzard 1974 (Continued)
Outcomes Mortality, aspartate aminotransferase, prothrombin time ratio, bilirubin, clotting factors and encephalopa-
thy grade.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Gazzard 1974a
Methods A randomised clinical trial.
Control of bias:
- Generation of the allocation sequence: not described
- Allocation concealment: by sealed envelopes
- Blinding: no.
Participants 16 patients with a plasma paracetamol level of greater than 200 µg/l at any time in the first 12 hours after
overdosage.
Interventions All patients were treated by gastric lavage when first seen and fresh frozen plasma and fluid were admin-
istrated as clinically indicated.
Haemoperfusion group: two catheters (14 French gauge 50 cm length) were positioned in the saphe-
nous vein and attached to a perfusion column. Charcoal used was covered with a thin coating of poly
hydroxyethylmethacrylate. This was done under X-ray control and in local anaesthesia. Patients were
heparinized before with an iv loading dose of 2000 units 10 min. before the procedure, and thereafter a
constant infusion pump delivered 1500-2000 heparin units/hour. Haemoperfusion was continued until
the patients paracetamol level was less than 30 µg/ml.
Outcomes Mortality, fall in paracetamol level versus time after ingestion, and
number of patients experiencing any adverse events.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
32Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
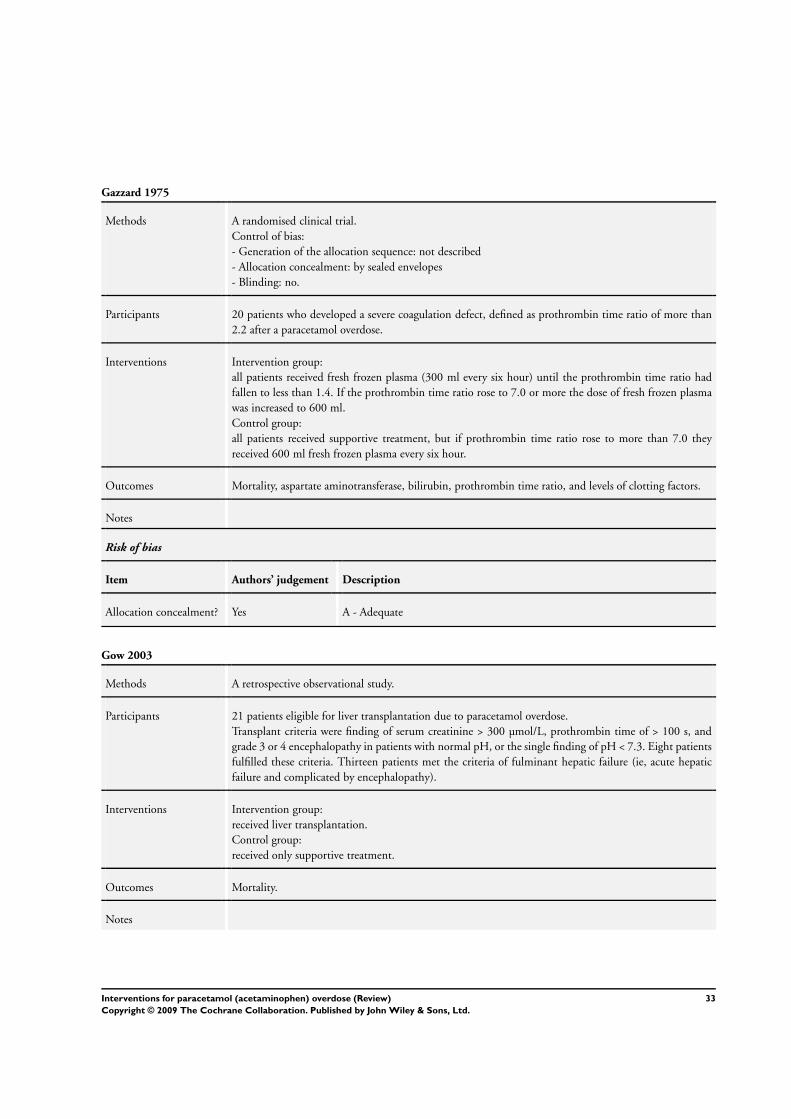
Gazzard 1975
Methods A randomised clinical trial.
Control of bias:
- Generation of the allocation sequence: not described
- Allocation concealment: by sealed envelopes
- Blinding: no.
Participants 20 patients who developed a severe coagulation defect, defined as prothrombin time ratio of more than
2.2 after a paracetamol overdose.
Interventions Intervention group:
all patients received fresh frozen plasma (300 ml every six hour) until the prothrombin time ratio had
fallen to less than 1.4. If the prothrombin time ratio rose to 7.0 or more the dose of fresh frozen plasma
was increased to 600 ml.
Control group:
all patients received supportive treatment, but if prothrombin time ratio rose to more than 7.0 they
received 600 ml fresh frozen plasma every six hour.
Outcomes Mortality, aspartate aminotransferase, bilirubin, prothrombin time ratio, and levels of clotting factors.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Gow 2003
Methods A retrospective observational study.
Participants 21 patients eligible for liver transplantation due to paracetamol overdose.
Transplant criteria were finding of serum creatinine > 300 µmol/L, prothrombin time of > 100 s, and
grade 3 or 4 encephalopathy in patients with normal pH, or the single finding of pH < 7.3. Eight patients
fulfilled these criteria. Thirteen patients met the criteria of fulminant hepatic failure (ie, acute hepatic
failure and complicated by encephalopathy).
Interventions Intervention group:
received liver transplantation.
Control group:
received only supportive treatment.
Outcomes Mortality.
Notes
33Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Gow 2003 (Continued)
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Green 2001
Methods A randomised cross-over trial including human volunteers.
Participants 7 males and 3 females from 22 to 31 years old. Weight 77.4 ± 14.1 (mean ±SE).
Interventions All participants ingested four grams of acetaminophen with 250 ml water.
Intervention groups:
One, two, or three hours later the participant ingested 50 g of activated charcoal.
Control group:
no intervention.
Outcomes Plasma paracetamol and area under the concentration-
time curve (AUC) and maximum level of paracetamol in the blood.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Green 2004
Methods A randomised cross-over trial including human volunteers.
Participants 6 males and 4 females from 23 to 37 years old.
Interventions All participants ingested four grams of paracetamol with 250 ml water.
Intervention group 1:
one hour later the participant ingested 50 g of activated charcoal and atropine sulfate i.m. 0.01 mg/kg
prior to paracetamol.
Intervention group 2:
one hour later the participant ingested 50 g of activated charcoal.
Control group:
no intervention.
34Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Green 2004 (Continued)
Outcomes Plasma paracetamol and area under the concentration-
time curve (AUC) and maximum level of paracetamol in the blood.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Grierson 2000
Methods A randomised cross-over trial including human volunteers.
Participants Eight healthy males and two females from 22 to 31 years old.
Interventions All participants ingested four grams of acetaminophen in a solution of 60 ml of water.
Intervention group:
one hour later the participant underwent gastric lavage.
Control group:
no intervention.
Outcomes Plasma paracetamol and area under the concentration-
time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
35Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
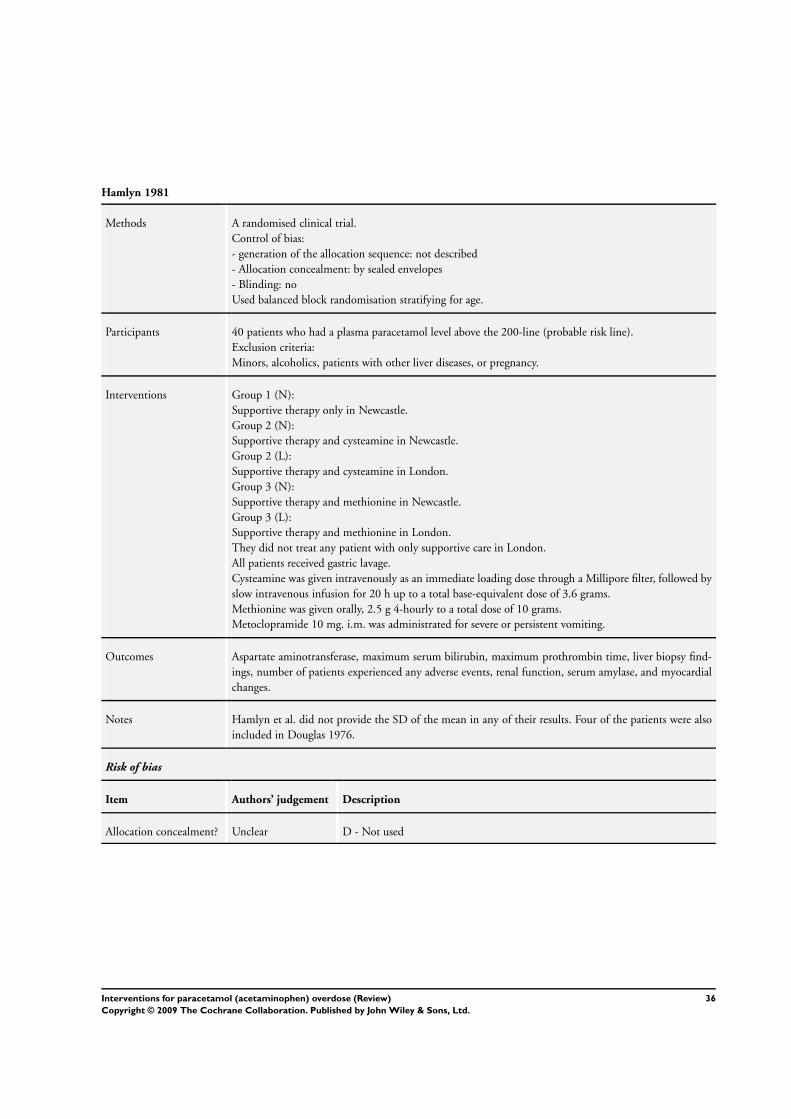
Hamlyn 1981
Methods A randomised clinical trial.
Control of bias:
- generation of the allocation sequence: not described
- Allocation concealment: by sealed envelopes
- Blinding: no
Used balanced block randomisation stratifying for age.
Participants 40 patients who had a plasma paracetamol level above the 200-line (probable risk line).
Exclusion criteria:
Minors, alcoholics, patients with other liver diseases, or pregnancy.
Interventions Group 1 (N):
Supportive therapy only in Newcastle.
Group 2 (N):
Supportive therapy and cysteamine in Newcastle.
Group 2 (L):
Supportive therapy and cysteamine in London.
Group 3 (N):
Supportive therapy and methionine in Newcastle.
Group 3 (L):
Supportive therapy and methionine in London.
They did not treat any patient with only supportive care in London.
All patients received gastric lavage.
Cysteamine was given intravenously as an immediate loading dose through a Millipore filter, followed by
slow intravenous infusion for 20 h up to a total base-equivalent dose of 3.6 grams.
Methionine was given orally, 2.5 g 4-hourly to a total dose of 10 grams.
Metoclopramide 10 mg. i.m. was administrated for severe or persistent vomiting.
Outcomes Aspartate aminotransferase, maximum serum bilirubin, maximum prothrombin time, liver biopsy find-
ings, number of patients experienced any adverse events, renal function, serum amylase, and myocardial
changes.
Notes Hamlyn et al. did not provide the SD of the mean in any of their results. Four of the patients were also
included in Douglas 1976.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
36Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
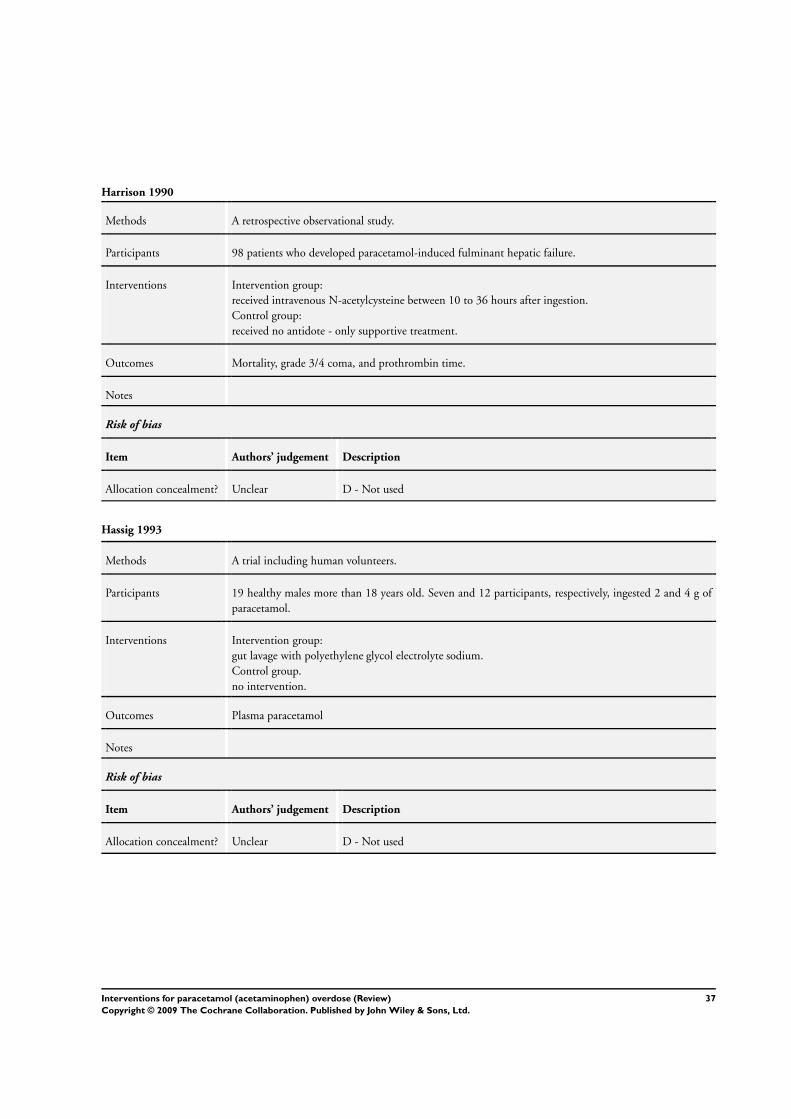
Harrison 1990
Methods A retrospective observational study.
Participants 98 patients who developed paracetamol-induced fulminant hepatic failure.
Interventions Intervention group:
received intravenous N-acetylcysteine between 10 to 36 hours after ingestion.
Control group:
received no antidote - only supportive treatment.
Outcomes Mortality, grade 3/4 coma, and prothrombin time.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Hassig 1993
Methods A trial including human volunteers.
Participants 19 healthy males more than 18 years old. Seven and 12 participants, respectively, ingested 2 and 4 g of
paracetamol.
Interventions Intervention group:
gut lavage with polyethylene glycol electrolyte sodium.
Control group.
no intervention.
Outcomes Plasma paracetamol
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
37Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
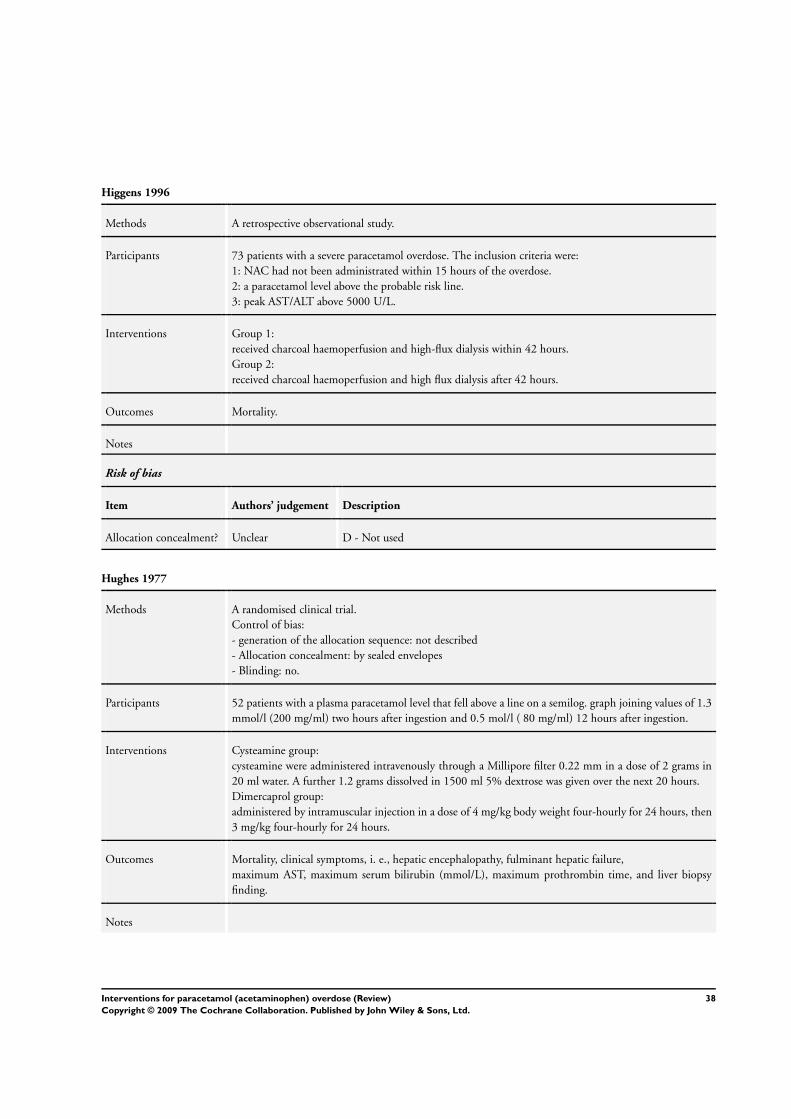
Higgens 1996
Methods A retrospective observational study.
Participants 73 patients with a severe paracetamol overdose. The inclusion criteria were:
1: NAC had not been administrated within 15 hours of the overdose.
2: a paracetamol level above the probable risk line.
3: peak AST/ALT above 5000 U/L.
Interventions Group 1:
received charcoal haemoperfusion and high-flux dialysis within 42 hours.
Group 2:
received charcoal haemoperfusion and high flux dialysis after 42 hours.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Hughes 1977
Methods A randomised clinical trial.
Control of bias:
- generation of the allocation sequence: not described
- Allocation concealment: by sealed envelopes
- Blinding: no.
Participants 52 patients with a plasma paracetamol level that fell above a line on a semilog. graph joining values of 1.3
mmol/l (200 mg/ml) two hours after ingestion and 0.5 mol/l ( 80 mg/ml) 12 hours after ingestion.
Interventions Cysteamine group:
cysteamine were administered intravenously through a Millipore filter 0.22 mm in a dose of 2 grams in
20 ml water. A further 1.2 grams dissolved in 1500 ml 5% dextrose was given over the next 20 hours.
Dimercaprol group:
administered by intramuscular injection in a dose of 4 mg/kg body weight four-hourly for 24 hours, then
3 mg/kg four-hourly for 24 hours.
Outcomes Mortality, clinical symptoms, i. e., hepatic encephalopathy, fulminant hepatic failure,
maximum AST, maximum serum bilirubin (mmol/L), maximum prothrombin time, and liver biopsy
finding.
Notes
38Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
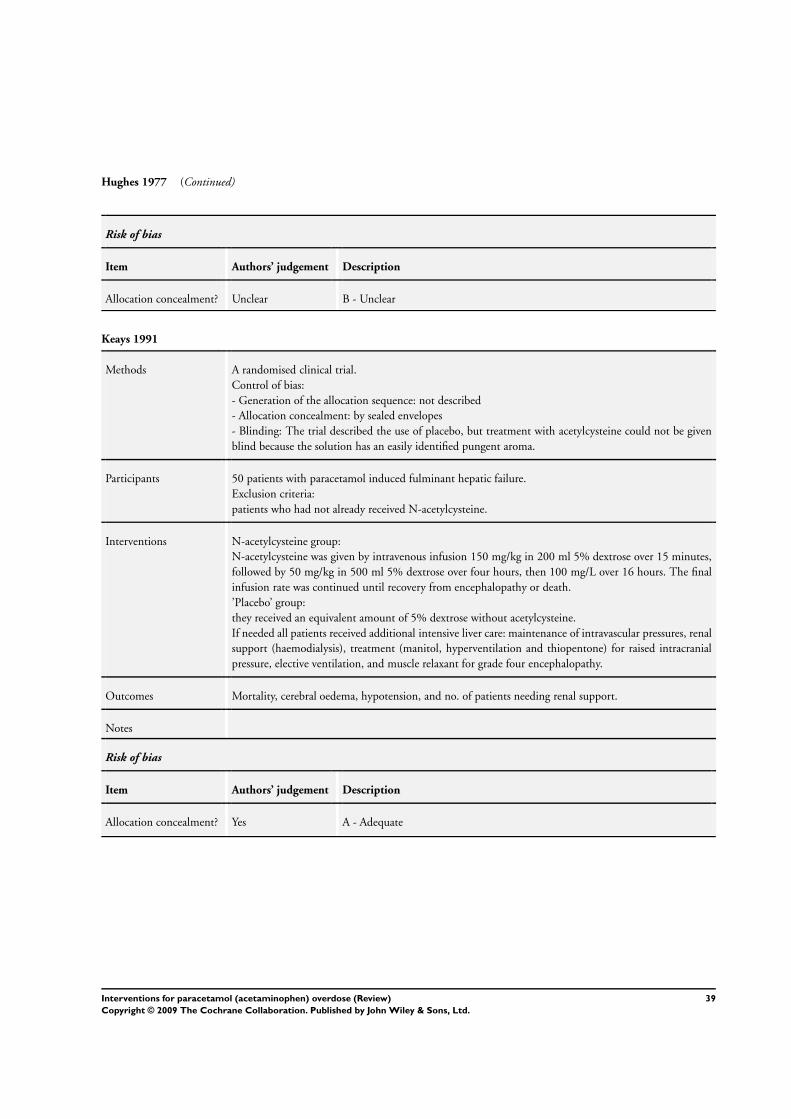
Hughes 1977 (Continued)
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Keays 1991
Methods A randomised clinical trial.
Control of bias:
- Generation of the allocation sequence: not described
- Allocation concealment: by sealed envelopes
- Blinding: The trial described the use of placebo, but treatment with acetylcysteine could not be given
blind because the solution has an easily identified pungent aroma.
Participants 50 patients with paracetamol induced fulminant hepatic failure.
Exclusion criteria:
patients who had not already received N-acetylcysteine.
Interventions N-acetylcysteine group:
N-acetylcysteine was given by intravenous infusion 150 mg/kg in 200 ml 5% dextrose over 15 minutes,
followed by 50 mg/kg in 500 ml 5% dextrose over four hours, then 100 mg/L over 16 hours. The final
infusion rate was continued until recovery from encephalopathy or death.
’Placebo’ group:
they received an equivalent amount of 5% dextrose without acetylcysteine.
If needed all patients received additional intensive liver care: maintenance of intravascular pressures, renal
support (haemodialysis), treatment (manitol, hyperventilation and thiopentone) for raised intracranial
pressure, elective ventilation, and muscle relaxant for grade four encephalopathy.
Outcomes Mortality, cerebral oedema, hypotension, and no. of patients needing renal support.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
39Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
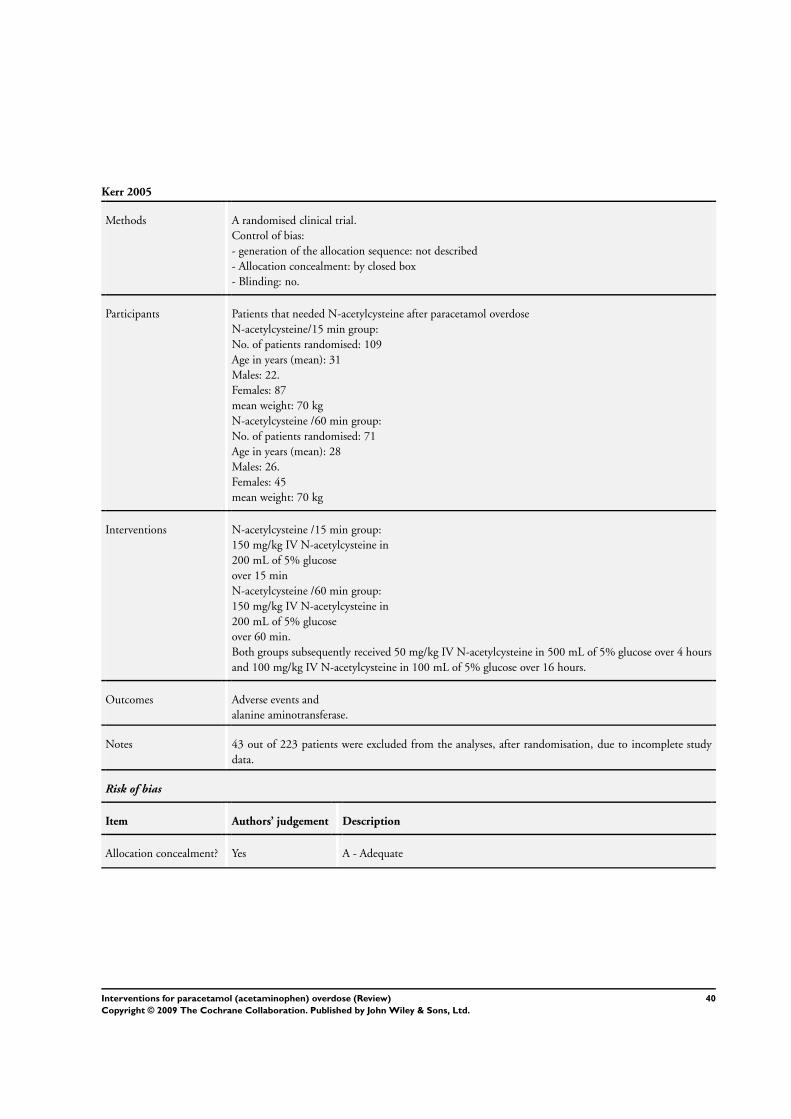
Kerr 2005
Methods A randomised clinical trial.
Control of bias:
- generation of the allocation sequence: not described
- Allocation concealment: by closed box
- Blinding: no.
Participants Patients that needed N-acetylcysteine after paracetamol overdose
N-acetylcysteine/15 min group:
No. of patients randomised: 109
Age in years (mean): 31
Males: 22.
Females: 87
mean weight: 70 kg
N-acetylcysteine /60 min group:
No. of patients randomised: 71
Age in years (mean): 28
Males: 26.
Females: 45
mean weight: 70 kg
Interventions N-acetylcysteine /15 min group:
150 mg/kg IV N-acetylcysteine in
200 mL of 5% glucose
over 15 min
N-acetylcysteine /60 min group:
150 mg/kg IV N-acetylcysteine in
200 mL of 5% glucose
over 60 min.
Both groups subsequently received 50 mg/kg IV N-acetylcysteine in 500 mL of 5% glucose over 4 hours
and 100 mg/kg IV N-acetylcysteine in 100 mL of 5% glucose over 16 hours.
Outcomes Adverse events and
alanine aminotransferase.
Notes 43 out of 223 patients were excluded from the analyses, after randomisation, due to incomplete study
data.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
40Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kirk 1991
Methods A retrospective observational study.
Participants 123 children younger than six years old that ingested more than 150 mg/kg of paracetamol.
Interventions Group 1:
ipecac at home within one hour.
Group 2:
Activated charcoal within two hours at emergency department.
Group 3:
No intervention.
Outcomes Plasma paracetamol.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Larson 2005
Methods A retrospective observational study.
Participants 40 patients with fulminant hepatic failure and listed for transplantation according to Kings College
Criteria.
Interventions group 1:
Liver transplantation
group 2
No intervention
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
41Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
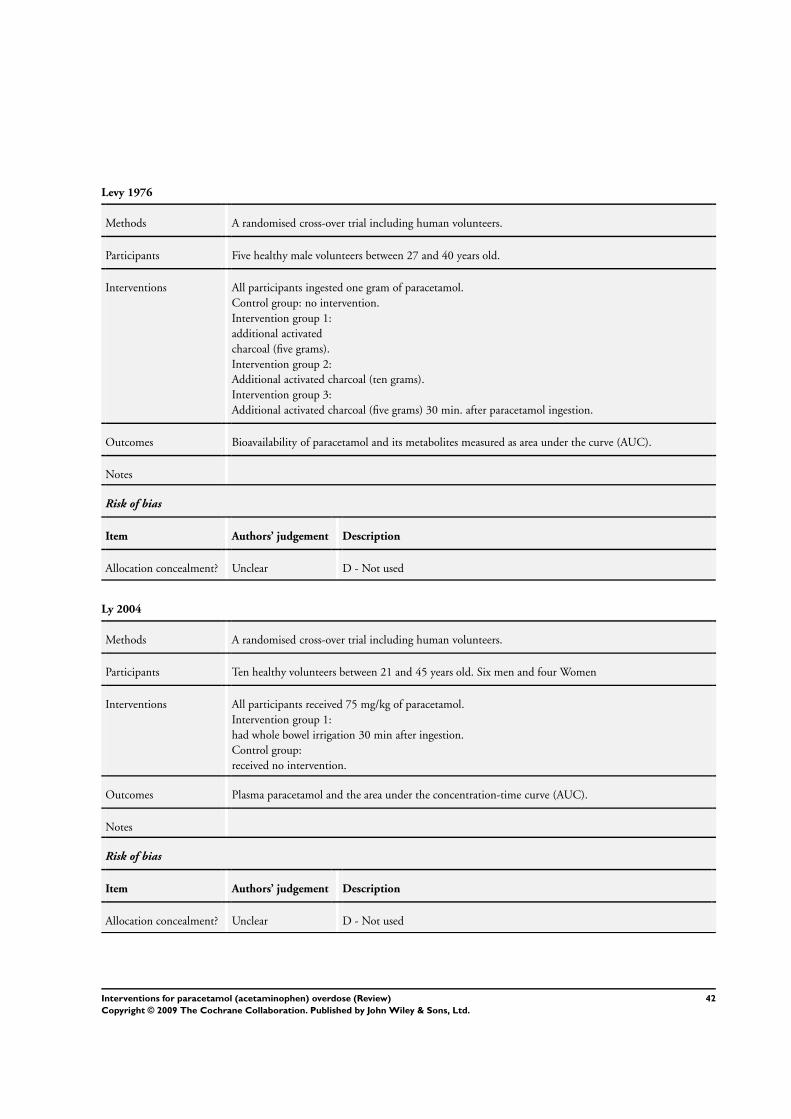
Levy 1976
Methods A randomised cross-over trial including human volunteers.
Participants Five healthy male volunteers between 27 and 40 years old.
Interventions All participants ingested one gram of paracetamol.
Control group: no intervention.
Intervention group 1:
additional activated
charcoal (five grams).
Intervention group 2:
Additional activated charcoal (ten grams).
Intervention group 3:
Additional activated charcoal (five grams) 30 min. after paracetamol ingestion.
Outcomes Bioavailability of paracetamol and its metabolites measured as area under the curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Ly 2004
Methods A randomised cross-over trial including human volunteers.
Participants Ten healthy volunteers between 21 and 45 years old. Six men and four Women
Interventions All participants received 75 mg/kg of paracetamol.
Intervention group 1:
had whole bowel irrigation 30 min after ingestion.
Control group:
received no intervention.
Outcomes Plasma paracetamol and the area under the concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
42Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

McNamara 1988
Methods A randomised cross-over trial including human volunteers.
Participants Ten healthy male volunteers 18 to 35 years old.
Interventions All participants received three grams of paracetamol.
Intervention group 1:
received 50 g of activated charcoal per 70% sorbitol solution (30 g activated charcoal/110 g sorbitol) one
hour after ingestion.
Intervention group 2:
received 50 grams of activated charcoal one hour after ingestion.
Control group 3:
received no intervention.
Outcomes Plasma paracetamol and the area under the concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
McNamara 1989
Methods A randomised cross-over trial including human volunteers.
Participants Ten healthy male volunteers 18 to 35 years old.
Interventions All received three grams of paracetamol.
Intervention group 1:
received 30 ml syrup of ipecac one hour after ingestion.
Intervention group 2:
received 50 grams of activated charcoal one hour after ingestion.
Control group:
received no intervention.
Outcomes Plasma paracetamol and the area under the concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
43Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

McNamara 1989 (Continued)
Allocation concealment? Unclear D - Not used
Montoya-Cabrera 1999
Methods A prospective observational study.
Participants 14 paediatric patients with a paracetamol overdose.
Interventions Control group:
received N-acetylcysteine.
Intervention group:
received N-acetylcysteine and activated charcoal.
Outcomes ACT-disappearance, half-life elimination of paracetamol, and exogenous body clearance of paracetamol.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Mutimer 1994
Methods A retrospective observational study.
Participants 17 patients eligible for liver transplantation due to paracetamol overdose.
Transplant criteria were serum creatinine > 300 µmol/L, prothrombin time of > 100 s, and grade 3 or 4
encephalopathy in patients with normal pH, or the single finding of pH < 7.3.
Interventions Intervention group:
received liver transplantation.
Control group: received only supportive treatment.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
44Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
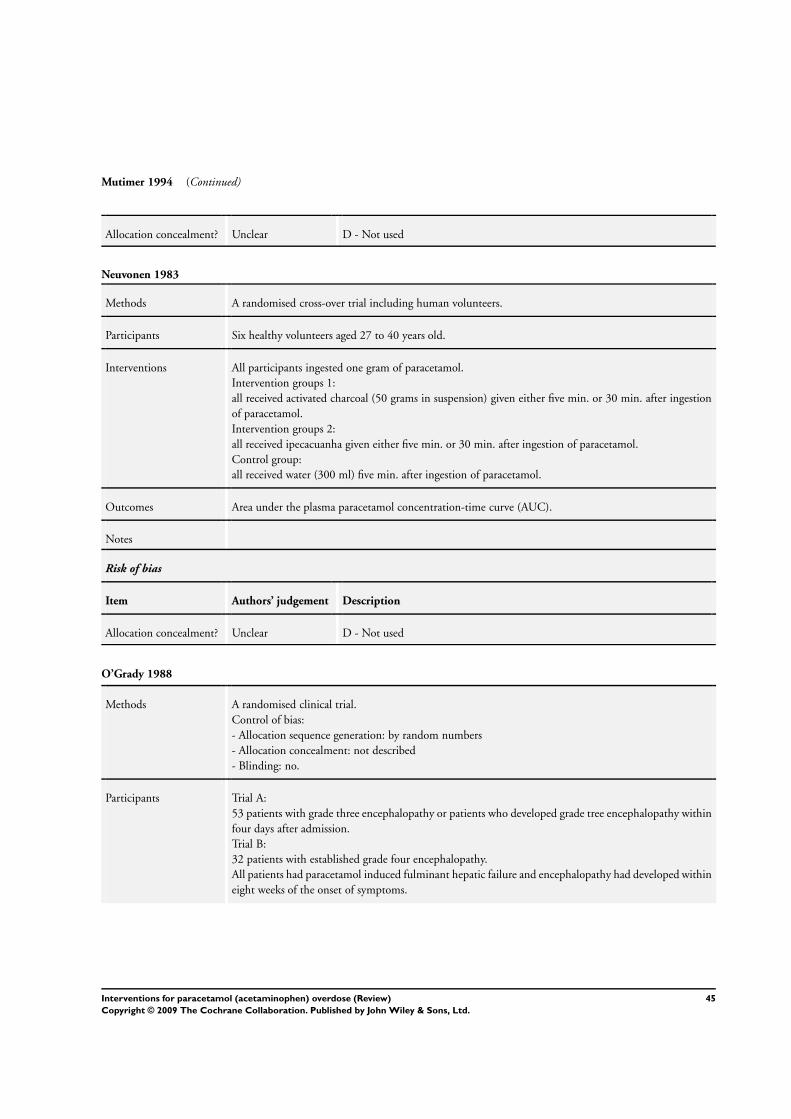
Mutimer 1994 (Continued)
Allocation concealment? Unclear D - Not used
Neuvonen 1983
Methods A randomised cross-over trial including human volunteers.
Participants Six healthy volunteers aged 27 to 40 years old.
Interventions All participants ingested one gram of paracetamol.
Intervention groups 1:
all received activated charcoal (50 grams in suspension) given either five min. or 30 min. after ingestion
of paracetamol.
Intervention groups 2:
all received ipecacuanha given either five min. or 30 min. after ingestion of paracetamol.
Control group:
all received water (300 ml) five min. after ingestion of paracetamol.
Outcomes Area under the plasma paracetamol concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
O’Grady 1988
Methods A randomised clinical trial.
Control of bias:
- Allocation sequence generation: by random numbers
- Allocation concealment: not described
- Blinding: no.
Participants Trial A:
53 patients with grade three encephalopathy or patients who developed grade tree encephalopathy within
four days after admission.
Trial B:
32 patients with established grade four encephalopathy.
All patients had paracetamol induced fulminant hepatic failure and encephalopathy had developed within
eight weeks of the onset of symptoms.
45Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

O’Grady 1988 (Continued)
Interventions Charcoal haemoperfusion:
The Smith and Nephew and the Gambro charcoal column was used. Blood flow was maintained at 150-
200 ml/min. Initial bolus of 5000 U of heparin was given and a continuous infusion to maintain the
clotting times (hemochron) between 250 and 300 seconds.
Trial A:
patients were randomised to five hours or ten hours of daily haemoperfusion.
Trial B:
patients were randomised to 10 hours of daily haemoperfusion or only supportive treatment.
Charcoal haemoperfusion intervention was continued until the patients regained consciousness or until
the onset of irreversible brainstem damage or preterminal refractory hypotension. Cerebral edema was
treated with manitol. Haemodialysis was performed if s-creatinine > 400 µmol/l, arterial pH < 7.20,
or fluid overload. Hypovolemia, haemorrhage, respiratory dysfunction, and blood glucose level were all
treated. All patients received cimetidine and lactulose.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? No C - Inadequate
O’Grady 1991
Methods A prospective observational study.
Participants 14 patients eligible for liver transplantation due to paracetamol overdose.
Transplant criteria were serum creatinine > 300 µmol/L, prothrombin time of > 100 s, and grade 3 or 4
encephalopathy in patients with normal pH, or the single finding of pH < 7.3.
14 were registered for liver transplantation and six of these patients underwent transplantation.
Interventions Intervention group:
received liver transplantation.
Control group:
received only supportive treatment.
Outcomes Mortality.
Notes
Risk of bias
46Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

O’Grady 1991 (Continued)
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Parker 1990
Methods A prospective observational study.
Participants 20 patients presenting between 12 and 24 hours after an overdose of paracetamol. All had a plasma
paracetamol concentration above the 200 risk line.
Interventions All patients received N-acetylcysteine (300 mg/kg in 20 hours). Gastric lavage was performed in five
patients.
Control group:
none.
Outcomes Mortality, aspartate aminotransferase, bilirubin, and prothrombin time.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Prescott 1976
Methods A retrospective observational study.
Participants 121 patients with paracetamol overdose. all patients receiving antidotes had plasma paracetamol level
above the 150 risk-line.
Interventions Intervention group 1:
received cysteamine given intravenously as an initial loading dose (2.0 g) followed by an infusion of 1.6
g for 20 hours.
Intervention group 2:
received methionine given intravenously as an loading dose (2.0 g) followed by 15.0 g infused over 20
hours.
Control group:
received only supportive treatment.
Outcomes Aspartate aminotransferase, alanine aminotransferase, bilirubin, and prothrombin time ratio.
47Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
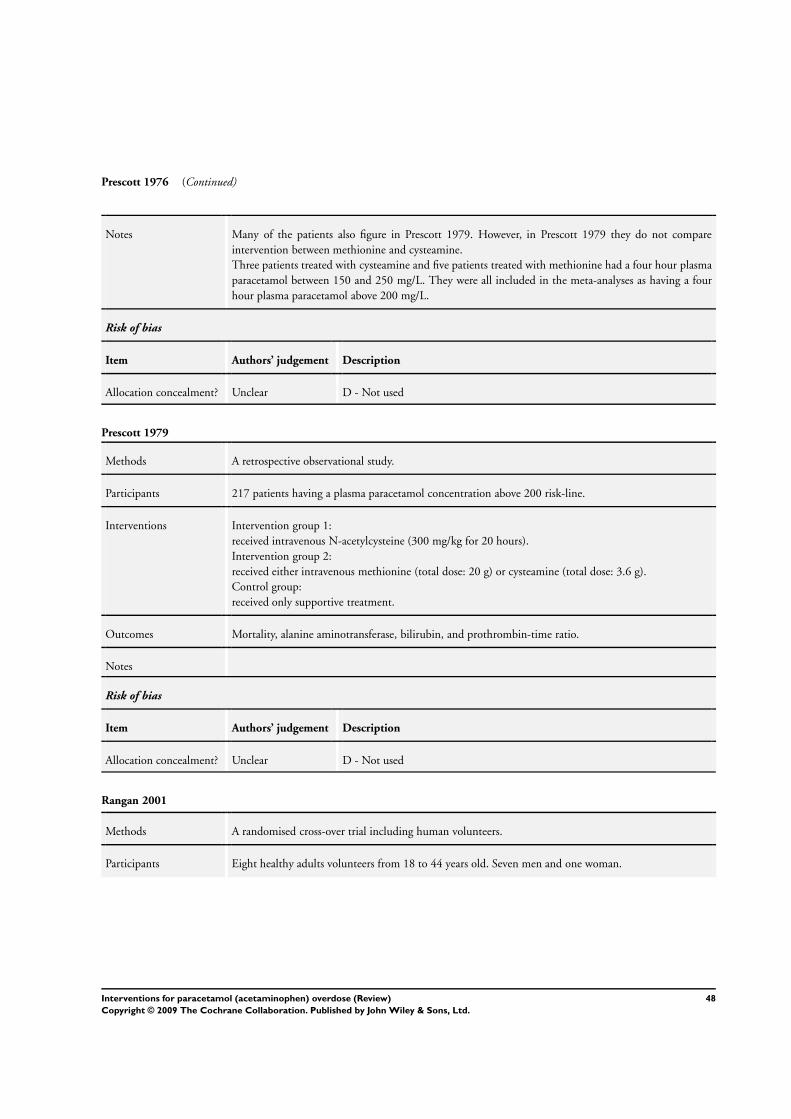
Prescott 1976 (Continued)
Notes Many of the patients also figure in Prescott 1979. However, in Prescott 1979 they do not compare
intervention between methionine and cysteamine.
Three patients treated with cysteamine and five patients treated with methionine had a four hour plasma
paracetamol between 150 and 250 mg/L. They were all included in the meta-analyses as having a four
hour plasma paracetamol above 200 mg/L.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Prescott 1979
Methods A retrospective observational study.
Participants 217 patients having a plasma paracetamol concentration above 200 risk-line.
Interventions Intervention group 1:
received intravenous N-acetylcysteine (300 mg/kg for 20 hours).
Intervention group 2:
received either intravenous methionine (total dose: 20 g) or cysteamine (total dose: 3.6 g).
Control group:
received only supportive treatment.
Outcomes Mortality, alanine aminotransferase, bilirubin, and prothrombin-time ratio.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Rangan 2001
Methods A randomised cross-over trial including human volunteers.
Participants Eight healthy adults volunteers from 18 to 44 years old. Seven men and one woman.
48Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
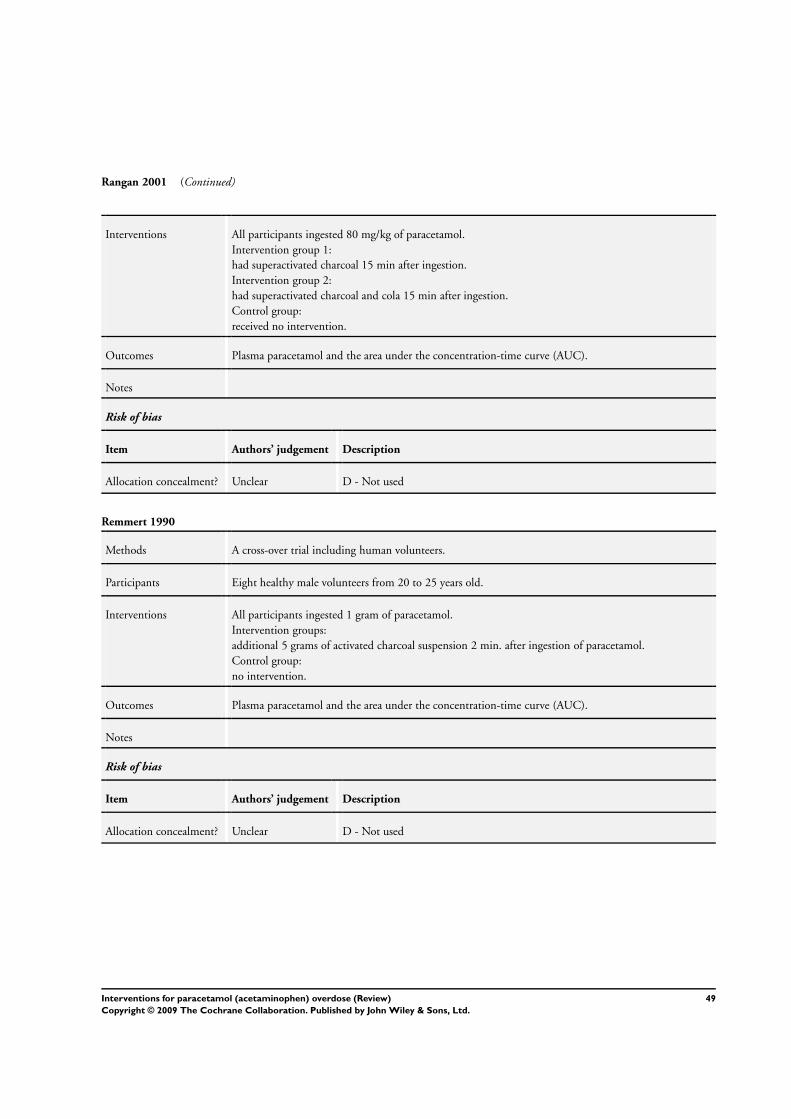
Rangan 2001 (Continued)
Interventions All participants ingested 80 mg/kg of paracetamol.
Intervention group 1:
had superactivated charcoal 15 min after ingestion.
Intervention group 2:
had superactivated charcoal and cola 15 min after ingestion.
Control group:
received no intervention.
Outcomes Plasma paracetamol and the area under the concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Remmert 1990
Methods A cross-over trial including human volunteers.
Participants Eight healthy male volunteers from 20 to 25 years old.
Interventions All participants ingested 1 gram of paracetamol.
Intervention groups:
additional 5 grams of activated charcoal suspension 2 min. after ingestion of paracetamol.
Control group:
no intervention.
Outcomes Plasma paracetamol and the area under the concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
49Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rose 1991
Methods A randomised cross-over trial including human volunteers.
Participants Ten healthy, adult male volunteers from 21 to 39 years old.
Interventions All participants ingested five grams of paracetamol
Intervention groups:
additional 30 grams of activated charcoal either 15, 30, or 120 min. after ingestion of paracetamol.
Control group:
no intervention
Outcomes Bioavailability of paracetamol and its metabolites measured as area under the curve (AUC).
Notes We only included the trial with the maximal time between paracetamol ingestion and activated charcoal
in the meta-analysis because this is most relevant for the clinical situation.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Saincher 1997
Methods A randomised cross-over trial including human volunteers.
Participants Ten healthy adult volunteers.
Interventions All participants ingested 3.9 g of paracetamol.
Intervention groups:
had ipecac 5, 30, or 60 min after ingestion.
Control group:
received no intervention.
Outcomes Plasma paracetamol and area under the concentration-time curve (AUC).
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
50Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
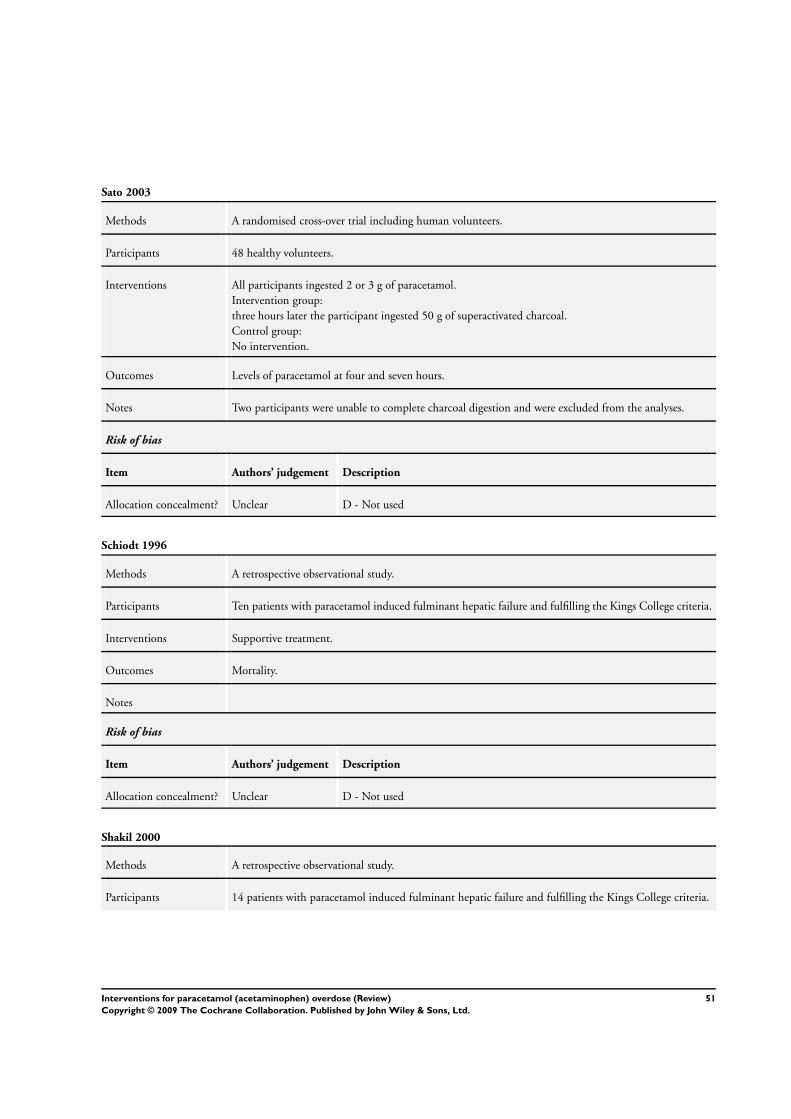
Sato 2003
Methods A randomised cross-over trial including human volunteers.
Participants 48 healthy volunteers.
Interventions All participants ingested 2 or 3 g of paracetamol.
Intervention group:
three hours later the participant ingested 50 g of superactivated charcoal.
Control group:
No intervention.
Outcomes Levels of paracetamol at four and seven hours.
Notes Two participants were unable to complete charcoal digestion and were excluded from the analyses.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Schiodt 1996
Methods A retrospective observational study.
Participants Ten patients with paracetamol induced fulminant hepatic failure and fulfilling the Kings College criteria.
Interventions Supportive treatment.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Shakil 2000
Methods A retrospective observational study.
Participants 14 patients with paracetamol induced fulminant hepatic failure and fulfilling the Kings College criteria.
51Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Shakil 2000 (Continued)
Interventions Supportive treatment.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Silk 1978
Methods A retrospective observational study.
Participants Patients with fulminant hepatic failure and grade 4 coma.
Interventions All patients received glucose, lactulose, neomycin, magnesium, and vitamins. Hypotension was treated
with fresh frozen plasma.
Haemoperfusion:
the chromatography columns were filled with 220 - 300 grams of charcoal, produced by Smith and
Nephew Research Ltd. Blood from an arterio-venous shunt was pumped through the column at a rate of
between 100 and 300 ml/min, and the patients were heparinised so as to maintain the Lee-White clotting
time at between 10 and 20 min.
Outcomes Mortality.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Smilkstein 1988
Methods A prospective observational study.
Participants 2540 patients with paracetamol overdose.
2023 patients had a plasma paracetamol concentration above 200 risk-line.
52Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
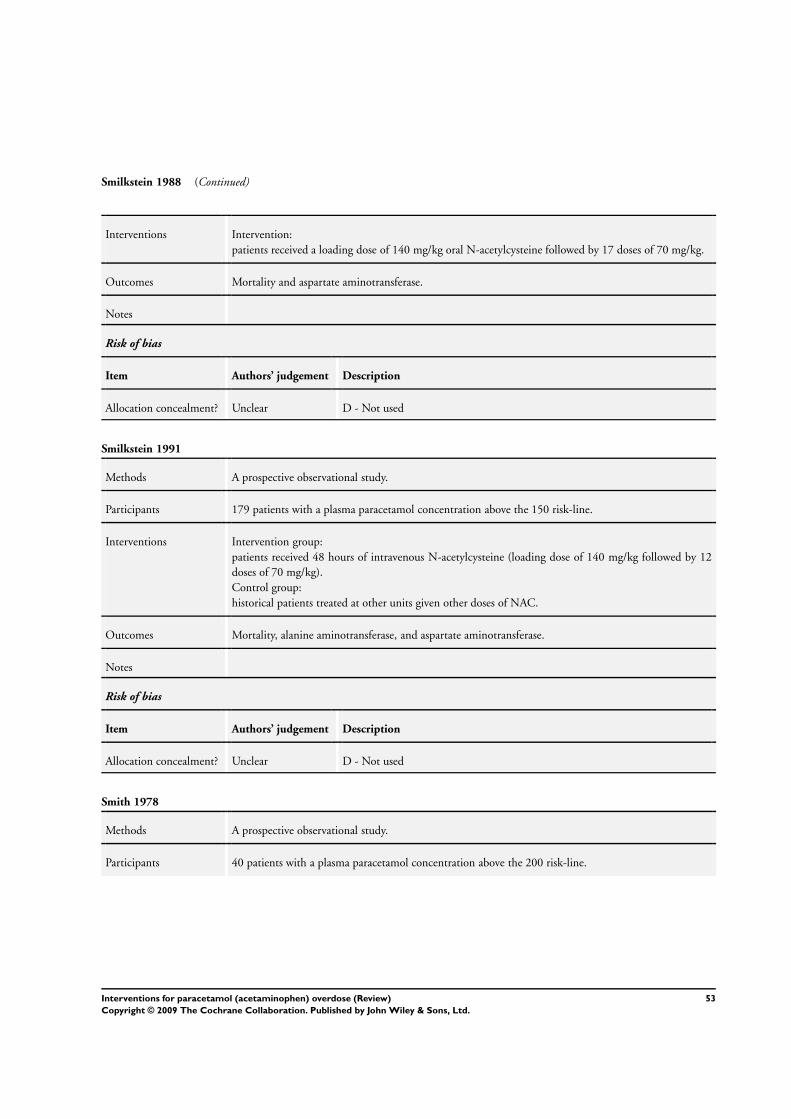
Smilkstein 1988 (Continued)
Interventions Intervention:
patients received a loading dose of 140 mg/kg oral N-acetylcysteine followed by 17 doses of 70 mg/kg.
Outcomes Mortality and aspartate aminotransferase.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Smilkstein 1991
Methods A prospective observational study.
Participants 179 patients with a plasma paracetamol concentration above the 150 risk-line.
Interventions Intervention group:
patients received 48 hours of intravenous N-acetylcysteine (loading dose of 140 mg/kg followed by 12
doses of 70 mg/kg).
Control group:
historical patients treated at other units given other doses of NAC.
Outcomes Mortality, alanine aminotransferase, and aspartate aminotransferase.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Smith 1978
Methods A prospective observational study.
Participants 40 patients with a plasma paracetamol concentration above the 200 risk-line.
53Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
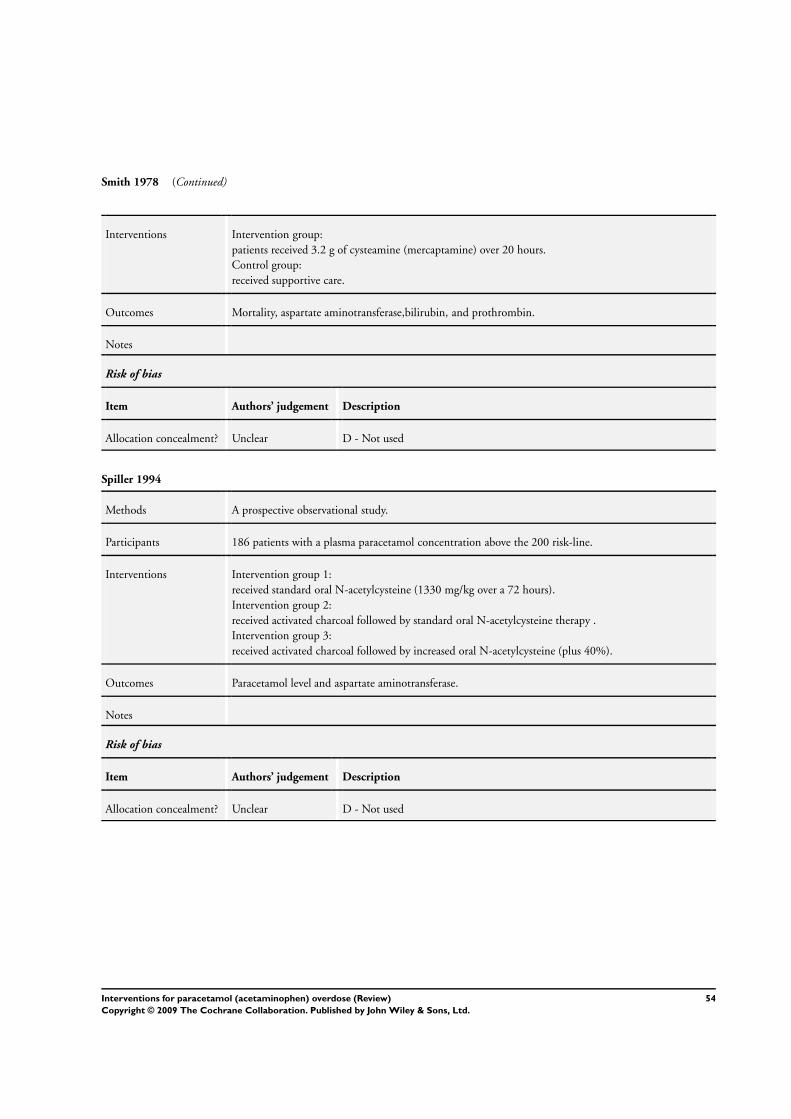
Smith 1978 (Continued)
Interventions Intervention group:
patients received 3.2 g of cysteamine (mercaptamine) over 20 hours.
Control group:
received supportive care.
Outcomes Mortality, aspartate aminotransferase,bilirubin, and prothrombin.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Spiller 1994
Methods A prospective observational study.
Participants 186 patients with a plasma paracetamol concentration above the 200 risk-line.
Interventions Intervention group 1:
received standard oral N-acetylcysteine (1330 mg/kg over a 72 hours).
Intervention group 2:
received activated charcoal followed by standard oral N-acetylcysteine therapy .
Intervention group 3:
received activated charcoal followed by increased oral N-acetylcysteine (plus 40%).
Outcomes Paracetamol level and aspartate aminotransferase.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
54Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Underhill 1990
Methods A randomised clinical trial.
Control of bias:
- Generation of the allocation sequence: not described
- Allocation concealment: not described
- Blinding: no.
The 12 patients taking additional drugs were spread throughout the treatment groups and the statistical
results were similar when these patients were excluded.
Participants 60 patients aged 16 and over who had ingested five or more grams of paracetamol within four hours of
admission.
Exclusion criteria:
not reported.
Interventions Intervention group 1:
gastric lavage was carried out with a 36 FG tube.
Intervention group 2:
administration of activated charcoal was carried out with Carbomix to drug ratio of 10:1.
Intervention group 3:
ipecacuanha syrup 30 ml. This was repeated after 30 min. if there was no response.
Control group:
no intervention to limit absorption. (This group was treated in a different hospital in Derby).
Plasma paracetamol levels were measured on samples taken from an indwelling cannula prior to any
treatment, and following treatment at 60, 90, 150 minutes after the first sample.
Group 4 (no treatment) was stopped for ethical reasons after only five patients.
Outcomes Fall in plasma paracetamol concentration versus time.
Notes In the latter group, the plasma paracetamol concentration increased during treatment in 4/5 patients and
lead to cessation of the supportive treatment group.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Vale 1981
Methods A retrospective observational study.
Participants 132 patients with a plasma paracetamol concentration above a risk-line from 220 mg/L at four hours and
70 mg/L at 12 hours.
Interventions Intervention:
each patient received four doses of 2.5 gram of oral methionine over 12 hours.
55Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Vale 1981 (Continued)
Outcomes Mortality, hepatotoxicity and serum creatinine.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Woo 2000
Methods A retrospective observational study.
Participants 75 patients with a plasma acetaminophen concentration above the a possible risk line from 140 mgL at 4
hours to 50 mg/l at 10 hours.
Interventions Intervention:
140 mg/kg of oral N-acetylcysteine as a loading dose followed by 70 mg/kg every four hours until the
serum paracetamol level was zero.
Outcomes Mortality, aspartate aminotransferase, and alanine aminotransferase.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
Yeates 2000
Methods A randomised cross-over trial including human volunteers.
Participants Ten healthy volunteers between 20 to 41 years old. Six males and four females.
Interventions All participants ingested three grams of paracetamol.
Intervention group:
Additional 50 grams of activated charcoal 120 or 240 min after ingestion.
Control group:
no intervention.
Outcomes Area under the plasma paracetamol concentration-time curve (AUC).
56Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Yeates 2000 (Continued)
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear D - Not used
AUC: area under the plasma paracetamol concentration-time curve
g: grammes
h: hours
IU: international units
kg: kilogrammes
L: litre
mg: milligrammes
min.: minutes
ml: millilitre
SD: standard deviation
SE: standard error
µ: micro
Characteristics of excluded studies [ordered by study ID]
Alander 2000 Did not report hepatotoxicity as ALT > 1000 IU/L as defined in out protocol. Instead reported hepatotoxicity
as two times the normal upper limit.
Beckett 1989 Case series involving less than 20 patients.
Beckett 1990 Case series involving less than 20 patients.
Bond 1999 Included less than 20 patients ingesting single dose paracetamol.
Bray 1991 Not clearly consecutive, unreferred patients.
Brotodihardjo 1992 Contained insufficient information on hepatotoxicity, ingestion-treatment interval, and plasma paracetamol
concentration of each patient.
Chamberlain 1993 Assessed activated charcoal in human volunteers ingesting 3 g of paracetamol. However, the two comparison
groups ingested different doses on NAC.
Chan 1993 Case series involving less than 20 patients.
57Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Chan 1994 Case series involving less than 20 patients.
Chan 1996 Case-control study.
Dordoni 1973 Not randomised. Study including human volunteers.
Gee 1998 No information on the time between ingestion and treatment with activated charcoal.
James 2002 A retrospective observational study. Contained insufficient information on hepatotoxicity, ingestion-treatment
interval, and NAC treatment protocol.
Levy 1985 A retrospective observational study. Contained insufficient information on hepatotoxicity, ingestion-treatment
interval, plasma paracetamol concentration, and NAC treatment protocol.
Makin 1995 Regarding N-acetylcysteine treatment:
- Selected patients transferred from other hospitals in high risk of liver failure..
Regarding transplantation:
- No clear data on mortality in patients listed for transplantation without a transplant.
Included the same patients as Bernal 1998 and O’Grady 1991 which are included.
Oh 1980 Case series involving less than 20 patients.
Oren 1992 A retrospective observational study. Contained insufficient information on hepatotoxicity, ingestion-treatment
interval, plasma paracetamol concentration, and N-acetylcysteine treatment protocol.
Perry 1998 Not clearly consecutive, unreferred patients.
Prescott 1989 Case series involving less than 20 patients.
Read 1986 Not clearly consecutive, unreferred patients. Less than 20 patients had paracetamol above the 200-line.
Riggs 1989 Not clearly consecutive, unreferred patients.
Rivera-Penera 1997 Did not clearly define transplantation criteria.
Schiodt 1997 A retrospective observational study. Contained insufficient information on hepatotoxicity and, ingestion-
treatment interval.
Schmidt 2002a Not clearly consecutive, unreferred patients.
Singer 1995 Not clearly consecutive, unreferred patients.
58Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Charcoal haemoperfusion versus no intervention (randomised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 16 Peto Odds Ratio (Peto, Fixed, 95% CI) 7.39 [0.15, 372.38]
Comparison 2. Cysteamine versus no intervention (randomised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 2 65 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.53 [0.05, 5.22]
2 Hepatotoxicity (aspartate
aminotransferase > 1000 IU/L)
2 65 Odds Ratio (M-H, Fixed, 95% CI) 0.09 [0.02, 0.34]
Comparison 3. Cysteamine versus dimercaprol (randomised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 52 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.14 [0.00, 6.82]
2 Maximum alanine
aminotransferase (IU/L)
1 52 Mean Difference (IV, Fixed, 95% CI) -32.0 [-512.90,
448.90]
Comparison 4. Cysteamine versus methionine (randomised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 27 Peto Odds Ratio (Peto, Fixed, 95% CI) Not estimable
2 Hepatotoxicity (aspartate
aminotransferase > 1000 U/L)
1 27 Odds Ratio (M-H, Fixed, 95% CI) 0.92 [0.05, 16.46]
59Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 5. Methionine and supportive treatment versus supportive treatment (randomised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 26 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.14 [0.00, 6.82]
2 Hepatotoxicity (aspartate
aminotransferase > 1000 U/L)
1 26 Odds Ratio (M-H, Fixed, 95% CI) 0.07 [0.01, 0.72]
Comparison 6. Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine (randomised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 180 Peto Odds Ratio (Peto, Fixed, 95% CI) Not estimable
2 Hepatotoxicity 1 175 Odds Ratio (M-H, Fixed, 95% CI) 0.75 [0.22, 2.56]
3 Any adverse event 1 180 Odds Ratio (M-H, Fixed, 95% CI) 1.98 [1.04, 3.77]
Comparison 7. Charcoal haemoperfusion in patients with fulminant hepatic failure (randomised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 32 Peto Odds Ratio (Peto, Fixed, 95% CI) 1.64 [0.41, 6.47]
Comparison 8. 5 h versus 10 h of charcoal haemoperfusion in patients with fulminant hepatic failure (randomised
trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 53 Peto Odds Ratio (Peto, Fixed, 95% CI) 1.30 [0.44, 3.81]
60Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
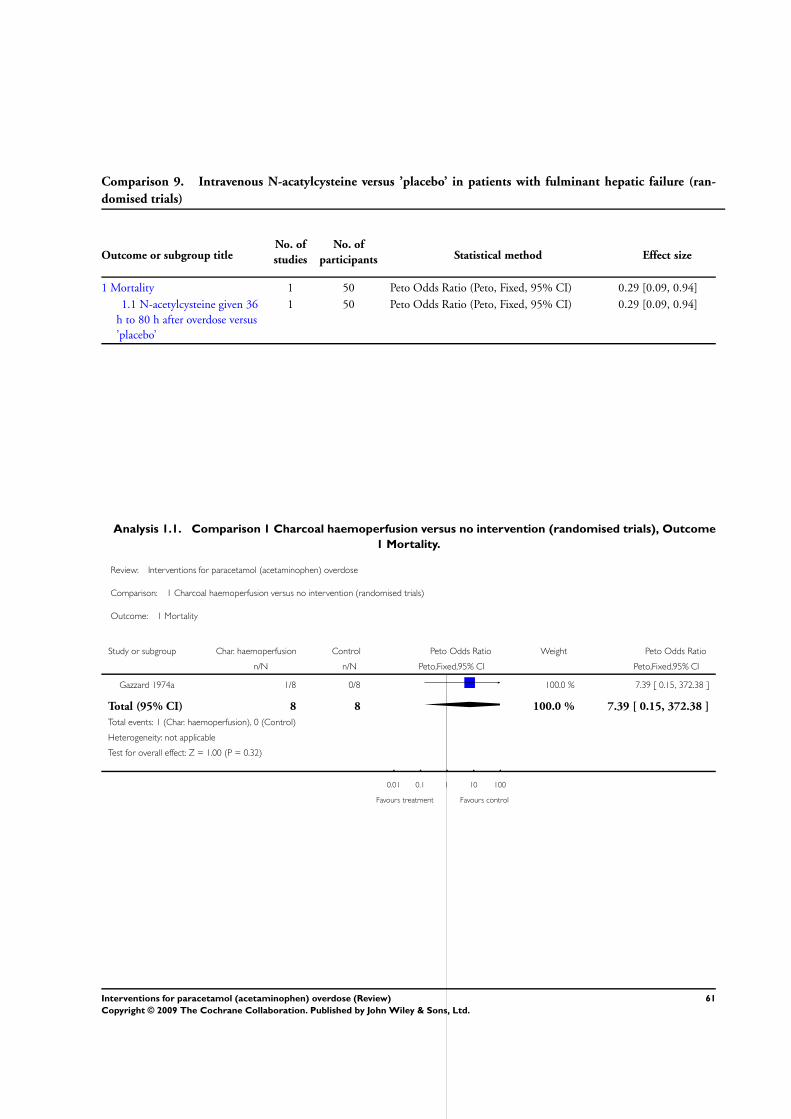
Comparison 9. Intravenous N-acatylcysteine versus ’placebo’ in patients with fulminant hepatic failure (ran-
domised trials)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mortality 1 50 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.29 [0.09, 0.94]
1.1 N-acetylcysteine given 36
h to 80 h after overdose versus
’placebo’
1 50 Peto Odds Ratio (Peto, Fixed, 95% CI) 0.29 [0.09, 0.94]
Analysis 1.1. Comparison 1 Charcoal haemoperfusion versus no intervention (randomised trials), Outcome
1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 1 Charcoal haemoperfusion versus no intervention (randomised trials)
Outcome: 1 Mortality
Study or subgroup Char. haemoperfusion Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Gazzard 1974a 1/8 0/8 100.0 % 7.39 [ 0.15, 372.38 ]
Total (95% CI) 8 8 100.0 % 7.39 [ 0.15, 372.38 ]
Total events: 1 (Char. haemoperfusion), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.00 (P = 0.32)
0.01 0.1 1 10 100
Favours treatment Favours control
61Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.1. Comparison 2 Cysteamine versus no intervention (randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 2 Cysteamine versus no intervention (randomised trials)
Outcome: 1 Mortality
Study or subgroup Cysteamine Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Douglas 1976 1/18 1/20 66.0 % 1.11 [ 0.07, 18.59 ]
Hamlyn 1981 0/14 1/13 34.0 % 0.13 [ 0.00, 6.33 ]
Total (95% CI) 32 33 100.0 % 0.53 [ 0.05, 5.22 ]
Total events: 1 (Cysteamine), 2 (Control)
Heterogeneity: Chi2 = 0.79, df = 1 (P = 0.37); I2 =0.0%
Test for overall effect: Z = 0.54 (P = 0.59)
0.01 0.1 1 10 100
Favours cysteamine Favours control
Analysis 2.2. Comparison 2 Cysteamine versus no intervention (randomised trials), Outcome 2
Hepatotoxicity (aspartate aminotransferase > 1000 IU/L).
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 2 Cysteamine versus no intervention (randomised trials)
Outcome: 2 Hepatotoxicity (aspartate aminotransferase > 1000 IU/L)
Study or subgroup Cysteamine Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Douglas 1976 2/18 11/20 57.9 % 0.10 [ 0.02, 0.57 ]
Hamlyn 1981 1/14 7/13 42.1 % 0.07 [ 0.01, 0.66 ]
Total (95% CI) 32 33 100.0 % 0.09 [ 0.02, 0.34 ]
Total events: 3 (Cysteamine), 18 (Control)
Heterogeneity: Chi2 = 0.09, df = 1 (P = 0.76); I2 =0.0%
Test for overall effect: Z = 3.49 (P = 0.00049)
0.001 0.01 0.1 1 10 100 1000
Favours cysteamine Favours control
62Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.1. Comparison 3 Cysteamine versus dimercaprol (randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 3 Cysteamine versus dimercaprol (randomised trials)
Outcome: 1 Mortality
Study or subgroup Cysteamine Dimercaprol Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Hughes 1977 0/26 1/26 100.0 % 0.14 [ 0.00, 6.82 ]
Total (95% CI) 26 26 100.0 % 0.14 [ 0.00, 6.82 ]
Total events: 0 (Cysteamine), 1 (Dimercaprol)
Heterogeneity: not applicable
Test for overall effect: Z = 1.00 (P = 0.32)
0.01 0.1 1 10 100
Favours cysteamine Favours dimercaprol
Analysis 3.2. Comparison 3 Cysteamine versus dimercaprol (randomised trials), Outcome 2 Maximum
alanine aminotransferase (IU/L).
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 3 Cysteamine versus dimercaprol (randomised trials)
Outcome: 2 Maximum alanine aminotransferase (IU/L)
Study or subgroup Cysteamine Dimercaprol Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Hughes 1977 26 722 (902) 26 754 (867) 100.0 % -32.00 [ -512.90, 448.90 ]
Total (95% CI) 26 26 100.0 % -32.00 [ -512.90, 448.90 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.13 (P = 0.90)
-1000 -500 0 500 1000
Favours cysteamine Favours dimercaprol
63Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.1. Comparison 4 Cysteamine versus methionine (randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 4 Cysteamine versus methionine (randomised trials)
Outcome: 1 Mortality
Study or subgroup Cysteamine Methioninel Peto Odds Ratio Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Hamlyn 1981 0/13 0/14 0.0 [ 0.0, 0.0 ]
Total (95% CI) 13 14 0.0 [ 0.0, 0.0 ]
Total events: 0 (Cysteamine), 0 (Methioninel)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P < 0.00001)
0.1 0.2 0.5 1 2 5 10
Favours cysteamine Favours methionine
Analysis 4.2. Comparison 4 Cysteamine versus methionine (randomised trials), Outcome 2 Hepatotoxicity
(aspartate aminotransferase > 1000 U/L).
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 4 Cysteamine versus methionine (randomised trials)
Outcome: 2 Hepatotoxicity (aspartate aminotransferase > 1000 U/L)
Study or subgroup Cysteamine Methionine Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Hamlyn 1981 1/14 1/13 100.0 % 0.92 [ 0.05, 16.46 ]
Total (95% CI) 14 13 100.0 % 0.92 [ 0.05, 16.46 ]
Total events: 1 (Cysteamine), 1 (Methionine)
Heterogeneity: not applicable
Test for overall effect: Z = 0.05 (P = 0.96)
0.001 0.01 0.1 1 10 100 1000
Favours cysteamine Favours methionine
64Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
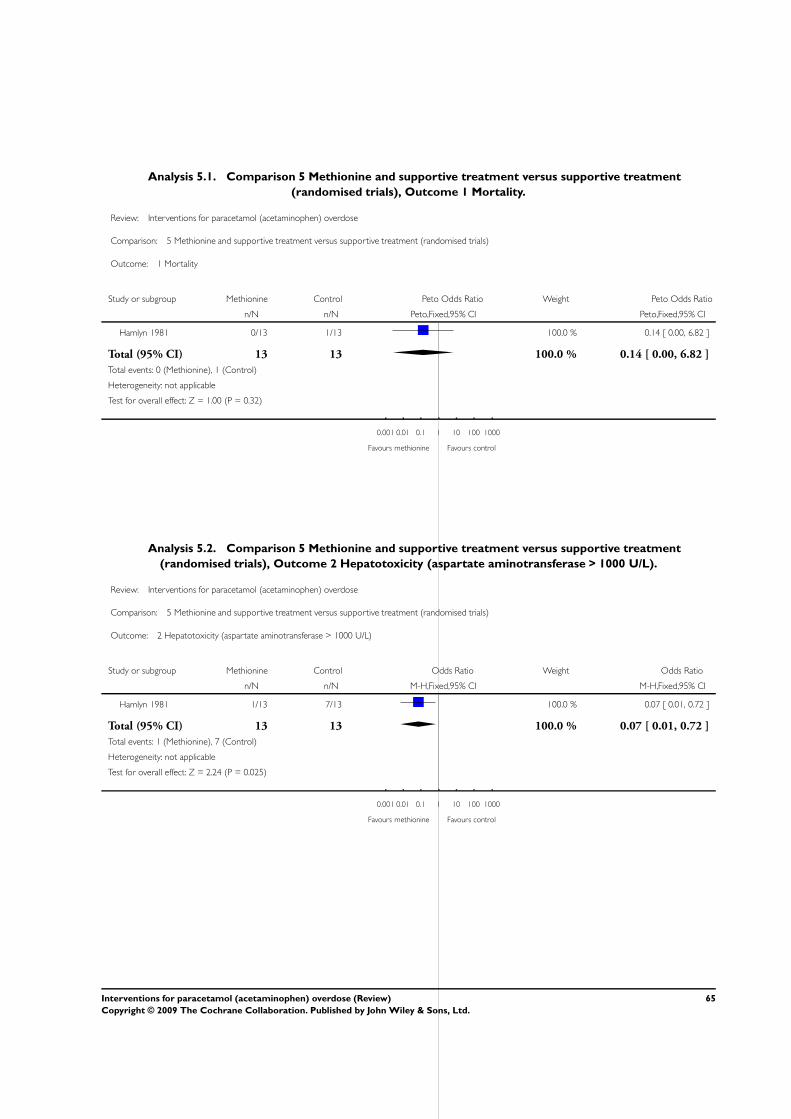
Analysis 5.1. Comparison 5 Methionine and supportive treatment versus supportive treatment
(randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 5 Methionine and supportive treatment versus supportive treatment (randomised trials)
Outcome: 1 Mortality
Study or subgroup Methionine Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Hamlyn 1981 0/13 1/13 100.0 % 0.14 [ 0.00, 6.82 ]
Total (95% CI) 13 13 100.0 % 0.14 [ 0.00, 6.82 ]
Total events: 0 (Methionine), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.00 (P = 0.32)
0.001 0.01 0.1 1 10 100 1000
Favours methionine Favours control
Analysis 5.2. Comparison 5 Methionine and supportive treatment versus supportive treatment
(randomised trials), Outcome 2 Hepatotoxicity (aspartate aminotransferase > 1000 U/L).
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 5 Methionine and supportive treatment versus supportive treatment (randomised trials)
Outcome: 2 Hepatotoxicity (aspartate aminotransferase > 1000 U/L)
Study or subgroup Methionine Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Hamlyn 1981 1/13 7/13 100.0 % 0.07 [ 0.01, 0.72 ]
Total (95% CI) 13 13 100.0 % 0.07 [ 0.01, 0.72 ]
Total events: 1 (Methionine), 7 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.24 (P = 0.025)
0.001 0.01 0.1 1 10 100 1000
Favours methionine Favours control
65Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
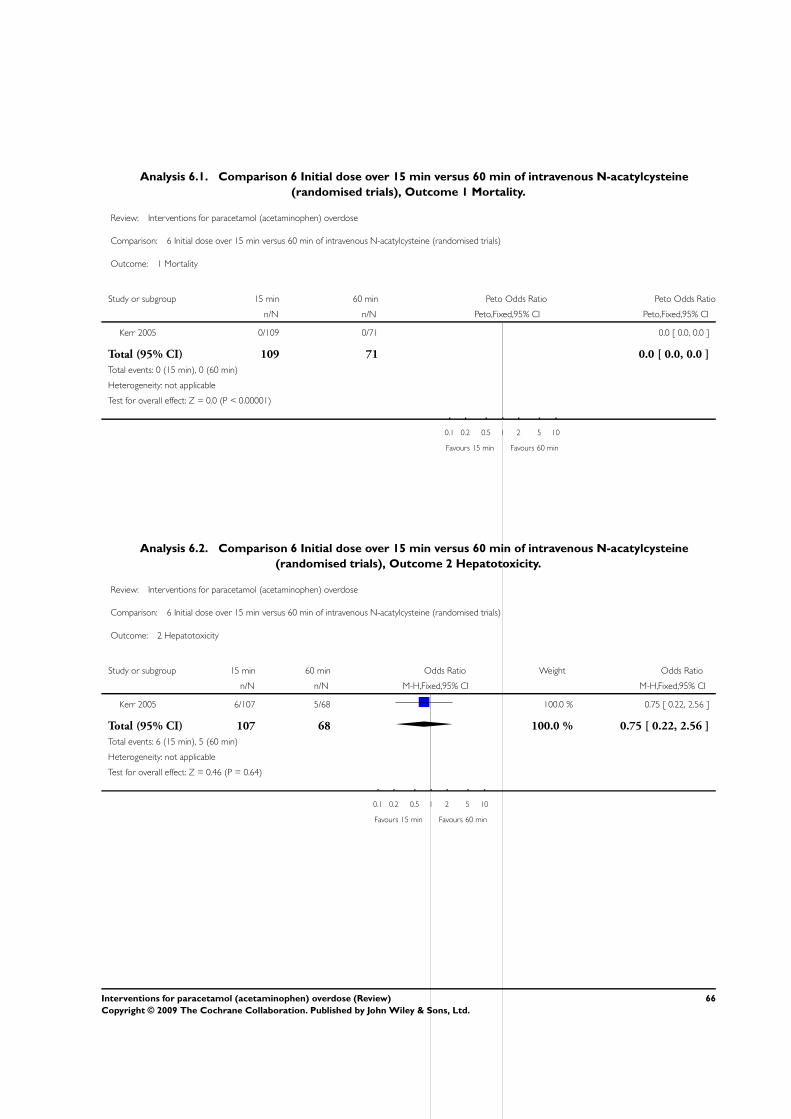
Analysis 6.1. Comparison 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine
(randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine (randomised trials)
Outcome: 1 Mortality
Study or subgroup 15 min 60 min Peto Odds Ratio Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
Kerr 2005 0/109 0/71 0.0 [ 0.0, 0.0 ]
Total (95% CI) 109 71 0.0 [ 0.0, 0.0 ]
Total events: 0 (15 min), 0 (60 min)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P < 0.00001)
0.1 0.2 0.5 1 2 5 10
Favours 15 min Favours 60 min
Analysis 6.2. Comparison 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine
(randomised trials), Outcome 2 Hepatotoxicity.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine (randomised trials)
Outcome: 2 Hepatotoxicity
Study or subgroup 15 min 60 min Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Kerr 2005 6/107 5/68 100.0 % 0.75 [ 0.22, 2.56 ]
Total (95% CI) 107 68 100.0 % 0.75 [ 0.22, 2.56 ]
Total events: 6 (15 min), 5 (60 min)
Heterogeneity: not applicable
Test for overall effect: Z = 0.46 (P = 0.64)
0.1 0.2 0.5 1 2 5 10
Favours 15 min Favours 60 min
66Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
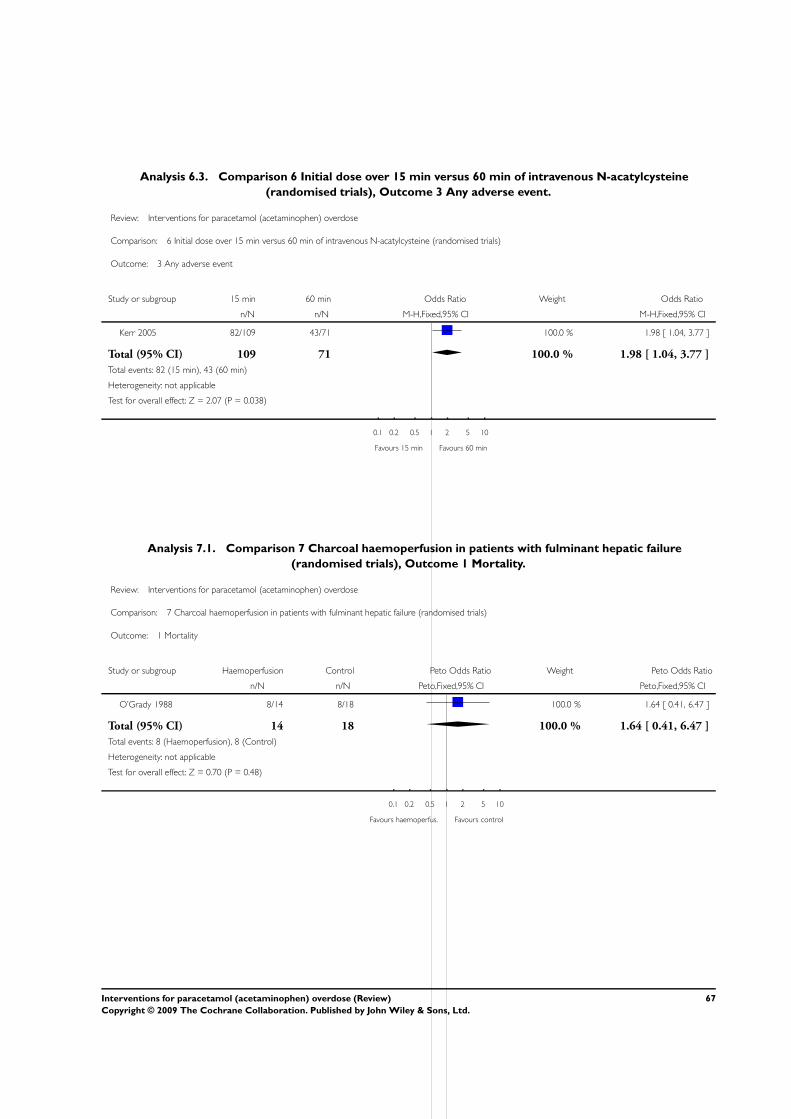
Analysis 6.3. Comparison 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine
(randomised trials), Outcome 3 Any adverse event.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 6 Initial dose over 15 min versus 60 min of intravenous N-acatylcysteine (randomised trials)
Outcome: 3 Any adverse event
Study or subgroup 15 min 60 min Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Kerr 2005 82/109 43/71 100.0 % 1.98 [ 1.04, 3.77 ]
Total (95% CI) 109 71 100.0 % 1.98 [ 1.04, 3.77 ]
Total events: 82 (15 min), 43 (60 min)
Heterogeneity: not applicable
Test for overall effect: Z = 2.07 (P = 0.038)
0.1 0.2 0.5 1 2 5 10
Favours 15 min Favours 60 min
Analysis 7.1. Comparison 7 Charcoal haemoperfusion in patients with fulminant hepatic failure
(randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 7 Charcoal haemoperfusion in patients with fulminant hepatic failure (randomised trials)
Outcome: 1 Mortality
Study or subgroup Haemoperfusion Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
O’Grady 1988 8/14 8/18 100.0 % 1.64 [ 0.41, 6.47 ]
Total (95% CI) 14 18 100.0 % 1.64 [ 0.41, 6.47 ]
Total events: 8 (Haemoperfusion), 8 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.70 (P = 0.48)
0.1 0.2 0.5 1 2 5 10
Favours haemoperfus. Favours control
67Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
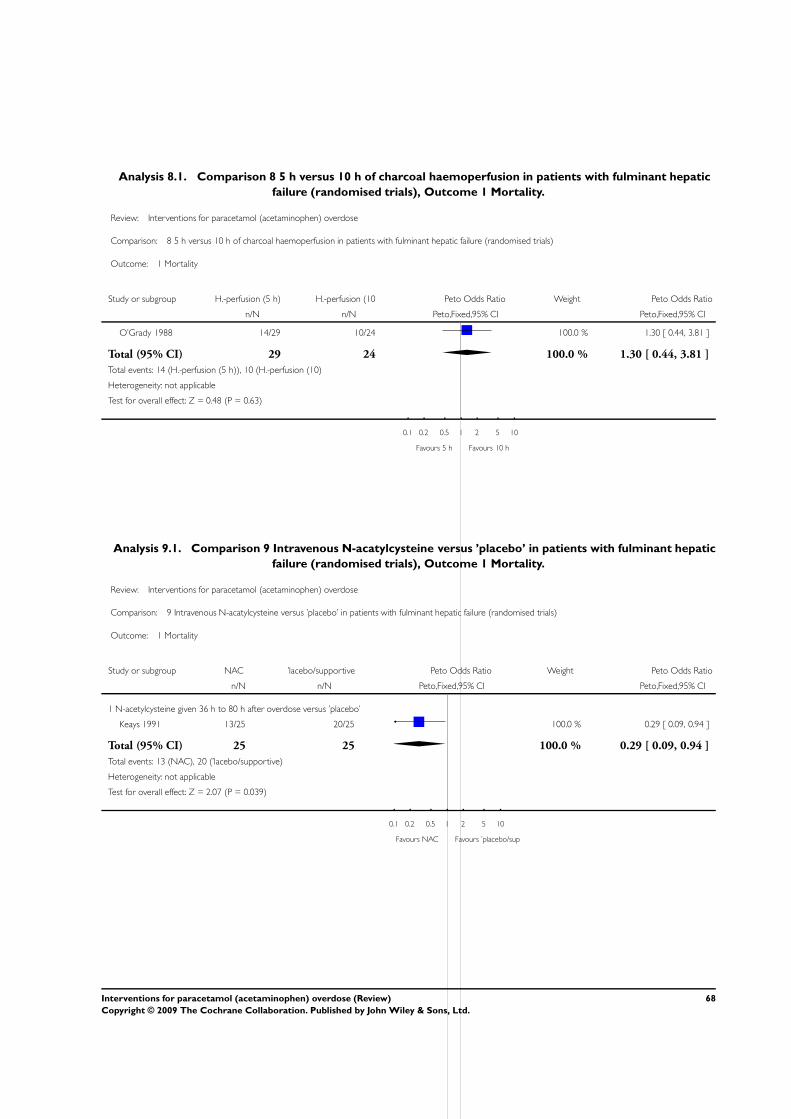
Analysis 8.1. Comparison 8 5 h versus 10 h of charcoal haemoperfusion in patients with fulminant hepatic
failure (randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 8 5 h versus 10 h of charcoal haemoperfusion in patients with fulminant hepatic failure (randomised trials)
Outcome: 1 Mortality
Study or subgroup H.-perfusion (5 h) H.-perfusion (10 Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
O’Grady 1988 14/29 10/24 100.0 % 1.30 [ 0.44, 3.81 ]
Total (95% CI) 29 24 100.0 % 1.30 [ 0.44, 3.81 ]
Total events: 14 (H.-perfusion (5 h)), 10 (H.-perfusion (10)
Heterogeneity: not applicable
Test for overall effect: Z = 0.48 (P = 0.63)
0.1 0.2 0.5 1 2 5 10
Favours 5 h Favours 10 h
Analysis 9.1. Comparison 9 Intravenous N-acatylcysteine versus ’placebo’ in patients with fulminant hepatic
failure (randomised trials), Outcome 1 Mortality.
Review: Interventions for paracetamol (acetaminophen) overdose
Comparison: 9 Intravenous N-acatylcysteine versus ’placebo’ in patients with fulminant hepatic failure (randomised trials)
Outcome: 1 Mortality
Study or subgroup NAC ’lacebo/supportive Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N Peto,Fixed,95% CI Peto,Fixed,95% CI
1 N-acetylcysteine given 36 h to 80 h after overdose versus ’placebo’
Keays 1991 13/25 20/25 100.0 % 0.29 [ 0.09, 0.94 ]
Total (95% CI) 25 25 100.0 % 0.29 [ 0.09, 0.94 ]
Total events: 13 (NAC), 20 (’lacebo/supportive)
Heterogeneity: not applicable
Test for overall effect: Z = 2.07 (P = 0.039)
0.1 0.2 0.5 1 2 5 10
Favours NAC Favours ’placebo/sup
68Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

A P P E N D I C E SAppendix 1. Search strategies
Database Search strategy Time span
CHBG Controlled Trials Register (acetaminophen OR paracetamol) AND
(overdos* OR poison*) AND (methionin*
OR cystein* OR cysteamin* OR dimer-
caprol OR cimetidin* OR acetylcystein*
OR NAC OR ’gastric lavage*’ OR ’gas-
tric decontamination*’ OR charcoal OR
ipecacuanha OR ipecac OR hemoperfu-
sion* OR haemoperfusion*)
Last search performed 1 December 2005.
11 references were identified.
CHBG Miscellaneous database (acetaminophen OR paracetamol) AND
(overdos* OR poison*) AND (methionin*
OR cystein* OR cysteamin* OR dimer-
caprol OR cimetidin* OR acetylcystein*
OR NAC OR ’gastric lavage*’ OR ’gas-
tric decontamination*’ OR charcoal OR
ipecacuanha OR ipecac OR hemoperfu-
sion* OR haemoperfusion*)
Last search performed 1 December 2005.
21 references were identified.
Cochrane Central Register of Controlled
Trials (CENTRAL) in The Cochrane Li-
brary
#1 MeSH descriptor Acetaminophen ex-
plode all trees in MeSH products 1169
#2 acetaminophen* or paracetamol* in All
Fields in all products 2566
#3 (#1 OR #2) 2566
#4 MeSH descriptor Overdose explode all
trees in MeSH products 62
#5 overdos* or poison* in All Fields in all
products 986
#6 (#4 OR #5) 986
#7 methionin* OR cystein* OR cys-
teamin* OR dimercaprol OR cimetidin*
OR acetylcystein* OR NAC OR gastric
lavage* OR gastric decontamination* OR
charcoal OR ipecacuanha OR ipecac OR
hemoperfusion* OR haemoperfusion* in
All Fields in all products 4154
#8 (#3 AND #6 AND #7) 46
Issue 4, 2005. 44 references were identified.
MEDLINE #1 explode “Acetaminophen”/ all subhead-
ings
#2 (acetaminophen* or paracetamol*) in
TI
1950 to December 2005. 252 references
were identified.
69Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
#3 (acetaminophen* or paracetamol*) in
AB
#4 #1 or #2 or #3
#5 explode “Overdose”/ all subheadings
#6 (overdos* or poison*) in TI
#7 (overdos* or poison*) in AB
#8 #5 or #6 or #7
#9 (methionin* or cystein* or cysteamin*
or dimercaprol or cimetidin* or acetyl-
cystein* or NAC or gastric lavage* or
gastric decontamination* or charcoal or
ipecacuanha or ipecac or hemoperfusion*
or haemoperfusion*) in TI
#10 (methionin* or cystein* or cysteamin*
or dimercaprol or cimetidin* or acetyl-
cystein* or NAC or gastric lavage* or
gastric decontamination* or charcoal or
ipecacuanha or ipecac or hemoperfusion*
or haemoperfusion*) in AB
#11 #9 or #10
#12 #4 and #8 and #11
#13 ((random* or clinical or controlled or
observational) near (trial* or stud*)) in TI
#14 ((random* or clinical or controlled or
observational) near (trial* or stud*)) in AB
#15 #13 or #14
#16 (human* or patient* or volunteer* or
healthy subject*) in TI
#17 (human* or patient* or volunteer* or
healthy subject*) in AB
#18 #16 or #17
#19 #12 and (#15 or #18)
#20 animal* in TG
#21 #19 not #20
EMBASE #1 explode “paracetamol”/ all subheadings
#2 (acetaminophen* or paracetamol*) in
TI
#3 (acetaminophen* or paracetamol*) in
AB
#4 #1 or #2 or #3
#5 explode “drug-intoxication”/ all sub-
headings
#6 explode “drug-overdose”/ all subhead-
ings
#7 (overdos* or poison*) in TI
1980 to December 2005. 318 references
were identified.
70Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
#8 (overdos* or poison*) in AB
#9 #5 or #6 or #7 or #8
#10 (methionin* or cystein* or cysteamin*
or dimercaprol or cimetidin* or acetyl-
cystein* or NAC or gastric lavage* or
gastric decontamination* or charcoal or
ipecacuanha or ipecac or hemoperfusion*
or haemoperfusion*) in TI
#11 (methionin* or cystein* or cysteamin*
or dimercaprol or cimetidin* or acetyl-
cystein* or NAC or gastric lavage* or
gastric decontamination* or charcoal or
ipecacuanha or ipecac or hemoperfusion*
or haemoperfusion*) in AB
#12 #10 or #11
#13 #4 and #9 and #12
#14 ((random* or clinical or controlled or
observational) near (trial* or stud*)) in TI
#15 ((random* or clinical or controlled or
observational) near (trial* or stud*)) in AB
#16 #14 or #15
#17 (human* or patient* or volunteer* or
healthy subject*) in TI
#18 (human* or patient* or volunteer* or
healthy subject*) in AB
#19 #17 or #18
#20 #13 and (#16 or #19)
#21 animal* in DER
#22 #20 not #21
Science Citation Index Expanded
(http://portal.isiknowledge.com/portal.cgi?DestApp=WOS&Func=Frame)
#19 #17 NOT #18
#18 (TS=animal*) OR (TI=animal*)
#17 #10 AND (#13 OR #16)
#16 #15 OR #14
#15 TI=(human* or patient* or volunteer*
or healthy subject*)
#14 TS=(human* or patient* or volunteer*
or healthy subject*)
#13 #12 OR #11
#12 TI=((random* or clinical or controlled
OR observational) AND (trial* or stud*))
#11 TS=((random* or clinical or controlled
OR observational) AND (trial* or stud*))
#10 #9 AND #6 AND #3
#9 #8 OR #7
1945 to December 2005. 215 references
were identified.
71Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
(Continued)
#8 TI=(methionin* or cystein* or cys-
teamin* or dimercaprol or cimetidin* or
acetylcystein* or NAC or gastric lavage*
or gastric decontamination* or charcoal or
ipecacuanha or ipecac or hemoperfusion*
or haemoperfusion*)
#7 TS=(methionin* or cystein* or cys-
teamin* or dimercaprol or cimetidin* or
acetylcystein* or NAC or gastric lavage*
or gastric decontamination* or charcoal or
ipecacuanha or ipecac or hemoperfusion*
or haemoperfusion*)
#6 #5 OR #4
#5 TI=(overdos* or poison*)
#4 TS=(overdos* or poison*)
#3 #2 OR #1
#2 TI=(acetaminophen* or paracetamol*)
#1 TS=(acetaminophen* or paracetamol*)
W H A T ’ S N E W
Last assessed as up-to-date: 21 February 2006.
9 November 2008 Amended Converted to new review format.
H I S T O R Y
Protocol first published: Issue 4, 2001
Review first published: Issue 3, 2002
C O N T R I B U T I O N S O F A U T H O R S
Jesper Brok designed, drafted, and revised the protocol; performed the searches; selected trials and studies; extracted data; and drafted
and revised the review.
Nick Buckley retrieved papers; extracted data; and revised the protocol and the review.
Christian Gluud revised the protocol and the review.
72Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
None known.
S O U R C E S O F S U P P O R TInternal sources
• Copenhagen Trial Unit, Denmark.
External sources
• The 1991 Pharmacy Foundation, Denmark.
• Copenhagen Hospital Corporation’s Medical Research Council’s Grant on Getting Research into Practice (GRIP), Denmark.
• Danish Medical Research Council’s Grant on Getting Research into Practice (GRIP), Denmark.
• Copenhagen Hospital Corporation’s Medical Research Council, Denmark.
N O T E S
Since the publication of the protocol for this systematic Review, the following changes have been performed in the protocol part of the
Review:
The ’Objective’ section has been shortened and the more specific questions are now moved to ’Type of interventions’ .
Evidence from quasi-randomised studies, non-randomised studies, and randomised trials involving human volunteers has been placed
under ’Exploratory analysis’ at the end of the Result section. We caution readers that this evidence should be interpreted conservatively
due to the risk of systematic errors in non-randomised studies and the dangers of translating results from studies on human volunteers
into clinical practice.
Regarding ’The methods used to synthesize data’
We decided to analyse our data with both the fixed effect model as well as the random effects model. This was not included in the
primary protocol.
I N D E X T E R M S
Medical Subject Headings (MeSH)
Acetaminophen [pharmacokinetics; ∗poisoning]; Analgesics, Non-Narcotic [pharmacokinetics; ∗poisoning]; Antidotes [therapeutic
use]; Charcoal [therapeutic use]; Gastric Lavage; Intestinal Absorption; Liver Failure, Acute [chemically induced; surgery]; Liver
Transplantation; Overdose [therapy]
73Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

MeSH check words
Humans
74Interventions for paracetamol (acetaminophen) overdose (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.