intraoperative and postoperative management of · pdf fileintraoperative and postoperative...
TRANSCRIPT

Intraoperative and Postoperative Management of
Complications
Ashok R. Shaha, M.D., F.A.C.S. Professor of Surgery
Jatin P. Shah Chair in Head and Neck Surgery Head and Neck Service
Memorial Sloan-Kettering Cancer Center New York, New York

Samuel D. Gross - 1866 Philadelphia
A System of Surgery
Thyroid surgery: ‘Horrid butchery’
“No honest and sensible surgeon would ever engage in thyroid surgery”


The extirpation of thyroid gland typifies perhaps better than any operation the
supreme triumph of the surgeon’s art.
Halsted

Postoperative Complications
• Postoperative complications infrequent in experienced hands
• Early recognition and prompt initial management crucial for successful outcome
• Best prevented by meticulous surgical technique

Thyroid Literature
Thyroid disease 136,053 Thyroid tumors 33,554
Thyroid Google search 36 million
Medline
• New Paper on Thyroid Disease – Every 3 Hours • New Paper on Thyroid Cancer – Every 8 Hours
Thyroid Cancer Google search 21 million

Complications of thyroid surgery performed by residents
Ashok Shaha MD, FACS & Bernard M. Jaffe, MD, FACS
Surgery 1988; 104:1109-14.
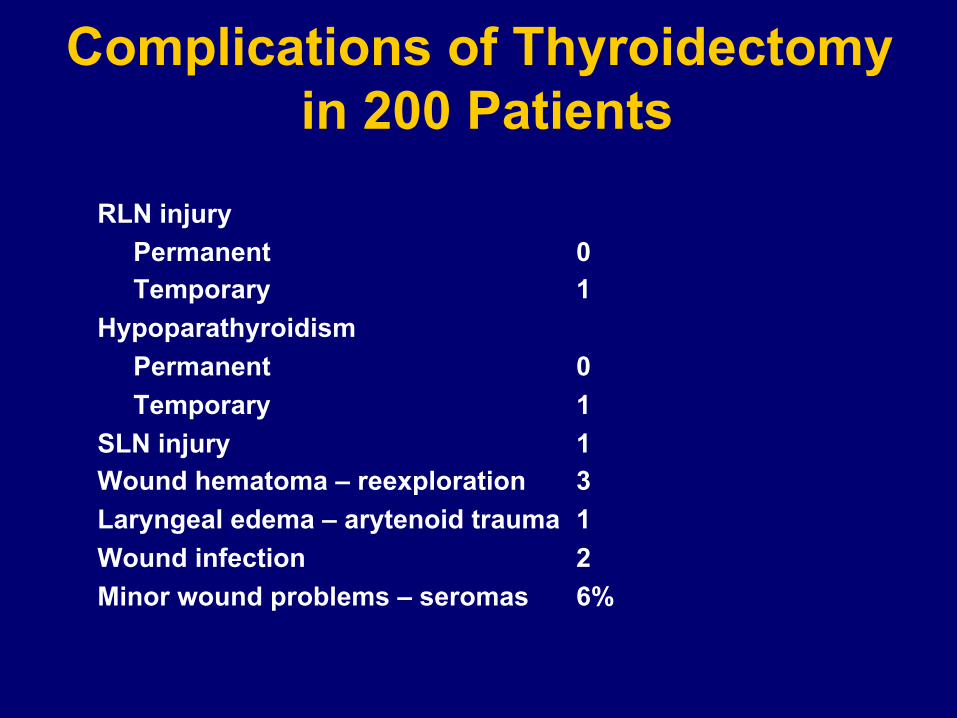
Complications of Thyroidectomy in 200 Patients
RLN injury Permanent 0 Temporary 1
Hypoparathyroidism Permanent 0 Temporary 1
SLN injury 1 Wound hematoma – reexploration 3 Laryngeal edema – arytenoid trauma 1 Wound infection 2 Minor wound problems – seromas 6%

Complications of Thyroidectomy Wound hematoma – airway obstruction
Seroma – collection Infection Hypertrophic scar Keloid
Recurrent laryngeal nerve injury – unilateral Bilateral – rare
Hypoparathyroidism – temporary Permanent
Recurrent hyperthyroidism Hypothyroidism Superior laryngeal nerve injury Chyle leak Horner’s syndrome – injury to sympathetic trunk – very rare
Iyer NG, Shaha AR. Minerva Chir 2010:65:71-82.

Complications in Thyroid Surgery Increased incidence with • Extent of disease (size) • Extent of surgery • Reoperative surgery • Extrathyroid extension and malignancy • Paratracheal dissection • Neck dissection • Substernal thyroid • Reoperation for hematoma • Less experienced surgeon Bigger the operation, bigger the complications

The risk of parathyroid injury is directly proportional to the extent of thyroidectomy and inversely proportional to the
surgeon’s experience.
Thyroid Surgery

UNADJUSTED AND ADJUSTED CLINICAL OUTCOMES FROM THYROIDECTOMY
BY SURGEON VOLUME GROUP Surgeon Volume Groups
OutcomesA 1-9cases
B10-29cases
C30-100cases
D>100cases
Complication rate Unadjusted (%) Adjusted (%)Length of stay Unadjusted (days) Adjusted (days)*
10.1†8.6†
2.8‡1.9‡
6.7†6.1†
2.1‡1.7‡
6.9†6.1†
2.2‡1.7‡
5.95.1
1.71.4
*Adjusted for patient age, race, comorbidities, diagnosis, procedure,surgeon and hospital volume† p<0.001 compared to Group D‡ p<0.05 compared to Group D
Sosa et al, 19

Medical malpractice and the thyroid gland Lydiatt DD. Head Neck 25:429-431, 2003.
• Jury verdict reviews from 1987-2000 were obtained from a computerized database
• 30 suits from 9 states occurred • Plaintiffs were women in 80% of the cases, with a mean
age of 41 • 50% of pts (15 of 30) had a bad outcome, (9 of 30 dead, 4 of
30 with neurologic deficits, 1 blind & 1 alive w/ cancer) • 30% alleged surgical complications, most RLN injury, and
75% of cancer pts alleged a delay, either through falsely negative biopsies or no biopsy taken
• Respiratory events occurred in 43% and frequently resulted in large awards
How to Avoid or Predict?
• Preop vocal cords evaluation
• Fixed mass to the central compartment
• CT scan (Imaging)
• Older patient
• FNA – Poorly differentiated cancer
• Preop endoscopy

Thyroidectomy
Imaging studies
• Ultrasound –Nodes - Superior Mediastinal - Lateral - Retropharyngeal
• CT scan without contrast
• MRI
How I Do It
• Arteria lusoria

Thyroidectomy Anesthesia considerations
• Pre-operative evaluation for intubation • Pre-operative laryngoscopy intubation without any trauma
• Small endotracheal tube • Cuff of endotracheal tube below the vocal cords
How I Do It
• Smooth induction and smooth extubation (Be Present) • Post-operative observation in Recovery Room


Thyroidectomy Position
• 3 flat sheets under shoulder • Head on the head board • Both hands tucked in • 30o reverse trendelenberg • Transparent drape
Thyroidectomy Incision
• Plan line of incision pre-op sitting or standing • Skin crease/ necklace line • Higher incision in women • Generous incision in large, fixed or substernal tumors • Incision for thyroidectomy & neck dissections
• Avoid J shaped incision

Thyroidectomy Incision
• Bold surgeons make small incisions • Timid surgeons make big incisions • Good surgeons make adequate incisions

Thyroidectomy Neck Release
• Open the “gift wrap” • Separate fascia from the muscles • Separate strap muscles • Separate sternomastoid muscle
Moraitis, Shaha. JSO 2006

The sternohyoid muscle is retracted laterally and the sternothyroid muscle is carefully lifted off the thyroid gland and transected superiorly for full exposure of the superior thyroid vessels. Moraitis D, Shaha AR. JSO 2006

The sternothyroid muscle is peeled off the thyroid gland and the superior thyroid vessels and nerve are exposed. The superior thyroid pedicle is ligated close to the thyroid parenchyma. Moraitis D, Shaha AR. JSO 2006


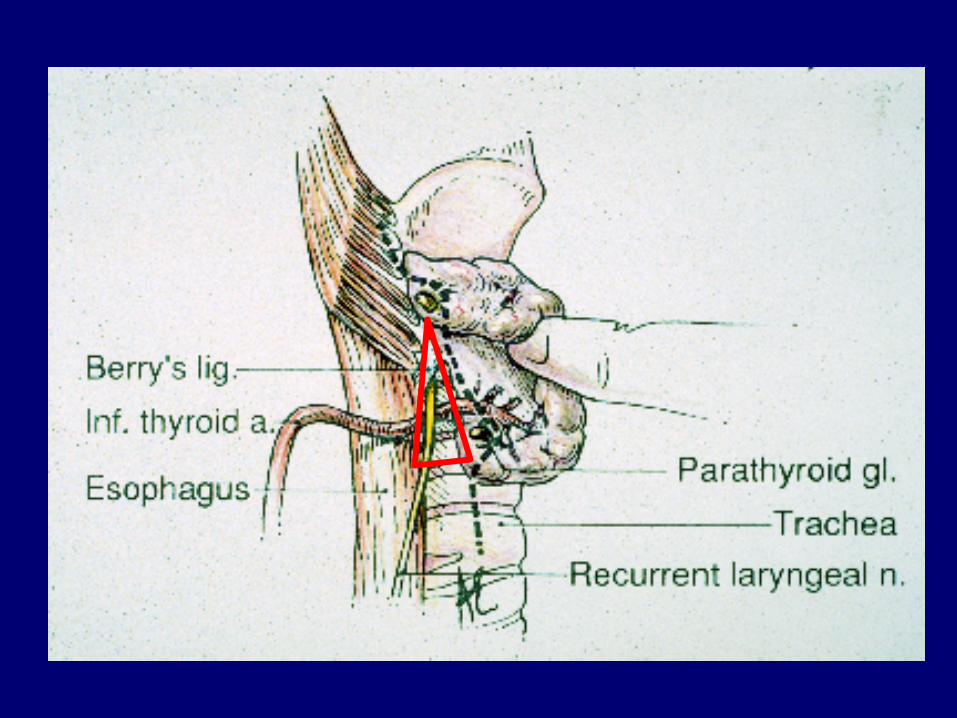
Thyroidectomy RLN Injury
• In the TE groove (nodal dissection) • At the crossing of the inferior thyroid artery • Near the ligament of Berry – small vessels
Traversing: Bipolar cautery


Risk Factors for RLN Injury
• Locally aggressive thyroid cancer • Extensive nodal disease and dissection
• Central Compartment • Multiple RLN branches • Massive goiter • Substernal goiters • Reoperations • Surgeon Experience (Skill, Patience) • Non-recurrent RLN

Thyroid
ICA
Cricothyroid muscle
Non recurrent laryngeal nerve
Trachea
Anterior
Superior Inferior
Posterior




Management of RLN Invaded by Cancer
• Pre-op palsy- sacrifice nerve • Dissect the nerve off the tumor
• No gross tumor left behind • Primary Anastomosis of RLN • Nerve grafting • Decision about other side • Nerve monitor
Intra-Op Management of RLN Injury
• Transaction of the nerve • Primary anastomoses
• Nerve graft • Ansa • Greater auricular • Sural
• Find the proximal end near cricoid by dissection through the cricopharyngeus muscle.

Technique of Thyroidectomy
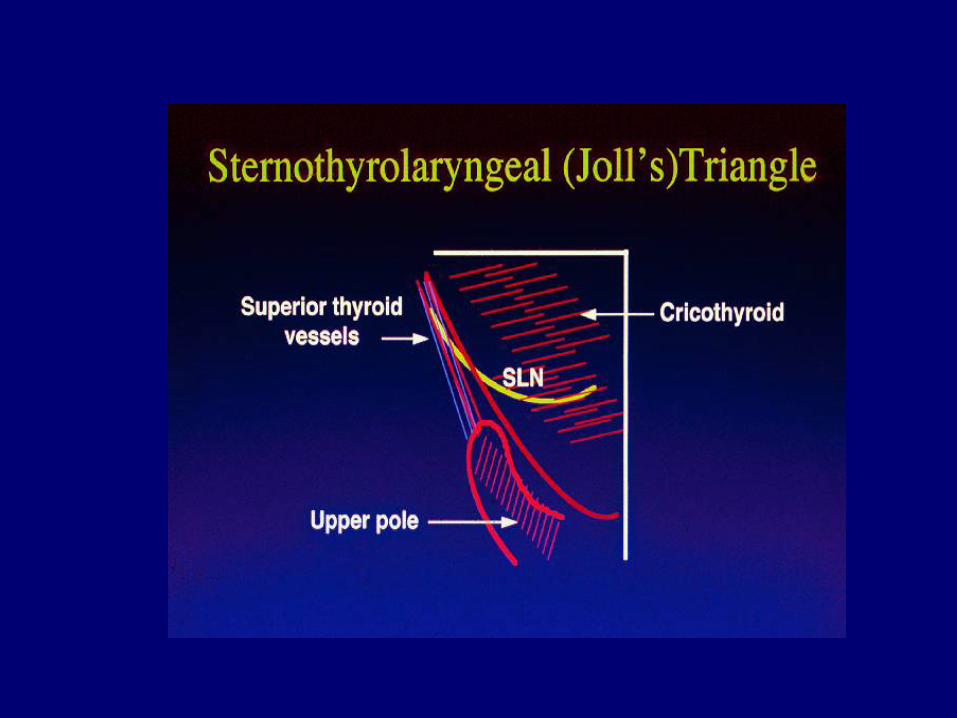
Dissection of the superior thyroid vessels parallel to the vessels on surface of thyroid & exposure of SLN
Shaha A. J Surg Onc, 1993.
Amelita Galli-Curci

Guidelines to Parathyroid Preservation
• Good exposure, light, hemostasis
• Recognition of parathyroids - color, size, location
• Meticulous dissection
• Identify and protect the blood supply to parathyroids
• Ligate inferior thyroid artery close to thyroid

Parathyroid Preservation
Dissect on the capsule; ligate vessels distal to parathyroid

• Technical considerations • Ligation of branches of inferior thyroid
artery close to thyroid • Avoid parathyroid hematoma • Avoid excessive irrigation and suction
• Post-op close follow-up & management • Autotransplantation
• Total thyroidectomy is really a parathyroid preservation operation
AVOID HYPERCALCEMIA
• 6 hours – postop PTH assay

Serum Total Calcium 12-24 hours post op
< 7.0* 7.0 - 7.4 7.5 - 8.0 > 8.0
Etiology Near total lack of PTH Mild PTH deficiency Mostly dilutional or parathyroid trauma
None
IV calcium As needed for acute symptoms+
As needed for acute symptoms+
As needed for acute symptoms+
Oral Calcium Tums Ultra (400 mg) 3 tabs po TID
Tums Ultra (400 mg) 3 tabs po TID
Tums Ultra (400 mg) 3 tabs po TID
Not needed Tums Ultra (400 mg) 1-2 tabs BID until postop visit
Vitamin D therapy
calcitriol 0.5 mg BID calcitriol 0.25 mcg qd Not needed Not needed
In House Monitoring
Serum calcium BID until trending upward
Serum calcium BID until trending upward
Serum calcium BID until stable
Not needed
Monitoring after DC
Serum calcium 48-72 hours after DC
Serum Calcium 7-10 days after DC
Serum Calcium 7-10 days after DC
Not needed
Management of Post-thyroidectomy Hypocalcemia
These guidelines assume a near normal serum albumin. * Check PTH if calcium below 7.0 in follow up No discharge if calcium is below 7.0 + IV solution – calcium gluconate 10 – 20 mL diluted in 200 mL of saline over 20 minutes First postop visit – If serum calcium is above 8.5, reduce one tablet weekly starting vit D.
If calcium is below 8, continue calcium and vit D and revisit in 3-4 weeks

Thyroidectomy
Indications for drains in thyroidectomy
• Large & substernal goiter
• Subtotal thyroidectomy
• Surgery for Graves disease
• Type of drain

Hemorrhage and Hematoma • Reported to occur in < 1% of the cases • Most commonly occur within 6 hours after
surgery (5 min-5 days) • Close monitoring for at least 6 hours after
surgery • Prevention:
Identification & ligation of blood vessels during surgery Meticulous hemostasis before wound closure Normalize blood pressure before wound closure Valsalva maneuver to identify potential venous bleeders
• Bedside evacuation of hematoma
Complications Associated with Thyroidectomy and Neck Dissection
Hypoparathyroidism • Transient • Permanent Chyle leak/chyloma Bleeding and hematoma Seroma Wound infection Nerve injuries • Accessory nerve • Hypoglossal nerve • Ramus mandibularis • Sympathetic chain (Horner’s syndrome) • Brachial plexus • Phrenic nerve • Cutaneous cervical plexus
Iyer NG, Shaha AR. Minerva Chir 2010:65:71-82.

Prospective Functional Voice Assessment in Patients Undergoing
Thyroid Surgery Stojadinovic/Shaha, et al. Ann Surg 2002.
• To analyze voice before & after thyroid surgery • Prospective study of 50 pts – functional voice testing • Acoustic/aerodynamic/glottographic/videostroboscopic testing • 30% pts reported early subjective voice changes • 14% reported late subjective voice changes • 84% had significant objective change in at least one voice parameter • 12% had significant alterations in more than 3 voice measures

Post Thyroidectomy Central Compartment Syndrome
• Submental anesthesia/paresthesia • Vague voice changes • Chronic throat discomfort • Swallowing difficulties • Feeling of choking
(Shaha)

Special Clinical Issues
• Superior laryngeal nerve
• Intraoperative nerve stimulation & monitoring
• Drains • Management of substernal goiter
• Management of post-op hypocalcemia
• Tracheomalacia • Harmonic/ Ligasure

Thyroid Surgery
• Brain • Hands • Loops • Bipolar cautery • Micro-clamps • Good exposure • Patience & meticulous dissection • Good assistance, retraction & exposure • Avoid excessive irrigation and suction • Harmonic scalpel
How I Do It

Technology in Thyroid Surgery
• Harmonic / Ligasure
• Nerve Monitor
• Endoscopic Thyroidectomy
• Robotic Thyroidectomy

Thyroidectomy • Nodulectomy • Lobectomy / Isthmusectomy • Subtotal Thyroidectomy • Local anesthesia / regional block • Outpatient Surgery • 23 hr discharge • Small incision surgery – 3-5 cm • Endoscopic - Video assisted
Cervical Chest approach Submammary Transaxillary
• Robotic Transaxillary • Bilateral Axillary Breast Approach (BABA) • Transoral thyroidectomy

“The good physician treats the disease;
the great physician treats the patient
who has the disease.”
- Sir William Osler