introduction to qualitative research methodologies … health... · the safe motherhood is based on...
TRANSCRIPT

Safe Motherhood
Dr. Durdana KhanAssistant Professor
Department of Community Health Sciences
Dated: November 4th, 2016

Outline…
Why to safe A “Mother” ?
A journey from human to human right
Millennium Development Goals
Goal 5
Sustainable Development Goals
Goal 1, 3, 5 and 10
Safe Motherhood Models
Case studies
Why to safe A “Mother”?

Every Minute in the World…
380 Women become pregnant
190 Women face an unplanned or unwanted
pregnancy
110 Women experience a pregnancy-related
complication
40 Women have an unsafe abortion
5 Babies are born dead
5 Newborns die
1 mother dies


Maternal mortality ratio by region, 1990, 2005 and 2013
Source: http://data.unicef.org/maternal-health/maternal-mortality#sthash.WW4wpPPI.dpuf


Balochistan's women suffer in silence
Source: http://www.dawn.com/news/1139853, PUBLISHED OCT 23, 2014 04:17PM

According to Pakistan Health
Demographic Survey (PHDS)
Balochistan stands first in terms of Maternal
Mortality Rate (MMR) as compared to other
provinces of the country
785 die in Balochistan as compared to 272 in rest
of the country, out of 100,000 women,
BIG reasons:
Long distances
Poor communication systems
Lack of basic health facilities
Safe Motherhood…
A journey to human Right
1930…
The League of Nations Health Section noted concerns
about maternal mortality
1978…
Primary Health Care sponsored by WHO and UNICEF
in Alma Ata
1985…
WHO with UNFPA, supported first community studies on
maternal mortality in developing countries
1976-85, The United Nations Decade for Women, focus
attention on women’s rights and health.

Safe Motherhood…
A journey to human Right
1987…
WHO, UNFPA and World Bank sponsored first
international Safe Motherhood Conference in Nairobi
The effective starting point of what came to be known
as the Safe Motherhood Initiative (SMI)
1989…
The World Summit for Children in New York
Maternal mortality was viewed within the context of
ensuring the survival and health of children
1990…(28th May)
International Day of Action for Women’s health

Safe Motherhood…
A journey to human Right
1990…
NGOs working in the area of safe motherhood, at a
very local level, engaging in community-based
research, participating in awareness-raising or public
education campaigns, promoting workshops, meetings
or media events and even delivering care
1998…
World Health Day devoted to safe motherhood, with
the slogan ‘Pregnancy is special: let’s make it safe’
2000…
Millennium Declaration defined MDGS


Safe Motherhood is…
“A human right….
We must empower women and ensure choices …Our
task and the task of many like us, is to ensure that in the
next decade safe motherhood is not regarded as a
fringe issue, but as a central issue”
James D. Wolfensohn
President – World Bank

MDGs

MDG:
Goal 5: Improve Maternal Health
Reduce Maternal Mortality by three quarters, till
2015
Indicators
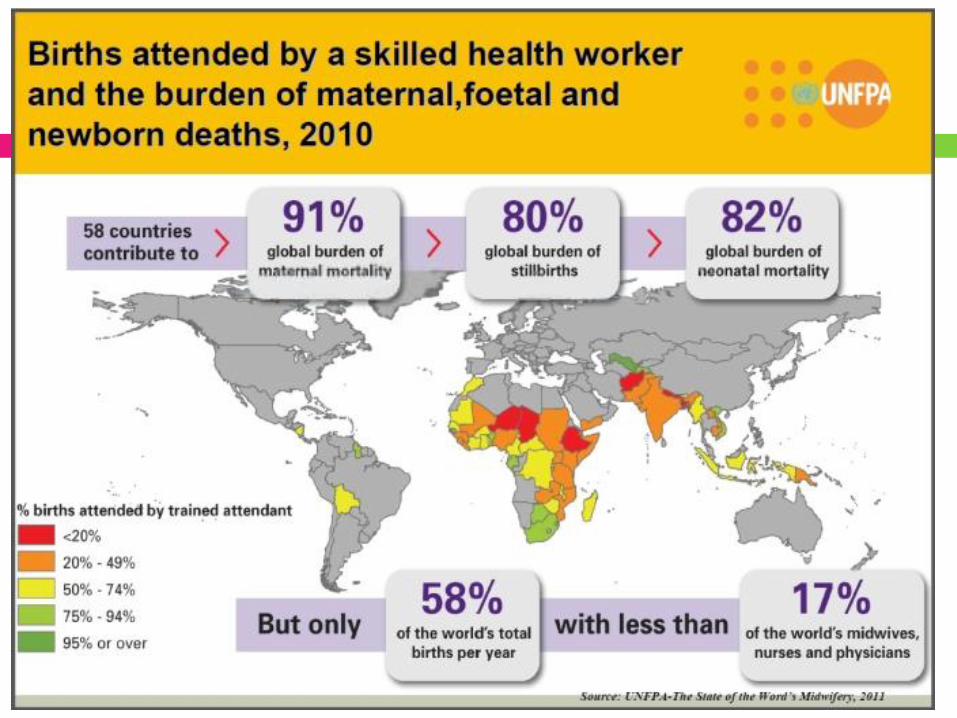
MMR & % of births attended by skilled health
personnel


Sustainable Development Goals
(SDGs)

TARGETS
3.1: By 2030, reduce the global maternal mortality
ratio to less than 70 per 100,000 live births
3.2: By 2030, end preventable deaths of newborns
and children under 5 years of age, with all
countries aiming to reduce neonatal mortality to at
least as low as 12 per 1,000 live births and under-
5 mortality to at least as low as 25 per 1,000 live
births

Targets
3.7: By 2030, ensure universal access to
reproductive health-care services, including for
family planning, information and education, and the
integration of reproductive health into national
strategies and programs
Definition
Safe Motherhood…
“Encompasses a series of initiatives, practices,
protocols and service delivery guidelines designed to
ensure that women receive high-quality gynecological,
family planning, prenatal, delivery and postpartum
care, in order to achieve optimal health for the
mother, fetus and infant during pregnancy, childbirth
and postpartum”
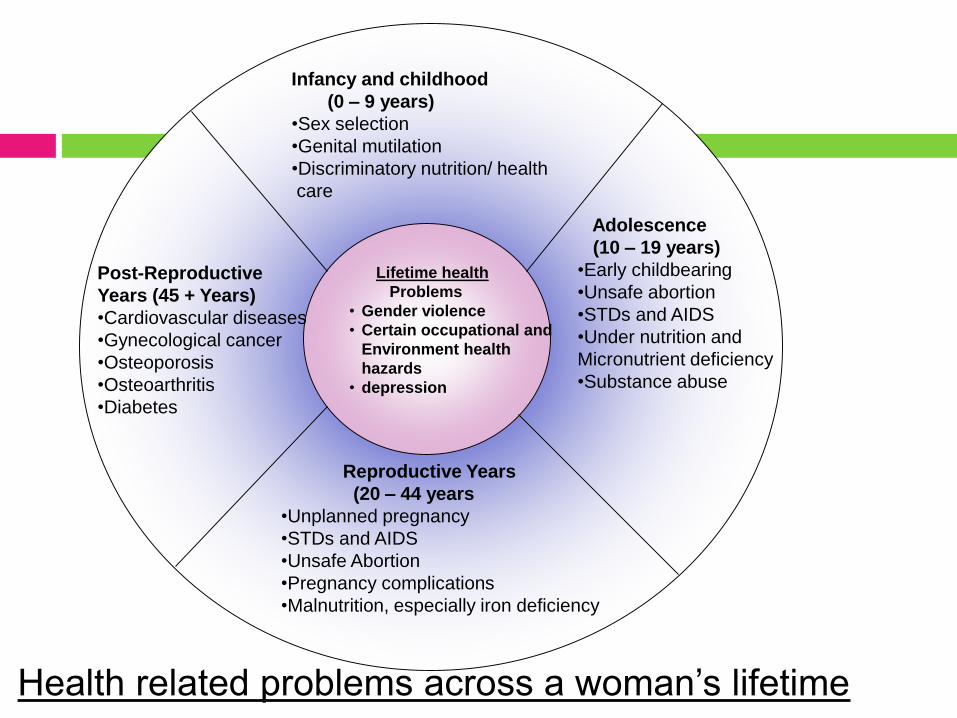
Lifetime health
Problems
• Gender violence
• Certain occupational and
Environment health
hazards
• depression
Infancy and childhood
(0 – 9 years)
•Sex selection
•Genital mutilation
•Discriminatory nutrition/ health
care
Adolescence
(10 – 19 years)
•Early childbearing
•Unsafe abortion
•STDs and AIDS
•Under nutrition and
Micronutrient deficiency
•Substance abuse
Reproductive Years
(20 – 44 years
•Unplanned pregnancy
•STDs and AIDS
•Unsafe Abortion
•Pregnancy complications
•Malnutrition, especially iron deficiency
Post-Reproductive
Years (45 + Years)
•Cardiovascular diseases
•Gynecological cancer
•Osteoporosis
•Osteoarthritis
•Diabetes
Health related problems across a woman’s lifetime

Safe Motherhood
WHO strategies for safe mother hood are;
The safe motherhood is based on four pillars, which
should be delivered through the primary health care
on the foundation of equity for women.
These pillars are
Family planning
Antenatal care
Clean/safe delivery
Essential obstetric care

Four Pillars Model
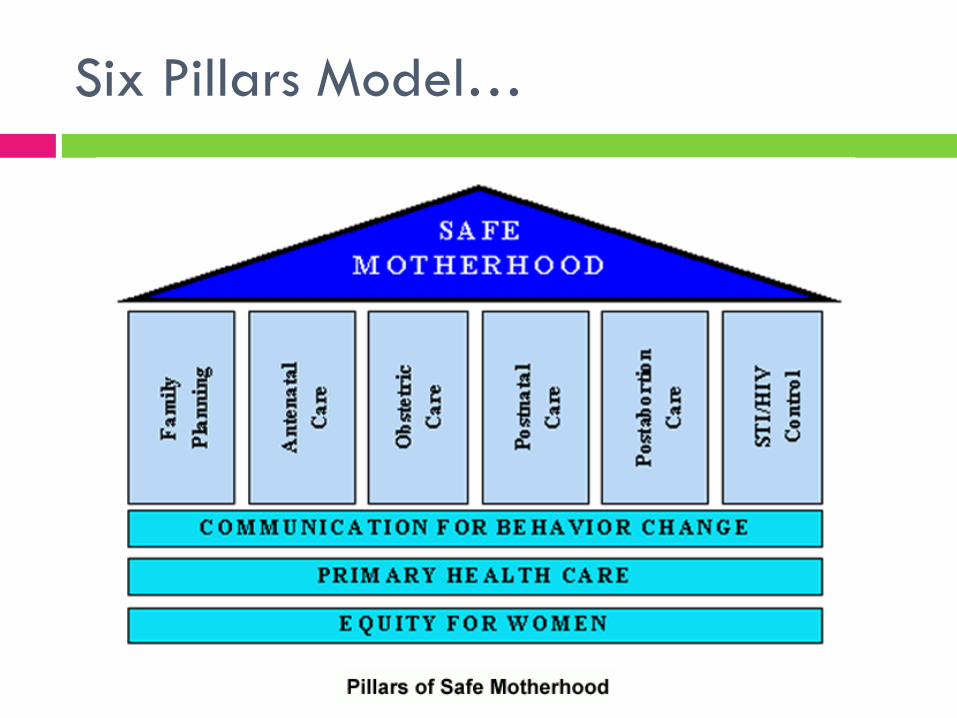
Six Pillars Model…

Services needed for safe
motherhood…
Prenatal services
Home visit by the midwives
Establishment of prenatal clinics
Intra-natal services
One midwife per 1000 births or3000 population
Medical advise by MO
Maternity homes
Supply of sterilized kits for delivery
Diagnostic and lab facilities
Ambulance services

Post natal services
Home visit by the midwives or LHV
Welfare centers for milk supply
Postnatal clinics for mothers
Hospital beds for complicated cases
Dai trainings
Supervision

Antenatal care
Care of mothers during pregnancy is ANC
The aim is to achieve healthy mothers and
healthy child at the end of pregnancy
It begin soon after conception till the end of
pregnancy

Objectives
To promote and maintain the health of mothers
during pregnancy
To detect high risk cases and give them attention
To foresee complication and prevent them
To sensitize mother for need of family planning
To teach mother the art of child health care

Components
Careful and complete obstetric history
Mother history especially in respect of diabetes,
hypertension and renal disease
Regular antenatal visits

Antenatal visits
Visits
-1st visit as soon as possible
-After every 4 weeks till 28 weeks
-After every 2 weeks till 36 weeks
-Once a week till she deliver

Antenatal visits
Minimum Antenatal visits
At least 4 visits are required
1st visit at 6-16 weeks –or before 12 weeks to confirm pregnancy
2nd visit at 24 weeks for baseline of health profile
3rd visit 32-34 weeks to find out position and presenting part
Last visit At 36 weeks where to deliver the baby

In routine 1st visits
To confirms the pregnancy
to confirm that she is fit to bear the strain of pregnancy
To know baseline of health
To detect any abnormalities and advise suitable treatment like referral if she needs.
Complete general physical examination
Routine investigation…. Blood complete, urine complete ,BP.
Special investigation like blood sugar. Urine for albumin, RH factor, etc

Clean/Safe Delivery…
2 interventions strategies have been proposed
Essential Obstetric Care (EOC)
Emergency Obstetric Care (EmOC)
EOC is a key to reducing maternal mortality

Essential obstetric care Emergency obstetric care
A broad strategy with
array of services:
Family planning
Antenatal care, intrapartum
and postpartum care
Focuses on all pregnant
women – based on the
concept of risk assessment
These are prompt intervention
measures:
Blood transfusion,
Intravenous antibiotics,
Caesarean delivery, vacuum
or forceps delivery
Focuses on prompt
identification; referral and
treatment of women with
obstetrical complications

AIMs of EOC…
To accelerate country-level action to improve
maternal health by focusing on preventing,
detecting and managing the major causes of
maternal mortality
Increased coverage (availability, accessibility
and utilization) as well as the performance of
EOC facilities
Levels of EOC…
Health center level (basic EOC)
District hospital level (comprehensive EOC)

Health center level (basic EOC)
One or more trained worker(s)
Equipment Required:
Oxytocics, antibiotics, manual placental,
removal, assisted delivery, MVA for incomplete
abortion

District hospital level (comprehensive EOC)
General physicians and nurses
Blood transfusion, intravenous antibiotics, MVA for
incomplete abortion,
Surgical obstetrics – Caesarean section, repair of
vaginal, cervical or perineal tears or episiotomies
etc.
Neonatal resuscitation
Anaesthesia

Post-Natal Care…
Also, Postpartum Care
Care of the mother after delivery
Objectives…
To assess a woman in the postpartum period
properly
To be able to recognize and respond to
abnormalities recognized in the postpartum
period
To give proper counseling to postpartum
mothers
Schedule Return Visits
All postpartum women should have at least 2 routine postpartum visits
1st visit: 1st week postpartum, preferably within 48 -72 hours.
2nd visit 6 weeks postpartum
Women who do not return for postpartum visits should be visited at home

Components of Postpartum Care Visit
Early detection and management of
complications
Complication readiness
Promoting health and preventing disease
Woman-centered education and counseling

Steps to follow in Post partum care
1) Assess for emergency signs.
Vaginal bleeding
Fever
Pallor
Looks very ill
* Do not make a very sick woman wait, attend her
immediately.
2) Greet the mother. Make her feel comfortable
3) Assess breastfeeding
When, where delivered
Is there any difficulty?
Painful breast/abdomen? Fever?
Hard to void urine?/ Hard to pass stools?
Bleeding since delivery
Family Planning?
Other concerns?
Check records: complications, treatment during delivery?
Assess…
Postpartum Care
Providing GOOD CARE during
postpartum visit:
Make the woman comfortable
Tell the woman you will examine her
Wash your hands before and after
examining woman.
Maintain privacy
Inform and explain findings to woman

Is there any difficulty breastfeeding?
Observe how mother breastfeeds for at least
4 minutes
Is baby positioned well?
Is baby sucking effectively?
Assess breastfeeding…
Routine Postpartum Care
Mother feels well
BP, pulse & temperature
normal
No breast problems,
breastfeeding well
Uterus well contracted
No problem with urination
No pain or other concern
Give any treatment
or prophylaxis due
Iron
Vitamin A
Tetanus
Advise and Counsel
Health education
Schedule return visit
Abnormalities in Postpartum Period...
Elevated BP
Pallor
Vaginal Bleeding
Foul smelling lochia
Dribbling Urine
Pus or perineal pain
Feeling unhappy
Vaginal discharge
Breast Problem
Infection/ Breast abscess
Sore or cracked nipple
Engorgement
Insufficient milk
Cough or breathing
difficulty
REFER

ADVISE AND COUNSEL…
Postpartum care and hygiene
Wash hands before handling baby
Wash perineum daily
Have enough rest and sleep
Nutrition
Eat a greater amount and variety of healthy foods
Spend more time on nutrition counselling with thin women and adolescents.
Importance, benefits and management of breastfeeding
Teach correct positioning and attachment for
breastfeeding
Support exclusive breastfeeding for the first 6 months of
life
Encourage breastfeeding on demand
Need to avoid supplementary feeds
Encourage Breastfeeding
Counsel on importance of family planning
Inform about all contraceptive choices in postpartum
period (ideally done antenatal)
Facilitate free informed choice for all women
Reinforce that non-hormonal methods (LAM, barrier
methods, IUD and sterilization) are best options for
lactating mothers
Discuss other method options for the breastfeeding &
non-breastfeeding woman
Birth Spacing & Family Planning…

PRE / POST ABORTION CARE FOR
COMPLICATIONS
Create awareness about dangers of abortion
Detection and early management of complications of
abortion
Counseling to post abortion cases including advice
regarding FP to avoid recurrence.
INFANT HEALTH CARE
Resuscitation of the newborn.
Early and exclusive breastfeeding.
Management of infection (ophthalmia
neonatorum and cord infections).
Congenital abnormalities.
LBW and malnutrition management.
Weaning.
Safe and aseptic circumcision
Immunization.

PREVENTION AND MANAGEMENT OF STDs AND
HIV/AIDS
Information for prevention
Screening and management

DETECTION OF CANCER
BREAST
Inform and train for self examination.
Early detection and management.
Screening for breast lumps.
Supporting, counseling, rehabilitation.
CERVEX
Pap smear.
Early detection and management.

Levels and Practices of RHTertiary Level
(Teaching, Specialist Hosp)
Gynecologists, pediatricians
all services
Secondary Level
(Tehsil and Dirtrict Hosp)
Doctors, antenatal, postnatal, family planning, immunization,
normal/complicated delivery
Primary Level
(BHUs and RHCs)
LHVs, TBAs, Doctors, antenatal,
Postnatal, family planning, immunization
Normal dilivery
Community
TBA’s LHVs, Midwives
Antenatal, Postnatal, Family Planning, immunization

FACTORS INFLUENCING
PROVISION OF RH SERVICES
Number of service delivery points
Geographical, physical and social
accessibility
Proper advertisement of services
Quality of care

Case Studies…
Mumtaz et al. BMC International Health and Human
Rights 2011, 11(Suppl 2):S4
http://www.biomedcentral.com/1472-698X/11/S2/S4

Case study 1 - Shida

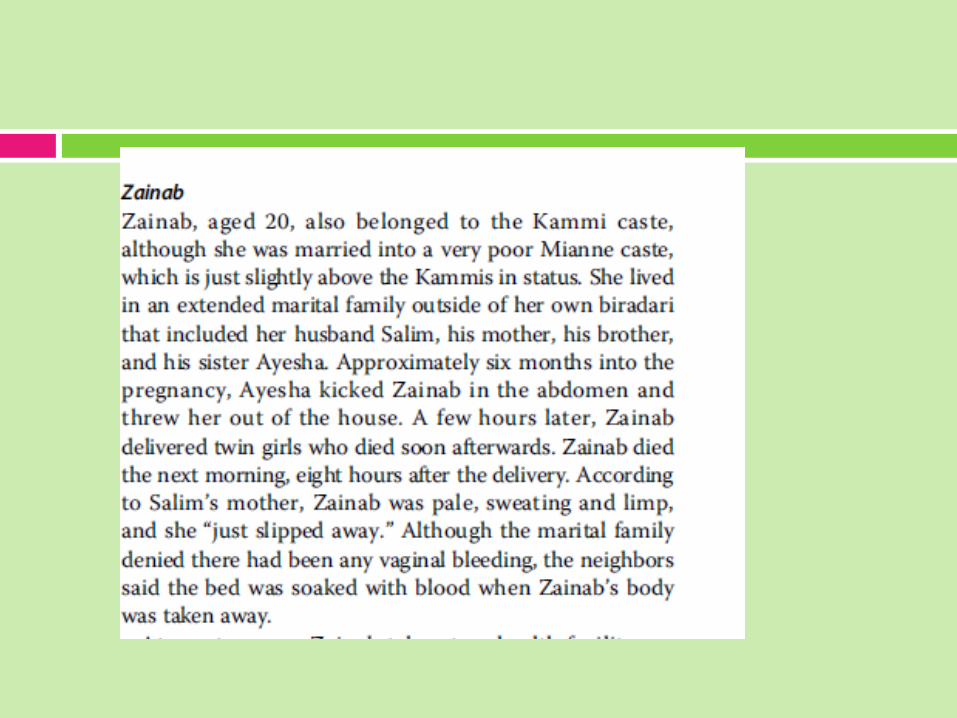
Case study 2 - Zainab

Findings
• Five maternal deaths in the last 5 years in a population of less than 2000 people.
• Despite availability of health services that include
1. Qualified physician - private clinic 20 minute drive
2. Two rural health centres - 20 minutes.
3. Basic health unit - 15 minute drive.
4. Large district hospital - 90 minute drive.

Discussion
Objective of this research is to explore the underlying
contextual factors that explain why some women
experience adverse maternal outcomes, while others do
not.
See that despite differences in details, the stories of
Zainab and Shida illustrate how rigidly structured castes,
poverty and gendered devaluating of women prevent
women from using lifesaving health services right at their
disposal

Caste and poverty
Both women belonged to lower
castes
Both women were Kammi, although
Zainab was married into a poor Mianne
family
Of the five maternal deaths in the village,
4 were Kammi women and one Mirza
Caste and poverty
Both women were poor
Data show poverty is not merely inherited or
accidental, but the consequence of numerous
structural factors intersecting to create and
perpetuate economic and social vulnerability in
certain groups of people
Chronic poverty and low castes act synergistically

Gender
Gender inequalities also emerge in
these case studies
Domestic violence is a gendered phenomena and
violence during pregnancy well documented
Serves to perpetuate male power and is sustained by a
culture of silence and denial of the seriousness of the
health consequences of the abuse

Reference
Mumtaz et al. BMC International Health and Human Rights 2011, 11(Suppl
2):S4 http://www.biomedcentral.com/1472-698X/11/S2/S4
Safe Motherhood: a brief history of the global movement 1947–2002
Carla AbouZahr World Health Organization, Geneva, Switzerland
file:///C:/Users/durdana/Desktop/PMC/Lectures/4th%20year%20MBBS
/Reproductive%20Health/History%20of%20safe%20motherhood.pdf
Thank You