introduction to the sts national database series · of these three specialty databases). these six...
TRANSCRIPT

OUTCOMES ANALYSIS, QUALITY IMPROVEMENT, AND PATIENT SAFETY
Introduction to the STS National Database Series:Outcomes Analysis, Quality Improvement, andPatient SafetyJeffrey P. Jacobs, MD, David M. Shahian, MD, Richard L. Prager, MD,Fred H. Edwards, MD, Donna McDonald, RN, MPH, Jane M. Han, MSW,Richard S. D’Agostino, MD, Marshall L. Jacobs, MD, Benjamin D. Kozower, MD,Vinay Badhwar, MD, Vinod H. Thourani, MD, Henning A. Gaissert, MD,Felix G. Fernandez, MD, Cam Wright, MD, James I. Fann, MD, Gaetano Paone, MD,Juan A. Sanchez, MD, Joseph C. Cleveland, Jr, MD, J. Matthew Brennan, MD,Rachel S. Dokholyan, MPH, Sean M. O’Brien, PhD, Eric D. Peterson, MD, MPH,Frederick L. Grover, MD, and G. Alexander Patterson, MDDivision of Cardiac Surgery, Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, Maryland (JPJ, MLJ,JAS); Division of Cardiovascular Surgery, Department of Surgery, Johns Hopkins All Children’s Heart Institute, All Children’s Hospitaland Florida Hospital for Children, Saint Petersburg, Tampa, and Orlando, Florida (JPJ, MLJ); Massachusetts General Hospital, HarvardMedical School, Boston, Massachusetts (DMS, CW, HAG); University of Michigan, Ann Arbor, Michigan (RLP); University of FloridaCollege of Medicine, Jacksonville, Florida (FHE); The Society of Thoracic Surgeons, Chicago, Illinois (DM, JMH); Lahey Hospital andMedical Center, Burlington, Massachusetts (RSD); University of Virginia, Charlottesville, Virginia (BDK); University of PittsburghMedical Center, Pittsburgh, Pennsylvania (VB); Emory University, Atlanta, Georgia (VHT, FGF); Stanford University, Stanford,California (JIF); Henry Ford Hospital, Detroit, Michigan (GP); University of Colorado, School of Medicine, Aurora, Colorado (JCC, FLG);Duke Clinical Research Institute, Duke University, Durham, North Carolina (JMB, RD, SMB, EDP); and Washington University Schoolof Medicine, St. Louis, Missouri (GAP)
The Society of Thoracic Surgeons (STS) National Data-base is the foundation for most of the Society’s quality,research, and patient safety activities. Beginning inJanuary 2016 and repeating each year, The Annals ofThoracic Surgery will publish a monthly Database seriesof scholarly articles on outcomes analysis, qualityimprovement, and patient safety. Six articles will bedirectly derived from the STS National Database and willbe published every other month: three articles on out-comes and quality (one each from the STS Adult CardiacSurgery Database, the STS Congenital Heart SurgeryDatabase, and the STS General Thoracic Surgery
Accepted for publication Oct 15, 2015.
Address correspondence to Dr Jeffrey P. Jacobs, Division of Cardiovas-cular Surgery, John Hopkins All Children’s Heart Institute, 601 Fifth St S,Saint Petersburg, FL 33701; e-mail: [email protected].
� 2015 by The Society of Thoracic SurgeonsPublished by Elsevier
Database), and three articles on research (one from eachof these three specialty databases). These six articles willalternate with five additional articles on topics relatedto patient safety. The final article, to be published inDecember, will provide a summary of the prior 11 man-uscripts. This series will allow STS and its Workforces onNational Databases, Research Development, and PatientSafety to convey timely information aimed at improvingthe quality and safety of cardiothoracic surgery.
(Ann Thorac Surg 2015;100:1992–2000)� 2015 by The Society of Thoracic Surgeons
he art and science of outcomes analysis, quality
Timprovement, and patient safety continue to evolve atan increasingly rapid pace, and cardiothoracic surgeryleads many of these advances. The Society of ThoracicSurgeons (STS) National Database is one of the principalreasons for this leading role, as it provides a platformfor the generation of important new knowledge in all ofthese domains.In order to care for patients and to be successful intoday’s rapidly evolving health care environment, un-derstanding these topics is an essential professional
responsibility of all cardiothoracic surgeons. Therefore,beginning in January 2016, The Annals of Thoracic Surgerywill publish a monthly series of scholarly articles onoutcomes analysis, quality improvement, and patientsafety. Some of these articles will be based on the STSNational Database and others will derive from a variety ofrelated areas, such as the learning sciences. The purposeof this article is to present general background informa-tion about the STS National Database and to describe theplanned content of this monthly series of articles.
The Society of Thoracic Surgeons NationalDatabase
The STS National Database was established in 1989 asan initiative to enhance the quality and safety of
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2015.10.060
1993Ann Thorac Surg JACOBS ET AL2015;100:1992–2000 OUTCOMES, QUALITY, AND SAFETY
cardiothoracic surgery and to provide an accurate andvalid basis for measuring performance in our specialty. In2002, the STS National Database for Thoracic SurgeryCommittee and the STS Database Liaison Committeemerged to become the STS Workforce on National Da-tabases under the STS Council on Quality Assurance andPatient Advocacy (now the STS Council on Quality,Research, and Patient Safety) [1]. The STS NationalDatabase has thus far had five chairs: Richard E. Clark(1989–1997), Frederick L. Grover (1997–2004), Fred H.Edwards (2004–2010), David M. Shahian (2010–2015), andJeffrey P. Jacobs (2015–).
The STS National Database has three major compo-nent databases, each focusing on a different area ofcardiothoracic surgery: the STS Adult Cardiac SurgeryDatabase (ACSD), the STS Congenital Heart Surgery
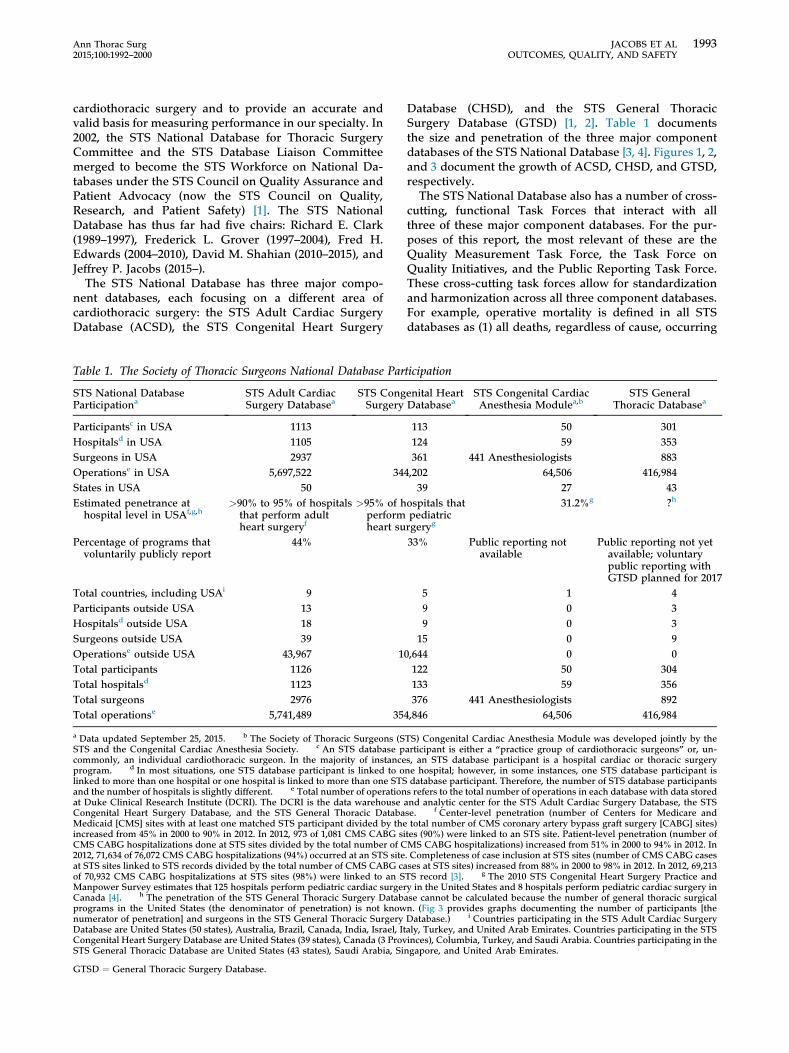
Table 1. The Society of Thoracic Surgeons National Database Par
STS National DatabaseParticipationa
STS Adult CardiacSurgery Databasea
STS CongSurgery
Participantsc in USA 1113Hospitalsd in USA 1105Surgeons in USA 2937Operationse in USA 5,697,522 34States in USA 50Estimated penetrance at
hospital level in USAf,g,h>90% to 95% of hospitals
that perform adultheart surgeryf
>95% of hperformheart su
Percentage of programs thatvoluntarily publicly report
44%
Total countries, including USAi 9Participants outside USA 13Hospitalsd outside USA 18Surgeons outside USA 39Operationse outside USA 43,967 1Total participants 1126Total hospitalsd 1123Total surgeons 2976Total operationse 5,741,489 35
a Data updated September 25, 2015. b The Society of Thoracic Surgeons (SSTS and the Congenital Cardiac Anesthesia Society. c An STS database pcommonly, an individual cardiothoracic surgeon. In the majority of instanceprogram. d In most situations, one STS database participant is linked to olinked to more than one hospital or one hospital is linked to more than one STSand the number of hospitals is slightly different. e Total number of operationat Duke Clinical Research Institute (DCRI). The DCRI is the data warehouseCongenital Heart Surgery Database, and the STS General Thoracic DatabaMedicaid [CMS] sites with at least one matched STS participant divided by theincreased from 45% in 2000 to 90% in 2012. In 2012, 973 of 1,081 CMS CABG siCMS CABG hospitalizations done at STS sites divided by the total number of C2012, 71,634 of 76,072 CMS CABG hospitalizations (94%) occurred at an STS siteat STS sites linked to STS records divided by the total number of CMS CABG caof 70,932 CMS CABG hospitalizations at STS sites (98%) were linked to an SManpower Survey estimates that 125 hospitals perform pediatric cardiac surgerCanada [4]. h The penetration of the STS General Thoracic Surgery Databprograms in the United States (the denominator of penetration) is not knownumerator of penetration] and surgeons in the STS General Thoracic SurgeryDatabase are United States (50 states), Australia, Brazil, Canada, India, Israel, ItCongenital Heart Surgery Database are United States (39 states), Canada (3 ProvSTS General Thoracic Database are United States (43 states), Saudi Arabia, Si
GTSD ¼ General Thoracic Surgery Database.
Database (CHSD), and the STS General ThoracicSurgery Database (GTSD) [1, 2]. Table 1 documentsthe size and penetration of the three major componentdatabases of the STS National Database [3, 4]. Figures 1, 2,and 3 document the growth of ACSD, CHSD, and GTSD,respectively.The STS National Database also has a number of cross-
cutting, functional Task Forces that interact with allthree of these major component databases. For the pur-poses of this report, the most relevant of these are theQuality Measurement Task Force, the Task Force onQuality Initiatives, and the Public Reporting Task Force.These cross-cutting task forces allow for standardizationand harmonization across all three component databases.For example, operative mortality is defined in all STSdatabases as (1) all deaths, regardless of cause, occurring
ticipation
enital HeartDatabasea
STS Congenital CardiacAnesthesia Modulea,b
STS GeneralThoracic Databasea
113 50 301124 59 353361 441 Anesthesiologists 883
4,202 64,506 416,98439 27 43
ospitals thatpediatricrgeryg
31.2%g ?h
33% Public reporting notavailable
Public reporting not yetavailable; voluntarypublic reporting withGTSD planned for 2017
5 1 49 0 39 0 315 0 9
0,644 0 0122 50 304133 59 356376 441 Anesthesiologists 892
4,846 64,506 416,984
TS) Congenital Cardiac Anesthesia Module was developed jointly by thearticipant is either a “practice group of cardiothoracic surgeons” or, un-s, an STS database participant is a hospital cardiac or thoracic surgeryne hospital; however, in some instances, one STS database participant isdatabase participant. Therefore, the number of STS database participantss refers to the total number of operations in each database with data storedand analytic center for the STS Adult Cardiac Surgery Database, the STSse. f Center-level penetration (number of Centers for Medicare andtotal number of CMS coronary artery bypass graft surgery [CABG] sites)tes (90%) were linked to an STS site. Patient-level penetration (number ofMS CABG hospitalizations) increased from 51% in 2000 to 94% in 2012. In. Completeness of case inclusion at STS sites (number of CMS CABG casesses at STS sites) increased from 88% in 2000 to 98% in 2012. In 2012, 69,213TS record [3]. g The 2010 STS Congenital Heart Surgery Practice andy in the United States and 8 hospitals perform pediatric cardiac surgery inase cannot be calculated because the number of general thoracic surgicaln. (Fig 3 provides graphs documenting the number of participants [theDatabase.) i Countries participating in the STS Adult Cardiac Surgeryaly, Turkey, and United Arab Emirates. Countries participating in the STSinces), Columbia, Turkey, and Saudi Arabia. Countries participating in thengapore, and United Arab Emirates.

Fig 1. Increasing center level pene-tration in The Society of ThoracicSurgeons (STS) Adult Cardiac Sur-gery Database (ACSD). This graphonly provides data through 2012because, at the time this article waswritten, 2012 was the last year ofavailable linked data from the link-age of STS ACSD and the Centers forMedicare and Medicaid (CMS)Medicare database. Linkage for 2013data is now under way and willlikely show continued increasingpenetration [3]. (The data in thisgraph is derived from the followingarticle that is in press: Jacobs JP,Shahian DM, He X, et al. Penetra-tion, completeness, and representa-tiveness of the STS database. AnnThorac Surg 2016;101, by permissionof Elsevier.)
1994 JACOBS ET AL Ann Thorac SurgOUTCOMES, QUALITY, AND SAFETY 2015;100:1992–2000
during the hospitalization in which the operation wasperformed, even if after 30 days (including patientstransferred to other acute care facilities); and (2) alldeaths, regardless of cause, occurring after dischargefrom the hospital, but before the end of the 30th post-operative day [5, 6].
Finally, joined with the STS Workforce on NationalDatabases, under the umbrella of the STS Council onQuality, Research, and Patient Safety, are two otherworkforces that interact closely with the database andwhich will also contribute to this series of articles: theSTS Workforce on Patient Safety, and the STS Workforceon Research Development. Figure 4 provides an organi-zational chart for the STS Council on Quality, Research,and Patient Safety.
Fig 2. Annual growth of The Societyof Thoracic Surgeons (STS)Congenital Heart Surgery Databaseby number of participating centerssubmitting data. The aggregatefeedback report from Spring 2015harvest of the STS Congenital HeartSurgery Database includes data from116 North American congenitaldatabase participants representing127 congenital heart surgery hospi-tals in North America, 124 in theUnited States and 3 in Canada.
All three component databases of the STS NationalDatabase support outcomes analysis, quality improve-ment, and research. The leadership of STS in thearea of quality measurement is demonstrated by thecommitment of STS to obtain endorsement for all itsperformance measures by the National Quality Forum(NQF). The NQF is a multiple stakeholder, nonprofit,membership-based organization that aims to improvethe quality of health care through the preferential useof only the most valid performance measures.NQF endorsement is the gold standard for health carequality measures, and NQF-endorsed measures arerecognized by the national health care communityas “best in class,” evidence-based, and valid. The STShas developed 34 quality measures that are endorsed

Fig 3. Increasing participation inThe Society of Thoracic Surgeons(STS) General Thoracic SurgeryDatabase. (A) Participating centers.(B) Participating surgeons. Note:number of surgeons counts surgeon/participant pairs; if a single surgeonis associated with more than oneparticipant, he or she is counted morethan once in this total.
Fig 4. Organizational chart for TheSociety of Thoracic Surgeons (STS)Council on Quality, Research, andPatient Safety. (TF ¼ Task Force;WF ¼ Workforce.)
1995Ann Thorac Surg JACOBS ET AL2015;100:1992–2000 OUTCOMES, QUALITY, AND SAFETY

1996 JACOBS ET AL Ann Thorac SurgOUTCOMES, QUALITY, AND SAFETY 2015;100:1992–2000
by NQF (Table 2), and STS is currently the steward formore NQF-endorsed measures than any other specialty-based medical professional organization (Table 3).
In this upcoming monthly series of scholarly articles inThe Annals of Thoracic Surgery, six of the 12 articles will bederived directly from the STS National Database. Threetimes per year (once each for ACSD, CHSD, and GTSD),a review manuscript in The Annals of Thoracic Surgerywill summarize current national aggregate outcomes andall quality measurement and improvement initiativesfrom each database over the past 12 months. Threeadditional review articles each year (one each for ACSD,CHSD, and GTSD) will summarize all research-relatedmanuscripts published from each database over the past12 months, along with an update on funded research
Table 2. National Quality Forum Endorsed Measures of The Socie
No. NQF No. Meas
1 0113 Participation in a systematic database for card2 0114 Risk-adjusted postoperative renal failure3 0115 Risk-adjusted surgical reexploration4 0116 Antiplatelet medication at discharge5 0117 Beta-blockade at discharge6 0118 Antilipid treatment at discharge7 0119 Risk-adjusted operative mortality for CABG8 0120 Risk-adjusted operative mortality for AVR9 0121 Risk-adjusted operative mortality for MV repla10 0122 Risk-adjusted operative mortality for MV repla11 0123 Risk-adjusted operative mortality for AVR þ C12 0126 Selection of antibiotic prophylaxis for cardiac s13 0127 Preoperative beta-blockade14 0128 Duration of antibiotic prophylaxis for cardiac s15 0129 Risk-adjusted postoperative prolonged intubat16 0130 Risk-adjusted deep sternal wound infection17 0131 Risk-adjusted stroke/cerebrovascular accident18 0134 Use of internal mammary artery in CABG19 0455 Recording of clinical stage before surgery for l20 0456 Participation in a systematic national database21 0457 Recording of performance status before lung o22 0459 Risk-adjusted morbidity: length of stay >14 da23 0460 Risk-adjusted morbidity and mortality for esop24 0696 STS CABG composite score25 0732 Surgical volume for pediatric and congenital h
programmatic volume stratified by the 5 ST26 0733 Operative mortality stratified by the 5 STAT m27 0734 Participation in a national database for pediatr28 1501 Risk-adjusted operative mortality for MV repa29 1502 Risk-adjusted operative mortality for MV repa30 1790 Risk-adjusted morbidity and mortality for lung31 2514 Risk-adjusted CABG readmission rate32 2561 STS AVR composite score33 2563 STS AVR þ CABG composite score34 2683 Risk-adjusted operative mortality for pediatric
a Data extracted from National Quality Forum Quality Positioning System; Sep
AVR ¼ aortic valve replacement; CABG ¼ coronary artery bypass graftSTAT ¼ The Society of Thoracic Surgeons (STS)—European Association forCategories; STS ¼ The Society of Thoracic Surgeons.
grants and grant proposals from that particular database.Research from the STS National Database has led toseveral hundred peer-reviewed publications. Figures 5, 6,and 7 demonstrate the type of research that can begenerated using ACSD, CHSD, and GTSD, respectively[7–10].
Planned Content for The Annals of Thoracic SurgerySTS National Database Monthly Series of Articles:Outcomes Analysis, Quality Improvement, andPatient Safety
The STS National Database monthly series of articleson outcomes analysis, quality improvement, and patientsafety will repeat each year over a 12-month cycle,
ty of Thoracic Surgeonsa
ure Title Domain
iac surgery AdultAdultAdultAdultAdultAdultAdultAdult
cement Adultcement þ CABG surgery AdultABG surgery Adulturgery patients Adult
Adulturgery patients Adultion (ventilation) Adult
AdultAdultAdult
ung cancer or esophageal cancer resection Adultfor general thoracic surgery Thoracicr esophageal cancer resection Thoracicys after elective lobectomy for lung cancer Thoracichagectomy for cancer Thoracic
Adulteart surgery: total programmatic volume andAT mortality categories
Congenital
ortality categories Congenitalic and congenital heart surgery Congenitalir Adultir þ CABG surgery Adultresection for lung cancer Thoracic
AdultAdultAdult
and congenital heart surgery Congenital
tember 28, 2015 (11:48 AM); www.qualityforum.org/qps.
surgery; MV ¼ mitral valve; NQF ¼ National Quality Forum;Cardio-Thoracic Surgery (EACTS) Congenital Heart Surgery Mortality
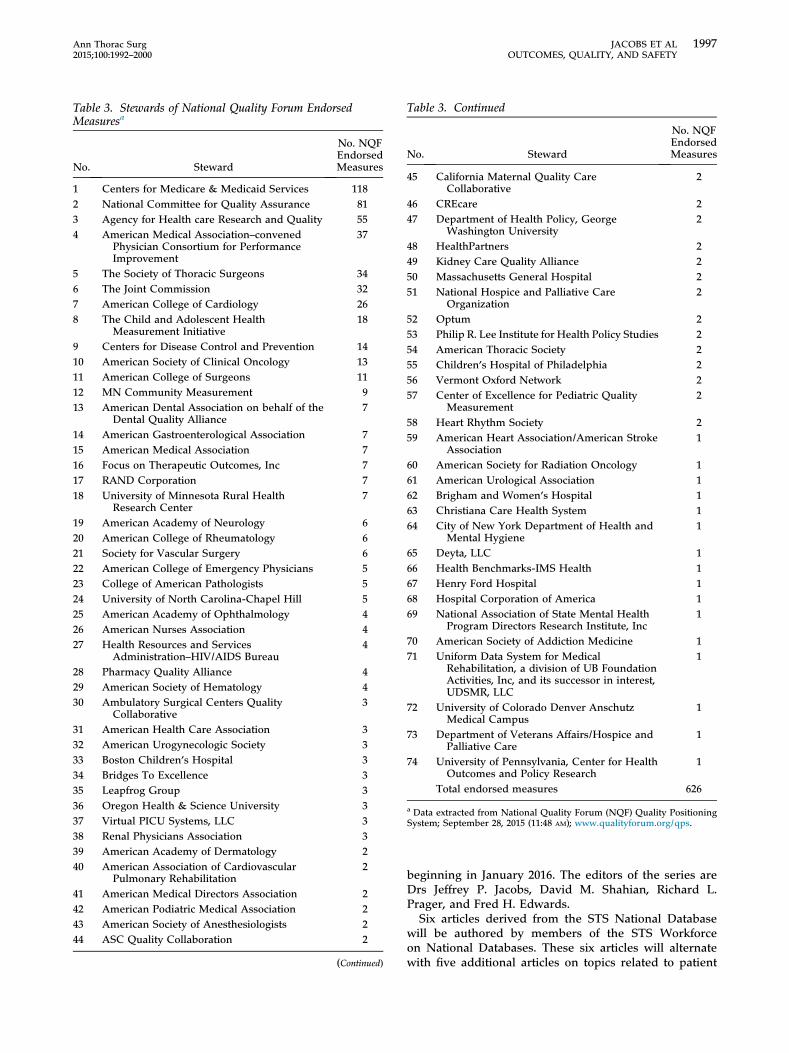
Table 3. Stewards of National Quality Forum EndorsedMeasuresa
No. Steward
No. NQFEndorsedMeasures
1 Centers for Medicare & Medicaid Services 1182 National Committee for Quality Assurance 813 Agency for Health care Research and Quality 554 American Medical Association–convened
Physician Consortium for PerformanceImprovement
37
5 The Society of Thoracic Surgeons 346 The Joint Commission 327 American College of Cardiology 268 The Child and Adolescent Health
Measurement Initiative18
9 Centers for Disease Control and Prevention 1410 American Society of Clinical Oncology 1311 American College of Surgeons 1112 MN Community Measurement 913 American Dental Association on behalf of the
Dental Quality Alliance7
14 American Gastroenterological Association 715 American Medical Association 716 Focus on Therapeutic Outcomes, Inc 717 RAND Corporation 718 University of Minnesota Rural Health
Research Center7
19 American Academy of Neurology 620 American College of Rheumatology 621 Society for Vascular Surgery 622 American College of Emergency Physicians 523 College of American Pathologists 524 University of North Carolina-Chapel Hill 525 American Academy of Ophthalmology 426 American Nurses Association 427 Health Resources and Services
Administration–HIV/AIDS Bureau4
28 Pharmacy Quality Alliance 429 American Society of Hematology 430 Ambulatory Surgical Centers Quality
Collaborative3
31 American Health Care Association 332 American Urogynecologic Society 333 Boston Children’s Hospital 334 Bridges To Excellence 335 Leapfrog Group 336 Oregon Health & Science University 337 Virtual PICU Systems, LLC 338 Renal Physicians Association 339 American Academy of Dermatology 240 American Association of Cardiovascular
Pulmonary Rehabilitation2
41 American Medical Directors Association 242 American Podiatric Medical Association 243 American Society of Anesthesiologists 244 ASC Quality Collaboration 2
(Continued)
Table 3. Continued
No. Steward
No. NQFEndorsedMeasures
45 California Maternal Quality CareCollaborative
2
46 CREcare 247 Department of Health Policy, George
Washington University2
48 HealthPartners 249 Kidney Care Quality Alliance 250 Massachusetts General Hospital 251 National Hospice and Palliative Care
Organization2
52 Optum 253 Philip R. Lee Institute for Health Policy Studies 254 American Thoracic Society 255 Children’s Hospital of Philadelphia 256 Vermont Oxford Network 257 Center of Excellence for Pediatric Quality
Measurement2
58 Heart Rhythm Society 259 American Heart Association/American Stroke
Association1
60 American Society for Radiation Oncology 161 American Urological Association 162 Brigham and Women’s Hospital 163 Christiana Care Health System 164 City of New York Department of Health and
Mental Hygiene1
65 Deyta, LLC 166 Health Benchmarks-IMS Health 167 Henry Ford Hospital 168 Hospital Corporation of America 169 National Association of State Mental Health
Program Directors Research Institute, Inc1
70 American Society of Addiction Medicine 171 Uniform Data System for Medical
Rehabilitation, a division of UB FoundationActivities, Inc, and its successor in interest,UDSMR, LLC
1
72 University of Colorado Denver AnschutzMedical Campus
1
73 Department of Veterans Affairs/Hospice andPalliative Care
1
74 University of Pennsylvania, Center for HealthOutcomes and Policy Research
1
Total endorsed measures 626
a Data extracted from National Quality Forum (NQF) Quality PositioningSystem; September 28, 2015 (11:48 AM); www.qualityforum.org/qps.
1997Ann Thorac Surg JACOBS ET AL2015;100:1992–2000 OUTCOMES, QUALITY, AND SAFETY
beginning in January 2016. The editors of the series areDrs Jeffrey P. Jacobs, David M. Shahian, Richard L.Prager, and Fred H. Edwards.Six articles derived from the STS National Database
will be authored by members of the STS Workforceon National Databases. These six articles will alternatewith five additional articles on topics related to patient

Fig 5. Observed and expected mor-tality rates, observed to expected (O/E)ratios, and prevalence of six majorrisk factors, by quarter, 2004 to 2014,in the STS Adult Cardiac SurgeryDatabase [7]. (Republished fromShahian DM, Grover FL, Prager RL,et al. The Society of Thoracic Sur-geons voluntary public reportinginitiative: the first 4 years. Ann Surg2015;262, by permission of WoltersKlower Health; permission conveyedthrough Copyright Clearance Center,Inc.)
1998 JACOBS ET AL Ann Thorac SurgOUTCOMES, QUALITY, AND SAFETY 2015;100:1992–2000
safety that will be authored by members of theSTS Workforce on Patient Safety, under the leadershipof James I. Fann (Chair, STS Workforce on PatientSafety). The final article (for publication in December)will provide a summary of the prior 11 manuscripts.
Fig 6. (A) Estimated adjustedodds ratios for in-hospital mor-tality by week of gestational age atbirth (reference, 39.5 weeks) andpiecewise 95% confidence in-tervals (shaded area) [8]. (B)Estimated adjusted ratios of me-dians of postoperative length ofstay (reference, 39.5 weeks) andpiecewise 95% confidence in-tervals (shaded area) [8]. (Repub-lished from Costello JM, PasqualiSK, Jacobs JP, et al. Gestationalage at birth and outcomes afterneonatal cardiac surgery: ananalysis of The Society ofThoracic Surgeons CongenitalHeart Surgery Database. Circula-tion 2014;129:2511–7, by permis-sion of Wolters Klower Health.)
SummaryThe STS National Database is one of the leading clinicalregistries in the world. This series of articles will allowSTS and the STS Workforces on National Databases,Research Development, and Patients Safety to convey

Fig 7. (A) The standardized inci-dence ratio of mortality or majormorbidity after lung cancer resec-tion among The Society ofThoracic Surgeons (STS) partici-pating sites [9]. (Reprinted fromKozower BD, Sheng S, O’BrienSM, et al. STS database riskmodels: predictors of mortality andmajor morbidity for lung cancerresection. Ann Thorac Surg2010;90, by permission ofElsevier.) (B) Risk-adjusted ratesof morbidity after esophagectomyfor cancer among STS partici-pating sites [10]. (Reprinted fromWright CD, Kucharczuk JC,O’Brien SM, et al. Predictors ofmajor morbidity and mortalityafter esophagectomy for esopha-geal cancer: a Society of ThoracicSurgeons General Thoracic Sur-gery Database risk adjustmentmodel. J Thorac Cardiovasc Surg2009;137, by permission ofElsevier.)
1999Ann Thorac Surg JACOBS ET AL2015;100:1992–2000 OUTCOMES, QUALITY, AND SAFETY
timely summaries of important topics related to out-comes, quality, and safety. The members of these Work-forces would like to thank G. Alexander Patterson, Editorof The Annals of Thoracic Surgery, for the opportunity topublish this monthly series of articles.
References
1. Grover FL, Shahian DM, Clark RE, Edwards FH. The STSNational Database. Ann Thorac Surg 2014;97(Suppl):48–54.
2. STS National Database. Available at: http://www.sts.org/national-database. Accessed September 28, 2015.
3. Jacobs JP, Shahian DM, He X, et al. Penetration, complete-ness, and representativeness of the STS database. AnnThorac Surg 2016;101 (in press).
4. Jacobs ML, Daniel M, Mavroudis C, et al. Report of the 2010Society of Thoracic Surgeons congenital heart surgery prac-tice and manpower survey. Ann Thorac Surg 2011;92:762–9.
5. Jacobs JP, Mavroudis C, Jacobs ML, et al. What is operativemortality? Defining death in a surgical registry database: areport from the STS Congenital Database Task Force and theJoint EACTS-STS Congenital Database Committee. AnnThorac Surg 2006;81:1937–41.
6. Overman D, Jacobs JP, Prager RL, et al. Report from TheSociety of Thoracic Surgeons National Database Work Force:

2000 JACOBS ET AL Ann Thorac SurgOUTCOMES, QUALITY, AND SAFETY 2015;100:1992–2000
clarifying the definition of operative mortality. World JPediatr Congenit Heart Surg 2013;4:10–2.
7. Shahian DM, Grover FL, Prager RL, et al. The Society ofThoracic Surgeons voluntary public reporting initiative: thefirst 4 years. Ann Surg 2015;262:526–35.
8. Costello JM, Pasquali SK, Jacobs JP, et al. Gestationalage at birth and outcomes after neonatal cardiac sur-gery: an analysis of The Society of Thoracic Surgeonscongenital heart surgery database. Circulation 2014;129:2511–7.
9. Kozower BD, Sheng S, O’Brien SM, et al. STS database riskmodels: predictors of mortality and major morbidity for lungcancer resection. Ann Thorac Surg 2010;90:875–83.
10. Wright CD, Kucharczuk JC, O’Brien SM, Grab JD, Allen MS,for The Society of Thoracic Surgeons General ThoracicSurgery Database. Predictors of major morbidity and mor-tality after esophagectomy for esophageal cancer: a Societyof Thoracic Surgeons general thoracic surgery databaserisk adjustment model. J Thorac Cardiovasc Surg 2009;137:587–96; [Erratum in: J Thorac Cardiovasc Surg 2009;137:1581].