intubation success rates by a children’s hospital ... · prior research on tracheal intubation...
TRANSCRIPT
CentralBringing Excellence in Open Access
Archives of Emergency Medicine and Critical Care
Cite this article: Dugan MC, Hebbar KB, Leong T, Callis AC, Petrillo TM (2017) Intubation Success Rates by a Children’s Hospital Transport Team. Arch Emerg Med Crit Care 2(3): 1028.
*Corresponding authorMark C. Dugan, Pediatric Critical Care, 4th Floor – Trauma Building, 1800 W. Charleston Blvd, Las Vegas, NV 89102, USA, Email:
Submitted: 01 August 2017
Accepted: 04 September 2017
Published: 06 September 2017
ISSN: 2476-2016
Copyright© 2017 Dugan et al.
OPEN ACCESS
Keywords•Pediatric•Intubation•Critical care transport
Research Article
Intubation Success Rates by a Children’s Hospital Transport TeamMark C. Dugan1,2*, Kiran B. Hebbar3,4,6, Traci Leong5, Amy C. Callis6, and Toni M. Petrillo3,4,6
1Division of Pediatric Critical Care, Children’s Hospital of Nevada at UMC, USA 2Department of Pediatrics, University of Nevada Las Vegas School of Medicine, USA3Division of Pediatric Critical Care, Emory University School of Medicine, USA4Department of Pediatrics, Emory University School of Medicine, USA5Department of Biostatistics and Bioinformatics, Emory University School of Public Health, USA6Children’s Healthcare of Atlanta, Atlanta, USA
Abstract
Objectives: Prior research on tracheal intubation (TI) of pediatric patients demonstrates highly variable success rates. We hypothesize that overall intubation and first-attempt success of our children’s critical care transport team is high, and, in the rare event of intubation failure, pediatric airways can be successfully managed with available extra-glottic devices.
Methods: Retrospective chart review of a children’s hospital-based pediatric/neonatal critical care transport team (CCT). All pediatric/neonatal patients in whom intubation was attempted by the CCT during the 34-month study period (January 2011—October 2013) were included.
Results: Overall success of pediatric TI was confirmed in 140/146 patients (96%) while first-attempt success was 72%. Six patients were not able to be intubated by the team, 4 of these patients were intubated by an alternate provider. The other two patients were managed through use of a laryngeal mask airway (LMA). 79% of patients (115/146) had no TI attempts by referring hospital prior to CCT’s arrival. Of these, CCT successfully intubated 99% (114/115) of patients. 21% of patients (31/146) had failed TI attempts by referring hospital physicians, and CCT’s success rate after failed attempts by referring hospital physicians was 84% (p = .00015). Patients successfully intubated on a first attempt were significantly older than patients requiring multiple attempts. Of patients requiring multiple attempts, the average number of attempts was 2.2 (SD 0.41).
Conclusions: Pediatric TI performed by an experienced children’s CCT has an excellent success rate. Despite failed intubation attempts by referring providers, the CCT still maintained a high success rate at pediatric TI.
INTRODUCTIONTracheal intubation (TI) is performed by a variety of
providers in emergency medical service (EMS) systems. Current controversy exists regarding the safety and efficacy of EMS providers performing TI in the pediatric population [1-3]. Published literature surrounding prehospital pediatric intubation reveals highly variable proficiency [4-10], with one large study demonstrating an overall success rate of just 57% and complications, such as esophageal intubation or unrecognized tube dislodgement, resulting in an increase in mortality of 3% [11]. Due to varying success rates, some experts have gone as far as to advocate abandoning prehospital intubation in favor of methods of non-invasive respiratory support [2]. Small studies have supported these non-invasive methods and suggest that bag-valve-mask ventilation may be equivalent to tracheal intubation for hypoxic or hypopneic children [2,12]. Others have advocated for allowing intubation by prehospital providers when supervised by either trained emergency medicine or other physicians with airway expertise [13,14].
Once patients have arrived at an emergency department, pediatric patients remain at risk for adverse events related to TI attempts. As with any skill, pediatric intubation is a skill that deteriorates with lack of repetition [15-17]. By itself, differences in a child’s age presents the practitioner highly variable baseline anatomy and physiology, with younger patients having reduced functional residual capacity, relatively larger tongues, in addition to a more cephalad and anterior position of their airway. Unique pediatric co-morbid conditions coupled with limited exposure to pediatric patients make proficiency with pediatric TI a challenge for even pediatric emergency medicine providers [18]. Mittiga and colleagues note that in their tertiary pediatric emergency department there was minimal exposure per provider to advanced procedures such as intubation, a problem exacerbated in a primarily adult-based emergency department [18]. Anecdotally, physicians who primarily care for adults in our region have begun to defer intubation until a dedicated pediatric transport team can assume care.

CentralBringing Excellence in Open Access
Dugan et al. (2017)Email:
Arch Emerg Med Crit Care 2(3): 1028 (2017) 2/6
Pediatric critical care transport teams are becoming a larger part of the healthcare team, and as such have been tracking their quality metrics [19]. Prior reports of dedicated pediatric transport team TI successes and failure are few [20,21], with only one study specifically examining risk factors for failed TI. This literature noted specific risk factors for intubation failure such as age of the patient, use of an uncuffed tracheal tube (OR 6.85), and the presence of comorbid conditions [22]. The primary objective of this study is to assess the performance of a single pediatric critical care transport team (CCT), specifically with regard to pediatric TI success and failure. Secondary objectives include describing factors contributing to the success and failure of TI, including patient demographics and underlying medical conditions. We hypothesize that first-attempt and overall intubation success of our CCT is high.
MATERIALS & METHODSThis was a retrospective cross-sectional descriptive study
of pediatric/neonatal patients in whom tracheal intubation was attempted by a children’s hospital-based pediatric/neonatal critical care team (CCT) during a 34-month study period (January 2011 - October 2013).This study was approved by the Children’s Healthcare of Atlanta IRB prior to data collection, and a waiver for informed consent was granted. Patients were identified from a standard “intubation form” collected on all tracheal intubations and tracheal intubation attempts by the CCT. These forms are kept in addition to the transport chart. Additional variables were gathered from the CCT transport paper charts including patient demographics, mode of transportation, primary and secondary diagnosis when available, conditions surrounding intubation, TI attempts by prior medical professionals, the demographics of the CCT airway operator and overall success rates. Chart reviews were not blinded, however accuracy of the data assurance was addressed by performing separate chart reviews by a secondary observer.
Children’s transport team performs greater than 5000 patient transports annually, of which approximately 700 are transported via rotor-craft. The CCT operates a two-tier emergency response system, with the mode of transport determined by the referring institution in consultation with the accepting physician. The ground CCT consists of a paramedic with pediatric experience (EMT-P), a nurse with pediatric critical care or emergency medicine training (RN), and a basic life support (BLS) skilled emergency medical technician (EMT-B). In addition, when dictated by a validated transport pediatric early warning score (T-PEWS; scale of 0-9, 9 representing the most critically ill) [23], a respiratory therapist (RCP) with pediatric experience may also be deployed. When a patient’s T-PEWS score is greater than or equal to 6, signifying a high severity of illness, the rotor-wing team may be dispatched at the discretion of the referring providers or medical control physician. The rotor-wing team consists of a flight paramedic with pediatric experience (fEMT-P), a flight nurse with pediatric critical care or emergency medicine training (fRN), and a pilot. On rare occasions with particular advanced respiratory needs, a RCP will accompany the rotor-wing team.
CCT members are permitted to intubate patients in cardiac arrest without consultation with a medical control physician, or when patients are described as being “in extremis”. When
patients do not meet either of the above criteria, the medical control physician is required to be contacted prior to a TI attempt. The medical control provider is not available via telemedicine to support or assist the CCT during TI attempts .The CCT follows a strict protocol, modified from the Pediatric Fundamentals for Critical Care Support guidelines for advanced airway management24, including a rapid sequence intubation (RSI) algorithm that dictates oral airway placement if the child is unable to be oxygenated or ventilated via bag-valve-mask, and subsequent laryngeal mask airway placement if the child is still unable to be oxygenated or ventilated. If ventilation and oxygenation are possible with bag-valve-mask, an RSI algorithm is begun, including nasogastric (NG) tube insertion, pre-oxygenation, atropine administration if bradycardic for age, or if the patient is under 12 months of age, and then subsequent analgesia(fentanyl or morphine, typically), sedation (lorazepam, etomidate or ketamine) and neuromuscular blockade(rocuronium or vecuronium) based on the patient’s probable diagnosis. A standard algorithm utilized which begins with the CCT assessing the child for hypotension, asthma or cardiac disease. If the answer to any of these questions is “yes”, the child will receive ketamine, lorazepam and rocuronium prior to intubation. If none of the above are present, and the patient is under 2 months of age, the patient will receive atropine, fentanyl, lorazepam and rocuronium prior to intubation. If the child is over 2 months of age without any of the above factors, the patient will receive etomidate and rocuronium prior to intubation. Malleable stylets are used routinely by the CCT. Video laryngoscopy was not available for use at the time of the study. The CCT airway operators are permitted up to 3 attempts before a second operator from outside the CCT must be utilized. All intubations are attempted orally.
Prior to any field intubation attempts, CCT providers, including all EMT-Ps, RNs and RCPs have undergone classroom training with didactic and practical skills training with task-trainers, a minimum of ten pediatric operating room intubations while proctored by an attending pediatric anesthesiologist [25], and an observed “check-off” with the transport medical director, consisting of several intubation scenarios, and intubation of a high-fidelity mannequin simulator. Additionally, CCT providers maintain pediatric airway proficiency by completing a minimum of ten intubations and participate in a minimum of six high fidelity simulations with the transport medical director annually. These credentialing criteria are specific to this CCT.
Measurements
A single TI attempt was defined by the insertion of a laryngoscope and attempted visualization of the vocal cords. Then, CCT providers either successfully placed the tracheal tube, or aborted TI. Aborted attempts may have been due to oxygen desaturation or any other reason, and each aborted attempt was tallied as an unsuccessful attempt. Individual judgement, not specific oxygen saturation level nor duration of laryngoscopy was utilizated prior to aborting the TI attempt. A successful TI is defined by positive end tidal capnography, confirmation of bilateral breath sounds and chest rise following TI and, when available, chest radiography confirming tracheal tube placement, location and depth [26]. We characterized first-

CentralBringing Excellence in Open Access
Dugan et al. (2017)Email:
Arch Emerg Med Crit Care 2(3): 1028 (2017) 3/6
attempt intubation success and overall intubation success with descriptive statistics and calculated 95% confidence intervals. The airway operator completed a standardized intubation report with comments when deviation from standard protocol occurred. Recorded variables included patient age, sex, weight (in kilograms), ethnicity, mode of transport, primary and secondary diagnoses, T-PEWS, vitals prior to intubation (including heart rate, systolic and diastolic blood pressure, respiratory rate, and O2 saturation via pulse oximetry), pre-intubation blood gas values, and whether or not the patient suffered a cardiac arrest immediately prior to intubation. We also recorded pre-medications given, the credentials of the operator, number of TI attempts (whether successful or not) and when applicable, the reasons for documented TI failure. Summary patient population descriptive statistics were performed using the Statistical Package for Excel 2010 (Windows version 14.0; Chicago, Ill). All tests were computed with the R v3.0.0 statistical programming language [27]. Comparisons were performed between patients using the [chi] [2] test or Fisher exact test. Continuous variables were compared between groups using the Wilcoxon rank sum test. Age cutoffs for subgroup analysis were designed post-hoc to mirror prior studies of pediatric TI by transport teams [10].
RESULTS
Demographics
This cohort included 146 patients, of which 89/146 (61%) were male, and 57/146 (39%) were female. Also, 45% of patients were Caucasian, 34% African American, 13% Hispanic and 5% Asian; each had a minimum of one intubation attempt by either a paramedic (EMT-P), respiratory therapist (RCP) or registered nurse (RN).Operators had a median of 13 years of experience, credentials were EMT-P in 82% (115/146) of attempted intubations and CCT were transported via the rotor aircraft team 76% (111/146) of the time. Neither operator experience, mode of transportation nor staff credentials were statistically significant predictors of TI success or failure.
Study Results
Overall success of pediatric TI was confirmed in 140/146 patients (96%, 95% CI = 91-98), with first-attempt success confirmed in 105/146 patients (72%, 95% CI = 64-79).Of the 140 successful intubations, 105/140 (75%) occurred with one attempt, with 28/140 (20%) successful TIs on CCT’s second attempt and 7/140 (5%) successful TIs on CCT’s third attempt. Five of the 140 (4%) successful intubations occurred during patient transport. One hundred fifteen of 146 (79%) patients had no TI attempts by referring hospital prior to CCT’s arrival. Of these, CCT successfully intubated 114 of 115 (99%) of these patients. Thirty-one of 146 (21%) patients had failed TI attempts by referring hospital physicians. CCT’s success rate after failed attempts by referring hospital physicians was 26/31 patients (84%, 95% CI = 63-93). Comparison of patients with TI attempts by a referring hospital with those patients without prior TI attempts yielded a p value of .00015.Five patients were unable to be intubated by the CCT following failed attempts by referring hospital emergency medicine physicians. Of these five patients, four were successfully intubated by alternative providers available at referring hospitals (three anesthesiologists and
one otolaryngologist), with the anesthesiologists utilizing video laryngoscopy in each successful case, and the otolaryngologist with unknown equipment. Lowest saturations during successful and failed TI events were not recorded.
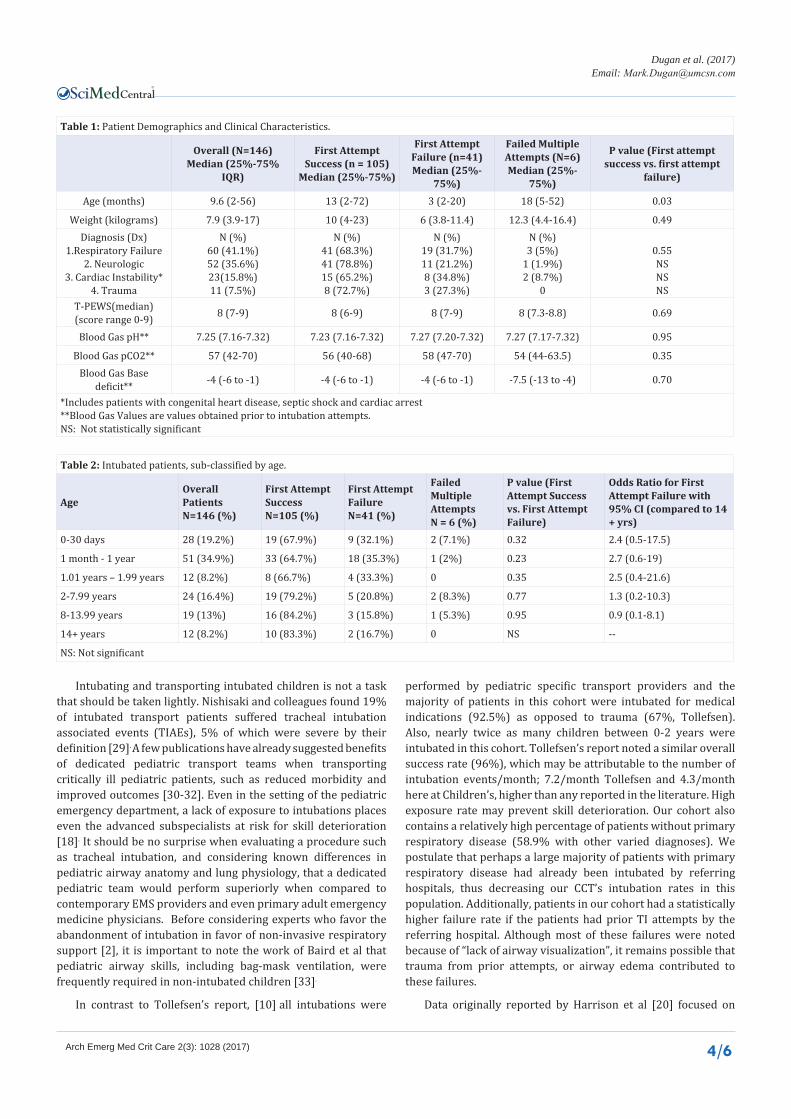
Patients successfully intubated on a first attempt were significantly older than patients requiring multiple attempts (p=0.03).Pre-intubation vital signs, use of pre-intubation sedative medications (including neuromuscular blocking agents), nor pre-intubation blood gas values were not statistically significant risk factors predicting TI Failure. Other characteristics of patients successfully intubated with one attempt compared with patients with an unsuccessful first attempt are further described in Table (1). Thirty-five percent of children 1 month-1 year of age had failed first-attempts at intubation, which was higher than any other age cohort. In addition, first-attempt failure occurred at a higher rate when combining patients aged 0-2 years of age with all other groups (OR = 4.9 when compared to children >14 years of age). Further description of intubated patients sub-classified by age is shown in Table (2).
Six of the 146 (4%) patients could not be intubated by CCT; fifty percent with respiratory diagnoses (Table 1). All six patients had atleast3 attempts by the CCT with one patient having 4 attempts. Four of these patients had documented lack of airway visualization as the reason for failure with each attempt, one patient had 3 attempts, each without confirmatory end-tidal carbon dioxide following TI, andan inability to safely perform alternative confirmatory tests, such as chest x-ray or repeated laryngoscopy by a second provider. In the remaining failed case, 2 attempts resulted in esophageal intubation and inability to visualize the airway with the third attempt. Two of these patients were safely managed with a laryngeal mask airway (LMA) and the other four patients were intubated by alternative advanced airway providers available at referring institutions, as noted above.
Cardiac arrest was noted in 10/146 (7%) overall, with 7/10 first attempt success. Six of these ten had at least one failed attempt by a non-CCT provider, 4/6 failures occurring prior to CCT’s arrival. One cardiac arrest event occurred following a failed TI attempt by the CCT, 4/10 had a documented cardiac arrest prior to any intubation attempt.
DISCUSSIONThis report is one of the largest single-center, mostly pediatric
transport study published to date, characterizing tracheal intubation success rates in pediatric patients with respiratory failure.This adds to the robust paper by Smith et al22 that also focused on both neonates and children requiring intubation. Our study’s reported first-attempt success rate of 72% is similar to reported results of pediatric critical care fellows and attending physicians in the intensive care unit [28], and superior to Smith’s data [22] (57% in their pediatric cohort) as well as a previously published multi-centered study by Bigelow et al [21] (64% first-attempt success).Additionally, Bigelow’s study focused primarily on success and failure rates of various programs nationally, though had a large preponderance of neonatal intubations, as opposed to pediatric intubations. As data was self-reported via a survey, data accuracy was not assured, nor were factors assessed that may have impacted success and failure rates.
CentralBringing Excellence in Open Access
Dugan et al. (2017)Email:
Arch Emerg Med Crit Care 2(3): 1028 (2017) 4/6
Table 1: Patient Demographics and Clinical Characteristics.
Overall (N=146)Median (25%-75%
IQR)
First Attempt Success (n = 105)
Median (25%-75%)
First Attempt Failure (n=41)Median (25%-
75%)
Failed Multiple Attempts (N=6)Median (25%-
75%)
P value (First attempt success vs. first attempt
failure)
Age (months) 9.6 (2-56) 13 (2-72) 3 (2-20) 18 (5-52) 0.03
Weight (kilograms) 7.9 (3.9-17) 10 (4-23) 6 (3.8-11.4) 12.3 (4.4-16.4) 0.49Diagnosis (Dx)
1.Respiratory Failure2. Neurologic
3. Cardiac Instability*4. Trauma
N (%)60 (41.1%)52 (35.6%)23(15.8%)11 (7.5%)
N (%)41 (68.3%)41 (78.8%)15 (65.2%)8 (72.7%)
N (%)19 (31.7%)11 (21.2%)8 (34.8%)3 (27.3%)
N (%)3 (5%)
1 (1.9%)2 (8.7%)
0
0.55NSNSNS
T-PEWS(median) (score range 0-9) 8 (7-9) 8 (6-9) 8 (7-9) 8 (7.3-8.8) 0.69
Blood Gas pH** 7.25 (7.16-7.32) 7.23 (7.16-7.32) 7.27 (7.20-7.32) 7.27 (7.17-7.32) 0.95
Blood Gas pCO2** 57 (42-70) 56 (40-68) 58 (47-70) 54 (44-63.5) 0.35Blood Gas Base
deficit** -4 (-6 to -1) -4 (-6 to -1) -4 (-6 to -1) -7.5 (-13 to -4) 0.70
*Includes patients with congenital heart disease, septic shock and cardiac arrest**Blood Gas Values are values obtained prior to intubation attempts. NS: Not statistically significant
Table 2: Intubated patients, sub-classified by age.
AgeOverall PatientsN=146 (%)
First Attempt SuccessN=105 (%)
First Attempt FailureN=41 (%)
Failed Multiple AttemptsN = 6 (%)
P value (First Attempt Success vs. First Attempt Failure)
Odds Ratio for First Attempt Failure with 95% CI (compared to 14 + yrs)
0-30 days 28 (19.2%) 19 (67.9%) 9 (32.1%) 2 (7.1%) 0.32 2.4 (0.5-17.5)
1 month - 1 year 51 (34.9%) 33 (64.7%) 18 (35.3%) 1 (2%) 0.23 2.7 (0.6-19)
1.01 years – 1.99 years 12 (8.2%) 8 (66.7%) 4 (33.3%) 0 0.35 2.5 (0.4-21.6)
2-7.99 years 24 (16.4%) 19 (79.2%) 5 (20.8%) 2 (8.3%) 0.77 1.3 (0.2-10.3)
8-13.99 years 19 (13%) 16 (84.2%) 3 (15.8%) 1 (5.3%) 0.95 0.9 (0.1-8.1)
14+ years 12 (8.2%) 10 (83.3%) 2 (16.7%) 0 NS --
NS: Not significant
Intubating and transporting intubated children is not a task that should be taken lightly. Nishisaki and colleagues found 19% of intubated transport patients suffered tracheal intubation associated events (TIAEs), 5% of which were severe by their definition [29]. A few publications have already suggested benefits of dedicated pediatric transport teams when transporting critically ill pediatric patients, such as reduced morbidity and improved outcomes [30-32]. Even in the setting of the pediatric emergency department, a lack of exposure to intubations places even the advanced subspecialists at risk for skill deterioration [18]. It should be no surprise when evaluating a procedure such as tracheal intubation, and considering known differences in pediatric airway anatomy and lung physiology, that a dedicated pediatric team would perform superiorly when compared to contemporary EMS providers and even primary adult emergency medicine physicians. Before considering experts who favor the abandonment of intubation in favor of non-invasive respiratory support [2], it is important to note the work of Baird et al that pediatric airway skills, including bag-mask ventilation, were frequently required in non-intubated children [33].
In contrast to Tollefsen’s report, [10] all intubations were
performed by pediatric specific transport providers and the majority of patients in this cohort were intubated for medical indications (92.5%) as opposed to trauma (67%, Tollefsen). Also, nearly twice as many children between 0-2 years were intubated in this cohort. Tollefsen’s report noted a similar overall success rate (96%), which may be attributable to the number of intubation events/month; 7.2/month Tollefsen and 4.3/month here at Children’s, higher than any reported in the literature. High exposure rate may prevent skill deterioration. Our cohort also contains a relatively high percentage of patients without primary respiratory disease (58.9% with other varied diagnoses). We postulate that perhaps a large majority of patients with primary respiratory disease had already been intubated by referring hospitals, thus decreasing our CCT’s intubation rates in this population. Additionally, patients in our cohort had a statistically higher failure rate if the patients had prior TI attempts by the referring hospital. Although most of these failures were noted because of “lack of airway visualization”, it remains possible that trauma from prior attempts, or airway edema contributed to these failures.
Data originally reported by Harrison et al [20] focused on

CentralBringing Excellence in Open Access
Dugan et al. (2017)Email:
Arch Emerg Med Crit Care 2(3): 1028 (2017) 5/6
TI success and failures, and did not report specifics of reasons for requiring intubation, nor were blood gas values available at the time of intubation. For this cohort, when examining those that CCT could not intubate, all patients had a larger base deficit via pre-intubation blood gas when compared to successful intubations, though not statistically significant. It is possible that given the metabolic status of these patients, the tolerance of prolonged laryngoscopy and safe apnea time was reduced, thus contributing to the inability to safely intubate these patients.
In contrast to EMS providers and other non-pediatric specific services, Children’s CCT is a referral service and as such serves only sick children, responds to virtually no scene calls, does not take care of adults, which exposes its team members to a more focused and robust experience. The advent of high-fidelity infant and pediatric simulators that combine realistic airway anatomy with live physiologic changes associated with direct laryngoscopy and intubation allows for a robust training experience prior to the CCT team member attempting their first intubation. One simulation based study, looking at capnography for TI confirmation, noted a 50% improvement in recognition time for tube dislodgement by paramedic students [34]. It remains unknown what percentage of referring institutions and providers have simulation as part of their airway competency training, though the work of Bigelow and colleagues suggests that simulation alone is not sufficient airway training, as their cohort with simulation-only training had lower first-attempt success rates [21].
The limitations of this study include its retrospective nature, and the fact that each patient’s airway registry was populated with self-reported data from the CCT, leaving some data subject to recall or provider bias. Some of this bias was mitigated by real-time requirement of CCT documentation regarding the events surrounding the intubation. In an effort to minimize bias, documentation is completed by the operator and observing CCT members. Pulse oximetry values during intubation could not be explicitly verified, and data cannot be reported to this effect. In addition, this study was not designed using a validated airway collection data tool, such as suggested by Lossius and colleagues [35]. This data may also not be generalizable to other communities, due to its single-center nature. Future studies would incorporate specific methods of education and skill maintenance, in order to compare superiority of certain methods of airway skill learning. Specifically, clarifying whether or not TI success and failure is accompanied by low pulse oximetry values, or other TIAEs would be of benefit. Additionally impact of high fidelity simulation on competency and skill maintenance should be assessed.
CONCLUSIONSPediatric TI performed by an experienced children’s CCT has
a high success rate. TI performance also remains high in spite of prior attempts by referring practitioners, when performed by our CCT. A robust airway-operator training program, specific to pediatric patients and pediatric exposures, likely enhances the success of pediatric TI. Further research is needed to determine predictors for success in maintaining TI competency of a CCT.
ACKNOWLEDGEMENTSThe authors would like to acknowledge Emory and Children’s
Healthcare of Atlanta Pediatric Research Center Biostatistics
Core for their assistance with the statistics for this manuscript. MD presented this work as a poster presentation at the Society of Critical Care Medicine Annual Congress, San Francisco, CA, January 17–21, 2014. MD also completed this research while employed by Emory University School of Medicine.
CONFLICT OF INTERESTThere is no conflict of interest to be disclosed. The paper
falls under non-human subject category and was approved by Children’s Healthcare of Atlanta IRB.
FINANCIAL SUPPORTAll expenses incurred were covered by funds originating
from the Division of Pediatric Critical Care of Emory University School of Medicine.
REFERENCES1. Easley RB, Segeleon JE, Haun SE, Tobias JD. Prospective study of
airway management of children requiring tracheal intubation before admission to a pediatric intensive care unit. Crit Care Med. 2000; 28: 2058-2063.
2. Gerritse BM, Draaisma JM, Schalkwijk A, van Grunsven PM, Scheffer GJ. Should EMS-paramedics perform paediatric tracheal intubation in the field? Resuscitation. 2008; 79: 225-229.
3. Prekker ME, Kwok H, Shin J, Carlbom D, Grabinsky A, Rea TD. The process of prehospital airway management: challenges and solutions during paramedic tracheal intubation. Crit Care Med. 2014; 42: 1372-1378.
4. Aijian P, Tsai A, Knopp R, Kallsen GW. Tracheal intubation of pediatric patients by paramedics. Ann Emerg Med. 1989; 18: 489-494.
5. Losek JD1, Bonadio WA, Walsh-Kelly C, Hennes H, Smith DS, Glaeser PW. Prehospital pediatric tracheal intubation performance review. Pediatr Emerg Care. 1989; 5: 1-4.
6. Sing RF1, Reilly PM, Rotondo MF, Lynch MJ, Mc Cans JP, Schwab CW. Out-of-hospital rapid-sequence induction for intubation of the pediatric patient. Acad Emerg Med. 1996; 3: 41-45.
7. Vilke GM1, Steen PJ, Smith AM, Chan TC. Out-of-hospital pediatric intubation by paramedics: the San Diego experience. J Emerg Med. 2002; 22: 71-74.
8. Sagarin MJ, Chiang V, Sakles JC, Barton ED, Wolfe RE, Vissers RJ, et al. Rapid sequence intubation for pediatric emergency airway management. Pediatr Emerg Care. 2002; 18: 417-423.
9. Wang HE, Kupas DF, Hostler D, Cooney R, Yealy DM, Lave JR. Procedural experience with out-of-hospital tracheal intubation.Crit Care Med. 2005; 33: 1718-1721.
10. Tollefsen WW, Brown CA 3rd, Cox KL, Walls RM. Two hundred sixty pediatric emergency airway encounters by air transport personnel: a report of the air transport emergency airway management (NEAR VI: “A-TEAM”) project. Pediatr Emerg Care. 2013; 29: 963-968.
11. Gausche M, Lewis RJ, Stratton SJ, Haynes BE, Gunter CS, Goodrich SM, et al. Effect of out-of-hospital pediatric tracheal intubation on survival and neurological outcome: a controlled clinical trial. JAMA. 2000;283:783-790.
12. Strote J, Roth R, Cone DC, Wang HE. Prehospital tracheal intubation: the controversy continues. Am J Emerg Med. 2009; 27: 1142-1147.
13. Eich C, Roessler M, Nemeth M, Russo SG, Heuer JF, Timmermann A. Characteristics and outcome of prehospitalpaediatric tracheal
CentralBringing Excellence in Open Access
Dugan et al. (2017)Email:
Arch Emerg Med Crit Care 2(3): 1028 (2017) 6/6
intubation attended by anaesthesia-trained emergency physicians. Resuscitation. 2009; 80: 1371-1377.
14. King B, King TM, Foster RL, McCans KM. Pediatric and neonatal transport teams with and without a physician: a comparison of outcomes and interventions. Pediatr Emerg Care. 2007; 23: 77-82.
15. King BR, Woodward GA. Procedural training for pediatric and neonatal transport nurses: Part 2-procedures, skills assessment, and retention. Pediatr Emerg Care. 2002; 18: 438-441.
16. Falck AJ, Escobedo MB, Baillargeon JG. Proficiency of pediatric residents in performing neonatal tracheal intubation. Pediatrics. 2003; 112: 1242-1247.
17. Patel J, Posencheg M, Ades A. Proficiency and retention of neonatal resuscitation skills by pediatric residents. Pediatrics. 2012; 130: 515-521.
18. Mittiga MR, Geis GL, Kerrey BT, Rinderknecht AS. The spectrum and frequency of critical procedures performed in a pediatric emergency department: implications of a provider-level view. Ann Emerg Med. 2013;61:263-270.
19. Bigham MT, Schwartz HP; Ohio Neonatal/Pediatric Transport Quality Collaborative. Quality metrics in neonatal and pediatric critical care transport: a consensus statement. PediatrCrit Care Med. 2013; 14: 518-524.
20. Harrison TH, Thomas SH, Wedel SK. Success rates of pediatric intubation by a non-physician-staffed critical care transport service. Pediatr Emerg Care. 2004; 20: 101-107.
21. Bigelow AM, Gothard MD, Schwartz HP, Bigham MT. Intubation in Pediatric/Neonatal Critical Care Transport: National Performance. PrehospEmerg Care. 2015; 19: 351-357.
22. Smith KA, Gothard MD, Schwartz HP, Giuliano JS Jr, Forbes M, Bigham MT. Risk Factors for Failed Tracheal Intubation in Pediatric and Neonatal Critical Care Specialty Transport. PrehospEmerg Care. 2015;19:17-22.
23. Petrillo-Albarano T, Stockwell J, Leong T, Hebbar K. The use of a modified pediatric early warning score to assess stability of pediatric patients during transport. Pediatr Emerg Care. 2012; 28: 878-882.
24. Mejia R, Fields A, Greenwald BM, Stein F (Eds). Pediatric fundamental
critical care support.Illinois, Society of Critical Care Medicine, 2008.
25. Brownstein DR, Quan L, Orr R, Wentz KR, Copass MK. Paramedic intubation training in a pediatric operating room. Am J Emerg Med. 1992;10:418-420.
26. Sanchez-Pinto N, Giuliano JS, Schwartz HP, Garrett L, Gothard MD, Kantak A, et al. The impact of postintubation chest radiograph during pediatric and neonatal critical care transport. PediatrCrit Care Med. 2013; 14: 213-217.
27. R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. 2008.
28. Sanders RC Jr, Giuliano JS Jr, Sullivan JE, Brown CA 3rd, Walls RM, Nadkarni V, et al. Level of trainee and tracheal intubation outcomes. Pediatrics. 2013;131:e821-828.
29. Nishisaki A, Marwaha N, Kasinathan V, Brust P, Brown CA 3rd, Berg RA, et al. Airway management in pediatric patients at referring hospitals compared to a receiving tertiary pediatric ICU. Resuscitation. 2011 ;82: 386-390.
30. Edge WE, Kanter RK, Weigle CG, Walsh RF. Reduction of morbidity in interhospital transport by specialized pediatric staff. Crit Care Med. 1994; 22: 1186-1191.
31. Ajizian SJ, Nakagawa TA. Interfacility transport of the critically ill pediatric patient. Chest. 2007; 132: 1361-1367.
32. Orr RA, Felmet KA, Han Y, McCloskey KA, Dragotta MA, Bills DM, et al. Pediatric specialized transport teams are associated with improved outcomes. Pediatrics. 2009; 124: 40-48.
33. Baird JS, Spiegelman JB, Prianti R, Frudak S, Schleien CL. Noninvasive ventilation during pediatric interhospital ground transport. PrehospEmerg Care. 2009; 13: 198-202.
34. Langhan ML, Ching K, Northrup V, Alletag M, Kadia P, Santucci K, et al. A randomized controlled trial of capnography in the correction of simulated tracheal tube dislodgement. Acad Emerg Med. 2011; 18: 590-596.
35. Lossius HM, Sollid SJ, Rehn M, Lockey DJ. Revisiting the value of pre-hospital tracheal intubation: an all time systematic literature review extracting the Utstein airway core variables. Crit Care. 2011; 15: 26.
Dugan MC, Hebbar KB, Leong T, Callis AC, Petrillo TM (2017) Intubation Success Rates by a Children’s Hospital Transport Team. Arch Emerg Med Crit Care 2(3): 1028.
Cite this article