investigations into the blood sugar in man : 6. on the rise of the optimal sugar percentage and...
TRANSCRIPT
(Contribution from the Children’s Department of the Riphospital Copenhagen.)
Investigations into the Blood Sugar in Man. 6, On the Rise of the Optimal Sugar Percentage and In- crease of the One-gram Rise in the Course of Diabetes.
BY KAREN MARIE HANSEN.
I n the second section of my thesis (Copenhagen 1923) a number of investigations were published in individuals who had never displayed symptoms of suffering from derangement of their carbohydrate metabolism either subjectively or objec- tively, and in whose families there were no known cases of diabetes mellitus.
On the administration of rising doses of pure glucose in these cases, who were chosen as especially healthy persons as regards the carbohydrate metabolism, i t was found that the total-rise of the blood sugar (the distance between the highest and the lowest point on the smooth curve determined by very many analyses), never exceeded a blood sugar concentration of 0.18 5.
The blood sugar percentage at which the organism showed the greatest power of getting rid of introduced sugar from the circulation was termed the optimal concentration, and as stated 0.18 % was the highest found.
I n ten diabetics investigated with different doses of glucose an acceleration power in no case was demonstrated (the power t o accelerate the removal of introduced sugar from the blood stream), and if the acceleration power was existent at all in these diabetics it appeared from the experiments that it did not begin t o function until an optimal sugar percentage was
586 KAREN MARIE HANSEN.
reached wich was higher than that found in normal persons, as it was above 0.20 to 0.24 or 0.29 %.
That the acceleration power may be preserved i n diabetics waq prowed by investigations in a mild case of diabetes in a woman who also suffered from adiposity. Her power of ac- celeration began at 0.24 % (Diab. No. 13 a).
That a hypernormal optimal concentration may exist in non- diabetics was shown by the investigation of a woman with lactation glycosuria. Her acceleration only began at 0.20 % and over, and the power was less than in normal persons, as far as the investigation went.
It was enquired whether an optimal blood sugar concentra- tion at a higher level than that found in normal persons must always be considered to be a sign of disease of the carbohy- drate metabolism and possibly of incipient diabetes, or whether a hypernormal optimal concentration merely indicates that the individual is less well equipped than the normal persons I investigated without there being any question of disease or disposition to disease on its account, just as we find for example people who are differently equipped intellectually. Only ex- perience in the course of time can decide this.
The question therefore arises whether the optimal percentage is perhaps constitutionally fixed both in the healthy and in the sick. If such is the case we can conclude nothing from its position as to the possibility of ensuing diabetes and the proposed function test for the unclassified glycosurias will then be devoid of prognostic value.
That the power of acceleration is a measure of the orga- nism’s power of carbohydrate metabolism seems certain. The problem is whether it is diminished by the rise in the optimal percentage or even completely disappears when the organism is diseased, and whether a high optimal percentage signifies a step towards diabetes.
It seems at first sight useless to follow a chance individual with a high optimal concentration because just this one person may perhaps by his habits evade the development of the agent causing his disease. When diabetes begins to progress in adults is also rather uncertain and the influence of the progression on the phenomena of the rise may easily elude investigation.
Only in diabetes in small children do statistics prove with certainty that the development of the disease proceeds so ra-

INVESTIGATIONS INTO THE BLOOD SUGAR IN MAN. 587
pidly that, as measured by the acceleration power, it can be followed fairly easily.
I investigated therefore a case of diabetes mellitus in a little girl, 2l/4 years old.
There was no history of diabetes in her family. Eight weeks before her admission to the State Hospital her parents noticed that she suffered from polyphagia and polydipsia. Glycosuria was demonstrated and she was admitted to a hospital near her home where she was treated with a special diet for 6 weeks. When ad- mitted to the hospital there was 6 $ sugar in the urine; later, gly- cosuria was only present now and then (below 1 %>. She was ad- mitted to the Children's Department of the Rigshospital on the 8. X. 1922. She appeared normal and lively. Height 95 em., weight 13.4 kg. There was frequent micturition and some thirst. The hair was scanty and dry, otherwise nothing abnormal on examinalion. I n the 24 hours' urine there was 3l/e 7: sugar and a trace of albumin. No ketonuria. Sahli, 90 %. On 12. X. the fasting blood sugar was 0.076 %. Morning urine, no sugar. Diminishing amount in the 24 hours' sample. On 6. XI. she was put on boiled milk and acorn cocoa on account of diarrhoea. She again got 3'12 % sugar in her urine and the fasting blood sugar rose to 0.19. On a diet poor in carbohydrates as before, the glycosuria however quickly disappeared and the blood sugar again became normal but there was a little acetone in the urine from time to time. On 13. XII. she was discharged feeling perfectly well on the following diet on which, for about 3 weeks. she had remained free from sugar: 50 gm. boiled or roasted meat or fish, 50 gm. whipped cream, 7 5 gm. butter, 1 egg, 15 gm. rye bread twice, 50 gm. bran biscuits, 200 gm. yegetables, coffee, tea, soup ad lib. Weight on disharge 1 4 kg.
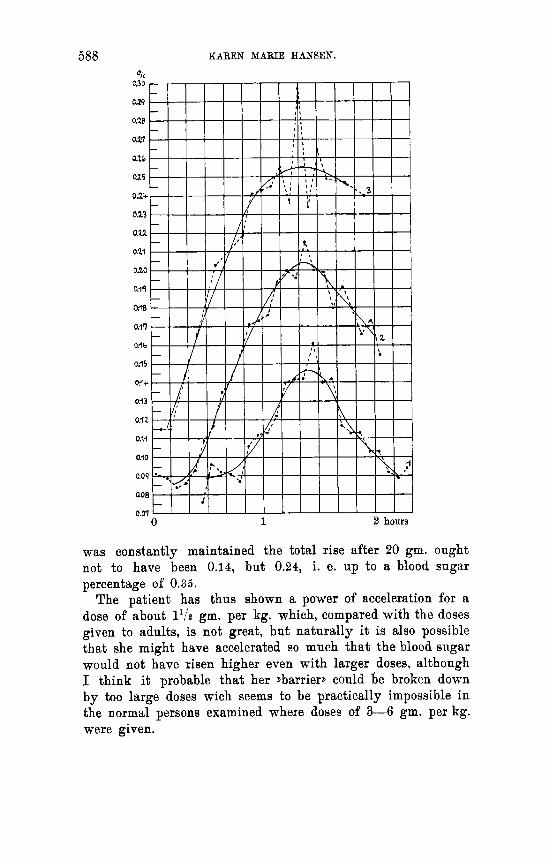
Curves 1, 2 and 3 show the results of the function tests while in hospital.
Curve 1 (8. XII.) represents a dose of 5 gm. glucose in 100 c. c. coffee. The total rise was 0.058, and the one-gram rise 0.0116. Curve 2 (6. XII.) was taken after a dose of 10 gm. glucose i n 100 c. c. coffee, and shows a total rise of 0.118 and a one-gram rise of 0.0118, in other words we see that the total rise is increased in proportion to the size of the dose while the one-gram rise is constant, that is to say the usual principle of the diabetic rise is valid.
Curve 3 shows a total rise of 0.140 and a rise per gram administered of 0.0070 after 20 gm. glucose in 100 c. c. coffee. The one-gram rise is diminished, that is to say acceleration has become established as will be seen from the curve, with a blood sugar percentage of 0.25. If the diabetic rise rule
558 KAREN MARIE HANSEN.
was constantly maintained the total rise after 20 gm. ought not to have been 0.14, but 0.24, i. e. up to a blood sugar percentage of 0.35.
The patient has thus shown a power of acceleration for a dose of about 1'12 gm. per kg. which, compared with the doses given to adults, is not great, but naturally it is also possible that she might have accelerated so much that the blood sugar would not have risen higher even with larger doses, although I think it probable that her >barrier, could be broken down by too large doses wich seems to be practically impossible in the normal persons examined where doses of 3 - 4 gm. per kg. were given.

INVESTIGATIONS INTO THE BLOOD SUGAR IN MAN. 589
The significance of the size of the one-gram rise is also discussed in the work referred to. According to the old in- terpretation of the tolerance, glycosuria or absence of glyco- suria after a certain dose of carbohydrate, it is asserted that the high one-gram rise must be a sign of slight tolerance.
I n recognising that this tolerance test, which is based upon the appearance of glycosuria, cannot be deemed t o be a good indication of the diabetic’s actual condition since the occur- rence of glycosuria depends upon other factors than the gravity of the disease, i t was proposed to employ the numericalvalue of the one-gram rise (without regard to the glycosuria) after the administration of pure glucose as a general measure of the diabetic’s condition. It cannot be concluded from the cases published there whether a high one-gram rise signifies a more severe case than a low one. A severe case, judging from the general clinical symptoms, showed a low one-gram rise but in this case (No. 13) there was a good effect from the dietetic treatment and as the subsequent course of this as of the other cases is unknown it is quite possible that a low one-gram rise, other things being equal, means a better prognosis than a high one. Experience will decide whether such is the case. Prima facie. it is probable that at any rate in the same individual the one-gram rise has prognostic importance. As will be ob- served from the above figures this diabetes case wich lead one to expect a rapid course had a very high one-gram rise, and it will appear from what follows that the one-gram rise be- comes still higher as the condition becomes worse. On returning home from the State Hospital the patient kept
strictly to the above-mentioned diet and the urine, which was examined every fortnight, contained no sugar until 10 days before she was again admitted to the Children’s Department on 2. 111. 1923. At home she had been bright and lively and had not complained of thirst or hunger. Her weight was 14 kg. as on discharge.
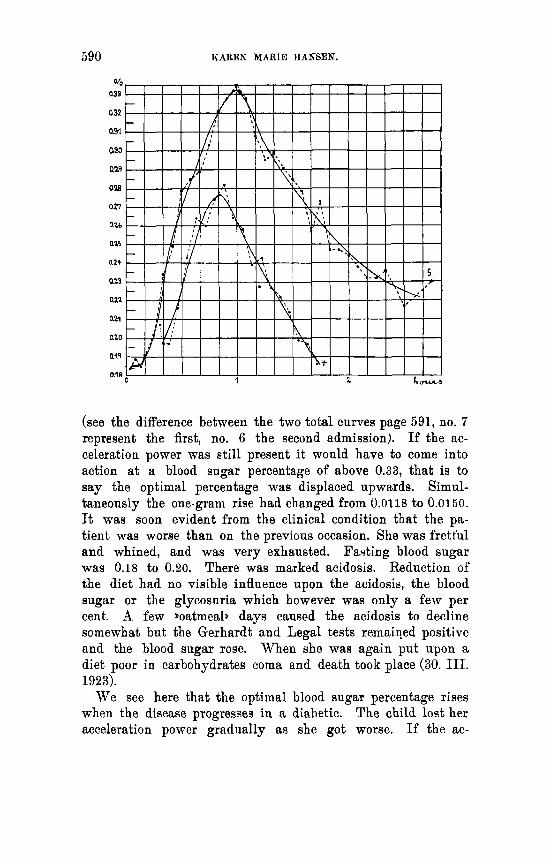
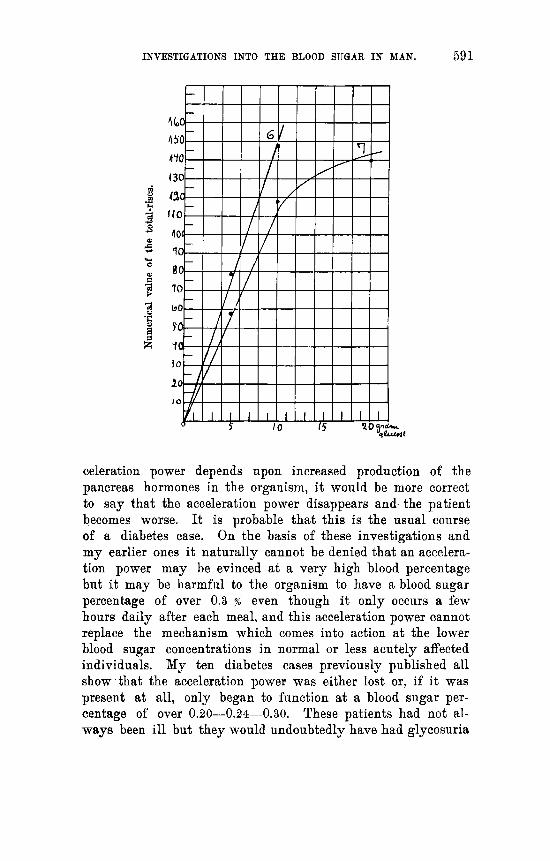
On 3. 111. and 5. 111. 1923 function tests were done with 5 and 10 ‘ gm. glucose in 100 c. c. coffee, respectively (see curves 4 and 5). The total rise after 5 gm. was 0.079 and after 10 gm. 0.148 with corresponding one-gram rises of 0.0156 and 0.0148. The highest point was at 0.33 %. No acceleration power was found this time although the blood sugar had been driven 0.080 higher than on the first admission to hospital
590 KAREN MARIE HANSEN.
(see the difference between the two total curves page 591, no. 7 represent the first, no. 6 the second admission). If the ac- celeration power was still present it would have to come into action at a blood sugar percentage of above 0.83, that is to say the optimal percentage was displaced upwards. Simul- taneously the one-gram rise had changed from 0.0118 to 0.0150. It was soon evident from the clinical condition that the pa- tient was worse than on the previous occasion. She was fretful and whined, and was very exhausted. Fading blood sugar was 0.18 to 0.20. There was marked acidosis. Reduction of the diet had no visible influence upon the acidosis, the blood sugar or the glycosuria which however was only a few per cent. A few ,oatmeal> days caused the acidosis to decline somewhat but the Gerhardt and Legal tests remaiqed positive and the blood sugar rose. When she waa again put upon a diet poor in carbohydrates coma and death took place (30. 111. 1923).
We see here that the optimal blood sugar percentage rises when the disease progresses in a diabetic. The child lost her acceleration power gradually as she got worse. If the ac-
INVESTIGATIONS INTO THE BLOOD SUQAFL IN MAN. 591
celeration power depends upon increased production of the pancreas hormones in the organism, it would be more correct to say that the acceleration power disappears and. the patient becomes worse. It is probable that this is the usual course of a diabetes case. On the basis of these investigations and my earlier ones it naturally cannot be denied that an accelera- tion power may be evinced at a very high blood percentage but it may be harmful to the organism to have a blood sugar percentage of over 0.3 % even though it only occurs a few hours daily after each meal, and this acceleration power cannot replace the mechanism which comes into action at the lower blood sugar concentrations in normal or less acutely affected individuals. My ten diabetes cases previously published all show that the acceleration power was either lost or, if it was present at all, only began to function at a blood sugar per- centage of over 0.20-0.24-0.30. These patients had not al- ways been ill but they would undoubtedly have had glycosuria
502 KAREN MARIE HANSEN.
on the ordinary food they ate before they were ill if they had only been able t o accelerate the reduction of their blood sugar at the higher blood sugar concentration. If we therefore assume that glycosuria was not present all through their liven, and we know this to be so at any rate in the case of patients previously treated in the hospital for other diseases, we are obliged to presuppose a progressive reduction of the accelera- tion power through rise of the optimnl percentage simultane- ously with the development of the disease.
I n the mild diabetes case (No. 13 a) the acceleration power still remained but at a blood sugar percentage of 0.24.
The way the acceleration power is diminished is thus through the high optimal blood sugar percentage, that is to say a stronger stimulus is gradually required to make the hormone production adequate.
It is of course not certain that healthy persons with a high optimal percentage have a predisposition to diabetes. There is always the question whether the repeated transgression of the blood sugar above a certain height may damage cells in the long run. It may be imagined that what is required and what asserts itself at a high optimal percentage, is a stronger stimules on account of the smaller number of pancreas islands present, or ou account of less active tissues, and that this hyper- irritation will at length exhaust t h e functioning power and thus cause diabetes. Even if we imagine that the pancreas islands originally had a diminished functioning power which was either congenital or had been induced by some lesion or other, for example, infection, there is reason to expect that a vicious circle may be set up by the high optimal concentration which facilitates the occurrence of diabetes. The relief of the de- mands made upon the functioning tissue would therefore be one of the tasks of insulin, and more particularly its action would be expected to be more than merely symptomatic, - a point of view which was also brought forward by Prof. Faber in the discuesion after Prof. Rrogh’s lecture on insulin in the Medical Society, Copenhagen in January 1923.
I have previously expressed the view that if i t is the pan- creas hormone which causes the elimination of sugar from the circulation, which must actually take place in diabetics during the rise in concentration of the blood sugar after ad- ministration, then the one-gram rise is, as it were, an inverse
INVESTIGATIONS INTO THE BLOOD SUGAR IN MAN. 593
expression of the degree of hormone production. It also in- dicates that the one-gram rise has prognostic significance since i t must be assumed that the more it is possible to eliminate per unit administered, the inore hormone can be produced although the power of hyperproduction which shows itself as the power of acceleration is no longer present. It is further seen, as mentioned, from the present investigations that the one-gram rise is increased a good deal as the disease progresses.