ios press selection of patients with tourette syndrome for...
TRANSCRIPT
Behavioural Neurology 27 (2013) 125–131 125DOI 10.3233/BEN-120288IOS Press
Selection of patients with Tourette syndromefor deep brain stimulation surgery
Mauro Portaa,∗, Andrea E. Cavannab,c, Edvin Zekajd, Francesca D’Addaa and Domenico Servellod
aTourette Centre, IRCCS Galeazzi Hospital, Milan, ItalybThe Michael Trimble Neuropsychiatry Research Group, Department of Neuropsychiatry, BSMHFT and Universityof Birmingham, Birmingham, UKcSobell Department of Motor Neuroscience and Movement Disorders, UCL and Institute of Neurology, London, UKdFunctional Neurosurgery Unit, IRCCS Galeazzi Hospital, Milan, Italy
Abstract. Deep brain stimulation (DBS) is an emerging therapeutic option for severe resistant Tourette syndrome (TS). To date,about 100 cases have been reported in the scientific literature. Different clinical guidelines have been proposed for this procedurefrom both USA and European centres. A number of issues remain unresolved, mainly in relation to eligibility criteria of patientswith TS. We highlight the need for a comprehensive assessment of associated co-morbidities, which are not considered integralpart of the syndrome and are not sufficiently evaluated in relation to DBS. The concept of refractoriness, the minimum age ofcandidates, and the optimal targets for DBS are also controversial.
Keywords: Deep brain stimulation, Tourette syndrome, tics, co-morbidities, selection criteria
1. Introduction
Tourette syndrome (TS) is a chronic neurodevelop-mental disorder defined by the presence of multiplemotor tics and at least one phonic tic [1]. It is estimatedthat about 90% of patients have at least one co-morbidbehavioural symptom, such as attention deficit hyper-activity disorder (ADHD), obsessive-compulsive dis-order (OCD), self-injurious behaviour (SIB), impulsedyscontrol and affective dysregulation [2]. Overall, thecourse of tic symptoms is relatively favourable overtime: up to 50% of patients with onset of tic disorderbefore age 10 experience a significant decrease in ticseverity during adolescence [3]. However, severe TScan have devastating effects on perceived well beingand relationships. Behavioural strategies, in additionto both standard and innovative pharmacological ther-apies, are the main treatment interventions for patients
∗Corresponding author: Mauro Porta, Tourette Centre, IRCCSGaleazzi Hospital, Via R. Galeazzi 4, 20161 Milan, Italy. Tel.:+39 02/66214933; Fax: +39 02/66214916; E-mail: [email protected].
who continue to experience severe symptoms with sig-nificant social impairment.
When patients are refractory to conservative treat-ments, deep brain stimulation (DBS) could be consid-ered as an emerging therapeutic option. Over the lastfew decades, DBS has been demonstrated to be a safeand efficacious procedure in different movement disor-ders, including Parkinson disease, essential tremor anddystonia [4]. More recently, DBS has also been usedto treat patients with severe and refractory psychiatricdisorders, such as OCD and depression [5].
The rationale for choosing specific targets for DBSto treat patients with severe and refractory TS was ini-tially based on the effects of historical procedures ofablative surgery, which are no longer ethically accept-able [6]. The results of preliminary reports on DBS inTS are encouraging, even though many aspects haveyet to be better clarified, in primis the issue of patientselection [7].
2. Assessment
Candidates to DBS in TS should undergo a compre-hensive neurological, neuropsychiatric and neuropsy-
ISSN 0953-4180/13/$27.50 2013 – IOS Press and the authors. All rights reserved

126 M. Porta et al. / Selection of patients with Tourette syndrome for deep brain stimulation surgery
chological pre-surgical assessment, to be carried outby a multidisciplinary team with clinical experience inTS and in collaboration with functional neurosurgeons.Detailed clinical assessment guidelines of tic disordersand common co-morbidities are discussed in the recent-ly published guidelines from the European Society forthe Study of Tourette Syndrome (ESSTS) [8]. Patientsshould be diagnosed according to DSM IV-TR criteriaand the diagnosis should be validated by instrumentssuch as the TS Diagnostic Confidence Index. With re-gards to the clinical picture, the tic symptoms shouldrepresent the primary problem significantly affectingQuality of Life (QoL).
Tic severity should be evaluated by means of directobservation (e.g. videorecording) and clinical scales,such as the Yale Global Tic Severity Scale (YGTSS).A YGTSS total tic severity score above 35/50 duringrepeated assessments for at least six months is a re-liable indicator of a degree of tic severity promptingconsideration of DBS.
The large majority of patients with TS have co-morbid psychopathology, including attention-deficitand hyperactivity disorder (ADHD), obsessive-compulsive disorders (OCD), anger control problems,mood disorders, conduct and oppositional defiant disor-ders. Co-morbidities have to be evaluated using specificscales: for example, the Yale-Brown Obsessive Com-pulsive Scale (YBOCS) has often been used for eval-uation of obsessive compulsive behaviours; the State-Trait Anxiety Inventory (STAI) assesses patients’ stateand trait anxiety, and the Beck Depression Invento-ry (BDI) reliably measures depression. It should al-ways be considered that co-morbidity can representthe main reason to seek help in patients with TS. Thedisease-specific health-related quality of life scale forTS (GTS-QOL) developed by Cavanna et al. [9] high-lights the relevance of the patient’s subjective point ofview. This scale comprises 27 items which examinefour components of quality of life: the psychologicaldomain, the physical/activities of daily living (ADL)domain, the obsessive-compulsive domain and the cog-nitive domain. Importantly, this scale can adequatelyand specifically evaluate aspects of social impairmentwhich often motivate DBS in refractory patients. TheGTS-QOL also captures other aspects of the TS-relatedimpact on life. Self injurious behaviour (SIB) is fre-quently present in the context of TS. For example, SIBof different severity was reported in 46.1% of patientsfrom a clinical sample of 639 subjects [10]. Patientswith life-threatening tics are classified as having “ma-lignant TS”. Jankovic et al. [11] in their experience
reported that 5% of patients with TS can present ma-lignant TS, often in association with severe obsessive-compulsive symptomatology. Finally, the GTS-QOLcan prove useful both as baseline and outcomemeasure,also in the longer term. For instance, a recent studyshowed that young patients with severe tics associat-ed with characteristic premonitory urges and a familyhistory of tics disorders appear to be at higher risk forpoorer quality of life as adults [12].
Both environmental and psychosocial stressors haveto be evaluated as factors aggravating clinical symp-toms. Surgical candidates should experience tics asso-ciated with a significant functional impairment.
“TS by history” has to be carefully evaluated by ask-ing patients, parents and caregivers. These data can behighly informative, although the value of these parame-ters is not yet formally validated. At least familiar, envi-ronmental and economic issues have to be carefully ex-amined as they are important factors that may influencepatient compliance. Analysis of the phenomenologicalaspects of TS according to Jankovic [13] seems essen-tial to choose targets for DBS; videotaping according toKompoliti and Goetz [14] and accelerometry [15] canbe used to objectively evaluate tic symptoms. The pa-tient or his/her legal representative must given writteninformed consent before the DBS procedure. If DBSis performed in the context of a trial, the study designhas to be approved by the local ethics committee [16].
3. Treatment refractoriness
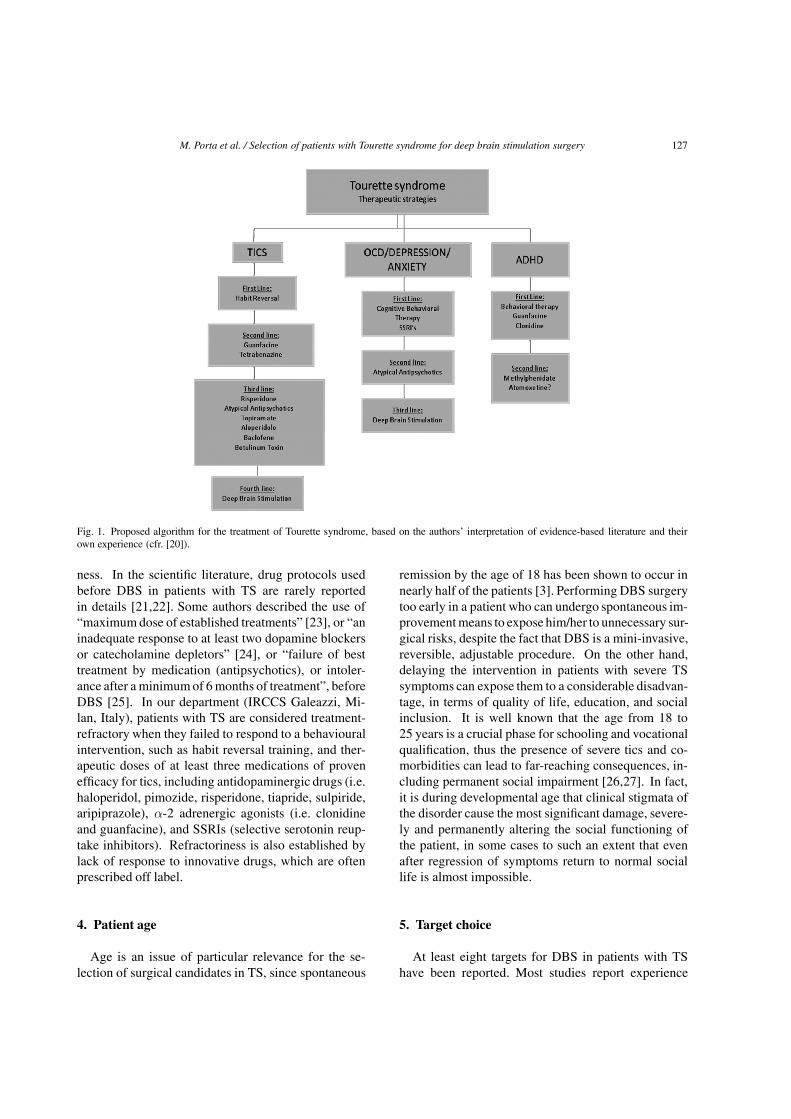
The exact definition of treatment refractoriness in TShas been debated [17]. A significant percentage of pa-tients with TS show spontaneous improvement up to acomplete disappearance of most if not all the symptomsduring adulthood: DBS is of course indicated for thosepatients failing to show such improvement of symp-toms and related social impairment [18]. The therapeu-tic strategies used to treat tics and co-morbidities arefar from being standardized; although there are manyopen studies on pharmacotherapy, only a limited num-ber of studies meets rigorous criteria for therapeutic tri-als. Cochrane reviews and expert views on the pharma-cological treatment of TS have recently been published(Fig. 1) [19,20].
Drug therapy often involves the use of antipsychoticagents, which can be associated with a higher risk ofadverse effects compared to other drugs. Side effectsmay persist during adulthood: this fact by itself rep-resent an important element in evaluating refractori-
M. Porta et al. / Selection of patients with Tourette syndrome for deep brain stimulation surgery 127
Fig. 1. Proposed algorithm for the treatment of Tourette syndrome, based on the authors’ interpretation of evidence-based literature and theirown experience (cfr. [20]).
ness. In the scientific literature, drug protocols usedbefore DBS in patients with TS are rarely reportedin details [21,22]. Some authors described the use of“maximum dose of established treatments” [23], or “aninadequate response to at least two dopamine blockersor catecholamine depletors” [24], or “failure of besttreatment by medication (antipsychotics), or intoler-ance after a minimumof 6 months of treatment”, beforeDBS [25]. In our department (IRCCS Galeazzi, Mi-lan, Italy), patients with TS are considered treatment-refractory when they failed to respond to a behaviouralintervention, such as habit reversal training, and ther-apeutic doses of at least three medications of provenefficacy for tics, including antidopaminergic drugs (i.e.haloperidol, pimozide, risperidone, tiapride, sulpiride,aripiprazole), α-2 adrenergic agonists (i.e. clonidineand guanfacine), and SSRIs (selective serotonin reup-take inhibitors). Refractoriness is also established bylack of response to innovative drugs, which are oftenprescribed off label.
4. Patient age
Age is an issue of particular relevance for the se-lection of surgical candidates in TS, since spontaneous
remission by the age of 18 has been shown to occur innearly half of the patients [3]. Performing DBS surgerytoo early in a patient who can undergo spontaneous im-provementmeans to expose him/her to unnecessary sur-gical risks, despite the fact that DBS is a mini-invasive,reversible, adjustable procedure. On the other hand,delaying the intervention in patients with severe TSsymptoms can expose them to a considerable disadvan-tage, in terms of quality of life, education, and socialinclusion. It is well known that the age from 18 to25 years is a crucial phase for schooling and vocationalqualification, thus the presence of severe tics and co-morbidities can lead to far-reaching consequences, in-cluding permanent social impairment [26,27]. In fact,it is during developmental age that clinical stigmata ofthe disorder cause the most significant damage, severe-ly and permanently altering the social functioning ofthe patient, in some cases to such an extent that evenafter regression of symptoms return to normal sociallife is almost impossible.
5. Target choice
At least eight targets for DBS in patients with TShave been reported. Most studies report experience

128 M. Porta et al. / Selection of patients with Tourette syndrome for deep brain stimulation surgery
with small case series (less than five). Overall, in thisdecade DBS for TS has brought more questions thananswers. In our department, fifty patients with TS havebeen treated with DBS. The most targeted area wasthe ventro-oralis-centromedian-parafascicular nucleusof the thalamus Vo-Cm-Pf (Lat: 5 mm, AP: −2 mm,Z: 0 mm), with optimal results concerning tics and im-provement in OCD and anxiety [28,29]. Stimulationof the nucleus accumbens-anterior limb of the internalcapsule (NA-ALIC) was used as first line procedureor as rescue procedure for patients with relevant OCDwho failed to respond to Vo-Cm-Pf stimulation. In se-lected patients with prevalence of dystonic tics, signif-icant reduction of tic severity was obtained targetingthe posterior portion of the globus pallidus-pars interna(Gpi). In patients with a clinical picture characterisedby significant co-morbidities, we targeted the anteriorportion of the GPi [30]. In our opinion, targets shouldbe selected case by case on the basis of the most rele-vant symptoms (tailoring approach), as different targetsseem to have different clinical effects.
6. Compliance
Poor patient and caregivers compliance should beconsidered as a major exclusion criterion. Patient withhistory of drug addiction have to be carefully evaluat-ed. The role of caregivers in determining outcome ofDBS is poorly elucidated. Frequently caregivers maynot appreciate amelioration of symptomatology afterDBS. The risk is to produce frustration on the patientsand decrease the compliance. In most cases physiciansfocus on patient compliance, while caregiver’s com-pliance is frequently underestimated. From our experi-ence we have learnt that caregiver compliance can beas important as patient compliance. We have had twodisposal removals due to caregiver’s poor compliancewhich prevailed over patient will, convincing them ofthe failure of the surgical procedure. In order to be eli-gible for DBS, patients should demonstrate compliancewith previous treatments [31]. Compliance should beassessed in terms of adherence to pharmacological pro-tocols and psychobehavioural training programs, andattendance to follow-up visits.
7. Other exclusion criteria
A controversial issue within exclusion criteria is thefinding of brain abnormalities on pre-operative MRI
scans. In clinical series of dystonic patients, focal sig-nal abnormalities in the basal ganglia do not contraindi-cate DBS [32]. On the other hand, in Parkinson dis-ease the presence of chronic ischemic disease or dif-fuse cerebral atrophy compatible with atypical Parkin-sonism represent exclusion criteria for DBS. In our TSseries, the presence of vascular abnormalities affectedthe positioning of the stimulating electrode near thetarget [33]. There are uncertainties also with regardsto general medical conditions representing contraindi-cation to DSB. In various reports, cardiovascular, pul-monary or hematological disorders are considered acontraindication for surgery. In our opinion, patientsshould be excluded from surgery if they have an Amer-ican Society of Anesthesiologists (ASA)score of 3 orabove which represent an increased risk for generalanaesthesia.
Another important aspect related to exclusion crite-ria is the presence of severe psychiatric co-morbidity.With regards to this, it has to be considered that about90% of patients with TS have at least one co-morbidbehavioural symptom, such as ADHD, OCD, SIB, im-pulse dyscontrol and affective dysregulation [2]. Thescientific literature is controversial about psychiatricdisorders representing exclusion criteria for DBS. Forinstance, Mink et al. [16] recommend that candidatesto DBS must not have co-morbid psychiatric disorders,while Shahed et al. [30] proposed that psychiatric co-morbidities in TS should not necessarily represent anexclusion criterion, because it is possible that these be-havioural problems will also improve with DBS. It ismandatory to evaluate psychiatric disorder case by case,while previous suicidal attempts should be considereda contraindication.
8. Conclusion
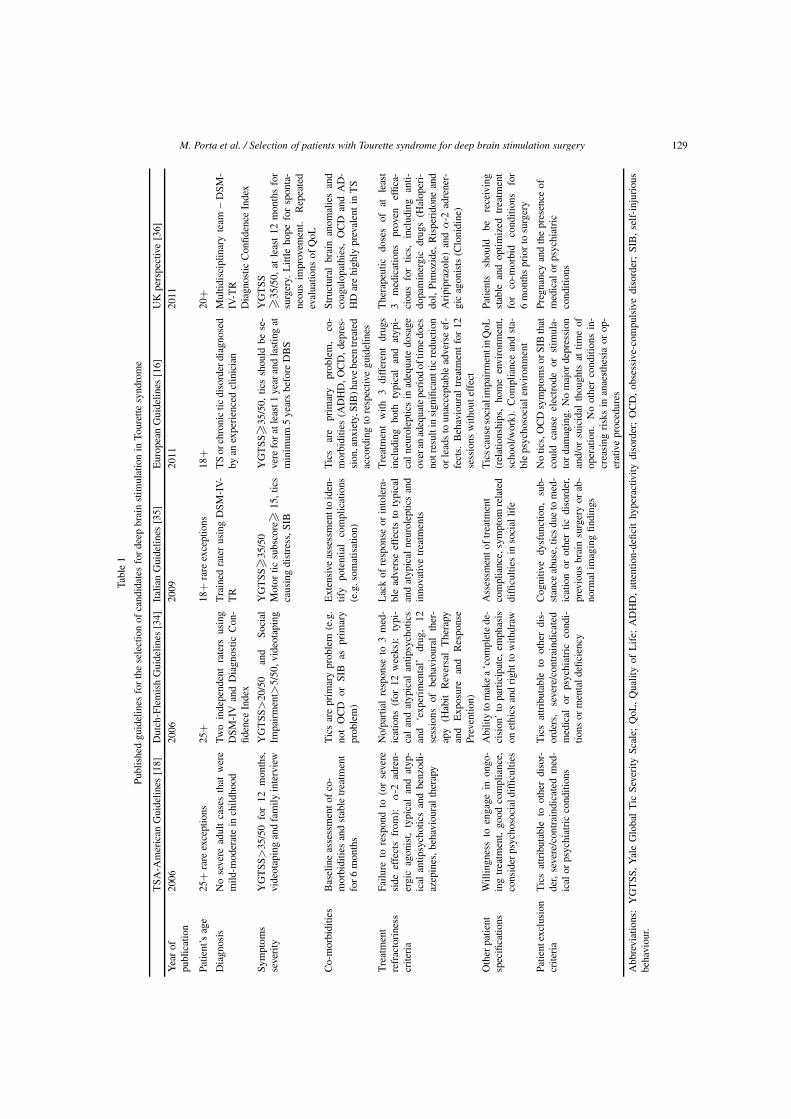
Different guidelines on the selection of candidatesfor DBS in TS have been published to date (Table 1).
From the critical evaluation of these guidelinesemerges a substantial difference regarding the mini-mum age at which DBS might be considered. As statedabove, we believe that surgical procedure have to beproposed to younger patients, starting from the age of18 years. It should also be highlighted that exceptionsin terms of younger patients may be considered forDBS when needed, as in the case of the 16-year-old pa-tient reported by Shahed et al. [30]. The second prob-lem concerns the behavioural spectrum of TS, whichis referred to as co-morbidity. The phenotype of TS
M. Porta et al. / Selection of patients with Tourette syndrome for deep brain stimulation surgery 129
Tabl
e1
Publ
ishe
dgu
idel
ines
forth
ese
lect
ion
ofca
ndid
ates
forde
epbr
ain
stim
ulat
ion
inTo
uret
tesy
ndro
me
TSA
-Am
eric
anG
uide
lines
[18]
Dut
ch-F
lem
ish
Gui
delin
es[3
4]Ital
ian
Gui
delin
es[3
5]Eur
opea
nG
uide
lines
[16]
UK
pers
pect
ive
[36]
Yea
rof
publ
icat
ion
2006
2006
2009
2011
2011
Patie
nt’s
age
25+
rare
exce
ptio
ns25
+18
+ra
reex
cept
ions
18+
20+
Dia
gnos
isN
ose
vere
adul
tca
ses
that
wer
em
ild-m
oder
ate
inch
ildho
odTw
oin
depe
nden
tra
ters
usin
gD
SM-I
Van
dD
iagn
ostic
Con
-fid
ence
Inde
x
Tra
ined
rate
rus
ing
DSM
-IV-
TR
TS
orch
roni
ctic
diso
rder
diag
nose
dby
anex
perien
ced
clin
icia
nM
ultid
isci
plin
ary
team
–D
SM-
IV-T
RD
iagn
ostic
Con
fiden
ceIn
dex
Sym
ptom
sse
verity
YG
TSS
>35
/50
for
12m
onth
s,vi
deot
apin
gan
dfa
mily
inte
rvie
wY
GTSS
>20
/50
and
Soci
alIm
pairm
ent>
5/50
,vid
eota
ping
YG
TSS
�35
/50
Mot
ortic
subs
core�
15,t
ics
caus
ing
dist
ress
,SIB
YG
TSS
�35
/50,
tics
shou
ldbe
se-
vere
fora
tlea
st1
year
and
last
ing
atm
inim
um5
year
sbe
fore
DB
S
YG
TSS
�35
/50,
atle
ast12
mon
ths
for
surg
ery.
Litt
leho
pefo
rsp
onta
-ne
ous
impr
ovem
ent.
Rep
eate
dev
alua
tions
ofQ
oL
Co-
mor
bidi
ties
Bas
elin
eas
sess
men
tofco
-m
orbi
ditie
san
dst
able
trea
tmen
tfo
r6
mon
ths
Tic
sar
epr
imar
ypr
oble
m(e
.g.
not
OC
Dor
SIB
aspr
imar
ypr
oble
m)
Ext
ensive
asse
ssm
entt
oid
en-
tify
pote
ntia
lco
mpl
icat
ions
(e.g
.som
atis
atio
n)
Tic
sar
epr
imar
ypr
oble
m,
co-
mor
bidi
ties
(AD
HD
,OC
D,d
epre
s-si
on,a
nxie
ty,S
IB)h
avebe
entrea
ted
acco
rdin
gto
resp
ectiv
egu
idel
ines
Stru
ctur
albr
ain
anom
alie
san
dco
agul
opat
hies
,O
CD
and
AD
-H
Dar
ehi
ghly
prev
alen
tin
TS
Tre
atm
ent
refr
acto
rine
sscr
iteria
Failu
reto
resp
ond
to(o
rse
vere
side
effe
cts
from
):α
-2ad
ren-
ergi
cag
onis
t,ty
pica
lan
dat
yp-
ical
antip
sych
otic
san
dbe
nzod
i-az
epin
es,b
ehav
iour
alth
erap
y
No/
partia
lre
spon
seto
3m
ed-
icat
ions
(for
12w
eeks
):ty
pi-
calan
dat
ypic
alan
tipsy
chot
ics
and
‘exp
erim
enta
l’dr
ug,
12se
ssio
nsof
beha
viou
ral
ther
-ap
y(H
abit
Rev
ersa
lThe
rapy
and
Exp
osur
ean
dR
espo
nse
Prev
entio
n)
Lac
kof
resp
onse
orin
tole
ra-
ble
adve
rse
effe
cts
toty
pica
lan
dat
ypic
alne
urol
eptic
san
din
nova
tive
trea
tmen
ts
Tre
atm
ent
with
3di
ffer
ent
drug
sin
clud
ing
both
typi
cal
and
atyp
i-ca
lneu
role
ptic
sin
adeq
uate
dosa
geov
eran
adeq
uate
period
oftim
edo
esno
tres
ulti
nsi
gnifi
cant
ticre
duct
ion
orle
adsto
unac
cept
able
adve
rse
ef-
fect
s.B
ehav
iour
altrea
tmen
tfo
r12
sess
ions
with
oute
ffec
t
The
rape
utic
dose
sof
atle
ast
3m
edic
atio
nspr
oven
effic
a-ci
ous
for
tics,
incl
udin
gan
ti-do
pam
iner
gic
drug
s(H
alop
eri-
dol,
Pim
ozid
e,R
ispe
rido
nean
dA
ripi
praz
ole)
and
α-2
adre
ner-
gic
agon
ists
(Clo
nidi
ne)
Oth
erpa
tient
spec
ifica
tions
Will
ingn
ess
toen
gage
inon
go-
ing
trea
tmen
t,go
odco
mpl
ianc
e,co
nsid
erps
ycho
soci
aldi
fficu
lties
Abi
lity
tom
akea‘c
ompl
ete
de-
cisi
on’to
partic
ipat
e,em
phas
ison
ethi
csan
drigh
tto
with
draw
Ass
essm
ento
ftrea
tmen
tco
mpl
ianc
e,sy
mpt
omre
late
ddi
fficu
lties
inso
cial
life
Tic
scau
seso
cial
impa
irm
enti
nQ
oL(r
elat
ions
hips
,ho
me
envi
ronm
ent,
scho
ol/w
ork)
.C
ompl
ianc
ean
dst
a-bl
eps
ycho
soci
alen
viro
nmen
t
Patie
nts
shou
ldbe
rece
ivin
gst
able
and
optim
ized
trea
tmen
tfo
rco
-mor
bid
cond
ition
sfo
r6
mon
thspr
iorto
surg
ery
Patie
ntex
clus
ion
crite
ria
Tic
sat
trib
utab
leto
othe
rdi
sor-
der,
seve
re/c
ontrai
ndic
ated
med
-ic
alor
psyc
hiat
ric
cond
ition
s
Tic
sat
trib
utab
leto
othe
rdi
s-or
ders
,se
vere
/con
trai
ndic
ated
med
ical
orps
ychi
atric
cond
i-tio
nsor
men
tald
efici
ency
Cog
nitiv
edy
sfun
ctio
n,su
b-st
ance
abus
e,tic
sdu
eto
med
-ic
atio
nor
othe
rtic
diso
rder
,pr
evio
usbr
ain
surg
ery
orab
-no
rmal
imag
ing
findi
ngs
No
tics,
OC
Dsy
mpt
omsor
SIB
that
coul
dca
use
elec
trod
eor
stim
ula-
torda
mag
ing.
No
maj
orde
pres
sion
and/
orsu
icid
alth
ough
tsat
time
ofop
erat
ion.
No
othe
rco
nditi
ons
in-
crea
sing
risk
sin
anae
sthe
sia
orop
-er
ativ
epr
oced
ures
Preg
nanc
yan
dth
epr
esen
ceof
med
ical
orps
ychi
atric
cond
ition
s
Abb
revi
atio
ns:
YG
TSS
,Yal
eG
loba
lTic
Seve
rity
Scal
e;Q
oL,Q
ualit
yof
Life;
AD
HD
,at
tent
ion-
defic
ithy
pera
ctiv
itydi
sord
er;
OC
D,ob
sess
ive-
com
puls
ive
diso
rder
;SI
B,se
lf-inj
urio
usbe
havi
our.
130 M. Porta et al. / Selection of patients with Tourette syndrome for deep brain stimulation surgery
Table 2Proposed inclusion criteria for deep brain stimulation in Tourette syndrome
Eligible candidates for deep brain stimulation should:
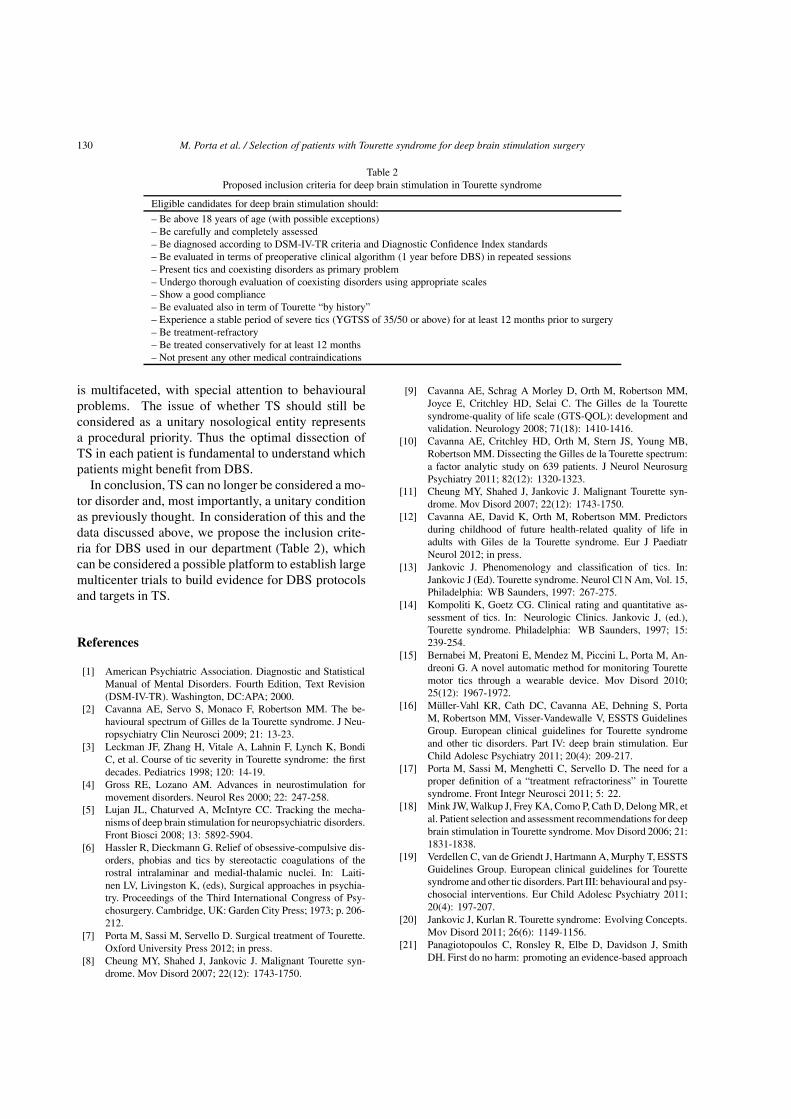
– Be above 18 years of age (with possible exceptions)– Be carefully and completely assessed– Be diagnosed according to DSM-IV-TR criteria and Diagnostic Confidence Index standards– Be evaluated in terms of preoperative clinical algorithm (1 year before DBS) in repeated sessions– Present tics and coexisting disorders as primary problem– Undergo thorough evaluation of coexisting disorders using appropriate scales– Show a good compliance– Be evaluated also in term of Tourette “by history”– Experience a stable period of severe tics (YGTSS of 35/50 or above) for at least 12 months prior to surgery– Be treatment-refractory– Be treated conservatively for at least 12 months– Not present any other medical contraindications
is multifaceted, with special attention to behaviouralproblems. The issue of whether TS should still beconsidered as a unitary nosological entity representsa procedural priority. Thus the optimal dissection ofTS in each patient is fundamental to understand whichpatients might benefit from DBS.
In conclusion, TS can no longer be considered a mo-tor disorder and, most importantly, a unitary conditionas previously thought. In consideration of this and thedata discussed above, we propose the inclusion crite-ria for DBS used in our department (Table 2), whichcan be considered a possible platform to establish largemulticenter trials to build evidence for DBS protocolsand targets in TS.
References
[1] American Psychiatric Association. Diagnostic and StatisticalManual of Mental Disorders. Fourth Edition, Text Revision(DSM-IV-TR). Washington, DC:APA; 2000.
[2] Cavanna AE, Servo S, Monaco F, Robertson MM. The be-havioural spectrum of Gilles de la Tourette syndrome. J Neu-ropsychiatry Clin Neurosci 2009; 21: 13-23.
[3] Leckman JF, Zhang H, Vitale A, Lahnin F, Lynch K, BondiC, et al. Course of tic severity in Tourette syndrome: the firstdecades. Pediatrics 1998; 120: 14-19.
[4] Gross RE, Lozano AM. Advances in neurostimulation formovement disorders. Neurol Res 2000; 22: 247-258.
[5] Lujan JL, Chaturved A, McIntyre CC. Tracking the mecha-nisms of deep brain stimulation for neuropsychiatric disorders.Front Biosci 2008; 13: 5892-5904.
[6] Hassler R, Dieckmann G. Relief of obsessive-compulsive dis-orders, phobias and tics by stereotactic coagulations of therostral intralaminar and medial-thalamic nuclei. In: Laiti-nen LV, Livingston K, (eds), Surgical approaches in psychia-try. Proceedings of the Third International Congress of Psy-chosurgery. Cambridge, UK: Garden City Press; 1973; p. 206-212.
[7] Porta M, Sassi M, Servello D. Surgical treatment of Tourette.Oxford University Press 2012; in press.
[8] Cheung MY, Shahed J, Jankovic J. Malignant Tourette syn-drome. Mov Disord 2007; 22(12): 1743-1750.
[9] Cavanna AE, Schrag A Morley D, Orth M, Robertson MM,Joyce E, Critchley HD, Selai C. The Gilles de la Tourettesyndrome-quality of life scale (GTS-QOL): development andvalidation. Neurology 2008; 71(18): 1410-1416.
[10] Cavanna AE, Critchley HD, Orth M, Stern JS, Young MB,Robertson MM. Dissecting the Gilles de la Tourette spectrum:a factor analytic study on 639 patients. J Neurol NeurosurgPsychiatry 2011; 82(12): 1320-1323.
[11] Cheung MY, Shahed J, Jankovic J. Malignant Tourette syn-drome. Mov Disord 2007; 22(12): 1743-1750.
[12] Cavanna AE, David K, Orth M, Robertson MM. Predictorsduring childhood of future health-related quality of life inadults with Giles de la Tourette syndrome. Eur J PaediatrNeurol 2012; in press.
[13] Jankovic J. Phenomenology and classification of tics. In:Jankovic J (Ed). Tourette syndrome. Neurol Cl N Am, Vol. 15,Philadelphia: WB Saunders, 1997: 267-275.
[14] Kompoliti K, Goetz CG. Clinical rating and quantitative as-sessment of tics. In: Neurologic Clinics. Jankovic J, (ed.),Tourette syndrome. Philadelphia: WB Saunders, 1997; 15:239-254.
[15] Bernabei M, Preatoni E, Mendez M, Piccini L, Porta M, An-dreoni G. A novel automatic method for monitoring Tourettemotor tics through a wearable device. Mov Disord 2010;25(12): 1967-1972.
[16] Muller-Vahl KR, Cath DC, Cavanna AE, Dehning S, PortaM, Robertson MM, Visser-Vandewalle V, ESSTS GuidelinesGroup. European clinical guidelines for Tourette syndromeand other tic disorders. Part IV: deep brain stimulation. EurChild Adolesc Psychiatry 2011; 20(4): 209-217.
[17] Porta M, Sassi M, Menghetti C, Servello D. The need for aproper definition of a “treatment refractoriness” in Tourettesyndrome. Front Integr Neurosci 2011; 5: 22.
[18] Mink JW, Walkup J, Frey KA, Como P, Cath D, Delong MR, etal. Patient selection and assessment recommendations for deepbrain stimulation in Tourette syndrome. Mov Disord 2006; 21:1831-1838.
[19] Verdellen C, van de Griendt J, Hartmann A, Murphy T, ESSTSGuidelines Group. European clinical guidelines for Tourettesyndrome and other tic disorders. Part III: behavioural and psy-chosocial interventions. Eur Child Adolesc Psychiatry 2011;20(4): 197-207.
[20] Jankovic J, Kurlan R. Tourette syndrome: Evolving Concepts.Mov Disord 2011; 26(6): 1149-1156.
[21] Panagiotopoulos C, Ronsley R, Elbe D, Davidson J, SmithDH. First do no harm: promoting an evidence-based approach
M. Porta et al. / Selection of patients with Tourette syndrome for deep brain stimulation surgery 131
to atypical antipsychotic use in children and adolescents. JCan Acad Child Adolesc Psychiatry 2010; 19: 124-137.
[22] Pringsheim T, Pearce M. Complications of antipsychotic ther-apy in children with Tourette syndrome. Pediatr Neurol 2010;43(1): 17-20.
[23] Kuhn J, Lenartz D, Mai JK, Huff W, Lee SH, KoulousakisA, Klosterkoetter J, Sturm V. Deep brain stimulation of thenucleus accumbens and the internal capsule in therapeuticallyrefractory Tourette-syndrome. J Neurol 2007; 254(7): 963-965.
[24] Maciunas RJ, Maddux BN, Riley DE, Whitney CM, Schoen-berg MR, Ogrocki PJ, et al. Prospective randomized double-blind trial of bilateral thalamic deep brain stimulation in adultswith Tourette syndrome. J Neurosurg 2007; 107: 1004-1014.
[25] Welter ML, Mallet L, Houeto JL, Karachi C, Czernecki V,Cornu P, et al. Internal pallidal and thalamic stimulation inpatients with Tourette syndrome. Arch Neurol 2008; 56: 952-957.
[26] Eddy CM, Cavanna AE, Gulisano M, Agodi A, Barchitta M,Calı P, Robertson MM, Rizzo R. Clinical correlates of qualityof life in Tourette syndrome. Mov Disord 2011; 26: 735-738.
[27] Eddy CM, Rizzo R, Gulisano M, Agodi A, Barchitta M, Calı P,Robertson MM, Cavanna AE. Quality of life in young peoplewith Tourette syndrome: A controlled study. J Neurol 2011;258: 291-301.
[28] Servello D, Sassi M, Brambilla A, Porta M, Haq I, FooteKD, Okun MS. De novo and rescue DBS leads for refracto-ry Tourette syndrome patients with severe comorbid OCD: amultiple case report. J Neurol 2009; 256(9): 1533-1539.
[29] Sassi M, Porta M, Servello D. Deep brain stimulation therapy
for treatment-refractory Tourette’s Syndrome: A review. ActaNeurochir (Wien) 2011; 153(3): 639-645.
[30] Shahed J, Poysky J, Kenney C, Simpson R, Jankovic J. GPideep brain stimulation for Tourette syndrome improves ticsand psychiatric comorbidities. Neurology 2007; 68: 159-160.
[31] Eddy CM, Rickards HE, Cavanna AE. The cognitive impactof antiepileptic drugs. Ther Adv Neurol Dis 2011; 4: 380-402.
[32] Gavarini S, Vayssiere N, Delort P, Cif L, Biolsi B, TancuC, Vasques X, Plagnol S, Bonafe A, Coubes P. StereotacticMRI in DYT1 dystonia: Focal signal abnormalities in thebasal ganglia do not contraindicate deep brain stimulation.Stereotact Funct Neurosurg 2008; 86(4): 245-252.
[33] Servello D, Sassi M, Brambilla A, Defendi S, Porta M. Long-Term, Post-Deep Brain Stimulation Management of a Seriesof 36 Patients affected with refractory Gilles de la Tourettesyndrome. Neuromodulation 2010; 13: 187-194.
[34] Ackermans L, Temel Y, Cath D, van der Linden C, BruggemanR, Kleijer M, Nederveen P, Schruers K, Colle H, Tijssen MA,Visser-Vandewalle V, Dutch Flemish Tourette Surgery StudyGroup. Deep brain stimulation in Tourette’s syndrome: Twotargets? Mov Disord 2006; 21(5): 709-713.
[35] Porta M, Servello D, Sassi M, Brambilla A, Defendi S, PrioriA, Robertson M. Issues related to deep brain stimulation fortreatment refractory Tourette syndrome. Eur Neurol 2009; 62:264-273.
[36] Cavanna AE, Eddy CM, Mitchell R, Pall H, Mitchell I, ZrinzoL, et al. An approach to deep brain stimulation for severetreatment-refractory Tourette syndrome: the UK perspective.Br J Neurosurg 2011; 25(1): 38-44.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com