is ginseng an ergogenic aid? - human kinetics ginseng an ergogenic aid? 301 that american ginseng is...
TRANSCRIPT
298
International Journal of Sport Nutrition and Exercise Metabolism, 2009, 19, 298-322© 2009 Human Kinetics, Inc.
Is Ginseng an Ergogenic Aid?
Michael S. Bahrke, William P. Morgan, and Aaron Stegner
Ginseng is one of the most popular herbal supplements in the world. Although it is used for the treatment and prevention of many ailments, it is also used to increase work efficiency and is purported to increase energy and physical stamina. Athletes use ginseng for its alleged performance-enhancing attributes. However, many studies examining the pharmacological effects of ginseng on physical performance have not employed sound scientific design and methodology. The purpose of this review is to provide an update on published empirical research focusing primarily on the efficacy of ginseng with respect to physical and athletic performance. Despite attempts in recent investigations to improve on the scientific rigor used in examining the ergo-genic properties of ginseng, the authors conclude that many of the same method-ological shortcomings observed in earlier studies persist. Enhanced physical perfor-mance after ginseng administration in well-designed investigations remains to be demonstrated.
Keywords: herbal supplement, pharmacological effects, performance enhancement, athletic performance
The world market for herbal supplements and remedies is increasing at a phenomenal rate (PRWeb Press Release Newswire, 2008). The top-selling herbal products in the United States include echinacea, saw palmetto, ginkgo biloba, ginseng, and St. John’s wort, among others (Healing Herbs and Natural Remedies, 2008). In a national survey examining the prevalence of herbal supplement use in a sample of adults residing in the United States, nearly one in five surveyed had consumed herbs during the preceding year (Bardia, Nisly, Zimmerman, Gryzlak, & Wallace, 2007). Additional survey results collected from college (Froiland, Koszewski, Hingst, & Kopecky, 2004) and elite athletes, both in the United States and abroad (Petroczi & Naughton, 2008; Slater, Tan, & Teh, 2003; Sundgot- Borgen, Berglund, & Torstveit, 2003; Ziegler, Nelson, & Jonnalagadda, 2003), indicate that ginseng is one of the most popular herbal supplements consumed by athletes.
Ginseng is used worldwide to treat and prevent many ailments, but it has also been administered to increase occupational efficiency involving physical labor and is purported to provide energy and increase physical stamina. Athletes use ginseng for its alleged performance-enhancing attributes (Froiland et al., 2004;
Bahrke is with Human Kinetics, Champaign, IL 61825-5076. Morgan and Stegner are with the Dept. of Kinesiology, University of Wisconsin–Madison, Madison, WI.
SCHOLARLY REVIEWS
Is Ginseng an Ergogenic Aid? 299
Petroczi & Naughton, 2008; Slater et al., 2003; Sundgot-Borgen et al., 2003; Ziegler et al., 2003). However, the efficacy of ginseng has been inferred primarily through anecdotes, testimonials, clinical experience, and animal research, as opposed to scientific verification of its pharmacological effects on humans engaged in the type of physical performance pursued by athletes.
The purpose of the current review is to provide an update on empirical research published since our two earlier reviews (Bahrke & Morgan, 1994, 2000). There have been other reviews published since our most recent review, but with a single exception (Palisin & Stacy, 2006), they did not focus on physical or athletic performance (Attele, Wu, & Yuan, 1999; Lieberman, 2001). Furthermore, these related reviews did not include the many varieties of ginseng (Davydov & Krikorian, 2000; Goulet & Dionne, 2005), nor have extensive and detailed summaries been provided (Vogler, Pittler, & Ernst, 1999). We focus primarily on the efficacy of ginseng with respect to physical and athletic performance in the current review. Specifically, in this article we provide an update on (a) the physiological effects of ginseng and ginseng-related products on physical activity, stress, and fatigue; (b) the psychological, behavioral, and cognitive effects of ginseng; (c) the quality, purity, and bioavailability of ginseng products; and (d) the potential adverse health effects, drug interactions, and safety of ginseng.
Varieties of GinsengGinseng root is processed and distributed in various forms including powder, liquid extracts, tablets, capsules, and chewing gum. Roots are graded (sorted) according to their source, age, part of the root, and method of preparation. The chemical composition of commercial ginseng products is variable because of the genetic nature of the plant source, the cultivation methods, and the drying and curing process (Hong et al., 2005; Hu, 1976; Lim, Mudge, & Vermeylen, 2005). In addition, some manufacturers add various substances (e.g., minerals and vita-mins) to ginseng products, and there have been reports of drugs and alcohol being present in ginseng products (“Ginseng Warning,” 1997).
Several species of ginseng are known to exist: American, Chinese, Korean, Japanese, and Siberian (Barna, 1985). Three medicinal species of ginseng are cur-rently recognized: Panax ginseng C.A. Meyer (Chinese or Korean ginseng, a perennial herb indigenous to the mountainous forests of eastern Asia), Panax japonicus C.A. Meyer (Japanese ginseng, from India, Southern China, and Japan), and Panax quinquefolius (American ginseng, found growing in rich woodland in the eastern and central United States and Canada; Court, 1975; Popov & Gold-wag, 1973; Williams, 1957).
A preparation of Korean ginseng containing a standardized concentration of ginsenosides has been used in a number of clinical and pharmacological studies. This preparation, known as G115 (G115 is the registered trademark of a ginseng extract containing all ginsenosides from the Korean Panax ginseng; GPL Ginsana Products SA, Lugano, Switzerland) and marketed under the name Ginsana, is widely used to treat a variety of problems such as reduced performance associated with general fatigue states. Because these preparations sometimes contain other substances (e.g., alcohol, vitamins, minerals; Pietta, Mauri, & Rava, 1986), it is difficult to conclude that ginseng per se is efficacious.

300 Bahrke, Morgan, and Stegner
Siberian or Russian ginseng, although reported to have the same stimulant and tonic effects as the other ginseng products, is an entirely different plant, Eleutherococcus senticosus (Baranov, 1982; Brekman, 1965). The terms ciwujia, devil’s bush, wild pepper, and shigoka are often used as synonyms for Siberian ginseng.
Eleutherococcus senticosus has been used as an inexpensive substitute for the ginseng roots of Panax ginseng C.A. Meyer (Araliaceae) in republics of the former Soviet Union and other countries. In reviewing the medicinal uses of ginseng and related plants in the Soviet Union, Baranov (1982) concluded that (a) administra-tion of E. senticosus (eleuthero), unlike ginseng, never produces excitation in patients; (b) the effect of eleuthero on the general immunity of an organism is more universal than that of ginseng; (c) ginseng has antistress effects but, under certain conditions, might produce a stresslike syndrome (eleuthero has no such effect); and (d) the effect of both ginseng and eleuthero varies seasonally, but this is less so for eleuthero.
Like Siberian or Russian ginseng, Panax japonicus C.A. Meyer has been used in Japan as a substitute for Panax ginseng C.A. Meyer in the treatment of gastro-enteric disorder and as an antitussive, expectorant, and antipyretic. American gin-seng (Panax quinquefolius) is sold worldwide in forms such as processed roots, powders, teas, and capsules. It is used as an analeptic, tonic, stomach-pain analge-sic, and adaptogenic agent (any substance that exerts effects on both sick and healthy individuals by “correcting” any dysfunction without producing unwanted side effects; Davydov & Krikorian, 2000). It has also been widely promoted as an aphrodisiac (Liberti & Der Marderosian, 1978).
The main active constituents of the Panax species are recognized to be triter-penoid glycosides or saponins and are termed ginsenosides by Chinese, Korean, and Japanese researchers, and the active components of Eleutherococcus sentico-sus, whose structures and distribution vary with species and variety, are termed panaxosides by Russian workers. Identification of the active elements, establish-ment of reliable techniques for isolating and standardizing the active components, and extensive evaluation of the active components and pharmacological proper-ties has occurred during the past few decades (Hou, 1977; Iwabuchi, Yoshikura, Ikawa, & Kamisako, 1987; Iwabuchi, Yoshikura, & Kamisako, 1988; Kasai, Yamaguchi, & Tanaka, 1987). Chromatographic methods are now available for identifying saponins that make ginseng detection and differentiation relatively simple (Liberti & Der Marderosian, 1978; Phillipson & Anderson, 1984; Pietta et al., 1986; Shibata, Fujita, Itokawa, Tanaka, & Ishii, 1963; Tanaka, Nagai, & Shibata, 1966; Yamaguchi, Kasai, Matsuura, Tanaka, & Fuwa, 1988). Ginseng saponins have been investigated (Iida, Tanaka, & Shibata, 1968; Tanaka et al., 1966; Li et al., 2000), and at least 31 have been isolated from extracts of Panax ginseng roots (Court, 1975; Hou). The major saponins have been named ginsenosides Rx, where x is a, b1, b2, c, d, e, f, g1, g2, g3, h1, h2, or o, according to their position on thin-layer chromatograms (Shibata et al., 1965).
Among the various types of ginseng, Korean ginseng appears to be relatively rich in ginsenosides. In Korean Panax ginseng, ginsenosides Rb1, Rc, and Rg1 are major saponins, and although American P. quinquefolius is similar in its constitu-ents there are significant differences (Besso et al., 1982; Phillipson & Anderson, 1984). The most significant difference between American and Korean ginsengs is

Is Ginseng an Ergogenic Aid? 301
that American ginseng is believed to have cooling and energizing effects on the body, whereas Korean ginseng is thought to have warming and calming effects. The roots of Japanese ginseng, Panax japonicus, contain mainly different saponins, which are known as chikusetsu-saponins. Only two saponin glycosides are common to Japanese, Chinese, Korean, and American ginseng, namely, Rg2 and Ro (Russian panaxosides do not correspond with those of the ginsenosides).
The active constituents of Russian ginseng (E. senticosus) are a series of eleutherosides coded A to F (Elyakov et al., 1964). The major eleutherosides are completely different in chemical structure from the ginsenosides. The resultant variety of saponins that can co-occur, each with its own pharmacological activity, is probably responsible for the lack of consensus among researchers on the phar-macology of ginseng. In fact, in the United States, the 2002 Farm Security and Rural Investment Act (U.S. Department of Agriculture, 2002) states that
the term “ginseng” may only be considered to be a common or usual name (or part thereof) for any herb or herbal ingredient derived from a plant classified within the genus Panax and only labeling or advertising for herbs or herbal ingredients classified within that genus may include the term “ginseng.” (pp. 407–408)
Ginseng grows wild, is also cultivated, and is generally harvested after grow-ing for 6–7 years. Although the entire ginseng plant contains pharmacologically active properties (Petkov et al., 1992), it is the root of the plant that is considered most valuable. In fact, over $81,000 has been paid for a small, 124-year-old gin-seng root (CNN.com/WORLD, 2001). Extracts of red and white ginseng contain different ginsenosides (Chong & Oberholzer, 1988). White ginseng is produced by air-drying the root, and red ginseng is produced by steaming the root, followed by drying. Red ginseng has been used to treat weak constitution, ulcers, cold symptoms, and anemia and as an analeptic, a stomachic, and an erythropoietic in traditional Chinese medicine (Matsuda, Namba, Fukuda, Tani, & Kubo, 1986). The latter function, erythropoiesis, is potentially relevant for application with ath-letes engaged in endurance events. The ginsenoside content of dried ginseng root can vary with root age, method of preservation, and season of harvest (Liberti & Der Marderosian, 1978). High-quality ginseng should be collected in the autumn and never before 5–6 years of growth (Popov & Goldwag, 1973). For example, although most roots present at least four detectable ginsenosides, after 6 years of growth roots show more extensive patterns and might yield up to nine ginseno-sides (Liberti & Der Marderosian).
Physiological EffectsPrevious reviews have documented the physiological effects of ginseng (Bahrke & Morgan, 1994, 2000). Studies dealing with the cardiovascular effects of gin-seng have reported that various preparations and concentrations can reduce, ele-vate, or stabilize blood pressure and influence platelet aggregation. It appears that ginsenosides can have hypertensive, as well as hypotensive, effects. These effects, however, are transient, relatively minor, and dose dependent. Research published since our last review also indicates that ginseng might improve cardiovascular and pulmonary function, and this could enhance physical performance.

302 Bahrke, Morgan, and Stegner
In a randomized, double-blind, placebo-controlled trial, Stavro, Woo, Heim, Leiter, and Vuksan (2005) investigated the effect of six batches of North American ginseng root that varied in quality and ginsenoside content on blood pressure in 16 hypertensive individuals (but not performance in healthy athletes). None of the North American ginsengs differed from placebo in their effect on overall mean blood-pressure change, suggesting that North American ginseng has no effect on blood pressure in hypertensive individuals.
The effects of ginseng on pulmonary function and exercise capacity have been reported in earlier studies. Many of these investigations, however, were con-ducted with patients suffering from compromised pulmonary function and low levels of exercise capacity. In an investigation designed to evaluate the effects of ginseng extract (G115) on pulmonary function and exercise capacity, Gross et al. (2002) assigned 94 patients with moderately severe chronic obstructive pulmo-nary disease to either an experimental group that received 100 mg of G115 twice daily or a control group that received a placebo over a 3-month study period. Pulmonary-function tests of maximum voluntary ventilation and maximum inspiratory pressure were administered before treatment and every 2 weeks during the 3-month period. Exercise tests and VO2max measurements were performed before beginning treatment, at 6 weeks, and after 3 months. In the experimental treatment, but not the placebo treatment, all parameters significantly increased above baseline and surpassed the changes noted in the placebo group. Maximum voluntary ventilation increased 40%, maximum inspiratory pressure improved 47%, and VO2max increased 38%. No side effects were observed. It appears that ginseng might have its most significant effects in individuals with compromised respiratory systems, but this cannot be taken to assume it would have an effect on healthy athletes.
Effects on Physical Activity, Stress, and FatigueGinseng and ginseng-related products have been used for years as an energy booster and as a general tonic. Some reports suggest that ginseng might enhance antibody production and natural-killer-cell activity and play a role in the preven-tion and therapy for respiratory disorders (Choi, 2008). There is evidence that intense physical training can produce temporary changes in the endocrine and immune systems, and one of the reasons athletes use Panax ginseng or Eleuthero-coccus senticosus is the belief that these herbs decrease the incidence of colds and infections and enhance recovery from intense training.
Stress and the Immune System
Gaffney, Hugel, and Rich (2001a), in a 6-week, double-blind, placebo-controlled study, examined the ability of Panax ginseng (type not specified) and Eleuthero-coccus senticosus to influence measures of stress and selected parameters of immune-system status in competitive club-level male athletes engaged in normal training during the competitive season. Thirty participants were matched for train-ing stress and received a 33% ethanolic extract containing Panax ginseng, Eleutherococcus senticosus, or a placebo. A pretest and posttest were used to evaluate the effects of 6 weeks of supplementation on cortisol, testosterone, and
Is Ginseng an Ergogenic Aid? 303
testosterone-to-cortisol ratio (TCR), as well as circulating numbers of T cells, T-helper cells (CD4), T-suppressor cells (CD8), CD4-to-CD8 ratio, natural killer cells, and B lymphocytes. None of the immune-system variables changed signifi-cantly or showed any clear trend from pre- to posttest in any of the treatment groups. No significant change in testosterone, cortisol, or total TCR was observed in the Panax ginseng treatment group. In the Eleutherococcus senticosus treat-ment group, however, TCR significantly decreased by 28.7%. The main contribu-tion to this decrease appeared to be a nonsignificant trend toward increased corti-sol rather than a small decrease in mean testosterone levels. These results suggest that Eleutherococcus senticosus increased rather than decreased hormonal indices of stress. Research has been done on animals that suggests a threshold of stress below which Eleutherococcus senticosus increases the stress response and above which it decreases the stress response (Gaffney et al., 2001a).
Gaffney, Hugel, and Rich (2001b) have proposed a mechanism of action for Panax ginseng and Eleutherococcus senticosus that attempts to explain why these herbs produce the paradoxical effect of sometimes increasing and sometimes decreasing the stress response. The mechanism suggests that this biphasic effect results from increased occupancy of positive- and negative-feedback stress- hormone receptors by their natural ligands to inhibition of specific enzymes that function to limit receptor occupancy. Specifically, Gaffney et al. (2001b) suggest that Panax ginseng inhibits 11-beta hydroxysteroid dehydrogenase 1 and Eleutherococcus senticosus inhibits catechol-O-methyl transferase, both of which reside in close proximity to stress-hormone receptors and catalyze the degradation of stress hormones into inactive compounds. In addition, Gaffney et al. (2001b) suggest that the increased energy claimed to result from Panax ginseng and Eleutherococcus senticosus might be a consequence of their increasing the occu-pancy of stress-hormone receptors that function to redistribute the body’s energy reserves from regeneration to activity.
In an investigation designed to examine the efficacy of ginseng in modulating secretory immunoglobulin A (SIgA), exercise performance, and recovery from repeated bouts of strenuous physical exertion, Engels, Fahlman, and Wirth (2003) used a double-blind, placebo-controlled, randomized design with 38 active healthy adults who supplemented their diets with a standardized ginseng concentrate (400 mg G115) or placebo for 8 weeks. Before and after the treatments, each partici-pant performed three consecutive 30-s Wingate tests interspersed with 3-min recovery periods. SIgA secretion rate (S-SIgA) and the relation of SIgA to total protein were calculated from measures of saliva flow rate, and absolute SIgA and salivary protein concentration samples were collected before and after exercise testing. Peak and mean mechanical power output and exercise heart-rate recovery were also measured. Of the 38 participants initially enrolled in this investigation, 11 failed to complete one or more basic study requirements, and the final data analyses were performed on measurements obtained from 27 participants. Com-pared with rest, S-SIgA, SIgA-to-protein ratio, and saliva flow rate were signifi-cantly lower after exercise than at baseline. Likewise, both peak and mean mechanical power output significantly declined across consecutive Wingate tests. Postintervention minus preintervention changes in scores for salivary parameters, exercise performance, and exercise heart-rate recovery were similar between the treatment groups. These findings do not support the hypothesis that ginseng affects
304 Bahrke, Morgan, and Stegner
mucosal immunity as indicated by changes in secretory IgA at rest and after an exercise-induced state of homeostatic disturbance. Supplementation with ginseng failed to improve physical performance and heart-rate recovery of individuals undergoing repeated bouts of exhaustive exercise.
Strength and Power Performance
In an investigation by Youl Kang, Hwan Kim, Jun Lee, and Byrne (2002) designed to assess the anabolic effects of ginseng ingestion on growth hormone, testoster-one, cortisol, and insulinlike growth factor-1 to acute resistance exercise, 8 male college students were randomly administered 20 g of Korean red ginseng root extract or water immediately after a standardized exercise bout. The exercise con-sisted of a seven-repetition maximum of the half squat, bench press, two-leg curl, arm curl, two-leg extension, abdominal crunch, leg press, and chest press. Venous blood samples were drawn before and immediately after exercise and at again at 15, 30, 60, and 120 min after exercise. Human growth hormone, testosterone, cortisol, and insulinlike growth factor-1 levels were determined by radioimmuno-assay. The responses of plasma hormones did not differ significantly after the treatments. These results do not support the use of ginseng to promote anabolic hormonal status after resistance exercise.
Aerobic Exercise Performance
To evaluate the effectiveness of 14 days of treatment with Eleutherococcus senti-cosus (900 mg/day) as an ergogenic nutritional supplement, Chase, Darby, Liang, and Morgan (2000) employed a double-blind, crossover study with 11 partici-pants performing four running trials before and after treadmill running at 80% of VO2max until volitional exhaustion after Eleutherococcus senticosus and placebo treatments. There was no statistically significant difference between trials for any of the dependent variables including time to exhaustion. The investigators con-cluded that 14 days of supplementation with Eleutherococcus senticosus has no ergogenic effect on metabolism and performance.
To determine whether Panax quinquefolium attenuates creatine kinase level induced by aerobic endurance exercise in humans, Hsu, Ho, Lin, Su, and Hsu (2005) divided 13 male college students into a ginseng group and a placebo group. In a double-blind study, participants received supplementation (400 mg, four per day) for 4 weeks, followed by a 4-week washout period, before crossing over and receiving the alternate treatment for the next 4 weeks. Treadmill running at 80% of VO2max was performed after each treatment. Plasma creatine kinase and lactate were measured before the exercise, at 15 and 30 min during exercise, immediately after exercise, and 20, 40, 60, and 120 min after exercise. In addition, time to exhaustion and oxygen pulse were also measured. Although ginseng supplemen-tation for 4 weeks before exhaustive aerobic treadmill running was associated with reduced leakage of creatine kinase from skeletal sarcoplasm into the blood during exercise, it did not enhance performance.
It has been reported by Kim, Park, Chang, and Sung (2005) that administra-tion of Panax ginseng increases endurance time to exhaustion. In their study, 7 sedentary males performed incremental exercise to volitional exhaustion on a treadmill before and after 8 weeks of Panax ginseng extract administration. Exer-

Is Ginseng an Ergogenic Aid? 305
cise duration until exhaustion was significantly increased by 1.5 min, leading the investigators to conclude that ginseng has ergogenic properties. There are a number of reasons that these findings and conclusions must be viewed with cau-tion. First, a small sample size of 7 males served as participants, and these indi-viduals served as their own controls. Second, the control testing was carried out before the ginseng intervention, and it is possible that there was an order effect. That is, the conditions should have been rotated and randomly assigned to the participants (i.e., AB and BA). Third, the participants were recruited on the basis that they “had not performed any systematic training,” and this is problematic for two reasons. First, pretest sensitization might have taken place, and second, the results cannot be generalized to athletes. Fourth, there was no blinding, and there-fore the observed results might have been caused by the halo effect, Hawthorne effect, demand characteristics, or expectancy effects.
In a double-blind, placebo-controlled investigation to determine the effective-ness of a moderately high dose of Panax notoginseng (a species of the genus Panax) on aerobic capacity, endurance, and blood pressure in young adults, Liang, Pod-olka, and Chuang (2005) randomly assigned 29 untrained adults to an experimental group or placebo control group. For 30 days, participants in the experimental group consumed 1,350 mg/day of Panax notoginseng, while participants in the control group consumed a placebo. Endurance time to exhaustion during cycle exercise was significantly improved in the experimental group by more than 7 min, and mean blood pressure and oxygen consumption decreased during endurance exer-cise. The significant improvement in endurance time demonstrated by this investi-gation compared with others is noteworthy for several reasons: A relatively high dose of assayed ginseng was used, duration of consumption was for 30 days, and the type of ginseng consumed was Panax notoginseng, as opposed to the more frequently used Panax ginseng. In addition, the experimental design was compara-tively rigorous, being double-blind with random assignment of a moderate number of participants to either a treatment or a placebo group. The investigators report that participants were randomly assigned to the placebo and ginseng treatments, but there was a substantial difference in VO2max at the outset of the study. The entire point of using randomization is to ensure that experimental and placebo groups are equivalent from the outset of a study on all variables of relevance to the inquiry. The effect size for the difference in VO2max was large (.81), and this is problematic. In other words, the ginseng group, for some reason, was superior to the placebo group from the outset on an important dimension of physical fitness.
Anaerobic Exercise Performance
To investigate the effects of ginseng supplementation on supramaximal exercise performance and short-term recovery, Engels, Kolokouri, Cieslak, and Wirth (2001) used a double-blind protocol and randomly assigned 24 healthy, active women to either a ginseng or a placebo treatment. Each participant added a stan-dardized extract (400 mg G115) of Panax ginseng C.A. Meyer or a placebo to their normal diet for 8 weeks. Before and after the treatment period, each participant performed an all-out-effort, 30-s leg-cycle-ergometry test followed by a controlled recovery. Nineteen participants completed the study. Of the 5 lost to follow-up, 3 were from the placebo group and 2 were from the ginseng group. Results revealed no significant differences between the ginseng and placebo treatment groups for

306 Bahrke, Morgan, and Stegner
peak or mean anaerobic power output, rate of fatigue, or immediate postexercise recovery heart rates. Engels et al. (2001) concluded that prolonged supplementa-tion with ginseng had no ergogenic benefits during and after brief, supramaximal exercise. Effect sizes for the ginseng treatment were small (peak anaerobic power, .00; mean anaerobic power, .06; rate of fatigue, .38).
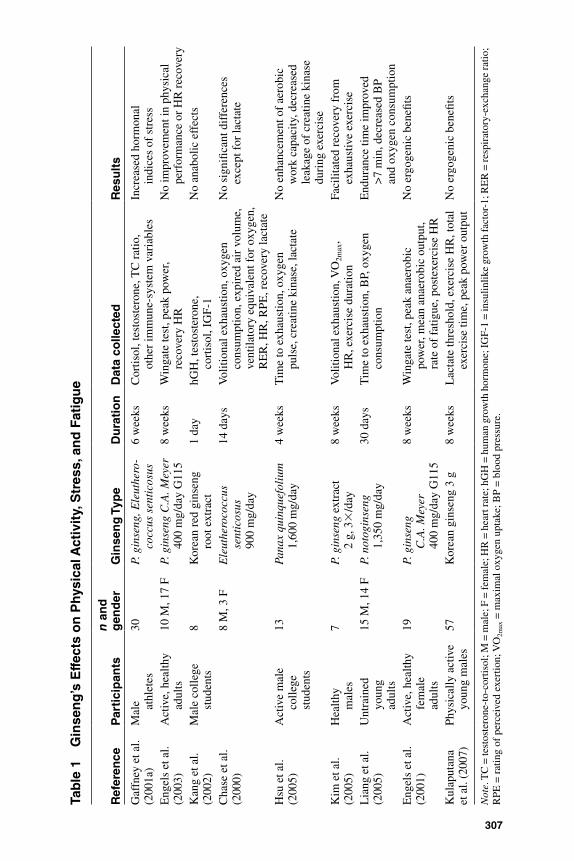
To determine the effects of ginseng supplementation on lactate threshold and physical performance, Kulaputana, Thanakomsirichot, and Anomasiri (2007) ran-domly assigned 57 physically active young men to either a ginseng (n = 28) or a placebo group (n = 29). Participants in the ginseng group consumed 3 g of ginseng orally each day for 8 weeks. Blood lactic acid levels and heart-rate responses were measured during incremental cycle-ergometer work before and after the 8 weeks of treatment. Selected markers for liver and renal function were also monitored. Lactate threshold, exercise heart rate, total exercise time, and peak power output did not differ between ginseng and placebo groups, demonstrating in a well- controlled study (randomized, double-blinded, placebo-controlled, treatment-compliance monitoring) that ginseng supplementation did not exert an ergogenic effect on the physical performance of a relatively large group of physically active young men. The reports described in this section are summarized in Table 1.
In conclusion, additional, well-designed research is needed to determine whether supplementation with ginseng and related products can improve perfor-mance and alleviate stress and fatigue when functional abilities are diminished, such as through repetitive bouts of strenuous physical work. Moreover, the poten-tial use of ginseng and related products to enhance performance, recovery, and muscle growth from anaerobic exercise has not yet been adequately investigated.
Psychological, Behavioral, and Cognitive EffectsAlthough the positive effects of ginseng and ginseng-related products on psycho-logical function, moods, behavior, stress reduction, and chronic pain in humans have been reported in a few of the earlier studies in this area—perhaps resulting from several central and peripheral physiological effects including cardiovascular, neural, and hormonal effects (Bahrke & Morgan, 1994, 2000)—a more recent research study failed to demonstrate enhanced mood after ginseng administration in healthy young adults. Using a double-blind, placebo-controlled, randomized clinical trial, Cardinal and Engels (2001) examined psychological well-being in healthy young adults. Ninety-six adults were randomly assigned to one of three experimental conditions: placebo, 200 mg ginseng (Panax ginseng C.A. Meyer concentrate G115 in capsular form), or 400 mg ginseng (Panax ginseng C.A. Meyer concentrate G115 in capsular form). Participants were given a 60-day supply of their respective supplement along with written instructions about proper intake and storage of the capsules over the 8-week study period, and a postinter-vention appointment was scheduled for each participant. Eighty-three (or 86.5%) of the original participants completed the study, with the primary reason for attri-tion being noncompliance with the study protocol. Positive affect, negative affect, and overall mood measures were obtained pre- and postintervention. Ginseng supplementation had no effect on positive affect, negative affect, or overall mood, leading the researchers to conclude that chronic ginseng supplementation at either the clinically recommended dose or at twice that level does not enhance mood in
307
Tab
le 1
G
inse
ng
’s E
ffec
ts o
n P
hysi
cal A
ctiv
ity,
Str
ess,
an
d F
atig
ue
Ref
eren
ceP
arti
cip
ants
n a
nd
g
end
erG
inse
ng
Typ
eD
ura
tio
nD
ata
colle
cted
Res
ult
s
Gaf
fney
et a
l.
(200
1a)
Mal
e
athl
etes
30P.
gin
seng
, Ele
uthe
ro-
cocc
us s
enti
cosu
s6
wee
ksC
ortis
ol, t
esto
ster
one,
TC
rat
io,
othe
r im
mun
e-sy
stem
var
iabl
esIn
crea
sed
horm
onal
in
dice
s of
str
ess
Eng
els
et a
l.
(200
3)A
ctiv
e, h
ealth
y
adul
ts10
M, 1
7 F
P. g
inse
ng C
.A. M
eyer
40
0 m
g/da
y G
115
8 w
eeks
Win
gate
test
, pea
k po
wer
, re
cove
ry H
RN
o im
prov
emen
t in
phys
ical
pe
rfor
man
ce o
r H
R r
ecov
ery
Kan
g et
al.
(2
002)
Mal
e co
llege
st
uden
ts8
Kor
ean
red
gins
eng
ro
ot e
xtra
ct1
day
hGH
, tes
tost
eron
e,
cort
isol
, IG
F-1
No
anab
olic
eff
ects
Cha
se e
t al.
(2
000)
8 M
, 3 F
Ele
uthe
roco
ccus
se
ntic
osus
90
0 m
g/da
y
14 d
ays
Vol
ition
al e
xhau
stio
n, o
xyge
n
cons
umpt
ion,
exp
ired
air
vol
ume,
ve
ntila
tory
equ
ival
ent f
or o
xyge
n,
RE
R, H
R, R
PE, r
ecov
ery
lact
ate
No
sign
ifica
nt d
iffe
renc
es
exce
pt f
or la
ctat
e
Hsu
et a
l.
(200
5)A
ctiv
e m
ale
co
llege
st
uden
ts
13Pa
nax
quin
quef
oliu
m
1,60
0 m
g/da
y4
wee
ksT
ime
to e
xhau
stio
n, o
xyge
n
puls
e, c
reat
ine
kina
se, l
acta
teN
o en
hanc
emen
t of
aero
bic
w
ork
capa
city
, dec
reas
ed
leak
age
of c
reat
ine
kina
se
duri
ng e
xerc
ise
Kim
et a
l.
(200
5)H
ealth
y
mal
es7
P. g
inse
ng e
xtra
ct
2 g,
3
/day
8 w
eeks
Vol
ition
al e
xhau
stio
n, V
O2m
ax,
HR
, exe
rcis
e du
ratio
nFa
cilit
ated
rec
over
y fr
om
exha
ustiv
e ex
erci
seL
iang
et a
l. (2
005)
Unt
rain
ed
youn
g
adul
ts
15 M
, 14
FP.
not
ogin
seng
1,
350
mg/
day
30 d
ays
Tim
e to
exh
aust
ion,
BP,
oxy
gen
co
nsum
ptio
nE
ndur
ance
tim
e im
prov
ed
>7
min
, dec
reas
ed B
P
and
oxyg
en c
onsu
mpt
ion
Eng
els
et a
l.
(200
1)A
ctiv
e, h
ealth
y
fem
ale
ad
ults
19P.
gin
seng
C
.A. M
eyer
40
0 m
g/da
y G
115
8 w
eeks
Win
gate
test
, pea
k an
aero
bic
po
wer
, mea
n an
aero
bic
outp
ut,
rate
of
fatig
ue, p
oste
xerc
ise
HR
No
ergo
geni
c be
nefit
s
Kul
aput
ana
et
al.
(200
7)Ph
ysic
ally
act
ive
youn
g m
ales
57K
orea
n gi
nsen
g 3
g8
wee
ksL
acta
te th
resh
old,
exe
rcis
e H
R, t
otal
ex
erci
se ti
me,
pea
k po
wer
out
put
No
ergo
geni
c be
nefit
s
Not
e. T
C =
test
oste
rone
-to-
cort
isol
; M =
mal
e; F
= fe
mal
e; H
R =
hea
rt ra
te; h
GH
= h
uman
gro
wth
hor
mon
e; IG
F-1
= in
sulin
like
grow
th fa
ctor
-1; R
ER
= re
spir
ator
y-ex
chan
ge ra
tio;
RPE
= r
atin
g of
per
ceiv
ed e
xert
ion;
VO
2max
= m
axim
al o
xyge
n up
take
; BP
= b
lood
pre
ssur
e.

308 Bahrke, Morgan, and Stegner
healthy young adults. It might be, however, that ginseng has little or no effect when administered to healthy adults scoring in the normal range on mood states. The investigators did not examine the effects of ginseng in study participants with elevated mood scores.
In sports in which quick decision making is required, it is not unusual for athletes to consume products thought to provide an advantage over the competi-tion. However, although previous research suggests that chronic administration of ginseng can improve cognitive performance in humans (Bahrke & Morgan, 1994, 2000), it has not examined the effects of a single dose of ginseng on cognitive performance in healthy adults or in athletes.
In an investigation to determine whether acute administration of ginseng (G115) had any consistent effect on mood and cognitive performance in humans, Kennedy, Scholey, and Wesnes (2001b) used a placebo-controlled, double-blind, balanced, crossover design. Quality of memory, speed of memory, quality of attention, and speed of attention served as the cognitive measures. Twenty healthy young-adult volunteers received 200, 400, and 600 mg of G115 and a matching placebo, in counterbalanced order, with a 7-day washout period between treat-ments. After a baseline cognitive assessment, further test sessions took place at 1, 2.5, 4, and 6 hr after the day’s treatment. Significant improvement was found for quality of memory and the associated factor known as secondary memory at all points after the administration of 400 mg of ginseng. The 200- and 600-mg doses were both associated with a significant decrement in attention speed at later test-ing times only. Subjective ratings of alertness were also reduced 6 hr after the two lowest doses (200 mg and 400 mg). These results indicate that modulation of mood and cognitive performance might occur after acute administration of gin-seng, but there is not a linear dose-response effect. That is, a moderate dose of 400 mg seems to enhance performance, whereas low (200 mg) and high (600 mg) doses impair it. It would be noteworthy, of course, if similar results were found in exercise and sport settings.
In a subsequent investigation, but with different dosages, Kennedy, Scholey, and Wesnes (2001a) examined the effects of a combination of standardized extracts of Ginkgo biloba (GK501) and Panax ginseng (G115) on mood and selected aspects of cognitive performance (quality of memory, speed of memory, quality of attention, and speed of attention). Using a placebo-controlled, double-blind, balanced, crossover design, 20 healthy young-adult volunteers received 320, 640, and 960 mg of the extract combination and a matching placebo in a random order, with a 7-day washout period between treatments. After a baseline cognitive assessment, further testing took place at 1, 2.5, 4, and 6 hr after the day’s treatment. There was a dose-response improvement in performance on the quality-of-memory factor at the highest dose (960 mg). Additional analysis indicated that this effect was differentially targeted at secondary memory rather than the work-ing-memory component. There was also a dose-response decrement in perfor-mance of the speed-of-attention factor for the 320- and the 640-mg dose. The results of this study suggest that ingesting single doses of a Ginkgo biloba and Panax ginseng combination can affect the cognitive performance of healthy young volunteers in a dose-response manner in that low doses are associated with perfor-mance decrements while high doses enhance performance. The underlying mech-anisms for these effects remain to be elucidated.

Is Ginseng an Ergogenic Aid? 309
In a related investigation, Kennedy, Scholey, and Wesnes (2002) directly compared the effects of single doses of Ginkgo biloba, ginseng, and a gingko–ginseng combination on aspects of mood and cognitive performance using partici-pants from the same cohort of healthy young-adult volunteers. In a randomized, placebo-controlled, double-blind, balanced, crossover design, 20 participants received what investigators referred to as “the most beneficial dose” from each of their previous Cognitive Drug Research battery–based studies: 360 mg of Ginkgo biloba, 400 mg of ginseng, 960 mg of a product combining the two extracts with an inert substance, and a matching placebo. Treatment was random and there was a 7-day washout period between treatments. Cognitive testing involved the Cogni-tive Drug Research Battery and two serial-subtraction mental-arithmetic tasks. Mood was assessed with the Bond–Lader visual analog scales. After a baseline cognitive assessment, further testing took place at 1, 2.5, 4, and 6 hr after the day’s treatment was taken. All three treatments were associated with improved secondary-memory performance as measured by the Cognitive Drug Research Battery, with the ginseng condition resulting in some improvement in the speed of performing memory tasks and in the accuracy of attentional tasks. After ginkgo and the ginkgo–ginseng combination, performance of both subtraction tasks was improved at the later testing sessions. No change in the speed of performing atten-tion tasks was found. Improvement in self-rated mood was also found after ginkgo and, to a lesser extent, the combination product. These results suggest that ingest-ing single doses of Ginkgo biloba, Panax ginseng, and a product combining the two extracts can beneficially influence the cognitive performance of healthy young volunteers. Although findings of this nature are often advanced as evidence of the efficacy of ginseng and related substances to enhance performance in athletes, there is an absence of compelling research evidence to support such views. This research lacks what is known as external validity, and it would be a fundamental scientific error to make such generalizations.
The electroencephalographic (EEG) effects of single doses of Ginkgo biloba and Panax ginseng in healthy young volunteers have also been examined by Ken-nedy et al.(2003). Using a double-blind, placebo-controlled, balanced crossover experiment, the effects of single doses of Ginkgo biloba (360 mg GK501), Panax ginseng (200 mg G115), and a placebo on auditory-evoked potential using contin-gent negative variation and resting power within the delta, theta, alpha, and beta wavebands were evaluated in 15 healthy volunteers. Each participant was assessed on three separate occasions, 4 hr after consuming the treatment of the day. Seven days elapsed between testing sessions. Results indicated that ginseng led to a significant shortening of the latency of the P300 component of the evoked poten-tial. Both ginseng and Ginkgo biloba led to significant reductions in frontal “eyes closed” theta and beta activity, with additional reduction for ginseng in the alpha waveband. These findings demonstrate that Panax ginseng can directly modulate cerebroelectrical activity and that these effects are more pronounced than those of Ginkgo biloba. This potential for ginseng to enhance cognitive performance and mood has been reviewed in greater detail by Kennedy and Scholey (2003) and Scholey and Kennedy (2002). It should also be noted that EEG data cannot be used as evidence of activity in subcortical regions, and there is a need for neu-roimaging research (e.g., MRI, PET, SPECT) designed to elucidate the impact of ginseng use on various brain regions.

310 Bahrke, Morgan, and Stegner
In one of the few ginseng-administration studies conducted with athletes, improved psychomotor performance at rest and during graded exercise after gin-seng treatment (350 mg/day for 6 weeks) in young athletes was demonstrated by Ziemba et al. (1999). In a double-blind study, 15 soccer players underwent either ginseng treatment or placebo treatment. Before and after treatment all participants performed an incremental bicycle-ergometer exercise with intensity increasing 50 W every 3 min until volitional exhaustion (time-to-exhaustion data not presented). Reaction time was measured before exercise and during the last 2 min of each exercise load. Although neither ginseng nor placebo influenced VO2max or lactate threshold, ginseng treatment was associated with shortened reaction times at rest and during exercise.
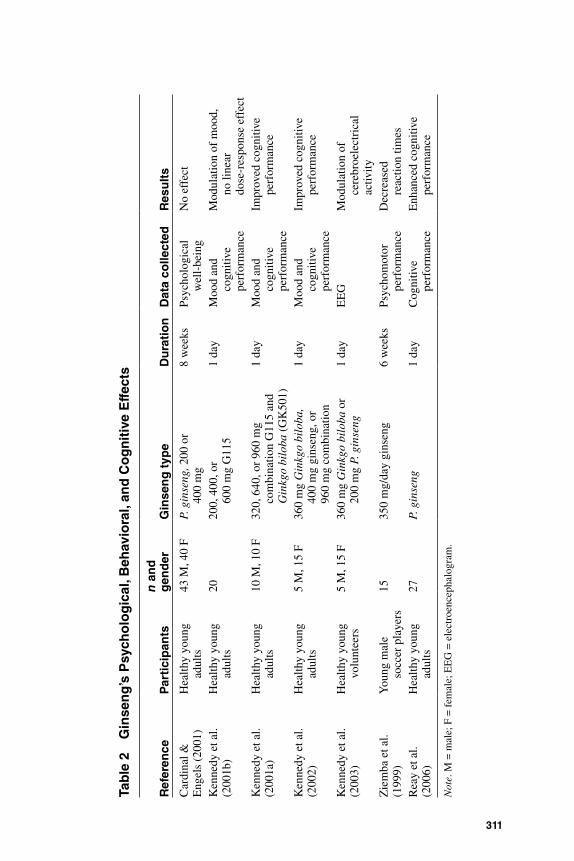
To elucidate the mechanisms for the glucoregulatory properties and enhance-ment of cognitive performance after ginseng administration, in a double-blind, balanced crossover study, Reay, Kennedy, and Scholey (2006) used a “cognitive demand” test battery at baseline, 30 min after administration of either ginseng or a placebo, and another 30 min later after consumption of a drink containing glu-cose or a placebo. Both ginseng and glucose were associated with enhanced cog-nitive performance. Ginseng was associated with a reduction in blood glucose levels 1 hr after consumption when ingested without glucose, confirming that gin-seng might lower blood glucose levels and enhance cognitive performance. Although the mechanisms responsible for ginseng’s glycemic effect or its cogni-tive effects were not clarified by that investigation, possible mechanisms for lower blood glucose levels and improved cognitive performance could include the mod-ulation of glucose disposal, glucose transport, or insulin secretion. The reports described in this section are summarized in Table 2.
In conclusion, although current research supports the general finding that supplementation with ginseng and related products might modulate mood, improve cognitive performance, and decrease reaction time, the ecological valid-ity of applying such results, primarily obtained using nonathletes in laboratory settings, to athletes and athletic environments is questionable.
Quality, Purity, and BioavailabilityVariability in herbal products, including ginseng, is a major concern because most dietary supplements are not subject to the same regulations as pharmaceuticals, and these herbal products might lack purity or potency. Hence, research involving herbal products is associated with major “sourcing” problems, and it is imperative that investigators assay the content of products employed in experiments designed to quantify efficacy. In our view, it is noteworthy that nearly all the investigations in the current review failed to include an assay of the actual content of the sub-stances used in the experiment.
To determine the variability in a range of ginseng-containing products avail-able in the United States, Harkey, Henderson, Gershwin, Stern, and Hackman (2001) identified and measured the concentration of marker compounds by using high-performance liquid chromatography and liquid-chromatography tandem mass spectrometry. Twenty-five commercial ginseng preparations of Panax gin-seng or Eleutherococcus senticosus were obtained from a local health food store and analyzed for seven ginsenosides and two eleutherosides. All plant species
311
Tab
le 2
G
inse
ng
’s P
sych
olo
gic
al, B
ehav
iora
l, an
d C
og
nit
ive
Eff
ects
Ref
eren
ceP
arti
cip
ants
n a
nd
g
end
erG
inse
ng
typ
eD
ura
tio
nD
ata
colle
cted
Res
ult
s
Car
dina
l &
Eng
els
(200
1)H
ealth
y yo
ung
ad
ults
43 M
, 40
FP.
gin
seng
, 200
or
400
mg
8 w
eeks
Psyc
holo
gica
l w
ell-
bein
gN
o ef
fect
Ken
nedy
et a
l.
(200
1b)
Hea
lthy
youn
g
adul
ts20
200,
400
, or
60
0 m
g G
115
1 da
yM
ood
and
co
gniti
ve
perf
orm
ance
Mod
ulat
ion
of m
ood,
no
line
ar
dose
-res
pons
e ef
fect
Ken
nedy
et a
l.
(200
1a)
Hea
lthy
youn
g
adul
ts10
M, 1
0 F
320,
640
, or
960
mg
co
mbi
natio
n G
115
and
G
inkg
o bi
loba
(G
K50
1)
1 da
yM
ood
and
co
gniti
ve
perf
orm
ance
Impr
oved
cog
nitiv
e
perf
orm
ance
Ken
nedy
et a
l.
(200
2)H
ealth
y yo
ung
ad
ults
5 M
, 15
F36
0 m
g G
inkg
o bi
loba
, 40
0 m
g gi
nsen
g, o
r
960
mg
com
bina
tion
1 da
yM
ood
and
co
gniti
ve
perf
orm
ance
Impr
oved
cog
nitiv
e
perf
orm
ance
Ken
nedy
et a
l.
(200
3)H
ealth
y yo
ung
vo
lunt
eers
5 M
, 15
F36
0 m
g G
inkg
o bi
loba
or
200
mg
P. g
inse
ng1
day
EE
GM
odul
atio
n of
ce
rebr
oele
ctri
cal
activ
ityZ
iem
ba e
t al.
(1
999)
You
ng m
ale
so
ccer
pla
yers
1535
0 m
g/da
y gi
nsen
g6
wee
ksPs
ycho
mot
or
perf
orm
ance
Dec
reas
ed
reac
tion
times
Rea
y et
al.
(2
006)
Hea
lthy
youn
g
adul
ts27
P. g
inse
ng1
day
Cog
nitiv
e
perf
orm
ance
Enh
ance
d co
gniti
ve
perf
orm
ance
Not
e. M
= m
ale;
F =
fem
ale;
EE
G =
ele
ctro
ence
phal
ogra
m.
312 Bahrke, Morgan, and Stegner
were correctly identified by botanical plant species, but concentrations of marker compounds differed significantly from labeled amounts. There was also signifi-cant product-to-product variability; concentrations of ginsenosides varied by 15- and 36-fold in capsules and liquids, respectively; and concentrations of eleuthero-sides varied by 43- and 200-fold in capsules and liquids, respectively. The results of the survey suggest that standardization for quality assurance is important in designing and evaluating ginseng studies.
In a study to determine whether the commercial formulations of several botanical dietary supplements, including ginseng, had consistent labeling and whether quantities of marker compounds agreed with the amounts on the label, Krochmal et al. (2004) purchased six bottles each of two lots of supplements from nine manufacturers and analyzed the contents using established commercial meth-odologies at an independent laboratory. Product labels were found to vary in the information provided, such as serving recommendations and information about the herb itself (e.g., species, part of the plant, marker compound). With regard to marker-compound content, little variability was observed between different lots of the same brand, but the content did vary widely between brands (e.g., total ginsenosides ranged from 5.3 to 18.2 mg per serving). Furthermore, the amounts recommended for daily use also differed between brands, increasing the potential range of a consumer’s daily dose. Ginseng was among the most variable. This study emphasizes the importance of standardized manufacturing practices and reliable labeling information.
Using high-performance liquid chromatography to evaluate the effects of dif-ferent samples of Panax quinquefolius cultivated in Wisconsin and Illinois, Yuan et al. (2001) found considerable variability in the brainstem activity of neonatal rats for the two samples. In a comparison of six ginsenosides from these two specimens, data revealed remarkable variability in the total concentration and in the percentages of individual ginsenosides. For example, of the two major ginse-nosides, the Illinois-cultivated Panax quinquefolius had 30% less ginsenoside Rb1 and 25% more ginsenoside Re than did the Wisconsin-cultivated Panax quinquefolius.
As part of a program for assessing the quality of herbal medicines, Khan et al. (2001) analyzed 21 over-the-counter Panax ginseng products in various doses, including 8 liquid samples and 13 solid samples. Chromium, mercury, and arsenic were not present in amounts above their limits of detection in both liquid and solid samples, but cadmium, lead, and nickel were present in most of the samples. Chlorinated pesticide levels varied widely in these samples. The total concentra-tion of pesticides was below 100 ppb in most samples, but the total concentration exceeded 100 ppb in five samples. In addition, the U.S. Food and Drug Adminis-tration recently issued a warning that certain ginseng products are considered adulterated because they contain unsafe chemical residues from the pesticides procymidone and quintozene (Anonymous, 2005). In another investigation exam-ining the concentrations of cadmium, lead, mercury, and metalloid arsenic in dietetic products, Dragun et al. (2003) found the highest concentration of mercury in a ginseng-based sample. Raman, Patino, and Nair (2004) failed to find unac-ceptable concentrations of metals such as lead and mercury in eight botanical dietary supplements including ginseng. However, these supplements were also evaluated for microbial contamination, and most samples showed the presence of

Is Ginseng an Ergogenic Aid? 313
bacteria, fungi, or both. These results serve to identify the problem of environ-mental contamination of dietary supplements and emphasize the necessity to develop validated quantitative methods to analyze such contaminants in the vari-ous herbal products currently available.
The results cited herein also emphasize that future investigations on the effec-tiveness of ginseng should rely on the use of standardized methods and prepara-tions. In fact, Sievenpiper, Arnason, Vidgen, Leiter, and Vuksan (2004), after con-ducting a systematic quantitative analysis of the literature and finding a high coefficient of variation in ginsenosides across species, assay technique, and ginse-noside type, concluded “that until these issues are resolved, the reproducibility of ginseng’s composition, safety, and efficacy cannot be trusted” (p. 840).
In an attempt to authenticate the differences between various types of Panax ginseng and to offer confidence to consumers, Hon, Chow, Zeng, and Leung (2003) developed a set of microsatellite markers with discrete genotypes for American ginseng (Panax quinquefolius) that are able to differentiate Panax quin-quefolius from Panax ginseng with resolution down to specific, individual farm level—that is, confirmation of its botanical identity and origin. Compared with other molecular techniques, microsatellite-marker technology is more robust, accurate, reproducible, reliable, and sensitive. Also to ensure quality control and standardization of ginseng, Asafu-Adjaye and Wong (2003), using liquid chroma-tography in an interlaboratory study involving 12 collaborating laboratories, reli-ably identified six common ginsenosides in dry root powder from Panax ginseng, Panax quinquefolius, and two selected commercial ginseng products. In response to the need to standardize the quality and purity of ginseng products, the Korean Ministry of Agriculture and Forestry (“Korea Promoting,” 2002) submitted a draft on the international food standard for ginseng to the Italian-based executive office of the Codex Alimentarius Commission. This commission was created by the Food and Agriculture Organization and the World Health Organization to facili-tate standardization of food. The draft includes basic conditions including the definition range and structural elements of ginseng.
One of the factors in determining the ergogenic effects of ginseng is the sys-temic availability and degradation of the constituent ginsenosides after oral admin-istration in humans. Using mass spectrometry, Tawab, Bahr, Karas, Wurglics, and Schubert-Zsilavecz (2003) studied the degradation of ginsenosides in the gastro-intestinal tract of humans after oral administration of ginseng. Plasma and urine samples from 2 human participants were screened for ginsenosides and their pos-sible degradation products. It was shown that two hydrolysis products of the pro-topanaxatriol ginsenosides G-Rh and G-F might reach the systemic circulation. In addition, compound K, the main intestinal bacterial metabolite of the protopanax-adiol ginsenosides, was detected in plasma and urine. These substances or compo-nents are probably responsible for the action of ginseng in humans.
Adverse Effects, Drug Interactions, and SafetyThe adverse effects associated with ginseng consumption have been reported pre-viously (Bahrke & Morgan, 1994, 2000). Although ginseng is thought to be rela-tively safe, several recent reports on its adverse effects have been published. A systematic attempt to document and evaluate all the available data on the safety of

314 Bahrke, Morgan, and Stegner
Panax ginseng root extracts was conducted by Coon and Ernst (2002). Data from clinical trials suggest that the incidence of adverse events with ginseng mono-preparations is similar to that of placebo. The most commonly experienced adverse effects are headache, sleep disturbances, and gastrointestinal disorders. The pos-sibility of more serious adverse effects is indicated in isolated case-study reports and data from spontaneous reporting schemes, but causality is often difficult to determine from the evidence provided. Combination products containing ginseng as one of several constituents have been associated with serious adverse events and even fatalities. Interpreting these cases is difficult, however, because ingredi-ents other than Panax ginseng might have caused the problems. Possible drug interactions have been reported between Panax ginseng and warfarin, phenelzine, and alcohol. Collectively, these data suggest that Panax ginseng monoprepara-tions are rarely associated with adverse events or drug interactions. Combined preparations are more often associated with such events, but causal attribution is usually not possible.
Although many investigations examining the effects of ginseng have been published, many of these studies involved small numbers of participants, includ-ing case-study reports. Case-study reports are limited in their representativeness. They do not necessarily allow valid generalizations to the population from which they came, and they are vulnerable to subjective biases. Case-study reports might be selected because of their dramatic rather than typical attributes or because they neatly fit an observer’s preconceptions. Case-study reports should prompt addi-tional investigation with a greater number of participants. Results of case studies can be used as hypotheses to be tested using rigorous experimental designs incor-porating appropriate control and placebo paradigms.
The efficacy and safety of ginseng have also been evaluated by Kitts and Hu (2000), who concluded that “while some epidemiological or clinical studies have reported indications of efficacy for specific health benefits or potential toxicity, there are an equal number of studies that provide contradictory evidence,” and furthermore “this situation has lead to questionable conclusions concerning spe-cific health benefits or risks associated with ginseng” (p. 473). Ernst (2002) also examined the risk–benefit profile of several commonly used herbal therapies including ginseng and concluded that “well-conducted clinical trials do not sup-port the efficacy of ginseng to treat any condition” and that “none of these herbal medicines are free of adverse effects” (p. 42).
When reports of adverse effects from herbal preparations are carefully assessed, it is often found that the effects are not caused by the herbs listed on the label but, rather, by adulteration or contamination of the declared ingredients. A case of ginseng-induced mania in a healthy 26-year-old man with no history of psychiatric illness was reported by Engelberg, McCutcheon, and Wiseman (2001). The presenting symptom at the time of hospitalization was the patient’s increas-ingly bizarre behavior. This individual had been consuming two or three capsules of Chinese red Panax ginseng 5 days per week for 2 months in an attempt to boost his energy. The product label claimed that each capsule contained the equivalent of 250 mg of ginseng root. Laboratory analysis of the same brand of product revealed no evidence of controlled drugs or other notable contaminants. The symptoms resolved after treatment and discontinuation of the ginseng prepara-tion, and the cause of the mania was attributed to the patient’s use of ginseng.
Is Ginseng an Ergogenic Aid? 315
Development of manic symptoms in a patient taking ginseng has been reported by Vazquez and Aguera-Ortiz (2002). The patient, a 56-year-old woman with previous affective disorder, and taking antidepressant medica-tion, developed a manic episode while consuming ginseng. Symptoms disap-peared after treatment including discontinuation of the ginseng supplement. Nonetheless, the question that remains unanswered in such cases is whether the development of mania was caused by the antidepressant drug, the ginseng, or the interaction of the two. A case of transient ischemic attack secondary to hypertensive crisis related to the consumption of Panax ginseng has been reported by Martinez-Mir, Rubio, Morales-Olivas, and Palop-Larrea (2004). The patient, a 64-year-old man, complained of fugax amaurosis on two occa-sions, with arterial blood pressure readings of 200/120 and 220/130 mm Hg after 13 days of ginseng consumption. Blood pressure returned to its previous level 1 week after cessation of the Panax ginseng. One year later at follow-up, the patient remained normotensive.
Photosensitivity reaction in a woman using an herbal supplement has been described by Palanisamy, Halter, and Olson (2003). This 32-year-old woman suf-fered a phototoxic reaction after taking a dietary supplement containing ginseng, goldenseal, bee pollen, and other ingredients. The condition slowly resolved after discontinuation of the supplement and treatment with subcutaneous and topical corticosteroids. Although the individual ingredients in the dietary supplement have not been associated with cases of photosensitivity it is possible that the com-bination of ingredients interacted to cause the toxic reaction. Caution is urged in the use of combined herbs and supplements in new formulations that have not been evaluated in controlled trials.
A case of anaphylactic reaction resulting from ingestion of Asian ginseng syrup in a 20-year-old man has also been reported by Wiwanitkit and Taungjaru-winai (2004). Because ginseng is a widely consumed herb, potential adverse effects such as allergic reaction need to be emphasized.
Ginseng and Eleutherococcus senticosis have also been reported to interact with certain oral-health drugs such as aspirin and corticosteroids, suggesting that use of these products might be associated with various adverse reactions that can influence oral health and treatment. According to Abebe (2003), dentists and dental hygienists need to be aware of these interactions and offer appropriate oral-health care to individuals using these substances.
A case of menstrual alterations related to ginseng consumption has been reported by Palop-Larrea, Gonzalvez-Perales, Catalan-Oliver, Belenguer-Varea, and Martinez-Mir (2000). A 48-year-old woman, who had never experienced menstrual disorders in the past, was admitted after a 3-week history of metror-rhagia after self-medication with three daily capsules for 2 months of a ginseng compound. A companion advised her to take the ginseng to improve her work performance. The metrorrhagia disappeared 4 days after she discontinued taking the ginseng. More recently, Kabalak, Soyal, Urfalioglu, Saracoglu, and Gogus (2004) also reported menometrorrhagia and tachyarrhythmia after use of oral and topical ginseng for cosmetic reasons in a 39-year-old female patient. The patient was advised to stop using ginseng capsules and ginseng cosmetics, and her menometrorrhagia did not recur during the following 6 months. Given the exten-sive literature documenting menstrual dysfunction among female endurance

316 Bahrke, Morgan, and Stegner
athletes, extra caution might be warranted when using various ginseng prepara-tions. With the many adverse effects associated with the use of ginseng, all users would be wise to exhibit caution.
ConclusionsGinseng is one of the most popular herbal supplements in the world. It is widely used by the general public to increase work capacity and output and by athletes to enhance performance. In the current review we have provided an update of empir-ical research published since our two earlier reviews by focusing primarily on the efficacy of ginseng with respect to physical and athletic performance. We have updated the physiological effects of ginseng and ginseng-related products on physical activity, stress, and fatigue in humans; the psychological, behavioral, and cognitive effects; the quality, purity, and bioavailability of ginseng products; and the adverse health effects, drug interactions, and safety of ginseng.
Although the effects of ginseng on pulmonary function, exercise capacity, and chronic fatigue have been reported in several earlier studies, many of these investigations were conducted with patients suffering from compromised pulmo-nary function and low levels of exercise capacity. In addition, older individuals suffering from chronic fatigue often turn to herbal products such as ginseng to help combat fatigue, whereas athletes often use ginseng for prevention and treat-ment of overtraining. The studies reviewed here have also been conducted with patients and elderly individuals, and these results, obtained from ill and older adults, cannot be applied to healthy, young athletes.
Athletes are also known to use Panax ginseng or Eleutherococcus senticosus believing that these herbs decrease the incidence of colds and infections and enhance recovery from intense training. However, although previous and recent investigations reveal that ginseng and ginseng-related products might reduce inflammation and produce antistress adaptogenic activity and excitability in mice and rats, as well as enhance physical performance, these effects are rarely evident in humans studied in well-designed investigations. Several recent investigations also revealed that supplementation with ginseng does not improve physical per-formance and recovery of individuals undergoing exhaustive exercise.
The positive effects of ginseng and ginseng-related products on psychologi-cal function, moods, behavior, stress reduction, and chronic pain in animals have been reported in a few of the earlier studies in this area that we have reviewed. Findings from recent investigations using animals generally tend to support these earlier reports. However, although a few investigations reviewed here demon-strated decreased levels of stress, anxiety, and pain after administration of ginseng and ginseng-related products to animals, ginseng administration in humans has not been shown to enhance mood in healthy young adults.
In sports in which quick decision-making is required, it is not unusual for athletes to consume products thought to provide an advantage over the competi-tion. Previous research suggests that chronic administration of ginseng can improve cognitive performance in animals and in humans. Although current research supports this general finding, the ecological validity of applying such results obtained in laboratory settings to athletes and athletic environments is questionable.

Is Ginseng an Ergogenic Aid? 317
Many studies examining the pharmacological effects of ginseng and related products on humans engaged in physical performance such as that pursued by athletes frequently have not employed sound scientific design and methodology. For example, small numbers of participants might have been inadequate to pro-vide the statistical power needed to detect significant changes. There has also been a noticeable lack of double-blind and placebo-controlled investigations. Many of the studies reporting a positive influence of ginseng were supported by the sup-plier of the ginseng used in the various studies, but this potential conflict of inter-est has not been clearly stated in the published research. This is especially prob-lematic where blind paradigms have not been employed.
Variability in ginseng preparations is also a major concern because most dietary supplements are not subject to the same regulations as pharmaceuticals, and these herbal products might lack purity or potency. Hence, research involving herbal products, including ginseng, is associated with major “sourcing” problems, and it is imperative that investigators assay the content of products employed in experiments designed to quantify efficacy. It is noteworthy that only a few of the investigations in the current review included an assay of the actual content of the substances used in the experiment. In addition, there has been little or no effort to confirm whether participants took the prescribed ginseng (i.e., compliance). This emphasizes the need for future investigations in this area to use standardized prep-arations and methods.
It is important to recognize that adverse effects associated with ginseng con-sumption have been reported. Ginseng is thought to be relatively safe, and the most commonly experienced adverse effects are headache, sleep disturbances, and gastrointestinal disorders. However, several recent reports on the adverse effects of ginseng indicate that more severe outcomes can occur. These include ginseng-induced mania, transient ischemic attack, photosensitivity reaction, ana-phylactic reaction, and menstrual dysfunction.
In summary, we conclude that despite attempts in recent investigations to improve on the scientific rigor used in examining the ergogenic properties of gin-seng, many of the same methodological shortcomings observed in earlier studies persist. Compelling evidence in support of enhanced physical performance after ginseng administration in humans participating in well-designed investigations remains to be demonstrated.
ReferencesAbebe, W. (2003). An overview of herbal supplement utilization with particular emphasis
on possible interactions with dental drugs and oral manifestations. Journal of Dental Hygiene, 77, 37–46.
Anonymous. (2005). Warning on imported ginseng. FDA Consumer, 39, 3.Asafu-Adjaye, E.B., & Wong, S.K. (2003). Determination of ginsenosides (ginseng
saponins) in dry root powder form from Panax ginseng, Panax quinquefolius, and selected commercial products by liquid chromatography: Interlaboratory study. Jour-nal of AOAC International, 86, 1112–1123.
Attele, A.S., Wu, J.A., & Yuan, C-S. (1999). Ginseng pharmacology: Multiple constituents and multiple actions. Biochemical Pharmacology, 58, 1685–1693.
Bahrke, M.S., & Morgan, W.P. (1994). Evaluation of the ergogenic properties of ginseng. Sports Medicine (Auckland, N.Z.), 18, 229–248.
318 Bahrke, Morgan, and Stegner
Bahrke, M.S., & Morgan, W.P. (2000). Evaluation of the ergogenic properties of ginseng: An update. Sports Medicine (Auckland, N.Z.), 29, 113–133.
Baranov, A.I. (1982). Medicinal uses of ginseng and related plants in the Soviet Union: Recent trends in the Soviet literature. Journal of Ethnopharmacology, 6, 339–353.
Bardia, A., Nisly, N.L., Zimmerman, M.B., Gryzlak, B.M., & Wallace, R.B. (2007). Use of herbs among adults based on evidence-based indications: Findings from the National Health Interview Survey. Mayo Clinic Proceedings, 82, 561–566.
Barna, P. (1985). Food or drug? The case of ginseng [letter]. Lancet II, 2(8454), 548. Besso, H., Kasai, R., Wei, J., Wang, J-F., Saruwatari, Y-I., Fuwa, T., et al. (1982). Further
studies on dammarane-sapogenins of American ginseng, roots of Panax quinquefo-lium L. Chemical & Pharmaceutical Bulletin, 30, 4534–4538.
Brekman, I.I. (1965). Eleutherococcus senticosus: A new medicinal herb of the araliaceae family. In K.K. Chen & B. Mukerji (Eds.), Pharmacology of oriental plants (pp. 97–102). New York: MacMillan.
Cardinal, B.J., & Engels, H-J. (2001). Ginseng does not enhance psychological well-being in healthy, young adults: Results of a double-blind, placebo-controlled, randomized clinical trial. Journal of the American Dietetic Association, 101, 655–660.
Chase, P.J., Darby, L.A., Liang, M.T.C., & Morgan, A.I. (2000). Efficacy of Eleutherococ-cus senticosus (Siberian ginseng) as an ergogenic nutritional supplement [abstract]. Medicine and Science in Sports and Exercise, 32, S61.
Choi, K.T. (2008). Botanical characteristics, pharmacological effects and medicinal com-ponents of Korean Panax ginseng C.A. Meyer. Acta Pharmacologica Sinica, 29, 1109–1118.
Chong, S.K.F., & Oberholzer, V.G. (1988). Ginseng: Is there a use in clinical medicine? Postgraduate Medical Journal, 64, 841–846.
CNN.com/WORLD. (November 21, 2001). Korean root spawns riches, cancer cure claims. Available at http://asia.cnn.com/2001/WORLD/asiapcf/east/11/21/korea.ginseng.reut/index.html
Coon, J.T., & Ernst, E. (2002). Panax ginseng: A systematic review of adverse effects and drug interactions. Drug Safety, 25, 323–344.
Court, W.E. (1975). Ginseng: A Chinese folk medicine of current interest. Pharmacy Jour-nal, 214, 180–181.
Davydov, M., & Krikorian, A.D. (2000). Eleutherococcus senticosus (Rupr. & Maxim.) Maxim. (Araliaceae) as an adaptogen: A closer look. Journal of Ethnopharmacology, 72, 345–393.
Dragun, Z., Puntaric, D., Prpic-Majic, D., Bosnir, J., Gmajnic, R., & Klaric, M. (2003). Toxic metals and metalloids in dietetic products. Croatian Medical Journal, 44, 214–218.
Elyakov, G.B., Strigina, L.I., Uvarova, N.I., Vaskovasky, V.E., Dzizenko, A.E., & Kochet-kov, N.K. (1964). Glycosides from ginseng roots. Tetrahedron Letters, 5(48), 3591–3597.
Engelberg, D., McCutcheon, A., & Wiseman, S. (2001). A case of ginseng-induced mania. Journal of Clinical Psychopharmacology, 21, 535–536.
Engels, H-J., Fahlman, M.M., & Wirth, J.C. (2003). Effects of ginseng on secretory IgA, performance, and recovery from interval exercise. Medicine and Science in Sports and Exercise, 35, 690–696.
Engels, H-J., Kolokouri, I., Cieslak, T.J., & Wirth, J.C. (2001). Effects of ginseng supple-mentation on supramaximal exercise performance and short-term recovery. Journal of Strength and Conditioning Research, 15, 290–295.
Ernst, E. (2002). The risk-benefit profile of commonly used herbal therapies: Gingko, St. John’s wort, ginseng, echinacea, saw palmetto, and kava. Annals of Internal Medicine, 136, 42–53.

Is Ginseng an Ergogenic Aid? 319
Froiland, K., Koszewski, W., Hingst, J., & Kopecky, L. (2004). Nutritional supplement use among college athletes and their sources of information. International Journal of Sport Nutrition and Exercise Metabolism, 14, 104–120.
Gaffney, B.T., Hugel, H.M., & Rich, P.A. (2001a). The effects of Eleutherococcus sentico-sus and Panax ginseng on steroidal hormone indices of stress and lymphocyte subset numbers in endurance athletes. Life Sciences, 70, 431–442.
Gaffney, B.T., Hugel, H.M., & Rich, P.A. (2001b). Panax ginseng and Eleutherococcus senticosus may exaggerate an already existing biphasic response to stress via inhibi-tion of enzymes which limit the binding of stress hormones to their receptors. Medical Hypotheses, 56, 567–572.
Ginseng warning. (1997, December 19). USA Today, p. 3A.Goulet, E.D.B., & Dionne, I.J. (2005). Assessment of the effects of eleutherococcus senti-
cosus on endurance performance. International Journal of Sport Nutrition and Exer-cise Metabolism, 15, 75–83.
Gross, D., Shenkman, Z., Bleiberg, B., Dayan, B.M., Gittelson, M., & Efrat, R. (2002). Ginseng improves pulmonary functions and exercise capacity in patients with COPD. Monaldi Archives for Chest Disease, 57, 242–246.
Harkey, M.R., Henderson, G.L., Gershwin, M.E., Stern, J.S., & Hackman, R.M. (2001). Variability in commercial ginseng products: An analysis of 25 preparations. The American Journal of Clinical Nutrition, 73, 1101–1106.
Healing Herbs and Natural Remedies. (2008, April 15). Top selling herbal products in the U.S. Available at www.herbsandnaturalremedies.com/top-sellers.htm
Hon, C.C., Chow, Y.C., Zeng, F.Y., & Leung, F.C. (2003). Genetic authentication of ginseng and other traditional Chinese medicine. Acta Pharmacologica Sinica, 24, 841–846.
Hong, D.Y., Lau, A.J., Yeo, C.L., Liu, X.K., Yang, C.R., Kob, H.L., et al. (2005). Genetic diversity and variation of saponin contents in Panax notoginseng roots from a single farm. Journal of Agricultural and Food Chemistry, 53, 8460–8467.
Hou, J.P. (1977). The chemical constituents of ginseng plants. Comparative Medicine East and West, 5, 123–145.
Hsu, C.C., Ho, M.C., Lin, L.C., Su, B., & Hsu, M-C. (2005). American ginseng supple-mentation attenuates creatine kinase level induced by submaximal exercise in human beings. World Journal of Gastroenterology, 11, 5327–5331.
Hu, S.Y. (1976). The genus Panax (ginseng) in Chinese medicine. Economic Botany, 30, 11–28.
Iida, Y., Tanaka, O., & Shibata, S. (1968). Studies on saponins of ginseng: The structure of ginsenoside-Rg1. Tetrahedron Letters, 9(52), 5449–5453.
Iwabuchi, H., Yoshikura, M., Ikawa, Y., & Kamisako, W. (1987). Studies on the sesqui-terpenoids of Panax ginseng C.A. Meyer: Isolation and structure determination of sesquiterpene alcohols, panasinsanols A and B. Chemical & Pharmaceutical Bulletin, 35, 1975–1981.
Iwabuchi, H., Yoshikura, M., & Kamisako, W. (1988). Studies on the sesquiterpenoids of Panax ginseng C.A. Meyer II: Isolation and structure determination of ginsenol, a novel sesquiterpene alcohol. Chemical & Pharmaceutical Bulletin, 36, 2447–2451.
Kabalak, A.A., Soyal, O.B., Urfalioglu, A., Saracoglu, F., & Gogus, N. (2004). Menom-etrorrhagia and tachyarrhythmia after using oral and topical ginseng. Journal of Wom-en’s Health, 13, 830–833.
Kasai, R., Yamaguchi, H., & Tanaka, O. (1987). High-performance liquid chromatography of glycosides on a new type of hydoxyapatite column. Journal of Chromatography, 407, 205–210.
Kennedy, D.O., & Scholey, A.B. (2003). Ginseng: Potential for the enhancement of cognitive performance and mood. Pharmacology, Biochemistry, and Behavior, 75, 687–700.

320 Bahrke, Morgan, and Stegner
Kennedy, D.O., Scholey, A.B., Drewery, L., Marsh, L.R., Moore, B., & Ashton, H. (2003). Electroencephalograph effects of single doses of Ginkgo biloba and Panax ginseng in healthy young volunteers. Pharmacology, Biochemistry, and Behavior, 75, 701–709.
Kennedy, D.O., Scholey, A.B., & Wesnes, K.A. (2001a). Differential, dose dependent changes in cognitive performance following acute administration of a Ginkgo biloba/Panax ginseng combination to healthy young volunteers. Nutritional Neuroscience, 4, 399–412.
Kennedy, D.O., Scholey, A.B., & Wesnes, K.A. (2001b). Dose dependent changes in cog-nitive performance and mood following acute administration of ginseng to healthy young volunteers. Nutritional Neuroscience, 4, 295–310.
Kennedy, D.O., Scholey, A.B., & Wesnes, K.A. (2002). Modulation of cognition and mood following administration of single doses of Ginkgo biloba, ginseng, and a ginkgo/ginseng combination to healthy young adults. Physiology & Behavior, 75, 739–751.
Khan, I.A., Allgood, J., Walker, L.A., Abourashed, E.A., Schenk, D., & Benson, W.H. (2001). Determination of heavy metals and pesticides in ginseng products. Journal of AOAC International, 84, 936–939.
Kim, S.H., Park, K.S., Chang, M.J., & Sung, J.H. (2005). Effects of Panax ginseng extract on exercise-induced oxidative stress. Journal of Sports Medicine and Physical Fit-ness, 45, 178–182.
Kitts, D., & Hu, C. (2000). Efficacy and safety of ginseng. Public Health Nutrition, 3(4A), 473–485.
Korea promoting international food standard for ginseng. (2002, March 20). Korea Herald.
Krochmal, R., Hardy, M., Bowerman, S., Lu, Q-Y., Wang, H-J., Elashoff, R.M., et al. (2004). Phytochemical assays of commercial botanical dietary supplements. Evidence-Based Complementary and Alternative Medicine, 1, 305–313.
Kulaputana, O., Thanakomsirichot, S., & Anomasiri, W. (2007). Ginseng supplementation does not change lactate threshold and physical performances in physically active Thai men. Journal of the Medical Association of Thailand, 90, 1172–1179.
Liang, M.T.C., Podolka, T.D., & Chuang, W.J. (2005). Panax notoginseng supplementation enhances physical performance during endurance exercise. Journal of Strength and Conditioning Research, 19, 108–114.
Liberti, L.E., & Der Marderosian, A. (1978). Evaluation of commercial ginseng products. Journal of Pharmaceutical Sciences, 67, 1487–1489.
Lieberman, H.R. (2001). The effects of ginseng, ephedrine, and caffeine on cognitive per-formance, mood, and energy. Nutrition Reviews, 59, 91–102.
Lim, W., Mudge, K.W., & Vermeylen, F. (2005). Effects of population, age, and cultivation methods on ginsenoside content of wild American ginseng (Panax quinquefolium). Journal of Agricultural and Food Chemistry, 53, 8498–8505.
Martinez-Mir, I., Rubio, E., Morales-Olivas, F.J., & Palop-Larrea, V. (2004). Transient ischemic attack secondary to hypertensive crisis related to Panax ginseng. The Annals of Pharmacotherapy, 38, 1970.
Matsuda, H., Namba, K., Fukuda, S., Tani, T., & Kubo, M. (1986). Pharmacological study on Panax ginseng C.A. Meyer: III. Effects of red ginseng on experimental dissemi-nated intravascular coagulation. (2) Effects of ginsenosides on blood coagulative and fibrinolytic systems. Chemical & Pharmaceutical Bulletin, 34, 1153–1157.
Palanisamy, A., Halter, C., & Olson, K.R. (2003). Photosensitivity reaction in a woman using an herbal supplement containing ginseng, goldenseal, and bee pollen. Journal of Toxicology. Clinical Toxicology, 41, 865–867.
Palisin, T.E., & Stacy, J.J. (2006). Ginseng: Is it the root? Current Sports Medicine Reports, 5, 210–214.
Palop-Larrea, V., Gonzalvez-Perales, J.L., Catalan-Oliver, C., Belenguer-Varea, A., & Martinez-Mir, I. (2000). Metrorrhagia and ginseng. The Annals of Pharmacotherapy, 34, 1347–1348.

Is Ginseng an Ergogenic Aid? 321
Petkov, V.D., Yinglin, C., Todorov, I., Lazarova, M., Getova, D., Stancheva, S., et al. (1992). Behavioral effects of stem-leaves extract from Panax ginseng C.A. Meyer. Acta Physiologica et Pharmacologica Bulgarica, 18, 41–48.
Petroczi, A., & Naughton, D.P. (2008). The age-gender-status profile of high performing athletes in the UK taking nutritional supplements: Lessons for the future. Journal of the International Society of Sports Nutrition, 5, 2. Retrieved from http://www.jissn.com/content/5/1/2
Phillipson, J.D., & Anderson, L.A. (1984). Ginseng: Quality, safety, and efficacy? Pharma-ceutical Journal, 232, 161–165.
Pietta, P., Mauri, P., & Rava, A. (1986). Improved high-performance liquid chromato-graphic method for the analysis of ginsenosides in Panax ginseng extracts and prod-ucts. Journal of Chromatography, 356, 212–219.
Popov, I.M., & Goldwag, W.J. (1973). A review of the properties and clinical effects of ginseng. The American Journal of Chinese Medicine, 1, 263–270.
PRWeb Press Release Newswire. (2008, February 25). World herbal supplements and rem-edies market to reach US$22.9 billion by 2010, according to new report by Global Industry Analysts, Inc. Available at www.prweb.com/releases/herbal_supplements/herbal_remedies/prweb707734.htm
Raman, P., Patino, L.C., & Nair, M.G. (2004). Evaluation of metal and microbial con-tamination in botanical supplements. Journal of Agricultural and Food Chemistry, 52, 7822–7827.
Reay, J.L., Kennedy, D.O., & Scholey, A.B. (2006). Effects of Panax ginseng, consumed with and without glucose, on blood glucose levels and cognitive performance during sustained “mentally demanding” tasks. Journal of Psychopharmacology (Oxford, England), 20, 771–781.
Scholey, A.B., & Kennedy, D.O. (2002). Acute, dose-dependent cognitive effects of Ginkgo biloba, Panax ginseng and their combination in healthy young volunteers: Differential interactions with cognitive demand. Human Psychopharmacology, 17, 35–44.
Shibata, S., Fujita, M., Itokawa, H., Tanaka, O., & Ishii, T. (1963). Studies on the constitu-ents of Japanese and Chinese crude drugs: XI. Panaxadiol, a sapogenin of ginseng roots. Chemical & Pharmaceutical Bulletin, 11, 759–761.
Shibata, S., Tanaka, O., Soma, K., Iida, Y., Ando, T., & Nakamura, H. (1965). Studies on saponins and sapogenins of ginseng: The structure of panaxatriol. Tetrahedron Let-ters, 6(3), 207–213.
Sievenpiper, J.L., Arnason, J.T., Vidgen, E., Leiter, L.A., & Vuksan, V. (2004). A system-atic quantitative analysis of the literature of the high variability in ginseng (Panax spp.): Should ginseng be trusted in diabetes? Diabetes Care, 27, 839–840.
Slater, G., Tan, B., & Teh, K.C. (2003). Dietary supplementation practices of Singapor-ean athletes. International Journal of Sport Nutrition and Exercise Metabolism, 13, 320–332.
Stavro, P.M., Woo, M., Heim, T.F., Leiter, L.A., & Vuksan, V. (2005). North American ginseng exerts a neutral effect on blood pressure in individuals with hypertension. Hypertension, 46, 406–411.
Sundgot-Borgen, J., Berglund, B., & Torstveit, M.K. (2003). Nutritional supplements in Norwegian elite athletes—Impact of international ranking and advisors. Scandinavian Journal of Medicine & Science in Sports, 13, 138–144.
Tanaka, O., Nagai, M., & Shibata, S. (1966). Chemical studies on the Oriental plant drugs: XVI. The stereochemistry of protopanaxadiol, a genuine sapogenin of ginseng. Chem-ical & Pharmaceutical Bulletin, 14, 1150–1156.
Tawab, M.A., Bahr, U., Karas, M., Wurglics, M., & Schubert-Zsilavecz, M. (2003). Deg-radation of ginsenosides in humans after oral administration. Drug Metabolism and Disposition: the Biological Fate of Chemicals, 31, 1065–1071.
U.S. Department of Agriculture. The Farm Security and Rural Investment Act of 2002—Public Law 107-17. Available at www.usda.gov/farmbill2002/
322 Bahrke, Morgan, and Stegner
Vazquez, I., & Aguera-Ortiz, L.F. (2002). Herbal products and serious side effects: A case of ginseng-induced manic episode. Acta Psychiatrica Scandinavica, 105, 76–77.
Vogler, B.K., Pittler, M.H., & Ernst, E. (1999). The efficacy of ginseng. A systematic review of randomised clinical trials. European Journal of Clinical Pharmacology, 55, 567–575.
Li, W., Gu, C., Zhang, H., Awang, D.V., Fitzloff, J.F., et al. (2000). Use of high-performance liquid chromatography-tandem mass spectrometry to distinguish Panax ginseng C.A. Meyer (Asian ginseng) and Panax quinquefolius L. (North American ginseng). Ana-lytical Chemistry, 72, 5417–5422.
Williams, L.O. (1957). Ginseng. Economic Botany, 11, 344–348.Wiwanitkit, V., & Taungjaruwinai, W. (2004). A case report of suspect ginseng
allergy. Medscape General Medicine, 6, 9. Retrieved from www.medscape.com/viewarticle/482833
Yamaguchi, H., Kasai, R., Matsuura, H., Tanaka, O., & Fuwa, T. (1988). High-performance liquid chromatographic analysis of acidic saponins of ginseng and related plants. Chemical & Pharmaceutical Bulletin, 36, 3468–3473.
Youl Kang, H., Hwan Kim, S., Jun Lee, W., & Byrne, H.K. (2002). Effects of ginseng ingestion on growth hormone, testosterone, cortisol, and insulin-like growth factor 1 responses to acute resistance exercise. Journal of Strength and Conditioning Research, 16, 179–183.
Yuan, C.S., Wang, X., Wu, J.A., Attele, A.S., Xie, J-T., & Gu, M. (2001). Effects of Panax quinquefolius L. on brainstem neuronal activities: Comparison between Wisconsin-cultivated and Illinois-cultivated roots. Phytomedicine, 8, 178–183.
Ziegler, P.J., Nelson, J.A., & Jonnalagadda, S.S. (2003). Use of dietary supplements by elite figure skaters. International Journal of Sport Nutrition and Exercise Metabolism, 13, 266–276.
Ziemba, A.W., Chmura, J., Kaciuba-Uscilko, H., Nazar, K., Wisnik, P., & Gawronski, W. (1999). Ginseng treatment improves psychomotor performance at rest and during graded exercise in young athletes. International Journal of Sport Nutrition, 9, 434–442.